")
Back to Journals » International Journal of General Medicine » Volume 17
Association of Regular Cervical Cancer Screening with Socioeconomic, COVID-19 Infection and Vaccine Status Among Japanese Population: Cohort Observational Study
Authors Mitoma T , Maki J, Ooba H , Ogawa C, Masuyama H, Tabuchi T
Received 6 December 2023
Accepted for publication 7 February 2024
Published 13 February 2024 Volume 2024:17 Pages 541—551
DOI https://doi.org/10.2147/IJGM.S453675
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Tomohiro Mitoma,1 Jota Maki,1 Hikaru Ooba,1 Chikako Ogawa,1 Hisashi Masuyama,1 Takahiro Tabuchi2
1Department of Obstetrics and Gynecology, Okayama University Graduate School of Medicine Dentistry and Pharmaceutical Sciences, Okayama, Japan; 2Department of Cancer Control Center, Osaka International Cancer Institute, Osaka, Japan
Correspondence: Jota Maki, Department of Obstetrics and Gynecology, Okayama University Graduate School of Medicine Dentistry and Pharmaceutical Sciences, 2-5-1 Shikata-cho, Kita-ku, Okayama, 700-8558, Japan, Tel +81-86-235-7320, Fax +81-86-225-9570, Email [email protected]
Purpose: Among the Organisation for Economic Co-operation and Development countries, Japan has one of the lowest cervical cancer screening coverages. Cancer screening coverage has worsened due to the coronavirus disease of 2019 (COVID-19) pandemic. This study investigated the relationship between socioeconomic background, COVID-19 infection history and vaccine status, and regular cervical cancer screening (CCS) during the two years of the COVID-19 era in Japan.
Patients and Methods: We used data from the Japan COVID-19 and Society Internet Survey, a nationwide, Internet-based, self-report cohort observational study conducted in 2022. The outcome variable was identified by asking whether the participants had undergone CCS within the last two years. Cervical cytology was performed in Japan by brushing the external cervical os. This study used multivariate log-binomial regression models to evaluate inequalities during regular checkups for CCS. Adjusted prevalence ratios (APRs) with 95% confidence intervals (CIs) were estimated to incorporate the socioeconomic background variables.
Results: Of the 12,066 participants, 5597 (46.4%) had undergone regular CCS for over two years. The prevalence ratio (PR) of patients who underwent CCS was 0.70 for those in their 20s and 0.78 for those in their 60s, compared to those in their 40s. Socioeconomic inequities were found in the following groups: unemployed/student, unmarried, high school graduate or lower, and household income below 4 million Yen. Our final multivariate analysis revealed that participants who were in their 20s or 60s, had a household income below 4 million Yen, were unmarried, had no annual health check-ups, and were unvaccinated with COVID-19 were at a higher risk of not undergoing CCS.
Conclusion: The relationship between socioeconomic inequality and CCS hesitancy is prevalent among younger participants. The CCS coverage in Japan during the COVID-19 pandemic year (2020– 2022) was not low compared with the pre-pandemic era.
Keywords: cervical cancer screening, social inequality, screening hesitation, internet survey
Introduction
Cervical cancer screening (CCS) significantly reduces the mortality rate of cervical cancer.1 Screening once every two years is recommended for those over 20 years old by Japan’s Ministry of Health, Labor, and Welfare. Among the Organization for Economic Co-operation and Development (OECD) countries, Japan has one of the lowest CCS screening coverages, approximately half of the rate in the United States (US) and 70–80% lower than that in European countries.2,3 The rate in 2019 was 43%, approximately 6% higher than that in 2010. However, only approximately 40% of women currently undergo regular checkups.3 Furthermore, it is estimated that cervical cancer deaths will increase by as much as 10,000 by 2069 due to withholding the Human Papilloma Virus (HPV) vaccine in Japan.4 Although Japan’s medical system provides access to medical facilities,5 there is still some CCS hesitancy. In Japan, the subsidy amount varies depending on the municipality of residence, but eligible individuals receive discounted screening coupons, allowing them to participate in CCS at a cost of approximately 500 to 1000 Yen. However, public surveys of general companies have identified time and financial problems as reasons for CCS hesitancy. Many published studies on the subject are questionnaire-based descriptive reports.6,7 These have also been largely based on psychological approaches. Two of the top three responses in this study were “Because I am confident in my health condition and do not feel the need” and “Because I can visit a medical facility whenever I am worried.” Moreover, criticism of obstetrics and gynecology visits from participants’ acquaintances and resistance to consultations by male physicians were identified as social challenges that needed to be addressed. However, few studies have considered the social backgrounds of those who did not undergo the test.8
The impact of coronavirus disease-19 (COVID-19) was significant in Japan. The first declaration of a state of emergency was issued in March 2020, followed by “stay-at-home restrictions” for approximately 2.5 years until the fourth declaration was lifted in September 2022.9 Regarding cancer screening and withholding of medical examinations because of the COVID-19 pandemic, the US National Cancer Institute reported in 2020 that the COVID-19 pandemic significantly affected the uptake rate for cancer screening in the U.S.10 Reports from Japan have also indicated that people refrained from undergoing cancer screenings during the pandemic, particularly in urban areas.11 Moreover, people with COVID-19 tend to refrain from going out even after their symptoms have improved,12 which may make it even more challenging to undergo cancer screenings before and after infection. Although there have been reports regarding the cancer screening coverage under conditions involving behavioral restrictions,13,14 such as during states of emergency, there have been no reports thus far on the CCS coverage during the 2-year COVID-19 pandemic in Japan. Furthermore, there are no reports on socioeconomic inequality in Japan as a cause of low screening coverage during the period of the significant societal changes that took place in the country during and following the COVID-19 pandemic.
This study aimed to analyze the relationship between socioeconomic background, the COVID-19 infection history and vaccine status, and regular cervical cancer screening (CCS) participants during the two years of COVID-19 pandemic era in Japan. Furthermore, by identifying issues related to CCS in Japan, this study will hopefully aid the Japanese government in formulating new policies to improve CCS coverage.
Materials and Methods
Study Setting and Population
The Japan COVID-19 and Society Internet Survey (JACSIS) is a nationwide, Internet-based, self-reported observational cohort study. It was conducted to assess social and health inequalities related to COVID-19. Similar studies have been ongoing since 2020.11,15–17 These surveys were managed by a nationwide internet research company, Rakuten Insight, which enrolled and recorded demographic information for 2.3 million registered candidates. This study was conducted using data from JACSIS 2022, a general population survey conducted between September and October 2022. The participants were randomly selected according to sex, age, and place of residence. An invitation to participate was sent via e-mail. The participants provided their consent, accessed the designated website, and responded to the survey. They had the option of either not responding to any portion of the survey or discontinuing it entirely. The survey was closed when the target number (32,000) of participants for each sex, age, and prefecture was met. To maintain data quality, invalid responses were excluded. Inconsistent responses were defined as follows: (1) choosing an invalid response without following specified instructions, for example, “Please select the second item from the bottom”; (2) checking all items regarding drug use such as “Are you currently drinking or using alcohol or drugs, that is, marijuana, cocaine, or heroin?”; and (3) checking all items for “having 20 underlying chronic diseases.” Details of the algorithms, excluding invalid responses, have been provided in a previous study.11,15–17 Of 32,000 total participants, 3370 with fraudulent responses were excluded. In total, 28,630 participants were included in this study. Of these, women, females at birth, and 20–69-year-olds were selected, resulting in a final sample of 12,066 participants (Figure 1).
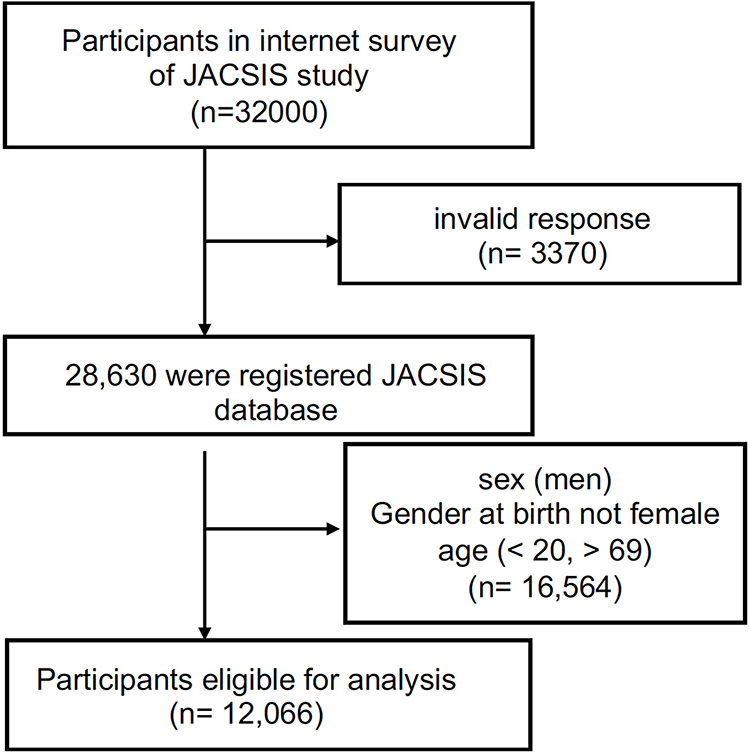 |
Figure 1 Flow chart of this study, from entries into the Japan COVID-19 and Society Internet Survey, the number of individuals targeted for this study is documented alongside excluded participants. |
Study Instruments
In Japan, CCS is recommended every 2 years from ages 20–69. During CCS, abnormalities are identified in the cervical cytology by brushing the external cervical os. CCS with HPV typing is not widely used in Japan; therefore, it was not included in this study.
Outcome Variable
The outcome variables were identified by a specific question regarding whether the participant underwent CCS: “Have you been screened for cervical cancer within the last 2 years?” The participant’s response was considered to be the outcome variable. Responses were selected from seven options: 1–3 corresponded to yes (1, no abnormality; 2, abnormality; 3, no results yet), while 4–7 corresponded to no (4, motivated to undergo screening and unaffected by COVID-19; 5, motivated to undergo screening and affected by COVID-19; 6, not motivated to undergo screening and not affected by COVID-19; and 7, not motivated to undergo screening and affected by COVID-19). Participants who selected options 1 through 3 were categorized into the “undergone CCS” group, while those who selected options 4 through 7 were categorized into the “never had CCS” group.
Statistical Analysis
Chi-squared tests were conducted to obtain the socioeconomic information, health-related statuses, and personal characteristics of the participants, in order to analyze the association between personal characteristics and screening behavior. We used multivariate log-binomial regression models to evaluate inequalities regarding regular CCS checkups. We chose log-binomial regression models, particularly those with cross-sectional data and an outcome percentage >10%.18 These are easier to interpret and correspond well with prevalence terms as measures of association.19 The dependent variables were undergone CCS and never had CCS. Adjusted prevalence ratios (APRs) with 95% confidence intervals (CIs) were calculated. The social background variables were age (20–29, 30–39, 40–49, 50–59, and 60–69 years), marital status (married, single/divorced/widow), employment status (unemployed/student, employed), education level (high school or less, junior college/bachelor’s degree, graduate degree/other), household income (<4 million Yen, 4–8 million Yen, >8 million Yen, no answer/other), smoking status (none, ex-smoker, every day), alcohol consumption (none, ex-drinker, every day), use of preventive care for general checkups and breast cancer within the preceding 2 years, chronic diseases (hypertension, diabetes, asthma, chronic heart disease, stroke, chronic obstructive pulmonary disease, chronic kidney disease, hepatitis, cancer, and depression), self-rated health status (excellent, good, fair, bad, very bad), COVID-19 vaccine doses (unvaccinated, 1–2, ≥3), and fear of COVID-19. We used the 7-item Japanese version of the fear of coronavirus-19 scale (FCV-19S) to assess fear of COVID-19.20,21 Spearman rank correlation coefficients were used to evaluate correlations to avoid multi-collinearity between independent variables. Among the variables suspected of having correlations, we evaluated only one at a time. All statistical tests were two-tailed, and p-values <0.05 were considered statistically significant. All analyses were performed using SAS OnDemand for Academics, a cloud-based software provided by SAS Institute Inc.
Ethical Approval
All the procedures were conducted in accordance with the ethical standards of the 1975 Declaration of Helsinki (revised in 2013). The study protocol was reviewed and approved by the Research Ethics Committee of the Osaka International Cancer Institute (approved on June 19, 2020; approval no. 20,084). Before responding to the online questionnaire, all participants provided informed consent. The Internet Survey Agency adhered to the Act on the Protection of Personal Information in Japan. To encourage participation, credit points were offered to participants, which could be redeemed for internet shopping discounts or as cash.
Results
Patients’ Characteristics
A total of 12,066 participants were included in the study: 5597 (46.4%) had undergone CCS, and 6469 (53.6%) never had CCS, over the preceding 2 years. Table 1 presents the number of participants and weighted distribution of the two groups according to participants’ characteristics. Participants with the following characteristics accounted for the majority of those who never had CCS within two years: 20–29 years old, unemployed/student, unmarried, high school education or lower, and household income <4 million Yen. There were no significant differences in screening coverage according to the smoking status. Table 2 shows the general health characteristics and COVID-19 statuses of the eligible participants. Those who had undergone screening for general checkups and breast cancer were more likely to have undergone CCS as well (78.3%–86.6%). There were no significant differences in the coexistence of chronic diseases or CCS between the FCV-19S items. The CCS coverage was higher among those who had received the COVID-19 vaccine (65.8%) than among those who had never been vaccinated (34.2%).
 |
Table 1 Characteristics of Eligible Women Depend on CCS Status Within the Last Two Years |
 |
Table 2 Characteristics of Eligible Women Depend on CCS Status with Health and COVID-19 Related Status |
Prevalence Ratios of Undergone CCS
Table 3 shows the prevalence of CCS among participants. The unadjusted prevalence ratio (PR) of CCS was determined using a univariate analysis. The PR was 0.70 (95% CI: 0.63–0.79) for participants in their 20s, and 0.78 (95% CI: 0.70–0.87) for those in their 60s, when the responses of those in their 40s were used as the reference age group. The PR for CCS has increased with increasing years of education and annual income. No significant differences were observed in tobacco or alcohol use. For each health-related status, the PR decreased as self-rated health decreased. The PR for CCS was also significantly lower in the group that did not undergo general checkups (PR: 0.36, 95% CI: 0.34–0.38) and breast cancer screening (PR: 0.43, 95% CI: 0.41–0.45).
 |
Table 3 Univariate and Multivariate Analysis Predicting Undergone Cervical Cancer Screening |
After multivariate analysis for social background factors, the adjusted prevalence ratio (APR) was calculated alongside the univariate analysis. Given the suspected correlations with factors such as age, independent variables including education level, FCV-19S, alcohol use, employment status, and breast cancer screening were excluded from the analysis. There was no significant difference in the APR according to COVID-19 history. However, the APR for CCS remained lower in the unvaccinated group than in the vaccinated group in terms of the COVID-19 vaccination history. Participants aged 20–29 years (APR: 0.85, 95% CI: 0.81–0.90), unmarried (APR: 0.80, 95% CI: 0.77–0.84); household income <4 million Yen (APR:0.81–0.90), and did not undergo general health checkups (APR: 0.45, 95% CI: 0.42–0.47) had a significantly lower APR for CCS than the reference in each category.
Discussion
This study aimed to analyze the differences in socioeconomic backgrounds between individuals who had undergone CCS and those who never had during the era of the COVID-19 pandemic. Additionally, this study aimed to explore the relationship between CCS and COVID-19 infection status.
In this study, the younger generation (participants aged 20–29 years) accounted for the majority of those who never had CCS within the two years of the COVID-19 era. In particular, the CCS coverage for persons aged 20–29 years, unmarried persons, and those with annual household incomes <4 million Yen were lower than those of the other groups, indicating the need for immediate attention. In terms of undergoing CCS within the last two years, the CCS coverage in Japan from 2020 to 2022 during the COVID-19 era showed an increasing trend compared to the period before the COVID-19 pandemic. Additionally, while a history of COVID-19 infection or fear of infection did not lead to a reluctance to undergo CCS, individuals who had not received the COVID-19 vaccine were more common among those who had not undergone CCS.
This study examined social practice policies using data obtained after adjusting for various social backgrounds. Previous global studies have reported that low-income individuals often refrain from undergoing gynecological examinations.22,23 This is similar in case of CCS among low-income individuals in Japan. This indicates that students, particularly those in their 20s, and socially vulnerable groups such as unemployed and low-income individuals, should be targeted when promoting CCS. At the moment, the low CCS rate among students has been attributed to excessive self-consciousness surrounding health and a lack of opportunities to visit hospitals.8 The small increase in screening rates that followed the distribution of free coupons in Japan suggests that financial and knowledge-based interventions should be considered as well.24 Non-financial studies are also underway to promote CCS uptake. Okuhara et al showed that a message targeting the fundamental motive of caring for kin was as effective as targeting disease avoidance.25 A review by the US Community Preventive Services Task Force on increasing cancer screening uptake recommends the use of small media such as pamphlets and newsletters, one-on-one education, and call-recall via letters and phone calls.26 Recent surveys on attitudes toward HPV vaccine implementation, particularly in urban areas, have revealed that recommendations from parents and best friends are more effective ways to promote vaccination.27 Therefore, information on cervical cancer, its prevention, and CCS should be actively provided to women aged <40 years.
A systematic review reported that behavioral restrictions implemented during the COVID-19 pandemic have significantly impacted the decline in cancer screening uptake rates.10,13 As physical movement was restricted, the use of online healthcare services and telemedicine replaced hospital visits and, thus, served as infection control measures. The resultant decrease in the cancer screening rate is significant because of the necessity of physical medical examinations. There is a concern that a reduction in the number of cancer screenings may lead to delays in diagnoses, delays in cancer treatments, and increased mortality.28 This study clarified the number of cancer examinations that took place in Japan over 2 years rather than short-term behavioral restrictions. The PR adjusted for social and other background factors showed no overall decline in visitation rates compared to pre-pandemic CCS coverage. This may be attributed to the fact that the behavioral restrictions during the four states of emergency in Japan lasted less than two months, providing an environment for regular check-ups afterward. Additionally, cancer screening is not considered a “nonessential and nonurgent outing” requiring self‐restraint in areas where a state of emergency has been declared.29 Interestingly, PRs for CCS visits tended to be higher among those with histories of COVID-19. It was difficult to conclude from this study whether COVID-19 increased the rate of CCS visits. After adjusting for confounding variables, individuals who were unvaccinated against COVID-19 still showed lower CCS rates compared to that of vaccinated individuals, with an APR of 0.89 (95% CI: 0.84–0.95). These findings may represent individuals with less access to information, suggesting the need to consider information dissemination for a broader audience in the future.
Worldwide, self-administered CCS kits have become popular in the US and Europe.30 These kits allow testing to be performed in the convenience of the user’s home and are expected to reduce CCS times and ensure privacy. However, this method has disadvantages regarding sample collection compared to testing at medical institutions. These include a decrease in testing accuracy owing to improper sample collection, the possibility of requirement of additional testing when abnormalities are detected, time required to receive a diagnosis, and a lack of coverage of the costs of these kits by health insurance services. Japan’s home-based HPV sampling test, a similar kit, currently remains at the clinical research stage.31 Given that this screening method is suited to the lifestyles of women in both psychological and accessibility terms, it is also necessary to develop and promote such approaches in Japan.
The strength of this study is that it used a large dataset to analyze undergoing regular CCS with adjustments for social background. Furthermore, considering the participants’ COVID-19 history and trend analyses in terms of hospital visits during the pandemic helped to identify related issues that must be addressed in Japan, as it has one of the lowest CCS coverages among developed countries—at 42.4% for the target age group, compared to the average of 60.7% among OECD member countries.2,3,32 This study had some limitations. 1) As this was an Internet-based, self-reported, observational cohort study, there were questions asked solely to ensure data reliability by excluding participants with inconsistent or invalid responses. Nevertheless, the possibility of participant bias or incorrect responses cannot be fully ruled out. 2) Although this study considered the impact of the COVID-19 pandemic, future trends in CCS coverage should be assessed after the pandemic has fully ended. 3) This study did not consider differences among different regions of Japan and may not accurately reflect national trends. 4) We investigated the relationship between medical visits for CCS from 2020 to 2022, COVID-related questions, and socio-economic backgrounds. However, as there were no data available prior to 2020, it was not possible to accurately assess the extent of the impact of COVID-19 infection on CCS. Therefore, it is necessary to continue this research, including follow-up investigations. Finally, although we identified low screening rates and a basis for future policies, further analyses are warranted to determine the appropriate approaches in different populations.
Conclusion
Socioeconomic inequalities of the group aged 20–29 years, students/unmarried persons, and those with annual household incomes below 4 million Yen were lower than those of the other groups, contributing significantly to CCS hesitancy and the need for immediate attention. The CCS coverage in Japan during the COVID-19 pandemic year (2020–2022) was not low compared with the pre-pandemic era. We hope that the findings of this study will help identify problems related to CCS and contribute to improving its uptake in Japan.
Abbreviations
COVID-19, coronavirus disease of 2019; CCS, Cervical cancer screening; OECD, Organization for Economic Co-operation and Development; US, United States; HPV, Human Papilloma Virus; JACSIS, Japan COVID-19 and Society Internet Survey; PR, prevalence ratio; APR, adjusted prevalence ratio; CI, confidence interval; FCV-19S, fear of coronavirus-19 scale.
Data Sharing Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
All the procedures were conducted in accordance with the ethical standards of the 1975 Declaration of Helsinki (revised in 2013). The study protocol was reviewed and approved by the Research Ethics Committee of the Osaka International Cancer Institute (approved on June 19, 2020; Approval No. 20084). Before responding to the online questionnaire, all the participants provided informed consent.
Acknowledgments
We thank all the participants for their participation. We appreciate valuable feedback from the JACSIS study group.
Funding
This research was supported by the Japan Society for the Promotion of Science (JSPS) KAKENHI Grants (grant numbers18H03062 and 23EA1001) and Local Development Secretariat, Cabinet Office, Government of Japan FY2023 Digital Rural City National Concept Grant Digital Implementation type 3.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Pimple SA, Mishra GA. Global strategies for cervical cancer prevention and screening. Minerva Ginecol. 2019;71(4):313–320. doi:10.23736/S0026-4784.19.04397-1
2. Aoki ES, Yin R, Li K, et al. National screening programs for cervical cancer in Asian countries. J Gynecol Oncol. 2020;31(3):e55. doi:10.3802/jgo.2020.31.e55
3. OECE Stat Web Browser. Organization for Economic Co-operation and Development, Health care utilisation; 2021. Available from: https://stats.oecd.org/Index.aspx?QueryId=30159.
4. Simms KT, Hanley SJB, Smith MA, et al. Impact of HPV vaccine hesitancy on cervical cancer in Japan: a modelling study. Lancet Public Health. 2020;5(4):e223–e234. doi:10.1016/S2468-2667(20)30010-4
5. Kaneko M, Matsushima M. Current trends in Japanese health care: establishing a system for board-certificated GPs. Br J Gen Pract. 2017;67(654):29. doi:10.3399/bjgp17X688669
6. Cui Z, Kawasaki H, Tsunematsu M, et al. Factors Affecting the Cervical Cancer Screening Behaviors of Japanese Women in Their 20s and 30s Using a Health Belief Model: a Cross-Sectional Study. Curr Oncol. 2022;29(9):6287–6302. doi:10.3390/curroncol29090494
7. Okui T. An analysis of health inequalities depending on educational level using nationally representative survey data in Japan, 2019. BMC Public Health. 2021;21(1):2242. doi:10.1186/s12889-021-12368-2
8. Kaneko N. Factors associated with cervical cancer screening among young unmarried Japanese women: results from an internet-based survey. BMC Womens Health. 2018;18(1):132. doi:10.1186/s12905-018-0623-z
9. Cabinet Office Japan. Response to COVID-19; 2022. Available from: https://www8.cao.go.jp/shougai/whitepaper/r03hakusho/zenbun/h2_01_02.html.
10. Edward Winstead. For Cancer Screening, COVID-19 Pandemic Creates Obstacles, Opportunities; 2021. Available from: https://www.cancer.gov/news-events/cancer-currents-blog/2021/cancer-screening-decreases-coronavirus-pandemic.
11. Toyoda Y, Katanoda K, Ishii K, et al. Negative impact of the COVID-19 state of emergency on breast cancer screening participation in Japan. Breast Cancer. 2021;28(6):1340–1345. doi:10.1007/s12282-021-01272-7
12. Ministry of Health, Labour and Welfare of Japan. Response to COVID 19 (Novel Coronavirus) after the classification change; 2022. Available from: https://www.mhlw.go.jp/stf/covid-19/kenkou-iryousoudan_00006.html.
13. Mayo M, Potugari B, Bzeih R, et al. Cancer Screening During the COVID-19 Pandemic: a Systematic Review and Meta-analysis. Mayo Clin Proc Innov Qual Outcomes. 2021;5(6):1109–1117. doi:10.1016/j.mayocpiqo.2021.10.003
14. Sasidharanpillai S, Ravishankar N. The Short-Term Impact Of COVID-19 Pandemic on Cervical Cancer Screening: a Systematic Review and Meta-Analysis. Asian Pac J Cancer Prev. 2022;23(5):1497–1504. doi:10.31557/APJCP.2022.23.5.1497
15. Obikane E, Nishi D, Ozaki A, et al. Association between Poverty and Refraining from Seeking Medical Care during the COVID-19 Pandemic in Japan: a Prospective Cohort Study. Int J Environ Res Public Health. 2023;20(3):2682. doi:10.3390/ijerph20032682
16. Gotanda H, Miyawaki A, Tabuchi T, et al. Association Between Trust in Government and Practice of Preventive Measures During the COVID-19 Pandemic in Japan. J Gen Intern Med. 2021;36(11):3471–3477. doi:10.1007/s11606-021-06959-3
17. Koga T, Okubo R, Chen C, et al. Associations of parent-child exercise with family relations and parental mental health during the COVID-19 pandemic. J Affect Disord. 2023;324:551–558. doi:10.1016/j.jad.2023.01.001
18. Richardson DB, Kinlaw AC, MacLehose RF, et al. Standardized binomial models for risk or prevalence ratios and differences. Int J Epidemiol. 2015;44(5):1660–1672. doi:10.1093/ije/dyv137
19. Tamhane AR, Westfall AO, Burkholder GA, et al. Prevalence odds ratio versus prevalence ratio: choice comes with consequences. Stat Med. 2016;35(30):5730–5735. doi:10.1002/sim.7059
20. Ahorsu DK, Lin CY, Imani V, et al. The Fear of COVID-19 Scale: development and Initial Validation. Int J Ment Health Addict. 2022;20(3):1537–1545. doi:10.1007/s11469-020-00270-8
21. Wakashima K, Asai K, Kobayashi D, et al. The Japanese version of the Fear of COVID-19 scale: reliability, validity, and relation to coping behavior. PLoS One. 2020;15(11):e0241958. doi:10.1371/journal.pone.0241958
22. Jolidon V, De Prez V, Willems B, et al. Never and under cervical cancer screening in Switzerland and Belgium: trends and inequalities. BMC Public Health. 2020;20(1):1517. doi:10.1186/s12889-020-09619-z
23. Abdel-Rahman O. Patterns and Trends of Cancer Screening in Canada: results From a Contemporary National Survey. J Natl Compr Canc Netw. 2021;19(1):68–76. doi:10.6004/jnccn.2020.7613
24. Ueda Y, Sobue T, Morimoto A, et al. Evaluation of a free-coupon program for cervical cancer screening among the young: a nationally funded program conducted by a local government in Japan. J Epidemiol. 2015;25(1):50–56. doi:10.2188/jea.JE20140080
25. Okuhara T, Okada H, Goto E, et al. Encouragement of cervical cancer screening via an evolutionary theoretical approach: a randomized controlled study in Japan. Prev Med Rep. 2022;27:101818. doi:10.1016/j.pmedr.2022.101818
26. Des Marais AC, Brewer NT, Knight S, et al. Patient perspectives on cervical cancer screening interventions among underscreened women. PLoS One. 2022;17(12):e0277791. doi:10.1371/journal.pone.0277791
27. Yagi A, Ueda Y, Tomine Y, et al. The ‘best friend effect’: a promising tool to encourage HPV vaccination in Japan. Int J Clin Oncol. 2022;27(11):1750–1757. doi:10.1007/s10147-022-02240-7
28. Mayo M, Potugari B, Bzeih R, et al. Cancer Screening During the COVID-19 Pandemic: a Systematic Review and Meta-analysis. Mayo Clin Proc Innov Qual Outcomes. 2021;5(6):1109–1117.
29. Ministry of Health, Labour and Welfare of Japan. The response in cancer screening in light of the declaration of a state of Emergency for COVID-19; 2021. Available from: https://www.mhlw.go.jp/content/000777298.pdf.
30. Serrano B, Ibáñez R, Robles C, et al. Worldwide use of HPV self-sampling for cervical cancer screening. Prev Med. 2022;154:106900. doi:10.1016/j.ypmed.2021.106900
31. Nishimura Y, Matsuura M, Terada N, et al. Mailing human papillomavirus self-sampling kits to women under-screened for cervical cancer improved detection in cervical cancer screening in a general population study in Japan. BMC Public Health. 2023;23(1):473. doi:10.1186/s12889-023-15402-7
32. Kakubari R, Egawa-Takata T, Ueda Y, et al. A survey of 20-year-old Japanese women: how is their intention to undergo cervical cancer screening associated with childhood HPV vaccination status? Hum Vaccin Immunother. 2021;17(2):434–442. doi:10.1080/21645515.2020.1788326
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.