")
Back to Journals » Open Access Surgery » Volume 15
Assessment of the Practice of Storage, Labeling and Usage of Anesthetic Medications in the Operation Theatres of Selected Southern Ethiopian Hospitals: A Multicenter Descriptive Cross-Sectional Study
Authors Hailu S
Received 25 March 2022
Accepted for publication 30 May 2022
Published 20 June 2022 Volume 2022:15 Pages 65—73
DOI https://doi.org/10.2147/OAS.S366258
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Luigi Bonavina
Seyoum Hailu
Department of Anesthesiology, Dilla University, Dilla, Ethiopia
Correspondence: Seyoum Hailu, Email [email protected]
Background: The practice of anesthesiology needs an anesthetist to administer multiple potent drugs with high accuracy in a highly confined area that has multiple distractions. Despite all efforts, the increased use of technology, and high standards of both invasive and non-invasive monitoring in anesthesia practice, medication errors can still occur even at well-equipped centers worldwide.
Methodology: A multicenter descriptive cross-sectional study using direct observations and interviews was done throughout the selected three hospitals to evaluate the practice of labeling, usage, and storage of anesthetic medications in the operation theatres. The data were confirmed, coded, and entered into SPSS version 25. Descriptive analysis was done. Narration and tables were used to present the findings, and results were explained in the form of frequencies and percentages.
Results: Out of all the tools designed to assess the practice of labeling, usage, and storage of anesthetic medications in the operation theatres, none of the criteria was 100% accomplished. There is the highest accomplishment for the muscle relaxants labeling with 48 (80%) of the observations clearly labeling the muscle relaxants. It was observed that in all three centers the indicator for emergency drug labeling and other patient-specific drugs were below the average accomplishment. Only 5 (8.3%) of the interviewed anesthetists report medication-related incidents, while the majority of them did not report or incompletely report them.
Conclusion and Recommendations: It is found that there were poor practices on most of the indicators for anesthetic drug storage, labeling, and usage in all sites as compared to the standards. Anesthesia practice must be understood as a high-risk activity that needs modified techniques and multimodal system redesign for a safe way to prepare and administer anesthesia drugs. The sample size for this study was small, and hence these findings should be dealt with caution and other studies with more sample size are recommended.
Keywords: drug storage, drug labeling, drug errors, anesthetics, patient safety
Background
The practice of anesthesiology needs an anesthetist to administer multiple potent drugs with high accuracy in a highly confined area that has multiple distractions. Drugs with a different mechanism of action, such as muscle relaxants, induction agents, vasopressors, vasodilators, and reversals, are often used during general anesthesia. It has been detected for some time that perioperative drug errors are a significant source of morbidity and, rarely, mortality.1,2 Most of the perioperative medication adverse events are preventable while some result in tragic outcomes.3
Despite all efforts, the increased use of technology, and high standards of both invasive and non-invasive monitoring in anesthesia practice, medication errors can still occur even at well-equipped centers worldwide.4 Most anesthetists encounter at least a single drug error from which syringe swap involving muscle relaxants is the commonest.2,5 The syringe swap of Suxamethonium chloride for fentanyl was the single commonest error with an incidence of 30%, of which 17.5% of errors were classified as dangerous which results in serious hemodynamic or other complications.6
In a study done in northern Ethiopia in 2020, the overall level of drug safety management in the operation theatre was unsatisfactory.7 Drug labeling should never be put on the empty syringes rather once the drug is drawn into a syringe before it leaves the operator’s hand.8 Drug packaging and labeling standards need urgent attention but making the system robust by protocolisation, adequate training, and work environment improvement is imperative.9
Recently, there was huge drug wastage as compared to the standard mainly due to improperly practiced pharmaceutical waste management.10 Though the overall extent of drug wastage in ORs and ICUs is a concerning issue,11 substance abuse is the most serious work environment safety issue related to the practice of anesthesiology, having an incidence of 1% per year of practicing.12 There were also some fatal incidents related to misuse and abuse of propofol among health-care providers.13
Anesthetic drug safety failures are a prevalent preventable reason for iatrogenic harm.14 The safe practice consists of timely giving drugs to the patients, preventing drug administration errors, and measures to minimize distractions.15,16 Anesthetists are given the mandate for the prescription, preparation, dispensing and labeling, administration, documentation, and monitoring of clinical effects of anesthesia drugs.15
Improper practice of labeling, usage, and storage of anesthetic medications in the operation theatres is the most fatal cause of injury to the patient. Sometimes inappropriate labeling of drugs and careless storage of drugs can cause damage to patients and external personnel. There should be clear guidelines on drug labeling and storage. The other thing is that hospitals should have a policy on how to handle critical drugs in the operation room. Anesthetists must also have awareness of the effective usage of drugs to minimize the financial loss of the hospital secondary to the wastage of drugs.
Recently in Ethiopia, the risk for patient safety from drug errors has not been elaborated on, and to my knowledge, no research has been conducted on anesthetic drug storage, labeling, and usage which is also a problem seen in most developing countries. Hence, this observational multicenter study was done to assess the practice of storage, labeling, and usage of anesthetic medications in the operation theatres of selected southern Ethiopian hospitals.
Methodology
Study Settings
A multicenter descriptive cross-sectional study using direct observations and interviews was undertaken across three hospitals. Two of the hospitals, the HUCSH and Adare general hospital are found in the Sidama region, in Hawassa town and serve as a teaching and practical center for both undergraduate and postgraduate students. The other one is DURH which is located in Dilla town and serves as a teaching and referral hospital of Dilla University. All hospitals are found in the south direction of Addis Ababa which is the capital city and has thousands of employees and give service to millions of surrounding southern Ethiopian communities in terms of multiple specialties of general medical, surgical, maternity, and child care, emergency, trauma, and critical care.
Sampling and Participants
A convenient sampling method was utilized to obtain a representative sample across the three sites. Ethical concern was exempted by the institutional review board of DURH since it was not an interventional study involving human participants, rather practice observation and only a support letter was enough to conduct this study. The practice of twenty different anesthetists with more than two years of work experience was conveniently observed and interviewed in each hospital. Written informed consent was obtained from each participant before they were enrolled in the study. The anonymity of every collected data was kept for every participant and they were allowed to withdraw from the study at any point without justifying if they feel discomfort. During a period from January 1, 2022, to February 30, 2022, four postgraduate anesthesia students were selected as data collectors and observed 20 routine elective cases in each hospital regarding the practice of storage, labeling, and usage of anesthetic medications in the operation theatres at study sites. Data was collected from all selected anesthetists on duty before, while, and after they had performed any case of elective operation during the period mentioned above. One anesthetist was observed and interviewed only once so that there were no repeated observations.
Data Collection Tool
A total of 23 indicators were developed from eleven standards from the European Board of Anaesthesiology (EBA)8 and Australian and New Zealand College of Anaesthetists (ANZCA)15 with a target achievability of 100% (Table 1). Each indicator was redefined and modified to increase its measurability while the `Yes`, `No`, `IC`, and `NA` response section was added to go in line with the local setup of the study areas. All indicators were developed in the English language, translated to the local language, and retranslated to the English language by language experts to ensure their consistency. Practice with a score of >90% was considered as an area of excellent practice, a score of 75–90% were areas of good practice and acceptable while scores of <75% were considered as areas that need critical improvements. Any additional comments provided by anesthetists were documented.
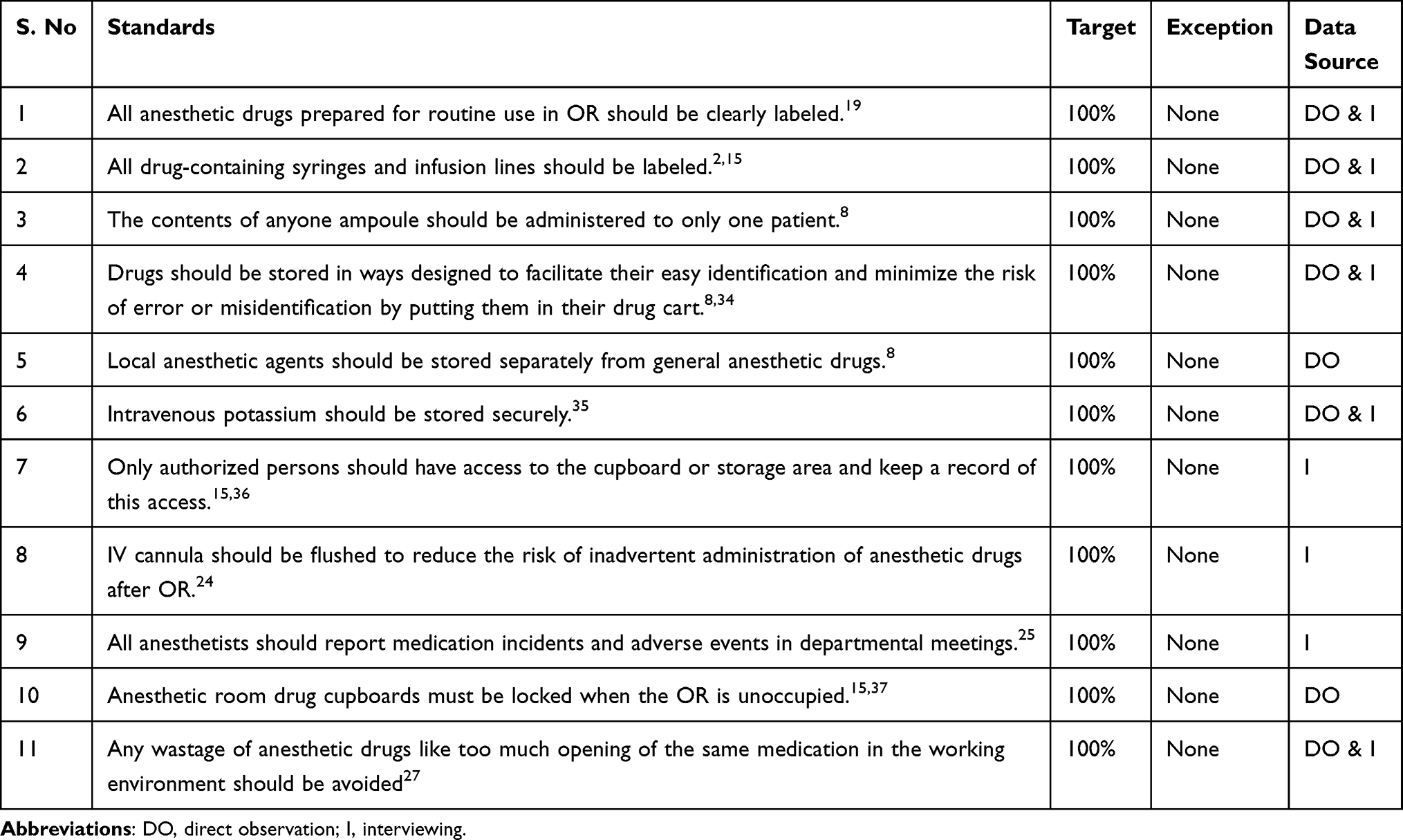 |
Table 1 Standards Developed from EBA and ANZCA |
Data Collection Process
The data collectors observed and documented their data in real-time, focusing on the practice of labeling, usage, and storage of anesthetic medications during the perioperative time. Direct observation was used to gather information on medication storage, checking procedures, and how medication syringes are labeled and stored before full administration while interviews were conducted with all 60 participants with each interview lasting 10–15 minutes conducted directly after observation. Interviews using semi-structured questionnaires were conducted with local language on issues related to who has access to propofol stores, whether they are flushing IV cannula, and whether they report any medication incidents and adverse events in departmental meetings. Before the interviews, a summary of the format questions was given to the participants to ensure that all questions were understood and discussions were made based on observations.
This study has been registered according to the Declaration of Helsinki 201317 on the Research Registry and has got a unique identifying number of the research registry researchregistry7719 (https://www.researchregistry.com/browse-the-registry#home/) Anonymity was kept throughout the data collection process. The data were checked, coded, entered, and cleaned using SPSS version 25. Descriptive analysis was done. Narratives and tables were used to present the data and results were explained in the form of frequencies and percentages.
Result
A total of sixty observations were done at the three study areas during the routine elective cases, from initial drug preparation to leaving the theatre. In all sites, anesthesia service is usually delivered by two anesthetists per table like a new graduate junior with a senior anesthetist that has more than two years of work experience plus advanced postgraduate study. Three subthematic findings were emerged from the collected data and presented in the subheading the practice of labeling, usage, and storage of anesthetic medications in the operation theatres, medication safety management, and anesthetic drug incident handling and wastage management.
The Practice of Labeling, Usage, and Storage of Anesthetic Medications in the Operation Theatres
Across all the three study areas, the key anesthetic agents were induction drugs like ketamine, thiopentone, propofol, muscle relaxants, vasopressors, narcotics, premedication drugs, reversal agents, emergency drugs and local anesthetics are usually available. At the two study sites, medications are usually prepared before the patient arrives while at the third center some of the anesthetic drugs were prescribed overnight and brought together with the patient to the OR. In none of the centers, medications were prepared for the whole schedule list ahead of time.
In all three sites, anesthetic induction solely takes in the confine of the OR table and there was no induction room. Regarding the practice of anesthetic drug preparation, the drawing up of the medication was done by either of the anesthetists who are responsible to handle the case.
Out of all the tools designed to assess the practice of labeling, usage, and storage of anesthetic medications in the operation theatres, none of the criteria was 100% accomplished. There is the highest accomplishment for the muscle relaxants labeling with 48 (80%) of the observations clearly labeling (specific name with its` concentration) the muscle relaxants like suxamethonium, vecuronium, and pancuronium while the preparation of any other drugs for a patient-specific need is at lowest accomplishment 6 (10%) as compared to the others (Table 2). Emergency drugs were not pre-prepared rather if needed they were usually drawn up from their vials at the moment of incident and given without any clear labeling.
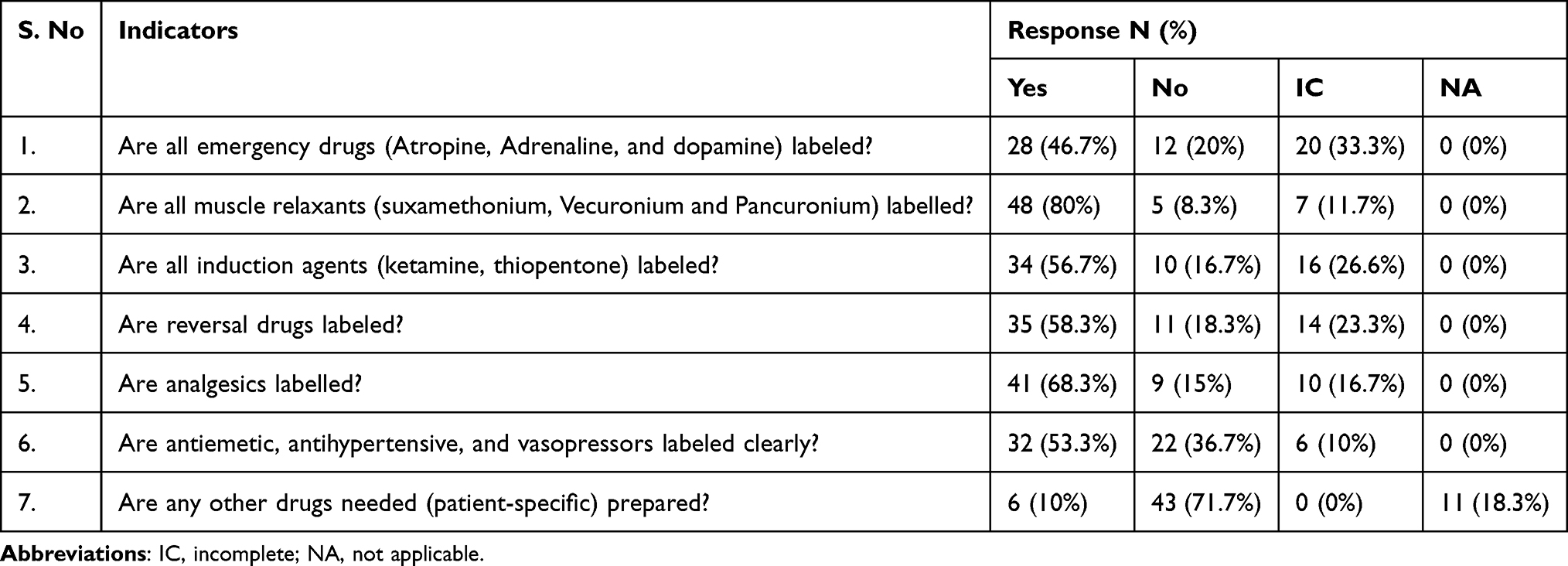 |
Table 2 A Tool Designed to Assess the Practice of Labeling, Usage, and Storage of Anesthetic Medications in the Operation Theatres |
In all sites, there were no pre-printed drug labels, and a plaster on which a complete drug name with its` concentration was written with a pen was used for labeling which might bring medication errors as there is a similarity in shape, size, and type of the syringe and label. It was observed that in all three centers the indicator for emergency drug labeling and other patient-specific drugs were below the average accomplishment.
Medication Safety Management
Regarding medication safety management, there is no or little achievement across the study areas. It was observed that there were anesthesia drug carts in all OR of the three sites with 100% accomplishment (Table 3). Despite this, there are still poor drug handling practices like drugs are poorly stored in ways designed to facilitate their easy identification and reduce the risks of error with a score of only 15 (25%) out of 60 observations. It was above average score of 44 (73.3%) that local anesthetic agents were stored separately from general anesthetic drugs while there was no IV potassium in the confines of the operation theatres of all the three study areas.
 |
Table 3 A Tool Designed to Assess Medication Safety Management |
Anesthetic Drugs Incident Handling and Wastage Management
From the total of 60 observations, there were only 12 (20%) of the observations where there was flushing of IV cannula to minimize the risk of unrecognized administration of anesthetic drugs outside the OR while in 44 (73.3%) and 4 (6.7%) of the observations they did not do or incompletely done, respectively. More importantly, there was a poor trend of reporting any medication incidents and adverse events in departmental meetings so that lessons can be learned and passed on. Only 5 (8.3%) of the interviewed anesthetists report medication-related incidents while the majority of them did not report or incompletely report them (Table 4). There was too much wastage of anesthetic or other emergency drugs 43 (71.7%) in the OR. Prepared drug syringes and vials/ampoules were put on the anesthetic table at all the three sites while ketamine, atropine, local anesthetics, and muscle relaxants were among the drugs with the most wastage as there was more than one vial at a time.
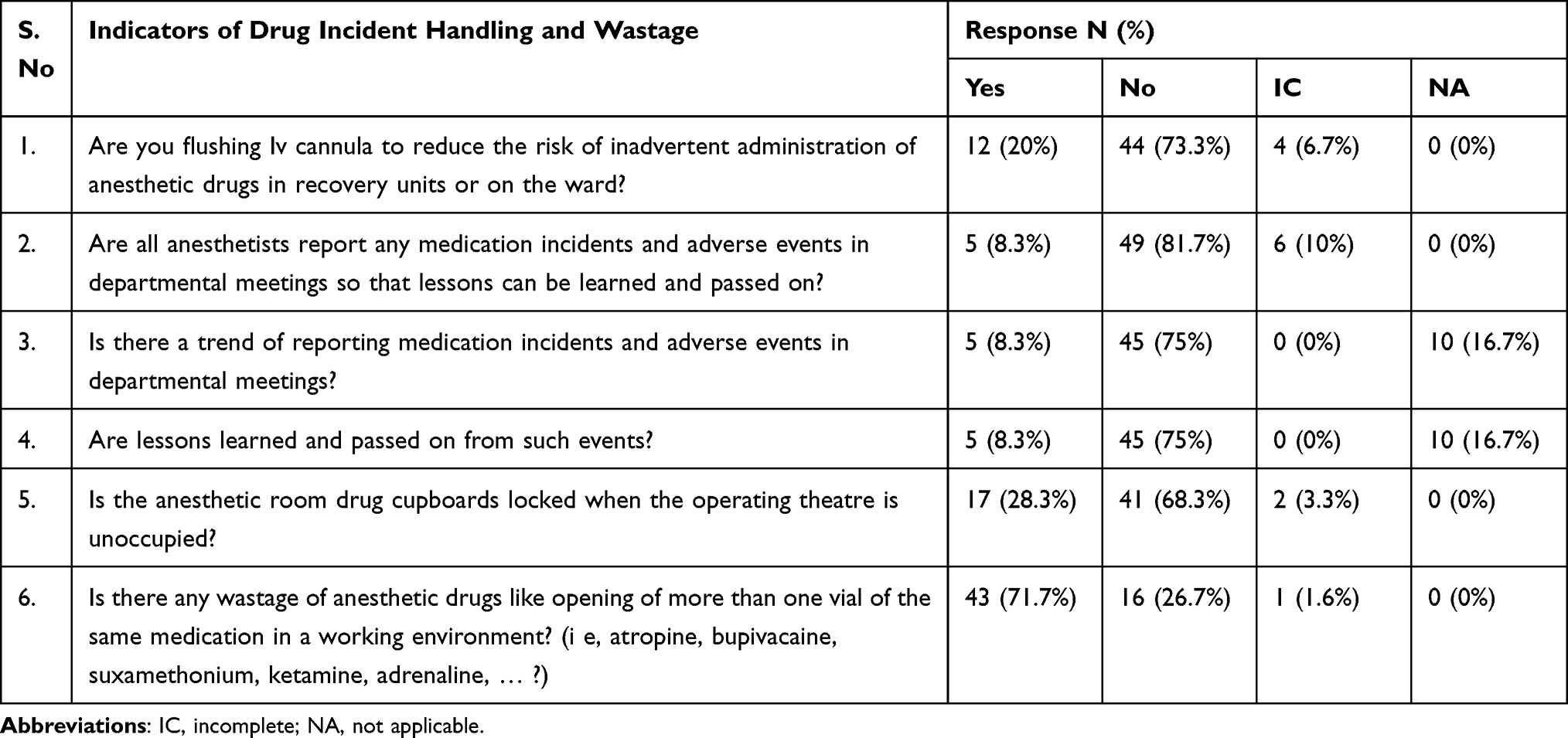 |
Table 4 A Tool Designed to Assess Anesthetic Drugs Incident Handling and Wastage Management |
Discussion
This study shows the current practices for drug storage, labeling, and usage in the three selected hospitals and aimed to contribute little not least to minimize the patient safety risks. In the current observed practice, the labeling, usage, and storage of anesthetic medications in the operation theatres were not satisfactory as the preparation of emergency drugs, and another patient-specific medication has a score of below average. These findings depict and suggest an immediate need for the improvement of anesthetic drug storage, labeling, and usage in the operation theatres.
Minimizing adverse drug events will require the involvement of all stakeholder anesthetists.18 Despite the presence of basic rules and guidelines that need to be followed whenever drugs are prepared, the practice in the observed area was by far below the standards. A study showed that the exact amount and concentration of any administered drug should be prescribed, prepared, and labeled with an ISO-normative label19 and any medicine or fluid that cannot be identified should be considered unsafe and discarded.
The result of this study shows muscle relaxants were one of the drug classes with better labeling practice 48 (80%) which is, in contrast, to a study done in India where anesthetists commonly incriminated the muscle relaxants.9 This discrepancy might be due to the anesthetists’ understanding of the serious problem of accidental administration of muscle relaxants to an un-anesthetized patient which can end up in a fatal physical or psychological problem, including death with over 90% of such incidents being related to inappropriate labeling as explained in another study.20
While the recent observation shows the availability of drug carts in the OR with 100% accomplishment there are still major safety issues concerning anesthetic drug handling as indicated with only 15 (25%) of drugs stored in ways designed to facilitate their easy identification and minimize the risks of error. The practice of anesthesiology is central to patient care and errors are unavoidable in any human endeavor but should be distinguished from negligence. The incidence of medication errors in anesthesia has been estimated as 1 per 13,000 administrations, excluding errors in recording.2 In this study, the practice of separating local anesthetics from general anesthetic agents is only in 44 (73.3%) of observations which is below the standard recommendation that states local anesthetic agents should be stored separately from general anesthetic drugs and high-risk medicines such as IV potassium should be stored securely.8
Drugs should be arranged in ways designed to facilitate their easy identification and reduce the risk of error or misidentification.21 Storing drugs according to their pharmacological groups can reduce the risk of between-class errors, which are generally more dangerous than within-class errors.21,22 Special concern should be given to storing drug ampoules that look similar, have similar names, or have labels that are difficult to read.8 There is disagreeing evidence regarding the sterility and efficacy of emergency drugs in the UK obstetric units as the majority of them routinely draw up every 24h which causes huge wastage and potential for drug error.23
Even though substance abuse is the most serious anesthesia work environment safety issue with an incidence of 1% per year of practice,12 there was no system to check that only authorized persons were accessing the cupboard or storage area among all the study areas. This might be explained by the lack of awareness and areas that are given less attention as some agents like opioids and even some of the misuse and abuse of propofol have been reported with fatal outcomes.13
Flushing of venous catheters with NS is important and probably the most crucial factor in the prevention of malfunction and minimizing the risk of unrecognized administration of anesthetic drugs out of the theatres.8,24 In this study, there was a poor report of medication incidents and adverse events in departmental meetings which is in contrast with the EBA recommendations for safe medication practice indicating that all anesthetists should report any medication incidents to their local and/or national incident reporting systems and these should be regularly reviewed in departmental meetings so that lessons can be learned from.8,25 Incomplete documentation of the drug adverse events, lack of experience, and the unavailability of local or national incident reporting systems might be the reason for this outcome.
At all sites, anesthetics and other drug preparation were done on a table near the bedside in the operating room which was prone to distractions and wastages of drugs as there were multiple vials/ampoules of the same medications were observed opened at a time. Distractions must be kept to a minimum or avoided by ensuring the availability of a designated drug preparation workspace. Anesthetic drug wastage is a common problem faced in recent anesthetic practice which significantly contributes to unwanted health-care budget allocation and financial loss.26 Even though the wastage amount in terms of financial cost was not covered in this study, there were significant wastages of anesthetic drugs in 43 (71.7%) of observations and mostly seen with ketamine, muscle relaxants, local anesthetic, and atropine were among the drugs which contribute highly to the total wastage. Proper use of all drugs and appropriate wastage management was recommended to minimize the wastage of anesthetic drugs.27 Poor team coordination and lack of a system to control the number of consumed drugs might lead to huge wastages.
Policies and guidelines should available to ensure improvement in the usage of drugs within the operation and induction rooms.28 The European Board of Anaesthesiologists (EBA) recommends the International Organisation for Standardisation (ISO) anesthetic and respiratory equipment.8 Local protocols would be needed for the minimum required drugs to be drawn up in each designated location and an assistant seems to be ideal for preparing and labeling the syringes in all set-ups.29
A multimodal system-designed approach can reduce errors in the recording and administration of drugs in anesthesia as compared to conventional methods.30–33 The lack of resources and technologies in developing countries hinders the implementation of this system redesign.
Study Strengths and Limitations
This was a multicenter study and built a complete image of the recent practice of storage, labeling, and usage of anesthetic medications in the operation theatres. It is believed to help the anesthetists to reduce the potential for anesthetic drug errors and wastage. The sample size for this study was small and hence these findings should be dealt with caution and other studies with more sample size are recommended.
Conclusion
It is very important to observe the practice of storage, labeling, and usage of anesthetic medications at a multicenter level as the complex nature of anesthesia practice confirms the risk of inevitable errors. It is found that there were poor practices on most of the indicators for anesthetic drug storage, labeling, and usage in all sites as compared to the standards.
Recommendations
Anesthesia practice must be understood as a high-risk activity that needs modified techniques and multimodal system redesign for a safe way to prepare and administer anesthesia drugs. These techniques should be endorsed to improve staff awareness and minimize drug errors or wastages.
Abbreviations
DURH, Dilla University Referral Hospital; HUCSH, Hawassa University Comprehensive Specialized Hospital; ICU, Intensive care Unit; OR, Operation Room; IV, Intravenous; NS, Normal Saline.
Ethical Approval
This research has been exempted by the Institutional Review Board of Dilla University College of Medicine and Health Science from requiring ethical approval as it does not involve interventional human participants. Registration of research studies – researchregistry7719.
Consent
All participants were asked to sign the informed consent and interviewed based on only their interests. Their response was kept anonymous and there was no identifier of the participants.
Acknowledgments
I would like to acknowledge all OR members and students for their cooperation and contribution to this work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
Guarantor – Seyoum Hailu. Provenance and peer review – not commissioned, externally peer-reviewed. The author reports no conflicts of interest in relation to this work.
References
1. Nanji KC, Patel A, Shaikh S, Seger DL, Bates DW. Evaluation of perioperative medication errors and adverse drug events. Anesthesiology. 2016;124(1):25–34. doi:10.1097/ALN.0000000000000904
2. Gordon PC, Llewellyn RL, James MF. Drug administration errors by South African anaesthetists–a survey. S Afr Med J. 2006;96(7):630–632.
3. Wahr J, Abernathy III J, Lazarra E, et al. Medication safety in the operating room: literature and expert-based recommendations. BJA. 2017;118(1):32–43. doi:10.1093/bja/aew379
4. Kothari D, Gupta S, Sharma C, Kothari S. Medication error in anaesthesia and critical care: a cause for concern. Indian J Anaesth. 2010;54(3):187. doi:10.4103/0019-5049.65351
5. Khan F, Hoda M. Drug related critical incidents. Anaesthesia. 2005;60(1):48–52. doi:10.1111/j.1365-2044.2004.04014.x
6. Gordon P. Wrong drug administration errors amongst anaesthetists in a South African teaching hospital. South African J Anaesth Analg. 2004;10(2):7–8. doi:10.1080/22201173.2004.10872353
7. Workie MM, Chekol WB, Fentie DY, Bizuneh YB, Ahmed SA. Drug safety management in the operation room of referral hospital: cross-sectional study. Int J Surg Open. 2020;26:97–100. doi:10.1016/j.ijso.2020.08.002
8. Whitaker D, Brattebø G, Trenkler S, et al. The European Board of Anaesthesiology recommendations for safe medication practice: first update. Eur J Anaesthesiol. 2017;34(1):4–7. doi:10.1097/EJA.0000000000000531
9. Kadhe NG, Patil S, Rustagi PS, Karnik HS, Thakur DP, Pawar SR. Survey of drug errors in anaesthesia at Tertiary Care Public Hospitals of Mumbai, India. Br J Pharm Med Res. 2020;05(03):2357–2364.
10. Mohammed SA, Kahissay MH, Hailu AD, Sapkota B. Pharmaceuticals wastage and pharmaceuticals waste management in public health facilities of Dessie town, North East Ethiopia. PloS one. 2021;16(10):e0259160. doi:10.1371/journal.pone.0259160
11. Barbariol F, Deana C, Lucchese F, et al. Evaluation of drug wastage in the operating rooms and intensive care units of a regional health service. Anesth Analg. 2021;132(5):1450–1456. doi:10.1213/ANE.0000000000005457
12. Tetzlaff J, Collins GB, Brown DL, Leak BC, Pollock G, Popa D. A strategy to prevent substance abuse in an academic anesthesiology department. J Clin Anesth. 2010;22(2):143–150. doi:10.1016/j.jclinane.2008.12.030
13. Monroe T, Hamza H, Stocks G, Scimeca PD, Cowan R. The misuse and abuse of propofol. Subst Use Misuse. 2011;46(9):1199–1205. doi:10.3109/10826084.2011.564705
14. Mackay E, Jennings J, Webber S. Medicines safety in anaesthetic practice. BJA Educ. 2019;19(5):151. doi:10.1016/j.bjae.2019.01.001
15. Anaesthetists AaNZCo. Guidelines for the Safe Management and Use of Medications in Anaesthesia. Australian and New Zealand College of Anaesthetists; 2021.
16. Marshall S, Chrimes N. Medication handling: towards a practical, human‐centred approach. J Anaesthesia. 2019;74(3):280–284. doi:10.1111/anae.14482
17. Association WM. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
18. Merry AF, Shipp DH, Lowinger JS. The contribution of labelling to safe medication administration in anaesthetic practice. Best Pract Res Clin Anaesthesiol. 2011;25(2):145–159. doi:10.1016/j.bpa.2011.02.009
19. Kaufmann J, Wolf AR, Becke K, Laschat M, Wappler F, Engelhardt T. Drug safety in paediatric anaesthesia. BJA. 2017;118(5):670–679. doi:10.1093/bja/aex072
20. Victorian AM. Therapeutic advisory group quality use of medicines time for change: proposed safety improvements to the labelling and packaging of neuromuscular blocking agents in Australia. Melbourne, Australia; 2014.
21. Bickham P, Golembiewski J, Meyer T, Murray CG, Wagner D. ASHP guidelines on perioperative pharmacy services. Am J Health Syst Pharm. 2019;76(12):903–920. doi:10.1093/ajhp/zxz073
22. Shultz J, Davies JM, Caird J, Chisholm S, Ruggles K, Puls R. Standardizing anesthesia medication drawers using human factors and quality assurance methods. Can J Anaesth. 2010;57(5):490–499. doi:10.1007/s12630-010-9274-8
23. Stone JP, Fenner LB, Christmas TR. The preparation and storage of anaesthetic drugs for obstetric emergencies: a survey of UK practice. Int J Obstet Anesth. 2009;18(3):242–248. doi:10.1016/j.ijoa.2009.01.013
24. Goossen GA. Flushing and locking of venous catheters. Nurs Res Pract. 2015;2015. doi:10.1155/2015/985686
25. MacLennan AI, Smith AF. An analysis of critical incidents relevant to pediatric anesthesia reported to the UK national reporting and learning system, 2006–2008. Paediatr Anaesth. 2011;21(8):841–847. doi:10.1111/j.1460-9592.2010.03421.x
26. Yimer HYS, Yalew S. Audit on wastage of commonly used anaesthetic and analgesic agents in developing country: the case of Ethiopian University Teaching Hospital. J Anesth Clin Res. 2017;8(11):778. doi:10.4172/2155-6148.1000778
27. Chaudhary K, Garg R, Bhalotra AR, Anand R, Girdhar K. Anesthetic drug wastage in the operation room: a cause for concern. J Anaesthesiol Clin Pharmacol. 2012;28(1):56–61. doi:10.4103/0970-9185.92438
28. Imran M, Khan FA, Abbasi S. Standards for labelling and storage of anaesthetic medications–an audit. J Pak Med Assoc. 2009;59(12):825–828.
29. Kulcsar Z, Bredin S, Seigne P, Iohom G. Anaesthetic emergency drug preparation and storage: 17AP2–4. Eur J Anaesthesiol. 2010;27(47):234. doi:10.1097/00003643-201006121-00755
30. Merry AF, Webster CS, Hannam J, et al. Multimodal system designed to reduce errors in recording and administration of drugs in anaesthesia: prospective randomised clinical evaluation. BMJ. 2011;343:d5543.
31. Maximous R, Wong J, Chung F, Abrishami A. Interventions to reduce medication errors in anesthesia: a systematic review. Can J Anaesth. 2021;68(6):880–893. doi:10.1007/s12630-021-01959-7
32. Bowdle T, Jelacic S, Nair B, et al. Facilitated self-reported anaesthetic medication errors before and after implementation of a safety bundle and barcode-based safety system. Br J Anaesth. 2018;121(6):1338–1345. doi:10.1016/j.bja.2018.09.004
33. Webster C, Larsson L, Frampton C, et al. Clinical assessment of a new anaesthetic drug administration system: a prospective, controlled, longitudinal incident monitoring study. Anaesthesia. 2010;65(5):490–499. doi:10.1111/j.1365-2044.2010.06325.x
34. Orser BA, Hyland S, Sheppard UD, Wilson CR, Wilson CR. Review article: improving drug safety for patients undergoing anesthesia and surgery. Can J Anaesth. 2013;60(2):127–135. doi:10.1007/s12630-012-9853-y
35. Charpiat B, Magdinier C, Leboucher G, Aubrun F. Erreurs medicamenteuses avec les solutes concentres de potassium injectable: donnees de la litterature, etat des lieux et prevention [Medication errors with concentrated potassium intravenous solutions: data of the literature, context and prevention]. Ann Pharm Fr. 2016;74(1):3–11. French. doi:10.1016/j.pharma.2015.07.004
36. ANZCA; Ministry of Health; Health Quality & Safey Commission New Zealand. Advisory statement on the storage of propofol in clinical settings; 2019. Available from: https://www.anzca.edu.au/resources/professional-documents/statements/advisory-statement-on-the-storage-of-propfol-in-cl.pdf. Accessed June 6, 2022.
37. (AAGBI) TRCoARaAoAoGBaI. Storage of Drugs in Anaesthetic Rooms. The Royal College of Anaesthetists (RCoA) and Association of Anaesthetists of Great Britain and Ireland (AAGBI); 2016.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.