")
Back to Journals » Adolescent Health, Medicine and Therapeutics » Volume 14
A Narrative Review: Phentermine and Topiramate for the Treatment of Pediatric Obesity
Authors Kim A, Nguyen J, Babaei M, Kim A , Geller DH, Vidmar AP
Received 22 April 2023
Accepted for publication 6 August 2023
Published 23 August 2023 Volume 2023:14 Pages 125—140
DOI https://doi.org/10.2147/AHMT.S383454
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor M Constantine Samaan
Anthony Kim,1 Jennifer Nguyen,2 Mahsa Babaei,2 Ahlee Kim,1,2 David H Geller,1,2 Alaina P Vidmar1,2
1Department of Pediatrics, Keck School of Medicine, University of Southern California, Los Angeles, CA, USA; 2Children’s Hospital Los Angeles and Keck School of Medicine of University of Southern California, Department of Pediatrics, Center for Endocrinology, Diabetes and Metabolism, Los Angeles, CA, USA
Correspondence: Alaina P Vidmar, Diabetes & Obesity Program, Center for Endocrinology, Diabetes and Metabolism, Department of Pediatrics, 4650 Sunset Boulevard, Mailstop #61, Los Angeles, CA, 90027, USA, Tel +1 323 361-3385, Fax +1 323 361-1301, Email [email protected]
Abstract: The prevalence of pediatric obesity has increased exponentially over the past four decades. The American Academy of Pediatrics recently released updated clinical practice guidelines highlighting the importance of identifying pediatric obesity as a chronic disease. The guidelines support consideration of concurrent treatment with intensive lifestyle interventions, obesity pharmacotherapy, and bariatric surgery. The dramatic rise in pediatric obesity has spurred interest in utilizing obesity pharmacotherapy to support sustained weight reduction in pediatric cohorts, in the hopes of preventing the emergence of later-appearing, significant co-morbidities. Despite the enormous demand, the obstacles posed by performance of needed clinical trials in the pediatric population markedly limits available pharmacotherapy for the treatment of obesity in pediatrics. Currently, there are five medications approved by the Food and Drug Administration for use in youth with obesity. In 2022, the phentermine/topiramate (PHEN/TPM), once-daily, controlled-release, combination product received FDA approval, for the indication of chronic weight management, in youth with obesity, ages 12 years and older. The objectives of this narrative review are to: (1) Review the mechanism of action of phentermine and topiramate, (2) Summarize the safety and efficacy data of topiramate and phentermine use as both monotherapies and in combination, and (3) Discuss clinical practice guidelines and clinical implications, for the use of these agents in youths with obesity.
Keywords: phentermine, topiramate, pediatric obesity, obesity pharmacotherapy
Introduction
The prevalence of pediatric obesity has increased exponentially over the past four decades.1,2 Youth-onset obesity is associated with comorbidities previously seen only in adult populations, such as type 2 diabetes, hypertension, dyslipidemia, nonalcoholic fatty liver disease, and obstructive sleep apnea.2–4 Obesity-related comorbidities, that occur in childhood, are more aggressive and more rapidly progressive than are those seen in adult onset obesity.3,5 The American Academy of Pediatrics (AAP) recently released updated clinical practice guidelines to highlight the importance of identifying pediatric obesity as a chronic disease.2 The AAP guidelines provide evidence in support of concurrent treatment for pediatric obesity with intensive lifestyle interventions, obesity pharmacotherapies, and bariatric surgery.2,6,7
Currently, there are five medications approved by the Food and Drug Administration (FDA) for use in children and adolescents with obesity.8 However, prior to 2022, there were just three medications with FDA approval for the treatment of pediatric obesity: orlistat (approved for adolescents 12 years and older),9,10 phentermine (approved for a 12-week course, in youth 16 years and older),11 and liraglutide 3 mg daily (approved for adolescents 12 years and older).12 In July 2022, the FDA approved the use of phentermine/topiramate (PHEN/TPM), a once-daily, controlled-release, combination product, for chronic weight management in adolescents with obesity, age 12 years and older.13,14 Most recently, in January of 2023, the FDA approved the use of once weekly semaglutide, 2.4 mg per week, a glucagon-like peptide-1 (GLP-1) receptor agonist, for chronic weight management in youth with obesity, ages 12 years and older.15
For many children living with obesity, lifestyle modifications alone result in only modest weight reduction, with the weight frequently regained after an initial period of success.16–18 This observation has fueled the growing interest in utilizing obesity pharmacotherapy to achieve more sustained, durable weight reduction in pediatric cohorts.8,19,20 Despite the immense interest and demand, the current use of pharmacotherapy for the treatment of obesity in the pediatric population is limited.6,7,17,21 A number of reasons have been proposed to explain this.6 First, pediatric obesity is generally not perceived as a chronic medical condition,2 and thus, obesity treatment is still often considered optional by healthcare providers, patients, families, payers, and policy makers.2 Secondly, obesity medicine is not a staple of most medical school curriculums,19 and thus, clinicians in training do not uniformly receive formal education into the diagnosis, evaluation, and management of pediatric obesity, and the available (and evolving) obesity pharmacotherapies.19,20 The result is too-few practitioners armed with the requisite experience and expertise to prescribe these agents most effectively.21 Thirdly, there are significant challenges procuring insurance authorization and coverage, and supply issues which limit access to these agents for families dealing with pediatric obesity.6,7,17,21 To overcome these barriers and to ensure that pediatric patients living with obesity have access to, and receive appropriate treatment, further investigation into the safety and efficacy of these agents in pediatric cohorts is needed, often limited by the difficulty in recruiting study participants and garnering human subjects approval for the conduct of clinical trials in this population.19 In addition, comprehensive educational programs are needed to support clinicians on the proper way in which to incorporate these treatment regimens into their standard practice as potential options for the care of a pediatric patient with obesity. The goal of this narrative review is to help bridge those gaps in knowledge. The specific objectives are: (1) Review the mechanism of action of phentermine and topiramate, (2) Summarize the safety and efficacy data of topiramate and phentermine as monotherapy and in combination in youth with obesity, and (3) Discuss clinical practice guidelines and clinical implications for the use of these agents in the pediatric population.
Phentermine Monotherapy
Phentermine is FDA-approved for the treatment of obesity in adolescents, ages 16 years and older, whose body mass index (BMI) exceeds 30 kg/m2 or exceeds 27 kg/m2 with an additional risk factor, such as hypertension, diabetes, or hyperlipidemia.22–26
Mechanism of Action
The exact mechanism of action by which phentermine works to reduce obesity remains obscure, and has not been well elucidated in humans.27–29 Most of the data on the mechanism of action of phentermine is derived from animals or in-vitro studies.26,30–34 Phentermine is an indirect-acting sympathomimetic agent, that both increases the release of norepinephrine from presynaptic vesicles in the lateral hypothalamus, and inhibits norepinephrine reuptake.27,35 Phentermine also stimulates the release of serotonin and dopamine from nerve terminals and acts as a weak, reversible monoamine oxidase and serotonin reuptake inhibitor.25,26,36–39 The resultant increase in norepinephrine concentration within the synaptic cleft in turn stimulates β-2 adrenergic receptors and inhibits appetite.27,28,40,41 Some reports propose that phentermine inhibits neuropeptide Y, whose signaling pathway is integral to the induction of hunger, although the exact mechanism remains unknown.27
Side Effect Profile and Prescribing Considerations
Phentermine is well absorbed from the gastrointestinal tract and 80% is excreted in the urine intact (unmetabolized). Phentermine is metabolized by cytochrome P450 (CYP) 3A426 and has a half-life of 20 h.33 Phentermine is distributed into all tissues, including the brain.42 The FDA has classified phentermine as a schedule IV controlled substance.27 Although phentermine is not an amphetamine, it does have a similar chemical structure, and thus has the potential for abuse and addiction.41 Emerging evidence in adult cohorts treated with phentermine for weight loss has not shown that phentermine monotherapy is associated with abuse or addiction.43 The most common side-effects of phentermine monotherapy, reported in both adult and pediatric patients, are tachycardia, palpitations, hypertension, anxiety, dizziness, insomnia, headache, dryness of the mouth, and gastrointestinal complaints.25,29,38,44,45 Although the dopaminergic and serotonergic effects are deemed clinically insignificant, patients are still advised against using phentermine within 14 days of having taken monoamine oxidase inhibitors or concurrent use with serotonin reuptake inhibitors.29,33,38 Phentermine is contraindicated when sympathomimetic drug administration may pose a significant risk, such as in patients with hyperthyroidism, unstable cardiovascular disease, or moderate-to-severe hypertension.33,43 Many adult and pediatric treatment protocols recommend close monitoring of blood pressure during the first 3 months of treatment initiation.44
Phentermine Monotherapy as Treatment of Obesity in Pediatric Populations
Despite FDA approval being granted over six decades ago (1959), the literature contains few studies investigating the use of phentermine monotherapy for obesity treatment in youth (Table 1).45 In 1966, Lorber et al conducted a 12-week, 3-parallel-arm trial in 68 patients with obesity, ages three to fifteen.46 Patients were randomized to one of the three treatment arms for the study duration: 1) Phenmetrazine 12.5 mg daily (a long-acting amphetamine), 2) Phentermine 15 mg daily, or 3) Placebo. All participants were instructed to not eat snacks between meals and to avoid desserts and sugar sweetened beverages for the duration of the study. By week 4, patients in the phenmetrazine arm demonstrated a mean weight loss of 3.4 kg compared to 2.2 kg lost by participants in the phentermine arm, and 2.1 kg lost among placebo recipients. By week 12, both the phenmetrazine and phentermine groups had lost an additional 3 kg, whereas the placebo group had begun to regain weight. One patient in the phentermine arm withdrew from the study due to insomnia.46 Of note, pediatric obesity studies from that time frame (1959 and on) utilized only changes in absolute body weight to assess efficacy of obesity treatment.47 However, this metric fails to take into account either height velocity or BMI.47 Nevertheless, at week 4, there was no statistically significant reduction in weight when comparing phentermine monotherapy to placebo, whereas by week 12, continued weight reduction in the phentermine group was observed, whereas the placebo group had begun to regain weight. These findings are consistent with the sustained weight reduction reported, at that time, in adults taking phentermine monotherapy, with continued weight loss observed during the recommended 12-week treatment course.
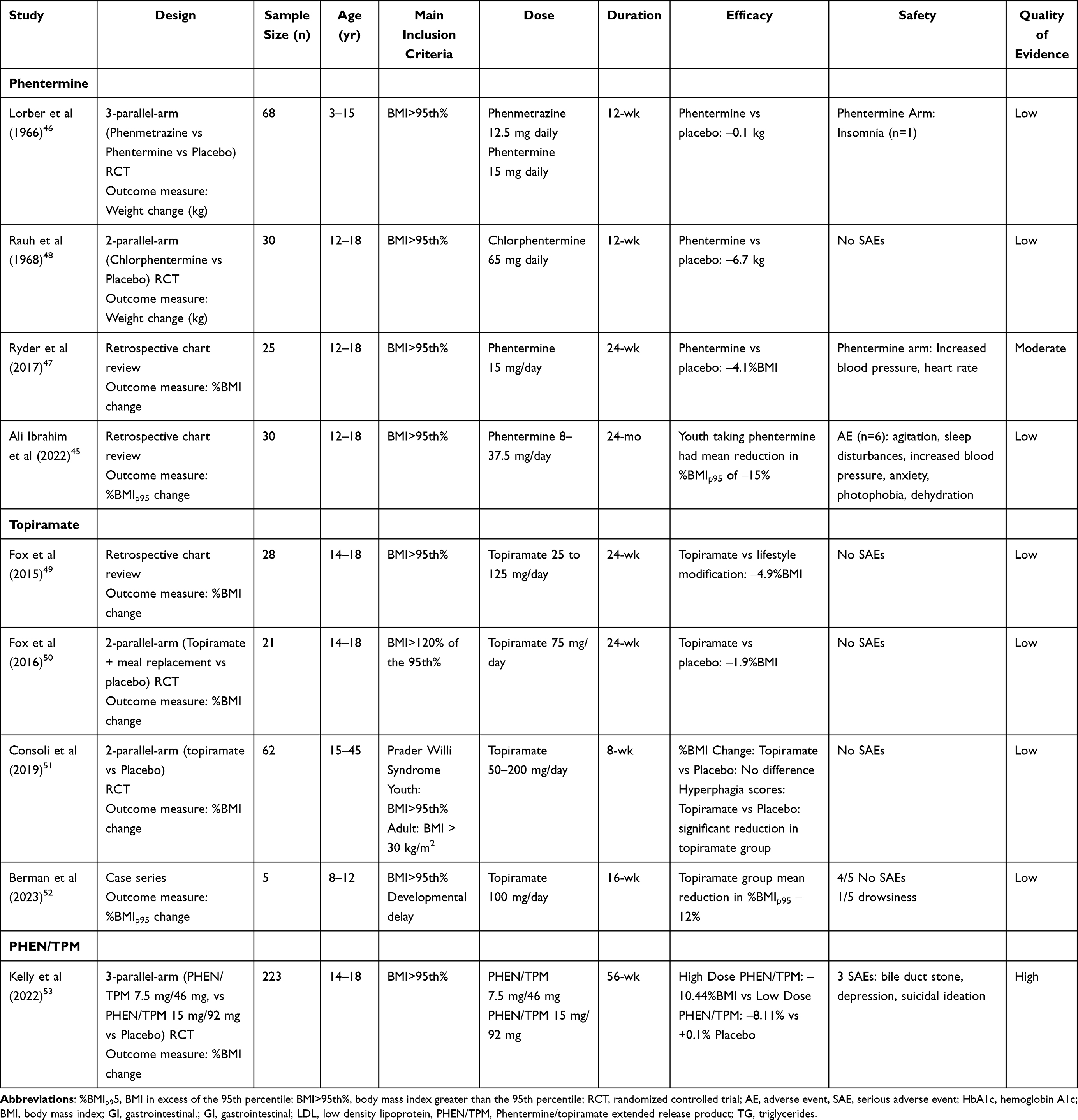 |
Table 1 Summary of Trials of Phentermine, Topiramate, and PHEN/TPM for Obesity Management in Pediatrics |
In 1968, Rauh et al conducted a 12-week, randomized controlled trial of chlorphentermine versus placebo in thirty adolescents with obesity.48 Developed in 1962, chlorphentermine, the 4-chloro derivative of phentermine, is a highly selective serotonin releasing agent54 which acts as a serotonergic appetite suppressant.28 Participants did not receive any specific instructions about diet or exercise. Patients randomized to the chlorphentermine group received 65 mg of this chlorinated phentermine analog daily and by week 12 had experienced an average weight loss of 6.7 kg, in contrast to the average weight gain of 0.5 kg observed in the placebo group (p < 0.001). In a 12-week, open-label extension, eight of the patients assigned to the chlorphentermine group remained on the study agent and lost an additional 14.5 kg at week 24, when compared to baseline. No adverse events were reported among participants receiving the study drug.48 Similar to the previous study, there was a significant weight reduction in the chlorphentermine group compared to placebo, most notable by week 24, further illustrating the sustained effect of phentermine-based treatments with prolonged use, as compared to the natural history of weight among patients with obesity.19,20 Of note, chlorphentermine is an agent more akin to fenfluramine with respect to its mechanism of action and acts primarily as a serotonin releasing agent, perhaps suggesting an explanation for the greater weight reduction observed with this agent than with other agents in the previous studies, similar to the robust effects of fenfluramine seen in adult studies.22,25,26
Between 1968 and 2017 there was a paucity of published studies on the use of phentermine for obesity treatment in pediatric populations. In 2017, a retrospective chart review reported a single center experience with 25 adolescents with obesity (mean baseline BMI 41.2 ± 6.9 kg/m2) prescribed phentermine 15 mg per day as an adjunct to standard lifestyle modification therapy (LMT), compared to age-matched controls completing LMT only. The adolescents on phentermine demonstrated a significantly greater percent change in BMI at weeks 12 and 24 compared to LMT alone (Week 12: ‒2.9%; 95% CI (‒4.5%, ‒1.4%); p<0.001; Week 24: ‒4.1%; 95% CI (‒7.1%, ‒1.0%); p = 0.009). At week 12, 40% of participants in the phentermine group achieved a greater than 5% reduction in BMI compared to only 9% in the LMT alone group; by week 24, 64% in the phentermine vs 21% in the LMT alone had achieved ≥ 5% BMI reduction. There were no significant differences in blood pressure between groups over the study period. At all three time points, patients in the phentermine group did have an increase in heart rate that was significantly greater than that observed with LMT alone (+8.53 beats per minute; 95% CI (1.59, 15.47); p = 0.02).11 Despite the intrinsic limitations of this study due to its retrospective study design and small study size, this was the first study in the 2000’s to highlight the benefit of phentermine in combination with intensive lifestyle modification therapy for weight reduction in pediatric patients. The study results suggested that phentermine monotherapy was both safe and effective in yielding clinically meaningful weight loss in patients with severe obesity when compared to lifestyle modification alone.
In 2022, a second, single-center retrospective chart review reported on 30 adolescents with obesity (mean age 15.6 ± 1.9 years; mean BMI of 37.7 ± 6.3 kg/m2) treated with phentermine monotherapy, in doses ranging from 8 to 37.5 mg, for a period ranging from 0.5 to 24 months (mean of 10 months). There was a mean reduction in BMI in excess of the 95th percentile (%BMIp95) of 15% in patients taking phentermine, with 70% of patients achieving a ≥ 5% reduction in %BMIp95 at within an average of 11 months (5–24 months). Six participants (20%) developed side effects, including agitation, sleep disturbances, increased blood pressure, anxiety, photophobia, abdominal pain, and dehydration.45 Although there clearly exists a paucity of studies investigating the use of phentermine monotherapy in youth cohorts, these two retrospective studies provide support for its use as adjunct to lifestyle modification. In contrast to the weight reduction seen with lifestyle modification alone, which rarely achieves clinical significance (defined as weight or BMI reduction of ≥ 5%),55,56 phentermine monotherapy in these 2 cohorts resulted in clinically and statistically meaningful BMI reductions. Although the quality of this evidence is low due to the retrospective nature of these study designs, the data do add to our appreciation of the benefits possible when phentermine monotherapy is implemented in cohorts of youth with obesity.
Topiramate Monotherapy
Topiramate, a well-established, second-generation anti-epileptic agent, was first FDA-approved for pediatric epilepsy in 1996, and for pediatric migraine prophylaxis in 2014.49,57 It is currently indicated as initial monotherapy or adjunctive therapy for patients ≥ 2 years of age with partial onset or primary generalized tonic-clonic seizures, patients ≥ 2 years of age with seizures associated with Lennox-Gastaut syndrome, and patients ≥ 12 years of age for use as prophylaxis for migraines.58 Weight loss and appetite suppression are well-characterized effects of topiramate monotherapy in pediatric cohorts,59 leading to studies to evaluate its efficacy as an obesity pharmacotherapeutic agent.42,59 Topiramate is not an FDA-obesity pharmacotherapeutic, although pediatric obesity medicine specialists continue to utilize it off-label for the treatment of obesity in youth.21 Pediatric providers have historically used topiramate off-label for other chronic conditions such as alcohol use disorder, binge eating disorder, and bulimia nervosa.58
Mechanism of Action
Topiramate is a sulfamate-substituted monosaccharide that modulates excitatory voltage-activated calcium and sodium channels and γ-aminobutyric acid (GABA)-A receptors, while simultaneously antagonizing alpha-amino-3-hydroxyl-4-isoxazole-propionic acid kainite (AMPA/KA) receptors.57,60,61 Animal studies demonstrated that food intake was significantly increased following administration of GABA-B and GABA-A antagonists into the nucleus accumbens shell and ventral tegmental area.61,62 Specific blockade of ionotropic GABA-A receptors in the lateral hypothalamus elicits eating behavior in satiated rodent models.61,62 The exact mechanism by which topiramate suppresses appetite is unknown. Extrapolating from animal data, it has been hypothesized that the anorectic action results from a combination of carbonic-anhydrase inhibition of taste and activation of GABA-A receptors in the lateral hypothalamus known to interact with the leptin pathway.61–63 In 2006, Liang et al, investigated the molecular effects of topiramate in rodents, demonstrating that topiramate regulates hepatic expression of genes involved in lipid metabolism, resulting in reduced plasma glucose and triglyceride levels.64,65 Animals treated with topiramate produced decreased messenger RNA for sterol regulatory element-binding protein-1c, stearoyl-coenzyme A desaturase-1, choline kinase, and fatty acid coenzyme A ligase long chain 4, and diminished expression of acetyl-CoA carboxylase 2 and stearoyl-CoA desaturase-1.64 Topiramate also upregulated three genes which are involved in cholesterol synthesis independent of reduced food intake.64
Side Effect Profile and Prescribing Considerations
Topiramate is well absorbed from the gastrointestinal tract and partially excreted in the urine with peak plasma levels being attained 3 hours after ingestion.42 The half-life is 25 hours in healthy volunteer individuals. The bioavailability exceeds 80% following an oral dose and is not significantly affected by food.42 Topiramate is distributed into all tissues, including the brain.42 Topiramate, like other carbonic anhydrase inhibitors, may produce central and peripheral nervous system effects, such as paresthesia, acute myopia, blurred vision, redness of the sclera, photophobia, fatigue, somnolence, depression, and difficulties with concentration and memory.42,57,58 The most common adverse effects associated with topiramate treatment for obesity are dose-related and include paresthesia/hypoesthesia, taste perversion, psychomotor impairment/concentration difficulty/memory impairment, anorexia, nervousness, visual disturbance, dry mouth, mood problems, constipation/dyspepsia/nausea/abdominal pain/diarrhea, dizziness, back pain, insomnia, upper respiratory tract infection, and migraine.59 In a pooled meta-analysis of topiramate treatment, in the adult population with obesity, there were no reports of cardiovascular events or any other major adverse events.42,58,59,66 Topiramate does have a mild diuretic effect and thus can induce mild weight loss, independent of a reduction in blood pressure.59 Topiramate is classified as Pregnancy Category D and use during pregnancy has been linked to a significantly increased risk of birth defects, affecting orofacial, cardiac and urogenital development.67–71 In addition, topiramate can reduce the estrogen component of oral contraceptive medications, thus precautions must be provided for females of reproductive age.42
Topiramate Monotherapy as a Treatment of Obesity in Pediatric Populations
The literature contains reports of the weight loss-promoting effects of topiramate in pediatric cohorts, both with and without obesity (Table 1). In 2003, Mikaeloff et al, reported a prospective study of 207 patients with epilepsy, without obesity (median age 6.5 years), treated with topiramate (starting dose 4.7 mg/kg/day) for seizure control.72 Patients were followed for an average of 5.6 months. Twelve percent of patients reported anorexia, 10% reported decreased appetite, and 7% reported weight loss over the study period. Other adverse effects included drowsiness (10.5%), fatigue (8.5%), and hyperactivity (7.5%).72 Similarly, in 2005, Winner et al conducted a randomized controlled trial of topiramate for migraine prevention in 162 patients without obesity, ages 6 to 15 years, identifying anorexia and weight loss in one third of study participants receiving topiramate compared to the placebo group.73 A 2015 retrospective chart review of patients without obesity treated with either topiramate or zonisamide at a clinic treating psychiatric conditions reported a mean reduction in BMI of 6.1 kg/m2 (n=47 patients) despite concurrent antipsychotic medication use, many of the latter known to cause weight gain.58,74
Thus, there appears to be both consistently observed appetite suppression and consequent weight reduction in adolescent patients treated with topiramate monotherapy for both seizure control and migraine prophylaxis, analogous to what has been described among adult patients on topiramate. Given this literature, clinical research sought to investigate topiramate as a pharmacotherapeutic agent in pediatric obesity. In 2019, Consoli et al conducted an eight-week, double-blind, randomized, placebo-controlled trial of topiramate (50–200 mg/day) in 62 individuals (both youth and adult, mean age of 24 years) with Prader Willi syndrome.51 While there were no significant reductions in mean BMI in the topiramate group compared to placebo, there was a significant improvement in the Dykens Hyperphagia Questionnaire (DHK) scores among the topiramate treated when compared to the control group.51
In 2015, Fox et al conducted a retrospective chart review of 28 youth with obesity (mean baseline BMI of 46.2 ± 10.3 kg/m2) attending a pediatric weight management program, on topiramate (25 to 125 mg daily) for six months in addition to LMT. At week 12, there was a significant decrease in %BMI of 2.5%, with an addition reduction by week 24 of 2.4% (p<0.001).49 In 2016, this same study group conducted a double-blinded, randomized, placebo-controlled trial of meal replacements followed by topiramate and compared to placebo, for the treatment of adolescents with severe obesity (n=21).50 Youth first underwent four weeks of meal replacement therapy, and then commenced 24 weeks of topiramate 75 mg daily or placebo. There were no significant differences in mean change in %BMI between topiramate and placebo at week 24 compared to baseline: ‒1.9% (p=0.3).50 Unfortunately, all three of these studies were of low quality due to small sample sizes and inadequate power to determine efficacy of topiramate compared to placebo; however, they do provide some indication of the benefits topiramate may provide in the management of pediatric obesity.
Phentermine/Topiramate Extended-Release Combination Therapy
Given the efficacy of individual phentermine and topiramate monotherapies for the treatment of obesity, a once-daily combination product was developed that allowed for use of both agents at lower doses, improving safety profiles, while also enhancing efficacy.36,39 This combination provides both immediate release phentermine for appetite reduction early in the day, and extended release [ER] topiramate for appetite reduction later in the day and into the evening.75,76 The combination phentermine/topiramate ER product is currently FDA approved at the following doses for chronic weight management in both adult and pediatric populations: 3.75 mg/23 mg, 7.5 mg/46 mg and 15 mg/92 mg (Table 2).36
 |
Table 2 Overview of Phentermine, Topiramate, and PHEN/TPM |
Mechanism of Action
As described above, the exact mechanism of action by which phentermine and topiramate works to reduce obesity has not been well elucidated in humans and thus the mechanism of action of the combination product remains uncertain as well.27–29 It has been postulated that the combination of a noradrenergic agonist effect from phentermine, in conjunction with topiramate, which acts on GABA-A receptors, induces greater decrease in caloric intake through appetite suppression than either taken as monotherapy.36,39
Pharmacokinetics and Pharmacodynamics
Phentermine/topiramate pharmacokinetics is dose dependent.77 Phentermine is primarily metabolized by cytochrome P450 (CYP) 3A4, whereas topiramate is metabolized by hydroxylation, hydrolysis, and glucuronidation. The phentermine terminal half-life is about 20 hours, and the mean topiramate ER half-life is about 65 hours.36,39 In contrast to the individual agents, Phentermine/topiramate ER is poorly bound by plasma proteins, does not undergo significant metabolism through induction of cytochrome P450 isoenzymes, and is mainly excreted in the urine unmetabolized.78,79
History of Combination Therapy in Obesity Treatment in Adults
In 1990, phentermine in combination with fenfluramine and dexfenfluramine became a popular weight-reducing agent for the treatment of obesity in adult cohorts known as Fen-Phen®.22,24–26 Fenfluramine itself was FDA-approved as a weight reduction agent in 1972, while dexfenfluramine was FDA-approved for weight loss monotherapy in 1996.25 The combination product, however, was for many years utilized off-label. In 1997, Connolly et al reported twenty-four cases of women on fenfluramine-phentermine developing valvular heart disease, with eight of these cases found to have new-onset pulmonary hypertension.80 By September 15, 1997, fenfluramine was withdrawn from the market and a black box warning was applied due to these concerns.80–83 Follow-up studies performed on fenfluramine and dexfenfluramine showed that over a third of individuals taking either agent developed abnormal cardiac valve findings which lasted for up to 24 months after stopping the agent.81 The evidence showed increased levels of circulating serotonin hyper-stimulating serotonin receptors on the cardiac valves, resulting in valve insufficiency, and leading to primary pulmonary hypertension (PPH). However, there is no evidence that phentermine monotherapy causes similar PPH.25,26,80,81
Phentermine/Topiramate, Once-Daily, Controlled-Release, Combination Product in Adults
In 2012, the phentermine/topiramate (PHEN/TPM), once-daily, controlled-release, combination product was FDA-approved for obesity management in adults.84,85 Containing both the immediate-release phentermine and the extended-release topiramate as a single daily dose, the following formulations are available: 3.75 mg/23 mg, 7.5 mg/46 mg, 11.25 mg/69 mg, and 15 mg/92 mg (phentermine/topiramate, respectively). This agent is indicated for adults with a BMI ≥ 30 kg/m2 or ≥ 27 kg/m2 with at least one weight-related comorbidity. To date, there have been three large, Phase III clinical trials exploring the efficacy, safety, and adherence of PHEN/TPM as a pharmacologic agent in the treatment of adult obesity, the studies frequently referred to by their trial names: EQUIP,86 CONQUER,84 and SEQUEL.85
EQUIP was a 56-week, randomized placebo-controlled trial with 1267 adults with obesity (mean BMI 42.0 kg/m2) randomized to one of three treatment arms: 1) PHEN/TPM 3.75/23 mg; 2) PHEN/TPM 15/92 mg; or 3) placebo. At week 56, compared to baseline, based on intention-to-treat analysis, both PHEN/TPM groups had a significant reduction in body weight of 10.9% in high dose and 5.1% in low dose, when compared to the 1.6% reduction in the placebo group. 67% of the high dose and 45% of the low dose participants achieved at least a 5% reduction in body weight compared to only 17% in the placebo group (p<0.0001). The high dose group experienced significant weight loss in the first 4 weeks, reaching 8–10% weight loss by week 12. There were no significant differences in heart rate profiles between groups over the study period. In contrast to baseline, there was a significant decrease in blood pressure in the treatment arms compared to placebo at week 56. Adverse effect-related dropouts were 8.4% in the placebo group, 11.3% in the low dose group, and 16.0% in the high dose group. The adverse events most commonly reported included paresthesia, dry mouth, constipation, dysgeusia, and insomnia and were reported in higher percentages in the high dose group compared to either the low dose or placebo.86
CONQUER was a 56-week, randomized, placebo-controlled trial with 2487 adults with obesity (mean BMI 36.6 ± 4.5 kg/m2) randomized to one of three treatment arms: 1) PHEN/TPM 7.5 mg/46 mg; 2) PHEN/TPM 15 mg/92 mg; or 3) placebo.84 At week 56 (compared to baseline), based on intention-to-treat analysis, both PHEN/TPM groups had a significant reduction in body weight, 9.8% in the high dose group, 7.8% in the mid dose group, and only 1.2% in the placebo group.70% of the high dose group and 62% of the mid dose group achieved at least a 5% reduction in body weight compared to only 21% in the placebo group (p<0.0001). Unlike EQUIP, there was a significant increase in heart rate over the study period of +1.7 beats per minute in the high dose group compared to both mid dose and placebo groups (p<0.01 and p = 0.003). Dose-related adverse events leading to discontinuation of the agent occurred at a rate of 9% in the placebo group, 12% in the mid dose group, and 19% in the high dose group. The most reported adverse events included paresthesia, dry mouth, constipation, dysgeusia, and insomnia and, as in the EQUIP study, were found in higher percentages in the high dose group compared to the mid dose or placebo groups.84
SEQUEL was an extension of the afore mentioned CONQUER trial, in which 676 adults with obesity in the CONQUER trial remained in the trial for an additional 52 weeks.85 By the end of this extension period, at a total study length of 108 weeks, the previously noted trends were maintained. At week 108 (compared to baseline), based on intention-to-treat analysis, there was a significant reduction in total body weight percentage of 10.5% in the high dose group, 9.3% in the mid dose group, and only 1.8% in the placebo group (p<0.001). Significantly more participants in the high (79%) and moderate (75%) dose PHEN/TPM groups were able to achieve 5% weight loss compared to placebo (30%; p<0.001) with more than 50% of the PHEN/TPM groups achieving ≥10% weight loss, and more than 24% achieving ≥15% weight loss.85 The treatment groups were found to have improvements in cardiometabolic variables, decreased triglycerides, decreased fasting glucose and insulin values, reduction in waist circumference, decreased incidence of diabetes, and decreased need for concomitant anti-hypertensive, lipid-lowering, and diabetes medications in comparison with the placebo group.85 The high dose PHEN/TPM group had a significant reduction in in systolic blood pressure of 1.2 mm Hg with an associated increase in heart rate of 2.4 beats per minute (mean heart rate 72.1 ± 9.9 beats per minute) compared to the placebo group.85
All three of the studies described above are considered to present high quality evidence, based on the Cochrane risk-of-bias 2.0 criteria. Four meta-analysis, and one systematic review of randomized controlled trials have been conducted investigating the efficacy and safety of PHEN/TPM in adults with obesity.39,87,88 Together, these studies have shown that PHEN/TPM results in statistically significant weight loss compared to placebo.87 All three studies emphasized a direct correlation between PHEN/TPM dose and degree of weight loss over time. PHEN/TPM resulted in average weight loss of 7–8 kg with associated improvement in cardiometabolic outcomes compared to placebo across all cohorts studied. Yanovski et al showed that the proportion of individuals achieving at least 5% weight loss with high dose PHEN/TMP was much greater than that for alternative oral obesity pharmacotherapies such as lorcaserin and orlistat.88 Shi et al conducted a systematic review and network meta-analysis of randomized controlled pharmacotherapy for adults with obesity and determined that the evidence supported phentermine-topiramate as the most effective agent for weight loss, followed by GLP-1 receptor agonists.87 However, further post-hoc analysis revealed that semaglutide is the most effective in achieving more than 5% weight reduction, when considering adverse events.87
PHEN/TPM as a Combination Therapy in Treatment of Obesity in Pediatrics
In 2022, Kelly et al conducted a 56-week, randomized, placebo-controlled, double-blind trial of PHEN/TPM plus lifestyle modification in adolescents with obesity.53 Adolescents with obesity (mean age of 14.0±1.4 years, mean BMI of 37.8±7.1 kg/m2) were randomized to either 1) placebo (n=56); 2) PHEN/TPM 7.5 mg/46 mg (n=54); or 3) PHEN/TPM 15 mg/92 mg (n=113) for the study duration. The primary end point was mean percent change in BMI from randomization to week 56.53 At week 56 (compared to baseline), based on intention-to-treat analysis, there was reduction in BMI percentage of 10.4% in the high dose group, 8.1% in the mid dose group, and a negligible 0.2% in the placebo group (p<0.001). There was a significant reduction in triglycerides (21%) and increase in high-density lipoprotein cholesterol (HDL-C; 10%) compared to placebo for both treatment arms. The study reported three serious adverse events (bile duct stone, depression, and suicidal ideation) in two participants who were both randomized to the PHEN/TPM 15 mg/92 mg group.
Side Effect Profile and Prescribing Considerations
The FDA has classified PHEN/TPM as a Schedule IV controlled substance. Common adverse events in clinical trials of PHEN/TPM were paresthesia, dizziness, dysgeusia, insomnia, constipation, palpitations, tachycardia, and dry mouth. Adverse events are generally dose related and mild to moderate in severity, occurring mostly during the titration period. There were low rates of serious adverse events reported, primarily classified as cardiac disorders. The contraindications for PHEN/TPM are comparable to those of phentermine and topiramate individual therapies. This medication should not be discontinued abruptly, as there is an increased risk of seizures. As with topiramate monotherapy, there is a teratogenic risk; thus, female patients of childbearing age should be apprised of the risk of birth defects and be strongly advised to utilize birth control.36,79
Prescribing Practices and Considerations in Pediatrics
Access
Given the increase in available obesity pharmacotherapies, their availability and cost across all cohorts and communities must be considered.89 Prescribing rates of obesity pharmacotherapies in pediatric cohorts remains under-studied. In 2021, members from the Pediatric Obesity Weight Evaluation Registry (POWER), in the United States published data regarding prescribing practice from 30 pediatric weight management programs.21 According to this data, in 2017, 53% of programs offered obesity pharmacotherapy, an increase of 19% when contrasted to the prescribing rates from the same programs in 2014. Metformin was reported as the most used agent in 2014, but by 2017, topiramate had ascended to the top spot. The largest reported increases in use over time were for topiramate and phentermine monotherapy.21
Despite phentermine having FDA approval for the treatment of obesity in adolescents ages 16 years and older, many insurance plans still do not cover its cost.90 As phentermine monotherapy has been available for many decades, phentermine tends to be fairly cost effective, allowing for many families to purchase this agent out-of-pocket. However, these out-of-pocket costs vary by country.89,90 In contrast, although topiramate does not have an FDA obesity indication in pediatrics, many insurers will cover it, given its other 2 pediatric indications. As with phentermine and owing to its historical usage and availability, topiramate tends not to be cost-prohibitive for many families opting to purchase it out-of-pocket if not covered under their insurance plan.89,90 For many payers, updates to their formularies and changes to the policies to add new medications and indications to their plans is both complicated and time-consuming. Although the combination product has recently obtained FDA approval, many payers have not yet included it on their formularies. In addition, many of these new agents have high baseline costs, requiring payers to determine how best to factor those baseline cost into their coverage analyses.90 PHEN/TPM is available in several different dose combinations, with escalating out-of-pocket costs which vary in relation to the dose increases. Thus, many clinicians elect to prescribe the agents separately, as a cost-saving approach.78
As an example, in the United States, a family can purchase a 30-day supply of phentermine 15-mg tablets, for $15/month, and a 30-day supply of topiramate, for $40/month. Whereas, a 30-day supply of the combination product, can cost up to $300/month.79 These prices certainly vary by country, region, patient age, and insurance; however, this example highlights the challenges to access faced by patients and their families, despite robust data regarding safety and efficacy of these agents. Nevertheless, it must be emphasized that, among the available obesity pharmacotherapy in pediatrics, phentermine and topiramate remain cost-effect options when compared to the newer GLP-1 agonists.
Dosing, Safety, and Monitoring
Currently, there are no universal dosing and monitoring guidelines for obesity pharmacotherapy in pediatric populations.21 Many institutions utilize single center protocols that incorporate consistent themes with regards to dosing and monitoring for these agents (Table 2).19 Phentermine monotherapy is available in 8 mg, 15 mg, 30 mg, and 37.5 mg tablets or capsules. Many clinicians opt to start at lower doses of 8 or 15 mg daily and monitor response to determine need for titration to a higher dose.19,91 Monitoring frequency differs by program. Many pediatric weight management programs will monitor blood pressure and heart rate trends over the first three months and assess BMI trajectory every one to three months to assess efficacy.6,17 Topiramate is titrated up slowly over 4–8 weeks, per standard practices outlined in pediatric neurology guidelines. Frequently, the patient is started on 25 mg nightly, increasing by 25 mg nightly each week, until reaching a target dose of 75 to 100 mg nightly, while being serially assessed for tolerability and efficacy.42,72 Typically, a maximum dose of 200 mg daily is set for pediatric obesity treatment. While there are no standard discontinuation rules for obesity pharmacotherapy, if the BMI continues to increase, or the patient experiences adverse side effects, most clinicians will transition to an alternative treatment modality.21
Discussion
Pediatric obesity is a multi-factorial, complex, chronic disease, that requires concurrent and frequently combination treatment with lifestyle modification, obesity pharmacotherapy, and bariatric surgery.2,6,7 The increasing availability of FDA-approved obesity pharmacotherapies for pediatric weight management provides clinicians with new and effective tools to treat this complex disease. While monotherapy with either phentermine or topiramate has been available for decades, PHEN/TPM is a once-daily, controlled-release, combination product that has a recent pediatric FDA indication, is safe, effective, and accessible as a treatment option for youth with obesity. The efficacy data is robust when compared to orlistat and phentermine monotherapy, the other two oral agents with FDA approval in this age group.9,10 The BMI reduction data for the combination product is only slightly inferior to the efficacy found with the GLP-1 agonists liraglutide (mean %BMI reduction 12%) and semaglutide (mean %BMI reduction 16%).15,92 Given the great heterogeneity of responses noted in obesity treatment, having multiple agents available allows clinicians to adopt a more personalized, precision medicine approach to identify the agent that is best suited for the individual youth and family.
Despite growing interest in the use of these agents in pediatric cohorts, the evidence remains limited and of generally low quality. There is an urgent need to design and conduct robust controlled trials to further investigate the safety, efficacy, and mechanism of action(s) of these agents in pediatric populations, both as monotherapy and in combination. The lack of high-quality evidence results in ongoing lower rates of utilization, despite additional agents obtaining pediatric FDA approval and clinical practice guidelines recommending their use as first-line treatment.21 This discrepancy appears to be related to the combination of limited medical training in (pediatric) obesity management, lack of clinical comfort with prescribing these agents, particularly in pediatrics and without satisfactory long-term safety and efficacy data, and both high costs and inadequate insurance coverage. Even though the efficacy and safety data of the available pharmacotherapy for obesity is promising, clinicians still demonstrate reluctance to prescribe these agents. These obstacles must be counteracted, by providing clinicians with suitable education regarding the efficacy data, safety of administration of these agents in pediatric cohorts, and the current FDA indications. Clinical workflows and increased comfort in prescribing these agents must be supported by increased advocacy to enable patients to obtain these much-needed agents at a reasonable cost and inclusive of all payers. Insurers must then see actuarial data that buttresses the argument that earlier and more aggressive intervention (in pediatrics) is preventative of later, devastating comorbidities (and their attendant costs to the healthcare system). Thus, enhanced awareness, both at the policy and clinical guidelines levels, must be encouraged and leveraged to support an equitable and accessible implementation of these agents into pediatric clinical care.
Abbreviations
BMI, Body mass index; zBMI, Body mass index Z-score; %BMIp95, Percent over the 95th percentile.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding
This work was supported by grants 1) K23DK134801 NIH NIDDK, 2) Sacchi Foundation Research Scientist, 3) Supported by American Diabetes Association grant #11-22-ICTSN-32, 4) The Southern California Center for Latino Health Pilot Award 2022, 5) UL1TR001855 and UL1TR000130 from the National Center for Advancing Translational Science (NCATS) of the US National Institutes of Health. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Disclosure
Dr Alaina P Vidmar reports non-financial support from Dexcom Inc., personal fees for product from Hippo Education Inc., personal fees for advisory board member in 2022 from Rythym Pharmaceutical, personal fees for educational consultant from Guidepoint, outside the submitted work. The authors report no other conflicts of interest relevant to this article.
References
1. Ogden CL, Fryar CD, Martin CB, et al. Trends in obesity prevalence by race and Hispanic origin - 1999-2000 to 2017–2018. JAMA. 2020;324(12):1208–1210. doi:10.1001/JAMA.2020.14590
2. Hampl SE, Hassink SG, Skinner AC, et al. Clinical practice guideline for the evaluation and treatment of children and adolescents with obesity. Pediatrics. 2023;151(2). doi:10.1542/PEDS.2022-060640
3. Jastreboff AM, Kotz CM, Kahan S, Kelly AS, Heymsfield SB. Obesity as a disease: the obesity society 2018 position statement. Obesity. 2019;27(1):7–9. doi:10.1002/OBY.22378
4. De Jesus JM. Expert panel on integrated guidelines for cardiovascular health and risk reduction in children and adolescents: summary report. Pediatrics. 2011;128(Suppl 5). doi:10.1542/PEDS.2009-2107C
5. Hales CM, Fryar CD, Carroll MD, Freedman DS, Ogden CL. Trends in obesity and severe obesity prevalence in US youth and adults by sex and age, 2007–2008 to 2015–2016. JAMA. 2018;319(16):1723–1725. doi:10.1001/JAMA.2018.3060
6. Raman V, Gupta A, Ashraf AP, et al. Pharmacologic weight management in the era of adolescent obesity. J Clin Endocrinol Metab. 2022;107(10):2716–2728. doi:10.1210/CLINEM/DGAC418
7. Czepiel KS, Perez NP, Campoverde Reyes KJ, Sabharwal S, Stanford FC. Pharmacotherapy for the treatment of overweight and obesity in children, adolescents, and young adults in a large health system in the US. Front Endocrinol. 2020;11:290. doi:10.3389/fendo.2020.00290
8. Kühnen P, Biebermann H, Wiegand S. Pharmacotherapy in childhood obesity. Horm Res Paediatr. 2022;95(2):177–192. doi:10.1159/000518432
9. Ozkan B, Bereket A, Turan S, Keskin S. Addition of orlistat to conventional treatment in adolescents with severe obesity. Eur J Pediatr. 2004;163(12):738–741. doi:10.1007/S00431-004-1534-6
10. Chanoine JP, Hampl S, Jensen C, Boldrin M, Hauptman J. Effect of orlistat on weight and body composition in obese adolescents: a randomized controlled trial. JAMA. 2005;293(23):2873–2883. doi:10.1001/JAMA.293.23.2873
11. Ryder JR, Kaizer A, Rudser KD, Gross A, Kelly AS, Fox CK. Effect of phentermine on weight reduction in a pediatric weight management clinic. Int J Obes. 2017;41(1):90–93. doi:10.1038/IJO.2016.185
12. Kelly AS, Auerbach P, Barrientos-Perez M, et al. A randomized, controlled trial of liraglutide for adolescents with obesity. N Engl J Med. 2020;382(22):2117–2128. doi:10.1056/NEJMOA1916038
13. Hsia DS, Gosselin NH, Williams J, et al. A randomized, double-blind, placebo-controlled, pharmacokinetic and pharmacodynamic study of a fixed-dose combination of phentermine/topiramate in adolescents with obesity. Diabetes Obes Metab. 2020;22(4):480–491. doi:10.1111/DOM.13910
14. Dhillon S. Phentermine/topiramate: pediatric first approval. Paediatr Drugs. 2022;24(6):715–720. doi:10.1007/S40272-022-00532-Z
15. Weghuber D, Barrett T, Barrientos-Pérez M, et al. Once-weekly semaglutide in adolescents with obesity. N Engl J Med. 2022;387(24):2245–2257. doi:10.1056/NEJMOA2208601
16. Johnson VR, Washington TB, Chhabria S, et al. Food as medicine for obesity treatment and management. Clin Ther. 2022;44(5):671–681. doi:10.1016/J.CLINTHERA.2022.05.001
17. Nicolucci A, Maffeis C. The adolescent with obesity: what perspectives for treatment? Ital J Pediatr. 2022;48(1). doi:10.1186/S13052-022-01205-W
18. Dabas A, Seth A. Prevention and management of childhood obesity. Indian J Pediatr. 2018;85(7):546–553. doi:10.1007/S12098-018-2636-X
19. Singhal V, Sella AC, Malhotra S. Pharmacotherapy in pediatric obesity: current evidence and landscape. Curr Opin Endocrinol Diabetes Obes. 2021;28(1):55–63. doi:10.1097/MED.0000000000000587
20. Elangovan A, Shah R, Smith ZL. Pharmacotherapy for obesity-trends using a population level national database. Obes Surg. 2021;31(3):1105–1112. doi:10.1007/S11695-020-04987-2
21. Borzutzky C, King E, Fox CK, et al. Trends in prescribing anti-obesity pharmacotherapy for paediatric weight management: data from the POWER Work Group. Pediatr Obes. 2021;16(1). doi:10.1111/IJPO.12701
22. Garrett SD, Cupp MJ. The fenfluramine/phentermine combination for weight loss. Nurse Pract. 1997;22(8):166, 168, 170.
23. Stunkard AJ. Anorectic agents lower a body weight set point. Life Sci. 1982;30(24):2043–2055. doi:10.1016/0024-3205(82)90445-3
24. Fishman AP. Aminorex to fen/phen: an epidemic foretold. Circulation. 1999;99(1):156–161. doi:10.1161/01.CIR.99.1.156
25. Torretta LK. Dexfenfluramine, fenfluramine, and phentermine for the treatment of morbid obesity. J Am Acad Nurse Pract. 1997;9(8):389–399. doi:10.1111/j.1745-7599.1997.tb01261.x
26. Howlin D. Fenfluramine and phentermine. Ann Intern Med. 2001;135(9):840–841. doi:10.7326/0003-4819-135-9-200111060-00018
27. Sehnert KW. Development of phentermine, an appetite-control drug. Clin Med. 1963;70:400–403.
28. Craig DDH. Chlorphentermine. Br Med J. 1963;2(5367):1269. doi:10.1136/bmj.2.5367.1269
29. Seaton DA, Rose K, Duncan LJP. A comparison of the appetite suppressing properties of dexamphetamine and phentermine. Scott Med J. 1964;9(11):482–485. doi:10.1177/003693306400901104
30. Ioannides-Demos LL, Proietto J, McNeil JJ. Pharmacotherapy for obesity. Drugs. 2005;65(10):1391–1418. doi:10.2165/00003495-200565100-00006
31. Lim S, Rogers LK, Tessler O, Mundinger GS, Rogers C, Lau FH. Phentermine: a systematic review for plastic and reconstructive surgeons. Ann Plast Surg. 2018;81(4):508. doi:10.1097/SAP.0000000000001478
32. Papasava M, Singer G, Papasava CL. Phentermine self-administration in naive free-feeding and food-deprived rats: a dose response study. Psychopharmacology. 1985;85(4):410–413. doi:10.1007/BF00429655
33. Becker BA. Pharmacologic activity of phentermine (phenyl-t-butylamine). Toxicol Appl Pharmacol. 1961;3(2):256–259. doi:10.1016/S0041-008X(61)80010-0
34. Go RE, Hwang KA, Kim SH, et al. Effects of anti-obesity drugs, phentermine and mahuang, on the behavioral patterns in Sprague-Dawley rat model. Lab Anim Res. 2014;30(2):73. doi:10.5625/LAR.2014.30.2.73
35. Klein S, Romijn JA. Obesity. In: Williams Textbook of Endocrinology. Elsevier; 2016:1633–1659. doi:10.1016/B978-0-323-29738-7.00036-8
36. Kiortsis DN. A review of the metabolic effects of controlled-release phentermine/topiramate. Hormones. 2013;12(4):507–516. doi:10.14310/HORM.2002.1438
37. Jo HS, Wang SM, Kim JJ. Recurrent Psychosis after Phentermine Administration in a Young Female: A Case Report. Clin Psychopharmacol Neurosci. 2019;17(1):130–133. doi:10.9758/cpn.2019.17.1.130
38. Murali S. Knowledge gaps in long-term phentermine use: making the case for maintenance. Obesity. 2019;27(8):1219. doi:10.1002/oby.22516
39. Lei XG, Ruan JQ, Lai C, Sun Z, Yang X. Efficacy and safety of phentermine/topiramate in adults with overweight or obesity: a systematic review and meta-analysis. Obesity. 2021;29(6):985–994. doi:10.1002/OBY.23152
40. Hung YM, Chang JC. Weight-reducing regimen associated with polymorphic ventricular tachycardia. Am J Emerg Med. 2006;24(6):714–716. doi:10.1016/j.ajem.2006.02.004
41. Phentermine: an appetite-suppressant amphetamine classified as a narcotic in France (Regulation). Prescrire Int. 2012;21(130):209.
42. Khalil NY, AlRabiah HK, Rashoud SS AL, Bari A, Wani TA. Topiramate: comprehensive profile. Profiles Drug Subst Excip Relat Methodol. 2019;44:333–378. doi:10.1016/BS.PODRM.2018.11.005
43. Hendricks EJ, Srisurapanont M, Schmidt SL, et al. Addiction potential of phentermine prescribed during long-term treatment of obesity. Int J Obes. 2014;38(2):292–298. doi:10.1038/IJO.2013.74
44. Lewis KH, Fischer H, Ard J, et al. Safety and effectiveness of longer-term phentermine use: clinical outcomes from an electronic health record cohort. Obesity. 2019;27(4):591–602. doi:10.1002/oby.22430
45. Ali Ibrahim AI, Mendoza B, Stanford FC, Malhotra S. Real-world experience of the efficacy and safety of phentermine use in adolescents: a case series. Child Obes. 2022. doi:10.1089/CHI.2022.0147
46. Lorber J. Obesity in childhood. A controlled trial of anorectic drugs. Arch Dis Child. 1966;41(217):309–312. doi:10.1136/ADC.41.217.309
47. Ryder JR, Kelly AS, Freedman DS. Metrics matter: toward consensus reporting of BMI and weight-related outcomes in pediatric obesity clinical trials. Obesity. 2022;30(3):571–572. doi:10.1002/OBY.23346
48. Rauh JL, Lipp R. Chlorphentermine as an anorexigenic agent in adolescent obesity. Report of its efficacy in a double-blind study of 30 teen-agers. Clin Pediatr. 1968;7(3):138–140. doi:10.1177/000992286800700305
49. Fox CK, Marlatt KL, Rudser KD, Kelly AS. Topiramate for weight reduction in adolescents with severe obesity. Clin Pediatr. 2015;54(1):19–24. doi:10.1177/0009922814542481
50. Fox CK, Kaizer AM, Rudser KD, et al. Meal replacements followed by topiramate for the treatment of adolescent severe obesity: a pilot randomized controlled trial. Obesity. 2016;24(12):2553–2561. doi:10.1002/OBY.21633
51. Consoli A, Çabal Berthoumieu S, Raffin M, et al. Effect of topiramate on eating behaviours in Prader-Willi syndrome: TOPRADER double-blind randomised placebo-controlled study. Transl Psychiatry. 2019;9(1). doi:10.1038/S41398-019-0597-0
52. Berman C, Naguib M, Hegedus E, Vidmar AP, Topiramate for Weight Management in Children With Severe Obesity. Child Obes. 2023;19(4):219–225. doi:10.1089/chi.2022.0062
53. Kelly AS, Bensignor MO, Hsia DS, et al. Phentermine/topiramate for the treatment of adolescent obesity. NEJM Evidence. 2022;1(6). doi:10.1056/EVIDOA2200014
54. Boxill GC, M BEN, Hillyard IW, Warren MR. The cardiovascular and extravascular smooth muscle actions of chlorphentermine hydrochloride (p-chloro-alpha, alpha-dimethylphenethylamine)-a new anorexigenic agent. J Pharmacol Exp Ther. 1962;137:198–205.
55. Tahrani AA, Morton J. Benefits of weight loss of 10% or more in patients with overweight or obesity: a review. Obesity. 2022;30(4):802–840. doi:10.1002/oby.23371
56. Horn DB, Almandoz JP, Look M. What is clinically relevant weight loss for your patients and how can it be achieved? A narrative review. Postgrad Med. 2022;134(4):359–375. doi:10.1080/00325481.2022.2051366
57. Glauser TA. Topiramate. Epilepsia. 1999;40(SUPPL. 5):s71–s80. doi:10.1111/J.1528-1157.1999.TB00922.X
58. Shapiro M, Reid A, Olsen B, Taasan M, McNamara J, Nguyen M. Topiramate, zonisamide and weight loss in children and adolescents prescribed psychiatric medications: a medical record review. Int J Psychiatry Med. 2016;51(1):56–68. doi:10.1177/0091217415621266
59. Kramer CK, Leitão CB, Pinto LC, Canani LH, Azevedo MJ, Gross JL. Efficacy and safety of topiramate on weight loss: a meta-analysis of randomized controlled trials. Obes Rev. 2011;12(5):e338–e347. doi:10.1111/J.1467-789X.2010.00846.X
60. Rawls SM, Thomas T, Adeola M, et al. Topiramate antagonizes NMDA- and AMPA-induced seizure-like activity in planarians. Pharmacol Biochem Behav. 2009;93(4):363–367. doi:10.1016/J.PBB.2009.05.005
61. Turenius CI, Htut MM, Prodon DA, et al. GABA(A) receptors in the lateral hypothalamus as mediators of satiety and body weight regulation. Brain Res. 2009;1262:16–24. doi:10.1016/J.BRAINRES.2009.01.016
62. Turenius CI, Charles JR, Tsai DH, et al. The tuberal lateral hypothalamus is a major target for GABAA--but not GABAB-mediated control of food intake. Brain Res. 2009;1283:65–72. doi:10.1016/J.BRAINRES.2009.05.064
63. Miner P, Borkuhova Y, Shimonova L, Khaimov A, Bodnar RJ. GABA-A and GABA-B receptors mediate feeding elicited by the GABA-B agonist baclofen in the ventral tegmental area and nucleus accumbens shell in rats: reciprocal and regional interactions. Brain Res. 2010;1355:86–96. doi:10.1016/J.BRAINRES.2010.07.109
64. Antel J, Hebebrand J. Weight-reducing side effects of the antiepileptic agents topiramate and zonisamide. Handb Exp Pharmacol. 2012;209:433–466. doi:10.1007/978-3-642-24716-3_20/FIGURES/1_20
65. Liang Y, She P, Wang X, Demarest K. The messenger RNA profiles in liver, hypothalamus, white adipose tissue, and skeletal muscle of female Zucker diabetic fatty rats after topiramate treatment. Metabolism. 2006;55(10):1411–1419. doi:10.1016/J.METABOL.2006.06.013
66. Sweeting AN, Tabet E, Caterson ID, Markovic TP. Management of obesity and cardiometabolic risk - role of phentermine/extended release topiramate. Diabetes Metab Syndr Obes. 2014;7:35–44. doi:10.2147/DMSO.S38979
67. Tennis P, Chan KA, Curkendall SM, et al. Topiramate use during pregnancy and major congenital malformations in multiple populations. Birth Defects Res a Clin Mol Teratol. 2015;103(4):269–275. doi:10.1002/BDRA.23357
68. Rafi SK, Goering JP, Olm-Shipman AJ, et al. Anti-epileptic drug topiramate upregulates TGFβ1 and SOX9 expression in primary embryonic palatal mesenchyme cells: implications for teratogenicity. PLoS One. 2021;16(2):e0246989. doi:10.1371/JOURNAL.PONE.0246989
69. Green MW, Seeger JD, Peterson C, Bhattacharyya A. Utilization of topiramate during pregnancy and risk of birth defects. Headache. 2012;52(7):1070–1084. doi:10.1111/j.1526-4610.2012.02190.x
70. Margulis AV, Mitchell AA, Gilboa SM, et al. Use of topiramate in pregnancy and risk of oral clefts. Am J Obstet Gynecol. 2012;207(5):405.e1–405.e7. doi:10.1016/j.ajog.2012.07.008
71. Mines D, Tennis P, Curkendall SM, et al. Topiramate use in pregnancy and the birth prevalence of oral clefts. Pharmacoepidemiol Drug Saf. 2014;23(10):1017–1025. doi:10.1002/pds.3612
72. Mikaeloff Y, De Saint-Martin A, Mancini J, et al. Topiramate: efficacy and tolerability in children according to epilepsy syndromes. Epilepsy Res. 2003;53(3):225–232. doi:10.1016/S0920-1211(03)00028-7
73. Winner P, Pearlman EM, Linder SL, Jordan DM, Fisher AC, Hulihan J. Topiramate for migraine prevention in children: a randomized, double-blind, placebo-controlled trial. Headache. 2005;45(10):1304–1312. doi:10.1111/J.1526-4610.2005.00262.X
74. Arnone D. Review of the use of topiramate for treatment of psychiatric disorders. Ann Gen Psychiatry. 2005;4(1). doi:10.1186/1744-859X-4-5
75. Bays H. Phentermine, topiramate and their combination for the treatment of adiposopathy (‘sick fat’) and metabolic disease. Expert Rev Cardiovasc Ther. 2010;8(12):1777–1801. doi:10.1586/ERC.10.125
76. Johnson DB, Quick J. Topiramate and phentermine. StatPearls; 2023. Available from: https://pubmed.ncbi.nlm.nih.gov/29489234/.
77. Smith SM, Meyer M, Trinkley KE. Phentermine/topiramate for the treatment of obesity. Ann Pharmacother. 2013;47(3):340–349. doi:10.1345/APH.1R501
78. Aronne LJ, Wadden TA, Peterson C, Winslow D, Odeh S, Gadde KM. Evaluation of phentermine and topiramate versus phentermine/topiramate extended-release in obese adults. Obesity. 2013;21(11):2163–2171. doi:10.1002/OBY.20584
79. Kartal Ö, Kartal AT. Phentermine plus topiramate for weight reduction: more tolerable and effective? Clin Pediatr. 2015;54(3):302. doi:10.1177/0009922814566935
80. Connolly HM, Crary JL, McGoon MD, et al. Valvular heart disease associated with fenfluramine-phentermine. N Engl J Med. 1997;337(9):141. doi:10.1056/NEJM199708283370901
81. Weigle DS. Pharmacological therapy of obesity: past, present, and future. J Clin Endocrinol Metab. 2003;88(6):2462–2469. doi:10.1210/JC.2003-030151
82. Jordan J, Astrup A, Engeli S, Narkiewicz K, Day WW, Finer N. Cardiovascular effects of phentermine and topiramate: a new drug combination for the treatment of obesity. J Hypertens. 2014;32(6):1178–1188. doi:10.1097/HJH.0000000000000145
83. Griffen L, Anchors M. Asymptomatic mitral and aortic valve disease is seen in half of the patients taking “phen-fen”. Arch Intern Med. 1998;158(1):102. doi:10.1001/ARCHINTE.158.1.102
84. Gadde KM, Allison DB, Ryan DH, et al. Effects of low-dose, controlled-release, phentermine plus topiramate combination on weight and associated comorbidities in overweight and obese adults (CONQUER): a randomised, placebo-controlled, Phase 3 trial. Lancet. 2011;377(9774):1341–1352. doi:10.1016/S0140-6736(11)60205-5
85. Garvey WT, Ryan DH, Look M, et al. Two-year sustained weight loss and metabolic benefits with controlled-release phentermine/topiramate in obese and overweight adults (SEQUEL): a randomized, placebo-controlled, phase 3 extension study. Am J Clin Nutr. 2012;95(2):297–308. doi:10.3945/AJCN.111.024927
86. Allison DB, Gadde KM, Garvey WT, et al. Controlled-release phentermine/topiramate in severely obese adults: a randomized controlled trial (EQUIP). Obesity. 2012;20(2):330–342. doi:10.1038/OBY.2011.330
87. Shi Q, Wang Y, Hao Q, et al. Pharmacotherapy for adults with overweight and obesity: a systematic review and network meta-analysis of randomised controlled trials. Lancet. 2022;399(10321):259–269. doi:10.1016/S0140-6736(21)01640-8
88. Yanovski SZ, Yanovski JA. Long-term drug treatment for obesity: a systematic and clinical review. JAMA. 2014;311(1):74–86. doi:10.1001/JAMA.2013.281361
89. Li J, Reaven NL, Funk SE, McGaughey K, Neovius M. 4-year cost trajectories in real-world patients matched to the metabolic profiles of trial subjects before/after treatment with phentermine-topiramate. Drugs Real World Outcomes. 2015;2(2):143–151. doi:10.1007/S40801-015-0021-X
90. Gómez Lumbreras A, Tan MS, Villa-Zapata L, Ilham S, Earl JC, Malone DC. Cost-effectiveness analysis of five anti-obesity medications from a US payer’s perspective. Nutr Metab Cardiovasc Dis. 2023;33(6):1268–1276. doi:10.1016/J.NUMECD.2023.03.012
91. Fox CK, Kelly AS. Pharmacotherapy for severe obesity in children. Clin Pediatr. 2015;54(13):1302. doi:10.1177/0009922815580407
92. Tamborlane WV, Barrientos-Pérez M, Fainberg U, et al. Liraglutide in children and adolescents with type 2 diabetes. N Engl J Med. 2019;381(7):637–646. doi:10.1056/NEJMOA1903822
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.