")
Back to Journals » Patient Preference and Adherence » Volume 18
Barriers to Medication Adherence Among Patients with Non-Communicable Disease in North Wollo Zone Public Hospitals: Socio-Ecologic Perspective, 2023
Authors Fenta ET , Ayal BG, Kidie AA, Anagaw TF , Mekonnen TS, Ketema Bogale E , Berihun S, Tsega TD , Mengistie Munie C, Talie Fenta T, Kassie Worku N , Shiferaw Gelaw S, Tiruneh MG
Received 14 December 2023
Accepted for publication 11 March 2024
Published 22 March 2024 Volume 2024:18 Pages 733—744
DOI https://doi.org/10.2147/PPA.S452196
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Qizhi (Cathy) Yao
Eneyew Talie Fenta,1 Birtukan Gizachew Ayal,2 Atitegeb Abera Kidie,2 Tadele Fentabil Anagaw,3 Tesfaye Shumet Mekonnen,2 Eyob Ketema Bogale,3 Sileshi Berihun,1 Tilahun Degu Tsega,1 Chernet Mengistie Munie,4 Tizazu Talie Fenta,5 Nigus Kassie Worku,6 Sintayehu Shiferaw Gelaw,7 Misganaw Guadie Tiruneh8
1Department of Public Health, College of Medicine and Health Sciences, Injibara University, Injibara, Ethiopia; 2Department of Public Health, College of Medicine and Health Sciences, Woldia University, Woldia, Ethiopia; 3Department of Health Promotion and Behavioral Science, School of Public Health, College of Medicine and Health Sciences, Bahir Dar University, Bahir Dar, Ethiopia; 4Resource Mobilization Directorate, Amhara Regional health Bureau, Bahir Dar, Ethiopia; 5Department of Medical Laboratory Science, Gamby Medical and Business College, Bahir Dar, Ethiopia; 6Department of Public Health, College of Medicine and Health Science, Dire Dawa University, Dire Dawa, Ethiopia; 7Department of Public Health, College of Medicine and Health Science, Debre Markos University, Debre Markos, Ethiopia; 8Department of Health System and Policy, Institute of Public Health, College of Medicine and Health Science University of Gondar, Gondar, Ethiopia
Correspondence: Eneyew Talie Fenta, Email [email protected]
Background: The practice of taking medication as directed by a healthcare provider is known as medication adherence. Therefore, the application of a socio-ecological model to this study identifies multilevel factors on barriers of medication adherence on chronic non-communicable disease and provides information to develop scientific health communication interventional strategies to improve medication adherence.
Objective: This study aimed to explore barriers of medication adherence on non-communicable disease prevention and care among patients in North Wollo Zone public hospitals, northeast Ethiopia.
Methods: A phenomenological study design was carried out between February 5 and February 30, 2023. The study participants were chosen using a heterogeneous purposive sampling technique. In-depth interviews and targeted focus groups were used to gather data. The focus group discussions and in-depth interviews were captured on audio, accurately transcribed, and translated into English. Atlas TI-7 was utilized to do the thematic analysis.
Results: Four main themes, intrapersonal, interpersonal, community level, and health care related, as well as seven subthemes, financial problems, lack of family support, poor communication with healthcare providers, effects of social ceremonies, remote healthcare facility, and drug scarcity, were identified by this study. In this study participants reported that lack of knowledge about the disease and drugs were the main barrier for medication adherence. The study revealed that financial problems for medication and transportation cost were the main factor for medication adherence for non-communicable disease patients.
Conclusion: This study explored that lack of knowledge, financial problem, lack of family support, poor communication with healthcare providers, social ceremony effects, remote healthcare facility, and scarcity of drugs were barriers of medication adherence among non-communicable disease patients. In order to reduce morbidity and mortality from non-communicable diseases, it is advised that all relevant bodies look for ways to reduce medication adherence barriers for patients at every level of influence.
Keywords: medication adherence, socio-ecological model, non-communicable disease
Introduction
Adhering to a doctor’s prescription means taking medication as directed by the healthcare provider. Medication non-adherence is a worldwide issue that affects society at large as well as patients and doctors. According to data compiled by the World Health Organization (WHO), only about half of patients in high-income nations took their medications exactly as directed by a medical professional. The study found that non-adherence to prescribed medication accounted for 4.3% of all hospital admissions in North America, Europe, Asia, and Australia.1–4 Worldwide, non-communicable diseases (NCDs) are the primary causes of morbidity and mortality. In order to maintain optimal health outcomes, stop the onset and progression of complications, and enhance quality of life, treatment for NCDs typically involves long-term medication adherence.5–7
Genetic, physiological, environmental, and behavioral factors all play a role in the development of chronic diseases.8 Globally, more than 74% of deaths are caused by non-communicable diseases, which include chronic respiratory illnesses, cancer, diabetes, and cardiovascular disorders, and 85% of these deaths take place in developing nations. These NCDs have considerable behavioral risk factors that can be modified, such as cigarette use, poor diet, inactivity, and alcohol use, which result in overweight and obesity, elevated blood pressure and cholesterol levels, and ultimately, disease.8,9 The most commonly reported non-communicable diseases with poor prognosis in COVID-19 patients are diabetes mellitus (DM), hypertension, cerebrovascular disease, coronary artery disease, and chronic obstructive pulmonary disease (COPD). Patients with comorbidities are more likely to have severe disease and die as a result of their condition.10–12
The psychological and sociological elements of medication adherence include mistrust of pharmaceuticals, how they affect relationships with others and healthcare providers, self-efficacy, awareness of the need for the drug, and anxiety about its negative effects.13–16 Because symptoms worsen during exacerbations, poor adherence raises hospitalizations and morbidity. More than 95% of diabetes patients did not follow any of the five healthy lifestyle suggestions examined, according to the study. Studies show varying levels of adherence to diabetic medication, ranging from 38.5 to 93.1%.17–19 Chronic illness exacerbation, cardiovascular hazards, a lower quality of life, a higher rate of hospitalizations, higher healthcare expenses, and an earlier death rate were all related to poor adherence.20–24
The studies' findings indicate that non-adherence was significantly influenced by the perception of medication inefficacy, the use of herbal medicine, and the reliance on spiritual or spiritual healing,25 unavailability of medication,26 and the absence of social support.27 Factors associated with medication non-adherence among patients with non-communicable diseases (NCDs) included patients’ beliefs, lack of access to medications, cultural sensitivity, relationships with healthcare professionals, and forgetfulness and drug side effects. Other factors included feelings of hopelessness, withdrawal from social networks, and potential declines in cognitive functioning that may affect memory.28,29
Better treatment outcomes and appropriate glycemic control depend on patient involvement in decision-making, active patient engagement, goal-setting techniques, treatment strategies that are customized to the needs, beliefs, and abilities of the patient, and effective self-management beyond consultations.30–36 The improvement of medication adherence for chronic non-communicable diseases proved complicated and ineffective even with additional interventions. Patients and society at large bear a greater share of the expense of healthcare if patients fail to adhere to their prescribed regimen and do not experience the anticipated improvements in their health. A behavioral issue pertaining to the patient’s plan of action may be the cause of their non-adherence.34,37–40
Patients can obtain information from a variety of sources in case they lack the knowledge and comprehension necessary to make an informed choice on their condition or treatment. In order to manage several drugs and integrate them into daily life, patients must be motivated. On the other hand, unfavorable behavior and non-adherence to medication may result from individual factors as well as systemic and organizational impediments.41–44
The five levels of influence that the social ecological model (SEM) focuses on are as follows: intrapersonal factors for individual characteristics, such as developmental history, knowledge, attitudes, behavior, self-concept, and skills; interpersonal processes, such as social networks and support systems; community elements relate to links between organizations, institutions, and networks; institutional factors deal with social institutions and their organizational traits as well as norms and regulations for operation; and public policy factors deal with local, state, and federal laws and policies.45 To the best of our knowledge there is no study in the study area so that the application of a socio-ecological model to this study identifies multilevel factors on barriers of medication adherence on chronic non-communicable disease and provides information to develop scientific health communication interventional strategies to improve medication adherence.
Methods and Materials
Study Design, Area, and Period
North Wollo is 521 km from Addis Ababa and is in the Amhara region. In North Wollo, there are six government hospitals. These are Wadila Hospital, Mersa Hospital, Mekiet Hospital, Lalibela Hospital, Kobo Hospital, and Woldia Hospital. An institutional-based phenomenological study was conducted to investigate medication adherence barriers among patients with non-communicable diseases: socio-ecological perspective, 2023.
Study Population and Sampling Procedure
The study population were all adult chronic patients receiving follow-up care in three selected public hospitals, which were Woldia Referral Hospital, Meket General Hospital, and Kobo General Hospital of North Wollo Zone Amhara region. The study used purposive sampling to select study participants from each chronic disease follow-up clinic with diverse cases in each hospital. The zonal health office report indicated that the most common reported chronic NCDs were hypertension, diabetes mellites, cardiovascular disease, and epilepsy. This study included all chronic non-communicable disease (NCD) patients who were at least eighteen years old and enrolled in a particular public hospital. It did not include participants who were critically ill, incapable of communicating, in need of emergency care, or who had mental or cognitive impairment during the data collection period. Saturation of the data, at which point no new information was found, was used for determining the sample size.
Data Collection Tool and Procedure
The data were collected through In-depth interview, and focus group discussion. IDI, and FGD guides were drafted through reviewing different related literatures. Each interview was audiotaped using digital voice recorder. The interview guides were initially drafted in English and then translated into Amharic; the local language spoken in the region. After conducting the interviews in Amharic, the responses were translated back into English for analysis. This process ensures that language barriers are minimized, and participants can express themselves comfortably in their native language.
Data Quality Control
To maintain the credibility of the research, peer-debriefing was done for the questioner and transcripts were given to my colleagues, and member checking was conducted by returning the preliminary findings to some participants to correct errors and challenge what they perceive as wrong interpretations. Dependability was attained through accurate documentation by minimizing spelling errors through frequently observing data and including all documents in the final report, such as including the notes written during the interview. The data analysis, interpretations, and conclusions were continuously peer reviewed.46,47
Raw data, interview notes, and other documents were documented for cross-checking and audit trail purposes. Triangulation is the use of multiple data sources and was employed to enhance the confirmability of the findings. To maintain the transferability of the finding, appropriate probes were used to obtain detailed information on responses, and study participants were selected based on their specific purpose to answer study questions and to get greater in-depth findings.
Data Processing and Analysis
After data collection, the investigators transcribed the audio-record data into Amharic, local language, translated into English, and then read and re-read the several times to code the data, to detect emerging themes and subthemes. The translated document was coded line-by-line and grouped into themes based on the concepts they contain. Responses were categorized under each theme and subtheme. Interpretation of the data was dependent upon patients’ descriptions of their experiences and perceptions, which the researchers checked against the verbatim transcripts for accuracy and consistency. Lastly, the investigator was interpreting the themes to reveal core meanings of the experiences and presenting the discoveries of the study specifically, and the thematic analysis technique was used to analyze the data. Atlas Ti Software version 7 was used for data analysis.
Result
Socio-Demographic Information of the Participants
In this study 26 in-depth interviews with 3 focus group discussions were conducted. A total of 22 individuals with chronic diseases follow-up participated in FGD. The most frequently reported diseases were hypertension, diabetes, chronic heart disease, and epilepsy. The participants were 9 DM patients (Kobo 4, Meket 3, Woldia 2), 11 HTN (5 Kobo, 2 Meket, 4 Woldia), 3 epilepsy (2 Meket,1 Kobo), 3 CHF patients (Woldia 2, Meket 1), and totally 26 in-depth interviews were conducted. Also 22 FGD were conducted in three hospitals from Meket Hospital, 7 chronic disease patients (3 HTNl DM, bronchial asthma, epilepsy, CHF 1 each) participated. In Woldia Referral Hospital totally 6 participants (3 HTN, 2 DM, and 1 CHF), and in Kobo Hospital 9 NCD patients (DM4, HTN 3, bronchial asthma 1, and 1 CHF) were included in the study (Tables 1 and 2).
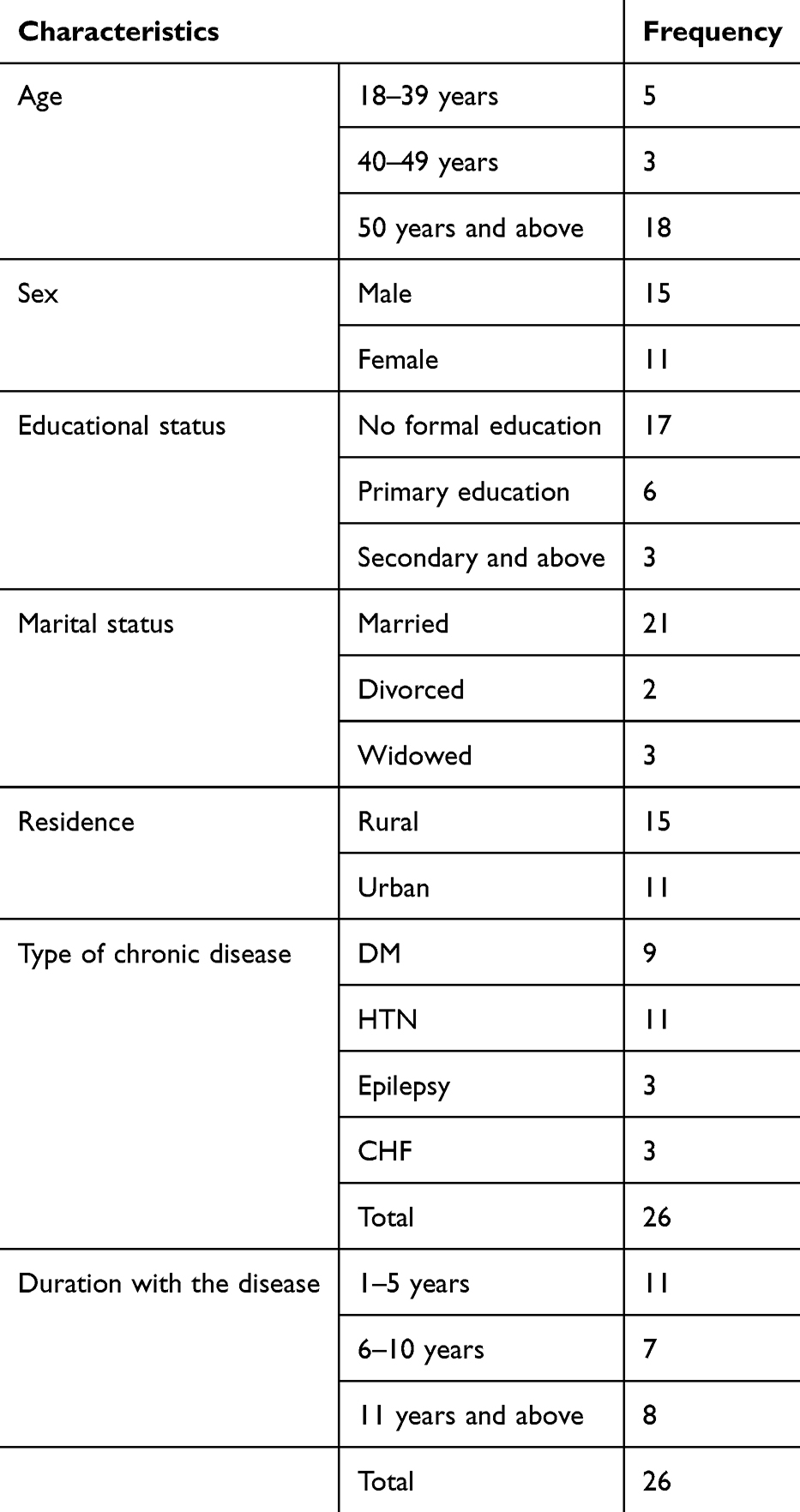 |
Table 1 Socio-Demographic Information on in-Depth Interviews to Explore Barriers to Medication Adherence Among Patients with Non-Communicable Disease in North Wollo Zone Public Hospitals |
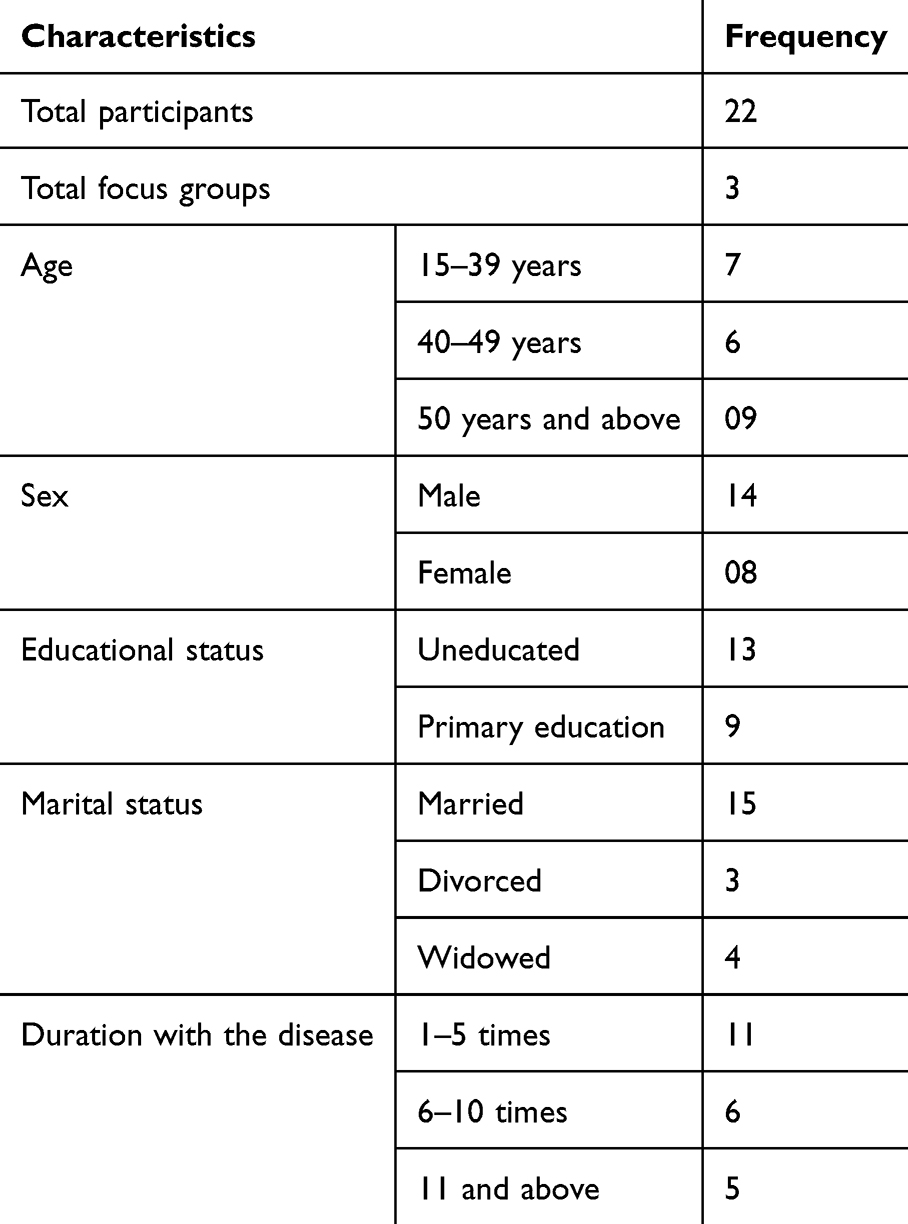 |
Table 2 Summary of Social Demographic Characteristics of the FGD Participants to Explore Barriers to Medication Adherence Among Patients with Non-Communicable Disease in North Wollo Zone Public Hospitals |
Thematic Findings
The findings that emerged from the analysis of the in-depth interview and focus group discussion were presented and arranged as major themes, subthemes, and categories. There are four4 main themes and seven7 subthemes (Figure 1).
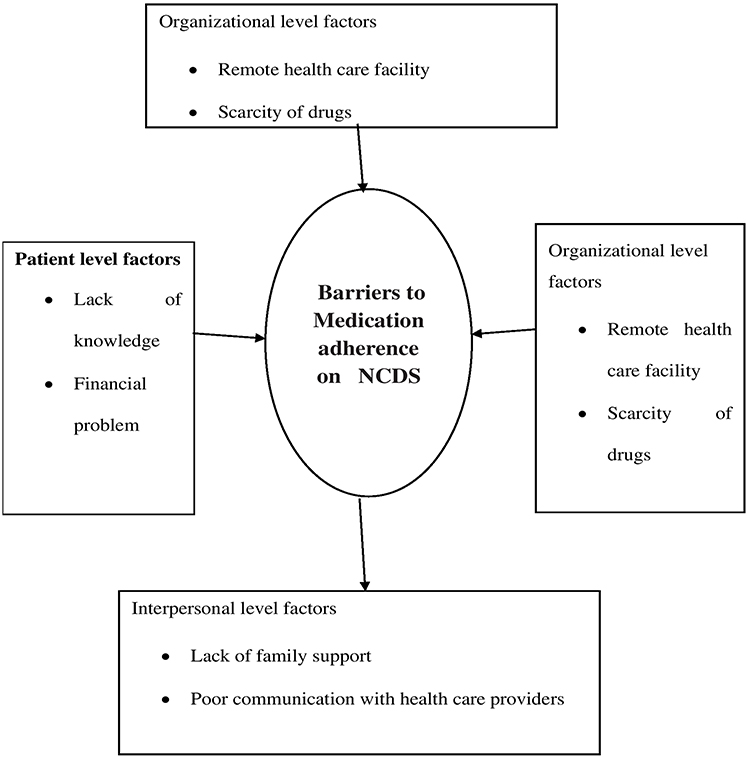 |
Figure 1 Flow chart of the study. |
Intra-Personal Factors
This theme has two subthemes which are lack of knowledge, and financial problem.
Lack of Knowledge
The participants reported that when they diagnosed and know their disease type at the first time, they had asked another person to know more about the drugs and how to take them. Even if most of the patients take their medication as prescribed by health professionals, some participants discussed that they did not take properly, were disappointed and forget it.
A 49-year-old male epileptic patient having a chronic follow up for 10 years said: “I did not know how to take the medicine before which made it difficult for me to control the disease”.
I am taking injection medication, but I cannot inject myself my child give me it, before one years he was not around me that made me discontinued the medication for eleven days. (60 years old, female with 7 years DM duration)
Male diabetic patient expressed as “since I have started the medication, I had taken it as prescribed by my doctor, but now I feel disappointed and don’t take regularly and sometimes forget it”. (29-year-old diabetic patient)
Female diabetic patient participated in FGD at hospital reported as: “The medicine is usually forgettable”.
Financial Problem
The patients explained that lack of money for transportation and to buy medication were the main problem face most non-communicable disease patients.
Male diabetic patient participated in FGD reported the drug cost when not available at government hospital as a barrier: “It is very difficult to buy the drug in private pharmacy. It is very expensive”.
I find it difficult to take more than one medication at once for my HIV, blood pressure, renal, and asthma. I also don’t have access to the hospital pharmacy and don’t have the money to buy all of my medications in private drug store. (60 years old, female, FGD participant)
I could not buy the medication timely because of expensiveness of medication and shortage of money. (77 years old, male DM patient with 4 years duration)
Inter-Personal Factors
This theme has two subthemes which are lack of family support, and poor communication with healthcare providers.
Lack of Family Support
Even if most chronic disease patients have good family support, some participants explored that they have no support from family. The participants also explained that since no one remindsthem, they forget their appointment and taking medication regularly. The following participant stated the same thing as:
I am tired of taking the medicine, the lack of support from the family, government, and the lack of money has become a severe problem for me. (Male, DM patient, age 61 years)
Another 49-year-old male epileptic patient having a chronic follow-up for 10 years explained that: “It’s hard for me to come, because of I am alone I’m afraid to fail, I used to forget my follow-up appointment. Now I come to hospital by calling”.
Poor Communication with Healthcare Providers
The study participants discussed that even if healthcare professionals provide health information about their disease status, they did not listen carefully, understand their need, and give time to ask questions and get feedback for their medication.
A hypertensive, female, 60-year-old patient with one year duration described as:
The health care professionals don’t give fair service to all equally, they don’t give enough health information for my disease mediation, it is better if they give full information on the disease and then written medicine information than oral.
Another HIV and hypertensive female participant reported as:
Since health care providers are busy, they did not care about me, except prescribing medication in my follow up, did not want to listen my complain and give advice by giving time is the main problem that I have to tell you.
Community Level Factors
Social Ceremony Effects
Even though most of the participants are committed to take their medication timely and take the recommended prevention practices, some participants explored that cultural traditions with in the family and social ceremonies enforce them to drink and eat the forbidden things that worsen their health condition. Another participant also described that when there were special ceremonies around their home, they had forgotten to take their medication, not taken it timely, and use alcohol and other foods not allowed for NCD patients.
The study participant explained as:
In our society, there are pressures to consume salty foods and alcoholic beverages at social events; there are occasional drug shortages; in my own negligence that I sometimes forget to take on time and at all. (DM patient, male, age 77 years)
Another female diabetic patient participated in FGD in also said:
when there was a wedding, I increased the amount of fat and sugar intake and my blood sugar became 400 in the last month. But now my blood sugar is 78 since I avoid taking these kinds of diet.
Healthcare Related Factors
This theme has two subthemes which are remote health care facility, and scarcity of drugs.
Scarcity of Drugs
The study showed that there is a shortage of drugs in the hospital and that patients are prone to extra expense to buy at private institutions:
Sometimes there is a shortage of medicines and laboratory resources, and I sometimes forget because of my negligence. (77 years old, DM patient).
A 39-year-old female hypertensive patient reported as:
The roads are not comfortable and the hospital is too far from the town. There is also a shortage of medicines, it is very expensive to buy drugs in private pharmacy.
Remote Healthcare Facility
The study participants described that distance of home from the hospitals and absence of comfortable roads to reach and get timely hospital care are the major obstacles. A male participant aged 54 years, diabetic and hypertensive patient, explored as: “I travelled on foot from a remote rural area and arrived too late to take medication for my follow-up appointment”.
Another 29-year-old, female cardiac patient reported as: “The roads are not comfortable and the hospital is too far from the town. It is not safe for me to reach and get treatment and appropriate health information”.
Lack of transportation and being at rural area makes me difficult to get health service and medication timely. (Hypertensive, 43-year-old patient)
Discussion
This study identified four4 main themes, intrapersonal factors, interpersonal factors, community level factors, health care related factors, and seven7 subthemes, lack of knowledge, financial problem, lack of family support, poor communication with healthcare providers, social ceremony effects, remote healthcare facility, and scarcity of drugs. Participants in this study stated that the biggest obstacle to medication adherence was ignorance regarding the illness and available medications. A few participants admitted to not taking their medications as prescribed and occasionally forgetting to do so. This aligned with research findings indicating that insufficient public awareness of the disease was a contributing factor to medication compliance.48,49
The other study likewise demonstrated that medication adherence and patient acceptance are negatively impacted by ignorance of standard treatment approaches.9 Medication adherence was hampered by forgetfulness and a lack of understanding about the condition and proper drug-taking practices.50,51 The study in China demonstrated that a major obstacle to medication adherence was patients’ ignorance of their prescriptions.52 The primary cause of poor drug adherence was a lack of understanding about the condition and the treatment.53 Participants in the Saudi Arabian study claimed that they had forgotten to take their prescriptions or did not comprehend the instructions, which prevented them from taking their drugs as prescribed.54
The study explored that financial problems for medication and transportation cost were the main factor for medication adherence for non-communicable disease patients. This was in line with the studies which discussed that poor socioeconomic status and high medication cost was influencing factor to poor medication adherence.52,55 According to the study conducted in Kenya, the two factors most strongly linked to inadequate medication adherence were transportation costs and population economic factors.56 A statistically significant correlation was found between the medication adherence of older patients and participants’ limited income in the Egyptian study.21 Another study in India revealed that lack of social support, financial constraints were barriers of medication adherence.20 The other studies also reported that lack of transportation costs to health facilities, individuals skip medication doses, take less medicine or delay filling their prescriptions due to cost and financial pressures, medication affordability secondary to financial constraints, and socioeconomic status were factors for poor drug adherence.57–60 A person’s overall health-related quality of life may suffer from low medication adherence, which can be caused by poor health behaviors and limited access to medical care in those with low socioeconomic level.61
The study also reported lack of family support, and poor communication with healthcare providers as the barrier for medication adherence. This was similar to the study in India that discussed that lack of social support, and improper rapport with healthcare professionals were factors associated with medication adherence.20 Perceived communication deficits among healthcare providers were documented in another study,62 poor communication within healthcare systems and lack of effective social support were the main factor for poor medication adherence.53,63,64 Studies found that inadequate family support is the strongest important factor in non-adherence to treatment in older adults with T2D.65 A study conducted in Saudi Arabia found a strong link between the degree of adherence and family assistance with medicine administration.66 Family support is helpful for both drug adherence and treatment.67 Stronger levels of social support and improved patient–physician relationships were associated with stronger medication adherence.68 Social support has been shown to lower stress, boost patients’ self-esteem, help them cope, and increase adherence to the treatment programme.69
This study explored that social ceremony has effects on medication adherence. Some participants explored that cultural traditions within the family and social ceremonies enforce them to drink and eat the forbidden things. This was comparable with the studies that explained that cultural norms, and cultural food preferences affect medication adherence.70 The studies also revealed that patients use alcohol for traditional ceremonies because friends persuaded them at social gatherings,71 culture has influences on diet management,72 and eating sugary food during festivals and social ceremonies has an effect on medication adherence.73
This research explored that a remote healthcare facility, and scarcity of drugs were factors associated with medication adherence. This finding was comparable with studies which stated that unavailability of drugs,74 lack of accessibility to healthcare,20 shortages in pharmacy supplies and limited accessibility in rural locations,75 and lack of access to medical facilities contribute to poor disease management among patients with diabetes.76 Medication adherence among patients with non-communicable diseases was hampered by the high cost of medications and the scarcity of NCD medications in public facilities.77,78
Strength and Limitations of the Study
The strength of this study was that the use of a phenomenology study design with the application of a socio-ecological model that could explore multilevel barriers of medication adherence on non-communicable disease prevention and care. These results cannot be automatically generalized to the entire population of patients with chronic non-communicable disease.
Conclusion
Four major themes were identified by this study: intrapersonal factors, interpersonal factors, community level factors, health care related factors; in addition, seven subthemes were identified: lack of knowledge, financial difficulties, lack of family support, poor communication with healthcare providers, effects of social ceremonies, remote healthcare facility, and scarcity of drugs/medicines.
Financial constraints related to medication and transportation costs were found to be the main factors influencing medication adherence in patients with non-communicable diseases. The research additionally discovered that the primary hindrances to medication adherence are lacking relationship with healthcare providers and insufficient family support. Some participants examined how familial traditions and social ceremonies force them to eat and drink things that are forbidden. This research showed that a remote healthcare facility, and scarcity of drugs were factors associated with medication adherence. Therefore, it is recommended that all the concerned bodies should work to avoid barriers of medication adherence on chronic non- communicable disease patients at each level of influence to decrease NCD morbidity and mortality.
Abbreviations
WHO, World Health Organization, NCD, non-communicable disease; HL, health literacy; HLL, health literacy level; DM, diabetes mellitus; CAD, cerebrovascular disease; COPD, chronic obstructive pulmonary disease; SEM, social ecological model.
Data Sharing Statement
The datasets used and/or analyzed during the current study available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Ethical clearance was obtained from Woldia University ethical review board with ethical review board protocol No WDU/IRB001/076. Written informed consent was obtained from each study participants including publication of anonymized responses. The study was conducted according to Helsinki Declaration.
Acknowledgment
We would like to acknowledge Woldia University, data collectors, and study participants.
Author Contributions
All authors made a significant contribution to the work reported, in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Woldia University.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. De Geest S, Sabaté E. Adherence to long-term therapies: evidence for action. Europ J Cardiovas Nurs. 2003;2(4):323.
2. Ho PM, Bryson CL, Rumsfeld J. Medication adherence: its importance in cardiovascular outcomes. Circulation. 2009;119(23):3028–3035. doi:10.1161/CIRCULATIONAHA.108.768986
3. Mongkhon P, Ashcroft DM, Scholfield CN, Kongkaew C. Hospital admissions associated with medication non-adherence: a systematic review of prospective observational studies. BMJ Qual Safet. 2018;27(11):902–914. doi:10.1136/bmjqs-2017-007453
4. Vrijens B, De Geest S, Hughes DA, et al. A new taxonomy for describing and defining adherence to medications. Br J Clin Pharmacol. 2012;73(5):691–705. doi:10.1111/j.1365-2125.2012.04167.x
5. Banatvala N, Bovet P. Noncommunicable Diseases: A Compendium. Taylor & Francis; 2023.
6. Han E, Suh D-C, Lee S-M, Jang S, Pharmacy A. The impact of medication adherence on health outcomes for chronic metabolic diseases: a retrospective cohort study. Res Soc Administ Pharm. 2014;10(6):e87–e98. doi:10.1016/j.sapharm.2014.02.001
7. Kanyongo W, Ezugwu AEJIi MU. Feature selection and importance of predictors of non-communicable diseases medication adherence from machine learning research perspectives. Informat Med Unlock. 2023;2023:101232.
8. World Health Organization. Noncommunicable Diseases Progress Monitor 2022. World Health Organization; 2022.
9. Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3(11):e442. doi:10.1371/journal.pmed.0030442
10. Wang D, Hu B, Hu C, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. JAMA. 2020;323(11):1061–1069.
11. Li Z, Shi J, Li N, et al. Temporal trends in the burden of non-communicable diseases in countries with the highest malaria burden, 1990–2019: evaluating the double burden of non-communicable and communicable diseases in epidemiological transition. JAMA. 2022;18(1):1–9.
12. Hegelund MH, Fjordside L, Faurholt‐Jepsen D, Christensen DL, Bygbjerg IC. Opportunistic non‐communicable diseases in times of COVID‐19. APMIS. 2023;131(1):13–18. doi:10.1111/apm.13274
13. Blaakman SW, Cohen A, Fagnano M, Halterman JSJJo A. Asthma medication adherence among urban teens: a qualitative analysis of barriers, facilitators and experiences with school-based care. J Asthma. 2014;51(5):522–529. doi:10.3109/02770903.2014.885041
14. Maghsoudi Z, Sadeghi A, Oshvandi K, Ebadi A, Tapak LJJo GN. Barriers to treatment adherence among older adults with type 2 diabetes: a qualitative study. J Gerontol Nurs. 2023;49(1):42–49. doi:10.3928/00989134-20221206-04
15. Nies YH, Ali AM, Abdullah N, Islahudin F, Shah N. A qualitative study among breast cancer patients on chemotherapy: experiences and side-effects. Pat Pref Adhere. 2018;12:1955–1964. doi:10.2147/PPA.S168638
16. Wan BK, Cheung WH, Ball PA, Jackson DM, Maynard GJJIJo PP. Beliefs about medicines among Hong Kong hospital outpatients. Internat J Pharm Pract. 2017;25(6):447–453. doi:10.1111/ijpp.12353
17. King DE, Mainous AG, Carnemolla M, Everett C. Adherence to healthy lifestyle habits in US adults, 1988-2006. Am J Med. 2009;122(6):528–534. doi:10.1016/j.amjmed.2008.11.013
18. Krass I, Schieback P, Dhippayom T. Adherence to diabetes medication: a systematic review. Diab Med. 2015;32(6):725–737. doi:10.1111/dme.12651
19. Vestbo J, Anderson JA, Calverley PM, et al. Adherence to inhaled therapy, mortality and hospital admission in COPD. Thorax. 2009;64(11):939–943. doi:10.1136/thx.2009.113662
20. Abaka MK, Chinemerem EE, Rejimon PM, et al. Medication adherence: gaining insights on patient-reported facilitators and barriers; 2023.
21. Ahmed EH, Abdel-Aziz HR, Ahmed S. Medication adherence and its influencing factors in community-dwelling older adults with chronic illnesses in a rural area. Nursing Practice Today. 2023. doi:10.18502/npt.v10i3.13434
22. Barr EL, Zimmet PZ, Welborn TA, et al. Risk of cardiovascular and all-cause mortality in individuals with diabetes mellitus, impaired fasting glucose, and impaired glucose tolerance: the Australian Diabetes, Obesity, and Lifestyle Study (AusDiab). Circulation. 2007;116(2):151–157.
23. Kasahun AE, Sendekie AK, Mekonnen GA, et al. Impact of personal, cultural and religious beliefs on medication adherence among patients with chronic diseases at university hospital in northwest Ethiopia. Pat Prefer Adhere. 2022;16:1787–1803. doi:10.2147/PPA.S370178
24. Wilson DH, Rein LJ, Fountain M, Brookhart A, Atchley D, Hohmeier K. A pilot study exploring the impact of a primary medication non-adherence intervention among four chronic disease states in one regional division of a large community pharmacy chain. Pharmacy. 2023;11(1):11. doi:10.3390/pharmacy11010011
25. Atinga RA, Yarney L, Gavu N. Factors influencing long-term medication non-adherence among diabetes and hypertensive patients in Ghana: a qualitative investigation. PLoS One. 2018;13(3):e0193995. doi:10.1371/journal.pone.0193995
26. Lulebo AM, Mutombo PB, Mapatano MA, et al. Predictors of non-adherence to antihypertensive medication in Kinshasa, democratic republic of congo: a cross-sectional study. BMC Res Note. 2015;8(1):1–8.
27. Lemstra M, Nwankwo C, Bird Y, Moraros J. Primary nonadherence to chronic disease medications: a meta-analysis. Pat Prefere Adhere. 2018;12:721–731. doi:10.2147/PPA.S161151
28. Wu J-R, Lennie TA, Dekker RL, Biddle MJ, Moser DK. Medication adherence, depressive symptoms, and cardiac event–free survival in patients with heart failure. J Card Fail. 2013;19(5):317–324. doi:10.1016/j.cardfail.2013.03.010
29. Malaeb D, Sacre H, Mansour S, et al. Assessment of medication adherence among Lebanese adult patients with non-communicable diseases during COVID-19 lockdown: a cross-sectional study. Front Pub Health. 2023;11:1145016. doi:10.3389/fpubh.2023.1145016
30. Amer MAK, Mohiuddin SI, Shafeeque Shaikh D. Enhancing medication adherence in chronic patients. Saudi J Med Pharm Sci. 2023;9(6):346–351.
31. Bhattarai B, Walpola R, Mey A, Anoopkumar-Dukie S, Khan S. Barriers and strategies for improving medication adherence among people living with COPD: a systematic review. Respirat Care. 2020;65(11):1738–1750. doi:10.4187/respcare.07355
32. Delamater AM. Improving patient adherence. Clinical Diabetes. 2006;24(2):71–77.
33. García-Pérez L-E, Álvarez M, Dilla T, Gil-Guillén V, Orozco-Beltrán D. Adherence to therapies in patients with type 2 diabetes. Diabet Thera. 2013;4(2):175–194. doi:10.1007/s13300-013-0034-y
34. Nieuwlaat R, Wilczynski N, Navarro T, et al. Interventions for enhancing medication adherence. Coch Datab System Rev. 2014;2014(11). doi:10.1002/14651858.CD000011.pub4
35. Peng Y, Wang H, Fang Q, et al. Effectiveness of mobile applications on medication adherence in adults with chronic diseases: a systematic review and meta-analysis. J Manag Care. 2020;26(4):550–561. doi:10.18553/jmcp.2020.26.4.550
36. Tolley A, Hassan R, Sanghera R, et al. Interventions to promote medication adherence for chronic diseases in India: a systematic review. Front Public Health. 2023;11:1194919.
37. Amankwaa I, Boateng D, Quansah DY, Akuoko CP, Evans C. Effectiveness of short message services and voice call interventions for antiretroviral therapy adherence and other outcomes: a systematic review and meta-analysis. PLoS One. 2018;13(9):e0204091.
38. Cutler RL, Fernandez-Llimos F, Frommer M, Benrimoj C, Garcia-Cardenas V. Economic impact of medication non-adherence by disease groups: a systematic review. BMJ Open. 2018;8(1):e016982. doi:10.1136/bmjopen-2017-016982
39. Haynes R, Ackloo E, Sahota N, McDonald H, Yao X. Interventions for enhancing medication adherenceCochrane. Database Syst Rev. 2008;2008:1.
40. Roebuck MC, Liberman JN, Gemmill-Toyama M, Brennan TA. Medication adherence leads to lower health care use and costs despite increased drug spending. Health Aff. 2011;30(1):91–99. doi:10.1377/hlthaff.2009.1087
41. Carpenter DM, DeVellis RF, Fisher EB, et al. The effect of conflicting medication information and physician support on medication adherence for chronically ill patients. Pat Educ Counsel. 2010;81(2):169–176. doi:10.1016/j.pec.2009.11.006
42. Hawes EM, Sanders KA. Medication management and treatment adherence. In: Chronic Illness Care: Principles and Practice. Springer; 2023:181–193.
43. Herrera PA, Moncada L, Defey D. Understanding non-adherence from the inside: hypertensive patients’ motivations for adhering and not adhering. Qualit Health Res. 2017;27(7):1023–1034. doi:10.1177/1049732316652529
44. Zairina E, Nugraheni G, Sulistyarini A, et al. Factors related to barriers and medication adherence in patients with type 2 diabetes mellitus: a cross-sectional study. J Diab Metab Dis. 2022;21(1):219–228. doi:10.1007/s40200-021-00961-6
45. McLeroy KR, Bibeau D, Steckler A, Glanz K. An ecological perspective on health promotion programs. Health Educ Quart. 1988;15(4):351–377. doi:10.1177/109019818801500401
46. Denzin NK, Lincoln YS. Introduction: the discipline and practice of qualitative research. Hand Qualit Res. 2000;2(1):1–20.
47. Tolley EE, Ulin PR, Mack N, Robinson ET, Succop SM. Qualitative Methods in Public Health: A Field Guide for Applied Research. John Wiley & Sons; 2016.
48. Berek PA, Siswanto BB, Irawati D, Jatmiko W. Individual characteristics, adherence, and barriers to medication adherence of hypertensive patients at the Indonesia-timor leste border. Nurs Med J Nurs. 2022;12:3.
49. O’Donnell M, Hankey GJ, Rangarajan S, et al. Variations in knowledge, awareness and treatment of hypertension and stroke risk by country income level. Heart. 2021;107(4):282–289.
50. Baiardini I, Rogliani P, Santus P, et al. Disease awareness in patients with COPD: measurement and extent. Internat J Chron Obstruc Pulm Dis. 2018;14:1–11. doi:10.2147/COPD.S179784
51. Berhane Y, Worku A. Adherence to antihypertensive treatment and associated factors in central Ethiopia. Internat J Hypert. 2020;2020:1.
52. Ni Z, Dardas L, Wu B, Shaw R. Cardioprotective medication adherence among patients with coronary heart disease in China: a systematic review. Heart Asia. 2019;11:2.
53. Kvarnström K, Airaksinen M, Liira H. Barriers and facilitators to medication adherence: a qualitative study with general practitioners. BMJ Open. 2018;8(1):e015332. doi:10.1136/bmjopen-2016-015332
54. Alosaimi K, Alwafi H, Alhindi Y, et al. Medication adherence among patients with chronic diseases in Saudi Arabia. Internat J Environ Res Public Health. 2022;19(16):10053. doi:10.3390/ijerph191610053
55. Yap AF, Thirumoorthy T, Kwan Y. Systematic review of the barriers affecting medication adherence in older adults. Geriat Gerontol Internat. 2016;16(10):1093–1101. doi:10.1111/ggi.12616
56. Gala P, Kamano JH, Sanchez MV, et al. Cross-sectional analysis of factors associated with medication adherence in western Kenya. BMJ Open. 2023;13(9):e072358. doi:10.1136/bmjopen-2023-072358
57. Macquart de Terline D, Kane A, Kramoh KE, et al. Factors associated with poor adherence to medication among hypertensive patients in twelve low and middle income Sub-Saharan countries. PLoS One. 2019;14(7):e0219266. doi:10.1371/journal.pone.0219266
58. Morgan SG, Lee A. Cost-related non-adherence to prescribed medicines among older adults: a cross-sectional analysis of a survey in 11 developed countries. BMJ Open. 2017;7(1):e014287. doi:10.1136/bmjopen-2016-014287
59. Mebrahtu G, M Moleki M, Okoth Achila O, et al. Antihypertensive medication adherence and associated factors: a cross-sectional analysis of patients attending a National Referral Hospital in Asmara, Eritrea. Patient Pref Adhere. 2021;2021:2619–2632.
60. De Avila JL, Meltzer DO, Zhang J. Prevalence and persistence of cost-related medication nonadherence among Medicare beneficiaries at high risk of hospitalization. JAMA Network Open. 2021;4(3):e210498–e. doi:10.1001/jamanetworkopen.2021.0498
61. Hong J, Kim G. Difference in health-related quality of life between medical aid beneficiaries and health insurance beneficiaries using the community health survey. J Korea Cont Assoc. 2016;16(5):477–487.
62. Yoon S, Kwan YH, Yap WL, et al. Factors influencing medication adherence in multi-ethnic Asian patients with chronic diseases in Singapore: a qualitative study. Front Pharmacol. 2023;14:1124297. doi:10.3389/fphar.2023.1124297
63. Nielsen JØ, Shrestha A, Neupane D, Kallestrup P. Non-adherence to anti-hypertensive medication in low-and middle-income countries: a systematic review and meta-analysis of 92443 subjects. J Hum Hypert. 2017;31(1):14–21. doi:10.1038/jhh.2016.31
64. Xu J, Zhao M, Vrosgou A, et al. Barriers to medication adherence in a rural-urban dual economy: a multi-stakeholder qualitative study. BMC Health Serv Res. 2021;21:1–9.
65. Olagbemide OJ, Omosanya OE, Ayodapo AO, Agboola SM, Adeagbo AO, Olukokun TA. Family support and medication adherence among adult type 2 diabetes: any meeting point? Anna Afr Med. 2021;20(4):282. doi:10.4103/aam.aam_62_20
66. Alhabib MY, Alhazmi TS, Alsaad SM, AlQahtani AS, Alnafisah A. Medication adherence among geriatric patients with chronic diseases in Riyadh, Saudi Arabia. Patient Prefere Adhere. 2022;16:2021–2030. doi:10.2147/PPA.S363082
67. Shruthi R, Jyothi R, Pundarikaksha H, Nagesh G, Tushar T. A study of medication compliance in geriatric patients with chronic illnesses at a tertiary care hospital. J Clin Diagn Res. 2016;10(12):FC40. doi:10.7860/JCDR/2016/21908.9088
68. Al-Noumani H, Alharrasi M, Lazarus ER, Panchatcharam SM. Factors predicting medication adherence among Omani patients with chronic diseases through a multicenter cross-sectional study. Scient Rep. 2023;13(1):7067. doi:10.1038/s41598-023-34393-4
69. Krishnamoorthy Y, Rajaa S, Rehman T, Thulasingam M. Patient and provider’s perspective on barriers and facilitators for medication adherence among adult patients with cardiovascular diseases and diabetes mellitus in India: a qualitative evidence synthesis. BMJ Open. 2022;12(3):e055226. doi:10.1136/bmjopen-2021-055226
70. Henry Osokpo O, James R, Riegel B. Maintaining cultural identity: a systematic mixed studies review of cultural influences on the self‐care of African immigrants living with non‐communicable disease. J Advan Nurs. 2021;77(9):3600–3617. doi:10.1111/jan.14804
71. Numsang P, Oumtanee A, Kurat S, Sananok R, Kraichan S, Sarapoke P. “Failure to control blood sugar” experiences of persons with type 2 diabetes mellitus. Internat J Nurs Sci. 2023;10:527–532. doi:10.1016/j.ijnss.2023.09.004
72. Sari Y, Yusuf S, Kusumawardani LH, Sumeru A, Sutrisna EJH. The cultural beliefs and practices of diabetes self-management in Javanese diabetic patients: an ethnographic study. Heliyon. 2022;8(2). doi:10.1016/j.heliyon.2022.e08873
73. Pardhan S, Upadhyaya T, Smith L, et al. Individual patient-centered target-driven intervention to improve clinical outcomes of diabetes, health literacy, and self-care practices in Nepal: a randomized controlled trial. Front Endocrinol. 2023;14:1076253. doi:10.3389/fendo.2023.1076253
74. Konstantinou P, Kassianos AP, Georgiou G, et al. Barriers, facilitators, and interventions for medication adherence across chronic conditions with the highest non-adherence rates: a scoping review with recommendations for intervention development. Translat Behav Med. 2020;10(6):1390–1398. doi:10.1093/tbm/ibaa118
75. Wilkinson R, Garden E, Nanyonga RC, et al. Causes of medication non-adherence and the acceptability of support strategies for people with hypertension in Uganda: a qualitative study. Internat J Nurs Stud. 2022;126:104143. doi:10.1016/j.ijnurstu.2021.104143
76. Kvarnström K, Westerholm A, Airaksinen M, Liira HJP. Factors contributing to medication adherence in patients with a chronic condition: a scoping review of qualitative research. Pharmaceutics. 2021;13(7):1100. doi:10.3390/pharmaceutics13071100
77. Vialle-Valentin CE, Serumaga B, Wagner AK, Ross-Degnan D. Evidence on access to medicines for chronic diseases from household surveys in five low-and middle-income countries. Health Pol Plann. 2015;30(8):1044–1052. doi:10.1093/heapol/czu107
78. Tusubira AK, Akiteng AR, Nakirya BD, et al. Accessing medicines for non-communicable diseases: patients and health care workers’ experiences at public and private health facilities in Uganda. PLoS One. 2020;15(7):e0235696. doi:10.1371/journal.pone.0235696
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.