")
Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 15
An Assessment of Medication Errors Among Pediatric Patients in Three Hospitals in Freetown Sierra Leone: Findings and Implications for a Low-Income Country
Authors Abiri OT , Ninka A, Coker J, Thomas F , Smalle IO, Lakoh S , Turay FU, Komeh J, Sesay M , Kanu JS , Mustapha AM, Bell NVT , Conteh TA , Conteh SK, Jalloh AA, Russell JBW , Sesay N, Bawoh M , Samai M, Lahai M
Received 25 November 2023
Accepted for publication 22 March 2024
Published 29 March 2024 Volume 2024:15 Pages 145—158
DOI https://doi.org/10.2147/PHMT.S451453
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Roosy Aulakh
Onome T Abiri,1,2 Alex Ninka,3 Joshua Coker,4 Fawzi Thomas,2,5 Isaac O Smalle,6 Sulaiman Lakoh,4 Foday Umaro Turay,7 James Komeh,2,3 Mohamed Sesay,2,7 Joseph Sam Kanu,8 Ayeshatu M Mustapha,9 Nellie VT Bell,9 Thomas Ansumus Conteh,2,5 Sarah Kadijatu Conteh,10 Alhaji Alusine Jalloh,10 James BW Russell,4 Noah Sesay,3 Mohamed Bawoh,1 Mohamed Samai,1 Michael Lahai7
1Department of Pharmacology and Therapeutics, College of Medicine and Allied Health Sciences, University of Sierra Leone, Freetown, Sierra Leone; 2Department of Pharmacovigilance and Clinical Trials, Pharmacy Board of Sierra Leone, Freetown, Sierra Leone; 3Department of Clinical Pharmacy and Therapeutics, College of Medicine and Allied Health Sciences, University of Sierra Leone, Freetown, Sierra Leone; 4Department of Internal Medicine, College of Medicine and Allied Health Sciences, University of Sierra Leone, Freetown, Sierra Leone; 5Department of Pharmaceutics, College of Medicine and Allied Health Sciences, University of Sierra Leone, Freetown, Sierra Leone; 6Department of Surgery, College of Medicine and Allied Health Sciences, University of Sierra Leone, Freetown, Sierra Leone; 7Department of Pharmaceutical Chemistry, College of Medicine and Allied Health Sciences, University of Sierra Leone, Freetown, Sierra Leone; 8Department of Community Medicine, College of Medicine and Allied Health Sciences, University of Sierra Leone, Freetown, Sierra Leone; 9Department of Pediatrics, Ola During Children Hospital, Freetown, Sierra Leone; 10Department of Pediatrics, King Harman Road Maternity and Children Hospital, Freetown, Sierra Leone
Correspondence: Onome T Abiri, Department of Pharmacology and Therapeutics, College of Medicine and Allied Health Sciences, University of Sierra Leone Freetown, Sierra Leone/Department of Pharmacovigilance and Clinical Trials, Pharmacy Board of Sierra Leone, Freetown, Sierra Leone, Tel +23276370315, Email [email protected]
Background: Pediatric patients are prone to medicine-related problems like medication errors (MEs), which can potentially cause harm. Yet, this has not been studied in this population in Sierra Leone. Therefore, this study investigated the prevalence and nature of MEs, including potential drug-drug interactions (pDDIs), in pediatric patients.
Methods: The study was conducted in three hospitals among pediatric patients in Freetown and consisted of two phases. Phase one was a cross-sectional retrospective review of prescriptions for completeness and accuracy based on the global accuracy score against standard prescription writing guidelines. Phase two was a point prevalence inpatient chart review of MEs categorized into prescription, administration, and dispensing errors and pDDIs. Data was analyzed using frequency, percentages, median, and interquartile range. Kruskal–Wallis H and Mann–Whitney U-tests were used to compare the prescription accuracy between the hospitals, with p< 0.05 considered statistically significant.
Results: Three hundred and sixty-six (366) pediatric prescriptions and 132 inpatient charts were reviewed in phases one and two of the study, respectively. In phase one, while no prescription attained the global accuracy score (GAS) gold standard of 100%, 106 (29.0%) achieved the 80– 100% mark. The patient 63 (17.2%), treatment 228 (62.3%), and prescriber 33 (9.0%) identifiers achieved an overall GAS range of 80– 100%. Although the total GAS was not statistically significant (p=0.065), the date (p=0.041), patient (p=< 0.001), treatment (p=0.022), and prescriber (p=< 0.001) identifiers were statistically significant across the different hospitals. For phase two, the prevalence of MEs was 74 (56.1%), while that of pDDIs was 54 (40.9%). There was a statistically positive correlation between the occurrence of pDDI and number of medicines prescribed (r=0.211, P=0.015).
Conclusion: A Low GAS indicates poor compliance with prescription writing guidelines and high prescription errors. Medication errors were observed at each phase of the medication use cycle, while clinically significant pDDIs were also reported. Thus, there is a need for training on prescription writing guidelines and medication errors.
Keywords: pediatrics, prescription, medication errors, drug-drug interactions, Sierra Leone
Introduction
Medication error (ME) is any preventable event that may lead to inappropriate use of medicines or patient harm while the patient or health professional controls it. Such events may be correlated to professional practice, including prescribing, order communication, product labeling, packaging, dispensing, administration, education, monitoring, and use.1
Pediatric patients are especially vulnerable to medication errors, which have the potential to cause harm at a rate three times greater than that observed in adults.2,3 Prescribing for pediatric patients can be a quagmire due to the small body mass, necessitating specialized formulations that entail dosage calculation based on weight, height, age, and clinical condition. This intricate process significantly amplifies the likelihood of errors.4–6 These errors are preventable incidents that may arise from the improper utilization of medication and have the potential to cause harm to the child.7 Prudent prescribing, dispensing, administration, and monitoring are, therefore, crucial in preventing medication errors.8,9
Medicines laws, such as the Sierra Leone Pharmacy and Drugs Act 2001, and guidelines, such as the WHO prescription guide, are important for good prescription practice. Adhering to prescription regulations and guidelines is crucial for enhancing patient safety, improving treatment results, avoiding medication errors, promoting rational prescribing practices, and complying with legal and regulatory requirements.10,11 Several studies have assessed adherence to prescription writing guidelines among pediatrics and reported incomplete prescriber, medicine, and patient information and illegible handwriting.12–15 Additionally, experienced and inexperienced healthcare professionals can commit medication errors such as prescription, transcription, dispensing, and administration errors.16–19 Clinically significant potential drug-drug interactions (pDDIs) have also been reported in pediatric patients in Turkey, the United States of America, India, and Nigeria hospitals, which may require avoiding combinations, switching to an alternate medicine, or careful patient monitoring.20–23 Drug-drug interactions and adverse drug reactions (ADRs) are consequences of ME.24,25 These may lead to significant health-related implications such as hospitalization, death, and economic loss, which can negatively affect patient confidence in the healthcare delivery system.26,27 Unfortunately, data in Africa is scarce, and these adverse effects are primarily under-reported in low-income countries like Sierra Leone with an embryonic pharmacovigilance system.28,29
Although Coker et al30 have previously conducted a study to determine adherence to prescription writing guidelines among adults in Sierra Leone, no study has specifically assessed the prevalence and nature of MEs, including pDDIs, in pediatric patients. As medication errors can arise from poor quality prescription writing and errors in dispensing and administration, this study provides baseline data on the prevalence and characteristics of medication errors. The data obtained will provide valuable insights for developing and implementing quality improvement initiatives pertaining to prescription writing, prescribing, dispensing, and administration programs in hospitals. Furthermore, the study findings can offer significant insights and evidence-based recommendations to enhance the national pharmacovigilance system, resulting in the safer use of medicines and improved patient outcomes.
Materials and Methods
Study Setting
This study was conducted in the pediatric departments of the Ola During Children’s Hospital (ODCH), Rokupa Government Hospital (RGH), and King Harman Maternity and Children Hospital (KHMCH) located in Freetown, the Capital city of Sierra Leone. Ola During Children’s Hospital (ODCH) is a national referral pediatric hospital located in the capital city of Freetown. The hospital provides both in-patient and outpatient pediatric services to about 600 children per month and has a capacity of 139 beds. It comprises high dependence, intensive care, therapeutic feeding, Special Care Baby, Infectious disease, cancer, and cardiology units. The Rokupa Government and KHMCH are secondary hospitals containing approximately 20 beds per hospital, and they provide comprehensive emergency obstetric and newborn care, inpatient and outpatient pediatric, and maternity services. Each hospital provides pediatric services to about 200 children per month. At the time of this study, all hospitals lacked an electronic health record (EHR) system.
Study Design and Duration
This study had two phases and was conducted from April 2021 to July 2021. Phase one was a descriptive cross-sectional retrospective study of pediatric prescriptions from the respective pharmacy departments from May 1 to May 31, 2021, for completion and accuracy against standard prescription writing guidelines. In phase two, we conducted a point prevalence descriptive inpatient chart review that lasted for one week among pediatric patients to identify MEs that were categorized into prescription, administration, and dispensing errors, including pDDIs.
Study Population
Pediatric prescriptions from the respective pharmacy departments in May 2021 were included in phase one of the study. Phase two included a medical chart review of inpatients <18 years irrespective of their working diagnosis and gender.
Sample Size Determination and Sampling
For phase one of the study, the sample size was determined using Fisher’s formula for single population studies where p=proportion of non-adherence to prescription writing guidelines from a previous study (38%),12 z = confidence level at 95%, and d = degree of precision of 5%. The minimum sample size was 362. Therefore, a second formula, nf=n/(1+n/N), was used to get the final sample size since the prescription population for May 2021 was 3848 (< 10,000) where; nf =final sample size; ni=initial sample size; N=study population. A final sample size of 366 was obtained after adding 10% for methodological inconsistencies. The Ola During Children’s Hospital had ten times more prescriptions for the period under review than the other two hospitals. This implies that ODCH would have received about 300 of the sample. Hence, the final sample size was divided equally among the three hospitals to distribute the prescriptions better.12 Simple random sampling was applied using the Research randomizer software, where prescriptions were allocated unique codes.31 In phase two, all 132 inpatients were included in this study which was dependent on the number of patients admitted to the hospitals during the study.
Data Collection Procedure and Tool
For phase one of the study, the data collection tool was adapted from the Sierra Leone Pharmacy and Drugs Act 2001, the World Health Organization (WHO) guidelines for prescription writing, and a previous study, as shown in Table 1.10–12 Seventeen essential elements were selected for this study and compiled into a single data collection tool, as shown in Table 1. The global accuracy score (GAS) employed in this study is validated and reliable and has been used in two studies in South Africa, although one is unpublished.12,32 Six researchers manually extracted all data by reviewing prescriptions accessed from the pharmacies. The data collection tool for phase two was adapted from the WHO guide on reporting and learning systems for medication errors, American Society of Health System Pharmacists (ASHP) guidelines for preventing medication errors in hospitals, and previous studies.8,9,17,33 The treatment charts were reviewed by five researchers, and the following were extracted and entered into the data collection tool: wrong patient, wrong dose, wrong route, wrong medicine, wrong dosage form, wrong time of administration, contraindication including allergy, wrong duration, dose omitted or delay, wrong frequency, wrong indication, unnecessary medicine therapeutic duplication, number of medicines prescribed and potential drug-drug interactions. Data collection tools were piloted, and feedback was used to develop the final versions used in the study. In addition, nurses were accompanied during the medicine administration rounds, and patients were monitored and observed.
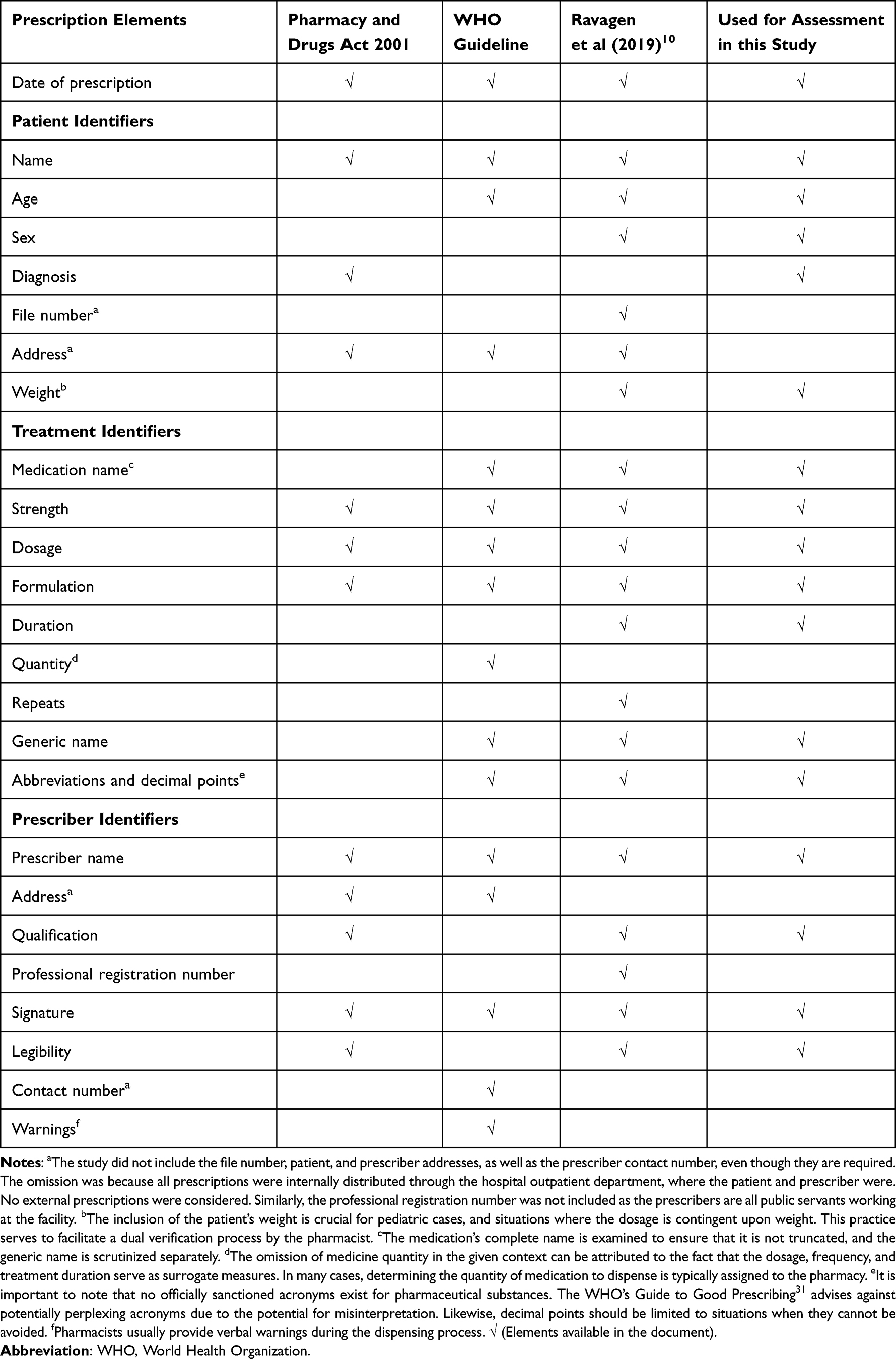 |
Table 1 Comparative Summary of Essential Elements of a Prescription, as per International and Local Standards |
Ethical Consideration
Clearance to conduct the study was obtained from the Research, Innovation, and Publication Review Committee of the Faculty of Pharmaceutical Sciences, College of Medicine and Allied Health Sciences, University of Sierra Leone (RIPC-008-21). The management of the hospitals permitted the study to be done in their facilities. Informed consent was obtained from parents/caregivers after explaining the study’s purpose and procedures. Parents gave consent before data was collected and were not coerced to participate in the study. Patient information was coded and kept confidential.
Data Analyses
The researchers evaluated the completion of the essential elements for each prescription, such as the use of generic names, recommended abbreviations, and prescription legibility. We determined the accuracy score out of 34 total points. Each element was assessed, scoring 0, 1, or 2 for “not completed”, “partially completed”, or “fully completed”. Legibility was scored subjectively according to the prescription quality index (PQI) as 0, 1, or 2 for “illegible”, “barely legible”, or “legible”, respectively, by two or more persons.34 The global accuracy score (GAS) for each prescription was determined by calculating the percentage achieved out of 34 possible points for the 17 prescription elements considered and broadly categorized as date, patient, treatment, and prescriber identifiers. The GAS was then classified into one of four scores: 100%, 80–99%, 40–79%, and less than 40%. The desired prescription-writing accuracy score, or gold standard, is 100%. However, from previous studies, attainment of the gold standard was negligible because 100% compliance with any standard is physically and cognitively impossible.12,32 Therefore, the accuracy score ranges from 80–100%, 40–79%, and less than 40% were employed, which are descriptive. The definition and severity categorization of the National Coordinating Council of Medication Error Reporting and Prevention (NCCMERP) was used.1 The definition states that medication errors are preventable incidents that can result in harm to the patient or inappropriate medication use while under the control of a healthcare professional, patient, or consumer. These errors can occur due to various factors such as prescribing, order communication, product labeling, packaging, nomenclature, compounding, dispensing, distribution, administration, education, monitoring, and use. The prevalence of ME was defined as the percentage of the total number of pediatric patients who had at least one error at the time of the study against the number of patients on admission.
The errors were also classified based on the severity of the outcome into nine categories (A-I) and broadly into four types: No Error, No error no harm, Error harm, and Error Death. Potential drug-drug interactions (pDDIs) were assessed using the Drug.com interaction checker and classified into no interaction, minor, moderate, and major, and pharmacokinetic and pharmacodynamic interactions.35 Major interaction is depicted as a highly clinically significant interaction that requires avoidance of combination, while moderate is described as clinically significant, but medicines can be used in special situations and can be avoided based on the risk. Minor describes a minimally clinically significant interaction that requires risk assessment, considering an alternate medicine, and instituting a monitoring plan. Descriptive statistics were applied, and results were presented as frequencies, percentages, median, and interquartile range. A Kruskal–Wallis H-test was used to show if there was a statistically significant difference in prescription accuracy scores among the different hospitals. The Mann–Whitney U-test was used to determine if there is a statistically significant difference in the GAS between the tertiary hospital and the secondary hospitals. Pearson’s correlation was used to assess the relationship between the number of medicines prescribed and the occurrence of pDDIs. The p-value of < 0.05 was considered statistically significant.
Results
Essential Elements of Prescriptions
We assessed 366 prescriptions from the three hospitals, each having approximately 33% of the entire sample. Figure 1 shows the level of completion in percentages of the 17 essential elements of a prescription across the hospitals. Prescribers achieved rates of over 90% for the date of prescription, name of the patient, medication strength, formulation, medication dosage, and legibility. Relatively high rates were also seen with the use of generic names 268 (74.3%), the use of recommended abbreviations and decimal points 280 (76.5%), and prescriber signature 291 (79.5%). Conversely, lower completion levels were seen for treatment duration 175 (47.8%), patient’s diagnosis 65 (17.8%), weight 61 (16.7%), and prescriber qualification 48 (13.1%).
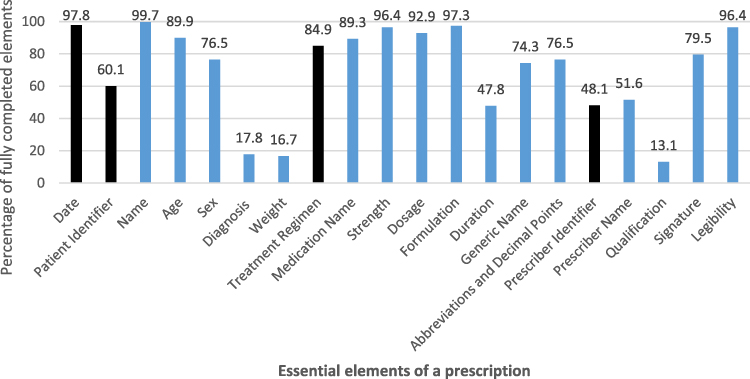 |
Figure 1 Scores of Prescription Completeness and Accuracy across 17 Essential Elements for King Harman Maternity and Children Hospital, Ola During Children’s Hospital, and Rokupa Government Hospital, 2021, (N=366). The 17 Elements are represented by the Blue bars, and the Black bars represent the four Broad Categorizations. |
Global Accuracy Score (GAS) of Prescription Elements
While no prescription attained the gold standard of 100%, 106 (29.0%) prescriptions achieved the 80–100% mark. In addition, the patient identifiers 63 (17.2%), treatment details 228 (62.3%), and prescriber identifiers 33 (9.0%) achieved the overall GAS range of 80–100%. Also, the attainment of the 80–100% GAS range was more prevalent for patient identifiers (25.4%) for ODCH, treat identifier 91 (74.6%) for RGH and prescriber identifiers 19 (15.5%) for KHMCH.
A Kruskal–Wallis H-test showed no statistically significant difference among the hospitals regarding the overall global accuracy of prescription writing score: χ2 = 5.471, P = 0.065 (Table 2). However, there was a statistically significant difference in prescription accuracy scores among the different hospitals in terms of date: χ2 = 6.372, P = 0.041; patient identifiers: χ2 = 19.807, P = <0.001; treatment identifiers: χ2 = 7.662, P = 0.022; and prescriber identifiers: χ2 = 49.702, P = <0.001 (Table 2). As a result, the overall median global accuracy of prescription writing score was 25.00 (IQR =6.00); patient identifier was 6.00 (IQR =0.00); treatment identifier was 12.00 (IQR =4.00); and prescriber identifiers was 4.00 (IQR = 2.00) (Table 2).
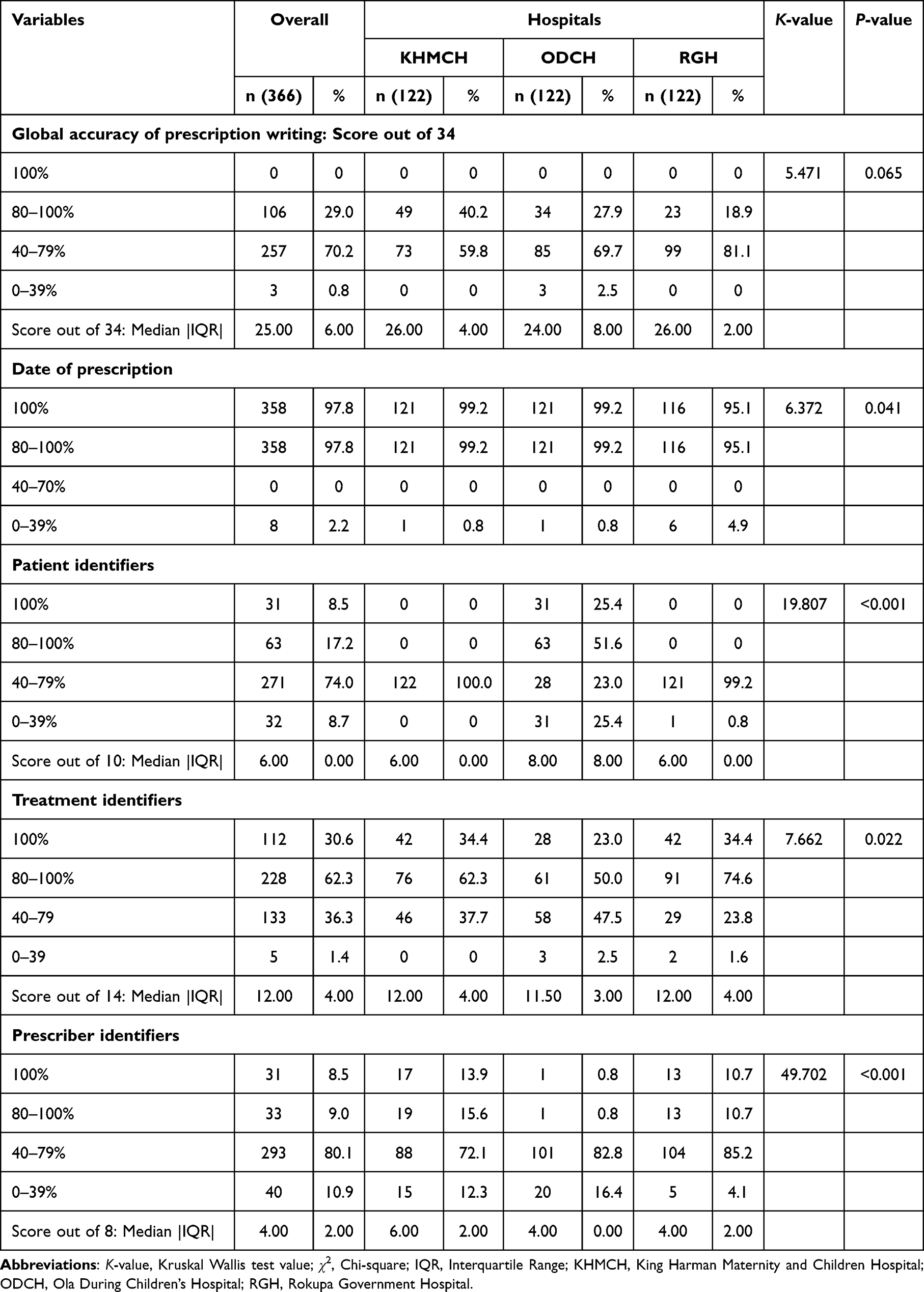 |
Table 2 Global Accuracy Scores per Prescription and by Elements for King Harman Maternity and Children Hospital, Ola During Children’s Hospital, and Rokupa Government Hospital, 2021 |
Furthermore, using the Mann–Whitney U-test, we investigated the differences in prescription accuracies between the hospitals. The comparison between KHMCH, a secondary healthcare facility, versus ODCH, a tertiary and teaching hospital, showed that there was a statistically significant difference in prescription accuracy scores in terms of patient identifiers (P =0.001) and prescriber identifiers (P<0.001). However, the overall accuracy of prescription writing (P=0.055), date of prescription (P=1.000), and treatment identifiers (P= 0.057) were not significant. Similarly, the comparison between RGH, a secondary level facility versus ODCH showed that there was a statistically significant difference in prescription accuracy scores in terms of patient identifiers (P=0.001), treatment identifiers (P=0.007), and prescriber identifiers (P<0.001). However, the overall global accuracy of prescription writing (P=0.122) and prescription date (P=0.056) were insignificant.
Types and Severity of Medication Errors
We reviewed 132 inpatient charts across all three hospitals, with ODCH having 104 (79%), RGH 15 (11%), and KHMCH 13 (10%). Table 3 showed that of the 132 charts, 74 (56.1%) had at least one medication error, and a total of 89 medication errors were observed. Of the 89 errors, 1 (1.1%) was a prescription error and 25 (28%) were dispensing errors, specifically errors of omission. Most of the medication errors were administration errors, 63 (70.7%) with wrong frequency 25 (28.1%), followed by a wrong time of administration, 16 (17.9%) being the most common ones. Assessment of medication error severity based on the NCCMERP classification revealed that 50 (56.2%) were in category C.
 |
Table 3 Types and Severity of Medication Errors for King Harman Maternity and Children Hospital, Ola During Children’s Hospital, and Rokupa Government Hospital, 2021 |
Potential Drug-Drug Interactions
Of the 132 inpatient charts, 54 (40.9%) had at least one pDDI. The number of pDDIs recorded was 64, and the maximum number of interactions, 28 (43.8%), occurred with prescriptions containing four medicines, followed by 19 (29.7%) interactions with three medications and 17 (26.6%) with five medicines. There was also a statistically significant correlation between the number of medicines prescribed and occurrence of pDDIs (r=0.211, P=0.015).
Table 4 showed that most of the interactions were moderate in severity 58 (90%), followed by 3 (5%) major and 3 (5%) minor. The major clinically significant pDDIs involved Furosemide and Gentamycin 2 (3.15%), followed by Diclofenac and Ibuprofen 1 (1.6%). The moderate clinically significant pDDIs were Gentamycin and Ampicillin 41 (64.1%) and Ceftriaxone and Furosemide 17 (26.6%). The 20 pharmacodynamic interactions observed were additive and could increase the potential for serious gastrointestinal toxicity (bleeding, ulceration, inflammation, and perforation) 1 (1.6%) and a synergistic mechanism that could increase the risk of ototoxicity and nephrotoxicity 2 (3.1%), and increase risk of nephrotoxicity 17 (26.6%). Of the 44 pharmacokinetic interactions, 41 (64.1%) could affect absorption through complexation, and 3 (4.7%) could affect excretion.
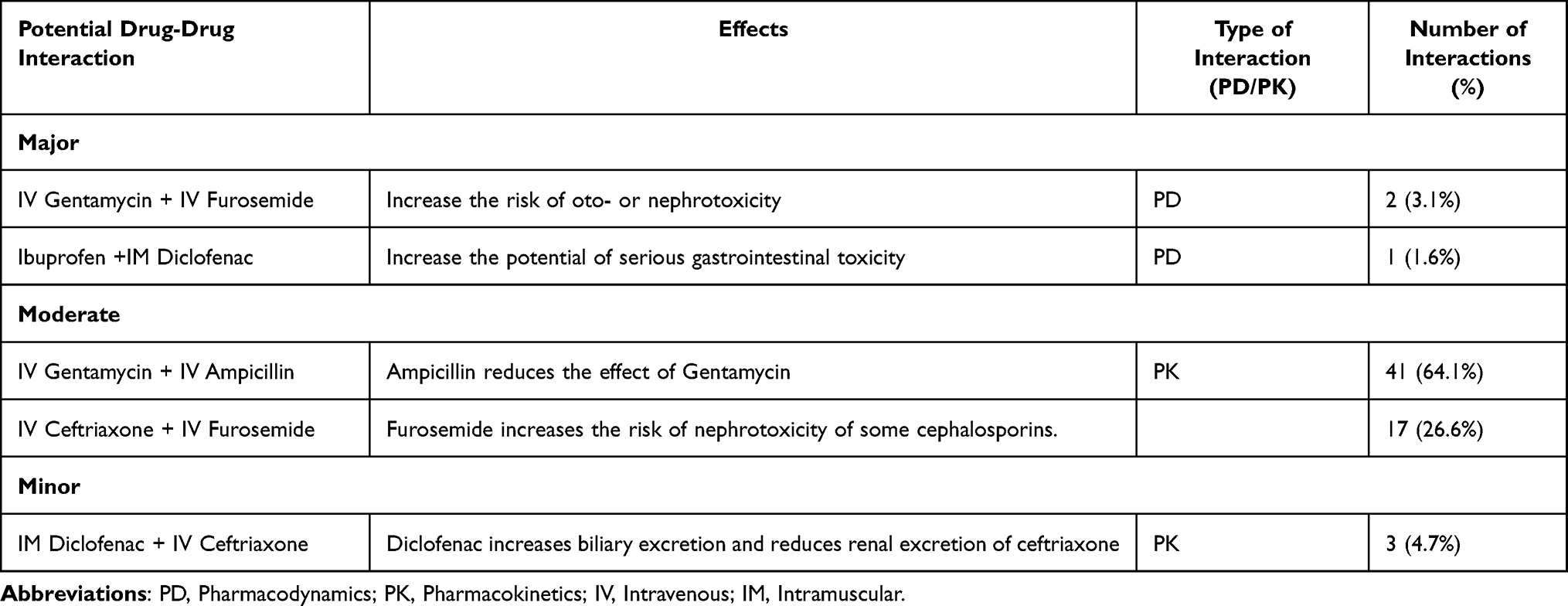 |
Table 4 Potential Drug-Drug Interactions for King Harman Maternity and Children Hospital, Ola During Children’s Hospital, and Rokupa Government Hospital, 2021 |
Discussion
This study assessed the prevalence and nature of MEs, including pDDIs, in pediatric patients. Missing prescription elements and a low GAS were observed. At least one medication error occurred at each stage of the medication use cycle, of which category C MEs based on severity were more prevalent. Also, potential clinically significant drug-drug interactions occurred.
Our study showed that essential elements were missing from all the prescriptions. This is comparable to studies conducted in India, Sudan, and Nigeria, where patient details such as age, weight, diagnoses, and medication duration were omitted in prescriptions.15,36,37 The availability of age and weight has implications in the pharmacodynamics and pharmacokinetics of the medicine as they aid the pharmacist in calculating the correct dose, whereas the diagnosis is vital in determining the prescription rationality.38–40
Furthermore, although pediatric doses can be calculated from adult doses using age or weight, pediatric patients usually require higher doses of water-soluble drugs than adults on a mg/kg basis.41,42 In situations where therapy duration is not available, it is challenging to monitor patient outcomes as this can result in over or under-dosing, predisposing patients to toxicity or sub-optimal therapeutic effects. Overall, an ideal prescription should contain vital elements such as date, patient, medicine, and prescriber details since incomplete information may lead to adverse consequences such as adverse drug reactions, suboptimal patient adherence, and poor quality of life.25 These consequently may cause dire economic consequences, preventable medication-related hospital admissions, and death since children are particularly prone due to the need for specialized formulations and their inability to communicate.26,27
The GAS obtained in this study further corroborates the findings of the essential elements of a prescription as close to a third of the prescriptions met the 80–100% standard; thus, it is similar to a study done in South Africa.12 The possible reason could be the poor infrastructure and resources for healthcare delivery, including inadequate staffing levels, stressful working conditions, a heavy workload, and poorly equipped healthcare facilities in our setting. Consequently, hospitals tend to be overcrowded and lack necessary resources such as computers or electronic health records, which are crucial in facilitating error-free prescription writing processes.43 Healthcare professionals frequently have substantial workloads and face time constraints when attending to patients, resulting in expedited prescription writing and heightened susceptibility to errors.19 There may also be weak regulatory oversight of professional practices and ensuring adherence to prescription-writing guidelines.44 Therefore, resolving these concerns necessitates a comprehensive and diverse strategy, encompassing enhancing healthcare infrastructure, strengthening continuous professional development, and enhancing regulatory oversight. There was also no statistically significant difference in the overall GAS between the tertiary and teaching (ODCH) and the secondary hospitals (KHMCH and RGH). The explanation for this could be attributed to the adherence of the tertiary and secondary hospitals to standardized treatment and prescription protocols that the national healthcare system has established.10,11 Healthcare personnel in both facilities usually undergo comparable training, particularly concerning prescription writing. This uniformity in adhering to guidelines can lead to similar prescribing practices. Notably, the absence of a statistically significant disparity in the quality of prescription writing does not automatically imply an equivalent quality of healthcare across different establishments. There may be notable variations in specialist and consultant service availability, access to modern diagnostic technologies, and patient outcomes between tertiary and secondary healthcare facilities.
This study reported that over half of the patients were exposed to at least one medication error, the most common being administration errors followed by dispensing errors. Most medication errors in our study were classified as NCC-MERP category C, indicating actual errors but no harm to the patients. Our study is consistent with those conducted in Kenya45 (75.8%), Western Ethiopia46 (68.0%), and Northeast Ethiopia47 (58.1%). However, lower values of 5.7% and 0.9% have been reported in the United States of America48 and France,49 respectively. Medication errors can occur at any point in the medicine’s use cycle, from prescribing, dispensing, transcribing, and administration, resulting in increased economic loss, morbidity, and mortality of patients.26 Low-income settings like ours typically have limited access to advanced technologies, such as computerized physician order entry systems and barcode medication administration systems. These technologies can help to reduce medication errors by providing real-time information and alerts about drug interactions, allergies, and dosing errors.3 In addition, healthcare professionals in our jurisdiction have poor awareness and limited access to extensive education and training resources on pharmacovigilance and medication error reporting systems.28 Furthermore, studies have reported that the involvement of clinical pharmacists in ward rounds, which is missing in our settings, can result in prompt identification, reporting, and reduction in MEs.50
In our study, about two-fifths of the reviewed charts had at least one pDDI, similar to studies done in the United States of America21 (49%) and Turkey20 (42%). Drug-drug interactions are responsible for morbidity, mortality, and economic loss and represent an essential and hugely unidentified source of medication errors.51,52 Children may exhibit increased vulnerability to negative consequences as a result of ethnic variances in pharmacokinetics and pharmacodynamics, organ functionality, and developmental stages, potentially leading to adverse outcomes.51–54 To address these concerns, healthcare practitioners must thoroughly evaluate the likelihood of drug-drug interactions and engage in vigilant monitoring to detect and manage any potential adverse effects or interactions swiftly. In this study, the maximum number of interactions occurred with prescriptions containing four medicines, similar to a study done in Pakistan.55 Polypharmacy could be detrimental and should be avoided in children to minimize the risk of DDIs.56 However, lower pDDI prevalence has been reported in the Czech Republic57 (3.8%) and Bangladesh58 (17%). On the other hand, higher values were reported in India59 (66.2%) and Brazil60 (70.0%). These variances in prevalence from our study and other studies could be due to differences in the study design and the software employed to detect pDDIs.
Most pDDIs were moderately clinically significant, implying that clinicians should avoid combinations or use them only under exceptional circumstances. This result is consistent with research conducted in India22 and Iran,61 which requires close monitoring to prevent adverse effects.52 Most of the pDDIs reported in this study were pharmacokinetic and could alter medicine absorption by increasing or decreasing it. Altered absorption due to DDIs can reduce the concentrations of other medicines. Although Gentamycin and Ampicillin are considered the first-line antibiotics for managing sepsis in children, this combination was the most common interaction observed and could reduce bioavailability.62 Ampicillin can deactivate aminoglycosides in vitro and in vivo by complexation, though their concurrent use confers the therapeutic advantage of enhancing bactericidal efficacy through synergistic effects in children with sepsis.63 This effect is substantial when healthcare professionals mix Gentamycin and Ampicillin in the same intravenous (IV) line or container for administration to patients, a common practice at the study sites or among patients with renal failure. As a result, lower serum concentrations of aminoglycosides may be seen, and dosage titration may be required.64,65 We advised the medical teams to ensure that Aminoglycosides like Gentamycin and Ampicillin are given separately during combined therapy since the reduction in absorption in such cases may result in therapeutic failure and antibiotic resistance.
The pharmacodynamic interactions observed were due to either synergism or additive effect. Potential nephrotoxicity and ototoxicity were observed for Furosemide and Gentamycin, Ceftriaxone, and Furosemide, while an increased risk of serious gastrointestinal toxicity was observed for Diclofenac and Ibuprofen.66–69 In such cases, we advised close monitoring of patients and dose titration. We further recommended that these combinations be circumvented or substituted with another medicine to prevent major clinically significant interactions like Gentamycin and Furosemide, Ibuprofen, and Diclofenac.
Limitations of the Study
This study has some limitations. Firstly, we intended to employ the probability proportional to size sampling. However, when we did, the samples we got for the two other hospitals were small since Ola During Children’s Hospital had ten times more prescriptions. As a result, this may not give a good picture of the situation at the two other hospitals. Therefore, we conducted a retrospective review of selected prescriptions that were not distributed by probability proportional to size sampling in the hospitals, which may not represent the entire picture. The sample size is small and period is short for the study such that it does not allow the evaluation of the influence of seasonality on the occurrence of medication errors. Because a point prevalence descriptive chart review design was employed, this might have contributed to the identification of only category B and C MEs. Thus, using a prospective study design in the future would aid in identifying other categories of MEs.
Although the results may not be representative of all pediatric hospitals in Freetown, Sierra Leone, this data can be inferred to other hospitals with similar characteristics as the study sites. The study was conducted in a few hospitals; therefore, the results cannot be generalized. Furthermore, the clinician’s viewpoint was not considered for the medication error component, which would have differed from the reported observations. The DDI software provided only a “potential” estimate of pDDI; therefore, prospective studies can be done to identify adverse effects. Finally, although this study was conducted at two different levels of care, it did not capture data from primary care facilities or private medical institutions.
Conclusion and Recommendation
The low GAS obtained indicates poor conformity with prescription writing guidelines, resulting in high prescribing errors. The optimum standard was not attained for all prescriptions due to the omission of fundamental elements. Medication errors occurred at each phase of the medication use cycle. In addition, potential clinically significant drug-drug interactions occurred, with pharmacokinetics interactions being the most common. Therefore, in-service prescription writing training should be enhanced, a quality improvement programs implemented, and the hospital management should provide standard prescription forms that contain the essential elements of a prescription. More studies with prospective designs and those considering the clinician’s viewpoint should be done. Pharmacists should be involved in routine medicine monitoring and review, ward rounds, conducting frequent prescription and medical chart audits, and providing feedback to other healthcare professionals. This could raise clinicians’ awareness of MEs and pDDIs and improve treatment outcomes and patient well-being.
Data Sharing Statement
The datasets analyzed in this study are available at https://doi.org/10.5281/zenodo.8185857.
Ethics Approval and Informed Consent
Clearance to conduct the study was obtained from the Research, Innovation, and Publication Review Committee of the Faculty of Pharmaceutical Sciences, College of Medicine and Allied Health Sciences, University of Sierra Leone (RIPC-008-21). The management of the hospitals permitted the study to be done in their facilities. Informed consent was obtained from parents/caregivers after explaining the study’s purpose and procedures. Parents gave consent before data was collected and were not coerced to participate in the study. Patient information was coded and kept confidential.
Acknowledgments
We thank the management and staff at the study sites for their support in conducting this study.
Disclosure
We declare no competing interests.
References
1. National Coordination Council for Medication Error Reporting and Prevention (NCCMERP). About medication errors: what is a medication? 2023. Available from: https://www.nccmerp.org/about-medication-errors.
2. Manias E, Cranswick N, Newall F, et al. Medication error trends and effects of person‐related, environment‐related, and communication-related factors on medication errors in a pediatric hospital. J Pediatric Child Health. 2019;55(3):320–326. doi:10.1111/jpc.14193
3. Rinke ML, Bundy DG, Velasquez CA, et al. Interventions to reduce pediatric medication errors: a systematic review. Pediatrics. 2014;134(2):338–360. doi:10.1542/peds.2013-3531
4. Kacew S, Lock S. Developmental aspects of pediatric pharmacology and toxicology. In: Drug Toxicity and Metabolism in Pediatrics. CRC Press; 2018:1–14.
5. Ghaleb MA, Barber N, Franklin BD, Yeung VW, Khaki ZF, Wong IC. Systematic review of medication errors in pediatric patients. Ann Pharmacother. 2006;40(10):1766–1776. doi:10.1345/aph.1G717
6. Kozer E, Berkovitch M, Koren G. Medication errors in children. Pediatr Clinics. 2006;53(6):1155–1168. doi:10.1016/j.pcl.2006.09.005
7. D’Errico S, Zanon M, Radaelli D, et al. Medication errors in pediatrics: proposals to improve the quality and safety of care through clinical risk management. Front Med. 2022;8:814100. doi:10.3389/fmed.2021.814100
8. Billstein-Leber M, Carrillo COLJD, Cassano AT, et al. ASHP guidelines on preventing medication errors in hospitals. ASHP guidelines on preventing medication errors in hospitals. Am J Health-Syst Pharm. 2018;75(19):1493–1517. doi:10.2146/ajhp170811
9. World Health Organization. Reporting and learning systems for medication errors: the role of pharmacovigilance centers; 2014. Available from: https://apps.who.int/iris/bitstream/handle/10665/137036/9789241507943_eng.pdf.
10. Pharmacy Board of Sierra Leone (PBSL). Pharmacy and drugs act 2001. Available from: http://www.sierra-leone.org/Laws/2001-12.pdf.
11. De Vries THR, Hogerzeil HV. Fresle D guide to good prescribing: a practical manual. World Health Organization; 1994. Available from: https://apps.who.int/iris/bitstream/handle/10665/59001/WHO_DAP_94.11.pdf.
12. Ragaven LB, Nkera-Gutabara JG. Adherence to prescription-writing guidelines for outpatients in Southern Gauteng district hospitals. Afr J Prim Health Care Fam Med. 2020;12(1):1–11.
13. Barbour E, Hughes J, Gill D. P11 improving the completion of the medication prescription and administration record on a pediatric ward.
14. Shimelis D. Quality of pediatric prescription writing at Department of Pediatrics and Child Health, Tikur Anbessa Specialized Teaching Hospital, Addis Ababa, Ethiopia. Ethiop J Ped Child Health. 2015;11(1):37–45.
15. Abdellah AE, Abdelrahman SM. Prescription writing quality in pediatric teaching hospitals in Khartoum. Sudan J Paediatr. 2012;12(1):64.
16. Azar C, Allué D, Valnet-Rabier MB, et al. Patterns of medication errors involving pediatric population reported to the French Medication Error Guichet. Pharm Pract. 2021;19(2):2360. doi:10.18549/PharmPract.2021.2.2360
17. Conn RL, Tully MP, Shields MD, Carrington A, Dornan T. Characteristics of reported pediatric medication errors in Northern Ireland and use in quality improvement. Pediatr Drugs. 2020;22:551–560. doi:10.1007/s40272-020-00407-1
18. Gates PJ, Baysari MT, Gazarian M, Raban MZ, Meyerson S, Westbrook JI. Prevalence of medication errors among pediatric inpatients: systematic review and meta-analysis. Drug Safety. 2019;42:1329–1342. doi:10.1007/s40264-019-00850-1
19. Alghamdi AA, Keers RN, Sutherland A, Ashcroft DM. Prevalence and nature of medication errors and preventable adverse drug events in pediatric and neonatal intensive care settings: a systematic review. Drug Safety. 2019;42:1423–1436. doi:10.1007/s40264-019-00856-9
20. Bebitoğlu BT, Oğuz E, Nuhoğlu Ç, et al. Evaluation of potential drug-drug interactions in a pediatric population. Turk Arch Pediatr. 2020;55(1):30.
21. Feinstein J, Dai D, Zhong W, Freedman J, Feudtner C. Potential drug-drug interactions in infant, child, and adolescent patients in Children’s hospitals. Pediatrics. 2015;135(1):e99–e108. doi:10.1542/peds.2014-2015
22. Rao C, Shenoy V, Udaykumar P. Potential drug–drug interactions in the pediatric intensive care unit of a tertiary care hospital. J Pharmacol Pharmacotherapeutics. 2019;10(2):63–68. doi:10.4103/jpp.JPP_27_19
23. Oshikoya KA, Oreagba IA, Godman B, et al. Potential drug-drug interactions in pediatric outpatient prescriptions in Nigeria and implications for the future. Expert Rev Clin Pharmacol. 2016;9(11):1505–1515. doi:10.1080/17512433.2016.1232619
24. Rodrigues MCS, Oliveira C. Drug-drug interactions and adverse drug reactions in polypharmacy among older adults: an integrative review. Rev Lat Am Enfermagem. 2016;24. doi:10.1590/1518-8345.1316.2800
25. Chiatti C, Bustacchini S, Furneri G, et al. The economic burden of inappropriate drug prescribing, lack of adherence and compliance, adverse drug events in older people: a systematic review. Drug Safety. 2012;35(S1):73–87. doi:10.1007/BF03319105
26. Elliott RA, Camacho E, Jankovic D, Sculpher MJ, Faria R. Economic analysis of the prevalence and clinical and economic burden of medication error in England. BMJ Qual Saf. 2021;30(2):96–105. doi:10.1136/bmjqs-2019-010206
27. Mulac A, Taxis K, Hagesaether E, Granas AG. Severe and fatal medication errors in hospitals: findings from the Norwegian Incident Reporting System. Eur J Hosp Pharm. 2021;28(e1):e56–e61.
28. Abiri OT, Johnson WCN. Pharmacovigilance systems in resource-limited settings: an evaluative case study of Sierra Leone. J Pharm Policy Pract. 2019;12:13. doi:10.1186/s40545-019-0173-2
29. Isah AO, Pal SN, Olsson S, Dodoo A, Bencheikh RS. Specific features of medicines safety and pharmacovigilance in Africa. Ther Adv Drug Saf. 2012;3(1):25–34. doi:10.1177/2042098611425695
30. Coker J, Bawoh M, Lahai M, Abiri O, Mambu T, Lisk D. Adherence to a standard prescription writing guidelines in a Tertiary Hospital in Sierra Leone. Int J Sci Res. 2021;10(2):177–180.
31. Geoffrey CU, Plou S. Research randomizer 1997–2021. Available from: https://www.randomizer.org.
32. N JG. Audit of medical prescriptions writing compliance with essential medicines list standards in the outpatient Department of South Rand Hospital, Johannesburg: a quality improvement project. Unpublished report. Johannesburg: Department of Family Medicine, University of the Witwatersrand; 2013.
33. Patel NM, Vaniya HV, Agrawal JM, Balat JD, Singh AP, Trivedi HR. Adverse drug reaction monitoring on antiretroviral therapy in human immunodeficiency virus patients in a tertiary care hospital. Int J Basic Clin Pharmacol. 2015;4:907–911. doi:10.18203/2319-2003.ijbcp20150864
34. Hassan NB, Ismail HC, Naing L, Conroy RM, Abdul Rahman AR. Development and validation of a new prescription quality index. Br J Clin Pharmacol. 2010;70(4):500–513. doi:10.1111/j.1365-2125.2009.03597.x
35. Drug.com. Drug interactions checker 2000–2022. Available from: https://www.drugs.com/drug_interactions.html.
36. Mishra S, Pathak PK, Ahmad S, et al. Quality of prescription writing practices in a Tertiary Care Teaching Hospital of Bihar: a Cross-Sectional Study. Int J Health Syst Implement Res. 2020;4(2):24–33.
37. Oshikoya K, Chukwura H, Ojo O. Evaluation of outpatient pediatric drug prescriptions in a teaching hospital in Nigeria for rational prescribing. Pediatr Perinat Drug Ther. 2006;7(4):183. doi:10.1185/146300906X167728
38. Mohammed-Jawad NK, Abdulrahman NM, Emad A, Jumaa S. Assessment of dosing errors in pediatric patients prescriptions in Basra city. Arch Pharm Pract. 2020;11(1):73–76.
39. Callaghan LC. Prescribing in pediatric obesity: methods to improve dosing safety in weight-based dose calculations. Arch Dis Child Educ Pract. 2018;103(5):274–277. doi:10.1136/archdischild-2016-311491
40. O’Hara K. Paediatric pharmacokinetics and drug doses. Austr Prescr. 2016;39(6):208. doi:10.18773/austprescr.2016.071
41. Lim SY, Pettit RS. Pharmacokinetic considerations in pediatric pharmacotherapy. Am J Health Syst Pharm. 2019;76(19):1472–1480. doi:10.1093/ajhp/zxz161
42. Bereda G. Pediatrics pharmacokinetics and dose calculation. J Pediatr Neonatal Cares. 2022;12:96–102. doi:10.15406/jpnc.2022.12.00463
43. Wimmer S, Toni I, Botzenhardt S, Trollmann R, Rascher W, Neubert A. Impact of a computerized physician order entry system on medication safety in pediatrics—The AVOID study. Pharmacol Res Perspect. 2023;11(3):e01092. doi:10.1002/prp2.1092
44. Bates DW. Preventing medication errors: a summary. Am J Health Syst Pharm. 2007;64(14_Supplement_9):S3–S9. doi:10.2146/ajhp070190
45. Khaemba CN. Incidence and determinants of medication errors among paediatric inpatients at Kisii level 5 hospital. Doctoral dissertation; University of Nairobi. Available from: http://erepository.uonbi.ac.ke/handle/11295/76448.
46. Fekadu G, Abdisa E, Fanta K. Medication prescribing errors among hospitalized pediatric patients at Nekemte Referral Hospital, western Ethiopia: a cross-sectional study. BMC Res Notes. 2019;12(1):1–6. doi:10.1186/s13104-019-4455-1
47. Zeleke A, Chanie T, Woldie M. Medication prescribing errors and associated factors at the pediatric wards of Dessie Referral Hospital, Northeast Ethiopia. Int Arch Med. 2014;7(1):1–6. doi:10.1186/1755-7682-7-18
48. Kaushal R, Bates DW, Landrigan C, et al. Medication errors and adverse drug events in pediatric inpatients. JAMA. 2001;285(16):2114–2120. doi:10.1001/jama.285.16.2114
49. Lalande J, Vrignaud B, Navas D, et al. A prospective observational study of medication errors in a pediatric emergency department. Arch Pediatr. 2018;25(6):355–358. doi:10.1016/j.arcped.2018.06.005
50. Drovandi A, Robertson K, Tucker M, Robinson N, Perks S, Kairuz T. A systematic review of clinical pharmacist interventions in pediatric hospital patients. Eur J Pediatr. 2018;177:1139–1148. doi:10.1007/s00431-018-3187-x
51. Lubinga S, Uwiduhaye E. Potential drug-drug interactions on in-patient medication prescriptions at Mbarara Regional Referral Hospital (MRRH) in western Uganda: prevalence, clinical importance and associated factors. Afr Health Sci. 2011;11(3):499–507.
52. Moura C, Prado N, Acurcio F. Potential drug-drug interactions associated with prolonged stays in the intensive care unit: a retrospective cohort study. Clin Drug Invest. 2011;31:309–316. doi:10.1007/BF03256929
53. Walsh EK, Hansen CR, Sahm LJ, Kearney PM, Doherty E, Bradley CP. Economic impact of medication error: a systematic review. Pharmacoepidemiol Drug Saf. 2017;26(5):481–497. doi:10.1002/pds.4188
54. Tan-Koi WC, Limenta M, Mohamed EH, Lee EJ. The importance of ethnicity definitions and pharmacogenomics in ethnobridging and pharmacovigilance. In: Pharmacogenomics. Academic Press; 2019:289–327.
55. Qorraj-Bytyqi H, Hoxha R, Krasniqi S, Bahtiri E, Kransiqi V. The incidence and clinical relevance of drug interactions in pediatrics. J Pharmacol Pharmacotherapeutics. 2012;3(4):304. doi:10.4103/0976-500X.103686
56. Hassanzad M, Tashayoie Nejad S, Mahboobipour AA, Salem F, Baniasadi S. Potential drug-drug interactions in hospitalized pediatric patients with respiratory disorders: a retrospective review of clinically important interactions. Drug Metab Pers Ther. 2020;35(1):20190012.
57. Langerová P, Prokeš M, Konvalinka M, Fürstová J, Urbánek K. Incidence of potential drug interactions in medication prescriptions for children and adolescents in the University Hospital Olomouc, Czech Republic. Eur J Pediatr. 2013;172:631–638. doi:10.1007/s00431-013-1933-7
58. Ahmed S, Yesmine S, Rahman M, Shahriar M. Assessment of interactions of drugs prescribed for pediatric patients in Bangladesh. Bangladesh Pharm J. 2021;24(2):91–98. doi:10.3329/bpj.v24i2.54706
59. Mistry M, Gor A, Ganguly B. Potential drug-drug interactions among prescribed drugs in the pediatric outpatients department of a tertiary care teaching hospital. J Young Pharm. 2017;9(3):371. doi:10.5530/jyp.2017.9.74
60. Costa HT, Leopoldino RWD, da Costa TX, Oliveira AG, Martins RR. Drug–drug interactions in neonatal intensive care: a prospective cohort study. Pediatr Neonatol. 2021;62(2):151–157. doi:10.1016/j.pedneo.2020.10.006
61. Ahmadi M, Nazemi A, Davoodpour SF, Gharaie Pour F, Montaseri M, Safa O. A retrospective and cross-sectional study to evaluate potential drug–drug interaction in hospitalized pediatrics, Bandar Abbas, Iran. Trends Pharmacol Sci. 2018;4(4):241–248.
62. Bibi S, Chisti MJ, Akram F, Pietroni MA. Ampicillin and gentamicin are a useful first-line combination for the management of sepsis in under-five children at an urban hospital in Bangladesh. J Health Popul Nutr. 2012;30(4):487–490. doi:10.3329/jhpn.v30i4.13418
63. Pickering LK, Rutherford I. Effect of concentration and time upon inactivation of tobramycin, gentamicin, netilmicin and amikacin by azlocillin, carbenicillin, mecillinam, mezlocillin and piperacillin. J Pharmacol Exp Ther. 1981;217(2):345–349.
64. Viollier A-F, Standiford HC, Drusano GL, Tatem BA, Moody MR, Schimpff SC. Comparative pharmacokinetics and serum bactericidal activity of mezlocillin, ticarcillin, and piperacillin, with and without gentamicin. J Antimicrob Chemother. 1985;15(5):597–606. doi:10.1093/jac/15.5.597
65. Kradjan WA, Burger R. In vivo inactivation of gentamicin by carbenicillin and ticarcillin. Arch Intern Med. 1980;140(12):1668–1670. doi:10.1001/archinte.1980.00330230114024
66. Le TA, Hiba T, Chaudhari D, et al. Aminoglycoside-related nephrotoxicity and ototoxicity in clinical practice: a review of pathophysiological mechanism and treatment options. Adv Ther. 2023;40(4):1357–1365. doi:10.1007/s12325-023-02436-x
67. Rostom A, Muir K, Dube C, Lanas A, Jolicoeur E, Tugwell P. Prevention of NSAID-related upper gastrointestinal toxicity: a meta-analysis of traditional NSAIDs with gastroprotection and COX-2 inhibitors. Drug Healthc Patient Saf. 2009;47–71. doi:10.2147/DHPS.S4334
68. Maideen NM, Balasubramanian R, Muthusamy S. A comprehensive review of the pharmacologic perspective on loop diuretic drug interactions with therapeutically used drugs. Curr Drug Metab. 2022;23(3):188–199. doi:10.2174/1389200223666220401092112
69. Getachew H, Assen M, Dula F, Bhagavathula AS. Potential drug–drug interactions in pediatric wards of Gondar University Hospital, Ethiopia: a cross-sectional study. Asian Pac J Trop Biomed. 2016;6(6):534–538. doi:10.1016/j.apjtb.2016.04.002
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.