")
Back to Journals » Lung Cancer: Targets and Therapy » Volume 14
ALESIA 5-Year Update: Alectinib at 600 mg Twice Daily Gives Lorlatinib a Run for Its Money in Asia
Received 30 April 2023
Accepted for publication 2 July 2023
Published 7 July 2023 Volume 2023:14 Pages 71—78
DOI https://doi.org/10.2147/LCTT.S419395
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Fengying Wu
Alexandria TM Lee,1 Saihong Ignatius Ou1,2
1Department of Medicine, University of California Irvine School of Medicine, Orange, CA, USA; 2Chao Family Comprehensive Cancer Center, Orange, CA, USA
Correspondence: Saihong Ignatius Ou, University of California Irvine School of Medicine, Department of Medicine, Division of Hematology-Oncology, Chao Family Comprehensive Cancer Center, 200 South Manchester, Suite 400, Orange, CA, 92868, USA, Tel +1 714-456-5153, Email [email protected]
Abstract: Alectinib, a next-generation anaplastic lymphoma kinase (ALK) tyrosine kinase inhibitor (TKI), has demonstrated superior progression-free survival over crizotinib with both 300 mg twice daily (J-ALEX) or 600 mg twice daily (ALEX, ALESIA) dosing in three pivotal clinical trials. Given the similar median PFS achieved in the J-ALEX trial and the Asian subgroup of the ALEX trial, there remains debate about the optimal alectinib dose for Asians. The third pivotal alectinib trial, ALESIA, which was conducted exclusively in Asia to support the registration of alectinib in China, utilized 600 mg alectinib twice daily. The mature PFS was not reached at the initial publication of ALESIA. At ESMO Asia 2022, the 5-year update of ALESIA was presented with an impressive mature investigator-assessed PFS of 41.6 months (95% CI 33.1– 58.9), which is numerically longer than the mature PFS of 34.1 months achieved by alectinib at 300 mg twice daily in the J-ALEX trial. Based on these results, as well as retrospective pharmacokinetic and responses and PFS data, Alectinib at 600 mg twice daily is the optimal dose for Asians. This has been based on the ALESIA trial and on the retrospective pharmacokinetic and responses and PFS data and has set the benchmark for ALK TKI as the first-line treatment for advanced ALK+ NSCLC in Asia. Importantly, lorlatinib, another next generation ALK TKI, also achieved an impressive hazard ratio with a still immature PFS in all patients, including Asian patients, in a recent subgroup analysis after a median follow-up time of 36.7 months. We await the final mature PFS of lorlatinib overall and for Asian patients in the CROWN trial to see if lorlatinib will set a new standard.
Keywords: ALESIA, CROWN, alectinib, lorlatinib, brigatinib, pharmacokinetics, dose response, ALK fusion, NSCLC
Introduction
Anaplastic lymphoma kinase (ALK) receptor tyrosine kinase fusions have been shown to be present in 3–5% of patients with non-small cell lung cancer (NSCLC), with frequency between both Asian and non-Asian patients.1 There are currently six ALK tyrosine kinase inhibitors (TKIs) (crizotinib, ceritinib, alectinib, brigatinib, lorlatinib, ensartinib) approved for the first-line (1L) treatment of advanced ALK fusion (ALK+) non-small cell lung cancer (NSCLC).2 However, only one ALK TKI, alectinib, has been studied in three randomized Phase 3 trials, based partially on the different approved doses of alectinib in Japan and ex-Japan. The J-ALEX trial, conducted solely in Japan, compared alectinib 300 mg twice daily to crizotinib 250 mg twice daily.3 Alectinib, initially developed by Chugai, Japan, was limited to 300 mg twice daily due to the Japanese government’s limit on the amount of sodium docecyl sulfate (SDS) in the formulation.4 Based on a Phase 1 dose escalation trial conducted in the US with a starting dose of 300 mg twice daily, the recommended Phase 2 dose of alectinib was determined to be 600 mg twice daily.4 The ALEX trial, the globally conducted phase 3 trial, compared alectinib 600 mg twice daily (which is the dose of alectinib approved outside Japan) to crizotinib 250 mg twice daily.5 The final median progression-free survival achieved by alectinib 300 mg twice daily in J-ALEX was 34.1 months, by blinded independent review committee,6 and 34.8 months in the Asian subgroup in the ALEX trial, by investigator assessment.7 These results raised the questions of whether 300 mg twice daily is sufficient for Asian patients, which could provide economic relief to patients by potentially halving the price of alectinib and could likely lower the risk of adverse events with alectinib treatment.
J-ALEX
In the J-ALEX trial, 207 TKI-naïve (but not all treatment naïve) advanced ALK+ NSCLC patients, all from Japan, were randomized 1:1 to receive alectinib 300 mg twice daily or crizotinib 250 mg twice daily.3 The stratification factors of J-ALEX were ECOG performance status (0 or 1 vs 2), treatment line (first vs second), and disease stage (IIIB or IV vs postoperative recurrence). Importantly, the presence or absence of baseline central nervous system (CNS) metastasis was not a stratification factor. ALK fusion confirmation by both immunohistochemistry (IHC) and fluorescence in-situ hybridization (FISH) or reverse transcriptase polymerase chain reaction (RT-PCR). Patients with asymptomatic CNS disease were permitted. The primary endpoint was blinded independent review committee (BIRC)-assessed PFS. At the time of first interim analysis, while BIRC-assessed PFS significantly statistically favored alectinib over crizotinib with an HR of 0.34 (99.7% CI: 0.17–0.71), the mature median PFS for alectinib was not reached.3 With a median follow-up time of 42.4 months in the alectinib group, the final mature median PFS of alectinib was 34.1 months (HR = 0.37; 95% CI: 0.26–0.52)6 (Table 1).
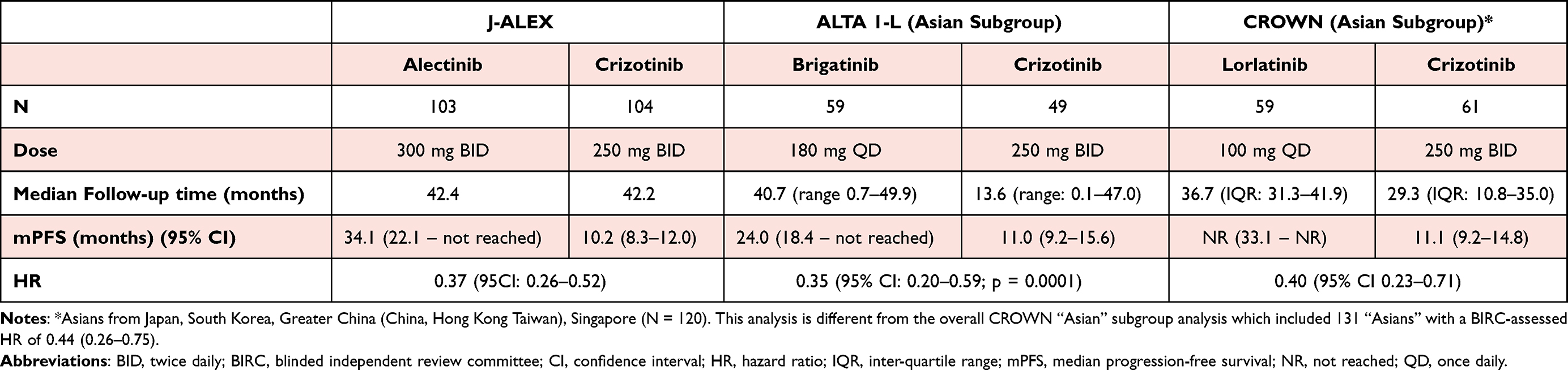 |
Table 1 Comparison of BIRC-Assessed PFS Among Randomized Pivotal Trials of Brigatinib, Alectinib, and Lorlatinib |
ALEX
The ALEX trial is a pivotal trial conducted globally that earned alectinib global approval ex-Japan. In the ALEX trial, 138 Asian and 165 non-Asian patients were randomized 1:1 to alectinib 600 mg twice daily or crizotinib 250 mg twice daily. Importantly, the patients were all treatment-naïve for their advanced ALK+ NSCLC. The stratification factors in ALEX were ECOG performance status (0/1), race, (Asian vs non-Asian) and presence or absence of CNS disease. The primary endpoint was investigator-assessed PFS.5 The detection of ALK fusions was performed by immunohistochemistry (IHC) by central laboratories.
The first report of the ALEX results was based on a median follow-up time of 18.1 months. The independent review committee (IRC)-assessed PFS was 25.7 months in the alectinib group, compared to 11.1 months in the crizotinib group, favoring alectinib with an HR of 0.47 (95% CI 0.34–0.65; p<0.001).4 In data from the second interim analysis, in which the median follow-up time was 27.8 months in the alectinib group and 22.8 months in the crizotinib group, the investigator-assessed PFS was 34.8 months in the alectinib group and 10.9 months in the crizotinib group, favoring alectinib with an HR of 0.43 (95% CI 0.32–0.58).7 In the Asian subgroup, the investigator-assessed PFS was 34.8 months in the alectinib group compared to 9.6 months in the crizotinib group, again favoring alectinib with an HR of 0.43 (95% CI 0.27–0.67)7 (Table 2).
 |
Table 2 Comparison of Investigator-Assessed PFS Among Randomized Pivotal Trials of Brigatinib, Alectinib, and Lorlatinib |
Cross-trial comparison can be fraught with bias as the selection and composition of patients are different in proportions of sex, body mass index (BMI), tumor burden, and diagnostic criteria for entry. In addition, PFS assessment was different among these trials, with PFS assessment by BIRC in the J-ALEX trial and by investigator in the ALEX trial. Nonetheless, the similarity between the BIRC-assessed median PFS of 34.1 months in the alectinib group in the J-ALEX trial6 and the investigator-assessed median PFS of 34.8 months overall and 34.8 months in the Asian subgroup in the ALEX trial7 must be acknowledged by oncologists. This raises the inevitable question of whether 300 mg alectinib twice daily is as efficacious as 600 mg twice daily in Asian patients, as this would lead to 50% cost savings for both patients and health systems.
Importantly, the ALEX and J-ALEX trials are different in that baseline CNS metastasis status was not a stratification factor in the J-ALEX trial. Thus, there was imbalance in the percentage of patients with CNS disease between the alectinib-arm (14%) and the crizotinib-arm (28%) that was likely significant especially because there were only 100 patients per treatment arm.3 Furthermore, regularly scheduled CNS imaging was not required for all patients enrolled, thus the analysis of intra-cranial progression among patients without baseline CNS metastasis may have been skewed, as CNS disease may have only been detected in the presence of symptoms. Additionally, the first interval scan in the J-ALEX trial was completed after only 4 weeks of treatment, as disease assessment was performed every 4 weeks during the first 12 weeks of treatment. Early surveillance scans allowed for early censoring of disease progression which could have artificially lowered the overall response rate and shortened the median PFS of crizotinib in J-ALEX when compared to initial assessment scans completed at week 8 and 16.
ALESIA
ALESIA was conducted to provide additional efficacy and safety data on alectinib to gain regulatory approval in China, in addition to the ALEX trial data. Unintentionally but coincidentally, ALESIA provided the potential “tiebreaker” on the optimal dose of alectinib for Asians. ALESIA enrolled 187 patients from China, Thailand, and South Korea who were randomized 2:1 to alectinib 600 mg twice daily or crizotinib 250 mg twice daily. The stratification factors in ALESIA were performance status and presence or absence of CNS metastasis. Stage 3B patients were allowed to enroll. Patients with asymptomatic brain metastasis or even asymptomatic leptomeningeal carcinomatosis were allowed to enroll per investigator recommendation. All patients had to be treatment-naïve for their advanced disease, similar to the ALEX trial. The primary endpoint was PFS as assessed by investigators.8
Data from the first interim analysis of ALESIA were published after a follow-up time of 16.2 months for alectinib and 15.0 months for crizotinib. Only 24% of the alectinib-treated patients were off-study at the first interim analysis. The PFS as assessed by BIRC revealed an HR 0.37 (95% CI 0.22–0.61; p<0.0001). Importantly, investigator-assessed PFS (primary endpoint) significantly favored alectinib over crizotinib with an HR of 0.22 (95% CI 0.13–0.38; log-rank p<0.0001). Nevertheless, the median PFS for alectinib was not reached in the first interim analysis, while the median PFS for crizotinib was 10.7 months (95% CI 7.4 – not evaluable) by BIRC assessment and 11.1 months (9.1–13.0) by investigator assessment.8 While the investigator-assessed HR was the best HR achieved at the time of data publication (J-ALEX; BIRC-assessed HR = 0.34) and is a more standard way to compare efficacy among trials involving alectinib, the lack of a median PFS has prevented cross-trial comparisons of ALESIA to ALEX or J-ALEX. Thus, the issue of optimal dose of alectinib for Asians remains unresolved without a mature PFS to allow cross-trials comparison even with all the accompanying caveats.
Recently, the 5-year update of ALESIA was presented at ESMO Asia 2022.9 The median follow-up time has increased to 61 months in the alectinib group and 51 months in the crizotinib group. A mature investigator-assessed PFS for alectinib-treated patients was reached at 41.6 months (95% CI 33.1–58.9) compared to the same 11.1 months (95% CI 9.1–18.4) for the crizotinib-treated patients, with an HR of 0.33 (95% CI 0.23–0.49)9 (Table 2). The investigator-assessed HR of 0.33 has moved closer to the previously reported BIRC-assessed HR of 0.37 (Table 2). Similarly, in patients with CNS disease at baseline, investigator-assessed PFS was 42.3 months (95% CI 27.8–60.7) in the alectinib group compared to 9.2 months (95% CI: 5.5–12.2) in the crizotinib group, again favoring alectinib with an HR of 0.17 (95% CI 0.09–0.33). Importantly, treatment with alectinib was also shown to delay time to CNS progression, with HR 0.16 (95% CI 0.08–0.32) by investigator assessment.9 The 41.6 months median PFS is numerically longer than the median PFS of 34.8 months for the Asian subgroup of ALEX trials or the median PFS of 34.1 months from J-ALEX and may provide the most convincing evidence that 600 mg twice daily is the optimal dose for Asians.
Exposure-Efficacy Relationship Study of Alectinib Comparing 300 mg versus 600 mg Twice Daily Dosing (J-ALEX, ALEX, ALESIA)
Roche, the manufacturer of alectinib, performed a pharmacokinetic (PK) clinical efficacy study of the three trials (J-ALEX, ALEX, ALESIA) to assess alectinib’s efficacy by dosing exposure.10 Overall, they found that body-weight affects exposure to alectinib and its major active metabolite (M4). Patients were classified into high and low level alectinib exposure groups, as measured by cumulative area under the molar concentration curve of alectinib and M4 for the first 6 weeks of treatment. The optimal response to alectinib was achieved with concentrations above 1040 nmol/L. Thus, a cutoff of Caverage _6week of 1040 nmol/L of alectinib classified patients into high- and low-level alectinib exposure groups. The HR of PFS for the alectinib low-exposure group when compared to crizotinib 250 mg twice daily was 0.76 (95% CI 0.46–1.25). On the other hand, the HR for the alectinib high-exposure group was 0.36 (95% CI 0.28–0.46). Ultimately, both high and low exposure groups were associated with improved PFS compared to the crizotonib group. However, high alectinib exposure was associated with a greater PFS benefit. Furthermore, at 300 mg twice daily, 70% of the Japanese, 50% of the Chinese, and only 40% of Caucasian patients achieved Caverage_6week > 1040 nmol/L.10 In contrast, at 600 mg twice daily, 92% of patients reached the same cutoff.
Alectinib 600 mg Twice Daily is the Optimal Dose for Both Asians and Non-Asians
The updated data after far longer follow-up time from the ALESIA trial in combination with internal Roche exposure-efficacy data should leave no doubt that the optimal dose of alectinib is 600 mg twice daily. In addition to alectinib, with its impressive PFS of 41.6 months, there are other next-generation ALK TKIs approved for treatment of advanced ALK+ NSCLC. Furthermore, the dose interruption/reduction rate was 67.3% and dose discontinuation rate was 23.1% for the 300 mg twice daily dose of alectinib in J-ALEX.8 The dose interruption, reduction and discontinuation rates were 30.6%, 27.4%, 14.5% for the 600 mg twice daily dose of alectinib in ALESIA.6 Hence alectinib 600 mg twice daily was as tolerable, if not more tolerable, than 300 mg twice daily dose.
Other Next-Generation ALK TKI: ALTA-1L (Brigatinib) and CROWN (Lorlatinib) Asian Subgroup
The Asian subgroup analysis from the ALTA-1L trial, which compared other next-generation ALK TKIs, brigatinib to crizotinib, has been reported.11 The BIRC-assessed PFS of brigatinib was 24 months (95% CI: 18.4 – not reached) with 3-year PFS rate of 47% (95% CI: 33–60), which is significantly better than that achieved by crizotinib, with a BIRC-assessed median PFS of 11.1 months (95% CI: 9.2–15.6) and 3-year PFS rate of 14% (95% CI 5–26). These results favor brigatinib with an HR of 0.35 (95% CI: 0.20–0.59; P = 0.0001). For a more relevant cross-trial comparison using investigator-assessed PFS, the investigator-assessed PFS of brigatinib was 26.7 months (95% CI 18.4 – not reached) compared to 11.0 months (95% CI: 9.2–18.6) in the crizotinib group. These results favor brigatinib with an HR = 0.42 (95% CI: 0. 25–0.73; P = 0.0024) (Table 2). However, the aforementioned caveats of cross-trial comparisons still apply to the median PFS achieved by brigatinib in the overall ALTA-1L group and its Asian subgroup.
On the other hand, lorlatinib, currently the next generation ALK TKI pre-clinically active against the widest spectrum of acquired ALK mutations, demonstrated statistically significant improvement in median PFS compared to crizotinib in the pivotal CROWN trial, with the first interim follow-up of 18.6 months.12 Stratification factors for the CROWN trial were presence or absence of brain metastases and ethnicity (Asians versus non-Asians). Of note, the HR of PFS among Asian patients was 0.47 (95% CI 0.27–0.84) compared to the HR among non-Asian patients of 0.19 (95% CI 0.11–0.32). No formal statistical comparison between these two HRs was performed but still the question on the efficacy of lorlatinib among Asians.12 The second interim update of the CROWN trial, with a median follow-up time of 36.7 months was recently published.13 The updated results showed that the BIRC-assessed for the intention-to-treat (ITT) population was 0.27 (95% CI 0.18–0.39). The BIRC-assessed PFS analysis of the Asian subgroup analysis revealed an HR of 0.44 (95% CI 0.26–0.75) from the Forest plot of the subgroup analysis.13
A separate analysis of Asians (N = 120) from Asia (Japan, South Korea, China, Taiwan, Hong Kong, Singapore) enrolled in the CROWN trial, which is different from ethnic Asians (N = 131) in the CROWN trial, revealed a BIRC-assessed HR of 0.40 (95% CI 0.23–0.71) among Asians14 (Table 1). Importantly, the lower limit of the median PFS for Asians treated with lorlatinib was 33.1 months with the median still not reached.14 The investigator-assessed median PFS with an HR of 0.24 (95% CI 0.14–0.41) among Asian patients again favors lorlatinib (Table 2). The lower 95% CI limit of the median PFS of lorlatinib among Asian patients was 32.9, while the median value is still not reached. Of note, the median PFS of crizotinib achieved by Asian patients was longer as assessed by BIRC (11.1 months; 95% CI 9.2–14.8) compared to investigator-assessed PFS (9.2 months; 95% CI 7.2–12.7), resulting in a “higher” or “less favorable” HR of PFS by BIRC assessment.14 This report re-affirmed previous reports on the efficacy of lorlatinib among Asians.15,16 Importantly, the projection of the median PFS achieved by lorlatinib among Asians in Asia could exceed that achieved by alectinib in ALESIA.
Limitations of Cross-Trial Comparison
Our editorial utilized cross-trial comparison to evaluate and compare efficacy of alectinib at two different doses and other ALK TKIs. Limitations of cross-trial comparisons include differences in patients’ characteristics such as percentage of patients with brain metastasis and body surface area between Japanese, Chinese, and Caucasian patients described previously. Also, in open-label, non-placebo-controlled trials, investigators may have unrecognized bias due to transitioning their patients to a more effective treatment (usually the investigational arm) when cross-over is allowed. Nonetheless, the severe lack of head-to-head comparison of compounds in oncology necessitates cross-trial comparisons.
Executive Summary
- ALESIA 5-year follow-up data demonstrated impressive median PFS survival data for ALK+ Asian patients treated with alectinib. Alectinib at 600 mg twice daily is the optimal dose of alectinib globally for Asians and non-Asians alike. Alectinib at 600 mg twice daily sets the current benchmark for ALK TKI as the first-line treatment for advanced ALK+ NSCLC.
- Lorlatinib seems to project an even longer median PFS among ALK+ NSCLC Asian and non-Asian patients alike. However, without mature PFS, it will take time for oncologists to realize the magnitude of PFS, which could potentially exceed 60 months.2,17
Disclosure
Dr Saihong Ignatius Ou reports personal fees from Pfizer, personal fees from JNJ/Janssen, personal fees from DAVA Oncology LLP, personal fees from Lilly, personal fees, stock holder of Elevation Oncology, stock holder of Turning Point Therapeutics, personal fees from BeiGene, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Tan AC, Tan DS. Targeted therapies for lung cancer patients with oncogenic driver molecular alterations. J Clin Oncol. 2022;40(6):611–625. doi:10.1200/JCO.21.01626
2. Ou SI, Nagasaka M, Brazel D, et al. Will the clinical development of 4th-generation “double mutant active” ALK TKIs (TPX-0131 and NVL-655) change the future treatment paradigm of ALK+ NSCLC? Transl Oncol. 2021;14(11):101191. doi:10.1016/j.tranon.2021.101191
3. Hida T, Nokihara H, Kondo M, et al. Alectinib versus crizotinib in patients with ALK-positive non-small-cell lung cancer (J-ALEX): an open-label, randomised phase 3 trial. Lancet. 2017;390(10089):29–39. doi:10.1016/S0140-6736(17)30565-2
4. Gadgeel SM, Gandhi L, Riely GJ, et al. Safety and activity of alectinib against systemic disease and brain metastases in patients with crizotinib-resistant ALK-rearranged non-small-cell lung cancer (AF-002JG): results from the dose-finding portion of a phase 1/2 study. Lancet Oncol. 2014;15(10):1119–1128. doi:10.1016/S1470-2045(14)70362-6
5. Peters S, Camidge DR, Shaw AT, et al. Alectinib versus crizotinib in untreated ALK-positive non-small-cell lung cancer. N Engl J Med. 2017;377(9):829–838. doi:10.1056/NEJMoa1704795
6. Nakagawa K, Hida T, Nokihara H, et al. Final progression-free survival results from the J-ALEX study of alectinib versus crizotinib in ALK-positive non-small-cell lung cancer. Lung Cancer. 2020;139:195–199. doi:10.1016/j.lungcan.2019.11.025
7. Camidge DR, Dziadziuszko R, Peters S, et al. Updated efficacy and safety data and impact of the EML4-ALK fusion variant on the efficacy of alectinib in untreated ALK-positive advanced non-small cell lung cancer in the global phase III ALEX study. J Thorac Oncol. 2019;14(7):1233–1243. doi:10.1016/j.jtho.2019.03.007
8. Zhou C, Kim SW, Reungwetwattana T, et al. Alectinib versus crizotinib in untreated Asian patients with anaplastic lymphoma kinase-positive non-small-cell lung cancer (ALESIA): a randomised phase 3 study. Lancet Respir Med. 2019;7(5):437–446. doi:10.1016/S2213-2600(19)30053-0
9. Zhou C, Lu Y, Kim S-W, et al. Alectinib (ALC) vs crizotinib (CRZ) in Asian patients (pts) with treatment-naïve advanced ALK+ non-small cell lung cancer (NSCLC): 5-year update from the phase III ALESIA study. Ann Oncol. 2022;33(suppl_9):S1560–S1597. doi:10.1016/annonc/annonc1134
10. Hsu JC, Jaminion F, Guerini E, et al. Pharmacometric analyses of alectinib to facilitate approval of the optimal dose for the first-line treatment of anaplastic lymphoma kinase-positive non-small cell lung cancer. CPT Pharmacomet Syst Pharmacol. 2021;10(11):1357–1370. doi:10.1002/psp4.12702
11. Ahn MJ, Kim HR, Yang JCH, et al. Efficacy and safety of brigatinib compared with crizotinib in Asian vs. non-Asian patients with locally advanced or metastatic ALK-Inhibitor-naive ALK+ non-small cell lung cancer: final results from the phase III ALTA-1L study. Clin Lung Cancer. 2022;23(8):720–730. doi:10.1016/j.cllc.2022.07.008
12. Shaw AT, Bauer TM, de Marinis F, et al. First-line lorlatinib or crizotinib in advanced ALK-positive lung cancer. N Engl J Med. 2020;383(21):2018–2029. doi:10.1056/NEJMoa2027187
13. Solomon BJ, Bauer TM, Mok TSK, et al. Efficacy and safety of first-line lorlatinib versus crizotinib in patients with advanced, ALK-positive non-small-cell lung cancer: updated analysis of data from the phase 3, randomised, open-label CROWN study. Lancet Respir Med. 2022;11:S2213–2600(22)00437–4. doi:10.1016/S2213-2600(22)00437-4
14. Zhou Q, Soo RA, Chang G-C, et al. Asian subgroup analysis of the randomized phase 3 CROWN study of first-line lorlatinib vs crizotinib in advanced ALK-positive non-small cell lung cancer. JTO Clin Res Rep. 2023;4:100499. doi:10.1016/j.jtocrr.2023.100499
15. Lu S, Zhou Q, Liu X, et al. Lorlatinib for previously treated ALK-positive advanced NSCLC: primary efficacy and safety from a phase 2 study in People’s Republic of China. J Thorac Oncol. 2022;17(6):816–826. doi:10.1016/j.jtho.2022.02.014
16. Soo RA, Huat Tan E, Hayashi H, et al. Efficacy and safety of lorlatinib in Asian and non-Asian patients with ALK-positive advanced non-small cell lung cancer: subgroup analysis of a global phase 2 trial. Lung Cancer. 2022;169:67–76. doi:10.1016/j.lungcan.2022.05.012
17. Nagasaka M, Ou SI. CROWN 2022 second interim updates: when will be the coronation of lorlatinib? J Thorac Oncol. 2022;2022:1.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.