")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 15
Association Between Overweight/Obesity and ART Drug Regimen Among Adult HIV Patients in Gamo Zone Public Health Facilities Southern Ethiopia
Authors Belete NK, Assefa DT , Gadore TF, Teshale MY , Tariku EZ
Received 15 March 2023
Accepted for publication 9 June 2023
Published 15 June 2023 Volume 2023:15 Pages 349—360
DOI https://doi.org/10.2147/HIV.S412586
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Nigus Kabtu Belete, Darik Temesgen Assefa, Tesfaye Feleke Gadore, Manaye Yihune Teshale, Eshetu Zerihun Tariku
School of Public Health, College of Medicine and Health Science, Arba Minch University, Arba Minch, Ethiopia
Correspondence: Nigus Kabtu Belete, Tel +251914552360, Email [email protected]
Introduction: Overweight/obesity is an emerging public health problem in low income countries. Currently sub-Saharan African countries are facing a double burden of malnutrition. Evidence has shown that overweight/obesity is becoming a problem for people living with HIV. But little is known in our setting. Thus, this study is designed to assess the association between overweight/obesity and ART drug regimen among adult HIV patients in Gamo zone public health facilities southern Ethiopia.
Objective: To assess the association between overweight/obesity and ART drug regimen among adult HIV patients in Gamo zone public health facilities southern Ethiopia.
Methods: Institution-based cross-sectional study was conducted from April 10 to May 10, 2022, among systematically selected adult HIV patients. The data were collected by using a structured interviewer-administered questionnaire, patient record review, and physical measurements. Multivariate logistic regression model was used to assess the association between dependent and independent variables. A p-value < 0.05 with its 95% CI was considered as a statistically significant and interpreted accordingly.
Results: The magnitude of overweight/obesity were 13.5% (95% CI:(10.4– 17.2)). Being male (2.484(1.308, 4.716)), duration on ART (took for ≥ 5 years) ((2.249(1.218, 4.152)), and ART drug regime (3.789(1.965, 7.304)) were significantly associated with overweight/obesity.
Conclusion: Overweight/obesity is significantly associated to ART drug regimen type among adult HIV patients. Furthermore, sex and duration on ART drug were found significantly associated with overweight/obesity of adult HIV patients.
Keywords: obesity, overweight, HIV, anti-retroviral therapy, drug, Gamo zone, Ethiopia
Introduction
Human immunodeficiency virus (HIV) infection is most of the time related to weight loss or underweight.1,2 However, now a days weight gain has been attributed to the increasing availability of highly active anti-retroviral therapy (ART). Overweight and obesity has been reported to be a common problem among HIV patients in Africa.3
The shift of HIV/AIDS clinical feature or the weight gain among PLWH may be associated to side effect of all ART drugs,4 while for others, it was considered to be an immunological response or a reaction of an increased CD4 cell count. Because of the reports of associations between CD4 cell increase and weight gain,5 for instance Protease inhibitors (PI), have been associated with weight gain, mainly with fat mass, condition like buffalo syndrome and increased central body fat distribution similar to metabolic syndrome, with no change in lean body mass.6
Obesity is becoming a problem for HIV-infected people in developed countries due to progressive economic development which leads to nutrition transition and several people are adopting a modern lifestyle, less physical activity, and consuming high-density food.7 Weight gain among ART patients is common and considered as a side effect of regimens, while for others, it was considered to be an immunological response.5
The first-line ART regimen is the best for viral suppression and immune recovery and can reduce the occurrence of opportunistic infection (OI). According to Ethiopia Federal Ministry of Health (FMoH) ART drug administration guideline the preferred first-line regimen for adults and adolescents is TDF+3TC+DTG or TDF+3TC+EFV as a once-daily dose.8
Still now, there is no cure for HIV/AIDS. After the initiation of ART, AIDS patients’ care and treatments have significantly improved. The drug can reduce morbidity and mortality, prevent from the occurrence of opportunistic infection, improves restoration of immunity, and prolonging of life; turning AIDS into a chronic disease.9
Among the United States of America HIV patients who were on ART, 22% were affected with overweight and 5% were affected with obesity.10 Sub Saharan African (SSA) is a state of malnutrition and characterized by a double burden of malnutrition with a high prevalence of undernutrition and increasing obesity along with diet-related non-communicable diseases. Studies from low income countries show a higher proportion of overweight and obesity among PLHIV (22.1%)11 and ART experienced PLWH (34–35%)5,12 compared to undernutrition (10.0–26.3%).11
Demographic Health Survey study of 32 SSA countries stated that the pooled prevalence of overweight was 15.9%, with the least value in Madagascar 5.6% and the highest in Swaziland 27.7%, likewise, the prevalence of obesity was also lower in Madagascar 1.1% and higher in Swaziland 23.0%.3 In our country Ethiopia, the pooled prevalence of overweight/obesity was found to be 3.58%.13
Overweight and obesity are risk factors for diabetes, hypertension, cardiovascular disease, and cancer in the general population that increasingly affect HIV-infected people.14 Moreover, obesity seems to have a detrimental effect on immune recovery after ART initiation.15 Among non-obese individuals during the initiating of ART, around 18.3% were developing obesity within an average of 2 years of ART initiation. The greatest risk factor for developing such a condition was having an Integrase Strand Transfer Inhibitor (INSTI) as the most-used ART core drug class.16
Now a days in developing countries overweight/obesity is getting more concern. As a result the emergence of obesity/overweight among HIV/AIDS patients in many developing countries is also an emerging public health problem. Overweight and obesity and its associated health problems among ART patients become the unfinished public health challenge.9
The aim of this study was, therefore, to assess the association between overweight/obesity and ART drug regimen among adult HIV patients in Gamo zone public health facilities.
Methods and Materials
Study Design, Area and Period
Institution based cross-sectional study design was employed in public health facilities of Gamo zones, which is one of the 15 zonal administrations of south nation nationality and people region. It has a total area of 7, 581, 4 square kilometers. This consists of 15 Woredas and one city administration. The administrative center of the Gamo zone is Arba Minch town. Arba Minch is located about 454km south of Addis Ababa, and 275km far from Hawassa. Gamo zone has six public hospitals and 57 Health centers. Out of those 11 health facilities are providing ART service (three hospital and eight health centers). The total population of the zone is around 2,019,687 and from this there are around 3339 adult ART patients under follow-up (Gamo zone health administration report). The data was collected from April 10 to May 10, 2022.
Populations
Source Population
All adult HIV patients in public health facilities of Gamo zones, southern Ethiopia.
Study Population
All adult patients on HIV who had regular follow up in the health facilities and visit the health facilities during the data collection period.
Eligibility Criteria
Inclusion Criteria
Adult patients with HIV who had regular follow-up and have taken ART medication for at least one month were included in the study.
Exclusion Criteria
Pregnant and lactating women (six month of postpartum) were excluded since our anthropometric measurement is BMI and it is not applicable for those population groups. And incomplete medical records which miss more than 20% of the independent variables.
Sample Size Determination and Sampling Techniques
Sample Size Determination
Sample size was determined by using a single population proportion with 95% level of confidence and 5% margin of error.
Where; n0 = Minimum sample size
Z =1.96, Normal deviant at the portion of 95% confidence interval two-tailed test
P = proportion of outcome variable.
d = margin of error acceptable is taken as 4%= 0.04
Magnitude of Obesity/Overweight and Its Associated Factors Among HIV/AIDS Patients on Antiretroviral Therapy in Jimma Zone Hospitals, South West Ethiopia was 21%.17
Finally, by adding 10% none response rate the total sample size was 438.
Sampling Techniques
Gamo zone has eleven health facilities which are providing ART service. All health facilities were included in the study because currently all health facilities are using appointment spacing model to which clients can return to the health facility after six months that can reduce patient flow and difficult to get optimal study population in one month study period.
The total sample size was proportionally allocated to the selected health facilities. The last one month registration was used to see patient flow and to predict the source population. Finally, a systematic random sampling technique was used to select the study participants. Per each health facility, three Ks was calculated by dividing the number of the population (N) by their respective number of the sample (n) based on a one-month report.
Data Collection Instruments and Procedures
Data were collected by healthcare providers who are working in ART clinic. Structured interviewer-administered questionnaire; patient record review and anthropometric measurement were used. The questionnaire has four parts: socio-demographic and economic factors, clinical characteristics, anthropometric measurements, behavioral related characteristics’ and data related to dietary factors. The data was collected by using kobo collect (smartphone for data collection) through face-to-face interviews. Check list was developed to assess clinical related factors from patient records.
Physical activity level was assessed by using Global Physical Activity Questionnaire Analysis Guide. Physical activity (or inactivity) was described to estimate a population’s mean or median physical activity using continuous indicators by metabolic equivalent (MET) minutes per week or time spent in physical activity. It was measured by WHO recommendations on physical activity for health. Throughout a week, including activity for work, during transport and leisure time, adults should do at least 150 minutes of moderate-intensity physical activity or 75 minutes of vigorous-intensity physical activity or an equivalent combination of moderate- and vigorous-intensity physical activity achieving at least 600 MET-minutes.18
The household food insecurity status of participants was assessed by using Household Food Insecurity Access Scale (HFIAS), the tool developed by Food and Nutrition Technical Assistance (FANTA) project and adapted to individual level. Each question is within a recall period of 30 days. The respondents were first asked an occurrence question that is, whether the condition in the question happened at all in the past 4 weeks (yes/no). If the respondent answer was “yes” to an occurrence question, a frequency-of-occurrence was asked to determine whether the condition happened rarely (once or twice), sometimes (3–10 times), or often (more than 10 times).19,20
Dietary Diversity Score (DDS) was determined by asking the respondents to list all the food items consumed in the previous 24 hours preceding the assessment date, starting with the first food consumed the previous morning. If a mixed dish was eaten, participants were asked about all the ingredients of the dish. Once the recall was finished, participant was probed for food groups to ask for food that was not mentioned. The reported food items were categorized into fourteen food groups: starchy staples, dark green leafy vegetables, white tubers and roots, vitamin A-rich fruits and vegetables, other fruits and vegetables, organ meat, meat and fish, flesh meats, fishes, eggs, legumes, nuts and seeds, milk and milk product and oils and fats. The DDS was calculated as the sum of the food groups consumed over 24 hours.21
Cigarette smoking, khat chewing, and alcohol consumption were assessed using a structured questionnaire adapted from a STEPS survey on non-communicable diseases risk factors in Ethiopia and WHO STEP wise approach to chronic disease risk factor surveillance.22
Anthropometric Measurements
Height and weight were measured according to the WHO steps procedure. A stadiometer (Seca Germany) was used to measure the height of the study participants to the nearest 0.1 cm with the subjects positioned at the Frankfurt Plane and the four points (heel, calf, buttocks, and shoulder) touching the vertical stand of the stadiometer and their shoes taken off. Before starting the measurement, the stadiometer was checked using calibration rods. It was measured three times and the average was taken.
An electric-powered digital scale (Seca Germany) was used to measure the weight to the nearest 0.1 kg with the subjects wearing light clothes and without shoes. Before starting the measurements, the tools were calibrated. A stone of weight 15 kg was used to check the validity of the scale every morning. The weight was measured three times and the average was taken. The coefficient of variation within data collectors was calculated at the time of training and it was below 3%. BMI was calculated as the ratio of weight in kilograms (kg) to the square of height in meters (m2).
Data Quality Assurance
Before data collection, the questionnaire was first prepared in English and translated to the local language, and then translated back to English to ensure its consistency. Five percent of questionnaire was pretested at sawula general hospital. The data collectors and supervisors (three health officers) took two days of training about the objective, procedure, tool, and ethics of the study. During the data collection period, the Principal investigator and supervisor made ongoing supervision and reviewed all the completed questionnaires to ensure completeness and consistency of the information collected. After data collection, all the questionnaires were revised, cleaned, and checked its completeness.
Data Processing and Analysis
Data were recorded in the mobile KOBO tool box application and exported to the SPSS version 25 software package for further management and analysis. DDS was calculated based on the number of food groups consumed by an individual over the past 24 hours.21 Using HFIAS, food security was categorized into two categories.23
A frequency table was used to describe the socio demographic, clinical and behavioral variables of the study. The magnitude of overweight/obesity with a 95% CI was estimated. Model fitness was checked by using the Hosmer-Lemeshow goodness-of-fit test and the model was fitted well. Bivariate analysis was executed for each variable and those variables with a p value of <0.25 were entered into multivariate binary logistic regression to identify factors associated with magnitude of overweight/obesity. An OR with a 95% CI was computed, and variables having a p value of <0.05 in the multivariate logistic regression were considered as statistically independent factors for overweight/obesity.
Ethical Consideration
All methods and procedures in this study were carried out by the Declaration of Helsinki and ethical clearance was obtained from the Arba Minch University, College of Medicine and Health Sciences, Institutional Ethical Review board (ref.no IRB/1229/2022). Informed written consent was obtained from each study participant. The name or any other identifying information was not recorded on the questionnaire. All information taken from the participants was kept strictly confidential and in a safe place. The information retrieved was used only for the study purpose.
Result
Socio Demographic and Economic Characteristics of Adult HIV Patients
A total of 415 adults who are on ART were included, making a response rate of 94.7%. Majority of the 214 (51.6%) study participants were males and 218 (52.5%) of the participants were in the age range of 30–44 years. High proportion of the study participants, 288 (69.4%), were from urban residence and higher of the study participants, 294 (70.8%), were employed. Regarding marital status 235 (56.6%) of the study participants were married. Also, 251 (60.5%) of the study participants had no formal education. Most of (253, 61%) the study participants had average monthly income of more than 200 Ethiopian birr (see Table 1).
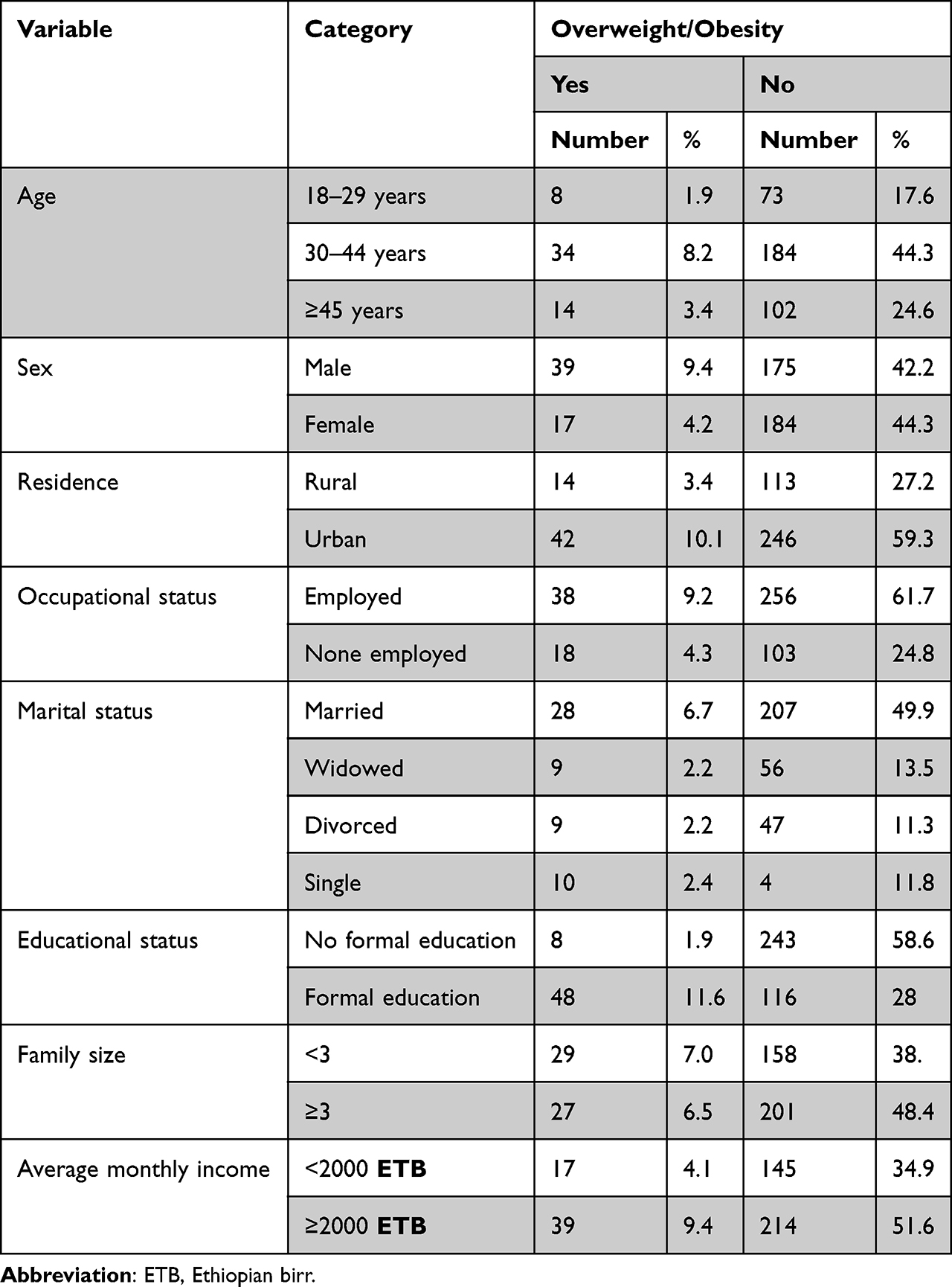 |
Table 1 Socio Demographic and Economic Characteristics of Adult HIV Patients in Gamo Zone Public Health Facilities, Southern Ethiopia 2022 |
Clinical Characteristics of Adult HIV Patients
Regarding duration on ART, 259 (62.4%) were taking ART medication for less than five years. Most of (329, 79.3%) the study participants were stage one WHO clinical staging, 318 (76.6%) had CD4 of more than 50 cell/mm3 and 175 (43.1%) of them had a viral load of less than 50 copies/mm3. Out of the total study participants, 275 (66.3%) had no history of OI in the last six months. Higher proportion of the study participants (339, 81.7%) were taking 1J ART drug regimen and 299 (72.0%) had good drug adherence. Majority, 324 (78.3%), of the study participants took IPT and 316 (76.1%) of them took CPT. Regarding other comorbidity, majority (377, 90.8%) had no other comorbid disease (see Table 2).
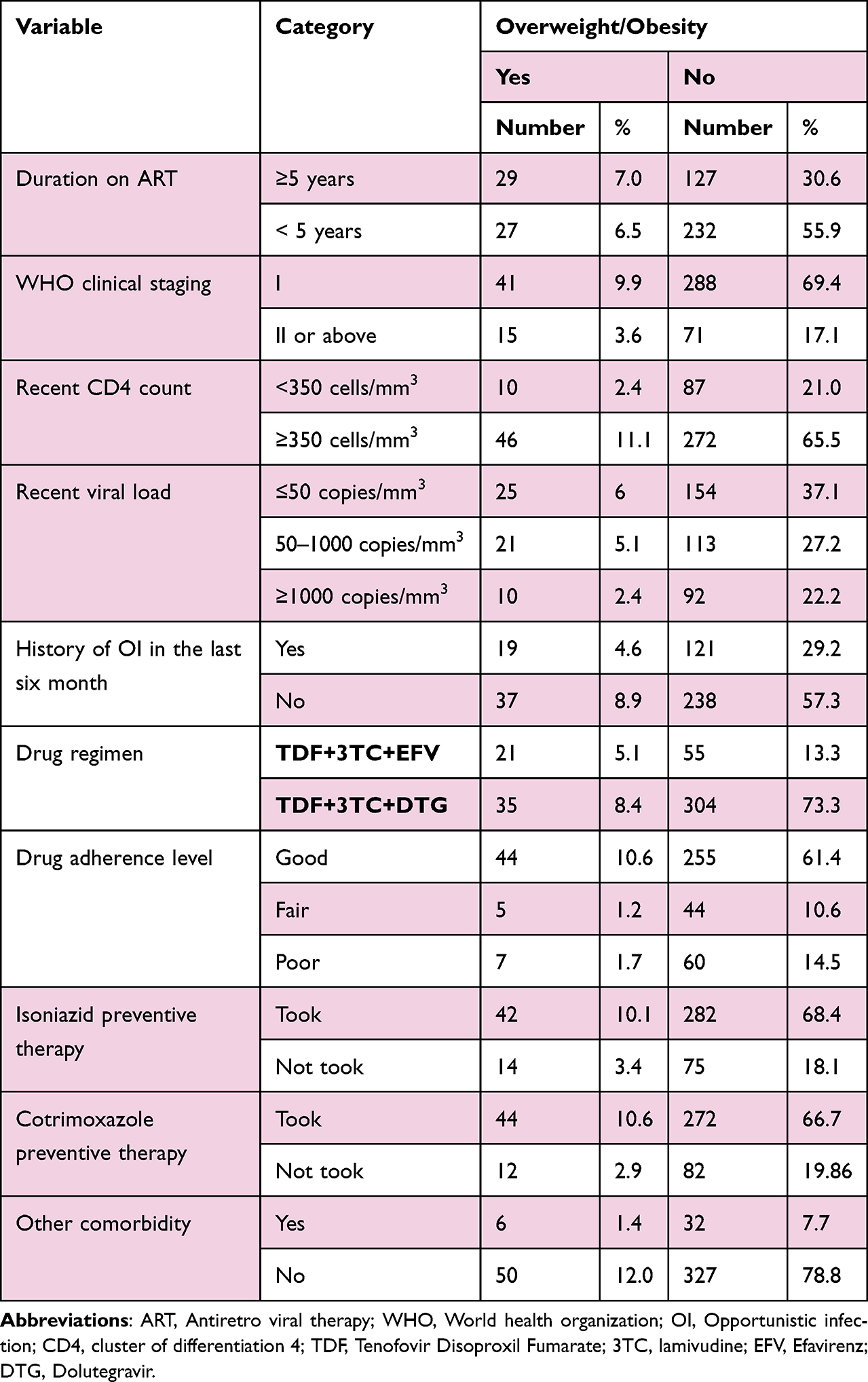 |
Table 2 Clinical Characteristics of Adult HIV Patients in Gamo Zone Public Health Facilities, Southern Ethiopia 2022 |
Behavioral Factors of Adult on ART
Regarding the behavioral characteristics of the participants, only 55 (13.3%) were alcohol drinkers, whereas 24 (5.8%) and 44 (10.6%) were smokers and khat chewers, respectively. Regarding physical activity level, only 88 (21.2%) of the study participants were achieving WHO recommendations on physical activity for health (See Table 3).
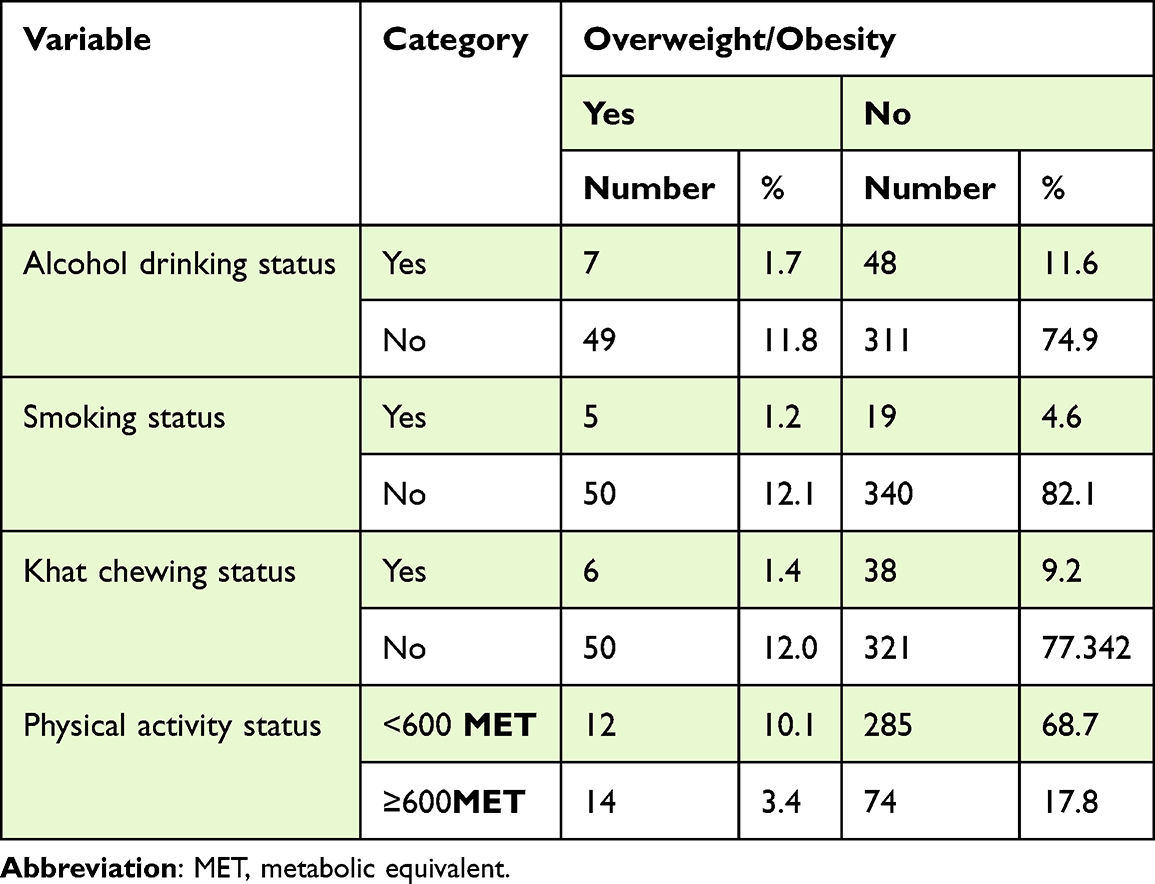 |
Table 3 Behavioral Characteristics of Adult HIV Patients in Gamo Zone Public Health Facilities, Southern Ethiopia 2022 |
Dietary Factors of Adult HIV Patients
This study showed that 273 (65.8%) of adult ART patients were food insecure and 283 (68.2%) of the study participants consumed more than five food group within 24 hours (see Table 4).
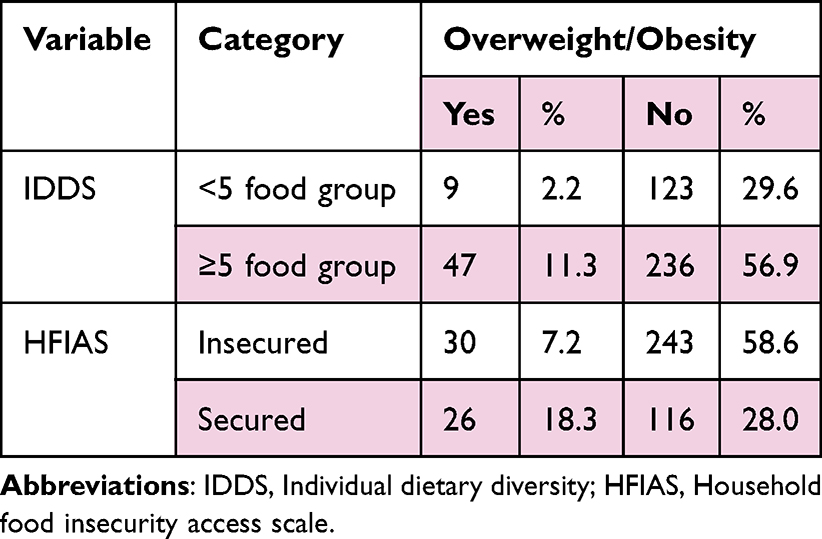 |
Table 4 Dietary Factors of Adult HIV Patients in Gamo Zone Public Health Facilities, Southern Ethiopia 2022 |
Magnitude of Overweight/Obesity and Abdominal Obesity Among Adult HIV Patients
Among 415 adult HIV patients, 56 (13.5%), 95% CI:(10.4–17.2)) were overweight/obese (BMI ≥25kg/m2). Regarding abdominal obesity, 135 (32.5%) of the study participants had abdominal obesity (see Figures 1 and 2).
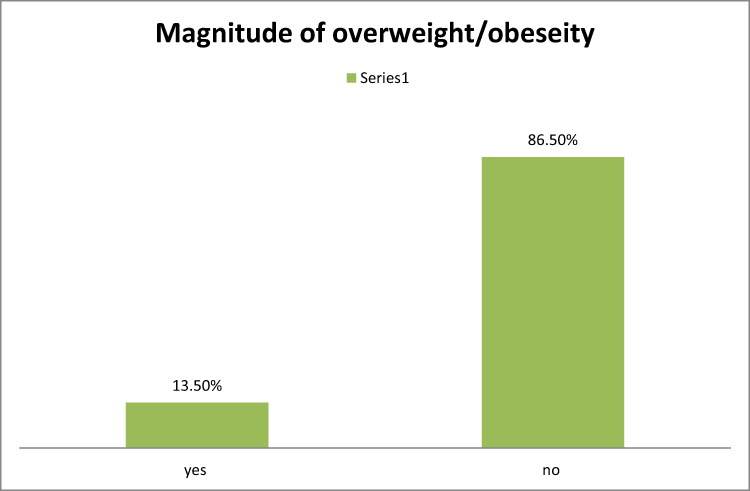 |
Figure 1 Magnitude of overweight/obesity among adult HIV patients in Gamo zone public health facilities Southern Ethiopia 2022. |

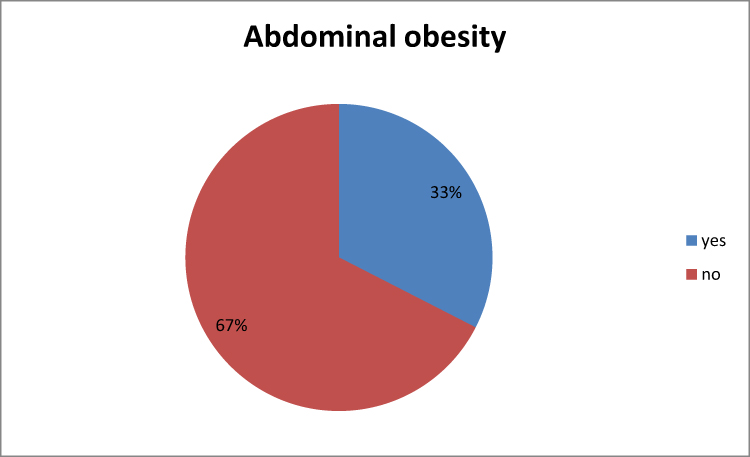 |
Figure 2 Proportion of abdominal obesity among adult HIV patients in Gamo zone public health facilities, Southern Ethiopia 2022. |


Factors Associated with Overweight/Obesity of Adult HIV Patients
In this study sex, duration on ART, WHO clinical stage, current CD4 count, drug adherence, history of OI in the last six months, ART drug regimen, abdominal obesity and alcohol drinking status were candidate variables for multivariate logistic regression. In multivariate logistic regression sex, duration on ART, and ART drug regimen were significantly associated with overweight/obesity of adult HIV patients.
The odds of overweight/obesity were two times higher among males as compared to females (2.484(1.308, 4.716)). Similarly, the odds of overweight/obesity were two times higher among adults who took ART drug for more than five years as compared to those who took for less than five years (2.249(1.218,4.152)). The odds of overweight/obesity were nearly four times higher among those who took 1F (TDF+3TC+EFV) ART drug regime as compared to those who took 1J (TDF+3TC+DTG) (3.789(1.965, 7.304)) (See Table 5).
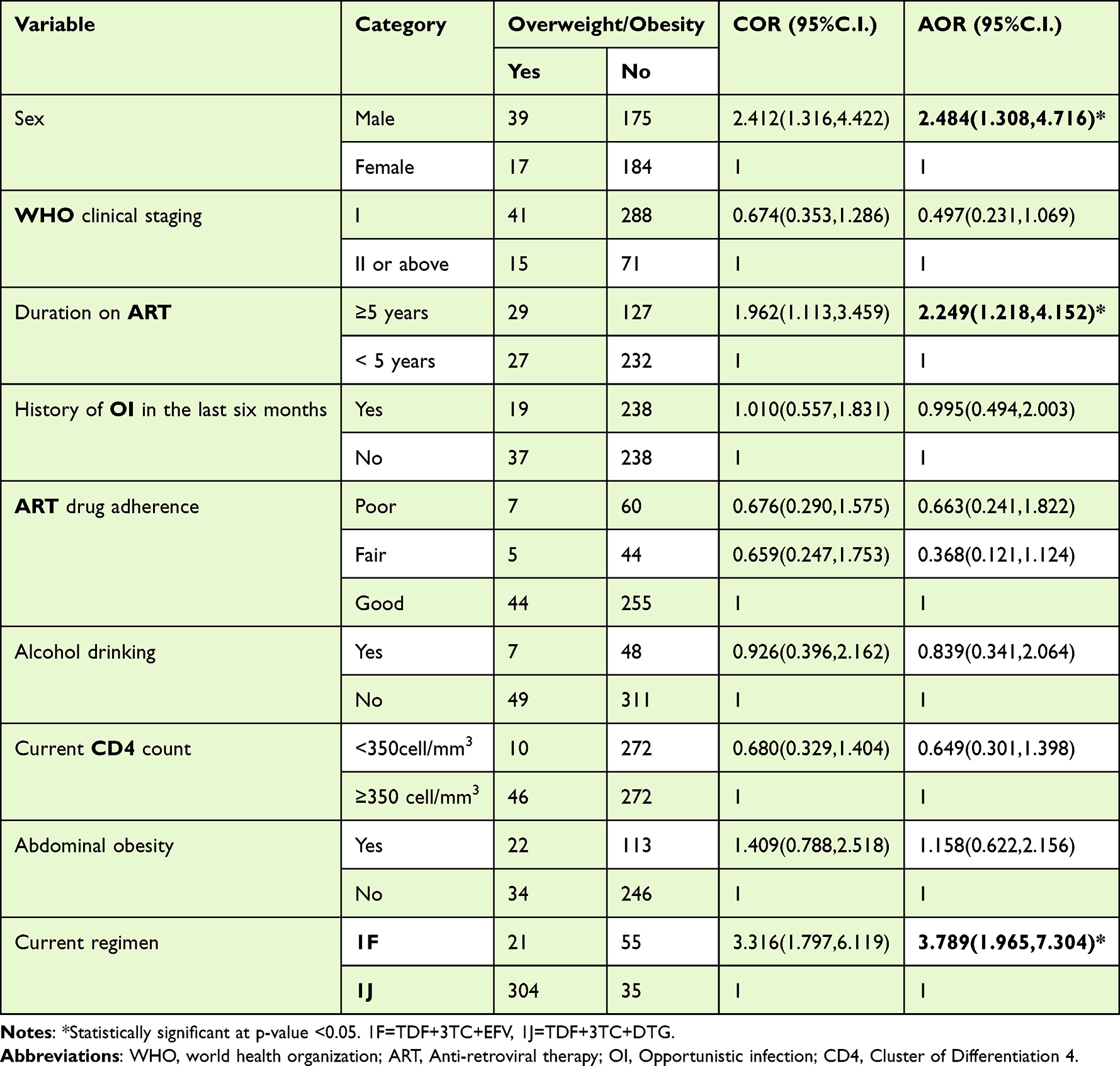 |
Table 5 Factors Associated with Overweight/Obese of Adult HIV Patients in Gamo Zone Public Health Facilities, Southern Ethiopia 2022 |
Discussion
The overall prevalence of overweight/obesity among the study participants in this study was found to be 13.5%. The magnitude in this study is lower than the cohort study done in USA and Canada that showed nearly 30% of HIV patients had developed overweight/obesity during the follow up period.24 This might be owing to HIV treatment complications and drug side effects in ART patients. Furthermore, it might be explained by the difference in the sample size and socio-demographic and economic variables. The magnitude of overweight/obesity in this study is also lower than study in Nepal (46.4%). The possible explanation for the difference might be difference in BMI cut off point. In which the previous study categorized nutritional status as underweight (BMI < 18.5 kg/m2), normal (BMI 18.5–22.9 kg/m2), overweight (BMI 23.0–27.4 kg/m2) and obese (BMI ≥ 27.5 kg/m2).1 In addition, difference in the socio-demographic and healthcare service might be responsible for the variation in magnitude. The overall magnitude of overweight/obesity in this study is also lower than that of previous study conducted in South Africa 39%,25 and Gahanna 28.3%.26 The possible explanation for this higher discrepancy might be due to socio-economic status, healthcare delivery system and socio-cultural variations. In this study around 65.5% of the study participants had household food insecurity that could expose them to undernutrition rather than overweight /obesity.
The magnitude in this study is also lower compared to the study done in Addis Ababa (22.1%).3 The existence of different socio-economic status of population and difference in the year of study could be the reason for the discrepancy. Another possible explanation for this discrepancy might be difference in sample size that may add or reduce the target population. The magnitude in this study is lower than the study from Jima (21%).17 It may be due to difference in sample size and study setting. Since this study was conducted and included all health facilities (hospitals and health centers), but the study from Jima zone was conducted only at hospital level on 252 participants.
On the other hand the magnitude of overweight/obese is more close to the study done in Bench Shako zone 9.6%.27 The potential explanation for this finding may be similarity in the health care service, socio demographic and economic status of both Bench Shako zone and Gamo zone populations.
Finding of this study showed that the odd of overweight/obese among adult on ART were four (3.789 (1.965, 7.304)) times more common in those who took (TDF+3TC+EFV) ART drug as compared to those who took (TDF+3TC+DTG) ART drug. Similar results had been reported in a study conducted in Addis Ababa, which showed that AZT+3TC+EFV based medication was significantly associated to overweight/obesity.28 On the contrary, this finding is not supported by comparative clinical trial studies, which revealed that participants taking INSTIs experienced the most weight gain than NNRTI and protease inhibitor (PI).29 Similarly, this finding is also not in line with another follow up study which stated that Dolutegravir is associated with more weight gain than Efavirenz.30 The possible explanation for the difference may be due to difference in body composition of white and black populations. And there is quite a difference in feeding style of American and Ethiopian peoples. This study finding showed that nearly 68% of the population had consumed less than five food group per day. This is the common problem for all developing and low income countries. This may be the possible explanation for the variation in the result.
In addition to this finding of current study also stated that being male had two times (2.484 (1.308, 4.716) more likely to be overweight/obesity as compared to females. This finding is supported by the study done in Addis Ababa on the magnitude of central obesity and associated factors among adult patients on ART in armed force comprehensive and specialized hospital showed that being male was identified as a risk factor to develop obesity.28 However, it is not supported by the cohort study done in USA and Canada that stated that women with HIV experience a significantly greater increase in BMI following ART initiation than men.24 The possible explanation for the discrepancy might be difference of the population, socio economic status and ART drug type. Similarly, this finding is also not in line with other studies done so far in Zimbabwe, Botswana, Uganda and Jima17,25,31,32 which showed that females were more likely to be overweigh/obesity as compared to male. This could be in the fact that in this study most of the population were from urban residence and employed. This made them have more sedentary life and more than two thirds of the participant had physical activity <600MET that exposes them to overweight/obesity.
This study also demonstrated that taking ART drugs for five or more years increases the risk of overweight/obesity by two (2.249(1.218, 4.152)). This result is in line with the study from Botswana and Uganda. This might be due to the fact that some ART drug like INSTI as the most-used ART core drug class has greatest risk factor for developing such a condition.30
Conclusion
In this study, overweight/obesity is significantly and independently associated to ART drug regimen type among adult HIV patients. Furthermore, being male and taking ART medication for more than five years were found significantly associated with overweight/obesity of adult HIV patients. In addition, the magnitude of overweight/obesity in this study was low among adult HIV patients as compared to other previous studies.
Abbreviations
AIDS, Acquired Immune Deficiency Syndrome; ART, Anti-Retroviral Therapy; ARV, Anti-Retro Viral; AZT, Zidovudine; BMI, Body Mass Index; CD4, Cluster of Differentiation 4; CPT, Cotrimoxazole Preventive Therapy; DDS, Dietary Diversity Score; DTG Dolutegravir; EFV Efavirenz; ETB, Ethiopian Birr; FANTA Food and Nutrition Technical Assistance; FAO, Food and Agricultural Organization; HFIAS, Household Food Insecurity Access Scale; HIV, Human Immune Viruses; IPT, Isoniazid Preventive Therapy; MET, Metabolic Equivalent; OI, Opportunistic Infection; PLHIV, People Living with Human Immune Viruses; SSA, Sub-Sahara Africa; TDF, Tenofovir; TB, Tuberculosis; UNAIDS, United Nation Program on Acquired Immune deficiency syndromes.
Data Sharing Statement
The datasets generated and/or analyzed during this study are not publicly available due to participant anonymity, but they are available from the corresponding author upon reasonable request.
Acknowledgments
First, we would like to thank Arba Minch University, College of Medicine and Health Sciences, School of Public Health, for giving me a chance to conduct this thesis work. Second, we would like to thank zone public health facilities for their collaboration by giving permission and required data. Third, we would like to thank all data collectors and supervisors. Finally, we would like to give my deepest appreciation to all study participants for their willingness and give the required data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Khatri S, Amatya A, Shrestha B. Nutritional status and the associated factors among people living with HIV: an evidence from cross-sectional survey in hospital based antiretroviral therapy site in Kathmandu, Nepal. BMC Nutr. 2020;6;1–13.
2. Odwee A, Acup CA, Kyamanywa P, et al. Malnutrition amongst HIV adult patients in selected hospitals of Bushenyi district in southwestern Uganda. African Health Sci. 2020;20(1):122–131. doi:10.4314/ahs.v20i1.17
3. Takarinda KC, Mutasa-apollo T, Madzima B, et al. Malnutrition status and associated factors among HIV-positive patients enrolled in ART clinics in Zimbabwe. BMC Nutr. 2017;3:1–11.
4. Taramasso L, Ricci E, Menzaghi B, et al. Weight gain: a possible side effect of all antiretrovirals. Open Forum Infect Dis. 2017;4(4):1–3. doi:10.1093/ofid/ofx239
5. Guehi C, Badjé A, Gabillard D, et al. High prevalence of being Overweight and Obese HIV-infected persons, before and after 24months on early ART in the ANRS 12136 Temprano Trial. AIDS Res Ther. 2016;13(1):1–12. doi:10.1186/s12981-016-0094-y
6. Anuurad E, Bremer A, Berglund L. HIV protease inhibitors and obesity. Curr Opin Endocrinol Diabetes Obes. 2010;17(5):478–485. doi:10.1097/MED.0b013e32833dde87
7. Hyle EP, Martey EB, Bekker LG, et al. Diet, physical activity, and obesity among ART-experienced people with HIV in South Africa. AIDS Care - Psychol Socio-Medical Asp AIDS/HIV. 2021:1–7.
8. Ethiopia FM. National consolidated guidelines for comprehensive HIV prevention, care and treatment. Addis Ababa: Fmoh. 2018.
9. Samji H, Cescon A, Hogg RS, et al. Closing the gap: increases in life expectancy among treated HIV-positive individuals in the United States and Canada. PLoS One. 2013;8(12):6–13. doi:10.1371/journal.pone.0081355
10. Global HIV & AIDS statistics — fact sheet | UNAIDS. Available from: https://www.unaids.org/en/resources/fact-sheet.
11. Adal M, Howe R, Kassa D, Aseffa A, Petros B. Malnutrition and lipid abnormalities in antiretroviral na ï ve HIV-infected adults in Addis Ababa: a cross-sectional study. PloS One. 2018;13:1–17.
12. Kintu A, Liu E, Hertzmark E, et al. Incidence and Risk Factors for Overweight and Obesity after Initiation of Antiretroviral Therapy in Dar es Salaam, Tanzania. J Int Assoc Provid AIDS Care. 2018;17:1–10. doi:10.1177/2325958218759759
13. Mengie T, Dejen D, Muche T, Getacher L. Under Nutrition and Its Determinants Among Adults Receiving Antiretroviral Therapy in Ethiopia: a Systematic Review and Meta-analysis. Int J Homeopathy Nat Med. 2021;7(1):1–6.
14. Koethe JR, Jenkins CA, Lau B, et al. Rising Obesity Prevalence and Weight Gain among Adults Starting Antiretroviral Therapy in the United States and Canada. AIDS Res Hum Retroviruses. 2016;32(1):50–58. doi:10.1089/aid.2015.0147
15. Crum-Cianflone NF, Mollie Roediger MS, Eberly LE, Vyas ML, Anuradha Ganesan MD. Genetic Alterations NIH Public Access. Bone. 2010;23(1):1–7.
16. Bakal DR, Coelho LE, Luz PM, et al. Obesity following ART initiation is common and influenced by both traditional and HIV-/ART-specific risk factors. J Antimicrob Chemother. 2018;73(8):2177–2185. doi:10.1093/jac/dky145
17. Getachew Y, Engidaw MT, Ayele BA, et al. Magnitude of Obesity / Overweight and Its Associated Factors Among HIV / AIDS Patients on Antiretroviral Therapy in Jimma Zone Hospitals, South West Ethiopia: hospital-Based Cross-Sectional Study. Diabetes, Metab Syndr Obes Targets Ther. 2020;13:1251–1258.
18. WHO. Global Physical Activity Questionnaire (GPAQ) Analysis Guide. Geneva World Heal Organ [Internet]; 2012;1–22. Available from: http://scholar.google.com/scholar?hl=en&btnG=Search&q=intitle:Global+Physical+Activity+Questionnaire+(GPAQ)+Analysis+Guide#1.
19. Hussein FM, Ahmed AY, Muhammed OS. Household food insecurity access scale and dietary diversity score as a proxy indicator of nutritional status among people living with HIV/AIDS, Bahir Dar, Ethiopia, 2017. PLoS One. 2018;13(6):1–9.
20. Coates J, Bilinsky P, Coates J. Household Food Insecurity Access Scale (HFIAS) for Measurement of Food Access: indicator Guide VERSION 3 Household Food Insecurity Access Scale (HFIAS) for Measurement of Food Access: indicator Guide VERSION 3. BMC Nutr. 2007:64.
21. Kennedy G, Razes M, Ballard T, Dop MC. Measurement of Dietary Diversity for monitoring the impact of food based approaches 1, 2 Gina Kennedy, Maylis Razes, Terri Ballard and Marie Claude Dop. Int Symp Food Nutr Secur Food-Based Approaches Improv Diets Rais Levels Nutr. 2010;1:46.
22. Shiferaw F, Letebo M, Misganaw A, Feleke Y, Gelibo T. Original article Non-communicable Diseases in Ethiopia: disease burden, gaps in health care delivery and strategic directions. Depression Research and Treatment. 2018;2018. doi:10.1155/2018/6135460
23. Castell GS, Rodrigo CP, de la Cruz JN, Bartrina JA. Escalas de evaluación de la inseguridad alimentaria en el hogar. Nutr Hosp. 2015;31:272–278. doi:10.3305/nh.2015.31.sup3.8775
24. Chang HH. Weight Gain and Metabolic Syndrome in Human Immunodeficiency Virus Patients. Infect Chemother. 2022;54(2):220–235. doi:10.3947/ic.2022.0061
25. Mahlangu K, Modjadji P, Madiba S. The Nutritional Status of Adult Antiretroviral Therapy Recipients with a Recent HIV Diagnosis; A Cross-Sectional Study in Primary Health Facilities. Healthcare. 2020;8(3):290. doi:10.3390/healthcare8030290
26. Nanewortor BM, Saah FI, Appiah PK, Amu H. Nutritional status and associated factors among people living with HIV / AIDS in Ghana: cross-sectional study of highly active antiretroviral therapy clients. BMC Nutr. 2021;7:1–8.
27. Molla A, Gichew S, Matiyas R, Yosef T. Malnutrition status, and its Associated Factors among Adult HIV Positive Attending ART at Public Hospitals of Bench Sheko Zone, South West. BMC. 2021:43.
28. Kemal A, Ahmed M, Teshome MS, Abate KH. Central Obesity and Associated Factors among Adult Patients on Antiretroviral Therapy (ART) in Armed Force Comprehensive and Specialized Hospital, Addis Ababa, Ethiopia. Journal of Obesity. 2021;2021. doi:10.1155/2021/1578653
29. Sax PE, Erlandson KM, Lake JE, et al. Weight gain following initiation of antiretroviral therapy: risk factors in randomized comparative clinical trials. Clin Infect Dis. 2020;71(6):1379–1389. doi:10.1093/cid/ciz999
30. Griesel R, Maartens G, Chirehwa M, et al. CYP2B6 Genotype and Weight Gain Differences between Dolutegravir and Efavirenz. Clin Infect Dis. 2021;73(11):E3902–9. doi:10.1093/cid/ciaa1073
31. Nalugga EA, Laker E, Nabaggala MS, et al. Prevalence of overweight and obesity and associated factors among people living with HIV attending a tertiary care clinic in Uganda. BMC Nutr. 2022;8:1–7.
32. Tshikuka JG, Gilbert M, Damas M, et al. Overweight and Obesity among Recipients of Antiretroviral Therapy at HIV Clinics in Gaborone, Botswana: factors Associated with Change in Body Mass Index. AIDS Research and Treatment. 2020;2020. doi:10.1155/2020/8016791.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.