")
Back to Journals » Blood and Lymphatic Cancer: Targets and Therapy » Volume 13
90Yttrium Ibritumomab Tiuxetan (Zevalin) for the Treatment of Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma: A Report of 5 Cases
Authors Wang J , Baidoun F, Tun HW , Alhaj Moustafa M
Received 23 December 2022
Accepted for publication 7 September 2023
Published 3 October 2023 Volume 2023:13 Pages 59—65
DOI https://doi.org/10.2147/BLCTT.S398809
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Wilson Gonsalves
Jing Wang,1 Firas Baidoun,2 Han W Tun,2 Muhamad Alhaj Moustafa2
1Department of Internal Medicine, Mayo Clinic Florida, Jacksonville, FL, 32224, USA; 2Division of Hematology and Medical Oncology, Mayo Clinic Florida, Jacksonville, FL, 32224, USA
Correspondence: Muhamad Alhaj Moustafa, Mayo Clinic Florida, Division of Hematology/Oncology, 4500 San Pablo Road S, Jacksonville, FL, 32224, USA, Tel +1 904-953-2000, Email [email protected]
Abstract: Radioimmunotherapy (RIT) with radio-labeled monoclonal antibodies to CD20 produces a high response rate in patients with low-grade B-cell lymphomas. The use of this modality in patients with chronic lymphocytic leukemia (CLL) has been sporadic in clinical trials and was hampered by the extensive marrow involvement seen commonly in patients with CLL, which would produce a high risk for marrow aplasia after treatment with RIT. Herein, we report our experience with RIT in 5 patients with CLL or SLL showing short-lived responses and significant myelosuppression. After 90Y-ibritumomab tiuxetan treatment, the median time to relapse was 65 days, and no cases of MDS or AML were observed during follow-up. All patients experienced grade ≥ 3 thrombocytopenia and neutropenia, with median durations of 39.5 days and 107 days, respectively.
Keywords: CD20, chronic lymphocytic leukemia, small lymphocytic lymphoma, radioimmunotherapy, targeted irradiation, Zevalin
Introduction
Chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) is a common type of mature B-cell neoplasm, characterized by the clonal proliferation and accumulation of mature B-cells within the blood, bone marrow, lymph nodes, and spleen.1 CLL is considered one of the indolent non-Hodgkin lymphomas (NHL) and has identical pathologic and immunophenotypic features as SLL. The term CLL is used when the disease manifests primarily in the blood, while SLL is used when involvement is primarily nodal.1,2 Only patients with progressive, symptomatic disease, or with advanced Binet or Rai stages require therapy.2 However, in most patients CLL/SLL progresses over time and requires multiple lines of therapies.3 CLL/SLL treatment has evolved from the use of chemotherapeutic agents to non-chemotherapeutic agents after the introduction of anti-CD20 monoclonal antibodies, BCL2 inhibitors, and BTK inhibitors.4 Radioimmunotherapy (RIT) is a modality that has been sporadically used in the treatment of CLL/SLL.3,5 RIT combines biologic and radiologic mechanisms to target and destroy tumor cells and has been an advancement in the treatment of patients with B-cell NHL.6 Two RIT agents have been approved by the United States Food and Drug Administration (US FDA) for the treatment of relapsed CD20+ NHL: yttrium Y 90 (90Y) ibritumomab tiuxetan and iodine I-131 tositumomab. Both agents work by binding to the B-cell CD20 antigen, which is present on most B-cell lymphocytes related malignancies.7,8 90Y ibritumomab tiuxetan is the only commercially available product. It comprises the radiolabeled isotope 90yttrium, a murine monoclonal antibody ibritumomab, and a linker chelator tiuxetan. It is efficacious in the treatment of B-cell NHL.6,9 The primary toxicity with 90Y-ibritumomab tiuxetan use in the standard doses is a transient delayed myelosuppression.10,11 Data regarding radioimmunotherapy treatment of CLL/SLL is limited. In this case series, we review 5 cases where 90Y-ibritumomab tiuxetan was used to treat CLL/SLL.
Materials and Methods
A retrospective analysis was conducted on a case series of patients diagnosed with chronic lymphocytic leukemia (CLL) who received 90Y-IT (yttrium-90 ibritumomab tiuxetan) treatment at Mayo Clinic between January 2000 and December 2020. The study aimed to evaluate the effectiveness and safety of 90Y-IT in CLL patients. All patients diagnosed with CLL who received 90Y-IT treatment during the specified timeframe were included in the study. No exclusion criteria were applied, ensuring that all patients meeting the diagnostic criteria for CLL and receiving 90Y-IT treatment were included for analysis. Patient data were meticulously collected from electronic medical records (EMRs) and other pertinent medical documentation.
Case 1
A 66-year-old male with a history of coronary artery bypass surgery (CABG), and a diagnosis of CLL 10 years before presentation was referred to our institution for management of CLL. His absolute neutrophil count was 6.05 × 109/L, white cell count was 10.3 × 109/L, hemoglobin was 14.9 × 109/L and platelets count was 161 × 109/L. Peripheral blood flow cytometry was positive for CD5, CD19, CD20, CD23, CD 38 and HLADR B lymphocytes. Fluorescence in situ hybridization (FISH) analysis on peripheral blood showed 16% of lymphocytes with 16% 13q deletion and 36% with 17p deletion. Quantitated immunoglobulins revealed panhypogammaglobulinemia with IgG of 279 mg/dL, IgM of 41 mg/dL, and IgA of 22 mg/dL.
Two years after diagnosis, the patient was treated with 4 doses of rituximab weekly with apparent transient improvement in adenopathy and leukocytosis. However, due to further progression of his adenopathy, he was treated with the combination of rituximab, cyclophosphamide, vincristine, and prednisone (R-CVP). The treatment was complicated by pseudomonas osteomyelitis involving the right skull base, and pseudomonas sepsis. Computed tomography (CT) scan of the chest, abdomen, and pelvis a year later showed progressive disease with bilateral axillary lymphadenopathy, extensive abdominal adenopathy, and right adrenal mass. He was treated with 12 weeks of alemtuzumab with further progression. Due to progression of CLL despite multiple lines of salvage regimen, he was treated with 90Y-ibritumomab tiuxetan. Pre-treatment bone marrow biopsy was negative for lymphoma.
After 90Y-ibritumomab tiuxetan treatment, patient experienced significant neutropenia and thrombocytopenia. Patient developed neutropenic fever. The nadir platelet count was 22x109/L at 28 days post 90Y-ibritumomab tiuxetan infusion and recovered on day 190 post 90Y-ibritumomab tiuxetan infusion. The nadir of absolute neutrophil counts (ANC) was 0.2 x109/L at 36 days after 90Y-ibritumomab tiuxetan infusion and recovered 65 days post 90Y-ibritumomab tiuxetan infusion. The patient did not require granulocyte stimulating factor (GCSF) support. Unfortunately, CT scan 2 months after treatment showed worsening lymphadenopathy. The patient was later treated with 3 cycles of rituximab and high dose IV Solu-Medrol. His disease course was complicated by multiple aspirations and a large right-sided chylothorax requiring pleuroperitoneal shunt. He passed away soon after the shunt placement.
Case 2
A 48-year-old male with diabetes mellitus, hypertension, renal stones, recurrent sinusitis and sinopulmonary infections, hypogammaglobulinemia, and bronchiectasis presented to our institution with lymphadenopathy, night sweats, and unintentional weight loss. He was diagnosed with stage IV SLL.
Patient was initially treated with R-CHOP for 8 cycles achieving partial response (PR) but progressed after 4 months. Patient was treated with 90Y-ibritumomab tiuxetan. The patient achieved stable disease (SD) to therapy on a CT scan after one month. Unfortunately, 5 months after treatment with 90Y-ibritumomab tiuxetan, CT scan of the chest, abdomen, and pelvis showed evidence of progression of disease with increase in the size of mediastinal, subcarinal, peripancreatic, and retroperitoneal lymph nodes.
The pretreatment bone marrow biopsy involvement was <5%. FISH showed 81% 13q deletion. After 90Y-ibritumomab tiuxetan treatment, patient experienced significant neutropenia and thrombocytopenia. The nadir platelet count was 16x109/L at 34 days post 90Y-ibritumomab tiuxetan infusion and recovered on day 58 post infusion. The nadir of absolute neutrophil counts (ANC) was 0.3 x109/L at 45 days post infusion and recovered at 58 days post infusion. The patient did not require granulocyte stimulating factor (GCSF) support.
He relapsed through multiple lines of therapies after 90Y-ibritumomab tiuxetan and he is still alive 19 years later.
Case 3
A 60-year-old female with a distant history of breast cancer presented with cervical and postauricular lymphadenopathies and was diagnosed with SLL by lymph node biopsy. FISH study showed 10.5% 13q deletion and 17.5% 17q deletion. She was asymptomatic and monitored for a year. Upon disease progression, she received pentostatin, cyclophosphamide, and rituximab (PCR) for 3 cycles complicated by persistent cytopenia.
Due to further disease progression 19 months after PCR, she was treated with 90Y-ibritumomab tiuxetan. The pretreatment bone marrow biopsy showed 15% lymphomatous involvement. After 90Y-ibritumomab tiuxetan treatment, patient experienced grade 3 neutropenia and grade 3 thrombocytopenia. He achieved stable disease (SD) to therapy on a CT scan after one month. The nadir platelet count was 42x109/L at 35 days post 90Y-ibritumomab tiuxetan infusion and recovered on day 252 post infusion. The nadir of absolute neutrophil counts (ANC) was 0.5 x109/L 44 days after infusion and recovered 231 days post infusion. The patient required granulocyte stimulating factor (GCSF) support. Patient had no infections. However, the disease progressed 5 months after treatment. The patient received multiple lines of therapy including R-CVP with disease progression then rituximab plus Bendamustine followed by autologous hematopoietic stem cell transplantation. She was started on ibrutinib therapy 8 years after bone marrow transplant for her relapsed disease. Patient is currently alive and continues to receive daily ibrutinib.
Case 4
A 69-year-old male with chronic obstructive pulmonary disease (COPD) and chronic renal insufficiency (CKD) presented with abnormal liver function tests and lymphadenopathy in left groin and right submandibular area. A left groin lymph node biopsy confirmed a diagnosis of SLL with plasmacytoid features. The patient was treated with chlorambucil with improvement in lymphadenopathy and liver function test. Patient had progressive adenopathy treated with Rituximab. Two years after rituximab treatment, the patient developed Richter’s transformation (diffuse large B-cell lymphoma) in the lung. Patient received 5 cycles of rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP). He developed severe neutropenia, and the course was complicated by multiple infections. Later on, SLL progressed, and the patient received 4 doses of rituximab with minimal response.
Due to lack of response to rituximab, the patient was treated with 90Y-ibritumomab tiuxetan. The pretreatment bone marrow biopsy showed 5–10% lymphomatous involvement with SLL. FISH was not performed or not available in the EMR. Patient experienced grade 3 thrombocytopenia but no neutropenia. The nadir platelet count was 42 × 109/L at 20 days post 90Y-ibritumomab tiuxetan infusion and recovered on day 85 postinfusion. The ANC nadir was 4.16 x109/L 14 days post infusion. The patient did not receive GCSF support. CT scan of the chest, abdomen, and pelvis 2 months showed progressive disease. The patient received multiple lines of therapy however, disease progressed, and he passed away from lung infection 10 months after 90Y-ibritumomab tiuxetan treatment.
Case 5
A 59-year-old male with benign prostatic hyperplasia presented with worsening lymphocytosis with a white cell count of 28.4 × 109/L with 50% lymphocytes and a chronic left cervical lymphadenopathy. Lymph node biopsy confirmed the diagnosis of CLL. The patient progressed through chlorambucil, 2 cycles of fludarabine, 6 cycles of R-CHOP, single agent rituximab, cyclophosphamide plus fludarabine, 2 cycles of DHAP, PCR, as well as alemtuzumab plus rituximab with minimal or no response.
Due to poor response to previous therapies, she was treated with 90Y-ibritumomab tiuxetan. The pretreatment bone marrow biopsy involvement was <1%. FISH showed 17.5% 11q deletion. After 90Y-ibritumomab tiuxetan treatment, patient experienced grade 4 neutropenia and grade 3 thrombocytopenia. The nadir ANC count was 0.4x109/L at 27 days post 90Y-ibritumomab tiuxetan infusion and recovered on day 77 post 90Y-ibritumomab tiuxetan infusion. The nadir of platelet count was 4 x109/L at 128 days after 90Y-ibritumomab tiuxetan infusion and recovered 140 days post 90Y-ibritumomab tiuxetan infusion. The patient received granulocyte stimulating factor (GCSF) support. Post infusion was complicated by a presumed community acquired pneumonia requiring hospitalization.
Unfortunately, 2 months after 90Y-ibritumomab tiuxetan treatment, the disease progressed, and multiple enlarged lymph nodes in the bilateral axillae, supraclavicular regions, mesentery, retroperitoneum, and pelvis were seen on the CT scan. Salvage regimen of cladribine and rituximab then ifosfamide, carboplatin and etoposide (ICE) were used. Patient achieved PR but developed neutropenic fever and pneumonia requiring hospitalization. He passed away 2 months after discharge.
Discussion
Our case series reported 3 refractory CLL and 2 refractory SLL patients who were treated with 90Yttrium ibritumomab tiuxetan with a median age at diagnosis of 61 (range 48–69) with 4 out of 5 patients are males. All patients had significant nodal involvement at diagnosis. All patients relapsed or progressed after 90Y-ibritumomab tiuxetan treatment achieving only transient responses with best responses being SD. The overall response rate (ORR) was 0% in our case series. Median time from 90Y-ibritumomab tiuxetan treatment to relapse was 65 (range 45–182) days. Of the 5 reported cases, the median lines of treatment prior to 90Yttrium ibritumomab tiuxetan is 3 (range 1–9). None of the 5 patients developed MDS or AML with the available follow-up. All patients developed grade ≥3 thrombocytopenia and grade ≥ 3 neutropenia. The median duration of grade 3 or 4 neutropenia is 39.5 days (range 58–231) with median nadir of 0.35 × 109/L (range 0.2–0.5 × 109/L) for ANC. One patient had prolonged neutropenia 7 months post-therapy. The median duration of grade 3 or 4 thrombocytopenia is 107 days (range 12–190) with median nadir of 19 × 109/L (range 4–42 × 109/L). One patient had persistent thrombocytopenias 6 months post-therapy.
Available data reported variable response rates in patients with CLL/SLL treated with radioimmunotherapy over the past 3 decades.3,12–14 One of the pharmacokinetics studies of I-131 tositumomab found that CLL tumors had lower concentration of I-131 tositumomab compared to other histologies.12 Moreover, in another study by DeNardo, out of the 5 patients with CLL treated with I-131 tositumomab, all achieved PR with >50% decrease in lymphadenopathy.13 Thrombocytopenia was the major hematological toxicity and 4 of the 5 patients died of infectious complications.13 In another study published in abstract form, Kaminski et al pooled data from 4 Phase 1–3 studies of the use of I-131 tositumomab RIT in patients with SLL and SLL with Richter’s transformation and reported a CR rate of 21% and PR rate of 42%. Hematological toxicity was seen in <15% of patients.14 The active radioactive moiety in 90Y-ibritumomab tiuxetan is 90Yttrium which emits β-particles that are 5 times more energetic than I-131 and has potentially better tumor mass penetration. However, in agreement with our current findings, the results of a Phase 2 clinical trial by Jain et al of 90Y-ibritumomab tiuxetan in 13 patients with relapsed CLL showed low response rate and increased hematologic toxicity.3 The response rate (15%) is significantly lower than that seen in other NHL.3,9 Grade 3 or 4 hematologic toxicity was seen in 92% evaluable patients in this trial with prolonged durations until recovery.
Myelosuppression is the major dose-limiting toxicity of 90Y-ibritumomab tiuxetan therapy and patients with significant bone involvement are excluded from clinical trials to prevent radiation of neighboring normal stem cells and prolonged myelosuppression.3,15 As shown in Table 1 and Table 2, the patients included in this case series all experienced profound myelosuppression. However, our patients did not have significant pre-treatment bone marrow involvement but developed grade 4 thrombocytopenia. This indicates that bone marrow involvement is not the only risk factor for hematological toxicity after 90Y-ibritumomab tiuxetan treatment. We think that the low expression of CD20 on the surface of CLL/SLL B-cell are likely the cause of the low efficacy. It is also possible that the low number of CD20 sites in these patients led to increased 90Y-ibritumomab tiuxetan in circulation and bone marrow thus increasing the incidence of myelosuppression.
 |
Table 1 Patient Characteristics and Treatment Outcomes |
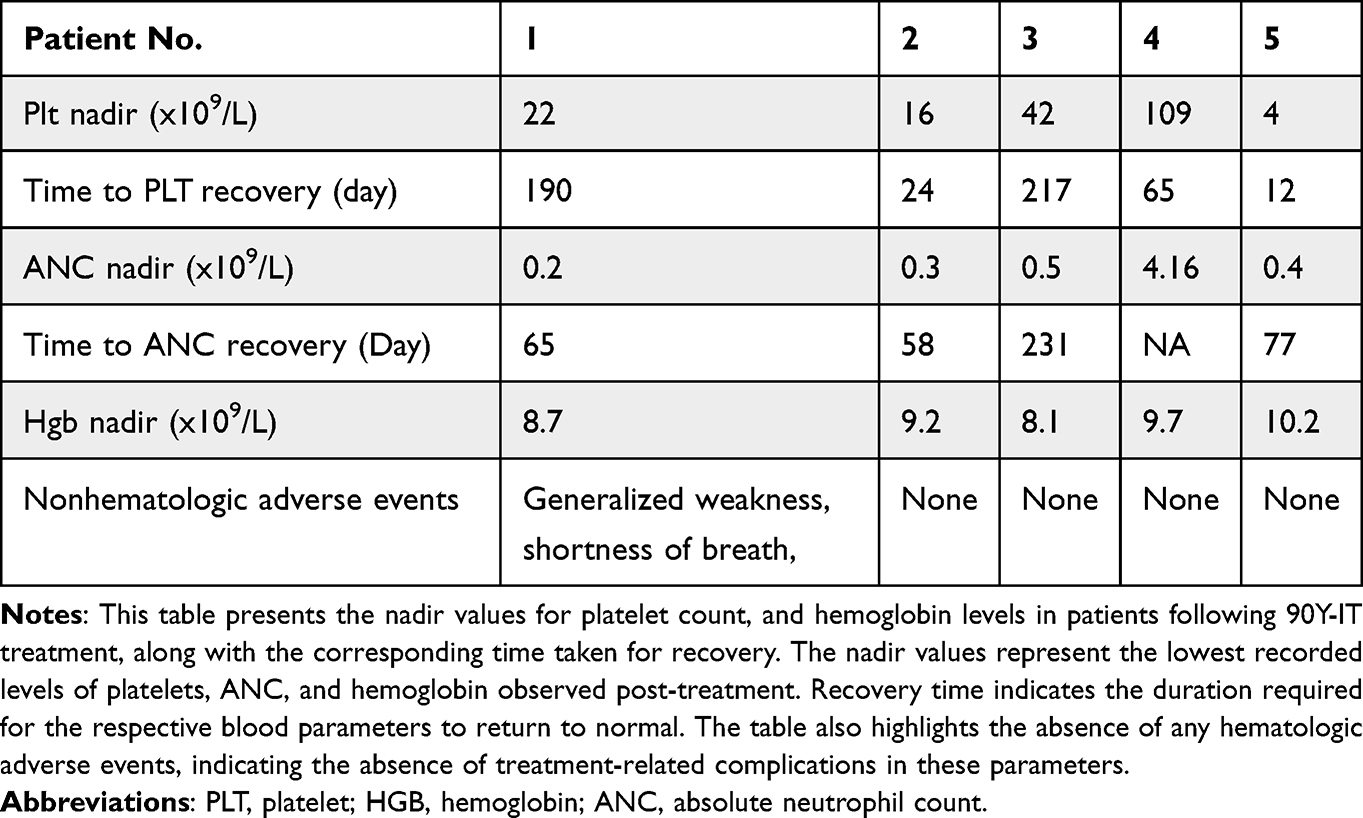 |
Table 2 Patient’s Hematologic Parameters and Recovery Post-Yttrium-90 Ibritumomab Tiuxetan Treatment |
Furthermore, it is important to acknowledge the absence of therapy-related acute myeloid leukemia (AML) or myelodysplastic syndromes (MDS) in any of the five patients in this case series, which has been a known concern in previous studies investigating 90Y-IT.16 For instance, Czuczman et al reported a therapy-related MDS or AML development rate of 2.5% (19 out of 746 patients) during a median follow-up of 4.4 years, with annualized rates of 0.3% per year after diagnosis of non-Hodgkin lymphoma (NHL) and 0.7% per year after treatment.16 Considering the low rate of MDS/AML development, the absence of such cases in our study can likely be attributed to the small sample size. Additionally, it is worth noting that the majority of previous studies on 90Y-IT primarily included patients with follicular lymphoma.16 In the study by Czuczman et al, 66% of the 746 patients had follicular lymphoma, while 9% had SLL and 16% had transformed lymphoma.16 Moustafa et al also demonstrated the effectiveness of 90Y-IT as a single-agent regimen for low-grade follicular lymphoma, with an ORR of 100% in untreated follicular lymphoma and 93% in relapsed follicular lymphoma.17 Given the predominance of follicular lymphoma patients in previous studies investigating the effect of radioimmunotherapy (RIT) on NHL,17,18 the lower ORR observed in our study among CLL/SLL patients treated with 90Y-IT further emphasizes the significance of reporting this case series and the distinctive response pattern observed within this specific subgroup. While our case series provides valuable insights, it is important to acknowledge that the small sample size of only five cases presents a limitation for achieving statistically significant results and may not allow for comprehensive generalization of these findings to the broader population.
In conclusion, although 90Y-ibritumomab tiuxetan has shown to be effective therapy for NHL, its use in patients with CLL/SLL led to significant myelosuppression and was of limited efficacy. This likely related to the dim expression of CD20 on CLL/SLL cells as compared to other NHL that responds well to treatment with 90Yttrium ibritumomab tiuxetan.
Ethics Statement
All five patients provided written informed consent to publish their case details. All patient information has been de-identified to maintain confidentiality. The Mayo Clinic Institutional Review Board, in accordance with the Declaration of Helsinki and the Health Insurance Portability and Accountability Act guidelines of 1996, approved the study.
Disclosure
Dr Han W Tun reports grants from Acrotech Biopharma, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Hallek M, Cheson BD, Catovsky D, et al. iwCLL guidelines for diagnosis, indications for treatment, response assessment, and supportive management of CLL. Blood. 2018;131(25):2745–2760. doi:10.1182/blood-2017-09-806398
2. Hallek M, Al‐Sawaf O. Chronic lymphocytic leukemia: 2022 update on diagnostic and therapeutic procedures. Am J Hematol. 2021;96(12):1679–1705. doi:10.1002/ajh.26367
3. Jain N, Wierda W, Ferrajoli A, et al. A phase 2 study of yttrium‐90 ibritumomab tiuxetan (Zevalin) in patients with chronic lymphocytic leukemia. Cancer. 2009;115(19):4533–4539. doi:10.1002/cncr.24522
4. Small S, Ma S. Frontline treatment for chronic lymphocytic leukemia/small lymphocytic lymphoma (cll/sll): targeted therapy vs. chemoimmunotherapy. Curr Hematol Malig Rep. 2021;16(4):325–335. doi:10.1007/s11899-021-00637-1
5. Emmanouilides, CE. Improved safety and efficacy of yttrium-90 ibritumomab tiuxetan radioimmunotherapy when administered as 2nd or 3rd line therapy for relapsed low-grade, follicular, and transformed B-cell non-Hodgkin’s lymphoma (NHL). Proc Am Soc Clin Oncol. 2003;22:595.
6. Rao AV, Akabani G, Rizzieri DA. Radioimmunotherapy for non-hodgkin’s lymphoma. Clin Med Res. 2005;3(3):157–165. doi:10.3121/cmr.3.3.157
7. Knox SJ, Goris ML, Trisler K, et al. Yttrium-90-labeled anti-CD20 monoclonal antibody therapy of recurrent B-cell lymphoma. Clin Cancer Res. 1996;2(3):p. 457–70.
8. Nadler LM, Ritz J, Hardy R, et al. A unique cell surface antigen identifying lymphoid malignancies of B cell origin. J Clin Invest. 1981;67(1):134–140. doi:10.1172/JCI110005
9. Alhaj Moustafa M, Peterson J, Hoppe BS, et al. Real world long-term follow-up experience with Yttrium-90 ibritumomab tiuxetan in previously untreated patients with low-grade follicular lymphoma and marginal zone lymphoma. Clin Lymphoma Myeloma Leuk. 2022;22(8):618–625. doi:10.1016/j.clml.2022.03.004
10. Hendrix CS, de Leon C, Dillman RO. Radioimmunotherapy for non-hodgkin’s lymphoma with yttrium 90 ibritumomab tiuxetan. Clin J Oncol Nurs. 2002;6(3):144–148. doi:10.1188/02.CJON.144-148
11. Witzig TE, White CA, Gordon LI, et al. Safety of yttrium-90 ibritumomab tiuxetan radioimmunotherapy for relapsed low-grade, follicular, or transformed non-hodgkin’s lymphoma. J Clin Oncol. 2003;21(7):1263–1270. doi:10.1200/JCO.2003.08.043
12. DeNardo GL, DeNardo SJ, Shen S, et al. Factors affecting 131I-Lym-1 pharmacokinetics and radiation dosimetry in patients with non-Hodgkin’s lymphoma and chronic lymphocytic leukemia. J Nucl Med. 1999;40(8):1317–1326.
13. DeNardo GL, Lamborn KR, Goldstein DS, Kroger LA, DeNardo SJ. Increased survival associated with radiolabeled lym‐1 therapy for non‐hodgkin’s lymphoma and chronic lymphocytic leukemia. Cancer. 1997;80(S12):2706–2711.
14. Kaminski MS, Press OW, Lister TA, Valente NK, Kroll S, Tidmarsh G. Iodine I131 tositumomab for patients with small lymphocytic lymphoma (SLL): overall clinical trial experience. Blood. 1999;88:1.
15. Witzig TE, Gordon LI, Cabanillas F, et al. Randomized controlled trial of Yttrium-90–labeled Ibritumomab Tiuxetan radioimmunotherapy versus rituximab immunotherapy for patients with relapsed or refractory low-grade, follicular, or transformed b-cell non-Hodgkin’s lymphoma. J Clin Oncol. 2002;20(10):p. 2453–2463. doi:10.1200/JCO.2002.11.076
16. Czuczman MS, Emmanouilides C, Darif M, et al. Treatment-related myelodysplastic syndrome and acute myelogenous leukemia in patients treated with ibritumomab tiuxetan radioimmunotherapy. J Clin Oncol. 2007;25(27):4285–4292. PMID: 17709799. doi:10.1200/JCO.2006.09.2882
17. Alhaj Moustafa M, Parrondo R, Wiseman G, Peterson J, Witzig TE, Tun HW. Long-term outcome of patients with low-grade follicular lymphoma treated with Yttrium-90 Ibritumomab tiuxetan: the Mayo clinic experience. Am Soc Hematol. 2019;2019:1. doi:10.1182/blood-2019-129391
18. Kaminski MS, Zelenetz AD, Press OW, et al. Pivotal study of iodine I 131 tositumomab for chemotherapy-refractory low-grade or transformed low-grade B-cell non-Hodgkin’s lymphomas. J Clin Oncol. 2001;19(19):3918–3928. PMID: 11579112. doi:10.1200/JCO.2001.19.19.3918.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.