")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 17
Abrocitinib as a Novel Treatment for Multiple Skin Disorders: 3 Case Reports and a Scoping Review
Authors Chen P, Liang J, Li C, Li Q, Liu W, Zhu J, Chen W, Zhang X
Received 24 October 2023
Accepted for publication 28 November 2023
Published 6 January 2024 Volume 2024:17 Pages 35—40
DOI https://doi.org/10.2147/CCID.S446369
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Pingjiao Chen,1,* Jingyao Liang,2,3,* Changxing Li,1 Qian Li,2,3 Wenyan Liu,2,3 Junhui Zhu,2,3 Weifeng Chen,2,3 Xibao Zhang2,3
1Department of Dermatology, Nanfang Hospital, Southern Medical University, Guangzhou, 510515, People’s Republic of China; 2Institute of Dermatology, Guangzhou Medical University, Guangzhou, 510095, People’s Republic of China; 3Department of Dermatology, Guangzhou Institute of Dermatology, Guangzhou, 510095, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xibao Zhang, Department of Dermatology Guangzhou Institute of Dermatology, 56 Hengfu Road, Guangzhou, 510095, People’s Republic of China, Tel +8620-83593476, Email [email protected]
Abstract: Janus kinase (JAK) inhibitors are increasingly being used in dermatology due to their broad potential in managing both local and systemic inflammation. More recently, abrocitinib, an oral JAK 1 inhibitor, has shown promising clinical efficacy in the treatment of various skin disorders beyond moderate to severe atopic dermatitis (AD). We firstly presented three cases, each with diagnosis of pyoderma gangrenosum (PG), livedoid vasculopathy (LV), or hidradenitis suppurativa (HS), and conducted a comprehensive scoping review of the available literature on the use of abrocitinib in the treatment of diverse skin disorders. We summarized a total of 16 skin disorders, including our cases. The results indicated that abrocitinib, whether used as monotherapy or in combination with other treatments, was effective and well-tolerated in these disorders. These findings expanded the range of diseases for which abrocitinib may serve as an alternative therapeutic choice.
Keywords: JAK inhibitors, abrocitinib, atopic dermatitis, pyoderma gangrenosum, livedoid vasculopathy, hidradenitis suppurativa
Introduction
The Janus kinase (JAK) family is composed of four types of cytoplasmic tyrosine kinases: JAK1, JAK2, JAK3, and tyrosine kinase 2 (TYK2), which mediate signal transduction from cell surface receptors to the nucleus.1 The JAK pathways play a crucial role in response to over 50 inflammatory cytokines and are also involved in the differentiation of naive T cells into various types of immune cells, such as Th1, Th2, and Th17 cells.2 These processes are closely associated with the pathogenesis of a wide range of inflammatory immune-mediated diseases,3 making these conditions theoretically treatable by JAK inhibitors. Abrocitinib, inhibitor of JAK1, has recently shown promising results in the off-label treatment of some skin diseases associated with JAK activity, including alopecia areata (AA), and others.4,5 Herein, we present a case series comprising three patients, each diagnosed with pyoderma gangrenosum (PG), livedoid vasculopathy (LV), or hidradenitis suppurativa (HS). These patients exhibited a favorable response to abrocitinib following inadequate outcomes with conventional therapies. Furthermore, we conducted a scoping review to provide a comprehensive summary of the current evidence concerning the off-label use of abrocitinib in dermatologic disorders.
Case Report
Patient A, a 16-year-old male, was admitted with growing, painful, ulcerative lesions that started as erythematous papules in perianal area for over 1 year. Physical examination showed multiple, painful swollen, centrally located deep ulcerations with massive purulent discharges (Figure 1Aa). A skin biopsy revealed extensive infiltration of lymphocytes and neutrophils, increased vascular proliferation and dilation (Figure 1Ab), which was consistent with the diagnosis of PG. The patient was prescribed doxycycline, isotretinoin, glucocorticoids, and cyclosporine A, but his symptoms continued to worsen. We initiated treatment with oral abrocitinib (100 mg daily) in combination with cyclosporine A (50 mg twice daily). The patient showed gradual improvement of his symptoms within one week (Figure 1Ac), and almost complete resolution of painful swelling and purulent discharges, significant reduction of the ulcer area and depth after four weeks (Figure 1Ad). Cyclosporine A was discontinued due to the good clinical response, and the patient continued to improve without any adverse events (AEs) over the 16-week follow-up.
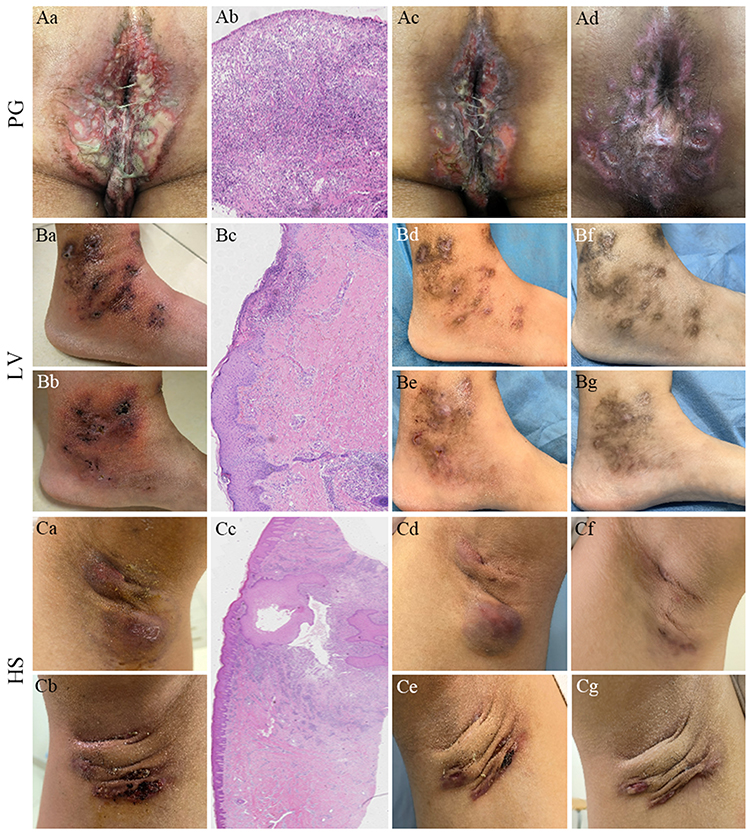 |
Figure 1 Patient (A) ulcerative lesions with massive purulent discharges in perianal area before abrocitinib treatment (Aa); extensive infiltration of lymphocytes and neutrophils and necrotising vasculitis (Ab, ×100); significant improvement of skin lesions 1 week after abrocitinib and cyclosporine A treatment (Ac) and 4 weeks after starting abrocitinib treatment (Ad). Patient (B) multiple ulcers and tan necrosis near both ankle joints (Ba, b); cellulose like degeneration of capillary wall, and vascular thrombosis and inflammation (Bc, ×100); markedly improvement of skin lesions 1 week (Bd, e) and 6 weeks (Bf, g) after abrocitinib treatment. Patient (C) nodules and abscesses of the axillary (Ca, b); hyperplasia of the hair follicle infundibulum epithelium and infiltration of lymphocyte (Cc, ×40); improvement of skin lesions 2 weeks after abrocitinib and doxycycline treatment (Cd, e) and 6 weeks after starting abrocitinib treatment (Cf, g). |
Patient B, a 31-year-old female, presented with more than 2-year history of multiple recurrent erythematous papules that had gradually progressed to open ulcers and tan necrosis, causing significant pain near both ankle joints (Figure 1Ba and Bb). The patient has been diagnosed with LV and had received unsuccessful treatments with various drugs in multiple hospitals. The diagnosis was confirmed based on our histopathological findings (Figure 1Bc). The patient received abrocitinib at a daily dose of 100 mg orally. Within one week of treatment, the patient reported a rapid improvement in painful swelling, inflammation, and ulceration (Figure 1Bd and Be). Complete remission was achieved after six weeks, with only post-inflammatory hyperpigmentation remaining on the previous lesions (Figure 1Bf and Bg). Abrocitinib was then tapered to 100 mg once every two days, with no reported recurrence or AEs during the 12-week follow-up period.
Patient C, a 17-year-old male, was referred with 3-year history of recurrent abscesses with pain in both armpits (Figure 1Ca and Cb). His condition did not respond to glucocorticoids, doxycycline, retinoic acid, cyclosporine A, and methotrexate. Due to the ineffectiveness of traditional medicines, the patient was recommended to undergo three surgical in the past two years. However, the skin lesions continued to appear, even on the excision site. Histopathological examination found hyperplasia of the hair follicle infundibulum epithelium, perifollicular infiltration of lymphocytes in the dermis (Figure 1Cc). The patient was diagnosed with HS and started on abrocitinib (100 mg daily) in combination with doxycycline (100 mg twice daily). The pain and the size of abscesses decreased significantly after two weeks (Figure 1Cd and Ce). Doxycycline treatment was then discontinued. Six weeks after starting abrocitinib treatment, the lesions continued to improve, with nearly complete clearance (Figure 1Cf and Cg). Abrocitinib was reduced to 100 mg once every two days, and the patient remained lesion-free within the 10-week follow-up period.
Discussion
In recent years, JAK inhibitors have been increasingly used in the treatment of various dermatologic disorders owing to their oral administration, favorable safety, and tolerability.2 We conducted a scoping review to summarize the literature on the treatment of abrocitinib for skin disorders, excluding AD, using PubMed database before September 1, 2023. We identified 14 articles,1–14 all of which were case reports. The total number of articles, including the present study, reached 15 (Table 1). Abrocitinib was utilized off-label for the treatment of 16 skin disorders (28 cases). These mainly include lichen sclerosus (10 cases),4 AA (5 cases),3,5–7 and lichenoid amyloidosis (2 cases).1 Additionally, other treated conditions encompassed eruptive pruritic papular porokeratosis,8 Hailey-Hailey disease,9 necrobiosis lipoidica,10 occupational airborne allergic contact dermatitis,2 Netherton syndrome,11 oral lichen planus,12 nipple and areola eczema,13 prurigo nodularis,14 PG, LV, and HS, each presenting 1 case. Patients who had previously failed to respond to traditional medicines and/or biological agents (such as secukinumab and dupilumab) achieved substantial clinical improvement within a median of 12 weeks (range 3–96) after abrocitinib monotherapy or in combination with other medications.
 |
Table 1 Overview of Abrocitinib as a Novel Treatment for Various Skin Disorders Including Our Cases |
Several studies, including head-to-head trials, have shown that abrocitinib 200 mg once daily was superior to dupilumab (300 mg every 2 weeks after a loading dose of 600 mg), while abrocitinib 100 mg once daily produced a similar therapeutic response to dupilumab.15 Moreover, abrocitinib not only maintained or increased clinical benefits in patients with AD who had previously responded to dupilumab but also resulted in significant clinical enhancements among patients who had initially shown no response to dupilumab.15 Similarly, a patient with occupational airborne allergic contact dermatitis reported only minimal improvement during dupilumab treatment.2 Additionally, a patient with Netherton syndrome experienced a recurrence within a week of discontinuing dupilumab.11 Notably, both patients achieved rapid and complete remission after switching to abrocitinib treatment. AA, whether occurring alone,5 comorbid with AD,3,7 or induced by drugs6 that have failed to respond to other therapies, all showed significant improvement with abrocitinib treatment. In our cases, a patient with PG and another with HS achieved rapid remission after receiving abrocitinib in combination with traditional medicines, and this improvement persisted even after discontinuing the traditional medications.
The most common AEs of abrocitinib included headache, nausea, acne, dizziness, and upper respiratory tract infection that often self-resolved and did not require discontinuation of treatment in the majority of cases.15 However, few cases may have potentially serious AEs such as herpes zoster, thrombocytopenia, and thrombosis.15 Like its efficacy, the AEs of abrocitinib exhibited a dose-dependent relationship, with a higher incidence of AEs observed in patients receiving the 200 mg dose compared to those receiving the 100 mg dose.15 In this scoping review, 2 of 28 patients (7.1%) experienced mild common AEs while initiating treatment with abrocitinib 200 mg daily, but had no AEs when the dosage was tapered to 100 mg daily.10,11
Conclusion
This scoping review suggests that abrocitinib could be a novel, effective, and safe therapeutic option for various dermatological conditions. As the existing evidence is primarily based on case reports and case series, further studies are warranted to confirm and expand on these findings.
Consent Statement
Written informed consent has been respectively obtained from the parent of patient A, the patient B, and the parent of patient C for publication of this case report and the accompanying images. Institutional approval was not required to publish the case details.
Disclosure
The authors declare no conflict of interest.
References
1. Bai J, Su W, Fang H, Qiao J. Treatment of primary cutaneous lichenoid amyloidosis with abrocitinib: a pilot study in two cases. Int J Dermatol. 2023;62(9):e480–e483. doi:10.1111/ijd.16698
2. Baltazar D, Shinamoto SR, Hamann CP, Hamann D, Hamann CR. Occupational airborne allergic contact dermatitis to invasive Compositae species treated with abrocitinib: a case report. Contact Dermatitis. 2022;87(6):542–544. doi:10.1111/cod.14204
3. Zhao J, Liu L. A case of atopic dermatitis with alopecia universalis in a patient treated with abrocitinib. JAAD Case Rep. 2022;22:99–100. doi:10.1016/j.jdcr.2022.02.027
4. Bao C, Xu Q, Xiao Z, et al. Abrocitinib as a novel treatment for lichen sclerosus. Br J Dermatol. 2023;189(1):136–138. doi:10.1093/bjd/ljad129
5. Huang J, Liu O. Effective treatment of refractory alopecia areata in pediatric patients with oral abrocitinib. J Cosmet Dermatol. 2023. doi:10.1111/jocd.15896
6. Zhang J, Zuo YG. Successful treatment of alopecia universalis with abrocitinib: a case report. J DermatolTreat. 2023;34(1):2242706. doi:10.1080/09546634.2023.2242706
7. Bennett M, Moussa A, Sinclair R. Successful treatment of chronic severe alopecia areata with abrocitinib. Australas J Dermatol. 2022;63(2):274–276. doi:10.1111/ajd.13836
8. Xia J, Jiang G. A report of eruptive pruritic papular porokeratosis treated with abrocitinib. Clin Cosmet Invest Dermatol. 2023;16:2223–2227. doi:10.2147/CCID.S424310
9. Li Y, Jiang Y, Sun J. Improvement of Hailey-Hailey disease with abrocitinib. Clin Exp Dermatol. 2023;48(5):532–533. doi:10.1093/ced/llad023
10. Arnet L, Erfurt-Berge C. Effect of abrocitinib in a patient with extensive necrobiosis lipoidica. J Eur Acad Dermatol Venereol. 2023;37(10):e1208–e1210. doi:10.1111/jdv.19189
11. Zheng CC, Chen XX, Zou RT, Cai GY, Chen RY. Treatment of Netherton syndrome with abrocitinib. JAMA Dermatol. 2023;159(7):791–793. doi:10.1001/jamadermatol.2023.0561
12. Solimani F, Mesas-Fernandez A, Dilling A, et al. The Janus kinase 1 inhibitor abrocitinib for the treatment of oral lichen planus. J Eur Acad Dermatol Venereol. 2023. doi:10.1111/jdv.19069
13. Teng Y, Tang H, Yu Y, Fan Y, Tao X, Xu D. Successful treatment of atopic dermatitis with a predominant nipple involvement by abrocitinib during COVID-19 pandemic: a case report. J Asthma Allergy. 2023;16:789–792. doi:10.2147/JAA.S422836
14. Vander Does A, Yosipovitch G. Failure of dupilimab with severe prurigo nodularis that responded well to abrocitinib. Dermatitis. 2023. doi:10.1089/derm.2022.0065
15. Shi VY, Bhutani T, Fonacier L, et al. Phase 3 efficacy and safety of abrocitinib in adults with moderate-to-severe atopic dermatitis after switching from dupilumab (JADE EXTEND). J Am Acad Dermatol. 2022;87(2):351–358. doi:10.1016/j.jaad.2022.04.009
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.