")
Back to Journals » Open Access Surgery » Volume 16
Affinity of Colonic Granular Cell Tumor Within the Right Colon: Case Report and Review of Literature
Authors Aggarwal A, Joshi S, Bhullar JS
Received 30 August 2023
Accepted for publication 7 December 2023
Published 20 December 2023 Volume 2023:16 Pages 115—119
DOI https://doi.org/10.2147/OAS.S424597
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Luigi Bonavina
Video abstract of “Colonic Granular Cell Tumor within the Right Colon” [424597].
Views: 83
Arpit Aggarwal,1 Saakshi Joshi,2 Jasneet S Bhullar3
1Department of Graduate Medical Education-Colorectal Surgery, Ascension Providence Hospital-Michigan State University/College of Human Medicine, Southfield, MI, USA; 2Department of Graduate Medical Education- Internal Medicine, Department of Internal Medicine, Mclaren- Macomb, Macomb, MI, USA; 3Department of Colorectal Surgery, Ascension Providence Hospital-Michigan State University/College of Human Medicine, Southfield, MI, USA
Correspondence: Saakshi Joshi; Jasneet S Bhullar, Email [email protected]; [email protected]
Abstract: Granular cell tumors (GCTs) are uncommon neoplasms that occur in various organs, including the integumentary system, respiratory tract, and gastrointestinal tract. Colonic granular cell tumors are rare and account for less than 0.5% of soft tissue tumors. The gross endoscopic diagnosis of colonic tumors can be challenging due to their submucosal predominance, and advanced endoscopic techniques are necessary for diagnosis and management. We present a right-sided granular cell tumor resected en bloc during colonoscopy and hypothesize that colonic granular cell tumors have a higher affinity for the right colon. The aim of this paper is to review the literature on granular cell tumors of the colon and assess the clinical and pathological characteristics, diagnosis, and management of granular cell tumors of the colon.
Keywords: granular cell tumor, colon, submucosal, endoscopic mucosal resection, endoscopic submucosal dissection, case report
Introduction
Granular cell tumors (GCTs) are uncommon neoplasms deriving from Schwann cells and most predominantly presenting as small, mobile soft tissue nodules. These tumors can occur in various organs, including the integumentary system, respiratory tract, and gastrointestinal tract. Colonic granular cell tumors are rare and account for less than 0.5% of soft tissue tumors.1 They are usually benign, but a couple malignant cases have been reported. Endoscopically, granular cell tumors usually resemble common submucosal lesions, and their small size makes them impossible to classify with preoperative workup. We hypothesize that colonic granular cell tumors have a higher affinity for the right colon. The aim of this paper is to review the literature on granular cell tumors of the colon and assess the clinical and pathological characteristics, diagnosis, and management of granular cell tumors of the colon.
Materials and Methods
Clinical Presentation
A 69-year-old female with a history of hypertension and osteoarthritis presented for diagnostic colonoscopy after a positive cologuard. A well-prepped colonoscopy revealed a 15 mm well-circumscribed, firm, yellow-tinged, submucosal nodule with normal overlying mucosa within the cecum and grade II internal hemorrhoids. A single-piece hot-snare polypectomy was used for en-bloc resection, and clips were placed to close the defect. Pathological evaluation revealed healthy mucosa and submucosa with proliferation of polygonal to slightly spindled cells containing granular eosinophilic cytoplasm and minimal nuclear atypia. Subsequent immunohistochemical staining revealed positive staining for S100 and CD68, and negative staining for SMA, CD117, and DOG-1. A PAS-D stain was also positive. Morphological and staining characteristics were diagnostic of a granular cell tumor. The patient was recommended to undergo routine surveillance colonoscopy in 3 years. After discussing unique pathology, written informed consent to have case details published was granted by the patient. Institutional consent was not required to publish case details.
Review of Literature
Literature review from January 2000 to November 2022 was performed using the electronic database OVID Medline. Keywords used were: granular cell tumor, colonoscopy, colon, and rectum. Retrospective studies and case reports in English were assessed for applicability. Exclusion criteria included GCTs located outside the colon and rectum. Additional studies were included when appropriate. Prior colorectal GCT studies were evaluated for age, indication for colonoscopy, location within the colon, size, gross morphology, immunohistochemical staining, management, and recurrence. Studies that did not provide half of these categories were excluded.
Results
A total of 14 studies pooled a total of 155 patients with colonic granular cell tumors, most of which were found on routine screening colonoscopy (Table 1). Age ranged from 27 to 70 years old, with an overall higher incidence in males. Morphologically, the smallest lesion was a 2 mm pale sessile lesion, and the largest was 2.1 cm and submucosal. A total of 124 lesions were in the right colon, 7 in the transverse and descending colon, 3 in sigmoid, and 15 in rectum. Granular cell tumor was diagnosed on immunohistochemical presence of S100+. Other stains found in GCT are CD68, neuron-specific enolase, SCOX10, and PAS. Endoscopic management included snare, mucosal lift, submucosal biopsy, and submucosal resection, and recurrence was rare and seen with positive mucosal or submucosal margins. Although some authors cite malignant cases outside the gastrointestinal tract, in our review no mortality was found as a sequela of colonic granular cell tumor.
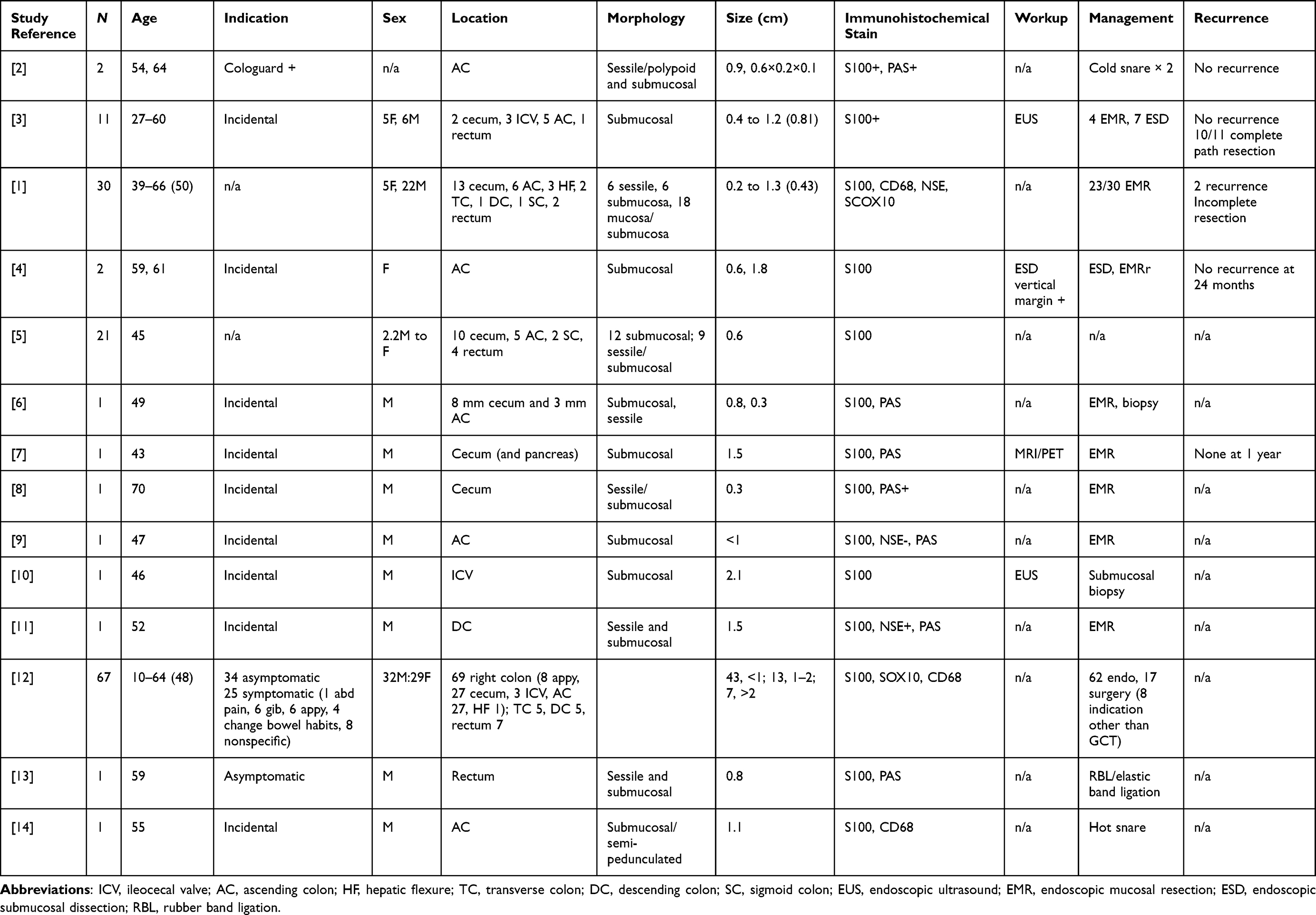 |
Table 1 Results |
Discussion
While the incidence of GCT is low, endoscopists should be aware of GCT in their differential diagnosis for submucosal lesions, especially in the right colon. GCT was originally named myoblastoma in 1926 by Abrikosoff and has since been called by various names, including granular cell glioblastoma, Abrikosoff’s tumor, and granulosa schwannoma.2 GCTs arise from Schwann cells, which form the myelin sheath that surrounds nerve fibers. The tumors are usually well-circumscribed and appear granular due to the accumulation of cytoplasmic granules.1 Histologically, the tumor cells are polygonal in shape, with eosinophilic cytoplasm containing small, uniform, round nuclei. A positive immunohistochemical staining for S100 protein confirms the neural origin of the tumor.5
In our study, colonic GCTs were found in adults between the ages of 27 and 70 and without any significant sex predominance. Pre-endoscopic diagnosis of GCT of the colon is challenging due to its small size, rarity, and nonspecific clinical features. Imaging studies such as computed tomography (CT) and magnetic resonance imaging (MRI) rarely help to identify the location and extent of the tumor. Given the small size of colonic GCT, endoscopic ultrasound is typically most helpful only within the rectum and to characterize previously localized submucosal lesions. However, it is not specific and cannot differentiate GCT from other types of colon tumors such as carcinoid or leiomyoma.5 Patients in our study were found to have incidental granular cell tumors during routine colonoscopy. Endoscopically, the tumor may appear as irregular surfaced sessile polyp if infiltrative, or as an encapsulated submucosal mass with smooth healthy mucosa. Hence, the overlying mucosa may be ulcerated if infiltrative or intact if encapsulated. The gold standard for diagnosis is immunohistological examination obtained with snare polypectomy, endoscopic mucosal resection, or endoscopic submucosal dissection. Immunohistochemical staining for S100 protein, CD68, and neuron-specific enolase confirms the diagnosis of GCT.5 Morphologically, tumor cells are arranged in nests, cords, or sheets and are separated by thin fibrous septa.1
Despite their predominantly benign nature, accurate recognition and application of advanced endoscopic techniques for submucosal lesions are necessary for the pathological diagnosis and management of GCT. Although GCTs are commonly benign lesions, malignant transformations are associated with a high risk of recurrence and mortality of 40%. Based on soft tissue GCT, the Fanburg-Smith histological criteria are used to characterize malignancy potential and include six histopathological elements: pleomorphism, high nuclear to cytoplasmic ratio, vesicular nuclei with prominent nuclei, necrosis, spindling, and mitotic activity greater than 2 mitoses/10 high-power field at 400× magnification. Benign GCT lesions only display focal pleomorphism, whereas atypical GCT include up to 2 of the 6 Fanburg-Smith elements. Histologically malignant GCTs are diagnosed when 3 more of the criteria are displayed.15 Given the poor outcomes associated with malignant transformation, it is necessary for endoscopists to safely resect these lesions and for pathologists to appropriately classify them.
Granular cell tumors of the colon occur in any part of the colon, but they seem to have a higher affinity for the right colon. Our study found 123/154 patients had right-sided lesions, followed by rectum, transverse, descending, and sigmoid colon. Several case reports have reported a higher incidence of these tumors in the right colon. Take et al retrospective study found 10 out of 11 patient with right sided granular cell tumors.3 The reason for predominance of these soft tissue tumors to the right is unclear, but it may be related to the neurological and/or embryological differences between the right and left colon. Furthermore, in our study the endoscopic management of these lesions included submucosal biopsy, snare resection without mucosal lift, endoscopic mucosal resection, and endoscopic submucosal resection. Risk factors for recurrence include positive margins and over three Fanburg-Smith histological features. Limitations in the study include various endoscopic techniques and nonstandardized histopathological evaluation of aggressive features. In clinical practice, endoscopists should be familiar with submucosal injection techniques like EMR and ESD, especially for lesions within the cecum due to their thinner caliber and elevated risk for perforation. Furthermore, the Fanburg-Smith criteria of aggressive features were determined through studies of granular cell tumor within the soft tissue structures such as subcutaneous tissue and deep musculature. Additional studies need to determine the applicability of these criteria to colonic lesions.
Conclusion
Granular cell tumors of the colon are rare benign neoplasms that are usually discovered incidentally during colonoscopy or surgery. The diagnosis of these tumors can be challenging, and advanced endoscopic techniques are critical in management of submucosal lesions. The preferred treatment of GCTs of the colon/rectum is endoscopic mucosal resection or submucosal dissection, and surgical resection is uncommon. The long-term outcomes of GCT of the colon are generally favorable, with a low risk of recurrence or metastasis. Further research is needed to investigate the affinity of granular cell tumor for the right colon, optimize techniques for endoscopic management, and characterize pathological features of colorectal-specific granular cell tumors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Na JI, Kim HJ, Jung JJ, et al. Granular cell tumours of the colorectum: histopathological and immunohistochemical evaluation of 30 cases. Histopathology. 2014;65(6):764–774. doi:10.1111/his.12487
2. Jobrack AD, Goel S, Cotlar AM. Granular cell tumor: report of 13 cases in a veterans administration hospital. Mil Med. 2018;183(9–10):e589–e593. doi:10.1093/milmed/usx237
3. Take I, Shi Q, Qi ZP, et al. Endoscopic resection of colorectal granular cell tumors. World J Gastroenterol. 2015;21(48):13542–13547. doi:10.3748/wjg.v21.i48.13542
4. Kahng DH, Kim GH, Park DY, et al. Endoscopic resection of granular cell tumors in the gastrointestinal tract: a single center experience. Surg Endosc. 2013;27(9):3228–3236. doi:10.1007/s00464-013-2899-2
5. An S, Jang J, Min K, et al. Granular cell tumor of the gastrointestinal tract: histologic and immunohistochemical analysis of 98 cases. Hum Pathol. 2015;46(6):813–819. doi:10.1016/j.humpath.2015.02.005
6. Schreiner P, Valli P, Marques Maggio E, et al. Simultaneous endoscopic full-thickness resection of two synchronous colonic granular cell tumoursCase Reports 2018. BMJ Case Reports. 2018;2018:bcr-2017–222223. doi:10.1136/bcr-2017-222223
7. Garces-Descovich A, Callery MP, Anderson KR, Poylin VY, Mortele KJ. Synchronous granular cell tumors of the pancreas and cecum. Clin Imaging. 2018;52:95–99. doi:10.1016/j.clinimag.2018.07.011
8. Dias E, Santos-Antunes J, Santos AL, Coelho R, Melo D, Macedo G. Colonic granular cell tumor identified in an adenomatous polyp. Gastroenterol Hepatol. 2022;45(Suppl 1):41–42. doi:10.1016/j.gastrohep.2020.12.005
9. Berzal Cantalejo MF, González Medina AR, Torío Sánchez B. Granular cell tumor of cecum. Rev Esp Enferm Dig. 2016;108(6):364–365.
10. Kozan P, Bencharit S, Issa D. Colonic granular cell tumor with ileocecal valve involvement. Clin Gastroenterol Hepatol. 2022;20(3):e351. doi:10.1016/j.cgh.2020.11.033
11. Ahmad HS, Mahamid M, Jawabreh Q, Khoury T, Mari A. Granular cell tumor of the colon: an exceptionally rare finding. Israel Med Assoc J. 2020;22(2):125–126.
12. Pagano N, Impellizzeri G, Di Simone MP, et al. Granular data: a rare submucosal tumor of the colon-case report and review of the literature. Dig Dis Sci. 2021;66(3):714–722. doi:10.1007/s10620-020-06753-x
13. Sevilla Ribota S, Pérez-Bedmar Delgado J, Domínguez Cañete JJ, Dotor de Lama AM, Gómez-Rubio M. Endoscopic resection of rectal granular-cell tumor using elastic band ligation. Rev Esp Enferm Dig. 2016;108(10):677–680. doi:10.17235/reed.2016.3823/2015
14. Dhruv S, Atodaria KP, Gurala D, El Imad T, Abergel J. Granular Cell Tumor of the Ascending Colon. Case Rep Gastroenterol. 2023;17(1):104–108. doi:10.1159/000529170
15. Fanburg-Smith JC, Meis-Kindblom JM, Fante R, Kindblom LG. Malignant granular cell tumor of soft tissue: diagnostic criteria and clinicopathologic correlation. Am J Surg Pathol. 1998;22(7):779–794. doi:10.1097/00000478-199807000-00001
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.