")
Back to Journals » Psychology Research and Behavior Management » Volume 16
Yoga and Mindfulness for Social-Emotional Development and Resilience in 3–5 Year-Old Children: Non-Randomized, Controlled Intervention
Authors Bazzano AN , Sun Y, Zu Y, Fleckman JM, Blackson EA, Patel T , Shorty-Belisle A, Liederman KH, Roi C
Received 17 August 2022
Accepted for publication 19 December 2022
Published 13 January 2023 Volume 2023:16 Pages 109—118
DOI https://doi.org/10.2147/PRBM.S385413
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Igor Elman
Alessandra N Bazzano,1 Yaoyao Sun,2,3 Yuanhao Zu,4 Julia M Fleckman,1 Emma A Blackson,1 Tejal Patel,1 Angie Shorty-Belisle,5 Keith H Liederman,6 Cody Roi7
1Tulane University School of Public Health and Tropical Medicine, Department of Social, Behavioral, and Population Sciences, New Orleans, LA, USA; 2Peking University, Institute of Mental Health, Sixth Hospital, Beijing, People’s Republic of China; 3NHC Key Laboratory of Mental Health. National Clinical Research Center for Mental Disorders, Peking University, Beijing, People’s Republic of China; 4Tulane University School of Public Health and Tropical Medicine, Department of Biostatistics, New Orleans, LA, USA; 5Educare New Orleans, New Orleans, LA, USA; 6Kingsley House, New Orleans, LA, USA; 7Louisiana State University Health Science Center, Department of Child and Adolescent Psychiatry, New Orleans, LA, USA
Correspondence: Alessandra N Bazzano, Email [email protected]
Background: Early childhood is the key life course period for development of social-emotional skills, providing the foundation for school readiness and resilience in later life. Age-appropriate yoga and mindfulness programs may contribute to the development of critical skills in children. Young children from minoritized communities that face structural racism and health disparities may benefit from programs that support social-emotional development and contribute to future academic success. Systematic reviews of yoga interventions for young children have indicated the potential for effectiveness in supporting social-emotional development, executive function, and physical activity. However, studies of yoga and mindfulness with non-White children are sparse and, overall, the evidence base to date for such programs remains limited by non-controlled studies and the variable quality of studies evaluating programs in early childhood settings.
Methods: The analysis of data from a non-randomized, controlled intervention aimed to assess the effect of exposure to a yoga and mindfulness program for early childhood development of social-emotional skills in a majority Black/African American urban preschool setting in southeastern US. Children in the intervention received group yoga and mindfulness led by a certified children’s yoga teacher who also had training and experience as a school teacher. Intervention participants engaged in activities for 20 minutes once per week for 32 weeks, while the control group had no yoga. The final sample included 579 in the historical control group and 122 in the intervention group.
Results: Results indicated that children who participated in the yoga and mindfulness program had higher total protective factor (TPF) subscores on the Devereux Early Childhood Assessment over time than children who did not receive yoga and mindfulness programming, and that the difference was statistically significant (P< 0.05). Participation in the intervention group significantly predicted increases in initiative score, self-control score, and TPF score, as well as a decrease in the behavioral concerns.
Discussion: School based yoga and mindfulness programming can support social-emotional skills and resilience in young children. Additional studies with larger sample sizes and randomization are needed on use of yoga and mindfulness in young children for social-emotional development, particularly for Black/African American children and others from minoritized communities.
Keywords: child development, psychological resilience, child health, behavior
Introduction
A large proportion of children aged 3–5 years old in the United States (U.S.) attend preschool or early childhood centers during the day, where school characteristics influence child development opportunities.1,2 Early childhood education has been shown to improve children’s development and protect against adult disease and disability.3 Given the importance of early childhood experiences for later development, there is a strong need for preschools to provide experiences and environments where children may develop and acquire crucial skills that can enhance their academic, social, emotional, and behavioral competencies before entering elementary school.
Executive function and social-emotional skills develop across the whole life span and dramatically so during the preschool years, reflecting the increasing demands (both environmental and neurodevelopmental) for these competencies in the early childhood period.4,5 Social-emotional skills are considered important foundations for future school readiness and academic achievement.6 Evidence also indicates that social-emotional and executive function support children’s ability to grapple with stressful situations, get along with teachers and peers, and manage emotions.5,7 Early skills training has been identified as a strategy for reducing the academic achievement gap between advantaged and disadvantaged children.8 Fostering emotional self-regulation and stress management skills for preschool children enhances executive function and may be a meaningful way to support children to cope with challenges in both life and academic settings.9,10
One potential approach to support social-emotional development is through child-centered yoga and mindfulness interventions. Yoga consists of a system of exercises, such as physical poses, meditation, breathing practice, and relaxation techniques, which have been increasingly utilized with children to promote health and wellbeing.11 There is abundant neurobiological evidence supporting the effects of yoga in promoting cognitive, emotional, behavioral, and physiological regulation, enhancing resilience, and managing stress.11–13 In school settings, yoga has also been recommended to help students manage stress and anxiety,14 decrease obesity and other health issues,15 promote mental health, and reduce maladaptive behavior.16
Mindfulness has also been utilized for improving and benefiting social and emotional health. Various definitions of mindfulness exist, all centering on intentional awareness within the present moment.17 Studies have examined the effects of mindfulness-based interventions on health and have found that these have beneficial effects on physical health and can improve conditions such as hypertension,18 chronic pain,19 and stress in adults.20 Even when implemented for short periods of time, mindfulness has been shown to have compelling effects on psychological outcomes such as depression and anxiety.21 When implemented in the classroom, both mindfulness and yoga appear to have positive effects on physical, psychological, and emotional health.11,22–26 Given the promise of yoga and mindfulness interventions, there has been increased interest in incorporating these into early childhood and elementary classrooms to examine the effects on physical and psychological health, as well as increased interest in measuring the benefits.27
Whereas numerous studies on yoga have been conducted in adults and older students, well-designed, rigorous research within preschool-aged children has been limited. Among the few studies conducted with preschool children, yoga has often been used in children with special needs, such as students who were diagnosed with attention-deficit hyperactivity disorder28 or autism spectrum disorder (ASD).29 A 2016 review, focused on yoga in school settings, included only one study conducted among children aged 3–5 years.13 More recently a full review was conducted by the authors specifically on the effect of yoga and mindfulness programs (YMP) on social-emotional function among preschool-aged children (3–5 years).25 The review resulted in identification of 1,115 records, of which 80 full text articles were screened, with final inclusion of 16 studies. Included studies evaluated the effect of YMP on social-emotional functioning and identified the potential to improve regulatory skills such as behavioral self-regulation and executive function. Among studies reviewed, 13 reported improvements in these domains, but quality appraisal indicated significant variability in risk of bias across studies, and heterogeneity of outcome measurements hindered comparison. Programs appeared to produce better results when implemented for at least 6 weeks and among children who had lower baseline social-emotional functioning.25
Despite a lack of high-quality studies, the application of yoga in preschool settings has increased over the last several years, indicating both interest and acceptability. Use of yoga in the past 12 months in children aged 4–17 (including preschool children) increased from 3.1% in 2012 to 8.4% in 2017,30 indicating the acceptability of such interventions. Mindfulness interventions have also been reported in efforts to improve preschoolers’ prosocial behaviors, self-regulation, attention control, and academic performance.31–33
In understanding the need for social-emotional skills training in U.S. preschools, the impacts of racism and health disparities on early childhood and school readiness must also be addressed.34,35 Limited research regarding yoga and mindfulness interventions among diverse preschool populations is available, and there are disproportionately more White children observed in these interventions compared to children of color. In studies where children of color were of the majority participants, yoga and mindfulness were implemented to examine their effects on social-emotional skills and trauma.24,36 With the growing diversity in United States population, and increasing calls for social justice and equity, more studies are needed among children of color preschool populations to meet needs for social-emotional and executive function skills training.
Given the contemporary crisis in child mental health,37 the impact of the COVID-19 pandemic on mental and emotional health of both children and young adults37, and the potential of yoga and mindfulness interventions to support developing social-emotional skills in early childhood development, additional evidence on this topic is urgently needed. Thus, the present study aimed to assess the effect of exposure to a YMP intervention for early childhood development of social-emotional skills, as measured by the Devereux Early Childhood Assessment (DECA), in a majority Black/African American urban preschool setting. DECA provides an assessment of within-child protective factors central to social and emotional health and resilience. The items were developed based on prior literature and formative research, and the measure was tested and norm-referenced among a U.S. representative sample of children aged 2–5 years. Two composite scales include total protective factors (assessing children’s positive behaviors; this is composed of three factors – initiative, self-control, and attachment) and behavioral concerns (assessing children’s social and emotional problems).
Methods and Materials
This study used historical control data to assess the impact of yoga classroom activities during the preschool day on social-emotional functioning of children. Procedures consisted of secondary data analysis; specifically, data were obtained from electronic records of an early childhood center in the southeastern U.S., which is a member of the Educare national network of preschools. The early childhood center routinely collects data on children’s social-emotional skills as part of broader evaluation efforts for the national network. From 2014–2019, as part of the local evaluation of the early childhood center serving Early Head Start and Head Start families, children aged 0–5 and their primary caregivers participated in the Educare Learning Network (ELN) Implementation Study. This larger study is designed to document the features of Educare sites and how implementation of the model contributes to program quality and links to child and family outcomes. Nationally, there are 24 Educare schools from 16 states that are part of the ELN. The study site provides services for 168 children and their families. The early childhood center is also part of a broad urban community redevelopment effort that aimed to revitalize an area impacted by disaster, as well as address economic and racial disparities.
Yoga programming was provided by the early childhood center in the 2019–2020 school year to children 3–5 years old (further details on the sample and methods are provided below and in succeeding paragraphs). Yoga activities were led by a certified children’s yoga teacher. Data from 2014–2019 school years, when no yoga was provided, was used as historical control. Both intervention and control groups were assessed twice, in the beginning of fall semester (first/pre-intervention measurement) and spring semester (second/post-intervention measurement).
The study was approved by Tulane University Institutional Review Board (IRB) under number 2019–549-TUHSC. We confirm that the study complies with the Declaration of Helsinki. Only completely de-identified secondary data were utilized, that had previously been collected through internal program evaluation, therefore the approving organization did not require parental consent or participant assent for the study.
Intervention
During the 2019–2020 school year, eight groups (classrooms) of 3–5 year old children, with 17 children in each classroom, received group yoga training provided by a certified children’s yoga teacher who also had training and experience as a classroom teacher. Each preschool class practiced activities in the morning as a group, in a carpeted multipurpose room. Children participated in yoga and mindfulness activities for 20 minutes once per week for 32 weeks. The YMP activity was specifically designed for children to be developmentally appropriate (eg, without using Sanskrit names of poses, and using secular songs, stories, and instructions appropriate for very young children). The programming was provided using a formal curriculum with content that included combinations of the following elements: sequences of physical postures or poses specifically appropriate to children’s development and abilities, guided meditation in the form of stories or songs, and breathing exercises such as breathing synchronized with the expansion and contraction of a Hoberman sphere. In order for the activities to be engaging for young audiences, activities were all presented with recorded musical accompaniment.38
Measures
The Devereux Early Childhood Assessment for Preschoolers, Second Edition (DECA-P2)39 was used to assess social-emotional development and resilience in children aged 3–5 years old, with teachers who were well-trained on the assessment tools regularly assessing students each year on these domains as part of the school’s overall evaluation program. Previous studies reported stable and acceptable reliability and validity of DECA.40 The 38 items on the DECA are rated on a 5-point Likert-scale ranging from 0 (never) to 4 (very frequent). It includes four subscales: Initiative, Self-Control, Attachment, and Behavioral Concerns. The first three subscales consist of nine items in each subscale and are summed to total protective factors (TPF), with higher scores indicating higher social and emotional strengths. The Behavioral Concerns subscale contains 11 items, and higher scores represent behavioral problems such as “has temper tantrums”. T-scores of each subscale and TPF are provided and used as indicators to evaluate results. For TPF, T-scores ≤ 40 indicate “Concern”, 40 < T-scores > 60 indicate “Typical”, or T-scores ≥ 60 indicate “Strengths”. For Behavioral Concerns scale, T-scores ≥ 60 indicate “Concern” or T-scores < 60 indicate “Typical”.
DECA was assessed by teachers through observation of children. Paper versions of DECA were used in historical controls and an electronic version used during the intervention period (e-DECA). Observation and recording are done for DECA by teachers and then scored by a professional evaluator trained on this work. A web-based e-DECA platform was used in the intervention group, where T-scores of Initiative, Self-Control, Attachment, Behavioral Concerns, and TPF were provided directly by the e-DECA software.
De-identified demographic data were provided by the early childhood center, including age, gender, race/ethnicity, family composition, and the presence of an individualized education program or IEP denoting provision of special programming for a child with a disability.
Sample Size and Power Calculation
Sample size was calculated according to the anticipated effect of yoga training on executive functions. Effects of yoga on DECA were unknown, and not available through the existing literature, but information was available on a closely related measure, the Minnesota Executive Function Scale (MEFS), and we expected that there could be a similar effect of yoga on DECA. Using t-test to compare the mean difference between two independent groups in G*Power, we would require a total sample size of 192 (intervention group: 64, control group: 128), based on 90% power, a two-tailed 5% significance level, and an allocation ratio of 2, to reach the medium effect size of 0.5. Considering a 10% rate of loss-to-follow-up, the sample size should reach 212, with the intervention group containing 71 participants and the control group containing 141 participants. For this study, eight classes with around 17 children in each class received yoga training. The number of recruits in the intervention group (136) met the least sample size criterion (71). In practice, historical data from 2014–2019 is provided, so a 1:5 allocation ratio is achieved. A higher allocation ratio means a lower sample size needed in the intervention group to achieve the sample statistical power. For this study, 122 children had been receiving yoga, thus the number of recruits in the intervention group met the least sample size needed.
Data Description
In this study, the term “Black/African American” refers to the assigned racial category Black non-Hispanic, using the racial and ethnic categorization employed by the U.S. Census: Black non-Hispanic (nH), White (nH), American Indian/Alaskan Native (AN; nH), Asian/Pacific Is- lander (PI; nH), and Hispanic. We used these categories not as indicators of biologic differences, but as proxy indicators of the socially and politically constructed realities and histories that accompany racial identities in the United States. The racial and ethnic categories in the data set were self-selected on enrollment forms by families enrolling their children at the center, using pre-determined and closed-ended categories. Given that the majority of the children attending the center during the study period were Black/African American (94.6%) and given that race/ethnicity were assessed in order to address a gap in the literature regarding use of yoga and mindfulness programs with non-White children, only records of Black/African American children were included in the analysis, which also served to maintain statistical power. A total of 1,625 records were collected, with 1,492 in historical control and 133 in the intervention group. Including only Black/African American participants, a final sample of 1,536 was used for analysis, with 1,411 in historical control and 125 in the intervention group. After matching identification codes with fall and spring records of the same school year, 801 paired records of DECA scores were used to calculate any change of DECA for the same student in one school year, with a final number of 579 in the historical control group and 122 in the intervention group.
Statistical Analysis
The data analyses aimed to evaluate the difference on DECA between the yoga intervention group and the historical control group. Descriptive statistics, including means, standard deviations, frequencies, and proportions were first conducted. Comparisons between the yoga intervention group and control group at each timepoint and within each group were performed. Changes in DECA scores for each subscale in one school year were computed at second assessment and t-tests were conducted to test the difference of the mean change. Then, models accounting for potential within-group correlation were performed using multilevel modeling. In sensitivity analysis, the control group from 2014 to 2019 school years was used for comparison with the intervention group separately. Multivariate logistic models were used to analyze whether the intervention could help children achieve higher level scores in DECA. All the statistical tests were performed on the significance level of two-tailed alpha =0.05. SPSS 23.0 and R version 3.5.3 and SAS version 9.4 software were used for analysis in the current study.
Results
Participant Characteristics
The mean age of all children in the study was around 4 years or 47.94 months (±6.88). Boys and girls were about equally included (50.07% vs 49.93%). A total of 567 of 801 (80.88%) children had sibling and 621 of them (88.59%) reported an IEP. All children included for data analysis were Black/African American. None of the children were Hispanic, and English was the primary language of all students. There was no significant difference in age in months, proportion male/female, proportion with siblings or IEP between the historical control group and the intervention group (shown in Table 1).
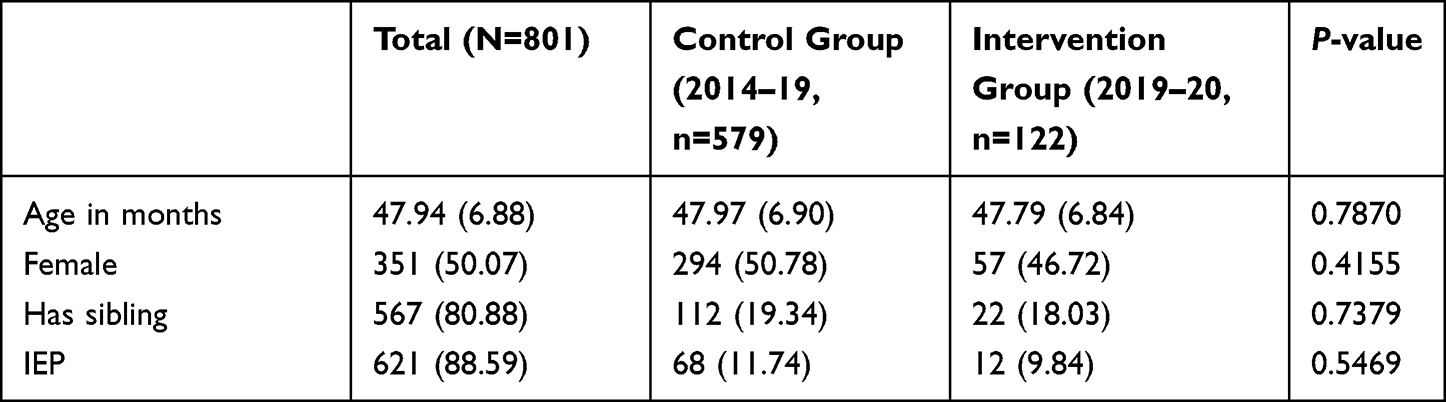 |
Table 1 Participant Characteristics |
Devereux Early Childhood Assessment
DECA scores are shown in Table 2 . Both the control group and intervention group showed a significant increase on the Initiative subscale between the first assessment (in fall) and the second assessment in spring (all P-value<0.05). However, the intervention group showed a significantly larger improvement in Initiative as compared with the control group (P=0.0037). For the Self-control subscale, no difference was found between fall and spring in the control group (P=0.1528). In contrast, the intervention group showed a significant improvement between fall and spring (P=0.0015), resulting in a significant between-within group difference (P=0.0010). For the Attachment subscale, both control and intervention groups showed gains at spring semester (all P-value<0.05), and there were no differences between the two groups in changes for the Attachment score (P=0.0689). For the TPF score, that contains the three subscales, the yoga intervention group had significantly greater gains than the control group (P=0.0008), although the control group and intervention group both had gains from the fall to the spring (all P-value<0.05).
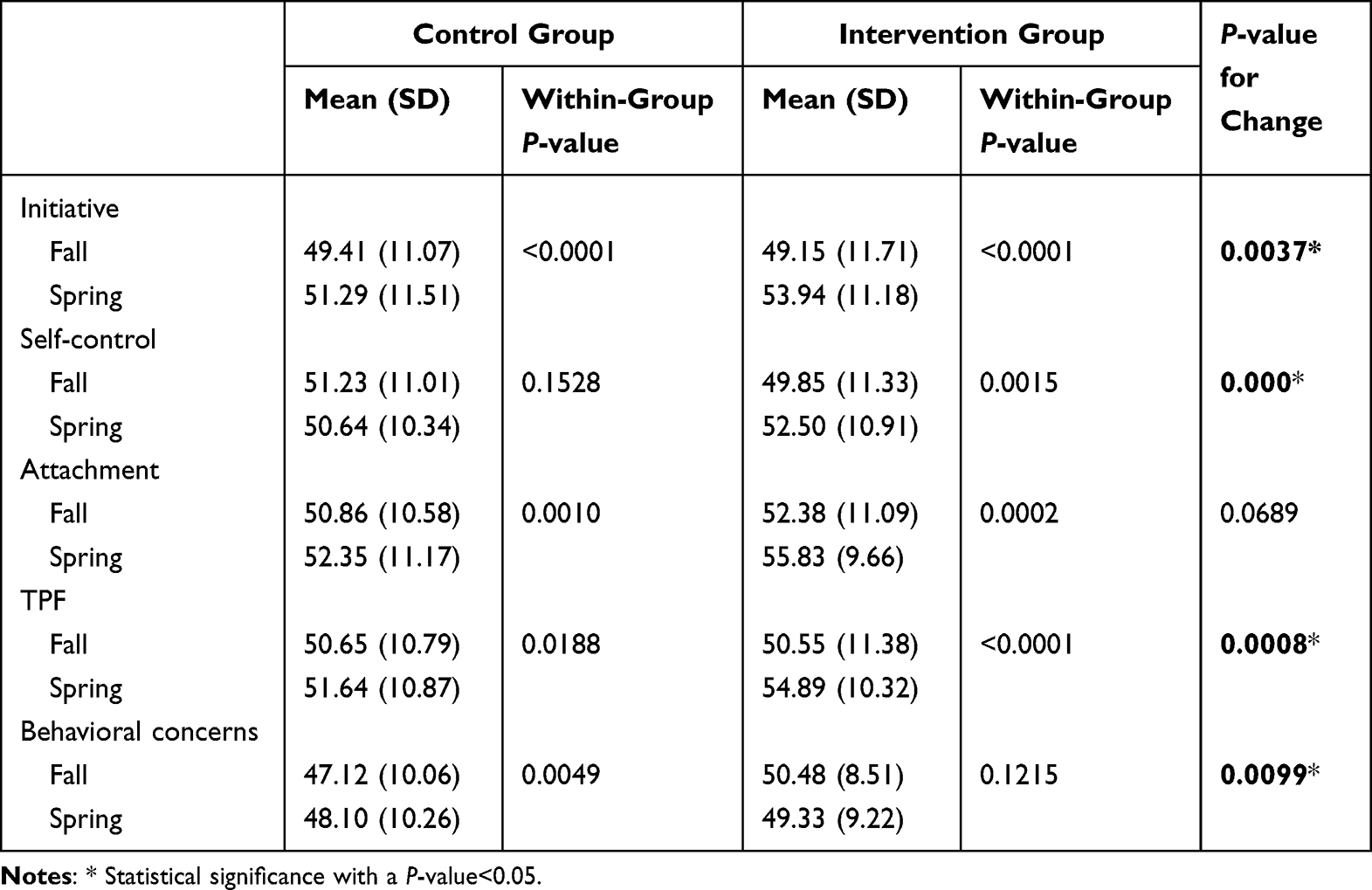 |
Table 2 Comparison of DECA Scores Between Intervention Group and Control Group |
For the Behavioral Concerns subscale, the control group had an increased score in spring (P=0.0049) as compared with fall. The intervention group had a decrease in Behavioral Concerns score from fall to spring, though it was non-significant (P=0.1215). The between–within group comparison showed a significant difference on change in Behavioral Concerns score between the intervention group and control group (P=0.0099).
A significant within-group difference (P=0.029) was found on TPF in the Intervention group (shown in Figure 1), where the Intervention group showed a higher proportion of Strength in TPF at spring as compared with fall (32.79% vs 24.59%). When comparing the categories of TPF and Behavioral Concerns, no within-group difference was found on TPF and Behavioral Concerns in the control group and Behavioral Concerns in the intervention group.
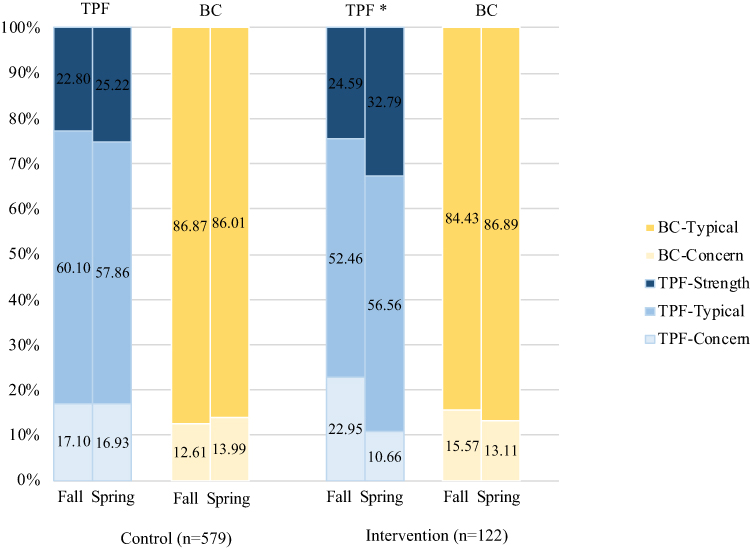 |
Figure 1 Within-group comparison. Abbreviations: TPF, Total Protective Factors; BC, Behavioral Concerns. Notes: *Significant difference among the distribution levels of TPH between spring and fall with a p-value of <0.05 using chi-square test when comparing the distribution. |
Multilevel Model Analysis
Multilevel models were further conducted to reveal the true prediction of participation in the intervention on DECA score change from fall to spring semester. After adjusting for age in months, gender, IEP, and has sibling, participation in the intervention group significantly predicted increases in initiative score, self-control score, and TPF score, as well as a decrease in the behavioral concerns score (β=2.938, P=0.0034; β=3.237, P=0.0010; β=3.368, P=0.0007; β=−2.101, P=0.0107; shown in Table 3) compared to the control group.
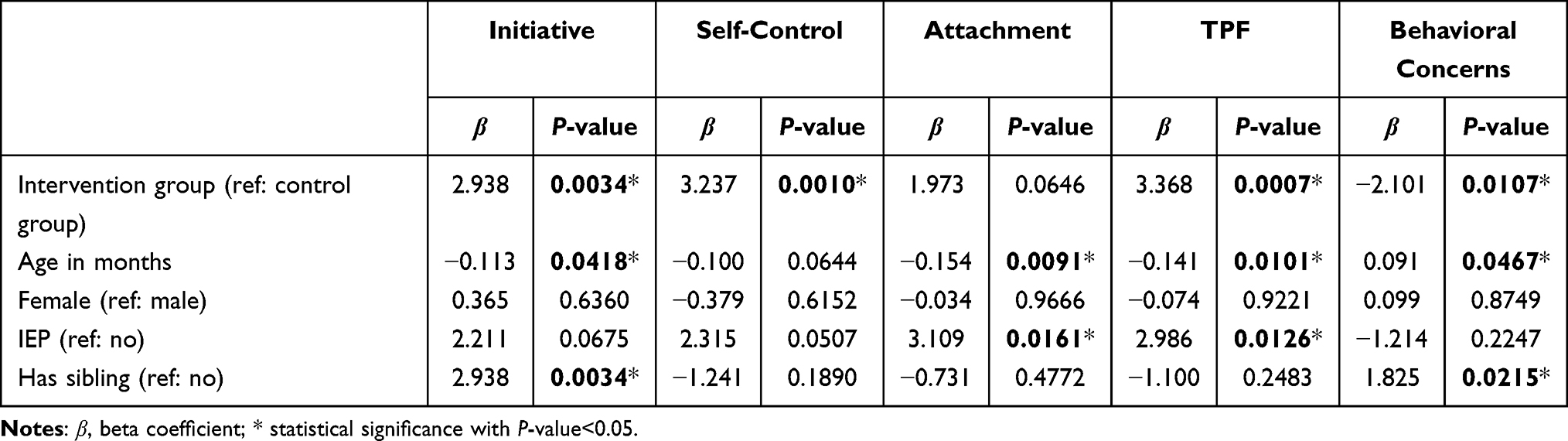 |
Table 3 Multilevel Models of Intervention on DECA Score Change from Fall to Spring Semester |
Sensitivity Analysis
Multilevel models by school year were conducted as sensitivity analysis (shown in Table 4). Compared to control groups of 2014–15, 2015–16, 2016–17, and 2017–18 school years, the intervention group of the 2019–20 school year significantly predicted an increase of TPF and predicted a decrease of behavioral concerns, which corresponds to the primary analysis. However, the intervention group of the 2019–20 school year failed to predict an increase of TPF when comparing with the control group of the 2018–19 school year.
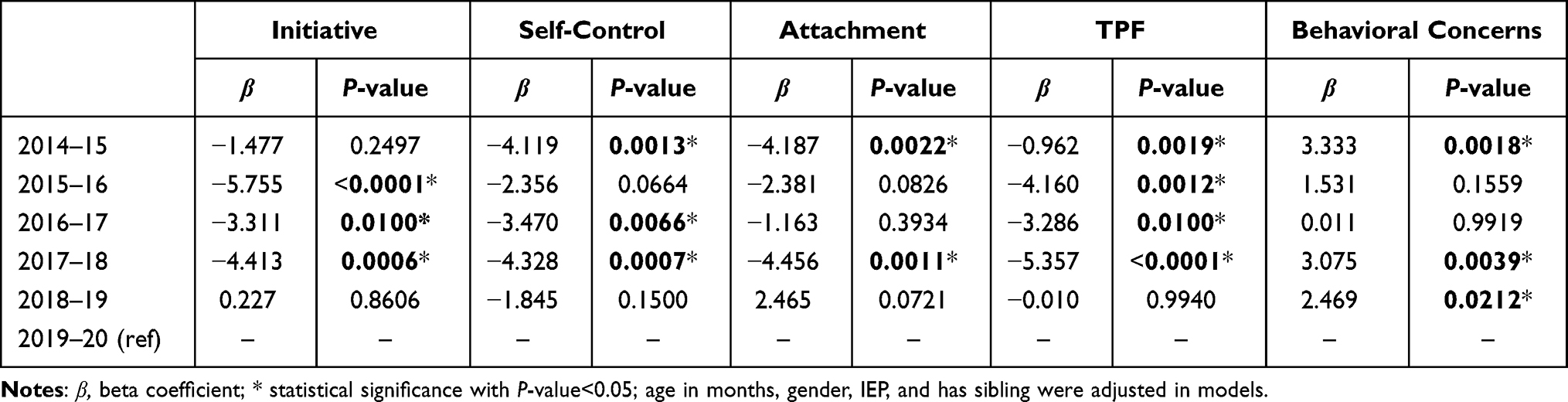 |
Table 4 Adjusted DECA Score Change Differing by School Year |
Discussion
The present study found the intervention appeared to be associated with improved scores indicative of preschool social-emotional health (specifically TPF subscores of the DECA) related to initiative and self-control, and scores indicating reduced behavioral concerns among intervention students compared to historical controls. The sensitivity analysis suggested differences between the 2018–19 school year and other years, however, overall the intervention appeared to be associated with better outcomes on certain DECA components than the control condition.
This study addresses a gap in the literature on yoga and mindfulness interventions among younger children, particularly young Black/African American children, and addresses the need to build the evidence base on strengthening children’s social-emotional skills through innovative approaches in early childhood settings. The intervention results appear promising, though there are limitations. The main limitation of the present study is the historical control trial design. Intervention studies without the benefit of randomization in allocation concealment principle may perform poorly in controlling covariates and may limit reliability. Because the study took place in a community-based context, the intervention was interrupted by holidays and other school schedule breaks or disruptions, which may have influenced the implementation of the intervention. In addition, the small sample size suggests caution is needed when interpreting the results. However, a small sample size is not unique to this study.
The reported effect of yoga on preschoolers’ social-emotional health was consistent with previous yoga studies conducted in school settings.13 Most studies report similar findings of improved attentional control and behavioral regulation, two elements of self-regulation critical to academic performance.38 Animated forms of physical education have also been identified as an ideal way to integrate social, emotional, and cognitive skills in early childhood education to achieve optimal health and wellbeing.41
Yoga and mindfulness programs may also contribute to children’s social-emotional development by addressing teacher stress.36 By reducing educator stress, teachers may more effectively respond and attend to the emotional needs of their students, thereby reinforcing children’s healthy social-emotional development.37
Importantly, provision of yoga and mindfulness programs could aid in serving as an informal method of identifying and treating emotional dysregulation in early childhood, and potentially reduce the risk of later psychopathology. As early childhood trauma may disrupt children’s typical emotion processing, addressing social-emotional development in the face of a traumatic event or exposure to chronic trauma, through yoga and mindfulness, may serve as an early intervention tool.38 Adoption of yoga and mindfulness programs within school settings may contribute to broadly addressing children’s social, emotional, and behavioral needs.
Conclusion
The results of this study can guide further research to explore the role of yoga and mindfulness for preschools and early childhood centers. Schools may consider offering further programming that builds social-emotional skills and resilience through yoga and mindfulness. Additional studies with randomization and larger sample sizes will provide more information related specifically to promoting these types of interventions and policy-level actions for preschoolers’ social, emotional, and cognitive development.
Data Sharing Statement
Data supporting the results reported in the manuscript can be requested from the local site and study investigators, by contacting the corresponding author, ANB.
Ethics Approval and Informed Consent
The study utilized completely de-identified secondary data and was approved by Tulane University IRB under study number 2019-549. We confirm the study complies with the Declaration of Helsinki.
Acknowledgments
We are grateful to the school staff who supported the study and to the parents, yoga teachers, community partners, and all volunteers who made this work possible.
Author Contributions
All authors have made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; have drafted or written, or substantially revised or critically reviewed the article; have agreed on the journal to which the article will be submitted; have reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage; and agree to take responsibility and be accountable for the contents of the article.
Funding
This study was supported through funding from the University of Nebraska Medical Center and the Buffett Early Childhood Fund.
Disclosure
Ms Angie Shorty-Belisle reports grants from Educare New Orleans, during the conduct of the study. The authors declare that they have no other competing interests.
References
1. True L, Pfeiffer KA, Dowda M, et al. Motor competence and characteristics within the preschool environment. J Sci Med Sport. 2017;20(8):751–755. doi:10.1016/j.jsams.2016.11.019
2. United States Census Bureau. Census Data; 2022. Available from: https://data.census.gov/cedsci/.
3. Centers for Disease Control and Prevention. Early childhood education: interventions addressing the social determinants of health; 2016. Available from: https://www.cdc.gov/policy/hst/hi5/earlychildhoodeducation/index.html.
4. Harvard University. Building the Brain’s “air traffic control” system: how early experiences shape the development of executive function: working paper no. 11. 2011. Available from: www.developingchild.harvard.edu.
5. Wolf S, McCoy DC. The role of executive function and social-emotional skills in the development of literacy and numeracy during preschool: a cross-lagged longitudinal study. Dev Sci. 2019;22(4):e12800. doi:10.1111/desc.12800
6. Fitzpatrick C, McKinnon RD, Blair CB, Willoughby MTJL. Do preschool executive function skills explain the school readiness gap between advantaged and disadvantaged children? Learn Instr. 2014;30:25–31. doi:10.1016/j.learninstruc.2013.11.003
7. Liew JJC. Effortful control, executive functions, and education: bringing self‐regulatory and social‐emotional competencies to the table. Child Dev Perspect. 2012;6(2):105–111. doi:10.1111/j.1750-8606.2011.00196.x
8. Diamond A, Lee KJS. Interventions shown to aid executive function development in children 4 to 12 years old. Science. 2011;333(6045):959–964. doi:10.1126/science.1204529
9. Blair C, Raver CC. School readiness and self-regulation: a developmental psychobiological approach. Ann Rev Psychol. 2015;66:711–731. doi:10.1146/annurev-psych-010814-015221
10. Rimm-Kaufman SE, Curby TW, Grimm KJ, Nathanson L, Brock LL. The contribution of children’s self-regulation and classroom quality to children’s adaptive behaviors in the kindergarten classroom. Dev Psychol. 2009;45(4):958–972. doi:10.1037/a0015861
11. Miller S, Mendelson T, Lee-Winn A, Dyer NL, Khalsa SBS. Systematic review of randomized controlled trials testing the effects of yoga with youth. Mindfulness. 2020;11(6):1336–1353. doi:10.1007/s12671-019-01230-7
12. Gard T, Noggle JJ, Park CL, Vago DR, Wilson AJF. Potential self-regulatory mechanisms of yoga for psychological health. Front Hum Neurosci. 2014;8(770). doi:10.3389/fnhum.2014.00770
13. Khalsa SB, Butzer B. Yoga in school settings: a research review. Ann N Y Acad Sci. 2016;1373(1):45–55. doi:10.1111/nyas.13025
14. Nanthakumar C. The benefits of yoga in children. J Integr Med. 2018;16(1):14–19. doi:10.1016/j.joim.2017.12.008
15. Chen DD, Pauwels L. Perceived benefits of incorporating yoga into classroom teaching: assessment of the effects of “yoga tools for teachers”. Adv Phys Educ. 2014;04(03):138–148. doi:10.4236/ape.2014.43018
16. Butzer B, Bury D, Telles S, Khalsa SBSJ. Implementing yoga within the school curriculum: a scientific rationale for improving social-emotional learning and positive student outcomes. J Child Serv. 2016;11(1):3–24. doi:10.1108/JCS-10-2014-0044
17. Kabat-Zinn J. An outpatient program in behavioral medicine for chronic pain patients based on the practice of mindfulness meditation: theoretical considerations and preliminary results. Gen Hosp Psychiatry. 1982;4(1):33–47. doi:10.1016/0163-8343(82)90026-3
18. Palta P, Page G, Piferi RL, et al. Evaluation of a mindfulness-based intervention program to decrease blood pressure in low-income African-American older adults. J Urban Health. 2012;89(2):308–316. doi:10.1007/s11524-011-9654-6
19. Chiesa A, Serretti A. Mindfulness-based interventions for chronic pain: a systematic review of the evidence. J Altern Complement Med. 2011;17(1):83–93. doi:10.1089/acm.2009.0546
20. Grossman P, Niemann L, Schmidt S, Walach H. Mindfulness-based stress reduction and health benefits: a meta-analysis. J Psychosom Res. 2004;57(1):35–43. doi:10.1016/S0022-3999(03)00573-7
21. Howarth A, Smith JG, Perkins-Porras L, Ussher M. Effects of brief mindfulness-based interventions on health-related outcomes: a systematic review. Mindfulness. 2019;10(10):1957–1968. doi:10.1007/s12671-019-01163-1
22. Felver JC, Razza R, Morton ML, Clawson AJ, Mannion RS. School-based yoga intervention increases adolescent resilience: a pilot trial. J Child Adolesc Ment Health. 2020;32:1–10. doi:10.2989/17280583.2019.1698429
23. James-Palmer A, Anderson EZ, Zucker L, Kofman Y, Daneault JF. Yoga as an intervention for the reduction of symptoms of anxiety and depression in children and adolescents: a systematic review. Front Pediatr. 2020;8:78. doi:10.3389/fped.2020.00078
24. Razza RA, Linsner RU, Bergen-Cico D, Carlson E, Reid S. The feasibility and effectiveness of mindful yoga for preschoolers exposed to high levels of trauma. J Child Fam Stud. 2020;29(1):82–93. doi:10.1007/s10826-019-01582-7
25. Sun Y, Lamoreau R, O‘Connell S, Horlick R, Bazzano, AN. Yoga and mindfulness programs for improving social emotional development in preschool children aged 3 to 5 years: a systematic review. Int J Environ Res Public Health. 2021;18(11):6091. doi:10.3390/ijerph18116091
26. Bazzano AN, Anderson CE, Hylton C, Gustat J. Effect of mindfulness and yoga on quality of life for elementary school students and teachers: results of a randomized controlled school-based study. Psychol Res Behav Manag. 2018;11:81–89. doi:10.2147/PRBM.S157503
27. Saunders D, Kober H. Mindfulness-based intervention development for children and adolescents. Mindfulness. 2020;11(8):1868–1883. doi:10.1007/s12671-020-01360-3
28. Cohen SCL, Harvey DJ, Shields RH, et al. Effects of yoga on attention, impulsivity, and hyperactivity in preschool-aged children with attention-deficit hyperactivity disorder symptoms. JDBP. 2018;39(3):200–209. doi:10.1097/DBP.0000000000000552
29. Rosenblatt LE, Gorantla S, Torres JA, et al. Relaxation response-based yoga improves functioning in young children with autism: a pilot study. J Altern Complement Med. 2011;17(11):1029–1035. doi:10.1089/acm.2010.0834
30. Black LI, Barnes PM, Clarke TC, Stussman BJ, Nahin RL. Use of yoga, meditation, and chiropractors among U.S. children aged 4–17 years. NCHS Data Brief. 2018;2018(324):1–8.
31. Flook L, Goldberg SB, Pinger L, Davidson RJ. Promoting prosocial behavior and self-regulatory skills in preschool children through a mindfulness-based kindness curriculum. Dev Psychol. 2015;51(1):44–51. doi:10.1037/a0038256
32. Lim X, Qu L. The effect of single-session mindfulness training on preschool children’s attentional control. Mindfulness. 2016;8(2):300–310. doi:10.1007/s12671-016-0600-2
33. Thierry KL, Bryant HL, Nobles SS, Norris KS. Two-year impact of a mindfulness-based program on preschoolers’ self-regulation and academic performance. Early Educ Dev. 2016;27(6):805–821. doi:10.1080/10409289.2016.1141616
34. Becker B, Schober P. Not just any child care center? Social and ethnic disparities in the use of early education institutions with a beneficial learning environment. Early Educ Dev. 2017;28(8):1011–1034. doi:10.1080/10409289.2017.1320900
35. Slopen N, Williams D. Resilience-promoting policies and contexts for children of color in the United States: existing research and future priorities | Development and Psychopathology | Cambridge Core. Dev Psychopathol. 2021;33(2):614–624. doi:10.1017/S095457942000173X
36. Thierry KL, Vincent RL, Bryant HL, Kinder MB, Wise CL. A self-oriented mindfulness-based curriculum improves prekindergarten students’ executive functions. Mindfulness. 2018;9(5):1443–1456. doi:10.1007/s12671-018-0888-1
37. U.S. Department of Health and Human Services. U.S. Surgeon general issues advisory on youth mental health crisis further exposed by covid-19 pandemic | HHS.gov; 2021. Available from: https://www.hhs.gov/about/news/2021/12/07/us-surgeon-general-issues-advisory-on-youth-mental-health-crisis-further-exposed-by-covid-19-pandemic.html.
38. Khalsa S, Hickey-Schultz L, Cohen D, Steiner N, Cope S. Evaluation of the mental health benefits of yoga in a secondary school: a preliminary randomized controlled trial. J Behav Health Serv Res. 2012;39(1):80–90. doi:10.1007/s11414-011-9249-8
39. LeBuffe PA, Naglieri JA. Devereux Early Childhood Assessment for Preschoolers, Second Edition. Lewisville, NC: Kaplan Early Learning Company; 2012.
40. Epstein MH, Synhorst L. Preschool Behavioral and Emotional Rating Scale, Examiner’s Manual. Austin, TX: Pro-Ed; 2009.
41. Madrona P, Honrubia Montesinos C, Jiménez J, Jiménez M. Motor Skills in Childhood and Its Development from an Animated Physical Education: Theory and Practice. Nova Science Publishers; 2018.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.