")
Back to Journals » Open Access Surgery » Volume 16
Appendicitis During Pregnancy: Best Surgical Practices and Clinical Management
Authors Smolkin C , Kiridly A , Pryor A
Received 11 September 2023
Accepted for publication 17 November 2023
Published 21 November 2023 Volume 2023:16 Pages 95—103
DOI https://doi.org/10.2147/OAS.S405514
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Luigi Bonavina
Caroline Smolkin,1 Adam Kiridly,1 Aurora Pryor2
1Department of Surgery, Northwell North Shore/Long Island Jewish, New Hyde Park, NY, USA; 2Department of Surgery, Long Island Jewish Medical Center, Northwell Health, New Hyde Park, NY, USA
Correspondence: Caroline Smolkin, Department of Surgery, Northwell North Shore/Long Island Jewish, 270-05 76th Avenue Research Building - C Level, Room 039AB, New Hyde Park, NY, 110400, USA, Tel +1 732-299-1494, Email [email protected]
Abstract: Appendicitis is a common abdominal surgical emergency. However, treatment becomes more complex when the patient is pregnant. It is important to consider the diagnostic differences in pregnant and non-pregnant patients, as well as the changes to surgical and non-surgical management. Commonly, appendicitis in pregnancy is diagnosed with radiographic imaging, preferably ultrasound or MRI. Due to increased risk with delay to surgery, surgical management is recommended, as opposed to non-operative management, and ultimately a laparoscopic appendectomy is the surgery of choice. We aim to provide a comprehensive review of the best practices and clinical management of appendicitis in pregnancy.
Keywords: appendicitis, pregnancy, appendectomy, surgery, laparoscopic
Introduction
Appendicitis is defined as “an inflammation of the appendix that may lead to an abscess, ileus, peritonitis, or death if untreated”. It is one of the most common abdominal surgical emergencies and is currently treated with surgery if deemed uncomplicated.1 However, pregnancy increases the complexity of diagnosis and treatment of appendicitis. We seek to discuss the diagnosis of appendicitis in pregnancy, as well as the operative and non-operative differences between management in pregnant patients vs non-pregnant patients. It is critical to consider these differences to allow for safe treatment of both mother and fetus.
Causes
Appendicitis was historically thought to be associated with obstruction of the appendiceal lumen – often by appendicolith (stone of the appendix) or other mechanical etiology. Other causes of obstruction also include appendiceal tumors such as adenocarcinoma, hypertrophied lymphatic tissue and carcinoid tumors.2 However, studies measuring the pressure in the appendix pre-operatively have shown that only one-third of cases are caused by obstruction.3 Ultimately, appendicitis is an inflammation of the organ wall, and inflammation is followed by localized ischemia, perforation, and further infectious development. Bacteria build up in the appendix, leading to inflammation and possible perforation and abscess formation.4 Men and women are both affected by appendicitis with lifetime incidence slightly higher in men – 8.6% vs 6.7%.4,5 Most often, appendicitis occurs between the ages of 5 and 45, with a mean age at presentation of 28.4
Appendicitis is typically a clinical diagnosis based on history and physical examination, laboratory results, and imaging.1,6 History and physical examination may reveal initial vague periumbilical pain with migration to the right lower quadrant, nausea, vomiting, fever, rebound tenderness over McBurney’s point (1.5 to 2 inches from the anterior superior iliac spine (ASIS) on a straight line from the ASIS to the umbilicus), and indirect tenderness (right lower quadrant pain elicited by palpation of the left lower quadrant).1,2 Other physical exam signs such as psoas sign (pain on external rotation or passive extension of right hip) or obturator sign (pain on internal rotation of the right hip) are rarer, and in reality not used.4
Changes with Pregnancy
The diagnosis rate of acute appendicitis in pregnancy has been reported to be around 7 per 10,000 person-years during the first two trimesters, and 4.6 per 10,000 person years, compared to the incidence of acute appendicitis in the general population – approximately 2.45 per 10,000 person-years.2,4,7–9 As previously mentioned, appendicitis often affects patients age 5 through 45 (with an average age of 28) which also includes a woman’s childbearing years, as well as average year for first childbirth of approximately 26.4,10 Diagnosis becomes difficult in pregnancy due to the presence of a gravid uterus and potential displacement of appendix from its normal anatomic position. Many appendicitis clinical scoring methods exist – including Alvarado, Eskelinen, Ohmann, AIR, RIPASA, Tzanakis, Lintula, Fenyo-Lindberg, and Karaman systems.11 According to a single-center retrospective study, the Tzanakis system was the most effective scoring system in non-pregnant women, while the RIPASA was the best scoring system for pregnant patients with the PPV (positive predictive value) at 94.40%, NPV (negative predictive value) at 44%, and sensitivity and specificity were 78.46% and 78.57%, respectively (Figure 1).11 The RIPASA score includes parameters such as: sex, age, migration of pain, anorexia, fever, Rovsing’s sign, etc.12 (Table 1).
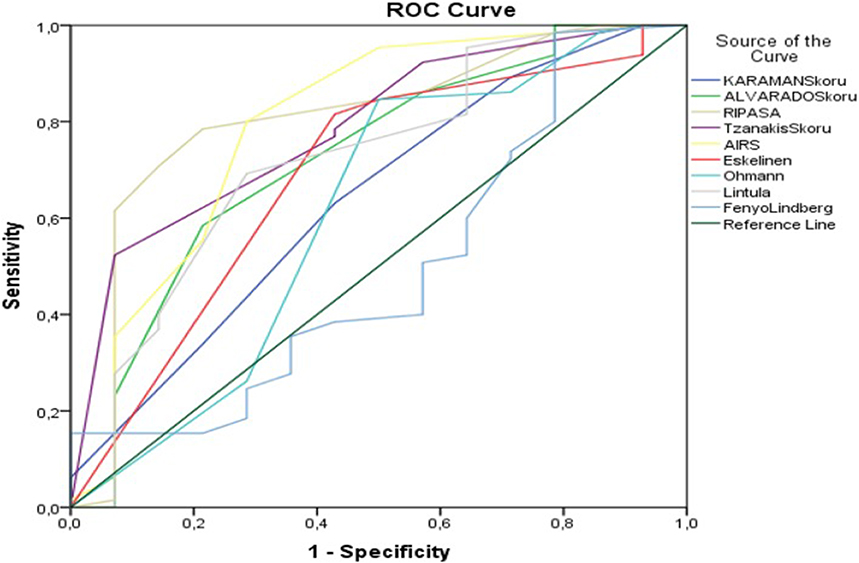 |
Figure 1 ROC curves for diagnostic performance of appendicitis scoring systems in pregnant women. Notes: Reprinted from Mantoglu B, Gonullu E, Akdeniz Y, et al. Which appendicitis scoring system is most suitable for pregnant patients? A comparison of nine different systems. World J Emerg Surg. 2020;15(1):34. Creative Commons.11 |
 |
Table 1 RIPASA Score for Acute Appendicitis |
Many symptoms of acute appendicitis may be confused with clinical manifestations of pregnancy. As mentioned, physical exam findings may not follow standard patterns as the gravid uterus may displace the appendix. Previous studies have reported the appendiceal displacement into the right upper quadrant, as high as the right hypochondrium. Alternatively, there are reports of the appendix not changing location in the abdomen from the right lower quadrant.13 This inconsistency in the location of the appendix in the pregnant patient decreases the reliability of history and physical exam in diagnosing acute appendicitis in this patient population. In addition, the white blood count is typically mildly elevated in pregnancy. The World Society of Emergency Surgery recommends not diagnosing acute appendicitis in pregnant patients on symptoms and signs alone, and emphasizes the importance to requesting laboratory testing and inflammatory markers (eg, CRP).14
Imaging with Pregnancy
Suspected appendicitis in pregnant patients can be investigated with several imaging modalities. Ultrasound can be utilized with the same diagnostic criteria used for non-pregnant patients – which includes visualization of a blind-ending, dilated (>6–7 mm in diameter) aperistaltic and noncompressible tubular structure arising from the cecum.15–17 Although ultrasound is the initial imaging modality used at many institutions for pregnant patients with suspected appendicitis, ultrasound has several limitations. Particularly, a large body habitus increases difficulty in obtaining a clear view of the appendix. Overlying bowel, gas, and the gravid uterus increases that difficulty further.18 Due to these barriers, the appendix can only be visualized in pregnant patients approximately 60% of the time.19
Other imaging modalities can be used when ultrasound is inconclusive, or if additional resources are available.
While MR imaging can be used to visualize the appendix, intravenous gadolinium cannot be used in pregnant patients.15 A normal appendix on MR imaging has the following appearance: <6 mm diameter, appendiceal wall thickness <2 mm, low luminal signal intensity on T1- and T2-weighted images, and no peri-appendiceal fat stranding or fluid.15,20 Alternatively, MR imaging features of appendicitis include diameter >7 mm, appendiceal wall thickness >2 mm, appendicoliths and surrounding hyperechoic inflamed fat or hypoechoic fluid on T2-weighted images.15,16 MRI is reported as the safest imaging modality in pregnancy, with a lack of consensus regarding the risk to the fetus. However, some studies have reported potential teratogenic effects and acoustic damages.21,22 The heating effort of MR gradient changes and direct non-thermal interaction of electromagnetic field have been raised as concerning when MRI is performed early in pregnancy.21,23
CT is also an option for imaging in diagnosing appendicitis in pregnancy. However, the risk of exposing the fetus to ionizing radiation that must be considered. Ionizing radiation exposure to a fetus can increase risks of congenital malformations, mental retardation, microcephaly, and embryonic and fetal death.24 It has been previously reported that fetal mortality is greatest when radiation exposure occurs within the first week of conception. Within the first trimester, the embryo is very vulnerable to growth retarding, teratogenic, and lethal effects in weeks 3–6 post conception.24 The vulnerability to multiple organ teratogenesis decreases in weeks 8–15, but the CNS and growth potential is still at risk to be significantly affected.24 The fetus is more likely to be resistant to potential harm during second and third trimesters, although a slight risk of adverse effects remains.25 CT scans are routinely clinically done to evaluate for and diagnose appendicitis in the third trimester of pregnancy.
Radiation dosage is important to consider in pregnant patients. 50–100 mGy has been recommended as the cumulative radiation dose to the fetus during pregnancy.19 CT of the pelvis is less than 30 mGy, while a plain abdominal radiograph is approximately 1–3 mGy, so these modalities, while associated with risk, are not absolutely contraindicated.19 Ultimately, due to ultrasound’s limitations, including low accuracy and false-negatives, MRI is the preferred first-line imaging study.14,26,27
Management
Laparoscopic (as opposed to open) appendectomy has become the gold standard for surgical management of appendicitis due to shorter lengths of stays, decreased need for analgesia, earlier food tolerance, earlier return to work, and lower infection rates.28,29 Comparative outcomes of laparoscopic and open appendectomy show similar trends in pregnancy – laparoscopic approach results in shorter operative time, length of stay, and complication rate.30 According to the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES), a laparoscopic appendectomy can be performed safely in any trimester of pregnancy and is the standard of care.19,31,32 The World Society of Emergency Surgery also suggests that laparoscopic appendectomy is preferred to open appendectomy when surgery is indicated.14 This mirrors trends seen with laparoscopic surgery as a whole and is not just applicable to appendicitis and/or pregnant patients.33,34 Historic studies suggested that the safest trimester to operate laparoscopically was the second trimester; however, newer studies have demonstrated that there is minimal difference in safety regardless of trimester during which the operation takes place.19,35 These previous studies cited concerns with spontaneous abortions in the first trimester and pre-term labor in the third trimester.35,36 More recent literature shows there is risk associated with waiting until the second trimester or until after delivery, including infection or perforation. These complications were more frequent than the previously reported complications of spontaneous abortions or pre-term labor.37 Therefore, current guidelines emphasize prompt diagnosis and operative management as the safest path for both mother and fetus.19,31,35–38
Operative Approach
Pregnant patients must be placed in the left lateral decubitus position to minimize compression on the vena cava.35,39 Compression of the vena cava can cause hypotension by decreasing preload and often affects pregnant women after 20 weeks’ gestation.39,40 Placing a patient into left lateral decubitus position allows gravity and the weight of the gravid uterus to assist with exposure by sweeping the omentum and small bowel away from the appendix.41
The first step to any laparoscopic operation is port site placement to access the site of surgery (in this case the peritoneal cavity). Fundal height, the distance from the pubic bone to the top of the uterus during pregnancy, must be strongly considered prior to starting the operation.42 Normally, entrance into the abdomen for a laparoscopic appendectomy can be safely done with a Hasson technique or Verres needle. These two techniques can both be used in pregnant patients as well.35 To accommodate the gravid uterus, port placement should be above the palpable fundus and recommendations to adjust the initial access point from the umbilical area to the subcostal region have been made (Figure 2).35,43 Alternatively, the right subcostal trocar shown in Figure 2 can be placed in the left subcostal position. Studies have shown that surgeons tend to use the Veress needle more in the first trimester, whereas the Hasson technique was frequently preferred during third trimester operations.44 This shift to use of the Hasson is largely due to fear of Veress needle injury to intestine, aorta, or uterus.43 This possibility increases as the uterus becomes larger, more anterior, and causes the intestines to occupy a smaller amount of space anteriorly. If Veress access is chosen, this must be carefully performed away from the gravid uterus. Case reports have been published describing pregnancy loss due to Veress needle injury to uterus causing pneumoamnion.45
Insufflation is an essential step in laparoscopic surgery; however, it must be done with caution in pregnant patients. Insufflation causes increased intraabdominal pressures and diaphragmatic elevation. In pregnant patients, the diaphragm is already elevated, resulting in alterations to the respiratory system. Expiratory reserve volumes and functional residual capacity (FRC) both decrease with pregnancy, while inspiratory capacity increases to maintain total lung capacity.46–48 As a result of reduced FRC, incidence of atelectasis increases.49 Furthermore, respiratory resistance increases while respiratory conductance decreases.47 General guidelines suggest that CO2 insufflation of 10–15 mmHg can be safely used in laparoscopic surgery in pregnancy.35 Although there are case reports and studies implementing pressures greater than 15 mmHg with no increase in adverse effects, the majority of cases are carried out between 10 and 15 mmHg.35
 |
Figure 2 Example trocar placement (indicated by circles) in nonpregnant (A) and pregnant women in the third trimester (B). Abbreviation: JSLS, Journal of the Society of Laparoendoscopic Surgeons/Society of Laparoendoscopic Surgeons. Notes: Donkervoort S, Boerma D. Suspicion of Acute Appendicitis in the Third Trimester of Pregnancy: Pros and Cons of a Laparoscopic Procedure. 2011;15:379–383. Creative Commons.43 |
Deep vein thrombosis (DVT) prophylaxis is another important consideration for surgical patients. All patients undergoing surgery and staying in the hospital are at an increased risk of DVTs. This is superimposed on pregnancy being a hypercoagulable state with a 0.1–0.2% risk of DVTs.50 The risk of venous thromboembolism is 5x higher in pregnant patients compared to non-pregnant patients.51,52 Current recommendations for DVT prophylaxis include intraoperative and postoperative pneumatic compression devices, as well as early ambulation.35 There is limited research regarding the use of chemical prophylaxis in pregnant patients, particularly unfractionated or low-molecular-weight heparin, but heparin can be safely used with monitoring because it does not cross the placenta.52,53 In the event of DVT, warfarin should be avoided because it crosses the placenta and causes embryopathy in first trimester, as well as central nervous system and ophthalmologic abnormalities in any trimester.52
Throughout the operation, it is important to consider the anatomic effects of pregnancy. For example, in a standard laparoscopic appendectomy and in the absence of endometriosis, it is unlikely there would be adhesions to the uterus from inflammatory response. Usually, adhesions are formed to the small bowel and cecum, and blunt dissection, sharp dissection and electrocautery can be used to separate these adhesions.41 In a pregnant patient with a larger uterus, it is not unlikely for there to be adhesions to the uterus. In this case, care must be taken to avoid the gravid uterus with dissection and/or lysis of adhesions. Subsequent steps of the procedure, including creating window in the mesoappendix, division of the mesoappendix, and removal of the appendix, may be more difficult with a larger body habitus and obstruction of view from the gravid uterus. When using a stapler for appendiceal division, articulation is helpful to accommodate the uterus, although case reports have been published documenting successful use of a non-articulating stapler in pregnant patients.54
Lastly, fascial closure is often performed through the largest port site (12 mm), while 5 mm port sites are usually left open and only the skin is closed.55 Since pregnancy is a significant risk factor for hernia formation due to hormonal changes and increased intra-abdominal pressure, fascial closure in large fascial defects is a critical step in this procedure to prevent future complications.56
A retrospective case series published by Machado and Grant analyzed twenty cases with surgery occurring in all three trimesters. Additionally, some cases were performed with Veress needle entry, but most utilized Hasson technique. Three ports were utilized with placement adjustment based on gestational age and uterus position as previously described. These cases used endoloops for ligation of the appendix. In the cases described, antibiotics were only administered for 1 day for non-perforated cases and 2–3 days for phlegmonous appendicitis. Tocolysis (indomethacin 100 mg suppository) was given to 20% of patients for uterine contractility.32 These case reports emphasize the importance of co-management by an obstetric team. All patients had fetal heart rate monitoring before and after surgery. Additionally, the administration of tocolytics was based on recommendations from the obstetric team. Obstetricians can also assist with antibiotic and pain management due to their increased experience managing pregnant patients. This emphasizes the importance of interdisciplinary and collaborative health care.
Role of Non-Operative Management
Recently, randomized control trials have evaluated the treatment of uncomplicated appendicitis in non-pregnant patients with antibiotics alone. These studies show success rates as high as 71%. However, these studies also report that over one-third of patients will require an appendectomy within 5 years.57–59 Some even report one-third of patients undergoing an appendectomy within 90 days.57
Studies have provided conflicting conclusions regarding the effectiveness and safety of medical management of appendicitis in pregnant patients. One report suggests antibiotic therapy is a good bridge-to-surgery therapy in remote areas where immediate surgical intervention is not available.60 Another retrospective study over 4 years with over 50 pregnant patients stated that medical management is a safe and feasible option for treatment of acute appendicitis in pregnant patients.61
Although there is evidence showing that antibiotics alone can have a role in the treatment of uncomplicated appendicitis in pregnancy, surgical management remains the preferred choice,62 and it is important to consider the safety of antibiotics in pregnant patients. Most common pathogens involved in appendicitis are gram negative – primarily E. coli.63 Bacteroides fragilis, Klebsiella spp., and Streptococcus spp. are also frequently associated with appendicitis but significantly less often.63,64 These organisms are often susceptible to ampicillin, piperacillin-tazobactam, ceftriaxone, cefepime, amikacin, gentamicin, and imipenem.63 Penicillins, including ampicillin and piperacillin, are the most common antibiotic class used in pregnancy and are generally safe. Penicillins, including ampicillin and piperacillin, are the most common antibiotic class used in pregnancy and are generally safe. Penicillins combined with beta-lactamase inhibitors, like piperacillin-tazobactam, are also safe. Although used less frequently, cephalosporins, carbapenems, monobactams, and cephamycins are all safe to use as well.65
Thoughtful consideration of the possibility of unsuccessful non-operative management must be given in clinical decision-making. Some have expressed concerns of increased risk of fetal loss and premature labor in pregnant patients with peritoneal appendicitis. In acute non-perforated appendicitis, approximately 83.9% of patients give birth at term, 10.7% have preterm labor and 5.4% have an abortion.66,67 The rates of preterm labor and abortion increase in perforated appendicitis – 33.3% and 11%, respectively.66,67 The rate of these adverse effects does not differ between trimesters.66 Since there is large increase in the rate of preterm labor and abortion between non-perforated and perforated appendicitis, there should be careful consideration in opting for medical management and delaying surgical management. The 2020 Jerusalem Appendicitis guidelines and the European Association of Endoscopic Surgery 2022 Rapid Guidelines recommend again treating acute appendicitis non-operatively during pregnancy until further evidence is available and go on to recommend planning laparoscopic appendectomy.14,38
Conclusion
Appendicitis in pregnancy is a clinical condition that can be managed safely and effectively if the surgical team is well educated. It is important to consider alterations to operative procedure when compared to non-pregnant patients. Likewise, it is also important to be cognizant of pre- and post-operative management, including alterations in radiographic diagnostics, changes in laboratory results, and antibiotic selections. Current guidelines published by many national and international organizations emphasise the importance of prompt operative management, with the laparoscopic appendectomy as the surgery of choice. Treating appendicitis in pregnancy is a great example of an opportunity for interdisciplinary care between surgery and OBGYN.
Disclosure
Dr Aurora Pryor reports personal fees from Gore, Medtronic, and Stryker, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. D’Souza N, Nugent K. Appendicitis. BMJ Clin Evid. 2014;2014:1.
2. Aptilon Duque G, Mohney S. Appendicitis in pregnancy. In: StatPearls. StatPearls Publishing; 2023.
3. Arnbjörnsson E, Bengmark S. Obstruction of the appendix lumen in relation to pathogenesis of acute appendicitis. Acta Chir Scand. 1983;149(8):789–791.
4. Jones MW, Lopez RA, Deppen JG. Appendicitis. In: StatPearls. Disclosure: Richard Lopez Declares No Relevant Financial Relationships with Ineligible Companies. Disclosure: Jeffrey Deppen Declares No Relevant Financial Relationships with Ineligible Companies. Treasure Island (FL): Ineligible Companies; StatPearls Publishing Copyright © 2023;2023
5. Addiss DG, Shaffer N, Fowler BS, Tauxe RV. The epidemiology of appendicitis and appendectomy in the United States. Am J Epidemiol. 1990;132(5):910–925. doi:10.1093/oxfordjournals.aje.a115734
6. Moris D, Paulson EK, Pappas TN. Diagnosis and management of acute appendicitis in adults: a review. JAMA. 2021;326(22):2299–2311. doi:10.1001/jama.2021.20502
7. Kave M, Parooie F, Salarzaei M. Pregnancy and appendicitis: a systematic review and meta-analysis on the clinical use of MRI in diagnosis of appendicitis in pregnant women. World J Emerg Surg. 2019;14(1):37. doi:10.1186/s13017-019-0254-1
8. Zingone F, Sultan AA, Humes DJ, West J. Risk of acute appendicitis in and around pregnancy: a population-based Cohort Study from England. Ann Surg. 2015;261(2):332–337. doi:10.1097/SLA.0000000000000780
9. Flum DR, Morris A, Koepsell T, Dellinger EP. Has misdiagnosis of appendicitis decreased over time? A population-based analysis. JAMA. 2001;286(14):1748–1753. doi:10.1001/jama.286.14.1748
10. Mathews TJ, Hamilton BE. Mean age of mothers is on the rise: United States, 2000–2014. NCHS Data Brief. 2016;232:1–8.
11. Mantoglu B, Gonullu E, Akdeniz Y, et al. Which appendicitis scoring system is most suitable for pregnant patients? A comparison of nine different systems. World J Emerg Surg. 2020;15(1):34. doi:10.1186/s13017-020-00310-7
12. Regar M, Choudhary G, Nogia C, Pipal D, Agrawal A, Srivastava H. Comparison of Alvarado and RIPASA scoring systems in diagnosis of acute appendicitis and correlation with intraoperative and histopathological findings. Int Surg J. 2017;4(5):1755. doi:10.18203/2349-2902.isj20171634
13. Ishaq A, Khan MJH, Pishori T, Soomro R, Khan S. Location of appendix in pregnancy: does it change? Clin Exp Gastroenterol. 2018;11:281–287. doi:10.2147/CEG.S154913
14. Di Saverio S, Podda M, De Simone B, et al. Diagnosis and treatment of acute appendicitis: 2020 update of the WSES Jerusalem guidelines. World J Emerg Surg. 2020;15(1):27. doi:10.1186/s13017-020-00306-3
15. Masselli G, Brunelli R, Monti R, et al. Imaging for acute pelvic pain in pregnancy. Insights Imaging. 2014;5(2):165–181. doi:10.1007/s13244-014-0314-8
16. Jeffrey RB, Jain KA, Nghiem HV. Sonographic diagnosis of acute appendicitis: interpretive pitfalls. AJR Am J Roentgenol. 1994;162(1):55–59. doi:10.2214/ajr.162.1.8273690
17. Gilo NB, Amini D, Landy HJ. Appendicitis and cholecystitis in pregnancy. Clin Obstet Gynecol. 2009;52(4):586–596. doi:10.1097/GRF.0b013e3181c11d10
18. Katz DS, Klein MA, Ganson G, Hines JJ. Imaging of abdominal pain in pregnancy. Radiol Clin North Amer. 2012;50(1):149–171. doi:10.1016/j.rcl.2011.08.001
19. Pearl JP, Price RR, Tonkin AE, Richardson WS, Stefanidis D. Guidelines for the Use of Laparoscopy During Pregnancy - A Sages Publication. Board of Governors of the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES);2017.
20. Spalluto LB, Woodfield CA, DeBenedectis CM, Lazarus E. MR imaging evaluation of abdominal pain during pregnancy: appendicitis and other nonobstetric causes. Radiographics. 2012;32(2):317–334. doi:10.1148/rg.322115057
21. Bulas DMD, Egloff AMD. Benefits and risks of MRI in pregnancy. Seminars Perinatol. 2013;37(5):301–304. doi:10.1053/j.semperi.2013.06.005
22. Yip YP, Capriotti C, Talagala SL, Yip JW. Effects of MR exposure at 1.5 T on early embryonic development of the chick. J Magn Reson Imaging. 1994;4(5):742–748. doi:10.1002/jmri.1880040518
23. Saunders R. Static magnetic fields: animal studies. Prog Biophys Mol Biol. 2005;87(2):225–239. doi:10.1016/j.pbiomolbio.2004.09.001
24. Brent RL. Protection of the gametes embryo/fetus from prenatal radiation exposure. Health Physics. 2015;108(2):242–274. doi:10.1097/HP.0000000000000235
25. Yoon I, Slesinger TL. Radiation exposure in pregnancy. In: StatPearls. Disclosure: Todd Slesinger Declares No Relevant Financial Relationships with Ineligible Companies. Treasure Island (FL): Ineligible Companies; StatPearls Publishing Copyright © 2023;2023
26. Amitai MM, Katorza E, Guranda L, et al. Role of emergency magnetic resonance imaging for the workup of suspected appendicitis in pregnant women. Isr Med Assoc J. 2016;18(10):600–604.
27. Baruch Y, Canetti M, Blecher Y, Yogev Y, Grisaru D, Michaan N. The diagnostic accuracy of ultrasound in the diagnosis of acute appendicitis in pregnancy. J Matern Fetal Neonatal Med. 2020;33(23):3929–3934. doi:10.1080/14767058.2019.1592154
28. Biondi A, Di Stefano C, Ferrara F, Bellia A, Vacante M, Piazza L. Laparoscopic versus open appendectomy: a retrospective cohort study assessing outcomes and cost-effectiveness. World J Emerg Surg. 2016;11(1):44. doi:10.1186/s13017-016-0102-5
29. Nazir A, Farooqi SA, Chaudhary NA, Bhatti HW, Waqar M, Sadiq A. Comparison of open appendectomy and laparoscopic appendectomy in perforated appendicitis. Cureus. 2019;11(7):e5105. doi:10.7759/cureus.5105
30. Cox TC, Huntington CR, Blair LJ, et al. Laparoscopic appendectomy and cholecystectomy versus open: a study in 1999 pregnant patients. Surg Endosc. 2016;30(2):593–602. doi:10.1007/s00464-015-4244-4
31. Korndorffer JR, Fellinger E, Reed W. SAGES guideline for laparoscopic appendectomy. Surg Endosc. 2010;24(4):757–761. doi:10.1007/s00464-009-0632-y
32. Machado NO, Grant CS. Laparoscopic appendicectomy in all trimesters of pregnancy. JSLS. 2009;13(3):384–390.
33. Agha R, Muir G. Does laparoscopic surgery spell the end of the open surgeon? J R Soc Med. 2003;96(11):544–546. doi:10.1177/014107680309601107
34. Velanovich V. Laparoscopic vs open surgery: a preliminary comparison of quality-of-life outcomes. Surg Endosc. 2000;14(1):16–21. doi:10.1007/s004649900003
35. Yumi H. Prepared by the guidelines committee of the society of American G, Endoscopic S. Guidelines for diagnosis, treatment, and use of laparoscopy for surgical problems during pregnancy. Surg Endosc. 2008;22(4):849–861. doi:10.1007/s00464-008-9758-6
36. McKellar DP, Anderson CT, Boynton CJ, Peoples JB. Cholecystectomy during pregnancy without fetal loss. Surg Gynecol Obstet. 1992;174(6):465–468.
37. Aggenbach L, Zeeman GG, Cantineau AEP, Gordijn SJ, Hofker HS. Impact of appendicitis during pregnancy: no delay in accurate diagnosis and treatment. Int J Surg. 2015;15:84–89. doi:10.1016/j.ijsu.2015.01.025
38. Adamina M, Andreou A, Arezzo A, et al. EAES rapid guideline: systematic review, meta-analysis, GRADE assessment, and evidence-informed European recommendations on appendicitis in pregnancy. Surg Endosc. 2022;36(12):8699–8712. doi:10.1007/s00464-022-09625-9
39. Soma-Pillay P, Nelson-Piercy C, Tolppanen H, Mebazaa A. Physiological changes in pregnancy. Cardiovasc J Afr. 2016;27(2):89–94. doi:10.5830/CVJA-2016-021
40. Krywko DM, King KC. Aortocaval Compression Syndrome. In: StatPearls. Disclosure: Kevin King Declares No Relevant Financial Relationships with Ineligible Companies. Treasure Island (FL): Ineligible Companies; StatPearls Publishing Copyright © 2023; 2023.
41. Nguyen A, Lotfollahzadeh S. Appendectomy. In: StatPearlsDisclosure: Saran Lotfollahzadeh Declares No Relevant Financial Relationships with Ineligible Companies. Treasure Island (FL): Ineligible Companies; StatPearls Publishing Copyright © 2023;2023
42. Fundal Height. Cleveland Clinic; 2022; Available from: https://my.clevelandclinic.org/health/diagnostics/22294-fundal-height.
43. Donkervoort S, Boerma D. Suspicion of acute appendicitis in the third trimester of pregnancy: pros and cons of a laparoscopic procedure. JSLS. 2011;15(3):379–383. doi:10.4293/108680811X13125733356837
44. Rollins MD, Chan KJ, Price RR. Laparoscopy for appendicitis and cholelithiasis during pregnancy: a new standard of care. Surg Endosc Interventional Techniques. 2004;18(2):237–241. doi:10.1007/s00464-003-8811-8
45. Friedman JD, Ramsey PS, Ramin KD, Berry C. Pneumoamnion and pregnancy loss after second-trimester laparoscopic surgery. Obstetrics Gynecol. 2002;99(3):512–513.
46. Gilroy RJ, Mangura BT, Lavietes MH. Rib cage and abdominal volume displacements during breathing in pregnancy. Am Rev Respir Dis. 1988;137(3):668–672. doi:10.1164/ajrccm/137.3.668
47. LoMauro A, Aliverti A. Respiratory physiology of pregnancy: physiology masterclass. Breathe. 2015;11(4):297–301. doi:10.1183/20734735.008615
48. Weinberger SE, Weiss ST, Cohen WR, Weiss JW, Johnson TS. Pregnancy and the lung. Am Rev Respir Dis. 1980;121(3):559–581. doi:10.1164/arrd.1980.121.3.559
49. Grott K, Chauhan S, Dunlap JD. Atelectasis. In: StatPearls. Disclosure: Shaylika Chauhan Declares No Relevant Financial Relationships with Ineligible Companies. Disclosure: Julie Dunlap Declares No Relevant Financial Relationships with Ineligible Companies. Treasure Island (FL): Ineligible Companies; StatPearls Publishing Copyright © 2023; 2023.
50. Melnick DM, Wahl WL, Dalton VK. Management of general surgical problems in the pregnant patient. Am J Surg. 2004;187(2):170–180. doi:10.1016/j.amjsurg.2003.11.023
51. NIH Consensus Development. Prevention of venous thrombosis and pulmonary embolism. . JAMA. 1986;256(6):744–749. doi:10.1001/jama.1986.03380060070028
52. Toglia MR, Weg JG. Venous thromboembolism during pregnancy. New Eng J Med. 1996;335(2):108–114. doi:10.1056/NEJM199607113350207
53. Casele HL. The use of unfractionated heparin and low molecular weight heparins in pregnancy. Clin Obstet Gynecol. 2006;49(4):895–905. doi:10.1097/01.grf.0000211958.45874.63
54. Austin CS, Jaronczyk M. Safe laparoscopic appendectomy in pregnant patient during active labor. J Surg Case Rep. 2021;2021(5):rjab127. doi:10.1093/jscr/rjab127
55. Gutierrez M, Stuparich M, Behbehani S, Nahas S. Does closure of fascia, type, and location of trocar influence occurrence of port site hernias? A literature review. Surg Endosc. 2020;34(12):5250–5258. doi:10.1007/s00464-020-07826-8
56. Danawar NA, Mekaiel A, Raut S, Reddy I, Malik BH. How to treat hernias in pregnant women? Cureus. 2020;12(7):e8959. doi:10.7759/cureus.8959
57. Flum DR, Davidson GH, Monsell SE, et al. A randomized trial comparing antibiotics with appendectomy for appendicitis. N Engl J Med. 2020;383(20):1907–1919.
58. Salminen P, Tuominen R, Paajanen H, et al. Five-year follow-up of antibiotic therapy for uncomplicated acute appendicitis in the APPAC randomized clinical trial. JAMA. 2018;320(12):1259–1265. doi:10.1001/jama.2018.13201
59. Varadhan KK, Neal KR, Lobo DN. Safety and efficacy of antibiotics compared with appendicectomy for treatment of uncomplicated acute appendicitis: meta-analysis of randomised controlled trials. BMJ. 2012;344(apr05 1):e2156. doi:10.1136/bmj.e2156
60. Carstens AK, Fensby L, Penninga L. Nonoperative treatment of appendicitis during pregnancy in a remote area. AJP Rep. 2018;8(1):e37–e38. doi:10.1055/s-0037-1620279
61. Liu J, Ahmad M, Wu J, et al. Antibiotic is a safe and feasible option for uncomplicated appendicitis in pregnancy - A retrospective cohort study. Asian J Endosc Surg. 2021;14(2):207–212. doi:10.1111/ases.12851
62. Joo JIMD, H-CMDP P, Kim MJMD, BHMDP L. Outcomes of antibiotic therapy for uncomplicated appendicitis in pregnancy. Amer J Med. 2017;130(12):1467–1469. doi:10.1016/j.amjmed.2017.04.046
63. Jeon HG, Ju HU, Kim GY, Jeong J, Kim M-H, Jun J-B. Bacteriology and changes in antibiotic susceptibility in adults with community-acquired perforated appendicitis. PLoS One. 2014;9(10):e111144. doi:10.1371/journal.pone.0111144
64. Chen CY, Chen YC, Pu HN, Tsai CH, Chen WT, Lin CH. Bacteriology of acute appendicitis and its implication for the use of prophylactic antibiotics. Surg Infect. 2012;13(6):383–390. doi:10.1089/sur.2011.135
65. Bookstaver PB, Bland CM, Griffin B, Stover KR, Eiland LS, McLaughlin M. A review of antibiotic use in pregnancy. Pharmacothe J Human Pharmacol Drug Therapy. 2015;35(11):1052–1062. doi:10.1002/phar.1649
66. Mantoglu B, Altintoprak F, Firat N, et al. Reasons for undesirable pregnancy outcomes among women with appendicitis: the experience of a tertiary center. Emerg Med Int. 2020;2020:6039862. doi:10.1155/2020/6039862
67. Yoo KC, Park JH, Pak KH, et al. Could laparoscopic appendectomy in pregnant women affect obstetric outcomes? A multicenter study. Int J Colorectal Dis. 2016;31(8):1475–1481. doi:10.1007/s00384-016-2584-8
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.