")
Back to Journals » Patient Preference and Adherence » Volume 16
A Smart-Phone App for Fluid Balance Monitoring in Patients with Heart Failure: A Usability Study
Authors Shen Z, Zhang Y, Yang C, Liu J, Huang C, Zhang X, Zhang Y , Lin Y
Received 20 May 2022
Accepted for publication 26 July 2022
Published 2 August 2022 Volume 2022:16 Pages 1843—1853
DOI https://doi.org/10.2147/PPA.S373393
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Video abstract presented by Zhiyun Shen.
Views: 234
Zhiyun Shen,1,* Yaping Zhang,2,* Chun Yang,3 Jie Liu,3 Chenxu Huang,1 Xian Zhang,1 Yuxia Zhang,1 Ying Lin1
1Department of Nursing, Zhongshan Hospital, Fudan University, Shanghai, People’s Republic of China; 2Department of Emergency, Zhongshan Hospital, Fudan University, Shanghai, People’s Republic of China; 3Network Center, Zhongshan Hospital, Fudan University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yuxia Zhang; Ying Lin, Department of Nursing, Zhongshan Hospital, Fudan University, Shanghai, People’s Republic of China, Tel +86 21-64041990, Email [email protected]; [email protected]
Background: For a long time, fluid balance monitoring has been one of the most difficult problems in the management of patients with heart failure (HF). There is considerable interest in technology-facilitated fluid balance monitoring. However, little is known about patient acceptance and the use of mobile technology for fluid balance monitoring.
Objective: The aim of this study was to develop a mobile app for technology-facilitated fluid balance monitoring and to determine its usability.
Methods: A mixed-methods study was conducted in a tertiary hospital in Shanghai, China. A mobile app named I-Self-Care was developed through a best practice implementation project. Patients and nurses both completed the System Usability Scale (SUS, 0– 100) and participated in semistructured interviews.
Results: I-Self-Care includes patients’ daily fluid intake and output (I&O), symptoms, hospitalization, and diuretic records. It can automatically calculate food water content and perform real-time analysis of I&O. The average SUS scores were 81.74 (SD 5.44) among 36 patients and 80.80 (SD 13.26) among 28 nurses (scale 0– 100, with 100 being the best usability), which means that I-Self-Care has high usability for both patients and nurses. Semistructured interviews about the usability of the app were conducted with 17 participants. During the interviews, the patients expressed the high ease of use of I-Self-Care, their expectations for a continuously updated database, and improved self-management behaviour. The nurses thought that family support and repeated operation demonstrations were needed for patients to use the app. The nurses also expressed the convenience of this app for nursing work and the information security of patients.
Conclusion: With participant feedback, we confirmed the usability of I-Self-Care for fluid balance monitoring in patients with HF. Continuously updated databases, family support, repeated operation demonstrations, and information security are important for HF patients to use I-Self-Care.
Keywords: fluid balance monitoring, intake and output, mobile applications, telemedicine, heart failure
Introduction
Background
Volume overload is one of the most prominent characteristics of patients presenting with decompensated heart failure (HF), and it implies an unfavourable prognosis for HF patients.1–3 Fluid balance monitoring is therefore vital for patients with HF.4,5 Maintaining records of the patient’s fluid intake and output (I&O) has long been considered an essential component of nursing care to assess hydration status.6 It is also an important basis for doctors to formulate and adjust treatment strategies.7 However, for a long time, fluid balance monitoring has been the most difficult problem in the management of patients with HF.8 Among the issues in fluid monitoring, the most difficult is determining the amount of water in the food that is consumed by patients every day.9 At present, almost all patients with HF and medical staff still use paper recording and a subjective method of manual estimation to record I&O. When recording I&O, different people have different calculation rules. If there is an error, it will cause doctors to misjudge the patient’s condition and will have a significant impact on the patient’s prognosis. In addition, due to the cumbersome calculation process of I&O, most patients with HF often cannot keep records after discharge.9 At this time, medical staff cannot monitor the volume status of patients in real time after discharge, resulting in aggravation of the patients’ condition due to the failure to correct the volume imbalance in time, which is also an important reason for the repeated hospitalizations of most patients with HF.10
Based on the above situation, we should now consider whether there is a method to accurately, efficiently, and continuously record the I&O of patients with HF. Can the water in food be automatically calculated with the help of a smartphone app similar to apps that can calculate the calories in food? With this idea, our team innovatively developed a smartphone app named I-Self-Care that can automatically determine the water content in food and can realize the real-time recording and analysis of I&O in patients with HF. Therefore, the objective of this study was to heuristically evaluate the usability and participant experience of this newly developed smartphone app among patients with HF on fluid balance monitoring and nurses’ beliefs about the potential benefits of using this app.
Significance of This Study
This study has some advantages over other similar studies: it achieves the automatic calculation of water in food, which makes the fluid balance monitoring of patients with HF more convenient and sustainable. The convenient recording method provided by the I-Self-Care app can enable patients with HF to continuously carry out self-management of fluid balance monitoring, which is helpful to avoid rehospitalization and disease deterioration. This project can even be extended to all patients who need to maintain their fluid balance, such as patients with kidney diseases.
Methods
Study Setting and Designs
The study was conducted at a tertiary hospital in Shanghai, China, and was approved by the institutional review board at Zhongshan Hospital, Fudan University (ethics approval number: B2021-528). No changes were made to the design after the study was approved. We confirm that all the methods in this study were carried out in accordance with relevant guidelines and regulations at Zhongshan Hospital, Fudan University. Prior to data collection, all participants were informed of the purpose of this study, and signed written informed consent forms were obtained. All data were deidentified. Instead of using participants’ real names, we identified each interviewee with a unique number, such as 1, 2, or 3. All information therefore could be used in a way that would not disclose the participants’ identities. The participant’s written informed consent also included the publication of anonymized data. We explained these terms in the written informed consent for participants. We employed mixed research methods to conduct the usability study, including the collection of quantitative and qualitative data. Participants could indicate on the informed consent form whether they gave permission to be approached for the questionnaire survey, collection of app usage data, and a face-to-face interview. We followed the CONSORT EHEALTH (Electronic and Mobile Health Applications and Online Telehealth) checklist.11
Participants
To better evaluate the usability of I-Self-Care, we included both patients and nurses. The eligibility criteria of the patients included being aged 18 years or older, being diagnosed with HF, having the ability to understand and communicate in Chinese, having sufficient hearing and vision for compliance with the assessment that was required for fluid balance monitoring, and having access to a mobile phone with internet access. Patients suffering from other serious diseases (acute infection, malignant tumour, acute cerebrovascular diseases, delirium, terminal illness) or severe mental disorders were excluded. Registered nurses in the department of cardiology who engaged in clinical nursing work were included. Patient characteristics (age, gender, education status, marital status, and living conditions) and nurse characteristics (education status, years of work experience, years of experience working with the nursing information system) were collected to describe the sample.
Data Collection
Quantitative Data
A quantitative data questionnaire survey was used to collect quantitative data. The Chinese translation of the System Usability Scale (SUS) was used to assess the usability among all app users. The SUS is a reliable and valid 10-statement usability scale suitable to assess a wide range of eHealth technologies. The total SUS score ranges from 0 to 100, and higher scores reflect higher usability.12 A SUS score of at least 62.7 was considered acceptable,12 and 68 or above was regarded as above average in terms of usability quality.13 Participants completed the SUS two weeks after app use. In addition, with the help of our information technology team, we collected other usage data that reflected engagement with the app., eg, how many logins and any drop-outs from the app usage.
Qualitative Data
Semistructured face-to-face interviews were conducted to collect quantitative data with a selection of participants to gain more detailed insight into the usability of the app. The interviews took 20 to 30 minutes. During the interviews, sample questions were utilized (Multimedia Appendix 1). The interviews were conducted 2 or more days after using the app. The interviews were audio-recorded and transcribed to determine common themes. Once the audio files were transcribed, we utilized qualitative software to identify key concepts and themes. Participants were included until there was a maximum variation in the patient characteristics (age, gender, education status, living conditions, years of work experience, years of experience working with the nursing information system, and days of app use). Data saturation was reached with 9 consecutive interviews with patients and 8 consecutive interviews with nurses.
Development of I-Self-Care
The idea for this app originated from a best practice implementation project that used the JBI Practical Application of Clinical Evidence System. During the implementation of the project, we learned that the lack of standard methods for the calculation of water in food and intelligent recording methods for I&O are the main obstacles to fluid balance monitoring in patients with HF. Based on these findings, we began to think about whether daily fluid balance monitoring could be implemented by referring to apps for calculating food calories. To test this hypothesis, we first needed to determine the amount of water in each kind of food and then create a table The amount of water in each food was determined based on the relevant data in the Chinese Food Composition Tables published by Chinese nutritionists14 and the instruction manual of I&O of Zhongshan Hospital. Finally, a food water content table was established including 348 kinds of food. This table was then used as the database for our app. Based on this database, as long as the patient inputs the amount of food eaten every day, the app can automatically determine the amount of water the patient consumes. Therefore, this table is the core content of our whole app. The amount and type of fluid outflow by patients every day can be recorded in a customized way. At the same time, considering that symptoms and diuretic use are equally important for fluid balance monitoring in patients with HF, a function for the recording of symptoms and diuretics taken was also added to our app to carry out comprehensive volume management for patients with HF. In addition, I-Self-Care is equipped with a patient portal and a medical staff portal. Medical staff can view the data of patients anytime and anywhere, and they can also supplement some I&O data that the patient cannot fill in, such as intravenous rehydration and drainage. The features of the app enable patients to record their daily I&O, symptoms, hospitalization, and diuretic use. I-Self-Care also has an analysis and summary function for the patient’s 24-hour I&O, as well as a function for alerting patients of a fluid imbalance.
Multimedia Appendix 2 shows the user interfaces (UIs) of I-Self-Care. The UI of the app was codesigned by a graphic user interface (UI) designer, an information technology team, a research team, and users. First, the graphic UI designer and the research team conducted a group interview with users (5 patients with HF and 5 nurses) to clarify how to meet their needs and how to design functional modules. Second, based on the discussion results, the graphic UI designer made the draft drawing of the UI. Third, the research team and the graphic UI designer showed the draft drawing to the users to collect their suggestions on the colour, style, module settings, etc. Then, the graphic UI designer revised and confirmed the final draft. Last, the research team handed the draft drawing over to the information technology team for app development. After the app was developed, we contacted the users who had participated in the discussion again for user testing and made a total of 34 modifications according to the user experience. We did not release the app until everyone agreed, including the graphic UI designer, information technology staff, research team, and the users.
The final version of I-Self-Care includes a food-water content database, interaction module, and I&O conversion module. The interaction module is used to collect the user’s I&O information through the user interface. The I&O information includes the type and amount. The food water content database is used to store the unit water content of various types of food. The I&O conversion module is connected with the interaction module and the food water content database, matching the unit water content in the database based on the type of food and then determining the user’s I&O quantity through the amount. Through the interactive module, the I&O information is collected, and the I&O quantity is obtained by converting the I&O information based on the food water content database, which can automatically convert the water content of the food so that the user can conveniently record, count, and query the I&O quantity.
Data Analysis
Descriptive statistics were used to describe the patients’ characteristics and SUS scores. No a priori level of statistical significance was set, as this pilot study was not powered to assess the effect. Quantitative data were analysed using SPSS Statistics version 26.0 (IBM Corporation). Qualitative analysis of interview data was performed following the steps of thematic analysis: compiling, disassembling, reassembling, interpreting, and concluding.15,16 An iFLYTEK recording pen was used to record the interview and transcribe the video into text. Two researchers listened to the original video repeatedly and compared it with the text until the interviews were transcribed verbatim. Then, qualitative data were imported into NVivo for analysis. The data were coded through open coding. The axial coding was discussed by two researchers to define the definitive codes. Subsequently, the codes were put into context with each other to create themes. Differences were discussed until a consensus was reached. Next, analytical conclusions were made from the data presented as codes and themes. The main themes and findings regarding the usability of the app are described in the Results section, as an addition to the quantitative analysis of the usability.
Results
Participants’ Characteristics
From February 8, 2022, to March 31, 2022, we enrolled 36 patients and 28 nurses in the usability testing. Table 1 shows the details of the participant characteristics. The patients ranged in age from 23 to 84 years (mean 54.40 years). There were 23 males and 13 females. The education status included primary school and below (9/36, 25.00%), high school or vocational training (17/36, 47.22%), and college and above (10/36, 27.78%). Thirty patients were married. Thirty-five patents lived with families, and 1 patient lived alone. Among the 28 nurses, their education status included college (7/28, 25.00%), undergraduate (19/28, 67.86%), and postgraduate (2/28, 7.14%). There were 2 nurses who had worked for less than 2 years, 7 nurses who had worked for 2–5 years, 7 nurses who had worked for 6–10 years and 12 nurses who had worked for 11–20 years. There were 10 nurses with less than 5 years of experience working with the nursing information system.
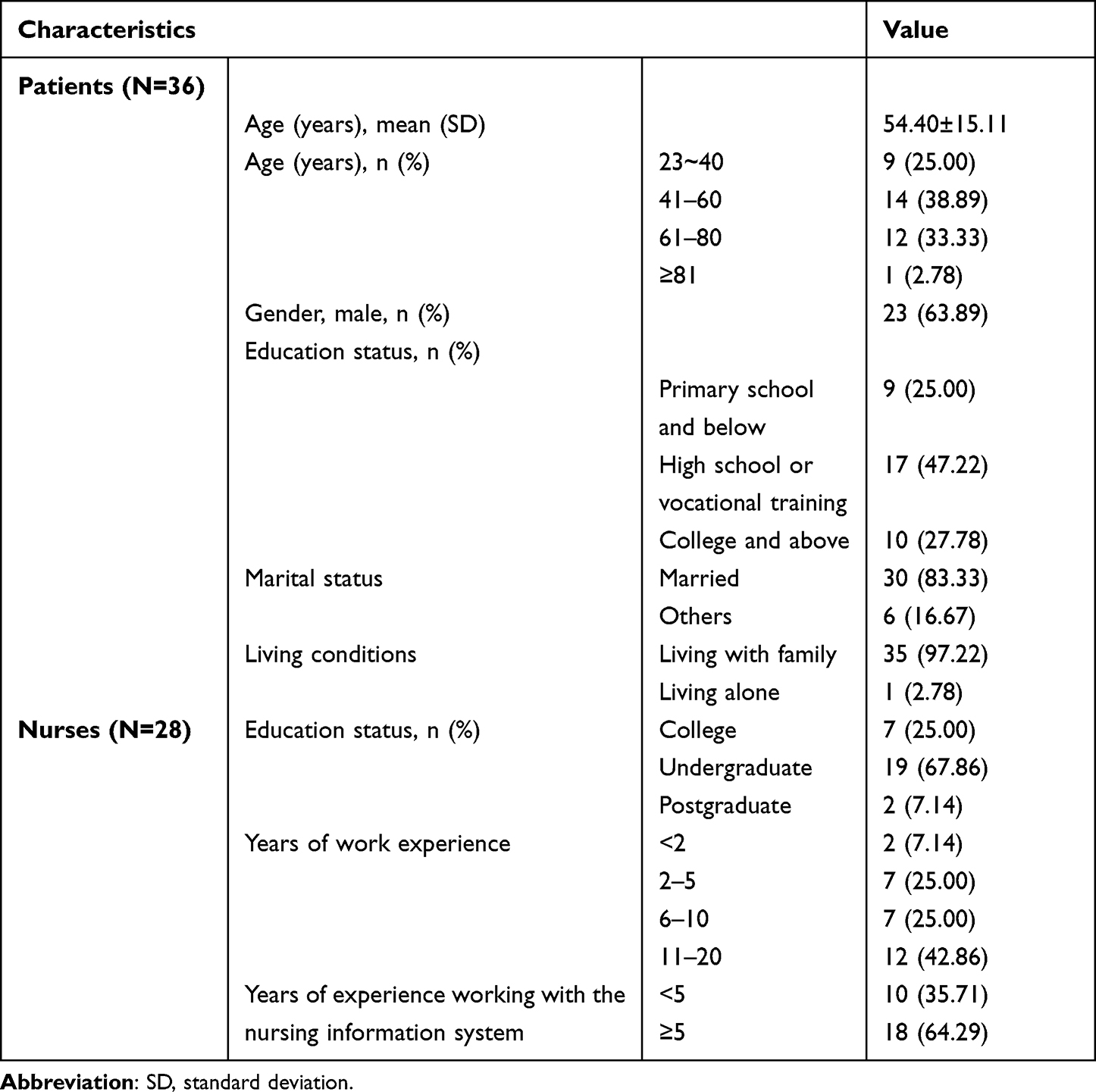 |
Table 1 Participant Characteristics |
Usability
Quantitative results
Interviewees
The SUS was completed by 36 patients and 28 nurses, and the response rate was 100%. The usability of the I-Self-Care app for the patients scored 81.74 (SD 5.44). The mean SUS scores per usability aspect were as follows: satisfaction, 85.76 (SD 11.73); learnability, 80.32 (SD 9.99); and efficiency, 77.78 (SD 8.68). Figure 1 shows the SUS scores for each statement and usability aspect in the patients. The usability of the I-Self-Care app in nurses scored 80.80 (SD 13.26). The mean SUS scores per usability aspect were as follow: satisfaction, 83.00 (SD 17.00); efficiency, 80.36 (SD 12.04); and learnability, 78.27 (SD 18.19). Figure 2 shows the SUS scores for each statement and usability aspect in the nurses.
 |
Figure 1 System Usability Scale scores for each statement and usability aspect in the patients (higher scores reflect higher usability). |
 |
Figure 2 System Usability Scale scores for each statement and usability aspect in the nurses (higher scores reflect higher usability). |
App Usage
Among the 36 patients surveyed, 2 patients (5.56%) did not log in and record every day within 1 month after the first registration (recording days per week ≤ 5 days) and no longer used the app. Twenty-nine patients (80.56%) kept records almost every day since their first registration (recording days per week ≥6 days). Five patients (13.89%) kept records almost every day for 30 days after the first registration (recording days per week ≥6 days) but showed intermittent records after 1 month (recording days per week ≤ 5 days). In addition, at present, using the app to record the I&O has become routine nursing practice in the Department of Cardiology in our hospital, so the usage rate of the app among nurses was high.
Qualitative Results
Interviewees
Of the participants, 25% (9/36) of the patients and 28.57% (8/28) of the nurses were approached for a face-to-face interview. After 9 interviews of patients and 8 interviews of nurses, data saturation was reached. Table 2 presents the characteristics of the interviewees. After axial coding, 7 themes were formed. The qualitative results are described for each theme.
 |
Table 2 Characteristics of the Interviewees |
Themes Based on the Patients’ Results
Ease of Use of the App
The log-in procedure was easy for many interviewees, and the interviewees did not experience problems when using the app.
Under the detailed and patient guidance of the nurse, I can easily learn to log in and use this app. Male, Age 70.
At first, I always forgot my medical record number, so I could not log in. Later, the nurse told me that the app had a login memory function for my account and password, so I can log in easily. Male, Age 58.
My family used this app for me; they said it was easy to use. Female, Age 84.
Continuously Updated Database
The database of the app should be continuously updated based on the data customized by the patients.
I hope the app will have a memory function, which can remember my customized food and directly generate options next time, which is convenient for me to record. Male, Age 23.
The customization function in the app is very important because the database does not include all kinds of food and all types of water output.
This program already contains almost all kinds of food. However, I sometimes cannot find some kind of foods in the app, so I wish I could customize it. Male, Age 23.
Improving Self-Management
Push notifications that target behaviours can remind patients to record their fluid I&O, symptoms and diuretics every day.
Sometimes I forget to record in the app, but the app will send me a reminder, and then I remember it. Female, Age 73.
After the app sends the reminder, the medical staff should give the patient related health education by telephone or internet in time.
After receiving the abnormal warning reminder from the app, I was very nervous due to the fear that my condition would deteriorate. Male, Age 65.
Themes Based on the Nurses’ Results
Need for Family Support
Most patients with HF and their families are willing to use this app, and some elderly patients may need family help.
When the patients were admitted to the hospital, I introduced the app to them, and they were very willing to use it. Nurse, Code 1.
Some elderly patients may not be able to operate the app independently and need to invite their families to participate in the operation. Nurse, Code 4.
The families of patients with HF are willing to use the app. Nurse, Code 2.
Need for Repeated Operation Demonstrations
Patients and family members may need consecutive demonstrations to master the application method of the app.
Generally, they (patients and their families) need continuous education for 1–2 days and 2–3 times a day before they can thoroughly master the use of this app. Nurse, Code 7.
At the time of discharge, patients and their families can learn how to use this app. Nurse, Code 6.
Compared with the operation manual, patients and family members may prefer our on-site explanation and demonstration to show them. Nurse, Code 5.
Improvement of the Workflow Efficiency of Nursing Work
The app allows nurses not to go to the patient’s bedside each time but to remotely see the amount of fluid I&O and the symptoms recorded by patients, as well as the corresponding situation after discharge.
It is very convenient. I can see the fluid intake and outflow of patients at the nurse desk. Nurse, Code 6.
I can also see the situation of the patients after discharge, which makes it convenient for me to give them comprehensive guidance in the joint medical clinic of HF. Nurse, Code 5.
The customized function of the app allows me to correct the data at any time and to supplement some data, such as with intravenous rehydration and drainage flow. Nurse, Code 7.
The summary data in the app make it convenient for me to write medical records. I do not have to manually calculate the fluid intake and outflow one by one or input them into the computer as before. Nurse, Code 2.
Information Security of Patients
The technicians of the hospital should ensure the information security of patients.
This app is associated with the hospital’s information system, so technicians should take rigorous measures to ensure the patient’s information security, but I think this app is relatively safe. At present, I have not found anything that can threaten the patient’s information security. Nurse, Code 7.
Discussion
The primary aim of this study was to investigate the usability of I-Self-Care in patients with HF. Both quantitative and qualitative data support the usability of the app and provide insight into adjustments that can be made to improve the app. Data from the SUS showed that both the patients and nurses thought that the I-Self-Care had acceptable usability (mean 81.74 [SD 5.44] in patients, mean 80.80 [SD 13.26] in nurses). A SUS score of at least 62.7 was considered acceptable,12 and 68 or above was regarded as above average in terms of usability quality.13 The app scored the best on the aspect of satisfaction. Data on app usage suggested that most patients wanted to stay logged into I-Self-Care and that most completed records almost every day since their first registration. This result encourages us to continue to promote this app. Furthermore, the satisfaction with the app is supported by our qualitative findings, as the majority of the interviewees showed that participants liked to use the app. In addition, we found that there were some differences in the scores of learnability and efficiency between the patients and nurses. Among the patients, the learnability score was greater than that the efficiency score, while in the nurse population, the efficiency score was greater than the learnability score. Under the detailed guidance of nurses, patients can quickly learn how to use the app. However, nurses should not only learn how to use the app by themselves but also learn how to teach patients how to use the app so that their learnability scores are low. However, for both nurses and patients, the total SUS scores were higher than 68, which is significantly higher than the average score. Therefore, the results suggest that compared to paper recording and the subjective method of manual estimation to record patient I&O, the app provides a more intelligent, convenient, and continuous method of volume balance monitoring for patients with HF with the help of mobile information technology. Moreover, the SUS score and the data on app usage show that this idea and method is feasible.
Combined with the qualitative results, we found that patients prefer the database to be continuously updated to cover all foods they consume in their daily lives. The reminder function of the app can improve their self-management behaviour and keep them in the habit of continuously recording information. At the same time, elderly patients may need the support and help of their families. This is consistent with previous studies.17,18 A review17 on the state of the art of research and development in smart home-based remote healthcare technologies for elderly individuals also reported that family members play an important role for elderly individuals participating in smart home-based remote healthcare technology programs. From the perspective of nurses, repeated operation demonstrations are necessary to ensure that patients with HF learn to use the app. Physicians’ recommendations and adequate training have also been reported to be facilitators of mHealth adoption in older adults with HF.19 In addition, nurses also pointed out that the I-Self-Care app can make fluid balance monitoring of patients with HF more convenient. However, nurses have also expressed concern that information security is still an important topic. With the wide application of information technology in the field of health care, health care is becoming increasingly convenient, but information security is still an important issue.20–22 Ensuring patient information security is the premise and necessary condition for carrying out health care based on information technology. The qualitative results told us which aspects of user experience we should pay attention to in the future to further optimize and promote the application of mobile information technology in the volume balance monitoring of patients with HF.
To our knowledge, this is the first study to achieve the automatic calculation of water in food, which greatly facilitates the fluid balance monitoring of patients with HF. At the same time, the app also includes a record of the patient’s symptoms, hospitalization and diuretics, which helps patients, families, and medical staff know the situation of the patient anytime and anywhere. Restricting fluid is a common recommendation for patients with HF and has long been recommended for patients with HF in the guidelines.3,23 There is also a clinical guideline regarding fluid restrictions for the Chinese population.24 However, most references on fluid restrictions in the guidelines are based on expert consensus. There have been only a few randomized trials that can provide high-quality evidence for fluid restriction in patients with HF and for the development of guidelines. Therefore, some questions have been raised. For example, we still do not know whether patients with volume overload should restrict their fluid intake to 1.5–2 L a day or should restrict it according to the patient’s weight. Due to the lack of large sample research, the answer to this question is still unknown. With the help of the I&O records, symptom records, hospitalization records, and diuretic records in I-Self-Care, a large database can be formed to analyse what kind of fluid restriction strategy is the most suitable strategy for patients with volume overload. Based on this, the app has considerable application prospects and value. Additionally, the app can be extended to all patients who need fluid balance management, such as patients with kidney disease and patients after cardiac surgery.
Limitations
This study is only a usability study and does not further explore the effectiveness of the app in improving the symptoms and outcomes of patients with HF. In addition, a health education module was not included in the app. However, the patients did not express their needs in this regard during their qualitative interviews. If the patients need health education in the future, we can add a health education module to the app. We also acknowledge that the screen time monitoring function was not set, so screen time data cannot be obtained to reflect engagement with the app. Finally, the app has been online for one year now. After a period of time, new functions need to be updated to meet the needs of patients and clinical nurses. However, we firmly believe that our efforts and improvements will make this app more accessible.
Conclusions
Overall, the results of this study demonstrate that the I-Self-Care app has potential in terms of usability for patients with HF. The app seems to fit the needs of patients with HF to conduct fluid balance monitoring. This suggests that in the future, we can use this concept for more intelligent fluid balance monitoring in patients with HF. Several points of improvement for the app have also been identified, which supports the further development of the I-Self-Care app. These include the adaptation of custom functions, continuous database updates, additional support by family members, and information security of patients.
Abbreviations
HF, heart failure; I&O, intake and output; SUS, System Usability Scale; SD, standard deviation.
Acknowledgments
We thank all the volunteers who participated in this research. The authors disclose the receipt of the following financial support for the research, authorship, and/or publication of this article: this study was supported by the Fuxing Nursing Research Fund of Fudan University (FNF201935), the National Key R&D Program of China (2020YFC2008100), and the Cardiovascular Disease Nursing Program of Zhongshan Hospital, Fudan University (xk-082-011).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. Equal contribution: Zhiyun Shen and Yaping Zhang should be considered joint first authors.
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. Albert NM. Fluid management strategies in heart failure. Crit Care Nurse. 2012;32(2):
2. Costanzo MR. The cardiorenal syndrome in heart failure. Heart Fail Clin. 2020;16(1):81–97. PubMed PMID: 31735318. doi:10.1016/j.hfc.2019.08.010
3. McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42(36):3599–3726. PubMed PMID: 34447992. doi:10.1093/eurheartj/ehab368
4. Sindelić R, Vlajković G, Davidović L, Marković D, Marković M. Perioperative fluid balance in patients with heart failure. Lijec Vjesn. 2010;132 Suppl 1:13–18. PubMed PMID: 20715712.
5. Ronco C, Kaushik M, Valle R, Aspromonte N, Peacock W. Diagnosis and management of fluid overload in heart failure and cardio-renal syndrome: the “5B” approach. Semin Nephrol. 2012;32(1):129–141. PubMed PMID: 22365171. doi:10.1016/j.semnephrol.2011.11.016
6. Yang SH, Mu PF, Wu HL, Curia M. Fluid balance monitoring in congestive heart failure patients in hospital: a best practice implementation project. JBI Database System Rev Implement Rep. 2019;17(10):2202–2211. PubMed PMID: 31464851. doi:10.11124/jbisrir-2017-004021
7. Miller WL. Fluid volume overload and congestion in heart failure: time to reconsider pathophysiology and how volume is assessed. Circ Heart Fail. 2016;9(8):e002922. PubMed PMID: 27436837. doi:10.1161/circheartfailure.115.002922
8. Tuy T, Peacock W. Fluid overload assessment and management in heart failure patients. Semin Nephrol. 2012;32(1):112–120. PubMed PMID: 22365169. doi:10.1016/j.semnephrol.2011.11.014
9. Philipson H, Ekman I, Forslund HB, Swedberg K, Schaufelberger M. Salt and fluid restriction is effective in patients with chronic heart failure. Eur J Heart Fail. 2013;15(11):1304–1310. PubMed PMID: 23787719. doi:10.1093/eurjhf/hft097
10. Fujimoto W, Konishi A, Iwasaki M, et al. Precipitating factors and clinical impact of early rehospitalization for heart failure in patients with heart failure in Awaji Island, Japan. J Cardiol. 2021;77(6):645–651. PubMed PMID: 33419613. doi: 10.1016/j.jjcc.2020.12.014
11. Eysenbach G. CONSORT-EHEALTH: improving and standardizing evaluation reports of Web-based and mobile health interventions. J Med Internet Res. 2011;13(4):e126. PubMed PMID: 22209829; PubMed Central PMCID: PMC3278112. doi:10.2196/jmir.1923
12. Brooke J. A “Quick and Dirty” Usability Scale. Boca Raton: CRC Press; 1996.
13. Usability.gov. System Usability Scale (SUS). Available from: https://www.usability.gov/how-to-and-tools/methods/system-usability-scale.html.
14. Yang Y. China Food Composition. Beijing, China: Peking University Medical Press; 2018.
15. Castleberry A, Nolen A. Thematic analysis of qualitative research data: is it as easy as it sounds? Curr Pharm Teach Learn. 2018;10(6):807–815. PubMed PMID: 30025784. doi:10.1016/j.cptl.2018.03.019
16. Malterud K. Qualitative research: standards, challenges, and guidelines. Lancet. 2001;358(9280):483–488. PubMed PMID: 11513933. doi:10.1016/s0140-6736(01)05627-6
17. Majumder S, Aghayi E, Noferesti M, et al. Smart homes for elderly healthcare-recent advances and research challenges. Sensors. 2017;17(11):2496. PubMed PMID: 29088123; PubMed Central PMCID: PMC5712846. doi:10.3390/s17112496
18. Engelsma T, Jaspers MWM, Peute LW. Considerate mHealth design for older adults with Alzheimer’s disease and related dementias (ADRD): a scoping review on usability barriers and design suggestions. Int J Med Inform. 2021;152:104494. PubMed PMID: 34015657. doi:10.1016/j.ijmedinf.2021.104494
19. Cajita MI, Hodgson NA, Lam KW, Yoo S, Han HR. Facilitators of and barriers to mHealth adoption in older adults with heart failure. Comput Inform Nurs. 2018;36(8):376–382. PubMed PMID: 29742549; PubMed Central PMCID: PMC6086749. doi:10.1097/cin.0000000000000442
20. Moghbeli F, Langarizadeh M, Aliabadi A. Application of ethics for providing telemedicine services and information technology. Med Arch. 2017;71(5):351–355. PubMed PMID: 29284905; PubMed Central PMCID: PMC5723167. doi:10.5455/medarh.2017.71.351-355
21. Alessa T, Hawley MS, Hock ES, de Witte L. Smartphone apps to support self-management of hypertension: review and content analysis. JMIR mHealth UHealth. 2019;7(5):e13645. PubMed PMID: 31140434; PubMed Central PMCID: PMC6658295. doi:10.2196/13645
22. Dehling T, Gao F, Schneider S, Sunyaev A. Exploring the far side of mobile health: information security and privacy of mobile health apps on iOS and android. JMIR mHealth UHealth. 2015;3(1):e8. PubMed PMID: 25599627; PubMed Central PMCID: PMC4319144. doi:10.2196/mhealth.3672
23. Heidenreich PA, Bozkurt B, Aguilar D, et al. AHA/ACC/HFSA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Joint Committee on clinical practice guidelines. Circulation. 2022. PubMed PMID: 35363499. doi:10.1161/cir.0000000000001063
24. Heart Failure Group CB, Chinese Medical Association, Heart Failure Professional Committee of Chinese Medical Doctor Association, Editorial Board of Chinese Journal of Cardiovascular Disease. China heart failure diagnosis and treatment guidelines 2018. Chinese J Cardiol. 2018;46(10):760–789. doi:10.3760/cma.j.issn.0253-3758.2018.10.004
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.