")
Back to Journals » Patient Preference and Adherence » Volume 18
Are Saudi Arabian Patients Willing to Be Deprescribed Their Medications? An Exploratory Study
Authors Alhurishi SA , AlQahtani MF
Received 27 October 2023
Accepted for publication 5 March 2024
Published 27 March 2024 Volume 2024:18 Pages 779—786
DOI https://doi.org/10.2147/PPA.S446873
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Sultana A Alhurishi,1 Munerah Fahad AlQahtani2
1Community Health Sciences Department, College of Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia; 2Health Education Department, Muzahimiyah General Hospital, Riyadh, Saudi Arabia
Correspondence: Sultana A Alhurishi, Email [email protected]
Purpose: Deprescribing is a complex process that requires active patient involvement, so the patient’s attitude to deprescribing is crucial to its success. This study aimed to assess predictors of Saudi Arabian patients’ willingness to deprescribe.
Patients and Methods: In this cross-sectional study, adult patients from two hospitals in Riyadh completed a self-administered questionnaire gathering data on demographic information and the Arabic revised Patients’ Attitudes Towards Deprescribing (rPATD) questions. Descriptive analysis and binary logistic regression were used to analyze the data.
Results: A total of 242 patients were included (mean age 59.8 (SD 11.05) years, range 25– 87 years; 40% 60– 69 years; 54.1% female). The majority (90%) of participants were willing to have medications deprescribed. Willingness to deprescribe was significantly associated with the rPATD involvement factor (OR=1.866, 95% CI 1.177– 2.958, p=0.008) and the patient’s perception of their health status (OR=2.08, CI=1.058– 4.119, p=0.034).
Conclusion: The majority of patients were willing to have one or more medications deprescribed if recommended by their doctors. Patient perceptions about their own health and their involvement in deprescribing were important predictive factors that could shape counseling and education strategies to encourage deprescribing.
Keywords: polypharmacy, deprescribing, Arabic, rPATD, Saudi Arabia, patients attitude and health services administration
Introduction
Polypharmacy describes the use of multiple medicines,1 and its prevalence is increasing, especially in high-income countries.2 However, polypharmacy, especially in older people, poses risks of adverse drug reactions, cognitive and physical changes, increased hospital admissions, and even death.2 Deprescribing is an important concept that aims to reduce adverse outcomes due to polypharmacy.2 Reeve et al3 defined deprescribing as the process of withdrawal of an inappropriate medication, supervised by a healthcare professional, with the goal of managing polypharmacy and improving outcomes. Indeed, deprescribing has been shown to improve patient outcomes.4 Given the other physiological and social changes faced by older adults,5 reducing unnecessary prescribing in older patients might be a good way to improve their function and/or quality of life.4,5
Effect of deprescribing varied by age. Reduction in mortality was noted among older people less than 80 years; however, mortality of those aged 80 years or more did not change.6 Effective communication with patients is crucial to limit the withdrawal and relapse effects.7 Patients’ might depend on the clinician’s decision and initiation to start deprescribing even though they were willing to cease medications.7 Topics related to medication deprescribing include the body's response to medications, medication effectiveness, medication adverse effects and emerging treatment plan should be discussed thoroughly, especially with older aged patients.8
Nevertheless, deprescribing faces several challenges including patient and physician attitudes to deprescribing as well as organizational factors.9 From the physician perspective, deprescribing is challenged by a lack of knowledge about the deprescribing process, decisions and coordination of the process between patient, doctor, and pharmacist, and time constraints.10
The prevalence of polypharmacy among Saudi older patients was 51.5%.11 There were significant differences in polypharmacy among patients according to the region where they live, their income, and the health problems they suffered from.11 The consequences of polypharmacy on patients4 and the benefits of deprescribing12 suggest the need to implement deprescribing. However, patients as medication users play a fundamental role in the success of medication cessation process. The revised Patients’ Attitudes Towards Deprescribing (rPATD) questionnaire was developed to describe patients’ attitude toward deprescribing13 the rPATD was validated in Arabic;14 however, context-specific evidence about attitudes towards deprescribing among Saudi patients is limited. This study aimed to assess patients’ willingness to deprescribe, and factors associated with medication deprescription in Saudi Arabia.
Methods
This was a cross-sectional study conducted between October and November 2022 at two public hospitals in Riyadh. Study participants were selected by convenience sampling of adults visiting outpatient clinics. The inclusion criteria were patients aged 18 years or over and taking three or more prescribed medications. Any patient who was unable to consent or who had mental health issues was excluded from the study. This study was reviewed and approved by the ethics committee at King Saud Medical City (no. H1RE-19-Oct22-01).
Potential participants were approached by a member of the healthcare team during one of their outpatient appointments with support from the lead author to provide assistance and answer questions. The nature of the study was described to each potential participant and, after agreeing to participate, a laminated barcode of the online link to the questionnaire was provided and technical guidance provided to help with accessing, consenting, and completing the survey. The data collection team did not intervene or help in answering any questions in the survey. If the patient had visual impairment, the data collection team helped with reading questions. No incentives were provided to participate in the study.
Measures
The revised Patients’ Attitudes Toward Deprescribing (rPATD) questionnaire,13 a validated tool, was used to assess patient attitudes towards medication deprescribing. The rPATD contains 22 statements and is assessed using a five-point Likert scale: strongly agree to strongly disagree. These statements are split into domains of burden, appropriateness, concerns about stopping, involvement factors, and two questions about the overall satisfaction with medications and willingness to deprescribe.13 The rPATD has previously been translated and validated in Arabic,14 and that version was used here.
Statistical Analysis
A total of 242 patients were included in the analysis, consistent with sample sizes in other studies on the topic.15,16
Data were analyzed using SPSS v28.17 Descriptive statistics were used to analyze participant characteristics and their attitudes towards deprescribing. Pearson’s chi-squared test was used to assess for differences in characteristics between patients who were or were not willing to have one medication deprescribed. In this study, the dependent variable was the global question about patients’ willingness to deprescribe one medication, which was dichotomized into agree (including agree and strongly agree answers) and disagree (including unsure, disagree, and strongly disagree answers). The independent variables were age (≤29, 30–39,40–49, 50–59, 60–69, ≥70), sex, education (less than high school, high school, diploma, bachelor, postgraduate), health status (poor, fair, good, very good, excellent), and number of prescribed medications (3, 4, 5, 6, 7–10).
Multivariable binary logistic regression was used to determine predictors of patient willingness to be deprescribed, with the same dependent variable and demographic categorizations as above. rPATD statements were grouped into burden, appropriateness, concerns about stopping, and involvement factors, with responses dichotomized into agree (strongly agree and agree) and disagree (strongly disagree, disagree, and uncertain). In the adjusted binary logistic model, patient willingness to deprescribe was dichotomized as in a similar analysis16 into as (1) unsure, disagree, or strongly disagree and (2) strongly agree or agree. Odds ratios (OR) with 95% confidence intervals (CI) were calculated, and the significance level was set to p < 0.05.
Results
A total of 521 patients were approached to participate, and 400 were enrolled in the study, of whom 158 were excluded due to incomplete questionnaires or not meeting the inclusion criteria of taking three or more medications. A total of 242 participants who completed the survey in full and who had three or more prescribed medications were included in the analysis, a response rate of 60.5% (Figure 1).
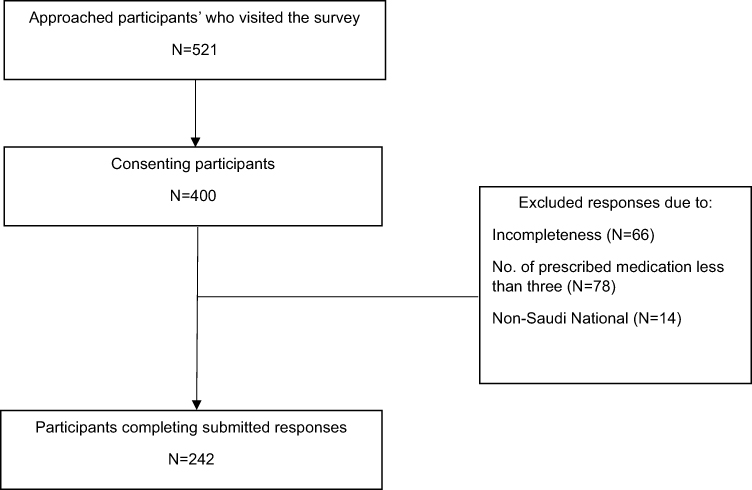 |
Figure 1 Flow chart of participant inclusion. |
The mean age of the study population was 59.8 (SD 11.05) years (range 25–87 years; 40% in the 60–69-year-old group). There was a slight female predominance in the sample (54.1%). The majority had a high school education (80%). Over half the sample rated their health as good (57.4%), and the majority (57%) were prescribed 3 or 4 medications (range 3–10, mean 4.5 (SD 1.349) (Table 1).
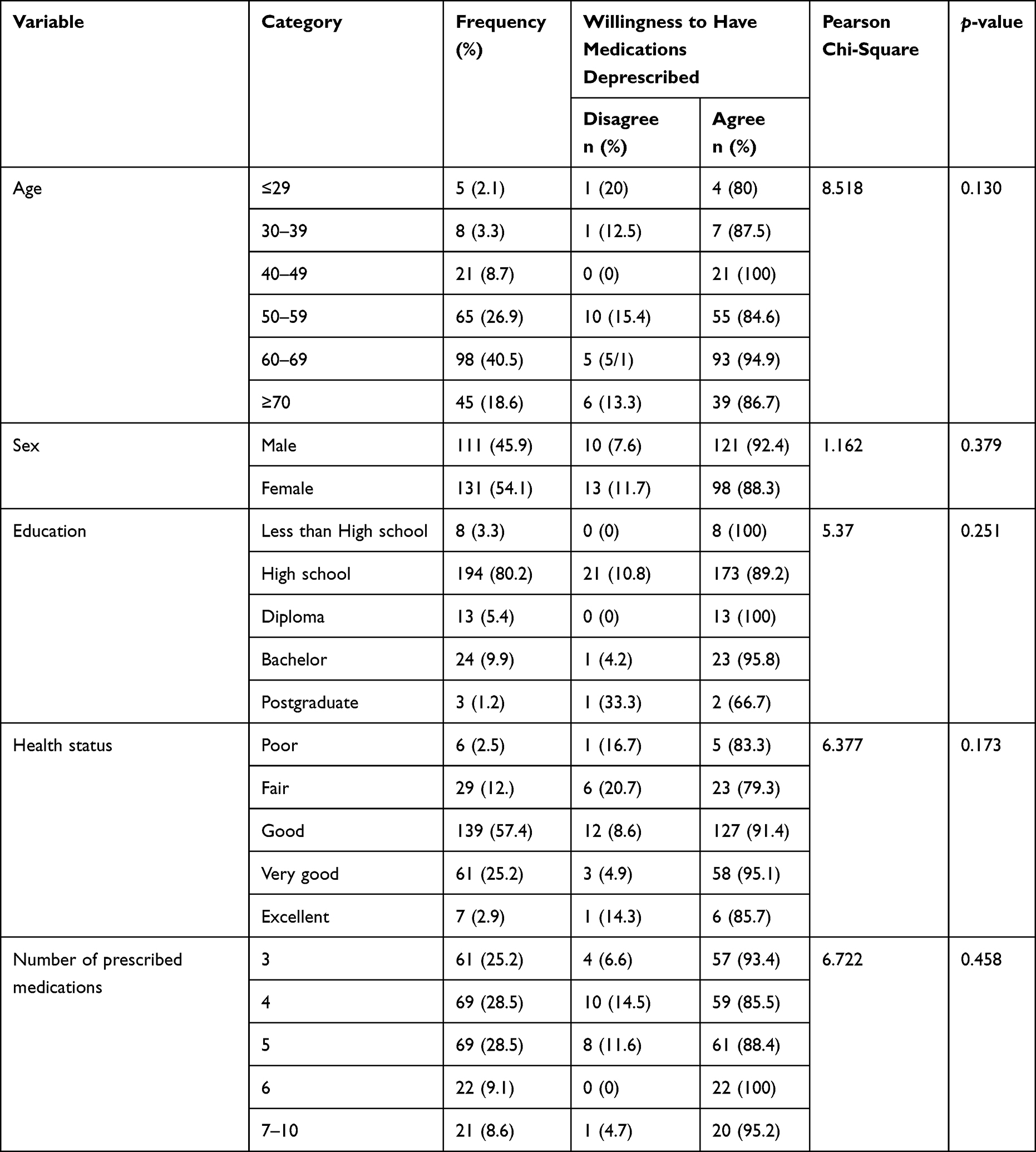 |
Table 1 Distribution of the Study Sample According to Willingness to Have Medications Deprescribed (N = 242) |
The majority of study participants (90%) were willing to stop one or more of their regular medications if the doctor said it was possible (agree 70.2%, strongly agree, 20.2%) (Table 2). Less than half of the participants (43%) were satisfied with their current medications (agree 34.7%, strongly agree 8.3%) (Table 2). The median rPATD sum scores were 4 for the burden factor, 4 for the appropriateness factor, 3.2 for the concerns about stopping factor, and 4 for the involvement factor (see Supplementary Table S1 for details). There were no significant differences in sociodemographic variables between those who were willing to be deprescribed and those who were not.
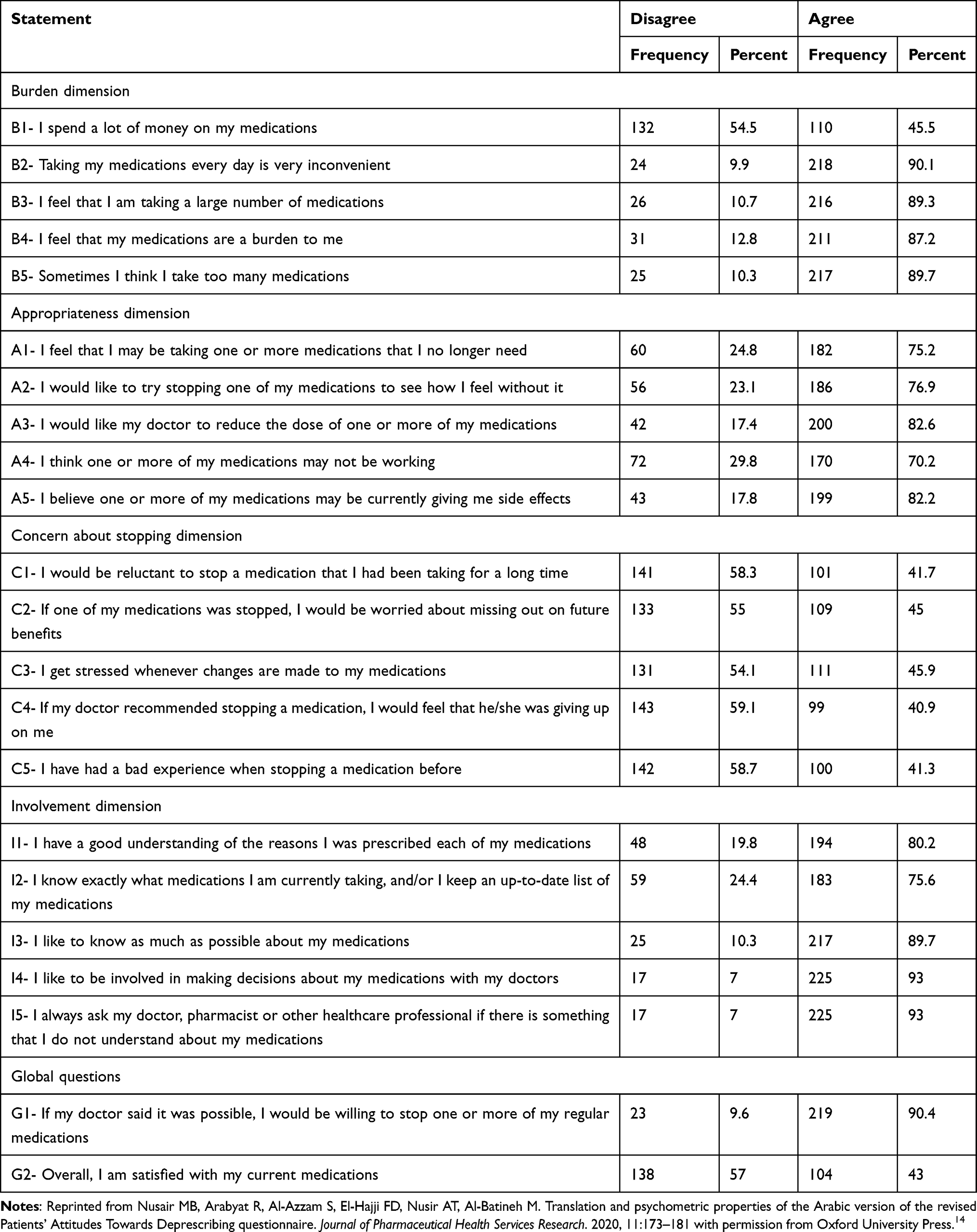 |
Table 2 Participant Responses to the rPATD Questionnaire |
Dichotomized responses (agree or disagree) to the rPATD questions are shown in Table 2. While for many questions patients were about equally split in terms of agreement, there were a few majority perceptions. The majority (~90%) agreed that taking medications every day is very inconvenient, felt that they took a large number of medications, and regarded their medications as a burden. Approximately three-quarters of patients agreed that they took one or more medications that they no longer needed and agreed that they would like to try stopping one or more of their medications and reduce the dose of one or more medications (82.6%). Many thought that one or more of their medications may not be working and that one or more of their medications may be giving them side-effects (82.2%). About 80.2% of patients agreed that they had a good understanding of the reasons they were prescribed their medications, and most (75.6%) knew exactly what their medications were and liked to know as much as possible about their medications (89.7%). The vast majority wanted to be involved in medication decision-making (93%) and asked healthcare workers if they were unsure about their medications (93%).
Results of the multivariable binary logistic regression model to identify predictors of accepting deprescribing are presented in Table 3. Patients’ willingness to deprescribe one or more medications was significantly associated with two factors: rPATD involvement factor (OR=1.866, 95% CI 1.177–2.958, p=0.008) and the patient’s perception of their health status (OR=2.08, CI=1.058–4.119, p=0.034). However, demographic factors such as age, sex, education, and other rPATD factors were not significantly associated with patients’ willingness to deprescribe.
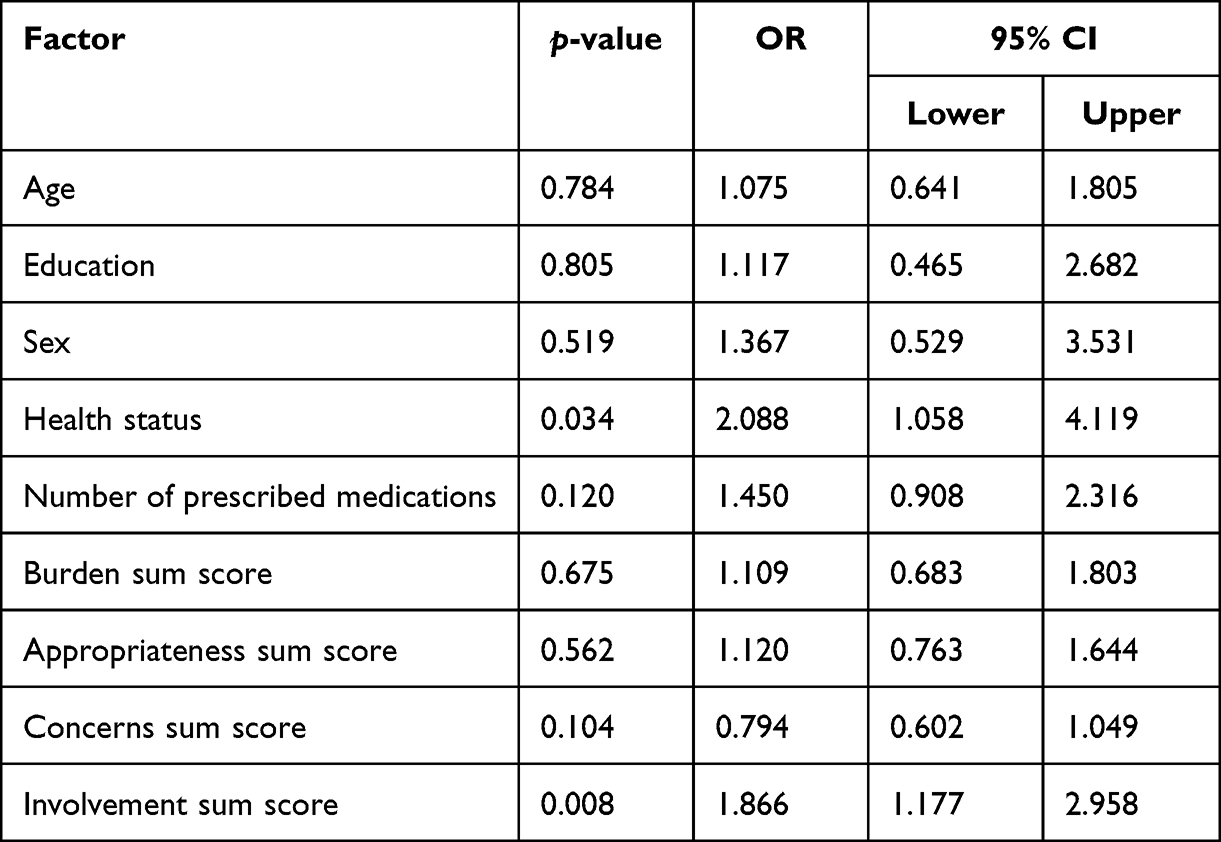 |
Table 3 Factors Associated with Willingness to Accept Deprescribing by Doctors (n=242) |
Discussion
This study examined factors related to patients’ willingness to deprescribe in Saudi Arabia. The most important predictor of willingness to deprescribe was the patient’s perception about their health status: they were more likely to deprescribe one or more medications if recommended by their doctor if they perceived their health as good to excellent. The odds of medication deprescribing also increased if they perceived greater involvement in decision-making regarding their medications.
Our findings indicate that the majority (90%) of patients were willing to be deprescribed. This is in line with previous studies that used the rPATD questionnaire, which reported that the majority of older patients15 and patients with type 2 diabetes16 were willing to deprescribe their medication. However, only 43% were satisfied with their prescribed medications, and previous studies have reported that willingness to be deprescribed was positively associated with satisfaction with current medications.15 These differences might be explained by the complexity of patient decision-making15 and differences in the baseline health status of the populations.
Issues related to optimizing medications might explain differences in willingness to deprescribe,18 but we did not enquire about involvement and communication about medication prescription in this study. Neither sex nor education was associated with attitudes to deprescribing, consistent with the literature.18 Older age is generally considered a predictor of willingness to deprescribe at the individual level,18 but age was not a significant predictor in this study, possibly due to the age distribution in our population.
Multiple factors might enable or embed deprescription. A systematic review of the attitudes of older adults with limited life expectancy and their relatives towards deprescribing grouped possible influencing factors into four main items: patient well-being, involvement of patients and their relatives in deprescribing, healthcare professionals’ role in deprescribing, and medication-related factors.19
We also examined related attitudes to deprescribing. A qualitative study found a lack of understanding of the concept of deprescribing, the process, and patient resistance to deprescribing as barriers to deprescribing among physicians in Saudi Arabia.10 Many factors might be associated with deprescribing, and future research should take into account what might influence implementing deprescribing in practice. Our study supports the need for health education interventions to support patient decision-making toward deprescribing, especially in those who do not feel involved in their medications.
There is no consensus on the definition of polypharmacy. Many studies have defined polypharmacy as the use of five or more medications. However, some studies have defined polypharmacy simply as the use of multiple medications.20 Here, the majority of our population took 3–5 medications, lower than reported for patients with hemodialysis (average 14 ± 4.6).21 This low number of prescribed medications might have influenced attitudes towards deprescribing. A more focused analysis of older people with polypharmacy of five or more medications with specific health conditions may be helpful. Additionally, this study did not focus on the reasons for patients’ preferences describing preferences or the type of medication used. Appropriateness of and the fear of side effects, the influence of others, the process, and the dislikes the patients had might enable preferences to stop medications.22 However, barriers to medication cessation include fear and the process of deprescribing. Support for patients during medication cessation is crucial.
However, our study shows that the majority of patients were willing to have one or more medications deprescribed if recommended by their doctors. Patient perception of their own health and their involvement in the deprescribing were important predictive factors that could shape counseling and education strategies to encourage deprescribing. It is important to provide more information and feedback to patients about when stopping medications could be applied and beneficial. Because of the variation of health outcomes if a target medication is deprescribed.6 The complexity of deprescribing, the needs for individualized approach, role of healthcare professionals in supporting deprescribing, and the existing evidence about interventions to improve describing may contribute to the success of implementing depressing medications.6 Future studies could focus on barriers and facilitators to implement deprescribing, support the patients need to optimize deprescribing to control their health conditions, and clinical decision aids to support healthcare professionals’ assessment when medication needs to discontinue. Reviewing the positive effect of deprescribing diabetes medication is promising. It indicated that medication cessation can be successful among diabetic patients.23 Medication optimization is a major area that needs more research. Some medications can be stopped without harmful effects.6 The individualized care of deprescribing among older people stresses the need for guidelines to support evidence-based clinical practice.
This study has several strengths. There is only limited research into medication deprescribing in Saudi Arabia, and this study is one of few published on this topic. We used the rPATD questionnaire,13 a validated tool used worldwide,14,24,25 which may allow international comparisons. Study participants were recruited from different outpatient clinics and, although the rPATD was self-administered and data collected online, patients were approached face-to-face during one of their routine follow-up appointments so technical assistance could be given on request, important for capturing data from older individuals. However, the study was limited by restricting the analysis to complete responses only, which reduced the sample size, which may have particularly excluded some older patients with multiple comorbidities and introduced bias. We relied on estimated the sample size based on reviewing the literature; however, it would be more useful if sample size estimation was used with consideration of the response rate of participation. Additionally, we used convenience sampling to recruit participants from two health institutions, so there may have been selection bias, and the results should be generalized with caution.
Conclusion
Most patients were willing to have one or more medications deprescribed if recommended by their doctors. Patient perceptions about their own health and their involvement with their physicians in decisions about medication cessation were important predictive factors that could shape the future direction of interventions to support deprescribing.
Data Sharing Statement
All data are summarized in this manuscript, and the raw data are available from the corresponding author.
Ethics Approval and Informed Consent
This study was reviewed and approved by the ethics committee at King Saud Medical City (no. H1RE-19-Oct22-01). This study was performed according to the institutional and national research ethics committee standards and in adherence to the tenets of the Declaration of Helsinki. All participants provided informed consent to participate in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This paper did not receive any specific funding.
Disclosure
The authors have no competing interests in this work.
References
1. Masnoon N, Shakib S, Kalisch-Ellett L, Caughey GE. What is polypharmacy? A systematic review of definitions. BMC Geriatr. 2017;17:1–10.
2. Wastesson JW, Morin L, Tan ECK, Johnell K. An update on the clinical consequences of polypharmacy in older adults: a narrative review. Expert Opin Drug Saf. 2018;17(12):1185–1196. doi:10.1080/14740338.2018.1546841
3. Reeve E, Gnjidic D, Long J, Hilmer S. A systematic review of the emerging definition of ‘deprescribing’ with network analysis: implications for future research and clinical practice. Br J Clin Pharmacol. 2015;80(6):1254–1268. doi:10.1111/bcp.12732
4. Scott IA, Hilmer SN, Reeve E, et al. Reducing inappropriate polypharmacy: the process of deprescribing. JAMA Intern Med. 2015;175(5):827–834. doi:10.1001/jamainternmed.2015.0324
5. Gokula M, Holmes HM. Tools to reduce polypharmacy. Clin Geriatr Med. 2012;28(2):323–341. doi:10.1016/j.cger.2012.01.011
6. Page AT, Clifford RM, Potter K, Schwartz D, Etherton‐Beer CD. The feasibility and effect of deprescribing in older adults on mortality and health: a systematic review and meta‐analysis. Br J Clin Pharmacol. 2016;82(3):583–623. doi:10.1111/bcp.12975
7. Reeve E, Wiese MD, Hendrix I, Roberts MS, Shakib S. People’s attitudes, beliefs, and experiences regarding polypharmacy and willingness to deprescribe. J Am Geriatr Soc. 2013;61(9):1508–1514. doi:10.1111/jgs.12418
8. Farrell B, Mangin D. Deprescribing is an essential part of good prescribing. Am Fam Physician. 2019;99(1):7–9.
9. Stewart D, Mair A, Wilson M, et al. Guidance to manage inappropriate polypharmacy in older people: systematic review and future developments. Expert Opin Drug Saf. 2017;16(2):203–213. doi:10.1080/14740338.2017.1265503
10. AlRasheed MM, Alhawassi TM, Alanazi A, Aloudah N, Khurshid F, Alsultan M. Knowledge and willingness of physicians about deprescribing among older patients: a qualitative study. Clin Interv Aging. 2018;13:1401–1408. doi:10.2147/CIA.S165588
11. Aljawadi MH, Khoja AT, Alaboud NM, et al. Prevalence of polypharmacy and factors associated with it among Saudi older adults – results from the Saudi National Survey for Elderly Health (SNSEH). Saudi Pharm J. 2022;30(3):230–236. doi:10.1016/j.jsps.2022.01.003
12. Reeve E, Wiese MD. Benefits of deprescribing on patients’ adherence to medications. Int J Clin Pharm. 2014;36(1):26–29. doi:10.1007/s11096-013-9871-z
13. Reeve E, Low L-F, Shakib S, Hilmer SN. Development and validation of the revised patients’ attitudes towards deprescribing (rPATD) questionnaire: versions for older adults and caregivers. Drugs Aging. 2016;33(12):913–928. doi:10.1007/s40266-016-0410-1
14. Nusair MB, Arabyat R, Al-Azzam S, El-Hajji FD, Nusir AT, Al-Batineh M. Translation and psychometric properties of the Arabic version of the revised patients’ attitudes towards deprescribing questionnaire. J Pharm Health Ser Res. 2020;11(2):173–181. doi:10.1111/jphs.12340
15. Pereira A, Ó R, Veríssimo M. Predictors of older patients’ willingness to have medications deprescribed: a cross‐sectional study. Basic Clin Pharmacol Toxicol. 2023;133(6):703–717. doi:10.1111/bcpt.13874
16. Oktora MP, Yuniar CT, Amalia L, Abdulah R, Hak E, Denig P. Attitudes towards deprescribing and patient-related factors associated with willingness to stop medication among older patients with type 2 diabetes (T2D) in Indonesia: a cross-sectional survey study. BMC Geriat. 2023;23(1):1–11. doi:10.1186/s12877-022-03718-9
17. IBM Corp. IBM SPSS statistics for windows. Volume version 28.0. IBM Corp, Armonk,NY; Released 2021.
18. Oktora MP, Edwina AE, Denig P. Differences in older patients’ attitudes toward deprescribing at contextual and individual level. Front Public Health. 2022;10:795043. doi:10.3389/fpubh.2022.795043
19. Burghle A, Lundby C, Ryg J, et al. Attitudes towards deprescribing among older adults with limited life expectancy and their relatives: a systematic review. Drugs Aging. 2020;37:503–520. doi:10.1007/s40266-020-00774-x
20. Forest E, Ireland M, Yakandawala U, et al. Patient values and preferences on polypharmacy and deprescribing: a scoping review. Int J Clin Pharm. 2021;43(6):1461–1499. doi:10.1007/s11096-021-01328-w
21. Alshamrani M, Almalki A, Qureshi M, Yusuf O, Ismail S. Polypharmacy and medication-related problems in hemodialysis patients: a call for deprescribing. Pharmacy. 2018;6(3):76. doi:10.3390/pharmacy6030076
22. Reeve E, To J, Hendrix I, Shakib S, Roberts MS, Wiese MD. Patient barriers to and enablers of deprescribing: a systematic review. Drugs Aging. 2013;30(10):793–807. doi:10.1007/s40266-013-0106-8
23. Oktora M, Kerr K, Hak E, Denig P. Rates, determinants and success of implementing deprescribing in people with type 2 diabetes: a scoping review. Diabetic Med. 2021;38(2):e14408. doi:10.1111/dme.14408
24. Lukacena KM, Keck JW, Freeman PR, Harrington NG, Huffmyer MJ, Moga DC. Patients’ attitudes toward deprescribing and their experiences communicating with clinicians and pharmacists. Ther Adv Drug Saf. 2022;13:20420986221116465. doi:10.1177/20420986221116465
25. Gadisa DA, Gebremariam ET, Yimer G, Deresa Urgesa E. Attitudes of older adult patients and caregivers towards deprescribing of medications in Ethiopia. Clin Interv Aging. 2023;18:1129–1143. doi:10.2147/CIA.S400698
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.