")
Back to Journals » International Medical Case Reports Journal » Volume 17
Anesthesia Management in Massive Occipital Meningoencephalocele with Chiari III Malformation: A Case Report
Authors Cahyadi A , Firdaus R, Angkasa H
Received 26 December 2023
Accepted for publication 4 April 2024
Published 23 April 2024 Volume 2024:17 Pages 387—390
DOI https://doi.org/10.2147/IMCRJ.S453554
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Video abstract of “Anesthesia Management in Massive Occipital Meningoencephalocele” [453554].
Views: 32
Arief Cahyadi,1,2 Riyadh Firdaus,2 Hansen Angkasa2
1Department of Anestesiology, Univesitas Padjajaran, Hasan Sadikin General Hospital, Bandung, Indonesia; 2Department of Anesthesiology and Intensive Care, Faculty of Medicine University of Indonesia, Cipto Mangunkusumo General Hospital, Jakarta, Indonesia
Correspondence: Arief Cahyadi, Hasan Sadikin General Hospital, Pasteur Road, No. 38, Bandung, West Java, 40161, Indonesia, Email [email protected]
Abstract: Arnold–Chiari malformation is a displacement of the brain into the spinal canal, often leading to hemodynamic distress. Arnold-Chiari malformation type III (CM III) is a rare and severe type that requires early detection to prevent complications. We aim to report this rare presentation of CM III. A 16-month-old girl with a massive tumor of the occiput suspected to be a meningoencephalocele with CM III was referred to the neurosurgery department. The patient was assessed with class 3 American Society of Anesthesiologist classification, posed challenges due to a difficult airway and the presence of a meningoencephalocele. The patient was scheduled for an elective surgery. Preoperative, the patient was lethargic with an abnormal heart rate and blood pressure. Induction was performed while preserving spontaneous ventilation, but was assisted by an oropharyngeal airway due to a short neck and obesity. The patient later developed laryngospasm thus, muscle relaxant and propofol were administered. A rescue laryngeal mask airway was inserted due to desaturation. Intubation was performed with video laryngoscope. When the surgeon opened the cele and removed the cerebrospinal fluid, the blood pressure began to decline. Resection of brain tissue caused the patient started to bleed, fluid and blood products were administered. At the end of surgery, the patient had stable hemodynamics and was transferred to the pediatric intensive care for monitoring. In patients with massive occipital meningoencephalocele and CM III, anesthetic management requires smooth intubation and prevention of excessive manipulation of the cervical joint to prevent increased intracranial pressure. The patient was not extubated because the brainstem could not be sufficiently reduced coupled with significant autonomic dysfunction.
Keywords: Chiari malformation, children, management anesthesia, meningoencephalocele
Introduction
Arnold-Chiari malformation type III (CM III) is a rare, severe phenotype with a poor prognosis. Patients with CM III usually present with brain displacement into the spinal canal, which causes hemodynamic distress.1 This case is rare and requires early detection to prevent complications, with neurosurgery being the definitive treatment option. Nonetheless, literature on CM III is scarce, and its prognosis is poor. We report a late case of CM III with a massive occipital meningoencephalocele presented for corrective surgery. Informed consent for publication was obtained from the patient’s mother. Institutional approval was not required.
Case Presentation
A girl, 1 year and 4 months old of Malay ethnic origin, was referred to our neurosurgery department because of a massive tumor of the occiput, suspected to be a meningoencephalocele with CM III measuring 20×22 × 8 cm, with a circumference of 51 cm. The patient was assessed with American Society of Anesthesiology (ASA) physical status classification of class 3 with a difficult airway due to obesity and meningoencephalocele (Figure 1). Magnetic resonance imaging confirms the location and content of the cele (Figure 2). There was no family history of similar disease or other types of malignancy. The patient was scheduled for an elective surgery.
 |
Figure 1 Clinical presentation of the lesion, (A) from front (B) from the side. |
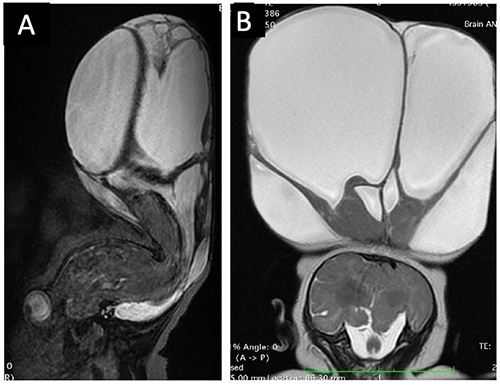 |
Figure 2 MRI Imaging of the lesion. (A) Sagittal view; (B) Coronal view. Hyperdensity showing the fluid cele, with hypodensity of the parenchyme denoting brain tissue. |
On the day of surgery, the patient was lethargic, with vital signs of heart rate (HR) 85 beat per minute (bpm), respiratory rate of 20 times per minute, blood pressure (BP) of 85/51 mmHg, and we decided to proceed with the operation. Induction was performed using Sevoflurane and Fentanyl (2 mcg/kg). The patient maintained spontaneous ventilation; however, assisted ventilation was difficult because of the short neck and obesity; thus, we decided to place an oropharyngeal airway. The patient soon developed laryngospasm and ventilation could not be controlled. The patient’s oxygen saturation plummeted, and the muscle relaxant atracurium (0.5 mg/kg) was administered together with propofol (1 mg/kg). Oxygen saturation decreased to 35%, and a rescue laryngeal mask airway (LMA, Unique size 1.5) was inserted. The laryngospasm resolved, and the patient was intubated using a reinforced non-kinking endotracheal tube (ETT), with internal diameter of 4 mm, at a depth of 11 cm (Portex). A central venous catheter was inserted with ultrasonography on the right femoral vein. The patient was placed in the prone position. Anesthesia was maintained with Sevoflurane 0.8 minimum alveolar concentration (MAC), intermittent Fentanyl and Atracurium boluses. Fluid maintenance was given using Ringer Acetate containing dextrose 1% at 46 mL/hour. Surgery was then initiated.
Intraoperatively, the patient was stable up until the surgeon opened the cele and removed cerebrospinal fluid. blood pressure started to decrease and she became tachycardic. Upon resection of the brain tissue, the patient started to bleed profusely. Fluid and blood products were administered. The patient was suspected to have intraoperative diabetes insipidus due to the position of the cele. Urine production was massive at approximately 15–20 mL/kg/hour. The volume was then replaced with balanced salt solution. Patient was kept normothermic. The surgery lasted for 9 hours, and the remaining brainstem component within the cele was covered with an artificial dura (Redura), skin, and dressing. At the end of the surgery, the patient had stable hemodynamics, with a BP of 86/50 mmHg and an HR of 123–128 bpm.
The patient was placed in a lateral position to replace the ETT from reinforced to an uncuffed ETT size of 4.5. The patient was placed in the lateral position and transferred to the pediatric intensive care unit (PICU) for monitoring. The patient remained stable in the lateral position without seizures or fever, and urine output started to normalized after 24–72 hours. The postoperative hemoglobin level (Hb) was 9.1 without active bleeding. Two months after, the lesion started to swell, and a lumboperitoneal shunt was placed to prevent recurrence.
Discussion
Arnold-Chiari malformation is a congenital abnormality involving the cerebellum, brainstem, and junction, with the cerebellum displaced into the spinal canal. Chiari malformation (CM) is commonly divided into four distinct types (Types I to IV), depending on the severity of brainstem displacement. CM III is rare and usually presents with severe features, including brainstem and autonomic dysfunction, and has a high mortality rate.1 We present a rare case of anesthetic management of CM III presenting with both brainstem and autonomic dysfunction, complicated by a massive occipital meningoencephalocele with obesity and a short neck.
Classically, the management of Arnold-Chiari malformation involves prevention of increased intracranial pressure, which requires smooth intubation and prevention of excessive manipulation of the cervical joint.2 Patients with CM are usually complicated by autonomic and/or brainstem dysfunction, which frequently leads to apnea or arrhythmia. The intraoperative risk of hemodynamic instability and bradycardia is high in patients with CM owing to manipulation of the brainstem.3 In patients with a large occipital meningoencephalocele, positioning for intubation and surgery is an issue.4 Previously Ganeriwal et al5 reported the use girdle cushion platform made of gauze to position the patient’s lesion (12.1 x 11.7 × 8.4 cm) for airway manipulation. However, it was difficult in our case due to the larger size of the anomaly (20 × 22 × 8 cm). Hence, in this patient, we opted the use of a video laryngoscope to prevent excessive neck manipulation and a large meningoencephalocele mechanically preventing extension of the head. The patient also had a short neck and obesity, which posed problems with both ventilation and intubation. Hemodynamic instability was apparent as the patient presented with stable bradycardia prior to induction. In our case, induction was performed slowly with an inhalation agent; however, the patient developed laryngospasm, and we had to perform rescue ventilation with LMA insertion after deepening the anesthesia with propofol and a muscle relaxant.
Drainage of the cerebrospinal fluid also causes activation of the reflex, which causes the heart rate to become more tachycardic as blood pressure decreases.6 This was superimposed with bleeding and probably transient diabetes insipidus (DI) due to the cele manipulation. Fluid resuscitation and blood products were given to maintain blood pressure and heart rate with the target to be as close to physiologically normal level. The transfusion trigger for pediatric neurosurgery is poorly defined,7 and our institution uses Hb 7–8 to as the trigger, especially if the patient experiences hemodynamic instability. The patient was kept normothermic to prevent acidosis. We also kept the patient in 0.8 MAC with adequate analgesia using Fentanyl and immobilization using Atracurium. Dextrose 1% was administered to prevent hypoglycemia owing to the extended duration of surgery.
Compared to Ganeriwal et al5 and Panigraphy et al,4 our case did not end in sufficient reduction of the brain mass to allow bony defect, thus a certain portion of the brainstem was still outside the cranium, thus the need of sufficient sedation and careful positioning (avoid supine position). Hence, we decided not to extubate the patient. As our center requires all non-kinking ETT to be replaced with kinking ETT, we replaced the ETT in the lateral position using a video laryngoscope and pediatric bougie. The patient was kept in lateral position under sedation and placed with shaped cushion and was transferred to the PICU. Two months after, the patient developed fluid accumulation (cele) and was scheduled for a lumboperitoneal shunt, showing the need for a long-term follow-up to prevent recurrence.
We did not, however, perform urine analysis to confirm our suspicion of Diabetes Insipidus (DI), however, urine production started to normalize after 24–72 hours, which was supportive of a transient DI. We were extremely focused with maintaining spontaneous ventilation, that led to insufficient depth of anesthesia, which we thought caused the laryngospasm triggered by oropharyngeal airway insertion. We were unable to give an accurate estimate of the bleeding as both the cele and blood were mixed. Though we had multiple limitations and pitfalls, this case is unique as it is one of the rare cases where late presentation of CM III causes anatomical and physiological disturbances. We highlight our pitfall in inadequate sedation, leading to spasm due to our fear of inability of manage the airway. We hope our experience may contribute to better future management of CM III cases. To our knowledge, this case serves as one of the largest CM III lesions available in the literature.
Conclusion
In patients with massive occipital meningoencephalocele and CM III malformation, anesthetic management involves smooth intubation and prevention of excessive manipulation of the cervical joint using video laryngoscopy, which prevents increased intracranial pressure. The drainage of cerebrospinal fluid activates reflexes that increase the heart rate. Bleeding and transient diabetes insipidus caused by cele manipulation may reduce blood pressure. There is an increased risk of autonomic and brainstem dysfunctions. All of these risks must be considered before performing the operation.
Abbreviations
CM-III, Arnold Chiari malformation type III; ASA, American Society of Anesthesiologist; HR, heart rate; bpm, beat per minute; BP, blood pressure; LMA, laryngeal mask airway; ETT, endotracheal tube; MAC, minimum alveolar concentration; PICU, pediatric intensive care unit; Hb, hemoglobin; DI, Diabetes Insipidus.
Acknowledgments
We thank the neurosurgery team, scrub and nurses, as well as the pediatric ICU team for their amazing dedication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Azahraa HF, Qaisi I, Joudeh N, et al. The newer classifications of the Chiari malformations with clarifications: an anatomical review. Clin Anat. 2018;31(3):314–322. doi:10.1002/ca.23051
2. Soriano SG, McManu ML. Pediatric neuroanesthesia and critical care. In: Cottrell JE, Young WL, editors. Cottrell and Young’s Neuroanesthesia. Philadelphia: Mosby Elsevier; 2010:327–342.
3. Goyal K, Philip FA, Rath GP, et al. Asystole during posterior fossa surgery: report of two cases. Asian J Neurosurg. 2012;7(2):87–89. doi:10.4103/1793-5482.98654
4. Panigrahy S, Samal S, Dash S, Mohapatra S. Airway management of type-III Arnold Chiari malformation: an anaesthetic challenge. Rom J Anaesth Int Care. 2021;28(2):57–60.
5. Ganeriwal V, Dey P, Bawage R, Gore B. Giant meningoencephalocele with Arnold-Chiari type III malformation and anaesthetic challenges: a rare case report. Saudi J Anaesth. 2019;13(2):136–139. doi:10.4103/sja.SJA_616_18
6. Alfery DD, Shapiro HM, Gagnon RL. Cardiac arrest following rapid drainage of cerebrospinal fluid in a patient with hydrocephalus. Anesthesiology. 1980;52(5):443–444. doi:10.1097/00000542-198005000-00016
7. Wittenmeier E, Trober C, Zier U, et al. Red blood cell transfusion in perioperative pediatric anesthesia: a survey of current practice in Germany. Transfusion. 2018;58(7):1597–1605. doi:10.1111/trf.14581
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.