")
Back to Journals » Open Access Surgery » Volume 17
A Metastatic Follicular Thyroid Carcinoma to Clavicle and Sternum: A Case Report
Authors Negasa GA, Bayleyegn NS, Merga OT, Gebremariyam ZT, Woldemariam ST
Received 26 November 2023
Accepted for publication 8 February 2024
Published 13 February 2024 Volume 2024:17 Pages 35—41
DOI https://doi.org/10.2147/OAS.S451821
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Luigi Bonavina
Gemechu Abera Negasa, Nebiyou Simegnew Bayleyegn, Osias Tilahun Merga, Zenebe Teklu Gebremariyam, Samuel Tesfaye Woldemariam
Department of Surgery, Faculty of Medicine, Institute of Health, Jimma University, Jimma, Ethiopia
Correspondence: Samuel Tesfaye Woldemariam, Department of Surgery, Faculty of Medicine, Institute of Health, Jimma University, Jimma, Ethiopia, Tel +251911554180, Email [email protected]
Introduction: The incidence of thyroid cancer has increased in the last few decades, and follicular thyroid cancer (FTC) is the second most common differentiated thyroid cancer. Metastases outside the neck occur in 10% to 20% of patients with differentiated thyroid cancer and the most frequent locations are the lungs and bones.
Case presentation: A 35 years old female patient presented with anterior neck swelling of 3 years duration and anterior chest swelling of 2 years duration. Objectively, there is a multilobulated 10 * 8 cm anterior neck mass, which is hard and moves with deglutition. She has 7*9 cm midline anterior chest mass, which is hard and also 3*3 cm hard mass on the medial end of the right clavicle. FNAC from the thyroid gland shows follicular carcinoma with the anterior chest mass of secondary deposits of similar malignant cells. Neck and chest CT scans were taken that showed enlargement of bilateral thyroid lobes showing internal flecks of calcifications with heterogeneously enhancing malignant sternal mass with lytic destruction of sternal cortex measuring 9*7*6 cm in widest dimensions and right medial clavicular mass, which is 2*3*2 cm with lytic destruction of the cortex. The patient was managed with total thyroidectomy + proximal clavicle resection + sternectomy + chest wall reconstruction. Postoperatively the patient stayed in the ward for 12 days and the course was uneventful, and both serum calcium and thyroid function tests were normal and discharged with levothyroxine.
Conclusion: Patients with follicular thyroid carcinoma can present with multiple metastasis to flat bone at initial presentation. Individuals who present with resectable bony metastatic follicular thyroid cancer best be treated aggressively with thyroidectomy, resection of the bony metastasis and levothyroxine in a resource-limited setting were radio iodine ablation therapy is not available.
Keywords: metastatic follicular carcinoma, clavicular metastasis, sternal metastasis, sternectomy, chest wall reconstruction
Introduction
The thyroid gland, consisting of two connected lobes, is one of the largest endocrine glands in the human body, weighing 20–30 g in adults. Thyroid lesions are often found on the gland, with a prevalence of 4–7%. Most of them are asymptomatic, and thyroid hormone secretion is normal.1 The incidence of thyroid cancer has increased over the last few decades and is common in women.2,3 Follicular thyroid cancer (FTC) is the second most common differentiated thyroid cancer, which accounts for approximately 10–15% of all thyroid cancers.4
Metastases outside the neck occur in 10% to 20% of patients with differentiated thyroid cancer and the most frequent locations are the lungs and bones.5
Bone metastases are more common in FTC than PTC. The spinal and pelvic bones are the most frequently involved, followed by the chest, extremities, shoulder girdle, and craniomaxillofacial bones.3,5 Bone involvement was multiple in 59.3% of 86 patients with thyroid cancer and bone metastasis.6
Radioactive iodine therapy is the gold-standard treatment modality for metastatic thyroid cancer. The results of ablation therapy are good for lung metastases, but bone metastases cannot be cured with ablation therapy alone.7
Surgery is indicated as a first-line therapy in individual patients and should be advocated in cases of solitary bone metastasis amenable to resection.7,8 Individuals who present with metastatic FTC should therefore be treated aggressively with thyroidectomy, radioiodine ablation, and resection of the metastasis where possible.4
Here, we present the case of a 35 yrs old female patient with metastatic follicular carcinoma of the sternum and clavicle, who was managed with total thyroidectomy, proximal clavicle resection, sternectomy, and chest wall reconstruction according to the Surgical case report (SCARE) 2020 guidelines.9
Case Presentation
A 35 years old female patient presented to our hospital with anterior neck swelling of 3 years duration. She also had anterior chest swelling for 2 years. She had no neck pain, chest swelling, dysphagia, dyspnea, or dysphonia. The patient showed no symptoms of toxicity. Objectively, there is a multilobulated 10 * 8 cm anterior neck mass that is non-tender, hard, moves with deglutition, and the lower border is reachable. There was also a 7*9 cm midline anterior chest mass, which was hard and fixed to the underlying structure, as well 3*3 cm hard mass on the medial end of the right clavicle.
The thyroid function test results were normal. Neck ultrasonography showed a diffuse, heterogeneously enlarged thyroid gland. FNAC of the thyroid gland shows follicular carcinoma with an anterior chest mass of secondary deposits of malignant cells, similar to the smear of the thyroid gland.
The neck and chest CT scan showed likely benign enlargement of the bilateral thyroid lobes on the right side, internal flecks of calcifications, and no cervical lymphadenopathy with heterogeneously enhancing malignant sternal mass with lytic destruction of the sternal cortex with an associated soft tissue component measuring 9 × 7 × 6 cm in the widest dimensions and a right medial clavicular mass of 2 × 3 × 2 cm with lytic destruction of the cortex (Figure 1). CT tomography revealed no evidence of pleural or lung deposits. Echocardiography revealed no abnormalities.
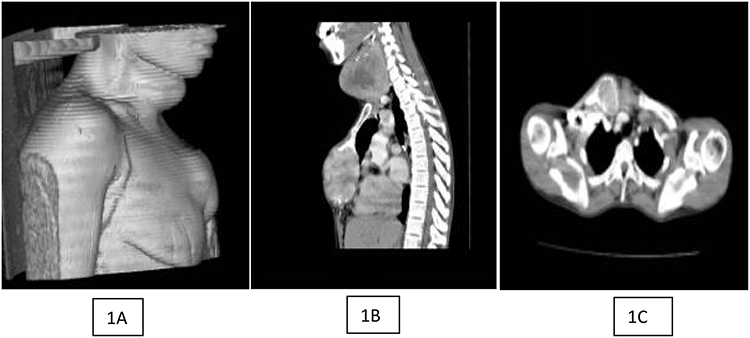 |
Figure 1 Chest CT scan showing thyroid enlargement with metastatic right clavicular mass and sternal mass. (A) 3D reconstruction (B): Sagittal view (C): Axial view showing right medial clavicular metastatic mass. |
The patient was informed about her illness, and after discussions with a multidisciplinary team, which includes General, Cardiothoracic, and Plastic and Reconstructive surgeons about possible management options, the patient was admitted to the surgical ward after taking informed consent.
The patient was placed in the operating room and in the supine position. The neck and chest were prepped and draped, and total thyroidectomy and therapeutic central node dissection were performed initially through a Kocher transverse collar incision. The intraoperative finding revealed diffusely enlarged and hardened right lobe and a diffusely enlarged soft left lobe of the thyroid. Three enlarged level six cervical lymph nodes were also identified and resected. During thyroidectomy, bilaterally both recurrent laryngeal nerves and parathyroid glands were visualized and spared.
After thyroidectomy, the surgical incision was extended through the midline anterior chest, and the medial or proximal clavicle mass, which was 3 × 3 cm, was dissected away from the sternocleidomastoid and scalene muscle, disarticulated at the sternoclavicular joint, and excised from the distal half of the clavicle. Anterior chest skin and pectoralis flaps were raised bilaterally. The sternal mass (Figure 2), which was 7 × 9 × 4 cm, was excised along with the costochondrium starting from rib 3, including the xiphoid, and dissected from the anterior mediastinum and pleura, and homeostasis was secured. A bilateral chest tube was inserted into the pleural cavity and placed under a water seal (Figure 3).
 |
Figure 2 Intraoperative picture of the sternal mass after thyroidectomy and medial clavicular partial resection. |
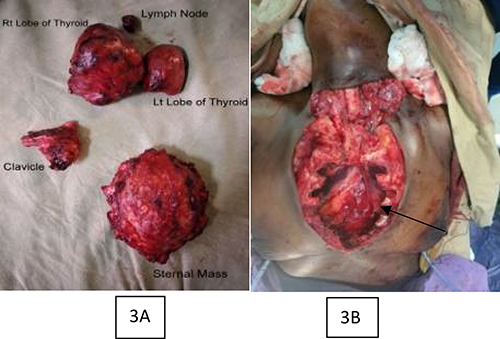 |
Figure 3 (A): Specimen of total thyroidectomy plus level 6 lymph node and the resected clavicular and sternal mass (B): Chest wall defect after sternectomy done. |
Chest wall reconstruction made by initially making a wire bridge between the free edges of bilateral ribs starting from rib 3 to rib 6 after which sterile propylene mesh 15*15 cm is placed on the wire bridge and fixed circumferentially to the underlying chest wall and bilateral pectoralis major advancement flap is done (Figure 4) and chest wall drainage left bilaterally in the subcutaneous space and skin closed. The patient was transferred with stable vital signs intraoperatively and transfused with one unit of cross-matched whole blood.
 |
Figure 4 Intraoperative picture showing chest wall reconstruction done by bridging wire, propylene mesh and bilateral pectoralis major advancement flap. (A) Propylene mesh fixed over a bridging sternal wire connecting opposite side rib 3 to 6 (B): Bilateral pectoralis major advancement flap over the mesh. |
Postoperatively, the patient stayed in the ward for 12 days, the course was uneventful, both serum calcium and thyroid function tests were normal, and the patient was discharged with levothyroxine. Histopathological examination revealed follicular carcinoma and secondary deposits in the resected clavicular and sternal mass (Figure 5). The patient was clinically stable, and the wound healed with no chest wall deformities or functional problems. TSH and serum calcium levels were normal in the 3rd post op month, and she was on follow-up (Figure 6).
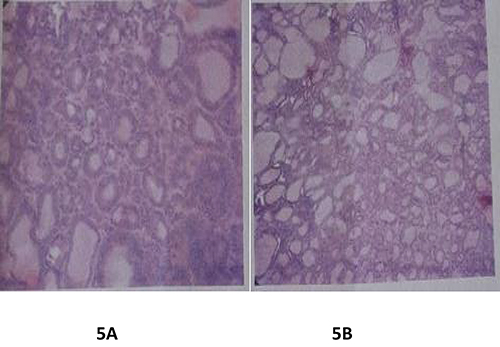 |
Figure 5 Slides showing histology of resected thyroid and chest wall mass. (A). Section showing variable increased small follicles along with sheets of malignant follicular cells having features of capsular and vascular invasion (B). Tissue sent from resected chest wall mass showing similar malignant cells with formation of colloid filled follicles. |
 |
Figure 6 Post op picture of the patient taken at follow-up clinic. |
Discussion
Differentiated thyroid cancer (ie, Papillary, Follicular, and Hürthle cell) comprises the vast majority (>90%) of all thyroid cancers. Of the differentiated cancers, follicular carcinomas of the thyroid are less common than papillary carcinomas of the thyroid.2
Patients with differentiated thyroid carcinoma can have distant metastases at the initial presentation.10 Half of the cases were present when the tumor was first discovered, whereas the others were found later.3 The most common sites of metastasis are the lungs and bones, with bone metastases being more common in FTC (7–28%).5 Clavicular and sternal metastases from differentiated thyroid cancer are uncommon.11,12 Our patient initially presented with multiple bone metastases in the sternum and clavicle.
Fine-needle aspiration cytology (FNAC) is a very useful diagnostic tool with high sensitivity and predictive value for diagnosis of thyroid malignancy. The Bethesda System for Reporting Thyroid Cytopathology (BSRTC) uses six categories for thyroid cytology reporting (I –nondiagnostic, II – benign, III – atypia of undetermined significance (AUS)/follicular lesion of undetermined significance (FLUS), IV – follicular neoplasm/suspicious for follicular neoplasm (SFN), V – suspicious for malignancy, and VI – malignant and the rate of malignancy increases from 1.53% in II and 15 to 40% in III–IV13,14), and FNAC from our patients thyroid gland showed follicular carcinoma (Bethesda VI) with the anterior chest mass of secondary deposits of similar malignant cells to the smear of thyroid gland. The diagnosis of follicular thyroid carcinoma is confirmed after analysis of histological sections obtained from lobectomy or thyroidectomy specimens showing tumor capsular or vascular invasion by follicular cells.2 In our patient, histology of the surgical specimens revealed follicular carcinoma with secondary deposits in the bones (Figure 5).
Surgery is the management of choice for differentiated (ie, papillary, follicular, Hürthle cell) thyroid carcinoma, followed by radioactive iodine (RAI) ablation (iodine-131) in selected patients and thyroxin therapy in most patients.2,3
For patients with thyroid cancer >4 cm, or with gross extra thyroidal extension (clinical T4), clinically apparent metastatic disease to nodes (clinical N1), or distant sites (clinical M1), the initial surgical procedure should include a near-total or total thyroidectomy and gross removal of all primary tumors unless there are contraindications to this procedure.15
Although there are controversies over the best approaches and complication rates after subtotal and total thyroidectomy, total thyroidectomy can be safely performed in patients with differentiated thyroid carcinoma without increasing the risk of early complications.16
Therapeutic central compartment (level VI) neck dissection for patients with clinically involved central nodes following total thyroidectomy to clear the central neck. Therapeutic lateral neck compartment lymph node dissection should be performed in patients with biopsy-confirmed metastatic lateral cervical lymphadenopathy.17 In our patient, total thyroidectomy with therapeutic central lymph node dissection was done because there were three lymph nodes were identified intraoperatively at level six.
Surgical resection of distant bony metastases in patients with DTC is recommended as it can be curative, provide symptomatic palliation, or allow for more effective radioiodine treatment.18 Surgical excision of clavicular and sternal masses was done in our patient with clavicular and sternal metastases. Currently, ligaSure vessel (LS) or harmonic scalpel (HS) can be used to secure homeostasis, and both devices exhibit identical safety profiles in thyroidectomies specifically regarding major bleeding complications that require reoperation. Additionally, HS was found to be more effective at achieving hemostasis, especially in the subgroup of patients with thyroid carcinoma, though we used hand tie technique and electro cautery because both instruments (LS, HS) are not available in our setting.19
RAI remnant ablation is routinely recommended after thyroidectomy for ATA high with ATA-high-risk DTC, including follicular carcinoma with distant metastases.12,17 Decreased recurrence and cancer-specific mortality rates for differentiated thyroid carcinoma have been reported in patients treated with thyroid hormone-suppressive therapy.2 Although radioactive iodine ablative therapy was indicated for our patient, it was not available in our setup, and she was administered levothyroxine.
Only a few cases of sternal metastasis arising from follicular thyroid carcinoma have been reported in literature.20 Thyroid carcinoma with metastasis, particularly to the sternum, is challenging to manage. A multidisciplinary team approach is paramount, including radio-oncologists, radiologists, and several surgical subspecialties such as cardiothoracic and plastic surgery15,21 as in our case where surgery was done by general surgeon, cardiothoracic surgeon, and plastic surgeons.
Sternal resection with mesh reconstruction of the chest wall defect proved to be a simple and effective method for managing sternal metastasis.12,20,22 Our patient was managed with partial sternectomy, the defect was closed with sternal wire, mesh, and pectoral muscle flap over it, and the skin was closed primarily (Figures 4 and 6).
The prognosis and clinical outcomes of patients with metastatic follicular thyroid cancer are poorer than those of patients without metastases. Resecting osseous metastasis, where possible, using an aggressive surgical approach may improve survival in patients with FTC.4,22
Conclusion
Patients with follicular thyroid carcinoma can initially present with multiple metastases to the flat bone.
Individuals who present with resectable bony metastatic follicular thyroid cancer best be treated aggressively with thyroidectomy, resection of the bony metastasis and levothyroxine in a resource-limited setting were radio iodine ablation therapy is not available.
A multidisciplinary team approach is paramount for managing thyroid carcinomas with metastasis, particularly to the sternum. Sternal resection and chest wall reconstruction with sternal wire, mesh, and bilateral pectoral muscle flap should be considered in the management of sternal metastasis.
Abbreviations
FTC, Follicular thyroid carcinoma; PTC, Papillary thyroid carcinoma; SCARE, Surgical case report; FNAC, Fine needle aspiration cytology; TSH, Thyroid stimulating hormone; RIA, Radio iodine ablation; T, Tumor; N, Node; M, Metastasis.
Ethical Consideration
As this was a case report, institutional approval for publication was not required. However, the patient provided verbal consent to publish the case and the images, which were approved by the Jimma University ethics committee. Verbal consent was obtained, and the details were stored in a file.
Acknowledgment
We thank the patient for providing consent to report this case.
Credit Authorship Contribution Statement
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
None.
Disclosure
The authors declare that they have no conflicts of interest related to this work.
References
1. Mulita F, Anjum F. Thyroid adenoma. In: Stat Pearls. Treasure Island (FL): StatPearls Publishing; 2023.1.
2. Haddad RI, Bischoff L, Ball D, et al. Thyroid carcinoma, version 2.2022, NCCN clinical practice guidelines in oncology. J Nat Compr Cancer Net. 2022;20(8):925–951. doi:10.6004/jnccn.2022.0040
3. Filetti S, Durante C, Hartl D, et al. Thyroid cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2019;30(12):1856–1883. doi:10.1093/annonc/mdz400
4. Parameswaran R, Shulin Hu J, Min En N, Tan W, Yuan N. Patterns of metastasis in follicular thyroid carcinoma and the difference between early and delayed presentation. Annals. 2017;99(2):151–154. doi:10.1308/rcsann.2016.0300
5. Osorio M, Moubayed SP, Su H, Urken ML. Systematic review of site distribution of bone metastases in differentiated thyroid cancer: bone metastases in thyroid cancer. Head Neck. 2017;39(4):812–818. doi:10.1002/hed.24655
6. Matta-Coelho C, Simões-Pereira J, Vilar H, Leite V. Bone metastases from thyroid carcinoma of follicular origin: a single Institutional experience. Eur Thyroid J. 2019;8(2):96–101. doi:10.1159/000494719
7. Meyer A, Behrend M. Partial resection of the sternum for osseous metastasis of differentiated thyroid cancer: case report. Anticancer Res. 2005;25(6C):4389–4392.
8. Id El Haj N, Hafidi S, Karam R, Boubia S, Karkouri M, Ridai M. Sternal metastasis as first manifestation of a papillary thyroid carcinoma: a case report. Int J Surg Case Rep. 2021;80:105663. doi:10.1016/j.ijscr.2021.105663
9. Agha RA, Franchi T, Sohrabi C, et al. The SCARE 2020 guideline: updating consensus surgical case report (SCARE) guidelines. Int j Surg. 2020;84:226–230. doi:10.1016/j.ijsu.2020.10.034
10. Lee J, Soh EY. Differentiated thyroid carcinoma presenting with distant metastasis at initial diagnosis: clinical outcomes and prognostic factors. Ann Surg. 2010;251(1):114–119. doi:10.1097/SLA.0b013e3181b7faf6
11. Gonzalez MNG, Palomo AS, Torres JHL. Cardiac metastasis from anaplastic thyroid carcinoma. J Endocr. 2021;5(Supplement_1):A885–A885. doi:10.1210/jendso/bvab048.1807
12. Isolated Sternal AA. Metastasis arising from well differentiated thyroid carcinoma. IJCTS. 2017;3(6):67. doi:10.11648/j.ijcts.20170306.11
13. Mulita F, Iliopoulos F, Tsilivigkos C, et al. Cancer rate of Bethesda category II thyroid nodules. medicinski glasnik ljekarske komore zenicko-dobojskog kantona. Med Glas. 2022;6:1. doi:10.17392/1413-21
14. Mulita F, Plachouri MK, Liolis E, Vailas M, Panagopoulos K, Maroulis I. Patient outcomes following surgical management of thyroid nodules classified as Bethesda category III (AUS/FLUS). Endokrynol Pol. 2021;72(2):143–144. doi:10.5603/EP.a2021.0018
15. Syazni MA. Follicular thyroid cancer with sternal metastasis - challenges and outcomes. Med J Malaysia. 2017;72:1.
16. Mulita F, Verras GI, Dafnomili VD, et al. Thyroidectomy for the management of differentiated thyroid carcinoma and their outcome on early postoperative complications: a 6-year single-centre retrospective study. Chr. 2022;117(5):556. doi:10.21614/chirurgia.2736
17. Haugen BR, Alexander EK, Bible KC, et al. 2015 American thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American thyroid association guidelines task force on thyroid nodules and differentiated thyroid Cancer. Thyroid. 2016;26(1):1–133. doi:10.1089/thy.2015.0020
18. Yanagawa J, Abtin F, Lai CK, et al. Resection of thyroid cancer metastases to the sternum. J Thorac Oncol. 2009;4(8):1022–1025. doi:10.1097/JTO.0b013e3181adef20
19. Comparison of postoperative bleeding using harmonic scalpel and LigaSure in thyroid surgery: a 15-year single-centre retrospective study; 2024. Available from: https://pubmed.ncbi.nlm.nih.gov/37585298/.
20. Ishinaga H, Miyamura T, Tenpaku H, Takeuchi K. Metastasis of thyroid cancer to the sternum after total thyroidectomy and laryngectomy. Case Rep Sur. 2013;2013:1–3. doi:10.1155/2013/346246
21. Moraitis S, Perelas A, Toufektzian L, Mazarakis N, Pechlivanides G. Giant sternal metastasis secondary to follicular carcinoma of the thyroid gland: report of a case. Surg Today. 2012;42(9):895–898. doi:10.1007/s00595-012-0192-y
22. Thobani H, Abbas M, Pervez M, Fatimi S. Follicular variant of papillary thyroid carcinoma: sternal resection to treat recurrent aggressive bone metastasis. Chest. 2020;157(6):A35. doi:10.1016/j.chest.2020.05.039
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.