")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 17
Anhedonia in Acne Vulgaris: A Cross-Sectional Study of 104 Consecutive Acne Patients
Authors Szepietowska M, Stefaniak AA, Krajewski PK , Matusiak Ł
Received 11 December 2023
Accepted for publication 25 January 2024
Published 7 February 2024 Volume 2024:17 Pages 349—357
DOI https://doi.org/10.2147/CCID.S451927
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Jeffrey Weinberg
Marta Szepietowska, Aleksandra A Stefaniak, Piotr K Krajewski, Łukasz Matusiak
Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, Wroclaw, Poland
Correspondence: Piotr K Krajewski, Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, Chalubinskiego 1, Wroclaw, 50-368, Poland, Email [email protected]
Background: Anhedonia is defined as a reduced ability to experience or even a total loss of pleasure.
Purpose: This study was undertaken to evaluate anhedonia in 104 consecutive acne patients.
Material and Methods: Acne severity was assessed with Investigator Global Assessment (IGA), anhedonia was studied with the Snaith-Hamilton Pleasure Scale (SHAPS), Anticipatory and Consummatory Interpersonal Pleasure Scale (ACIPS) and Temporal Experience of Pleasure Scale (TEPS). Moreover, the quality of life (QoL) and stigmatization, as well as depression and anxiety (Hospital Anxiety and Depression Scale – HADS), were additionally evaluated.
Results: Anhedonia was found in 20.19% of acne patients and was more common (p=0.007) in males (34.29%) than in females (13.04%). Based on SHAPS, males with acne showed significantly (p=0.049) higher levels of anhedonia (2.39 ± 3.18 points) than acne females (1.26 ± 2.36 points). Anhedonia significantly correlated with the clinical acne severity (SHAPS: r=0.205, p=0.038 and ACIPS: r=− 0.222, p=0.026). Although the intensity of anhedonia did not show any relationship with QoL and stigmatization assessments, there was a significant correlation between anhedonia and depressive symptoms (SHAPS: r=0.310, p< 0.001; ACIPS: r=− 0.364, p< 0.001). Such dependency was not documented for anxiety.
Conclusion: Anhedonia seems to be a common phenomenon in acne and should be considered in the holistic approach to acne patients.
Keywords: acne, anhedonia, depression, psychodermatology
Introduction
Acne vulgaris is a chronic, inflammatory disease of the pilosebaceous unit. It is considered the most frequent dermatosis and affects mainly both adolescents and young adults, however, older subjects may also suffer from acne.1,2 Epidemiological studies indicate that acne occurs in about 80% of adolescents and 40% of adults worldwide.3,4 Located predominantly on the face, it becomes visible to others. Acne is not a life-threatening disease, but it definitely should not be considered a cosmetic problem due to the vast psychosocial burden.5,6 Recently, our group has shown that acne patients, even those with mild acne, had decreased quality of life (QoL) and increased levels of stigmatization.7,8 We also documented that in subjects with facial acne alexithymia, which is defined as the ability to identify and verbalize emotions, correlated both with QoL impairment and stigmatization level.9 Moreover, based on the multicenter study performed in 13 European countries, acne appeared to be the condition of increased risk for depression, anxiety, and suicidality.5
In general, anhedonia is regarded as reduced motivation and/or ability to experience pleasure or diminished interest in engaging in pleasurable activities. Anhedonia refers to reduced anticipatory and consummatory pleasure as well as to deficits in reinforcement learning10 (10). Anhedonia may be a component of depressive disorders, psychotic disorders, and substance-related conditions, but it can also occur exclusively as a separate condition.10,11 As acne is a disease with severe psychosocial consequences,5 one cannot exclude that acne lesions may influence anhedonia in this group of patients. To the best of our knowledge, anhedonia has not been studied acne suffers yet.
Therefore, the current study was conducted to assess anhedonia in consecutive patients with acne vulgaris and to assess its relationship with clinical severity of acne, QoL, stigmatization and secondary psychiatric disturbances, like depression and anxiety.
Materials and Methods
Study Population
The study group consisted of 104 consecutive patients seeking dermatologic help due to acne. There were 69 (66.3%) females and 35 (33.7%) males. Their age ranged from 12 to 39 years, with a mean value of 20.38 ± 5.78 years. The mean duration of acne was 5.97 ± 4.73 years. Acne duration was significantly longer (p=0.048) in females than in males (6.71 ± 5.06 years and 4.47 ± 3.61 years, respectively). 72 (69.2%) patients reported a family history of acne. No one female patient presented with the signs of polycystic ovary syndrome. Demographic data of studied patients is given in Table 1. The study was run between February and May 2023 according to all the rules of the Declaration of Helsinki and was approved by the local Ethical Committee of Wroclaw Medical University (KB-250/2023). Moreover, each patient has signed an informed consent before entering the study.
 |
Table 1 Demographic Data of Acne Patients |
Measures
Assessment of Acne Clinical Severity
Investigator Global Assessment (IGA) was used to evaluate the clinical severity of acne. This instrument allows to grade acne severity from clear skin (0 points) to severe acne (4 points).12
Assessment of Anhedonia
Three different instruments, in the Polish language validated versions, were employed to study anhedonia: the Snaith-Hamilton Pleasure Scale (SHAPS)13 Anticipatory and Consummatory Interpersonal Pleasure Scale (ACIPS),14 and the Temporal Experience of Pleasure Scale (TEPS).15
SHAPS measures hedonic capacity/hedonic tone. It mainly focuses on getting satisfaction from experiencing pleasurable activities (consumptive pleasure). The tool consists of 14 items assessed by respondents on a 4-point scale (definitely agree, agree, disagree, and strongly disagree), where both disagree answers score 0 points and both agree answers 1 point. Therefore, the total score of the instrument ranges from 0 to 14 points. The higher the score, the higher the hedonic capacity/hedonic tone. Patients scoring above 2 points are considered as anhedonic ones.13
ACIPS was designed to measure the ability to experience interpersonal and social pleasure.14 It contains 17 items on establishing social interactions and maintaining relationships. 7 statements refer to anticipatory anhedonia, and 10 items to consumptive anhedonia. The tool has three domains: intimate social interactions (ACPIS-ISI), group social interactions (ACIPS-GSI), and social bonding and making connections (ACIPS-SBMC). A 6-point Likert scale (1 point – very false for me and 6 points – very true for me) is employed to score the statements. It ranges from 17 to 102 points; lower scores indicate a higher level of anhedonia.14
TEPS is a tool of 18 items, and its advantage is having two subscales capturing both anticipatory and consummatory pleasure.15 10 items refer to anticipatory, and the remaining 8 ones to consummatory anhedonia. Similarly to ACIPS, the answers are based on a 6-point Likert scale (1 point – very false and 6 points – very true). The final score for the whole TEPS ranges between 18 and 108 points, while for anticipatory anhedonia, from 10 to 60 points, and for consummatory anhedonia, from 8 to 48 points. The lower scoring represents a lower level of pleasure experience.15
Assessment of Quality of Life and Stigmatization
QoL impairment was studied with a dermatology-specific questionnaire – the Dermatology Life Quality Index (DLQI),16 and a disease-specific instrument – the Cardiff Acne Disability Index (CADI).17 DLQI is the oldest questionnaire, developed in the early nineties of the last century, specifically designed to measure QoL in skin conditions. The recall period of DLQI is one week. It consists of 10 items, each scored 0 points (not at all) to 3 points (very much). The final score ranges from 0 to 33 points; more points indicate a more impaired QoL.16 CADI contains 5 specific questions and has a recall period of one month. Similarly to DLQI, each answer is scored 0 to 3 points. The higher the sum of the points, the more decreased QoL is.17 The stigmatization assessment was based on the 6-Item Stigmatization Scale (6-ISS), which is an instrument containing 6 questions. Answering each question, one may receive from 0 points (not at all) to 3 points (always). The final score, which is a sum of all obtained points, ranges from 0 to 18 points. Greater perception of stigmatization is considered in patients with higher scoring.18
Assessment of Depression and Anxiety
Classical Hospital Depression and Anxiety Scale (HADS) was employed to measure the psychiatric disturbances, namely depression and anxiety. HADS is a self-assessment tool containing 7 questions related to depression and 7 questions related to anxiety. Scoring each item from 0 to 3 points, the final score ranges from 0 to 21 points for both depression and anxiety.19
Statistical Analysis
Statistical analysis was conducted with IBM SPSS Statistics v. 26 (SPSS INC., Chicago, IL, USA) software. All the data were assessed for parametric and non-parametric distribution using the Shapiro–Wilk normality test. The minimum, maximum, mean, standard deviations, and ranges were given. The Student’s T-test or Mann–Whitney U-test for parametric and non-parametric data were employed for quantitative data. Depending on normality, Spearman’s and Pearson’s correlations were used for the correlation assessments. Qualitative data were analyzed using the Chi2 test. P-values less than 0.05 were considered statistically significant.
Results
The mean acne severity in the whole study group, assessed with IGA, was 3.22 ± 0.7 points. Male patients suffered from significantly (p=0.012) more severe acne than females (3.46 ± 0.61 points and 3.10 ± 0.71 points, respectively). Very severe acne was diagnosed in 10 (9.6%) patients, severe acne in 28 (26.9%) patients, and moderate acne in 49 (47.1%) subjects. The remaining 17 (16.4%) patients suffered from mild acne (Table 1).
Anhedonia, based on the SHAPS assessment, was found in 21 out of 104 acne patients (20.19%). It was diagnosed significantly more commonly (p=0.007) in males – 12 (34.29%) than in females – 9 (13.04%) with acne. All tools used to evaluate the severity of anhedonia, including their subscales and domains, significantly correlated with each other (Table 2). According to SHAPS, the severity of anhedonia was assessed as 1.63 ± 2.69 points in the whole acne group, being significantly more severe (p=0.049) in males in comparison to females (2.39 ± 3.18 points and 1.26 ± 2.36 points, respectively). Such difference was not disclosed using other scales evaluating total anhedonia, like ACIPS and TEPS. Moreover, there was no difference in the severity of anticipatory and consummatory anhedonia (measured both by ACIPS and TEPS) between females and males. The only difference in the domains of anhedonia between the sexes was the one concerning intimate social interactions (ACPIS-ISI). ACIPS-ISI score was significantly lower (p=0.048) in males than in females (4.42 ± 0.84 points and 4.75 ± 0.8 points, respectively) (Table 3).
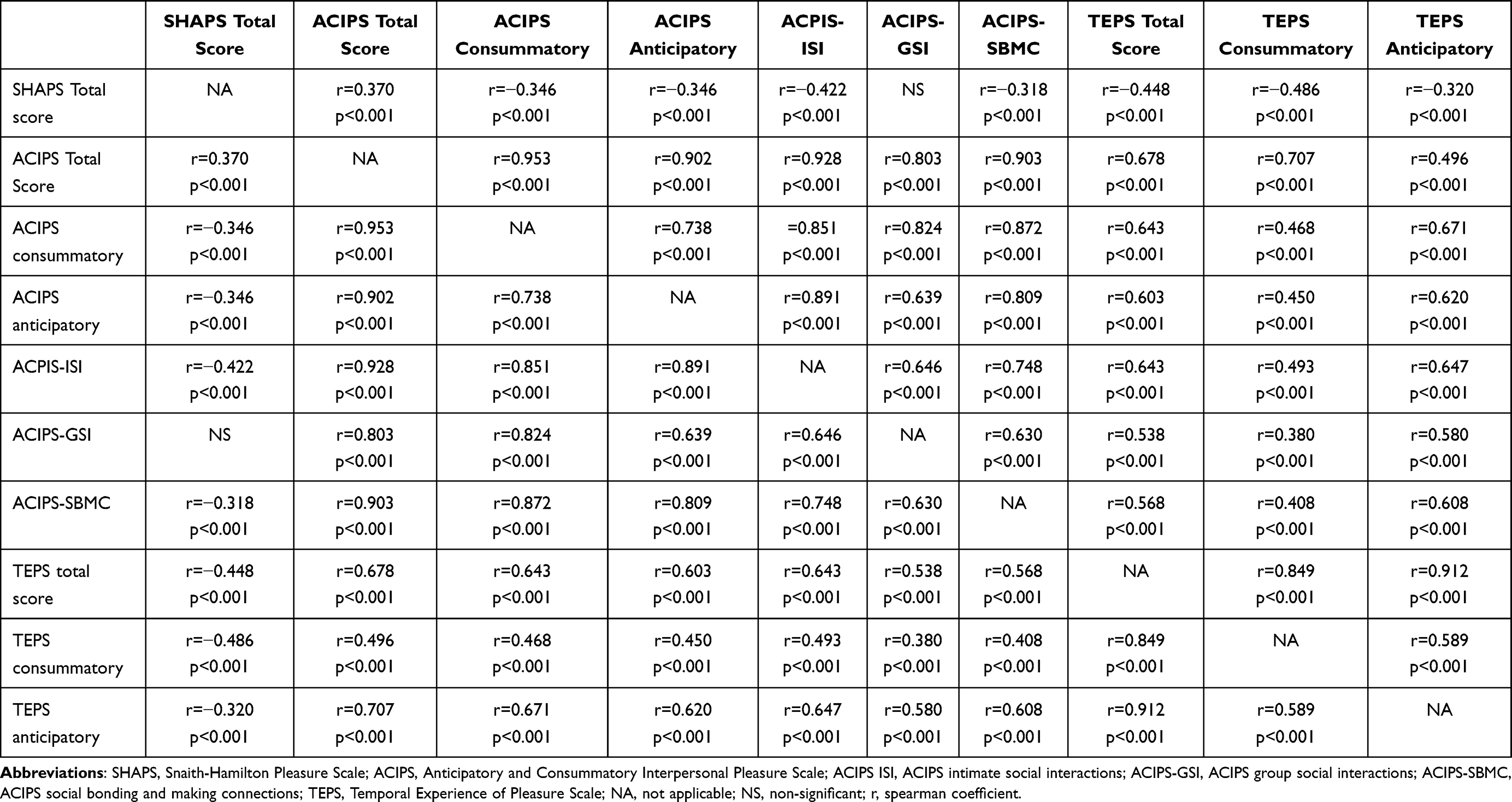 |
Table 2 Correlations Between Different Assessments of Severity of Anhedonia |
 |
Table 3 Differences in Anhedonia Severity Between Sexes |
Anhedonia correlated with the clinical severity of acne. This was documented with SHAPS (r=0.205, p=0.038) and ACIPS (r=−0.222, p=0.026), but not with TEPS. The more severe the acne was, the more expressed anhedonia was. Also, the intensity of consummatory anhedonia assessed with ACIPS and intimate social interactions – ACIPS-ISI correlated negatively with acne severity (r=−0.243, p=0.015 and r=−0.215 p=0.032). No other relationships between domains of anhedonia and severity of the disease were found (Table 4). Moreover, more enhanced anhedonia was found in patients with shorter duration of acne, which was documented for both SHAPS total score (r=−0.216 p=0.032) and TEPS consummatory anhedonia (r=0.230 p=0.021).
 |
Table 4 Correlations of Different Assessments of Anhedonia with Clinical Severity of Acne |
We were not able to find any relationships between anhedonia scales with their subscales and domains and QoL assessment with both DLQI and CADI. No correlations were also shown between anhedonia scores and the level of stigmatization (detailed data not shown). However, anhedonia significantly correlated with the intensity of depression, assessed with HADS-D (SHAPS: r=0.310, p<0.001; ACIPS: r=−0.364, p<0.001; ACIPS anticipatory: r=−0.396, p<0.001; ACIPS consummatory: r=−0.300, p=0.002; ACIPS-ISI: r=−0.347, p<0.001; ACIPS-GSI: r=−0.263, p=0.008; ACIPS-SBMC: r=−0.347, p<0.001). Only TEPS total score with TEPS anticipatory and TEPS consummatory scores did not show correlations with HADS-D (detailed data not shown). Moreover, anhedonia did not depend on the anxiety level. No relationships were found between HADS-A scores, and all used scales assessing anhedonia (detailed data not shown).
Discussion
The term anhedonia was introduced by French psychologist Théodule-Armand Ribot in 1896 year.20 It originates from the Greek language, where “an” means without and “hedeone” means pleasure.21 Originally, anhedonia was referred to as the total loss of pleasure, both physical and psychic. Currently, according to the fifth edition of The Diagnostic and Statistical Manual of Mental Disorders (DSM-V), anhedonia is defined as a lack of enjoyment from, engagement in, or energy for life’s experiences as well as deficits in the capacity to feel pleasure and take interest in things.10
Anhedonia is a common symptom of major depressive disorder.10,21,22 Having a personal history of depression, bipolar disorder, alcoholism, and other mental disorders is considered a risk factor for anhedonia. Anhedonia has also been treated as a trait or a state.10 It has extensively been studied in numerous psychiatric and neurologic disorders, including depression, schizophrenia, post-traumatic stress disorder, and Parkinson’s disease.22 It has been suggested that severe and/or chronic illness, like cancer, chronic pain, or heart disease, may influence the appearance of anhedonia.21,23–27 Anhedonia was also demonstrated to be more common in females with polycystic ovary syndrome (PCOS)28 PCOS Polish patients showed pronounced features of type D personality (higher scores for distress, anxiety and depression).29 As PCOS is associated with acne30 it was of importance that all our female patients did not present with any signs of polycystic ovary syndrome.
The pathogenesis of anhedonia is complex and not completely clear.10 Some authors suggested structural abnormalities, like reduced activity of the ventral striatum. This region of the brain is called the “pleasure center”, and it has been suggested it is involved in the reward system. Increased activity of the prefrontal cortex has also been reported. This part of the cortex is involved in planning and personality expression, which are of importance in anhedonia.
Moreover, changes in processing emotions and disturbed self-awareness observed in anhedonic individuals may be related to structural abnormalities within the amygdala and insula, respectively. One can also underline the role of disturbed homeostasis of neurotransmitters. Reduced expression of dopamine, a mediator playing a role in the reward pathway, as well as lowered levels of gamma-aminobutyric acid (GABA), were found in subjects suffering from anhedonia. Moreover, disturbances in serotonin and glutamate may contribute to the development and flare of anhedonia.10 It is also important to notice that an inflammatory process with an increased level of C-reactive protein (CRP) is present in depression, as well as in anhedonia.10,31
The prevalence of anhedonia in the general population is suggested to be between 5% and 11%.13,32 The literature concerning the prevalence of anhedonia in particular conditions is rather limited and mainly related to psychiatric and neurological disorders. Anhedonia occurs in up to 70% of patients with major depressive disorder,21,33 52% of those with bipolar disorder,21,34 up to 55% of patients with substance use disorders,22 in around 23% of those suffering from schizophrenia,22 up to 46% of subjects with Parkinson’s disease22,35 and up to 45.8% of patients with different types of epilepsy.36 Epidemiological data on anhedonia outside the psychiatry and neurology fields are almost nonexistent. We were only able to find data on the incidence of anhedonia in patients with chronic pain.22,27 In this group of subjects mean prevalence of anhedonia was calculated as 23% and ranged between 14% and 34%.22 A recent study by our group showed that 13.1% of patients suffering from chronic itch may be classified as anhedonic ones (Stefaniak et al, unpublished data). In the current project, it appeared that anhedonia was found in 20.19% of acne subjects, which is at least twice more higher incidence reported in the general population and similar to patients with schizophrenia and chronic pain. To the best of our knowledge, these are the first results of anhedonia communicated in dermatologic patients. It is well-known that acne causes severe psychological stress to patients.37,38 It is a disease with visible skin lesions located predominantly on the face.1 Moreover, it is a disorder mainly of adolescents and young adults, where first interpersonal relations are being established, when young people are seeking their first jobs. As anhedonia is related to stressful situations,10,21 one can hypothesize that acne stress may contribute to the increased prevalence of anhedonia in these subjects.
Concerning the severity of anhedonia, the SHAPS reference value for healthy people was established as 0.6 points. In our acne subjects mean SHAPS score was 1.63 ± 2.69 points. In the study of Trostheim et al,22 the following reference values of SHAPS were proposed for particular conditions: 5.8 points for major depressive disorder, 2.7 points for schizophrenia, 1.7 points for substance use disorders, 1.5 points for Parkinson’s disease, and 1.6 points for chronic pain patients. It seems that the severity of anhedonia in acne sufferers is on a similar level as in patients with substance use disorders, Parkinson’s disease, and those reporting chronic pain. In Chinese university studies, anhedonia was more severe in males than in females,39 which is in agreement with our results in acne patients. Our male patients scored higher on SHAPS than females, indicating that males with acne suffer from more severe anhedonia than acne females.
We also documented a positive correlation between anhedonia and clinical severity of acne. This is not surprising as, similarly, Witton and Pizzagalli21 reported that anhedonia is associated with a more severe and recurrent illness course of mood disorders. In patients with major depressive disorders, an increased level of anhedonia was found to be correlated with a greater number of prior depressive episodes, longer depressive episode durations, and greater overall illness severity. Similar findings were reported in bipolar disease.21 Interestingly, in our cohort of acne patients, SHAPS scores correlated negatively with acne duration, suggesting that those with a shorter course of acne may have a higher level of anhedonia. Although this was only observed with a few used scales assessing anhedonia – SHAPS and TEPS consummatory, the observed difference between acne and major depressive disorders may be due to the completely different character of the illness. First, acne lesions usually heavily influence patients’ well-being, and patients with longer acne duration may cope better with their skin disease.40
In our acne group, anhedonia correlated with the severity of depression assessed with HADS-D. One can predict such a situation as anhedonia is regarded as a hallmark feature of depression.21 Similarly to our acne patients, Roberts-West et al36 reported a correlation between anhedonia and the severity of depression in patients with epilepsy. Moreover, the reduction of depressive mood stimulated the recovery of pleasure. However, in contrast to our results, they found that anhedonia in epilepsy patients was additionally associated with the endorsement of anxiety symptoms on the HADS.36 Assessing QoL and stigmatization, we were not able to find any correlations with anhedonia. It is worth mentioning that in our cohort of acne patients, depression symptoms showed a positive correlation with QoL impairment assessed by both DLQI (r=0.423 p<0.001) and CADI (r=0.409 p<0.001). This confirms previous thought that anhedonia may be subjectively and biologically distinct from depressed mood.41 Barthel et al,42 based on patients with generalized anxiety disorder, suggested that anhedonia is a crucial element for the association between quality of life, sleep problems, and negative cognitions. The relationship between anhedonia and QoL in dermatology patients, including acne subjects, requires further studies.
We are aware of our study limitations. This was a single-center study with a limited number of involved acne patients (104 patients). The obtained results we compared to the standard/reference prevalence of anhedonia in the general population. An international, multicenter study with the involvement of healthy individuals from different geographical regions as a control group will be of help in confirming our results. We also do believe that assessment of psychological stress and sexual dysfunction in relation to anhedonia in patients suffering from acne may be beneficial in better understanding of anhedonia process in this group of subjects and should be addressed in future projects.
In conclusion, to the best of our knowledge, for the first time, anhedonia was assessed in patients with acne. Anhedonia was found in one-fifth of acne sufferers and correlated with both the clinical severity of acne and the severity of depressive symptoms. Based on current results, we suggest that anhedonia should be incorporated in the evaluation of psychological status of acne patients and should be considered in the holistic management of this group of patients.
Data Sharing Statement
Data available on request.
Ethics and Consent Statements
The study was approved by the local Ethical Committee of Wroclaw Medical University (KB-250/2023). Each patient has signed an informed consent before entering the study.
Funding
Ministry of Science and Education Grant “The best of the best! 4.0” Number: MEiN/2022/DIR/3184.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wolkenstein P, Machovcova A, Szepietowski JC, Tennstedt D, Veraldi S, Delarue A. Acne prevalence and associations with lifestyle: a cross-sectional online survey of adolescents/young adults in 7 European countries. J Eur Acad Dermatol Venereol. 2018;32(2):298–306. doi:10.1111/jdv.14475
2. Dreno B, Poli F. Epidemiology of acne. Dermatology. 2003;206(1):7–10. doi:10.1159/000067817
3. Dréno B. Recent data on epidemiology of acne. Annales de Dermatologie et de Vénéréologie. 2010;137(2):3–5. doi:10.1016/S0151-9638(10)70045-4
4. Rzany B, Kahl C. [Epidemiology of acne vulgaris]. Epidemiologie der Acne vulgaris. J Dtsch Dermatol Ges. 2006;4(1):8–9. doi:10.1111/j.1610-0387.2005.05876.x German.
5. Altunay IK, Ozkur E, Dalgard FJ, et al. Psychosocial aspects of adult acne: data from 13 European Countries. Acta Derm Venereol. 2020;100(4):adv00051. doi:10.2340/00015555-3409
6. Szepietowska M, Bien B, Krajewski PK, Stefaniak AA, Matusiak L. Prevalence, Intensity and psychosocial burden of acne itch: two different cohorts study. J Clin Med. 2023;12(12). doi:10.3390/jcm12123997
7. Szepietowska M, Dabrowska A, Nowak B, et al. Prevalence and quality of life of facial acne: a cross-sectional study in high school students in Poland. Postepy Dermatol Alergol. 2022;39(6):1035–1039. doi:10.5114/ada.2021.112765
8. Szepietowska M, Dabrowska A, Nowak B, et al. Facial acne causes stigmatization among adolescents: a cross-sectional study. J Cosmet Dermatol. 2022;21(12):6815–6821. doi:10.1111/jocd.15268
9. Szepietowska M, Dabrowska A, Nowak B, et al. Alexithymia in adolescents with acne: association with quality of life impairment and stigmatization. J Clin Med. 2022;11(3). doi:10.3390/jcm11030732
10. Guo L. Anhedonia. What Is It, Causes, Diagnosis, and More. Elsevier. Available from: https://www.osmosis.org/answers/anhedonia.
11. De Fruyt J, Sabbe B, Demyttenaere K. Anhedonia in depressive disorder: a narrative review. Psychopathology. 2020;53(5–6):274–281. doi:10.1159/000508773
12. Alsulaimani H, Kokandi A, Khawandanh S, Hamad R. Severity of acne vulgaris: comparison of two assessment methods. Clin Cosmet Invest Dermatol. 2020;13:711–716. doi:10.2147/CCID.S266320
13. Snaith RP, Hamilton M, Morley S, Humayan A, Hargreaves D, Trigwell P. A scale for the assessment of hedonic tone the Snaith-Hamilton Pleasure Scale. Br J Psychiatry. 1995;167(1):99–103. doi:10.1192/bjp.167.1.99
14. Gooding DC, Pflum MJ. The assessment of interpersonal pleasure: introduction of the Anticipatory and Consummatory Interpersonal Pleasure Scale (ACIPS) and preliminary findings. Psychiatry Res. 2014;215(1):237–243. doi:10.1016/j.psychres.2013.10.012
15. Gard DE, Gard MG, Kring AM, John OP. Anticipatory and consummatory components of the experience of pleasure: a scale development study. J Res Personality. 2006;40(6):1086–1102. doi:10.1016/j.jrp.2005.11.001
16. Finlay AY, Khan GK. Dermatology Life Quality Index (DLQI)--A simple practical measure for routine clinical use. Clin Exp Dermatol. 1994;19(3):210–216. doi:10.1111/j.1365-2230.1994.tb01167.x
17. Abdelrazik YT, Ali FM, Salek MS, Finlay AY. Clinical experience and psychometric properties of the Cardiff Acne Disability Index (CADI). Br J Dermatol. 2021;185(4):711–724. doi:10.1111/bjd.20391
18. Lu Y, Duller P, van der Valk PGM, Evers AWM. Helplessness as predictor of perceived stigmatization in patients with psoriasis and atopic dermatitis. Dermatol Psychosom. 2003;4(3):146–150. doi:10.1159/000073991
19. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
20. Ribot T. La Psychologie Des Sentiments. F. Alcan Paris; 1896.
21. Whitton AE, Pizzagalli DA. Anhedonia in Depression and Bipolar Disorder. In: Pizzagalli DA, editor. Anhedonia: Preclinical, Translational, and Clinical Integration. Springer International Publishing; 2022:111–127.
22. Trostheim M, Eikemo M, Meir R, et al. Assessment of anhedonia in adults with and without mental illness: a systematic review and meta-analysis. JAMA Network Open. 2020;3(8):e2013233. doi:10.1001/jamanetworkopen.2020.13233
23. Sharpley CF, Bitsika V, Christie DH. Do prostate cancer patients suffer more from depressed mood or anhedonia? Psychooncology. 2013;22(8):1718–1723. doi:10.1002/pon.3203
24. Kasyanov ED, Pinakhina DV, Rakitko AS, et al. [Anhedonia in mood disorders and somatic diseases: results of exploratory Mendelian randomization analysis]. Angedoniya pri rasstroistvakh nastroeniya i somaticheskikh zabolevaniyakh: rezul’taty razvedochnogo Mendelevskogo randomizatsionnogo analiza. Zh Nevrol Psikhiatr Im S S Korsakova. 2023;123(4):65–73. doi:10.17116/jnevro202312304265 Russian.
25. Ritsner MS. Anhedonia: a comprehensive handbook. In: Volume II, Neuropsychiatric and Physical Disorders. Springer Dordrecht; 2014.
26. Davidson KW, Burg MM, Kronish IM, et al. Association of anhedonia with recurrent major adverse cardiac events and mortality 1 year after acute coronary syndrome. Arch Gen Psychiatry. 2010;67(5):480–488. doi:10.1001/archgenpsychiatry.2010.36
27. Garland EL, Trostheim M, Eikemo M, Ernst G, Leknes S. Anhedonia in chronic pain and prescription opioid misuse. Psychol Med. 2020;50(12):1977–1988. doi:10.1017/S0033291719002010
28. Koric A, Singh B, VanDerslice JA, et al. Polycystic ovary syndrome and postpartum depression symptoms: a population-based cohort study. Am J Obstet Gynecol. 2021;224(6):591 e1–591 e12. doi:10.1016/j.ajog.2020.12.1215
29. Urban W, Niziol A, Pytlewski A, et al. Polycystic ovary syndrome: personality and temperamental characteristics. J Obstet Gynaecol Can. 2022;44(7):813–818. doi:10.1016/j.jogc.2022.03.011
30. Kutlu O, Karadag AS, Demirseren DD, et al. Epidemiological characteristics of different types of adult acne in Turkey: a prospective, controlled, multicenter study. Acta Dermatovenerol Alp Pannonica Adriat. 2023;32(2):49–55.
31. Bekhbat M, Treadway MT, Felger JC. Inflammation as a pathophysiologic pathway to anhedonia: mechanisms and therapeutic implications. Curr Top Behav Neurosci. 2022;58:397–419. doi:10.1007/7854_2021_294
32. Franken IH, Rassin E, Muris P. The assessment of anhedonia in clinical and non-clinical populations: further validation of the Snaith-Hamilton pleasure scale (SHAPS). J Affect Disord. 2007;99(1–3):83–89. doi:10.1016/j.jad.2006.08.020
33. Cao B, Park C, Subramaniapillai M, et al. The efficacy of vortioxetine on anhedonia in patients with major depressive disorder. Front Psychiatry. 2019;10:17. doi:10.3389/fpsyt.2019.00017
34. Mazza M, Squillacioti MR, Pecora RD, Janiri L, Bria P. Effect of aripiprazole on self-reported anhedonia in bipolar depressed patients. Psychiatry Res. 2009;165(1–2):193–196. doi:10.1016/j.psychres.2008.05.003
35. Loas G, Krystkowiak P, Godefroy O. Anhedonia in Parkinson’s disease: an overview. J Neuropsychiatry Clin Neurosci. 2012;24(4):444–451. doi:10.1176/appi.neuropsych.11110332
36. Roberts-West L, Vivekananda U, Baxendale S. Anhedonia in epilepsy. Epilepsy Behav. 2023;140:108966. doi:10.1016/j.yebeh.2022.108966
37. Aslan Kayiran M, Karadag AS, Jafferany M. Psychodermatology of acne: dermatologist’s guide to inner side of acne and management approach. Dermatol Ther. 2020;33(6):e14150. doi:10.1111/dth.14150
38. Jovic A, Marinovic B, Kostovic K, Ceovic R, Basta-Juzbasic A, Bukvic Mokos Z. The impact of psychological stress on acne. Acta Dermatovenerol Croat. 2017;25(2):1133–1141.
39. Zhou H, Liu W, Fan J, Xia J, Zhu J, Zhu X. The temporal experience of pleasure scale (TEPS): measurement invariance across gender in Chinese university students. Front Psychol. 2019;10:2130. doi:10.3389/fpsyg.2019.02130
40. Stamu-O’Brien C, Jafferany M, Carniciu S, Abdelmaksoud A. Psychodermatology of acne: psychological aspects and effects of acne vulgaris. J Cosmet Dermatol. 2021;20(4):1080–1083. doi:10.1111/jocd.13765
41. Amonoo HL, Fenech A, Greer JA, Temel JS, Huffman JC, El-Jawahri A. Does desire to pursue pleasurable activities matter? The impact of pretransplantation anhedonia on quality of life and fatigue in hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2020;26(8):1477–1481. doi:10.1016/j.bbmt.2020.04.014
42. Barthel AL, Pinaire MA, Curtiss JE, et al. Anhedonia is central for the association between quality of life, metacognition, sleep, and affective symptoms in generalized anxiety disorder: a complex network analysis. J Affect Disord. 2020;277:1013–1021. doi:10.1016/j.jad.2020.08.077
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.