")
Back to Journals » International Medical Case Reports Journal » Volume 17
A Case of a Young Military Officer with Bilateral Simultaneous Femoral Neck Stress Fracture
Authors Khired ZA
Received 7 March 2023
Accepted for publication 4 September 2023
Published 19 February 2024 Volume 2024:17 Pages 131—135
DOI https://doi.org/10.2147/IMCRJ.S411460
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Zenat Ahmed Khired
Department of Surgery, Faculty of Medicine, Jazan University, Jazan, 45142, Saudi Arabia
Correspondence: Zenat Ahmed Khired, Email [email protected]
Abstract: Stress fractures of the femoral neck are rare in young adults and usually happen when the bone is repeatedly put under a lot of stress or because of a bone disease. The incidence of stress fractures is a major health concern for soldiers. Most often, stress fractures affect the metatarsals and tibias, while injuries to the femoral neck are less common. Exertional groin or anterior thigh discomfort that develops gradually over time is often vague and subtle; therefore, a high index of clinical suspicion is indicated. In most cases, the first radiographs will be normal. In order to properly diagnose a stress fracture in the femur, a CT scan is very helpful. Because most femoral neck fractures are not displaced when patients present with them, a diagnosis is often delayed. In conclusion, new military soldiers feeling hip pain should have a thorough medical evaluation to establish an early diagnosis and prevent any consequences.
Keywords: femoral neck, stress fractures, young adults, FNSF
Introduction
Stress femoral neck fractures are uncommon in young, healthy people, but they happen often in soldiers. It is accountable for 1% of adult stress fractures. Bilateral femoral neck stress fractures (FNSF) affect around 3% of adults, the majority of whom are new military recruits.1 The majority of FNSF conditions are non-displaced. Fracture displacement is associated with a poor prognosis and numerous complications, thus early diagnosis is crucial.2,3 Young patients with FNSF may be fired from their jobs because of the long healing duration, frequent sick days, and comorbidities including non-union, persistent discomfort, and avascular necrosis at the femoral neck.4
The displacement of fractures and their consequences may be avoided with early identification and careful follow-up of those who have a history of severe groin pain during exercise.5 Patients typically present with anterior groin pain and an inability to bear weight. Limited range of motion, limping, and other symptoms such as shortening are commonly reported in displaced neck femur fractures.6 Pain with external and internal hip rotation is possible, although tenderness to palpation is uncommon; early radiographs of the hip failed to detect stress fractures in 30–70% of cases.7 Therefore, early diagnosis of the FNSF. Additionally, if a femoral neck fracture is suspected, an internal rotation hip view may reveal nondisplaced or impacted fractures.
Case Report
A 24-year-old man who had been in the military for three months and was physically active went to a field clinic one month after starting field training because his right hip hurt. He visited the field clinic more than once, and they diagnosed him as having adductor hip tendinitis with muscle spasm, nothing shown at an early radiographic examination. He returns to field training exercises. Three weeks later, his pain became severe, and he cannot stand on his lower limb. Physical examination revealed minimal shortening of the right lower limb. The patient had notable atrophy in the right gluteal region and thigh. Tenderness to palpation of the hip joint with limited range of motion in all directions Left hip anterior groin pain was elicited just inferior to the iliac crest, with a slightly decreased stance phase on the left lower extremity. The patient has pain in his left hip when the hip is abducted, flexed, and externally rotated. Strength and sensation were intact in both lower extremities. Reflexes were normal and symmetrical. All relevant biochemical and hormonal routine tests were normal for the patient. Radiographic examination by plain X-ray showed a displaced right intracapsular neck femur fracture (Figure 1) and an occult left intracapsular neck femur fracture (Figure 1). The patient underwent a computed tomography (CT) on his pelvis, which revealed the presence of a displaced right intracapsular neck femur fracture (Figure 2) and a nondisplaced left intracapsular neck femur fracture (Figure 2) in the coronal section. This is confirmed by the axial pelvic CT, which shows the same findings in the coronal plane (Figure 3). The fractures were reduced and stabilized with 7.0 mm cannulated screws bilaterally (Figure 4). Excellent fixation and compression across the fracture site were obtained. No intraoperative or postoperative complications occurred. He resumed training with some limitations three months after the surgery. He is participating in all prior activities without restriction nine months following surgery.
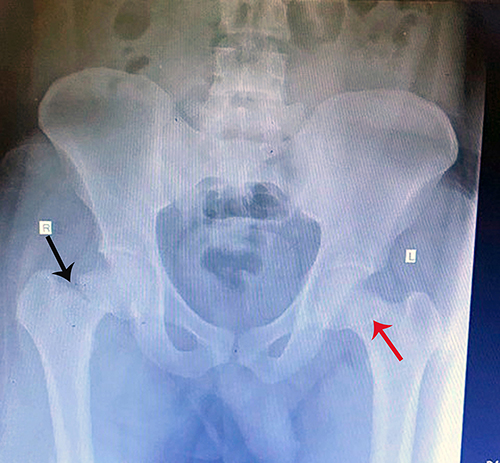 |
Figure 1 Antero-posterior (AP) radiograph showing the right neck of the femur with an intracapsular displaced fracture (black arrow). On the left side, the x-ray shows an occult fracture in the neck of the femur (red arrow). |
 |
Figure 2 A coronal view of a computerized tomography (CT) shows an intracapsular displaced fracture in the neck of the right femur (black arrow). On the left femur neck, the nondisplaced fracture is clearly seen (red arrow). |
 |
Figure 3 An axial CT scan reveals an intracapsular displaced fracture of the right femur neck (black arrow). There is a nondisplaced femoral neck fracture on the left side (red arrow). |
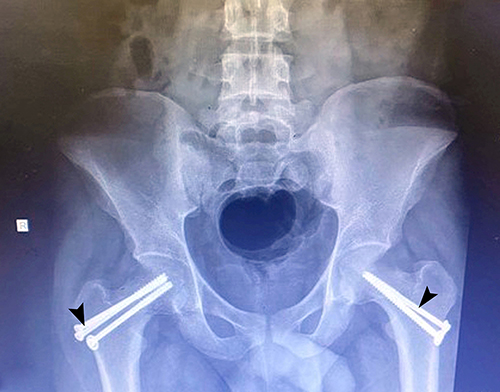 |
Figure 4 An anteroposterior radiograph of the 7.0 mm cannulated screws (arrowheads) implanted bilaterally to the neck femur on both the right and left sides of the body. |
Discussion
The FNSF is caused by mechanical failure due to repeated large strains along the femoral neck during activities that focus almost entirely on the lower extremities. At the femoral neck, compressive-type forces dominate.4,7 In terms of the quality of new recruit training and the emergence of symptoms, these studies provide a clear explanation of what occurred to the soldier in this research. Moreover, running is the major cause of FNSF among young athletes. Increased exercise intensity, hard surfaces, improper footwear, or incorrect training procedures induce bone resorption.5 This comes in line with that: exercise intensity, metabolic problems, smoking, and prior stress fractures increase femoral stress fracture risk. Hip geometry, or coxa vara, may be a factor in femoral stress fractures.6,8,9
Most individuals with FNSF have groin pain and trouble bearing weight. Extreme internal and external rotational pain is uncomfortable, although tenderness is rare. Displaced neck fractures often cause limb shortening. Analgesic gait and restricted range of motion are also frequent complaints.3,10 Alongside, patients with FNSF had smaller thigh muscles and worse levels of physical fitness than those who did not suffer a fracture.11 It is possible that this might explain what happened in our case, given that he was just picked for military deployment.
This report says that the soldier’s health got worse in the twelve weeks between when he joined the army and when the investigation began. The following studies shed light on the development of the case: The most common population with femoral neck stress fractures is parachute recruits. Symptoms often appeared between weeks 13 and 16 of training.12 FNSF are the most prevalent injuries resulting in basic training discharge. FNSF are more common among basic military trainees (BMTs) than the general military community. FNSF sufferers are four times more likely to be medically discharged from basic training.13 As well, this type of trauma is becoming increasingly common among civilians.14
Internal fixation with cannulated screws or a sliding hip screw (SHS) is the most popular contemporary surgical treatment option for injuries that do not respond to conservative measures.15 Subsequently, the use of internal fixation with cannulated screws, which was used in this case and was quite effective, was in line with what earlier research had shown.
Conclusion
In summary, young men who join the military and have never been hurt before having been shown to be at risk for FNSF. Difficulty in diagnosis comes from improper history-taking and physical examination. CT and X-rays work together to provide a powerful diagnostic tool. Since FNSF may lead to discharge and a long rehabilitation, new military recruits with hip pain should be carefully evaluated. Early diagnosis prevents complications.
Informed Consent Statement
Informed written consent was obtained from the patient for the publication of this report and any accompanying images. Ethical approval has been taken from Jazan University.
Funding
No funding was received for this study.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Fonte H, Rodrigues-Pinto R. Femoral neck stress fracture in a young female recruit: case report. SICOT-J. 2018;4:1–5. doi:10.1051/sicotj/2018011
2. Clough TM. Femoral neck stress fracture: the importance of clinical suspicion and early review. Br J Sports Med. 2002;36(4):308–309. doi:10.1136/bjsm.36.4.308
3. Johansson C, Ekenman I, Tornkvist H, Eriksson E. Stress fractures of the femoral neck in athletes: the consequence of a delay in diagnosis. Am J Sports Med. 1990;18(5):524–528. doi:10.1177/036354659001800514
4. Cichy B, Roche SJ, Wozniak A. Atypical femoral neck stress fracture in a marathon runner: a case report and literature review. Ir J Med Sci. 2012;181(3):427–429. doi:10.1007/s11845-010-0599-7
5. Polacek M, Småbrekke A. Displaced stress fracture of the femoral neck in young active adults. BMJ Case Rep. 2010;2010:bcr0220102749. doi:10.1136/bcr.02.2010.2749
6. Yavuz NC. Femoral neck stress fracture in a 21 years female: a case report. Int J Phys Med Rehabil. 2018;3:430–431.
7. Neubauer T, Brand J, Lidder S, Krawany M. Stress fractures of the femoral neck in runners: a review. Res Sports Med. 2016;24(3):283–297. doi:10.1080/15438627.2016.1191489
8. Kim DK, Kim TH. Femoral neck shaft angle in relation to the location of femoral stress fracture in young military recruits: femoral head versus femoral neck stress fracture. Skelet Radiol. 2021;50(6):1163–1168. doi:10.1007/s00256-020-03661-z
9. Carpintero P, Leon F, Zafra M, Serrano-Trenas JA, Roman M. Stress fractures of the femoral neck and coxa vara. Arch Orthop Trauma Surg. 2003;123(6):273–277. doi:10.1007/s00402-003-0514-z
10. Avrahami D, Pajaczkowski JA. Femoral neck stress fracture in a female athlete: a case report. J Chiropr Med. 2012;11(4):273–279. doi:10.1016/j.jcm.2012.05.010
11. Yoon HK, Ryu YK, Song DG, Yoon BH. Femoral neck stress fractures in South Korean male military recruits. Clin Orthop Surg. 2021;13(1):24. doi:10.4055/cios20074
12. Talbot JC, Cox G, Townend M, Parker PJ, Langham M. Femoral neck stress fractures in military personnel–a case series. BMJ Mil Health. 2008;154(1):47–50.
13. Kupferer KR, Bush DM, Cornell JE, et al. Femoral neck stress fracture in Air Force basic trainees. Mil Med. 2014;179(1):56–61. doi:10.7205/MILMED-D-13-00154
14. Bernstein EM, Kelsey TJ, Cochran GK, Deafenbaugh BK, Kuhn KM. Femoral neck stress fractures: an updated review. JAAOS. 2022;30(7):302–311. doi:10.5435/JAAOS-D-21-00398
15. Kolaczko JG, McMellen CJ, Magister SJ, Wetzel RJ. Comparison of time to healing and major complications after surgical fixation of nondisplaced femoral neck stress fractures: a systematic review. Injury. 2021;52(4):647–652. doi:10.1016/j.injury.2021.02.046
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.