")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 17
A Case of Persistent Pityriasis Rosea Successfully Treated by a Short Course of Therapy with Abrocitinib
Authors Wu H , Ji QJ, Xu YY, Zhu JW
Received 30 December 2023
Accepted for publication 24 March 2024
Published 12 April 2024 Volume 2024:17 Pages 843—846
DOI https://doi.org/10.2147/CCID.S455060
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Hao Wu, Qing-Jie Ji, Yu-Yang Xu, Jian-Wei Zhu
Department of Dermatology, Quzhou TCM Hospital at the Junction of Four Provinces Affiliated to Zhejiang Chinese Medical University, Quzhou, People’s Republic of China
Correspondence: Jian-Wei Zhu, Email [email protected]
Abstract: Pityriasis rosea (PR) is a common inflammatory, erythematous and scaly skin condition that usually affects individuals aged from 20 to 40 years old. The disease often exhibits a self-limiting course up to 6– 8 weeks. We report a 25-year-old female patient with a six-month history of red scaly rashes on the trunk and proximal limbs, accompanied by severe pruritus that has been remained ineffective conventional treatments. She was diagnosed as persistent pityriasis rosea. As abrocitinib has been proved to be effective for many inflammatory diseases, therefore in this case, we tried abrocitinib for the patient, and a good result had been achieved.
Keywords: pityriasis rosea, abrocitinib, JAK-STAT pathway
Introduction
Pityriasis rosea (PR) is a common skin condition characterized by reddish-colored and scaling lesions, typically affecting the trunk and proximal extremities. There is increasing evidence that pityriasis rosea is associated with reactivation of human herpes virus-6 (HHV-6) and/or human herpes virus-7 (HHV-7).1–3 With the emergence of the SARS-CoV-2 (COVID-19) pandemic, the possible viral role in PR eruptions was proposed once again.4 Generally considered a self-limited disease, PR typically lasts 6–8 weeks,5 while in less common situations, it can last longer than 12 weeks which is called persistent pityriasis rosea.6 Traditional treatment with oral antihistamines or topical and oral corticosteroids is advised based on expert consensus. Other treatment options are available including sunlight, artificial UV therapy and antiviral agents. However, the long-lasting, multiple itching lesions can cause significant discomfort, leading to anxiety and depression in some patients with persistent PR. Therefore, more aggressive treatment can be tried for some of these patients.
Case Report
A 25-year-old female patient presented to our clinic with a 6-month history of red scaly rashes on the trunk and proximal limbs, accompanied by severe pruritus. Dermatological examination showed coin-sized, round or oval-shaped, red scaly papules on her back, chest and abdomen, most of the rashes were along the lines of skin cleavage. Her Auspitz sign was negative (Figure 1A and B). According to the signs and symptoms of the patient, a diagnosis of pityriasis rosea was made, which was identical to that made by her previous physicians who had given therapies including oral antihistamines and topical corticosteroids with unsatisfactory results. The patient refused systemic therapy with oral or intra-muscular glucocorticoids as she had severe acne meanwhile, and she was inconvenient to receive narrow-band ultraviolet B therapy due to conflict with her work time. With sufficient communication and informed consent, we tried to initiate off-label use of abrocitinib (Pfizer, USA) for her, with a dosage of 100 mg orally per day. Two days after taking the drug, her pruritus was significantly relieved (Figure 2A and B), and the red skin lesions completely disappeared with residual pigmentation only after a 14-day course of treatment (Figure 3A and B).
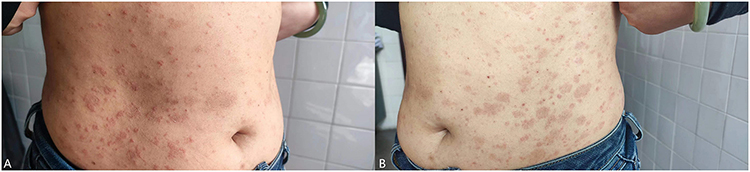 |
Figure 1 (A and B) Patient at baseline. |
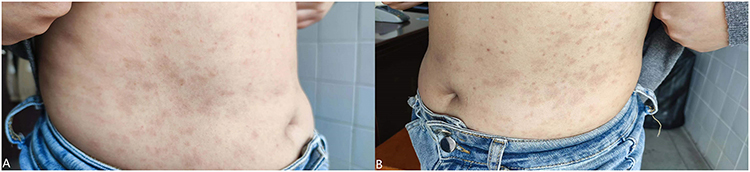 |
Figure 2 (A and B) After treatment of 2 days. |
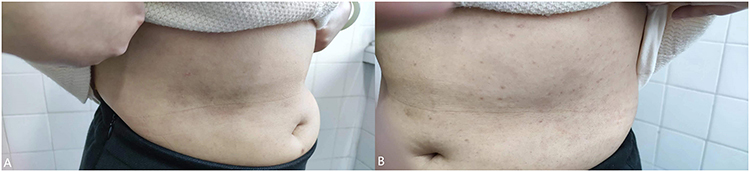 |
Figure 3 (A and B) 14 days after treatment with abrocitinib. |
Discussion
Pityriasis rosea is a common inflammatory, erythematous and scaly skin condition that usually affects individuals aged from 20 to 40 years old, with a peak incidence in the spring and fall seasons.7,8 Skin lesions typically start from a “herald patch” and develop into numerous smaller lesions on the trunk and extremities along the lines of skin cleavage.9 The disease often exhibits a self-limited course up to 6–8 weeks. Treatment options include oral antihistamines, topical corticosteroids and phototherapy. Some studies have suggested a potential association between pityriasis rosea and viral infections.6,10 In small studies with fewer than 100 patients, those who took acyclovir, 800 mg five times per day for seven days, had significant improvements in symptoms and lesion resolution.11–13 Notably, a small subset of patients experienced a prolonged course lasting beyond 12 weeks, which had been defined as persistent pityriasis rosea by Drago et al.6 These patients usually have severely pruritic skin lesions that do not respond well to conventional treatment, making management of the disease challenging.
The exact pathogenesis of pityriasis rosea remains unclear. Neoh et al identified a lack of natural killer cells and B cell activity in active lesions, indicating a predominantly T-cell-mediated immune response.10 Mokadem et al demonstrated the role of IL-22 through its proinflammatory cytokines in the inflammatory process of pityriasis rosea.14 Immunohistochemical studies further supported the significant role of T lymphocyte-mediated cellular immunity in the pathogenesis of pityriasis rosea.15
The JAK-STAT pathway is an intracellular signaling pathway closely associated with many cytokines, participating in various critical biological processes such as cell proliferation, differentiation, apoptosis and immune regulation. JAK inhibitors have been clinically used in the treatment of several immune-related diseases by targeting Janus kinases to interrupt signaling and transcription activation. Abrocitinib is a selective JAK1 inhibitor approved for atopic dermatitis worldwide. Moreover, abrocitinib has also been proved to be effective for other inflammatory diseases.16–19 Therefore in this case, we believed that abrocitinib could be useful for patients with persistent pityriasis rosea at least in alleviating skin rashes and improving severe pruritus by blocking the various inflammatory cytokine pathways.
Conclusion
The patients of persistent pityriasis rosea usually do not respond well to conventional treatment, making management of the disease challenging. Surprisingly as a result, a short course of therapy with abrocitinib completely resolved the patient’s problem, suggesting that abrocitinib can be considered as an alternative option for patients with persistent pityriasis rosea.
Ethics Statement
The study protocol was approved by the Institutional Review Board of the Quzhou TCM Hospital at the junction of four provinces affiliated to Zhejiang Chinese Medical University. Written informed consent was obtained from the patient for publication of this report and accompanying images.
Funding
This study received no external funding.
Disclosure
The authors have no conflicts of interest to declare for this work.
References
1. Rebora A, Drago F, Broccolo F. Pityriasis rosea and herpesviruses: facts and controversies. Clin Dermatol. 2010;28(5):497–501. doi:10.1016/j.clindermatol.2010.03.005
2. Chuh AA, Chiu SS, Peiris JS. Human herpesvirus 6 and 7 DNA in peripheral blood leucocytes and plasma in patients with pityriasis rosea by polymerase chain reaction: a prospective case control study. Acta Derm Venereol. 2001;81(4):289–290. doi:10.1080/00015550152572958
3. Broccolo F, Drago F, Careddu AM, et al. Additional evidence that pityriasis rosea is associated with reactivation of human herpesvirus-6 and −7. J Invest Dermatol. 2005;124(6):1234–1240. doi:10.1111/j.0022-202X.2005.23719.x
4. Potestio L, Martora F, Cacciapuoti S, et al. Pityriasis rosea and pityriasis rosea-like eruption following COVID-19 vaccination: a narrative review. Clin Cosmet Invest Dermatol. 2024;17:51–57. eCollection 2024. doi:10.2147/CCID.S447834
5. Litchman G, Nair PA, Le JK Pityriasis rosea. Treasure Island (FL); 2022.
6. Drago F, Broccolo F, Ciccarese G, et al. Persistent pityriasis rosea: an unusual form of pityriasis rosea with persistent active HHV-6 and HHV-7 infection. Dermatology. 2015;230(1):23–26. doi:10.1159/000368352
7. González L-M, Robert A, Camila-Krysicka J, et al. Pityriasis rosea: an important papulosquamous disorder. Int J Dermatol. 2005;9:757–764. doi:10.1111/j.1365-4632.2005.02635.x
8. John-C B. An update on pityriasis rosea and other similar childhood exanthems. Curr Opin Pediatr. 2009;4:481–485. doi:10.1097/MOP.0b013e32832db96e
9. Leung A-K-C, Lam J-M, Leong K-F, et al. Pityriasis rosea: an updated review. Curr Pediatr Rev. 2021;3:201–211. doi:10.2174/1573396316666200923161330
10. Neoh C-Y, Tan A-W-H, Mohamed K, et al. Characterization of the inflammatory cell infiltrate in herald patches and fully developed eruptions of pityriasis rosea. Clin Exp Dermatol. 2009;3:300–304. doi:10.1111/j.1365-2230.2009.03469.x
11. Drago F, Vecchio F, Rebora A. Use of high-dose Acyclovir in pityriasis rosea. J Am Acad Dermatol. 2006;54(1):82–85. doi:10.1016/j.jaad.2005.06.042
12. Ganguly S. A randomized, double-blind, placebo-controlled study of efficacy of oral Acyclovir in the treatment of pityriasis rosea. J Clin Diagn Res. 2014;8(5):YC01–YC04. doi:10.7860/JCDR/2014/8140.4360
13. Das A, Sil A, Das NK, et al. Acyclovir in pityriasis rosea: an observer-blind, randomized controlled trial of effectiveness, safety and tolerability. Indian Dermatol Online J. 2015;6(3):181–184. doi:10.4103/2229-5178.156389
14. Mokadem S-A, Ghonemy S, Zidan A, et al. The role of interleukin-22 in pityriasis rosea. Clin Exp Dermatol. 2016;1:30–35. doi:10.1111/ced.12976
15. Wang S, Fu L, Du W, et al. Subsets of T lymphocytes in the lesional skin of pityriasis rosea. Anais brasileiros de dermatologia. 2019;1:52–55. doi:10.1590/abd1806-4841
16. Xia J, Jiang G. A report of eruptive pruritic papular porokeratosis treated with abrocitinib. Clin Cosmet Invest Dermatol. 2023;16:2223–2227. doi:10.2147/CCID.S424310
17. Zhang J, Zuo YG. Successful treatment of alopecia universalis with abrocitinib: a case report. J DermatolTreat. 2023;34(1):2242706. doi:10.1080/09546634.2023.2242706
18. Ren M, Yang X, Teng Y, et al. Successful treatment of granulomatous rosacea by JAK inhibitor abrocitinib: a case report. Ren Clin Cosmet Investig Dermatol. 2023;16:3369–3374. doi:10.2147/CCID.S440138
19. Teng Y, Ren M, Ding Y, et al. A case of perioral dermatitis successfully treated with abrocitinib. Clin Cosmet Invest Dermatol. 2023;16:3035–3038. doi:10.2147/CCID.S433561
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.