")
Back to Journals » Drug Design, Development and Therapy » Volume 18
A Review of Dupilumab in the Treatment of Atopic Dermatitis in Infants and Children
Authors Wang M, Gao XH, Zhang L
Received 4 January 2024
Accepted for publication 18 March 2024
Published 27 March 2024 Volume 2024:18 Pages 941—951
DOI https://doi.org/10.2147/DDDT.S457761
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Georgios Panos
Mingyue Wang,1– 4 Xing-Hua Gao,1– 4 Li Zhang1
1Department of Dermatology, the First Hospital of China Medical University, Shenyang, 110001, People’s Republic of China; 2NHC Key Laboratory of Immunodermatology, China Medical University, Shenyang, People’s Republic of China; 3Key Laboratory of Immunodermatology, China Medical University, Ministry of Education, Shenyang, People’s Republic of China; 4National and Local Joint Engineering Research Center of Immunodermatological Theranostics, Shenyang, People’s Republic of China
Correspondence: Li Zhang, Department of Dermatology, the First Hospital of China Medical University, Shenyang, 110001, People’s Republic of China, Email [email protected]
Abstract: Atopic dermatitis (AD), a common pruritic and chronic inflammatory skin disease, has a major impact on a patient’s quality of life. It is characterized by dry, itchy, and eczema-like rashes. AD is more prevalent in young children and has been linked to a variety of other allergy disorders. Traditional drug therapy has certain limitations for treating young children with AD. However, biologics have good clinical application prospects in the medical treatment of young patients. Dupilumab, a fully human monoclonal antibody, specifically binds to the IL-4 Rα subunit, inhibiting IL-4 and IL-13 signaling and blocking the occurrence of type 2 inflammatory response. It has a good effect on treating infants and children with moderate-to-severe AD. This review explores the safety and efficacy of dupilumab in the treatment of AD in infants and children and the impact of early intervention on AD progression, with the aim of informing clinical practice in the use of dupilumab for the treatment of young patients with AD.
Keywords: atopic dermatitis, dupilumab, infant, child, treatment
Introduction
Atopic dermatitis (AD), a common chronic inflammatory skin disease, is characterized by recurrent eczematous lesions and intense itching. AD can occur at any age, with most cases starting in infancy or childhood, becoming more common in children aged 3–6 months, and developing in adulthood. The prevalence of AD is currently increasing globally in all age groups, ranging from 2.7% to 20.1% in children in different countries.1–4
The pathogenesis of AD is significantly influenced by genetic factors. Mutations in filaggrin (FLG) impair the functioning of epidermal barriers, which is manifested by increased transepidermal water loss (TWEL), increased contact with allergens, and adherence and colonization by S. aureus. In addition, damaged skin barriers make them susceptible to excessive immune-inflammatory responses, which can induce itchy skin.5–7 The immune-inflammatory response is the central key to the pathogenesis of AD, which is mainly characterized by the production of specific IgE antibodies by Th2 cells and B cells. Damage to the lipid membranes of the skin caused by low expression of FLG and loricrin (LOR) also facilitates the penetration of antigens, allergens, and pollutants into the stratum corneum of the skin, damaging the epidermal barrier. Alarmins released from this disruption of the epidermal barrier, such as IL-25, IL-33, and thymic stromal lymphopoietin (TSLP), activate the type 2 innate lymphoid cells (ILC2s) and dendritic cells (DCs) and ILC2s, causing them to produce IL-5 and IL-13, which in turn activate Th2 cells and eosinophils. Th2 cells that are activated release IL-4 and IL-13, which stimulate B cell IgE class switching and generate IgE specific to antigens through transcription activator and signal transduction pathways. When external antigens and allergens come into interaction with IgE on the mast cell surface, mast cell degranulation releases histamine to trigger itching.8–10 Although genetic and immunological factors are important in the development of atopic dermatitis, the role of environmental factors cannot be ignored as the global prevalence of the disease increases. Lifestyle changes, climate change, and allergenic stimuli may all contribute to the development of AD. In addition, AD is often associated with other atopic disorders, such as food allergies, asthma, and allergic rhinitis. These atopic comorbidities, with the sequential development from infancy through adolescence, typically begin with AD. This phenomenon is defined as atopic march, which reflects the sequential progression of different allergic diseases and the temporal relationship of the natural history of the disease. Mechanisms of the atopic march may be related to the circulating spread of inflammatory factors and specific IGE production.11–15
Due to the particularity of infants and children, a high body surface area to body weight ratio may cause the skin to absorb medications more readily, and the use of traditional systemic medications may raise the possibility of harmful systemic reactions, safe and effective biological therapies are increasingly being used as targeted medications to treat patients with AD. A fully human monoclonal antibody called dupilumab binds to the shared subunit of the IL-4 and IL-13 receptor complex and antagonizes the IL-4 receptor α subunit. Consequently, the downstream transmission of signals from Th2 cytokines IL-4 and IL-13 is blocked, and type 2 inflammation is downregulated.16–18 Dupilumab has been shown to rapidly improve pruritus and rash, with a marked improvement in clinical signs and symptoms observed in the first 4 weeks of treatment.19 It also has a good efficacy and safety profile in the treatment of AD patients with comorbidities, in addition to improving their quality of life and physical and mental health. A 36-month real-world study demonstrated that dupilumab showed similar efficacy and safety in patients with and without comorbidities and had a positive effect on the treatment of patients with comorbidities.20 In a three-year psychological study, dupilumab was observed to reduce anxiety and depression in patients while improving symptoms of the disease. It was worth noting that it was more pronounced in patients with early onset of AD, whereas psychological improvement was not as pronounced in patients with adult onset of AD. This may suggest a greater benefit of using dupilumab in the early stages of pathogenesis. Early and consistent use of dupilumab improves patients’ physical and mental health while reducing itching and improving skin lesions, resulting in improved quality of life and sustained benefits for patients.21
The US Food and Drug Administration (FDA) authorized dupilumab in May 2020 for the treatment of moderate-to-severe AD in children older than six years. Soon, dupilumab became the first biologic to be approved for the treatment of moderate-to-severe AD in infants and adults in June 2022, when its age of adaptation was increased from 6 months to 5 years. The expansion of the applicable age group of dupilumab offers a younger age group of children with AD a safe as well as effective therapy, and its applicability is expected to cover the whole age group.
Mechanisms of Dupilumab
Dupilumab, a monoclonal antibody to human immunoglobulin G4 that binds human immunoglobulin G4, is the first approved targeted biological therapy for the treatment of moderate to severe AD in children, infants, and adults. The cytokines IL-4 and IL-13 are essential to the pathophysiology of AD. The formation of T-cell-mediated humoral immune responses, linked to allergies and asthma, is facilitated by the important cytokines IL-4 and IL-13, which function by combining various co-receptors.22,23 IL-4 has two types of receptors: IL-4R, a type I receptor that binds only IL-4, and a type II receptor that binds both IL-4 and IL-13. Each receptor has two chains: the type II receptor-specific IL-13Rα1 chain, the type I receptor-specific γ-c chain, and the IL-4Rα chain for type I and type II receptors. When IL-4 or IL-13 binds to the receptor, it triggers the transphosphorylation and activation of receptor subunit-associated Janus family protein kinases, including Janus kinase (JAK) 1, JAK 3, and TYK 2 associated with IL-4 R α, γ-c, and IL-13 R α1 chains, respectively. JAK activation initiates a cascade of phosphorylation of specific tyrosine residues in the cytoplasmic structural domain of IL-4 R α. This results in different signaling pathways, such as signal transducer and activator of transcription (STAT) 6, STAT 3. By attaching itself to the IL-4Rα subunit, dupilumab inhibits the downstream signaling of IL-4 and IL-13, which attenuates the inflammatory and immunological response (Figure 1).17,18,24
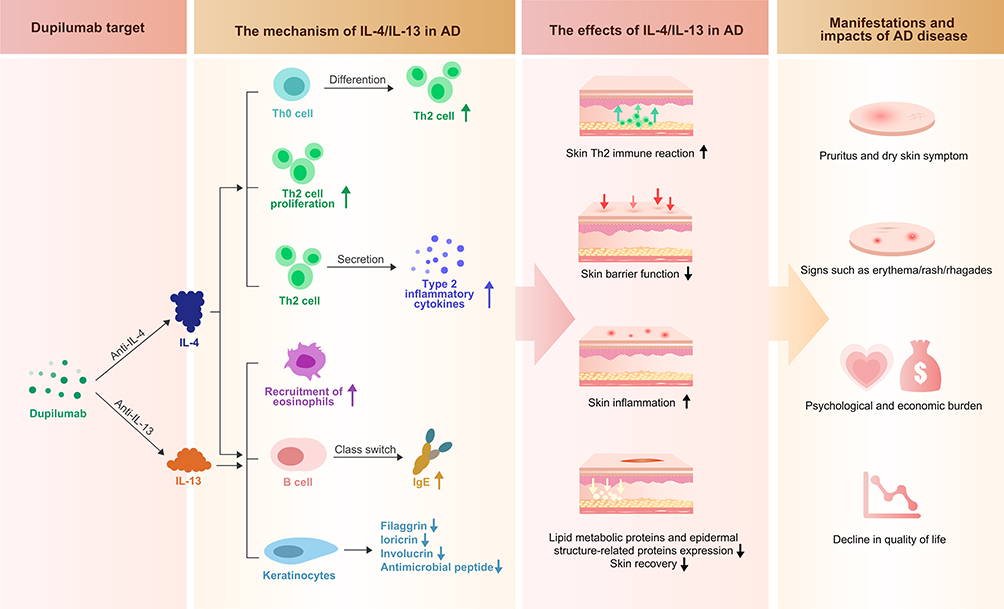 |
Figure 1 Mechanism of dupilumab. IL-4 and IL-13 can activate the type 2 inflammatory pathway, promote the conversion of Th0 to Th2, promote the proliferation and secretion of inflammatory cytokines by Th2 cells, recruit eosinophils, cause the conversion of B-cell antibody classes, as well as the under-expression of filaggrin and loricrin, involucrin, and reduce the secretion of antimicrobial peptide. By inhibiting the type 2 inflammatory pathway, dupilumab inhibits the downstream transmission of IL-4 and IL-13, reduces the inflammatory response of the skin, improves the epithelial dysfunction and lipid abnormality, promotes the expression of lipid metabolic proteins and epidermal structure-related proteins, relieves itchy and dry skin and reduces eczema, alleviates the physical and mental health of AD patients, reduces their financial burden, and improves the quality of life of the patients. |
Dupilumab can play a role in regulating skin barrier structure and function, inhibition of IL-4/IL-13 signaling by dupilumab restores skin lipid composition, barrier function, improving the microbiome, and reducing Staphylococcus aureus colonization in those with mild to severe AD. Silvia et al25 conducted a prospective study that enrolled 78 patients with severe adult AD and measured TWEL in the anterior elbow fossa at baseline, week 4, week 16, and week 32. The study’s findings showed that 4 months of therapy with dupilumab significantly improved the TEWL in lesional area and also the skin barrier function in non-lesional area, which was in parallel with the dupilumab-induced Eczema Area and Severity Index (EASI) reduction. Evgeny et al26 conducted a 16-week clinical trial enrolling 52 subjects. AD patients were injected with dupilumab subcutaneously on day 1 and at weeks 2, 4, 6, 8, 10, 12, and 14 with a loading dose of 600 mg, followed by a dose of 300 mg or a loading dose of 400 mg, and a follow-up dose of 200 mg (body weight < 60kg). The primary key study endpoint, TEWL AUC10, and other key study endpoints showed a significant improvement from baseline at Day 15 that persisted through week 16 (p<0.0001) and a significant improvement in the stratum corneum of the lesion area’s ceramide composition of AD subjects treated with dupilumab over a 4-week period (p<0.001). The findings suggest that dupilumab treatment significantly reduces TEWL in AD patients’ skin, lengthens the chain of fatty acids, and encourages the restoration of the lipid composition of the skin in AD patients’ lesional and non-lesional skin. Chris Callewaert et al examined bacterial DNA in swabs taken from lesional and non-lesional skin in a double-blind, placebo-controlled study. Pre-treatment lesional skin had less microbial diversity and more Staphylococcus aureus overall than non-lesional skin. In contrast, during dupilumab treatment, there was a decrease in S. aureus abundance and an increase in microbial diversity. The skin, both lesional and non-lesional, showed significant changes.27 The number of S. aureus was significantly reduced by dupilumab treatment compared to placebo after only 3 days, which was 11 days earlier than clinical improvement, according to a randomized, double-blind, controlled trial by Eric L. Simpson et al. The best clinical outcome was observed in patients with the greatest reduction in S. aureus.28 In a clinical investigation with microbiologic relevance, Jan Hartmann et al examined skin swabs from 157 patients for 16S rRNA gene amplicon sequencing both before and after they had a three-month course of treatment with dupilumab or cyclosporine.29 A possible impact of IL-4Rα blocking on the microbiome is suggested by the findings, which show that systemic therapy with dupilumab rather than cyclosporine tends to rebuild a healthy skin microbiome, mainly independent of clinical response. These studies suggest that microbiome and skin barrier function have been beneficially affected by biologics that target IL-4 and IL-13.
Efficacy and Safety of Dupilumab
Dupilumab Significantly Improves Clinical Scores in AD Patients
Three 16-week Phase III clinical trial studies (LIBERTY AD PRESCHOOL, LIBERTY AD PEDS, and LIBERTY AD ADOL) explored dupilumab’s efficacy and safety in AD patients in different age groups, the first two focusing on the infants and children AD patients using dupilumab in combination with topical corticosteroids (TCS), and the latter focusing on the adolescent AD patients using dupilumab as monotherapy. Each of the three trials utilized different doses of dupilumab based on the age and corresponding body weight of the AD patients(Table 1).
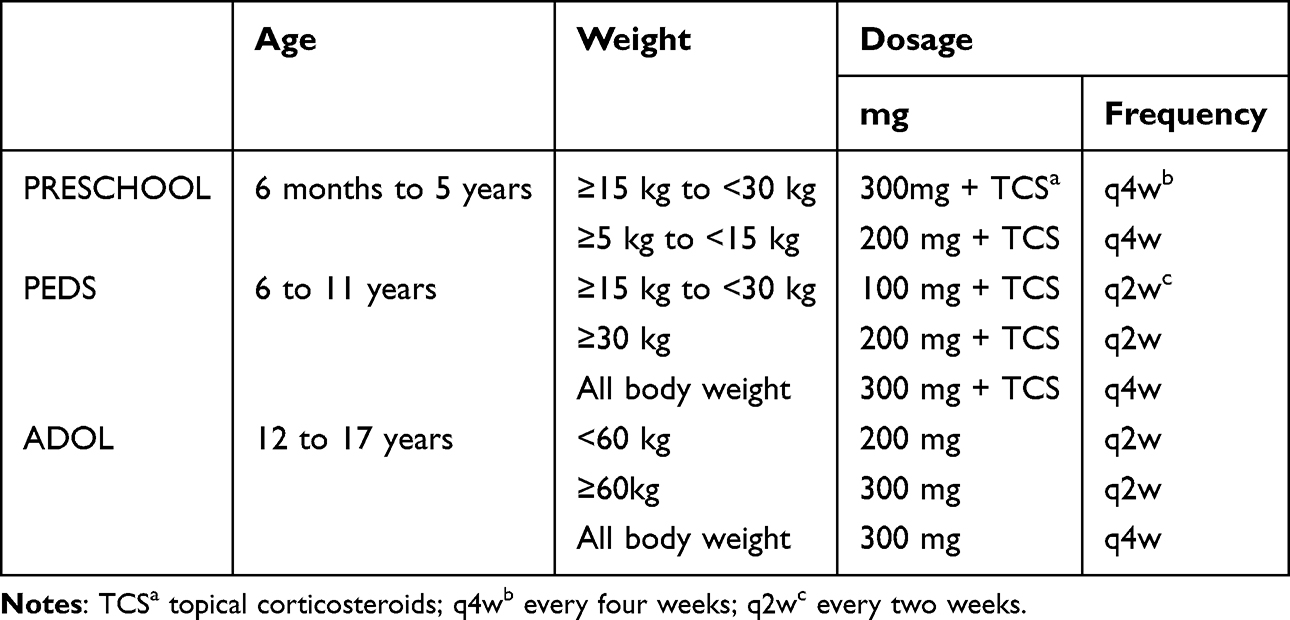 |
Table 1 Dosing Regimens for Phase III Clinical Trials |
According to the experimental results from phase III trials, at week 16, the dupilumab treatment group significantly improved the primary efficacy endpoints, IGA 0/1 and EASI-75, as well as secondary endpoints, EASI-50 and EASI-90, compared with placebo(Table 2).30–32 Thus, dupilumab significantly improved the signs, symptoms, and life quality of infants, children, and adolescents with AD, realizing the full benefits. It also confirmed the efficacy and tolerability of dupilumab monotherapy or in combination with TCS treatment, and the combination of drugs is more effective than monotherapy efficacy. In both PRESCHOOL and PEDS, the response rate to achieve the primary efficacy endpoints IGA 0/1 and EASI-75 and the secondary efficacy endpoints EASI-50 and EASI-90 was higher than that of the ADOL trial group. The results of PRESCHOOL suggest that early, aggressive intervention may be able to change the atopic march and reduce the risk of developing or the likelihood of severity of other atopic disorders, some of which are labeled indications for dupilumab treatment, more data is required to confirm the importance of early intervention in AD. This is now thought to be related to the acute and chronic manifestations of the disease lesions and the immuno-inflammatory mechanisms behind them. AD is characterized by acute episodes in infancy and early childhood, while with age the lesions gradually become chronic. Acute-phase AD lesions are dominated by Th2 cytokines, while chronic-phase is dominated by TH1 and Th22. Dupilumab, which inhibits the Th2 immune-inflammatory response, is more efficacious in treating AD in infants and young children with an acute exacerbation.33,34
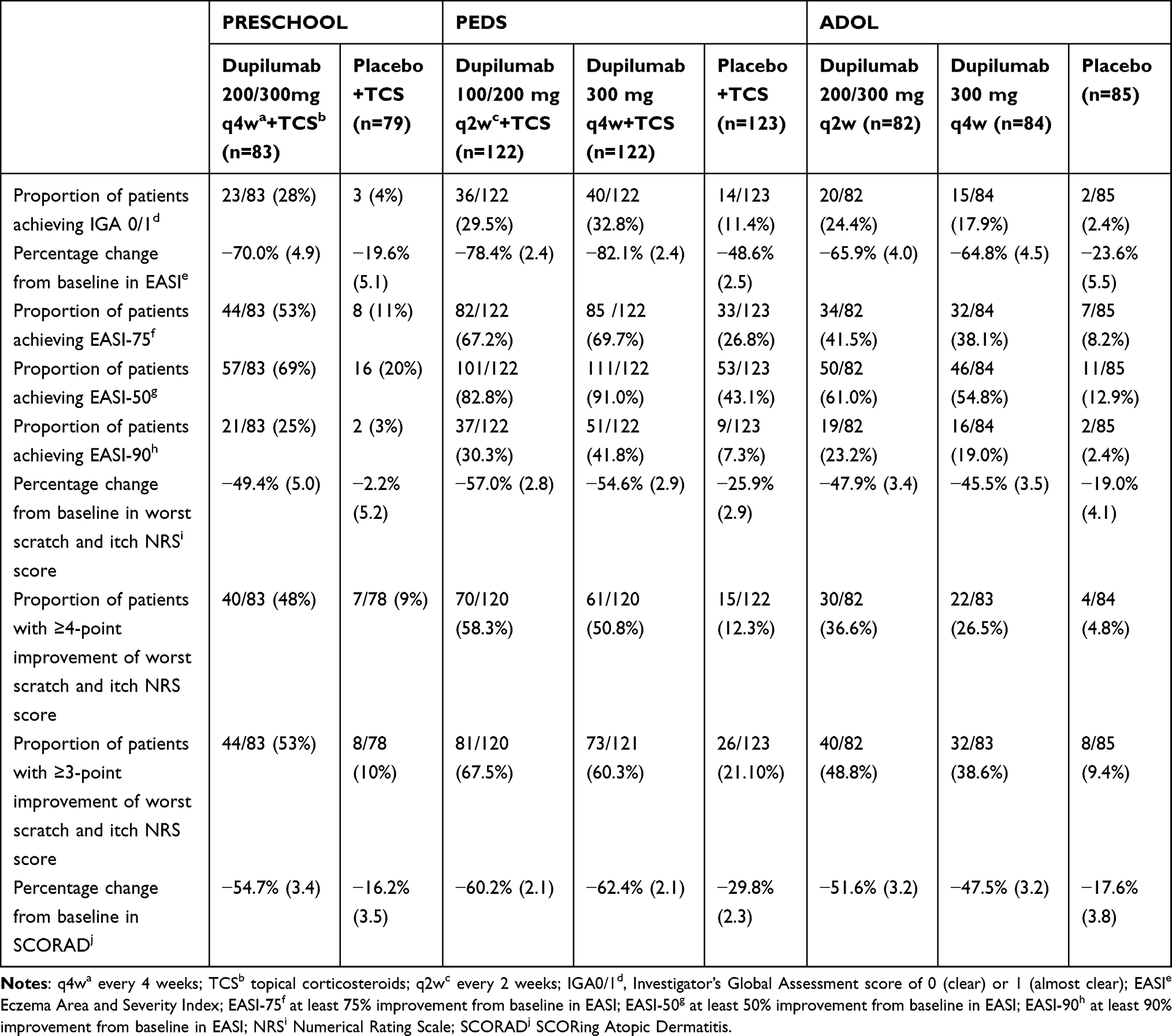 |
Table 2 Efficacy Outcomes in Patients with Moderate-to-Severe AD at Week 16 |
Compared to phase III clinical trials, dupilumab-treatment of AD patients of different ages has shown good efficacy in real-world studies as well. A 16-week multicentre study evaluating the efficacy of dupilumab in adolescents aged 6-11 years, which included 55 children, observed significant improvements in EASI, NRS, and Children’s Dermatology Life Quality Index (CDLQI) scores compared to baseline. In addition, the study observed that the proportion of patients achieving EASI-75 at week 16 was 74.54%, with significant improvement in EASI by week 4 and NRS and CDLQI by week 2. These results suggest that dupilumab has good efficacy in rapidly improving disease status in adolescent patients.35 A total of 155 AD patients were enrolled in a real-world study from China and were separated based on age into three groups (<6 years old group, 6 to 11 years old group, >11 years old group). Mean scores of SCORAD, EASI, Pruritus-NRS, Sleep-NRS, and BSA decreased significantly from baseline to 16 weeks in all three age groups. Furthermore, in patients <6 years of age, by the second week of treatment, 69.6% of patients who received the high loading dose had improved by at least 4 points from baseline in Pruritus-NRS, compared with only 23.5% of patients who received the standard loading dose. In addition, the percentage change in SCORAD, EASI and Sleep NRS, as well as the proportions of IGA0/1, EASI-75 and EASI-50 were significantly lower in the group receiving a high-loading dosage, compared to the standard loading dose group. Another real-world study, which included 120 AD patients aged 2-12 years, also found that there was a significant improvement in IGA, EASI and SCORAD from baseline to week 16. In the first four weeks, patients aged 2-6 years had higher efficacy with dupilumab than those aged 6-12 years, while at week 16, efficacy was similar in both groups. The researchers speculated that this may be related to loading dose/weight.36,37 Long-term efficacy of dupilumab was also confirmed in real-world studies. In a multicentre, retrospective real-world study, a total of 91 patients aged 6-11 years completed 52 weeks of treatment, and compared to baseline, patients showed significant decreases in EASI scores, CDLQI scores, and NRS scores, in addition to the proportion of patients who achieved EASI50, EASI-75, and EASI-90, which was 95.6%, 86.8%, and 42.9%, respectively.38 Another 24-week single centre retrospective study enrolled 48 adolescents patients (aged ≥12 years), 27 of these patients were treated for 24 weeks. It also confirmed that dupilumab showed highly significant improvements in EASI scores and NRS scores.39 Although the sample size was limited, these study demonstrated the efficacy of dupilumab for long-term sustained improvement from week 16 to week 52 and complemented the phase III clinical trials described above. Furthermore, there was no reported serious adverse events, the common adverse events were injection site reactions and conjunctivitis.38,39
According to these results, dupilumab is safe, efficient, and well-tolerated in children of all ages, and that increasing the loading dose can help to rapidly control the signs and symptoms as well as significantly improve patients’ quality of life. This demonstrates dupilumab’s efficacy in clinical applications, but dupilumab’s optimal dosage and long-term safety in infants and children need to be further investigated.
Common Adverse to Treatment with Dupilumab
Dupilumab has been shown in many clinical trials to be safe and effective in treating AD in children, with a low risk of side effects. Overall adverse reaction rate comparable to placebo, no need for experimental testing and monitoring for organ toxicity. It was confirmed in a clinical trial evaluating the efficacy and safety of dupilumab in a special group of people with serious diseases (patients affected by malignancy, patients with acquired immunodeficiency syndrome, patients who have received organ transplants, and patients with severe renal failure, etc.). The study results showed that dupilumab’s side effects and adverse event rates were similar in patients with severe disease, and in the control group, the common adverse events were injection site reactions and conjunctivitis. In addition, by early detection of adverse reactions in patients, discontinuation of dupilumab can be avoided. Adverse reactions that have occurred during dupilumab treatment include: injection site reactions, eosinophilia, eczema of the head and neck, rosacea, psoriasis, ocular complications (dry eye, conjunctivitis, blepharitis, keratitis, and ocular pruritis), arthritis, alopecia, and serosurge-like reactions.40–43
In the PRESCHOOL and PEDS phase III trials, most adverse events were reported at a higher rate in the placebo group than in the dupilumab group, whlie the incidence of treatment-emergent adverse events was similar across treatment groups in ADOL. In addition, the incidence of adverse reactions was higher with dupilumab q2w dosing group than with dupilumab q4w dosing group in PEDS and ADOL. Few patients of dupilumab group discontinued study treatment due to serious adverse effects, and no deaths occurred during the study period, with a low incidence of adverse effects and a satisfactory safety profile, comparable to outcomes in adults. The common adverse events in PRECHOOL and PEDS were exacerbation of atopic dermatitis, nasopharyngitis, upper respiratory tract infection, and asthma. In ADOL, however, the more common adverse effects were exacerbation of atopic dermatitis and skin infections. Notably, in all studies, the incidence of skin infections was reduced by half compared to placebo-treated subjects, which may reflect improved skin integrity and response to organisms. Additionally, in the three phase III trials, the group receiving dupilumab had a greater incidence of conjunctivitis than the group receiving a placebo(Table 3).33 Ashish et al evaluated three phase III trials (LIBERTY AD ADOL, LIBERTY AD PED-OLE, and LIBERTY ASTHMA QUEST). In the clinical trial of dupilumab for the treatment of moderate-to-severe AD in adolescents, the incidence of conjunctivitis was higher in individuals receiving dupilumab than in patients receiving a placebo, while the incidence of conjunctivitis was lower and similar in the clinical trial of dupilumab and placebo for the treatment of moderate-to-severe uncontrolled asthma in adolescents, supporting the hypothesis of a drug-disease interaction.44
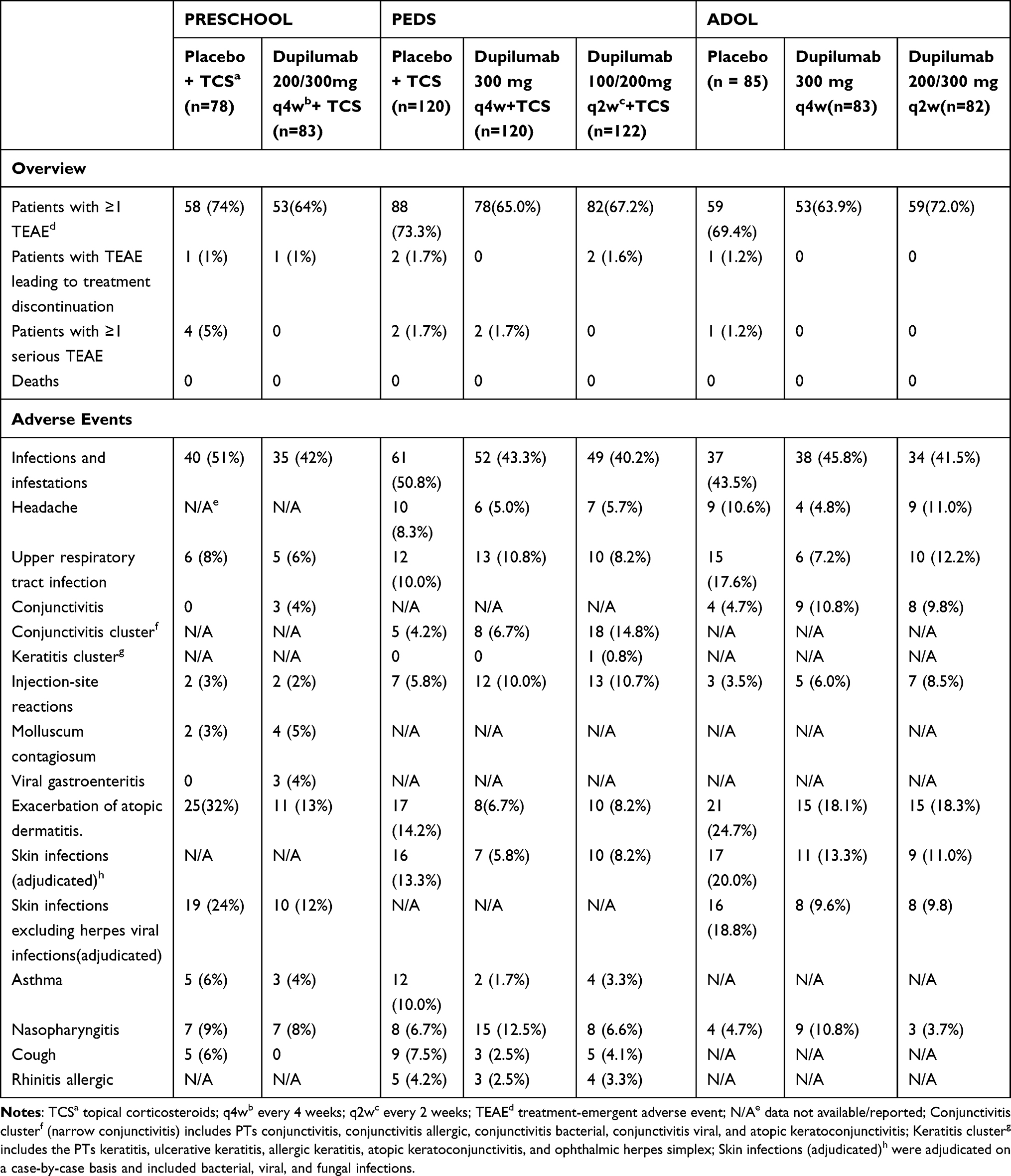 |
Table 3 Safety Outcomes in Patients with Moderate-to-Severe AD at Week 16 |
In conclusion, AD and dupilumab are associated with the development of ocular complications such as conjunctivitis, the etiology and pathogenesis of which are unclear. A variety of hypotheses have been put forward as to the underlying mechanisms for the increased incidence of conjunctivitis in AD patients treated with dupilumab, including the impact of IL-4 and IL-13 in inhibiting reduced expression of cuprocyte mucin, the interaction of dupilumab with AD, epithelial-barrier dysfunction and the increased incidence of helminth mites, and further studies are ongoing.44–46 A research trial exploring how the Th2 signaling pathway affects allergic conjunctivitis (AC) suggests that patients’ clinical symptoms of AC are reduced when the Th2 signaling pathway is blocked. The adverse effects of conjunctivitis observed in the clinical trial using dupilumab treatment may be attributable to either insufficient inhibition of IL-4Rα or to the alternate pathway through which Th2 inflammation is activated.47,48
Dupilumab Reduces Patients’ Disease Burden and Improve Quality of Life
Atopic dermatitis has a profound effect on the patient’s quality of life, and its chronic and recurrent nature increases the financial burden on the patient’s family. In infants and younger pediatric patients, the effect of sleep quality on the lives of patients is particularly critical, reduced sleep quality will cause anxiety, depression, and other symptoms, affecting the growth and development of infants and young children and children’s social functioning, and significantly reducing learning and work efficiency.49–51
Dupilumab can significantly improve the sleep and life quality, and effectively reduce the pain of the disease caused by itching. Real-world research and phase III clinical trials have shown that, compared to the placebo group, dupilumab significantly improved NRS scores and Quality of Life (QoL)-related scores.30–32,36,52–54 In addition, pediatric patients treated with dupilumab had good adherence and dosing persistence, which is consistent with adult results. In the 52-week open-label extension study (LIBERTY AD PED-OLE), patient adherence and medication persistence were good, with 253 of 294 patients continuing to be treated and only 11 patients dropping out of the trial due to lack of efficacy. However, there is fewer data on the long-term use of dupilumab in young patients, further research is needed on adherence and medication persistence in infants and young children.55,56 In conclusion, dupilumab is able to bring all-around improvement to patients, bringing a new therapy option for infants and children with AD, but many families are deterred from using dupilumab due to the high cost of the treatment. Marita Zimmermann et al conducted a cost-utility analysis of dupilumab, which showed that patients receiving dupilumab treatment were expected to have a lifetime cost of $509,600, which included $267,800 for the dupilumab drug and $241,800 for other medical expenses.57
Discussion and Conclusion
The treatment of AD has always been a hot and difficult issue in the treatment of non-fatal skin diseases. For special populations such as infants and children, traditional topical drug therapy and systemic drug therapy have certain limitations. With the understanding and deepening of the pathogenesis of AD, the wide application of biologics provides safer and more potent therapeutic alternatives for children with moderate to severe AD. As the first targeted drug approved for the treatment of moderate-to-severe AD in infants and children aged 6 months to 5 years, clinical trials have demonstrated the safety and efficacy of dupilumab.30 The above trials in this review demonstrated that dupilumab improved AD signs and symptoms rapidly and consistently, which is safe and well tolerated in all age groups. In addition, dupilumab has a low risk of adverse events, and few patients discontinue treatment. However, because of the recent approval of the age-range extension of the indication for dupilumab, it has not yet been widely used in children aged 6 months to 5 years, and in the real world, there is not enough observational data on its efficacy.
Previously, Yumiko Miyaji et al found that early aggressive topical corticosteroid treatment to shorten the duration of infantile eczema was significantly associated with a reduction in food allergies (FAs) later in life. This suggests the importance of early intervention in slowing down the development of atopic processes and subsequent other related type II inflammatory diseases, but it is not clear which of the time of onset and duration of eczema is more closely related to the development of FA.58 Dupilumab’s long-term clinical trials for the treatment of AD in children and infants may further elucidate the correlation between time of onset and duration and type 2 inflammatory diseases. Nevertheless, there are fewer data from long-term studies of adherence and persistence in pediatric patients receiving dupilumab, with studies focusing on the adult portion of the study. A meta-analysis of atopic march also showed that dupilumab-treatment group reduced new or worsening allergic events and changed the IgE category, effectively attenuating the atopic march compared to the placebo group. In addition, subgroup analyses revealed greater benefit of dupilumab in patients <18 years of age, those with early AD onset <2 years of age, and those with more severe AD at baseline. Patients with a past history of asthma and allergic disease were treated more effectively than those without such a history. Thus, targeted therapies with biologics targeting the Th2 cytokines IL4 and IL-13 possess the capacity to slow the onset of atopic co-morbidities and may be more effective in infancy and early childhood.59
Head and neck lesions are common in both infants and adults. In both adult and infant populations, dupilumab improved lesions at all anatomical sites and many patients with dermatitis of the face and neck improved significantly with dupilumab. In addition, similar improvements of the head and neck region as elsewhere have been observed in children and adolescents.42,60–62 However, in clinical practice, some patients have responded that dupilumab is not as effective in treating the face and neck as the trunk and extremities. In such cases, combinations may increase efficacy, but the safety of combinations on the face in infants and children is also a matter of concern. Further studies are needed on the safety and effectiveness of dubilumab in AD patients at different sites.
Furthermore, AD is not a single disease. There is limited clinical data about the possible effect of dupilumab on the atopic march. Therefore, additional enrollment will be needed to evaluate the durability of the potential effects of treatment with dupilumab for the atopic march. Finally, more in-depth studies on the safety as well as efficacy of dupilumab in treating pediatric patients are needed in future clinical practice, which will provide insight into the dupilumab’s effects on atopic march and look for early treatment windows of opportunity. Disease-modifying therapies that design different therapeutic strategies to target the specific march of AD and thereby precisely intervene in different immune processes promise greater breakthroughs in the treatment of AD.
Abbreviations
AC, allergic conjunctivitis; AD, atopic dermatitis; CDLQI, Children’s Dermatology Life Quality Index; DCs, dendritic cells; EASI, Eczema Area and Severity Index; EASI-50, at least 50% improvement from baseline in EASI; EASI-75, at least 75% improvement from baseline in EASI; EASI-90, at least 90% improvement from baseline in EASI; FDA, Food and Drug Administration; FLG, filaggrin; IGA, Investigator’s Global Assessment; IGA0/1, Investigator’s Global Assessment score of 0 (clear) or 1 (almost clear); ILC2s, type 2 innate lymphoid cells; JAK, Janus kinase; LOR, loricrin; NRS, Numerical Rating Scale; N/A data not available/reported; QoL, Quality of Life; q4w, every 4 weeks; q2w, every 2 weeks; SCORAD, SCORing Atopic Dermatitis; STAT, signal transducer and activator of transcription; TCS, topical corticosteroids; TEAE, treatment-emergent adverse event; TSLP, thymic stromal lymphopoietin; TWEL, transepidermal water loss.
Ethical Approval
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was funded by National Key R&D Program of China (2023YFC2508200) and China Medical Education Association (2023WSJSPGZXKT-14).
Disclosure
Professor Xing-Hua Gao reports personal fees from advisary, consultation and lecturer for the fllowing roles for Eli Lilly, GSK, Janssen, LEO Pharma, Novartis, Pfizer, Pierre Fabre, Regeneron Pharmaceuticals Inc., Sanofi and, consultancy/advisory board member for AbbVie, Boehringer Ingelheim, Novartis, Pfizer, Sanofi – investigator; AbbVie, AstraZeneca, BMS, Eli Lilly, Huarun, JiaLan, LEO Pharma, Pfizer, Puqi and Sanofi. The authors report no other conflicts of interest in this work.
References
1. Langan SM, Irvine AD, Weidinger S. Atopic dermatitis. Lancet. 2020;396(10247):345–360. doi:10.1016/S0140-6736(20)31286-1
2. Chovatiya R. Atopic Dermatitis (Eczema). JAMA. 2023;329(3):268. doi:10.1001/jama.2022.21457
3. Wollenberg A, Barbarot S, Bieber T, et al. Consensus-based European guidelines for treatment of atopic eczema (atopic dermatitis) in adults and children: part I. J Eur Acad Dermatol Venereol. 2018;32(5):657–682. doi:10.1111/jdv.14891
4. Silverberg JI, Barbarot S, Gadkari A, et al. Atopic dermatitis in the pediatric population: a cross-sectional, international epidemiologic study. Ann Allergy Asthma Immunol. 2021;126(4):417–28.e2. doi:10.1016/j.anai.2020.12.020
5. Weidinger S, Illig T, Baurecht H, et al. Loss-of-function variations within the filaggrin gene predispose for atopic dermatitis with allergic sensitizations. J Allergy Clin Immunol. 2006;118(1):214–219. doi:10.1016/j.jaci.2006.05.004
6. Osawa R, Akiyama M, Shimizu H. Filaggrin gene defects and the risk of developing allergic disorders. Allergology Int. 2011;60(1):1–9. doi:10.2332/allergolint.10-RAI-0270
7. Demessant-Flavigny AL, Connétable S, Kerob D, Moreau M, Aguilar L, Wollenberg A. Skin microbiome dysbiosis and the role of Staphylococcus aureus in atopic dermatitis in adults and children: a narrative review. J Eur Acad Dermatol Venereol. 2023;37(Suppl 5):3–17. doi:10.1111/jdv.19125
8. Gandhi NA, Bennett BL, Graham NM, Pirozzi G, Stahl N, Yancopoulos GD. Targeting key proximal drivers of type 2 inflammation in disease. Nat Rev Drug Discov. 2016;15(1):35–50. doi:10.1038/nrd4624
9. Facheris P, Jeffery J, Del Duca E, Guttman-Yassky E. The translational revolution in atopic dermatitis: the paradigm shift from pathogenesis to treatment. Cell Mol Immunol. 2023;20(5):448–474. doi:10.1038/s41423-023-00992-4
10. Nowowiejska J, Baran A, Flisiak I. Lipid Alterations and Metabolism Disturbances in Selected Inflammatory Skin Diseases. Int J Mol Sci. 2023;24(8):7053. doi:10.3390/ijms24087053
11. Silverberg JI. Comorbidities and the impact of atopic dermatitis. Ann Allergy Asthma Immunol. 2019;123(2):144–151. doi:10.1016/j.anai.2019.04.020
12. Barbarot S, Silverberg JI, Gadkari A, et al. The Family Impact of Atopic Dermatitis in the Pediatric Population: results from an International Cross-sectional Study. J Pediatr. 2022;246:220–6.e5. doi:10.1016/j.jpeds.2022.04.027
13. Paller A, Jaworski JC, Simpson EL, et al. Major Comorbidities of Atopic Dermatitis: beyond Allergic Disorders. Am j Clin Dermatol. 2018;19(6):821–838. doi:10.1007/s40257-018-0383-4
14. Davidson WF, Leung DYM, Beck LA, et al. Report from the National Institute of Allergy and Infectious Diseases workshop on “Atopic dermatitis and the atopic march: mechanisms and interventions”. J Allergy Clin Immunol. 2019;143(3):894–913. doi:10.1016/j.jaci.2019.01.003
15. Murota H, Koike Y, Morisaki H, Matsumoto M, Takenaka M. Exacerbating factors and disease burden in patients with atopic dermatitis. Allergology Int. 2022;71(1):25–30. doi:10.1016/j.alit.2021.10.002
16. Licari A, Castagnoli R, Marseglia A, et al. Dupilumab to Treat Type 2 Inflammatory Diseases in Children and Adolescents. Paediatric Drugs. 2020;22(3):295–310. doi:10.1007/s40272-020-00387-2
17. Harb H, Chatila TA. Mechanisms of Dupilumab. Clin exp allerg. 2020;50(1):5–14. doi:10.1111/cea.13491
18. Cabanillas B. Dupilumab for Atopic Dermatitis-From Clinical Trials to Molecular and Cellular Mechanisms. Dermatitis. 2022. doi:10.1097/DER.0000000000000905
19. Mastorino L, Viola R, Panzone M, et al. Dupilumab induces a rapid decrease of pruritus in adolescents: a pilot real-life study. Dermatologic Therapy. 2021;34(6):e15115. doi:10.1111/dth.15115
20. Mastorino L, Cantafio Duò VL, Vecco C, et al. Impact of comorbidities in the response of atopic patients treated with dupilumab: a real-life study up to 36 weeks. J Eur Acad Dermatol Venereol. 2022;36(12):e1021–e3. doi:10.1111/jdv.18427
21. Miniotti M, Ribero S, Mastorino L, et al. Long-term psychological outcome of patients with moderate-to-severe atopic dermatitis continuously treated with Dupilumab: data up to 3 years. Exp dermatol. 2023;32(6):852–858. doi:10.1111/exd.14786
22. LaPorte SL, Juo ZS, Vaclavikova J, et al. Molecular and structural basis of cytokine receptor pleiotropy in the interleukin-4/13 system. Cell. 2008;132(2):259–272. doi:10.1016/j.cell.2007.12.030
23. Andrews AL, Holloway JW, Holgate ST, Davies DE. IL-4 receptor alpha is an important modulator of IL-4 and IL-13 receptor binding: implications for the development of therapeutic targets. J Iimmunol. 2006;176(12):7456–7461. doi:10.4049/jimmunol.176.12.7456
24. Le Floc’h A, Allinne J, Nagashima K, et al. Dual blockade of IL-4 and IL-13 with dupilumab, an IL-4Rα antibody, is required to broadly inhibit type 2 inflammation. Allergy. 2020;75(5):1188–1204. doi:10.1111/all.14151
25. Ferrucci S, Romagnuolo M, Maronese CA, et al. Skin barrier status during dupilumab treatment in patients with severe atopic dermatitis. Therapeutic Adv Chronic Dis. 2021;12:20406223211058332. doi:10.1177/20406223211058332
26. Berdyshev E, Goleva E, Bissonnette R, et al. Dupilumab significantly improves skin barrier function in patients with moderate-to-severe atopic dermatitis. Allergy. 2022;77(11):3388–3397. doi:10.1111/all.15432
27. Callewaert C, Nakatsuji T, Knight R, et al. IL-4Rα Blockade by Dupilumab Decreases Staphylococcus aureus Colonization and Increases Microbial Diversity in Atopic Dermatitis. J Investigative Dermatol. 2020;140(1):191–202.e7. doi:10.1016/j.jid.2019.05.024
28. Simpson EL, Schlievert PM, Yoshida T, et al. Rapid reduction in Staphylococcus aureus in atopic dermatitis subjects following dupilumab treatment. J Allergy Clin Immunol. 2023.
29. Hartmann J, Moitinho-Silva L, Sander N, et al. Dupilumab but not cyclosporine treatment shifts the microbiome toward a healthy skin flora in patients with moderate-to-severe atopic dermatitis. Allergy. 2023;78(8):2290–2300. doi:10.1111/all.15742
30. Paller AS, Simpson EL, Siegfried EC, et al. Dupilumab in children aged 6 months to younger than 6 years with uncontrolled atopic dermatitis: a randomised, double-blind, placebo-controlled, Phase 3 trial. Lancet. 2022;400(10356):908–919. doi:10.1016/S0140-6736(22)01539-2
31. Paller AS, Siegfried EC, Thaçi D, et al. Efficacy and safety of dupilumab with concomitant topical corticosteroids in children 6 to 11 years old with severe atopic dermatitis: a randomized, double-blinded, placebo-controlled phase 3 trial. J Am Acad Dermatol. 2020;83(5):1282–1293. doi:10.1016/j.jaad.2020.06.054
32. Simpson EL, Paller AS, Siegfried EC, et al. Efficacy and Safety of Dupilumab in Adolescents With Uncontrolled Moderate to Severe Atopic Dermatitis: a Phase 3 Randomized Clinical Trial. JAMA Dermatol. 2020;156(1):44–56.
33. Butala S, Paller AS. Biologics in the management of childhood atopic dermatitis. J Allergy Clin Immunol. 2023;151(3):681–685. doi:10.1016/j.jaci.2023.01.010
34. Eyerich K, Novak N. Immunology of atopic eczema: overcoming the Th1/Th2 paradigm. Allergy. 2013;68(8):974–982. doi:10.1111/all.12184
35. Napolitano M, Fabbrocini G, Neri I, et al. Dupilumab Treatment in Children Aged 6-11 Years With Atopic Dermatitis: a Multicentre, Real-Life Study. Paediatric Drugs. 2022;24(6):671–678. doi:10.1007/s40272-022-00531-0
36. Wang A, Zhou Y, Luo Y, et al. High loading-dose of dupilumab resulted in rapid disease control in pediatric patients with atopic dermatitis. Front Immunol. 2023;14:1160710.
37. Zhou B, Peng C, Cao Q, Wang J, Chen X, Li J. Dupilumab therapy in children aged 2-12 years with uncontrolled moderate-to-severe atopic dermatitis: a Chinese real-world study. J Eur Acad Dermatol Venereol. 2023;38(1):e35–e38. doi:10.1111/jdv.19409
38. Patruno C, Fabbrocini G, Lauletta G, et al. A 52-week multicenter retrospective real-world study on effectiveness and safety of dupilumab in children with atopic dermatitis aged from 6 to 11 years. J Dermatol Treatment. 2023;34(1):2246602. doi:10.1080/09546634.2023.2246602
39. Napolitano M, Fabbrocini G, Potestio L, et al. A 24-weeks real-world experience of dupilumab in adolescents with moderate-to-severe atopic dermatitis. Dermatologic Therapy. 2022;35(8):e15588. doi:10.1111/dth.15588
40. Narla S, Silverberg JI, Simpson EL. Management of inadequate response and adverse effects to dupilumab in atopic dermatitis. J Am Acad Dermatol. 2022;86(3):628–636. doi:10.1016/j.jaad.2021.06.017
41. Kychygina A, Cassagne M, Tauber M, et al. Dupilumab-Associated Adverse Events During Treatment of Allergic Diseases. Clin Rev Allergy Immunol. 2022;62(3):519–533. doi:10.1007/s12016-022-08934-0
42. Blauvelt A, Rosmarin D, Bieber T, et al. Improvement of atopic dermatitis with dupilumab occurs equally well across different anatomical regions: data from phase III clinical trials. Br j dermatol. 2019;181(1):196–197. doi:10.1111/bjd.17703
43. Patruno C, Potestio L, Scalvenzi M, et al. Dupilumab for the treatment of adult atopic dermatitis in special populations. J Dermatol Treatment. 2022;33(7):3028–3033. doi:10.1080/09546634.2022.2102121
44. Bansal A, Simpson EL, Paller AS, et al. Conjunctivitis in Dupilumab Clinical Trials for Adolescents with Atopic Dermatitis or Asthma. Am j Clin Dermatol. 2021;22(1):101–115. doi:10.1007/s40257-020-00577-1
45. Treister AD, Kraff-Cooper C, Lio PA. Risk Factors for Dupilumab-Associated Conjunctivitis in Patients With Atopic Dermatitis. JAMA Dermatol. 2018;154(10):1208–1211. doi:10.1001/jamadermatol.2018.2690
46. Akinlade B, Guttman-Yassky E, de Bruin-Weller M, et al. Conjunctivitis in dupilumab clinical trials. Br j dermatol. 2019;181(3):459–473. doi:10.1111/bjd.17869
47. Tao Z, Liu W, Chen Q, et al. Blocking Th2 Signaling Pathway Alleviates the Clinical Symptoms and Inflammation in Allergic Conjunctivitis. Invest Ophthalmol Visual Sci. 2023;64(10):30. doi:10.1167/iovs.64.10.30
48. Han H, Cummings S, Shade KC, et al. Cellular mechanisms and effects of IL-4 receptor blockade in experimental conjunctivitis evoked by skin inflammation. JCI Insight. 2023;8(3). doi:10.1172/jci.insight.163495
49. Huang J, Choo YJ, Smith HE, Apfelbacher C. Quality of life in atopic dermatitis in Asian countries: a systematic review. Archives of Dermatological Res. 2022;314(5):445–462. doi:10.1007/s00403-021-02246-7
50. Ramirez FD, Chen S, Langan SM, et al. Association of Atopic Dermatitis With Sleep Quality in Children. JAMA Pediatrics. 2019;173(5):e190025. doi:10.1001/jamapediatrics.2019.0025
51. Patel KR, Immaneni S, Singam V, Rastogi S, Silverberg JI. Association between atopic dermatitis, depression, and suicidal ideation: a systematic review and meta-analysis. J Am Acad Dermatol. 2019;80(2):402–410. doi:10.1016/j.jaad.2018.08.063
52. Stingeni L, Bianchi L, Antonelli E, et al. Moderate-to-severe atopic dermatitis in adolescents treated with dupilumab: a multicentre Italian real-world experience. J Eur Acad Dermatol Venereol. 2022;36(8):1292–1299. doi:10.1111/jdv.18141
53. Stingeni L, Bianchi L, Antonelli E, et al. A 52-week update of a multicentre Italian real-world experience on effectiveness and safety of dupilumab in adolescents with moderate-to-severe atopic dermatitis. J Eur Acad Dermatol Venereol. 2023;37(3):e384–e8. doi:10.1111/jdv.18648
54. Lasek A, Bellon N, Mallet S, et al. Effectiveness and safety of dupilumab in the treatment of atopic dermatitis in children (6-11 years): data from a French multicentre retrospective cohort in daily practice. J Eur Acad Dermatol Venereol. 2022;36(12):2423–2429. doi:10.1111/jdv.18450
55. Blauvelt A, Guttman-Yassky E, Paller AS, et al. Long-Term Efficacy and Safety of Dupilumab in Adolescents with Moderate-to-Severe Atopic Dermatitis: results Through Week 52 from a Phase III Open-Label Extension Trial (LIBERTY AD PED-OLE). Am j Clin Dermatol. 2022;23(3):365–383. doi:10.1007/s40257-022-00683-2
56. Silverberg JI, Guttman-Yassky E, Gadkari A, et al. Real-world persistence with dupilumab among adults with atopic dermatitis. Ann Allergy Asthma Immunol. 2021;126(1):40–45. doi:10.1016/j.anai.2020.07.026
57. Zimmermann M, Rind D, Chapman R, Kumar V, Kahn S, Carlson J. Economic Evaluation of Dupilumab for Moderate-to-Severe Atopic Dermatitis: a Cost-Utility Analysis. J Drugs Dermatol. 2018;17(7):750–756.
58. Miyaji Y, Yang L, Yamamoto-Hanada K, Narita M, Saito H, Ohya Y. Earlier aggressive treatment to shorten the duration of eczema in infants resulted in fewer food allergies at 2 years of age. The Journal of Allergy and Clinical Immunology in Practice. 2020;8(5):1721–4.e6. doi:10.1016/j.jaip.2019.11.036
59. Geba GP, Li D, Xu M, et al. Attenuating the atopic march: meta-analysis of the dupilumab atopic dermatitis database for incident allergic events. J Allergy Clin Immunol. 2023;151(3):756–766. doi:10.1016/j.jaci.2022.08.026
60. Siegfried EC, Simpson EL, Cork MJ, et al. Dupilumab Treatment Leads to Rapid and Consistent Improvement of Atopic Dermatitis in All Anatomical Regions in Patients Aged 6 Months to 5 Years. Dermatol Ther. 2023;13(9):1987–2000. doi:10.1007/s13555-023-00960-w
61. Blauvelt A, de Bruin-Weller M, Simpson EL, Chen Z, Zhang A, Shumel B. Dupilumab with Topical Corticosteroids Provides Rapid and Sustained Improvement in Adults with Moderate-to-Severe Atopic Dermatitis Across Anatomic Regions Over 52 Weeks. Dermatol Ther. 2022;12(1):223–231. doi:10.1007/s13555-021-00638-1
62. Simpson EL, Paller AS, Siegfried EC, et al. Dupilumab Demonstrates Rapid and Consistent Improvement in Extent and Signs of Atopic Dermatitis Across All Anatomical Regions in Pediatric Patients 6 Years of Age and Older. Dermatol Ther. 2021;11(5):1643–1656. doi:10.1007/s13555-021-00568-y
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.