")
Back to Journals » Journal of Pain Research » Volume 12
Working towards a consensus on the oncological approach of breakthrough pain: a Delphi survey of Spanish experts
Authors Camps Herrero C, Antón Torres A , Cruz-Hernández JJ, Carrato A , Constenla M , Díaz-Rubio E , Feyjoo Saus M, Garcia-Foncillas J, Gascón P, Guillem V
Received 2 February 2019
Accepted for publication 2 July 2019
Published 29 July 2019 Volume 2019:12 Pages 2349—2358
DOI https://doi.org/10.2147/JPR.S203903
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Michael A Ueberall
Carlos Camps Herrero,1 Antonio Antón Torres,2 Juan Jesús Cruz-Hernández,3 Alfredo Carrato,4 Manuel Constenla,5 Eduardo Díaz-Rubio,6 Margarita Feyjoo Saus,7 Jesus Garcia-Foncillas,8 Pere Gascón,9 Vicente Guillem10
1Jefe de Servicio de Oncología Médica, Consorcio Hospital General Universitario, Valencia, Spain; 2Jefe del Servicio de Oncología Médica, Hospital Universitario Miguel Servet, Zaragoza, Spain; 3Jefe del Servicio de Oncología Médica, Hospital Universitario De Salamanca-IBSAL, Salamanca, Spain; 4Jefe del Servicio de Oncología Médica, Hospital Universitario Ramón y Cajal, Madrid, Spain; 5Jefe de Servicio de Oncología, Complejo Hospitalario Universitario de Pontevedra, Pontevedra, Spain; 6Jefe del Servicio de Oncología Médica, Hospital Universitario Clínico San Carlos, Madrid, Spain; 7Jefe del Servicio de Oncología Médica, Hospital La Moraleja, Madrid, Spain; 8Jefe de Servicio de Oncología Médica, Hospital Universitario “Fundación Jiménez Díaz”, Madrid, Spain; 9Jefe del Servicio de Oncología Médica, Hospital Clínic, IDIBAPS, Universidad de Barcelona, Barcelona, Spain; 10Jefe del Servicio de Oncología Médica, Instituto Valenciano de Oncología, Valencia, Spain
Purpose: There is a lack of standards for the diagnosis, assessment and management of breakthrough cancer pain (BTcP). La Fundación ECO (the Foundation for Excellence and Quality in Oncology) commissioned a study to establish a consensus and lay the foundations for the appropriate management of BTcP in oncology patients.
Patients and methods: A modified Delphi survey comprising two rounds was used to gather and analyze data, which was conducted over the Internet. Each statement that reached a consensus with the respondents was defined as a median consensus score (MED) of ≥7, and agreement among panelists as an interquartile range (IQR) of ≤3.
Results: In total, 69 medical oncologists responded, with a broad consensus that BTcP implied exacerbations of high-intensity pain, as opposed to moderate pain. Furthermore, they concurred that appropriate diagnostic equipment is needed, and that rapid-onset fentanyl formulations should be the preferred treatment for BTcP management. The panelists agreed that a lack of appropriate information and training to attend to patients, as well as limited patient visitation rights, were barriers to effective BTcP management. Regarding gaps in detected knowledge, the panelists were unsure of the measures necessary to assess the burden of the disease on the patient’s quality of life and associated medication costs. Alongside this, there was a lack of awareness of the technical specifics of the different formulations of rapid-onset fentanyl.
Conclusion: These results represent the current status of BTcP management. They may inform recommendations and provide a framework for future research.
Keywords: breakthrough pain, rapid-onset opioids, fentanyl, medical oncology, pain management
Introduction
Breakthrough cancer pain (BTcP) management is one of the most challenging problems associated with cancer pain, and has been linked to a negative impact on the patient’s quality of life (QoL) and ability to function. It can lead to higher levels of depression and anxiety, poorer prognostic on future pain relief, and an increased burden for families and health services.1–6
The prevalence of BTcP has been reported to range from 19% to 95%, depending on the BTP definition and the clinical setting.1,3,5,7 The International Association for the Study of Pain (IASP) estimates that between one half and two thirds of patients with chronic cancer-related pain experience BTcP episodes.
Despite its prevalence, BTcP remains an underdiagnosed and undertreated condition. The reasons for this are probably multifactorial, resulting from a lack of official definition, and unjustified attitudes and misconceptions held by healthcare professionals and patients regarding opioids.5,9–12
Despite international efforts, there is still no one universally accepted BTcP definition.13,14 Overall, BTcP can be considered as a relevant transitory increase in pain. However, there is controversy regarding the intensity of this pain and the patient’s basal pain (absence of BTcP, BTcP effectively treated with opioids or uncontrolled BTcP).15–17
Notwithstanding the proliferation of guidelines addressing pain in cancer patients,6–8,18,19 there is no consensus on BTcP management, and recommendations are heterogenous, which is preventing the establishment of an adequately analgesic approach.
Classically, treatment options involve the optimization of the scheduled background analgesia and supplementing it with “rescue” medication when BTcP occurs.18 Short-acting opioids (SAOs) — immediate-release formulations of morphine—were previously considered the standard of care. However, recent evidence shows that rapid-onset opioids (ROOs) provide safe and effective BTcP management. ROO formulations are characterized by a rapid onset and short duration of action, consistent with the nature of BTcP episodes (acute)7,14,17,20 and the rapid resolution of pain required by these patients.15
The pharmacokinetics and tolerability profile of rapid-acting fentanyl products render them suitable for managing the acute, severe pain intensity that generally characterizes BTcP episodes.19,21,22
Additionally, individualized therapy is made further possible due to the wide range of different rapid-onset fentanyl formulations and preparations available. However, the absence of comprehensive comparative trials means physicians must rely on their understanding and experience when prescribing the medication. This is important to determine the most effective and best-tolerated formulations for each patient.16,17,20
In light of the above, physicians should be aware that rapid-onset fentanyl formulations are not bioequivalent (as they have substantial practical differences); nor are they interchangeable. Each formulation will have a different type of titration, depending on the needs of the patient.17
In clinical practice, the successful management of BTcP requires careful assessment, ongoing reassessment, and a treatment that is tailored to the individual patient. The treatment should also consider the type and cause of the BTcP, as well as patient preferences.6,23
Within this context, the Foundation for Excellence and Quality in Oncology (ECO) commissioned a study to establish a consensus. This could subsequently be used to lay the foundations for the appropriate management of BTP (severely intense pain) in cancer patients. The goal of the study was to achieve a consensus among medical oncologists on a clinical approach towards the diagnostic evaluation and appropriate pharmacological management of patients with BTcP, specifically with rapid-onset fentanyl formulations.
Materials and methods
This study was carried out gathering and analyzing the opinion of expert using the Delphi method. In Spain this type of study is not included among those requiring Research Ethics Committees (RECs) approval or written consent.
A Scientific Committee (SC) was appointed, comprising three members from the Foundation for Excellence and Quality in Oncology and two support methodologists. The SC developed the questions for the first round, structured the questionnaire, set up the online questionnaire into the website created to the study, undertook statistical analysis of the data, produced interim documents and oversaw the process’s general management.
The expert panel members, selected by the SC, included 71 Spanish oncology experts who were invited to participate in the consensus process through a modified Internet-based Delphi survey made up of two rounds.
Experts were identified from a selection of physicians specializing in medical oncology, and each possessed documented clinical expertise in cancer management at referral hospitals. The Delphi participants were located in geographically diverse parts of Spain, and were sent an email inviting them to take part in the study, as well as a link to access the questionnaire on the survey website.
The questionnaire
A selection of 50 statements were developed, each of which was relevant to the diagnosis, assessment and management of BTcP, and based on controversies found in both clinical practice and existing literature.15,24–26 The questionnaire was administered in Spanish. The purpose was to reach a consensus on questions arising from: a) The definition and assessment of BTcP; b) The therapeutic approach to BTcP; and c) The clinical rationale for administering fentanyl ROOs for BTcP treatment.
There was a further text-based question that allowed the experts to provide a figure for the prevalence of BTcP, as informed by their own clinical practice.
Finally, we asked 10 closed-ended questions about any perceived differences between the different systems or routes to administer fentanyl ROOs and the preferences of participants.
Panelists were asked to indicate their level of agreement with each statement using a nine-point Likert scale (one being “strongly disagree,” nine being “strongly agree”). Free text space was also provided to encourage comments.
Consensus definition and data analysis
The median response (MED) and interquartile range (IQR) were calculated for each statement. The level of agreement required for consensus among the panel members was decided prior to commencing the study.
Each statement that reached a consensus with the respondents was defined as a median consensus score (MED) of ≥7, and agreement among panelists as an interquartile range (IQR) of ≤3. Similarly, a MED score of ≤3 was considered to represent a consensus to reject the statement.
An IQR of ≥4 required a review of the criteria by the SC (via discussion). The statements in question were then either revised and included in the second questionnaire, or rejected based on additional comments received from panel members.
The questionnaire used in the second round contained the previous median and IQR of the ratings obtained in the first round for each retested statement, as well as some comments to clarify the wording. Respondents were asked to re-rate each item, using the information from the previous round as feedback, and to comment upon their rating. After the second round, the revised MED and IQR values were calculated.
Results
The participants were made up of expert oncologists from 14 of Spain’s 17 Autonomous Communities. In the first round, 69 out of the 71 identified experts (97.2%) responded (male, n=29; 42%). Of the 69 questionnaires received, 66 were complete, two had two missing items and one had three missing items. All 69 respondents who took part in the first round also responded to the second one with a 100% compliance rate (no missing items). Response rates are shown in Figure 1. The statements provided for consideration and subsequent consensus among participants are shown in Table 1.
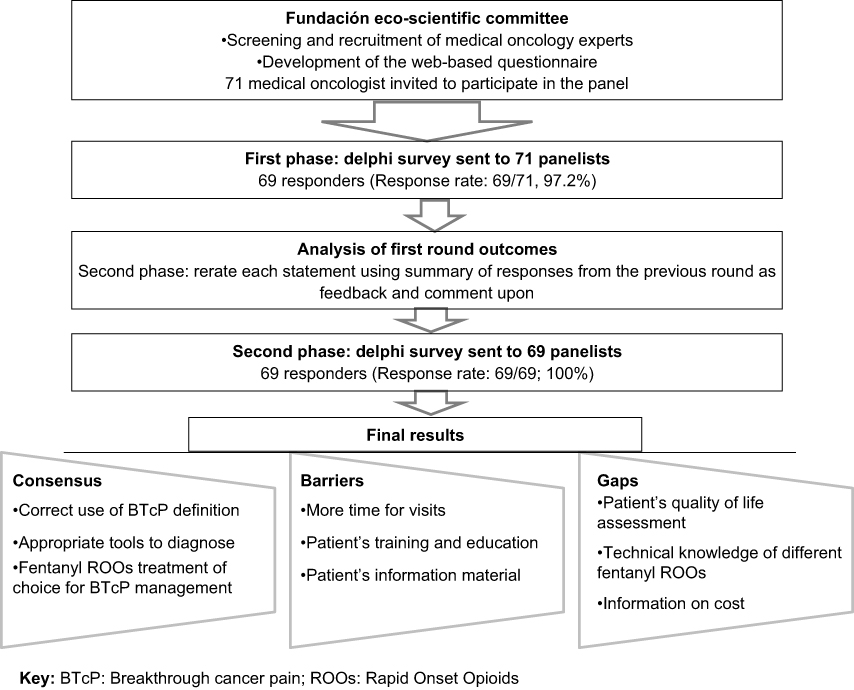 |
Figure 1 Flowchart of participants in the study. |
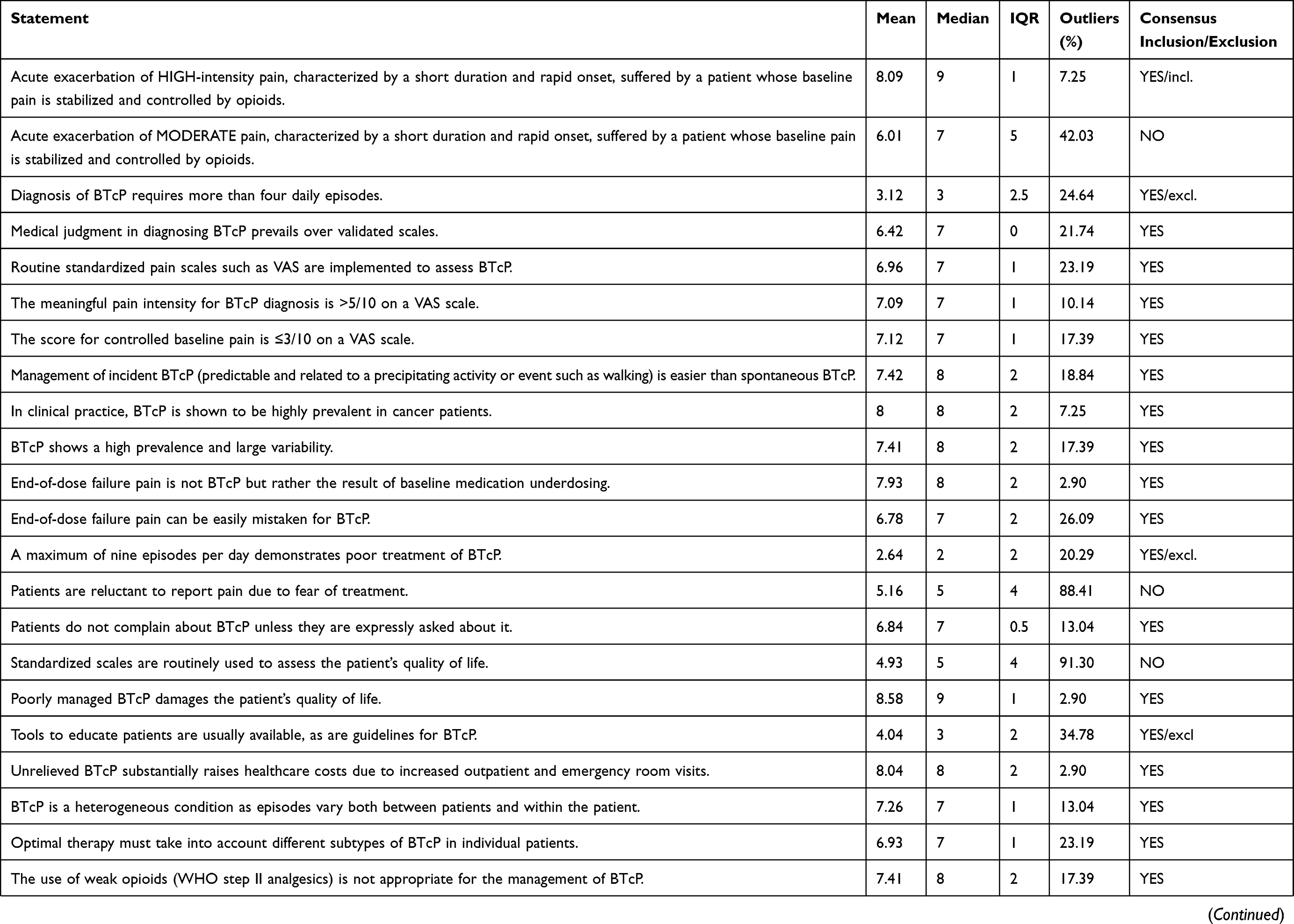 |
Table 1 Attributes considered for the diagnosis and management of BTcP by fentanyl rapid-onset opioids, and the consensus among participants |
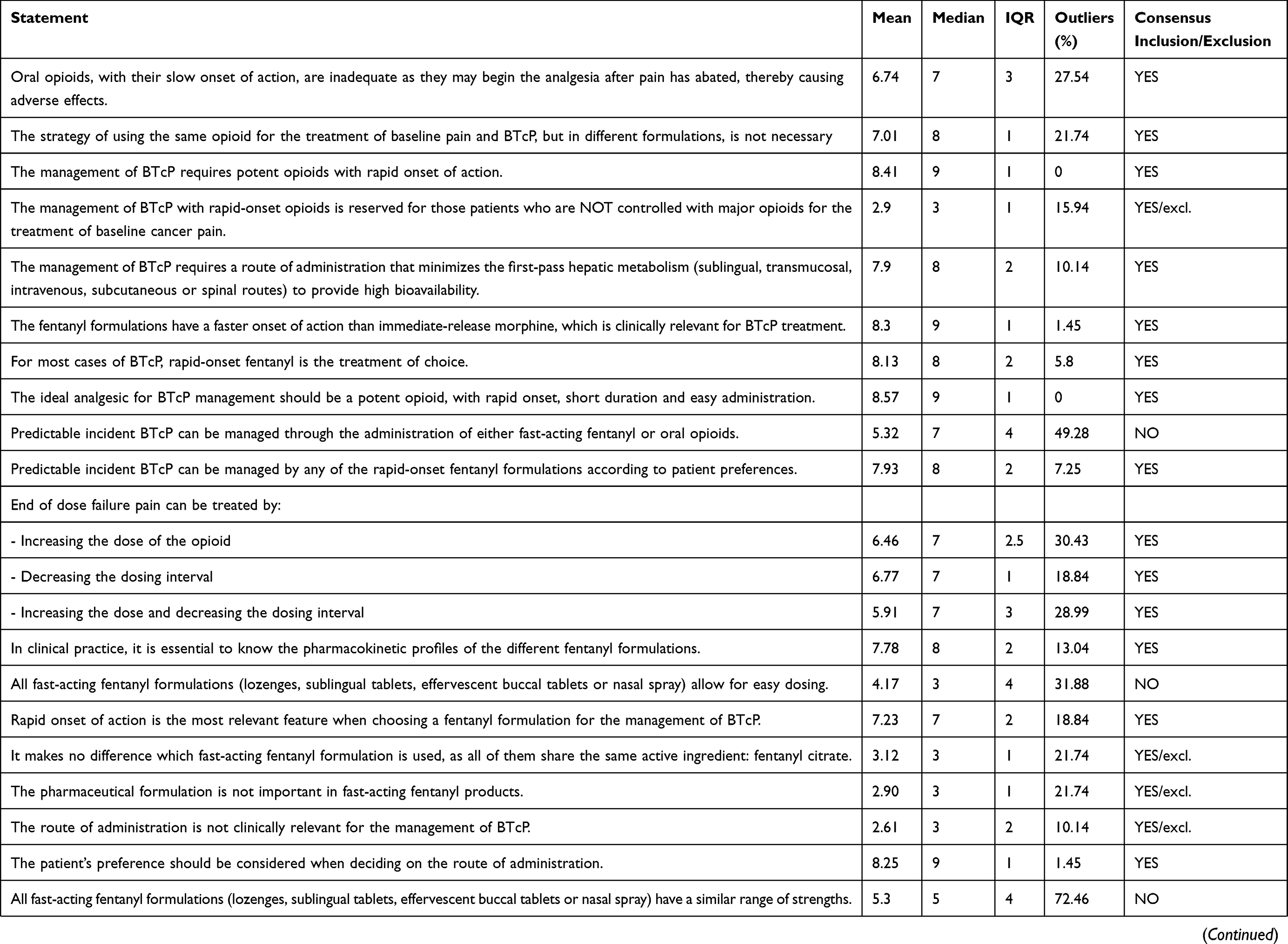 |
Table 1 (Continued). |
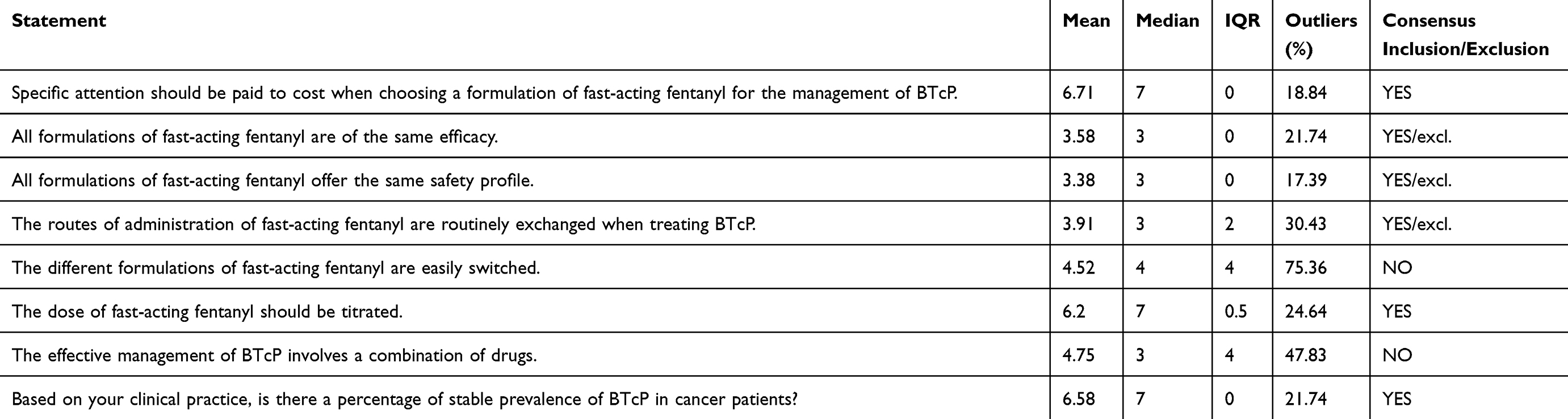 |
Table 1 (Continued). |
Definition and assessment of BTcP
Regarding the definition of BTcP, the experts strongly agreed upon it being an “Acute exacerbation of high-intensity pain of short duration and rapid onset, suffered by a patient whose baseline pain is stabilized and controlled by opioids” (MED=9, IQR=1). In contrast, the statement defining BTcP as “moderate” failed to reach an acceptable level of agreement after the second round (MED=7, IQR=5).
When rating the characteristics and assessment criteria for BTcP diagnosis, experts reached acceptable consensus scores after the second round on the majority of criteria. The statement “diagnosis of BTcP requires more than four daily episodes” failed to confirm a consensus, but did reach quite a high level of agreement (IQR=2.5). Qualitative comments made by the experts reflected the idea that establishing a minimum number of episodes could not help to define whether a patient was suffering from BTcP, and that an isolated episode could be diagnosed and managed as BTcP. Interestingly, in the first round, the statement “Validated pain assessment tools should be used in diagnosing BTcP” reached quite a high consensus score among the experts (MED =7, IQR=3). In the second round, the item was slightly changed to “Medical judgment in diagnosing BTcP prevails over validated scales”, which improved agreement levels (IQR=0). The statement “A maximum of nine episodes per day demonstrates a poor treatment of BTcP” was rejected (MED=2, IQR=2). This was done on the grounds that over four episodes a day should be considered a case of poor baseline pain analgesia rather than BTcP. There was no consensus on the statement “Patients are reluctant to report pain due to fear of treatment” (MED=5, IQR=4). The item regarding the assessment of QoL failed to reach a consensus (MED=5, IQR=4) and the item on the availability of tools to educate patients (MED=3, IQR=2) reached a negative consensus, indicating disagreement. Qualitative comments agreed that such statements were justified, but emphasized that they did not reflect daily clinical practice.
Therapeutic approach in BTcP
After the second round, a high level of consensus and an acceptable level of agreement were obtained in regard to almost all of the statements. Particularly the following statements: “potent, rapid-onset opioids should be used to treat BTcP” (MED=9, IQR=1); “rapid-onset fentanyl is the treatment of choice for most patients suffering from BTcP” (MED=8, IQR=2); “the strategy of using the same opioid, although in different formulations for baseline pain and BTcP, is not necessary” (MED=8, IQR=1); and “incidental BTcP related to a predictable trigger factor can be treated with different fentanyl formulations, taking the patient’s preference into account” (MED=8, IQR=2).
Panelists rejected the use of weak opioids (WHO step II analgesics) as the treatment of choice for BTcP (MED=8, IQR=2), as well as the use of immediate-release oral opioids due to their slow onset of action (MED=7, IQR=3).
Clinical rationale for administering rapid-onset fentanyl opioids for BTcP
After the first round, items relating to cost-effectiveness were removed from the questionnaire after panelists expressed their unfamiliarity with medication costs. Even so, they reached a consensus, and arrived at an adequate level of agreement, in terms of taking costs into account when choosing a formulation for BTcP management (MED=7, IQR=0). There was widespread consensus that clinical practice implies knowing the pharmacokinetic profile of the different fentanyl formulations (MED=8, IQR=2). Consequently, statements suggesting the bioequivalence or therapeutic equivalence with regard to prescribing the different formulations were ultimately rejected. Patients should play an increasingly active role in therapeutic choices (MED=9, IQR=1).
The survey which researched the preferred route of administration revealed a marked bias towards sublingual administration in terms of patient and clinician preferences, usability in different care settings, and ease of administration for physically disabled patients. The intranasal administrative route was considered to provide a faster onset of action, and to be more suitable for patients suffering mucositis. Oral transmucosal delivery scored the lowest across all items. Table 2.
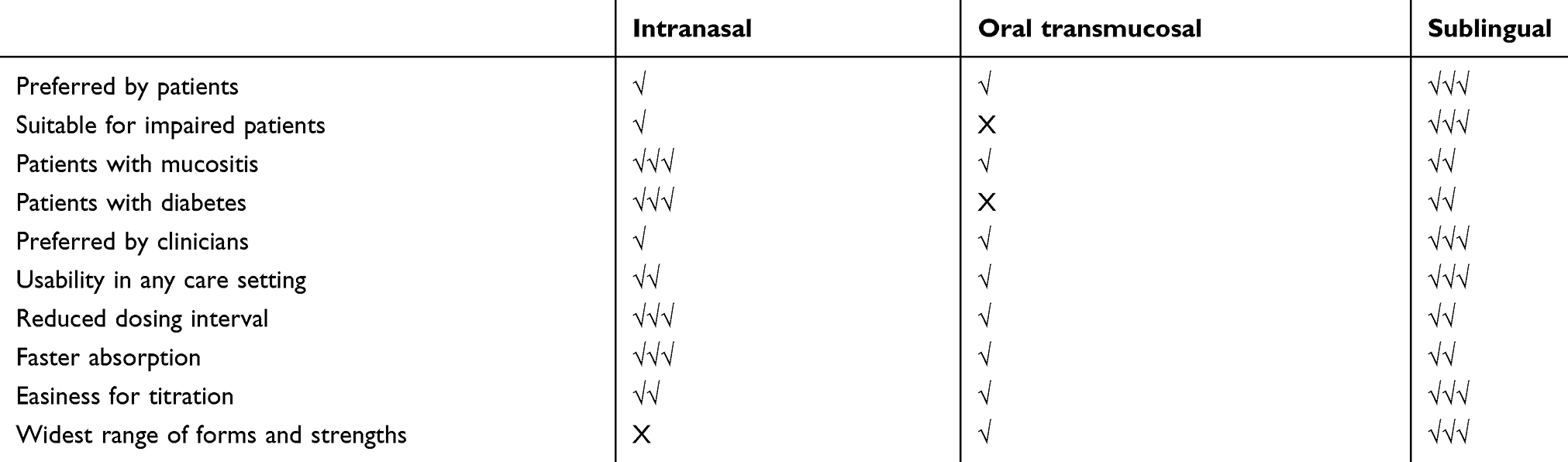 |
Table 2 Indications, contraindications and pharmacokinetics of the different routes of administration of rapid onset fentanyl |
Lastly, the open-ended question revealed a high consensus and total agreement with regard to the prevalence of BTP in cancer patients (MED=7; IQR=0). The figures, stated by the experts, ranged from 20–80%. Interestingly, one expert provided a figure of 100% for both lung and genitourinary cancers.
Discussion
The purpose of this study was to reach a consensus that would lay the foundations for the appropriate management of BTP in cancer patients. The first step of clinical diagnosis is to discuss the pain. Therefore, the physician should make sure to ask the patient explicitly about pain flares until a diagnosis of BTcP can be confirmed.27 There was a difference of opinion among respondents concerning the definition of BTcP. Most experts agreed that the qualifier “high” should be included in the definition, but rejected “moderate;” this is in line with the well-illustrated controversy present in medical literature.11,12,22 Therefore, this result demonstrates that BTcP implies a severe pain, in terms of intensity levels.
According to the experts, diagnosing BTcP depends on the presence of well-controlled background pain, which means that the development and progression of BTcP may also represent problems related to undertreated baseline pain. The guidelines consider that “adequate control of baseline pain” is an essential prerequisite to begin specific treatment for BTcP. However, no clear definition exists in scientific literature.15 In clinical practice, analgesic therapy for BTcP should be based on integration into the background pain’s therapeutic strategy. However, it is not always easy to distinguish BTcP from variations in the outcome assessment of baseline pain (for instance, end-of-dose pain).
A recent study found that where patients had background pain of ≤4/10 on a numerical scale, the meaningful pain intensity at which they asked for BTcP medication was approximately 7/10.28 The experts participating in the present study agreed that ≤3/10 on a VAS scale means “controlled,” implying very mild background pain. Consequently, >5/10 means “moderate” pain, and it is from this point on the scale that BTcP should be assessed.
Regarding the statements on the use of opioids in managing BTcP, oncologists showed a great amount of knowledge. The SEOM (Spanish Society for Medical Oncology) recommendations29 and ESMO30 and EAPC guidelines8 state that ROOs should be considered first-line treatment for BTcP. In 2008, a survey conducted in Spain reported that fentanyl was largely the opioid most commonly used for treating cancer pain.31 Indeed, clinicians showed appropriate knowledge in the safe and effective use of rapid-onset fentanyl preparations. However, they scored poorly when asked about specific clinical scenarios and their scientific and technical knowledge regarding the different systems and routes of administration. These gaps in their knowledge concur with the findings of previous studies conducted in the USA and Asia, indicating that oncologists may not fully realize these weaknesses in their knowledge.32,33
Experts also highlighted a noteworthy concern: limited attention is paid to QoL, despite its importance in patient well-being. In line with this, a recent pan-European survey found that adult oncology patients expressed that physicians were not interested in their QoL.5 Similarly, 52% of patients surveyed by the American Pain Foundation reported that they were told BTcP was a normal side effect of cancer and/or its treatment.34 In this context, the present study identified a need to disseminate information and raise awareness among medical oncologists about the burden of BTcP on QoL. With that in mind, they can carry out their role correctly when dealing with this condition.
As for barriers to managing BTcP, experts denied that patients were reluctant to report pain. They did emphasize, however, the absence of clear, appropriate information available to patients, as well as the limited amount of time they had in clinical practice to discuss pain and educate them about pain management. These results are similar to those reported in different surveys from all around the world,32,33,35 in which time limitations and patient training were identified as significant barriers to the effective management of BTcP. Thus, it is apparent that there is a need for the development of patient information resources that provide clear and simple instructions, as education and patient compliance have been identified as the most important factors in appropriately managing pain.2
While there was a strong consensus that “Specific attention should be paid to cost when choosing a fast-acting fentanyl formulation for BTcP management” (MED=7; IQR=0), it should be noted that questions about cost were withdrawn in the second round due to qualitative comments reporting a lack of knowledge about prices. This finding concurs with the lack of cost-effectiveness analyses on BTcP treatments36 and oral fentanyl formulations, as recently stated by Italian clinicians.37 Doctors who prescribe these medications are aware of the substantial difference in cost between fentanyl formulations and immediate-release morphine or oxycodone,38 but cost-effectiveness analyses are needed in order to help them to select the best formulation.37
In BTcP treatment, rapid onset of action and ease of use are universal variables in the prescription process across all care settings. That being said, we should note that the characteristics of BTcP, the preferences of the patient, and the therapeutic setting may influence their first therapeutic choice. A possible change in therapeutic choice and the route of administration should also be taken into consideration.
Although comparison studies among different fentanyl formulations are lacking, results from different studies showed that the sublingual route is well accepted by patients in terms of ease and modality of administration, mucoadhesivity, and their overall satisfaction,39,40 which is in line with the preferences reported in our study. Intranasal administration seems promising, but involves the mandatory use of specific delivery devices which affects usability.41 The oral transmucosal route of administration received a lower score for modality of administration and the time taken to achieve pain relief; furthermore, this approach requires experienced patients.16,17
In short, oncologists must be aware of the particular features of each medication, such as the different pharmacokinetics, titration specifics, dosing intervals, and the technical characteristics of its accessibility and delivery, as well as possible limitations in everyday clinical practice. According to our Delphi survey (items with or without consensus), there are apparent knowledge gaps to be filled. Therefore, our results will need to be taken into consideration when planning future trial analyses on fentanyl formulations, so as to extract all the necessary information to answer unresolved questions about its use; new trials must be also developed.
Furthermore, the needs identified, regarding the assessment and treatment of BTcP and the lack of awareness surrounding its impact on patients’ QoL, could be used to devise and disseminate useful indications and recommendations (which could then be included in training programs for oncologists).
The limitations of this study include its declared focus on opioids, which has led to a lack of results in terms of the final consensus concerning the integration of other treatment strategies and methods. Moreover, this survey was devised to develop and evaluate a consensus to specifically address severe BTP that results from cancer or cancer treatment. It is therefore possible that if an alternative approach were used, different criteria would be needed to carry out the study.
Finally, the consensus, based on expert opinion, represents a low level of evidence with potential for bias, and thus may not be entirely accurate. Although we selected our panel using an empirical approach based on clinical expertise, we must consider the possibility of collecting more diverse responses if we had a different selection of respondents as palliative care physicians or anaesthesiologists.
Conclusion
These findings represent a pragmatic approach to the diagnosis and pharmacological management of severe BTcP. The documented consensus can act as a useful tool to analyze current clinical practice. It also provides a framework for properly inquiring about RCTs and for evaluating the efficiency and safety of the various ROOs formulations.
This consensus does not include specific treatment recommendations. This is due to the currently established rule of adjusting the dosage and route of administration according to the individual needs of each patient: individualization of BTcP opioid therapy is key to implementing the most effective treatment.
Acknowledgments
The authors acknowledge all the medical oncologists who answered the survey, as their contribution to this research is invaluable. We also acknowledge the members of the Foundation for Excellence and Quality in Oncology for their support. This study was funded by Kyowa Kirin Farmacéutica S.L.U. through the Foundation. Kyowa Kirin Farmacéutica was not involved in the selection of participants nor the content of this study.
Disclosure
Professor A Carrato reports personal fees from Roche, Bayer, Merck, Servier, and MSD, outside the submitted work. Professor E Díaz-Rubio reports personal fees from Merck Serono, Amgen, Bayer, Servier, MSD, and Amgen, and grants from Amgen, Lilly, Roche, Merck Serono, and AstraZeneca, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Caraceni A, Martini C, Zecca E, et al. Breakthrough pain characteristics and syndromes in patients with cancer pain. Int Surv. 2004;18(3):177–183.
2. Webber K, Davies AN, Cowie MR. Breakthrough pain: a qualitative study involving patients with advanced cancer. Support Care Cancer. 2011;19(12):2041–2046. doi:10.1007/s00520-010-1062-z
3. Deandrea S, Corli O, Consonni D, Villani W, Greco MT, Apolone G. Prevalence of breakthrough cancer pain: a systematic review and a pooled analysis of published literature. J Pain Symptom Manage. 2014;47(1):57–76. doi:10.1016/j.jpainsymman.2013.02.015
4. Portenoy RK, Bruns D, Shoemaker B, Shoemaker SA. Breakthrough pain in community-dwelling patients with cancer pain and noncancer pain, part 2: impact on function, mood, and quality of life. J Opioid Manag. 2010;6(2):109–116.
5. Breivik H, Cherny N, Collett B, et al. Cancer-related pain: a pan-European survey of prevalence, treatment, and patient attitudes. Ann Oncol. 2009;20(8):1420–1433. doi:10.1093/annonc/mdp001
6. Davies AN, Dickman A, Reid C, Stevens A-M, Zeppetella G. The management of cancer-related breakthrough pain: recommendations of a task group of the science committee of the association for palliative medicine of great Britain and Ireland. Eur J Pain. 2009;13(4):331–338. doi:10.1016/j.ejpain.2008.06.014
7. Zeppetella G, Davies AN. Opioids for the management of breakthrough pain in cancer patients. Cochrane Database Syst Rev. 2013;10:Cd004311.
8. Caraceni A, Hanks G, Kaasa S, et al. Use of opioid analgesics in the treatment of cancer pain: evidence-based recommendations from the EAPC. Lancet Oncol. 2012;13(2):e58–e68. doi:10.1016/S1470-2045(12)70040-2
9. Breuer B, Fleishman SB, Cruciani RA, Portenoy RK. Medical oncologists’ attitudes and practice in cancer pain management: a national survey. J Clin Oncol. 2011;29(36):4769–4775. doi:10.1200/JCO.2011.35.0561
10. Greco MT, Roberto A, Corli O, et al. Quality of cancer pain management: an update of a systematic review of undertreatment of patients with cancer. J Clin Oncol 2014;32(36):4149–4154.
11. Haugen DF, Hjermstad MJ, Hagen N, Caraceni A, Kaasa S. Assessment and classification of cancer breakthrough pain: a systematic literature review. Pain. 2010;149(3):476–482. doi:10.1016/j.pain.2010.02.035
12. Lohre ET, Klepstad P, Bennett MI, et al. From “breakthrough” to “episodic” cancer pain? A European association for palliative care research network expert Delphi survey toward a common terminology and classification of transient cancer pain exacerbations. J Pain Symptom Manage. 2016;51(6):1013–1019. doi:10.1016/j.jpainsymman.2015.12.329
13. Davies AN, Elsner F, Filbet MJ, et al. Breakthrough cancer pain (BTcP) management: a review of international and national guidelines. BMJ Support Palliat Care. 2018;8(3):241–249. doi:10.1136/bmjspcare-2017-001467
14. O’Hagan P, Mercadante S. Breakthrough cancer pain: the importance of the right treatment at the right time. Eur J Pain. 2018;22(7):1362–1374. doi:10.1002/ejp.1225
15. Vellucci R, Mediati RD, Gasperoni S, Mammucari M, Marinangeli F, Romualdi P. Assessment and treatment of breakthrough cancer pain: from theory to clinical practice. J Pain Res. 2017;10:2147–2155. doi:10.2147/JPR.S135807
16. Mercadante S. Breakthrough pain in cancer patients: prevalence, mechanisms and treatment options. Curr Opin Anaesthesiol. 2015;28(5):559–564. doi:10.1097/ACO.0000000000000224
17. Simon SM, Schwartzberg LS. A review of rapid-onset opioids for breakthrough pain in patients with cancer. J Opioid Manag. 2014;10(3):207–215. doi:10.5055/jom.2014.0209
18. Scottish Intercollegiate Guidelines Network. Control of pain in adults with cancer. A national clinical guideline. Elliott House: Edinburgh; 2008.
19. Virizuela JA, Escobar Y, Cassinello J, Borrega P. Treatment of cancer pain: Spanish Society of Medical Oncology (SEOM) recommendations for clinical practice. Clin Transl Oncol. 2012;14(7):499–504. doi:10.1007/s12094-012-0831-1
20. Zeppetella G, Davies A, Eijgelshoven I, Jansen JP. A network meta-analysis of the efficacy of opioid analgesics for the management of breakthrough cancer pain episodes. J Pain Symptom Manage. 2014;47(4):772–785.e775. doi:10.1016/j.jpainsymman.2013.05.020
21. Smith H. A comprehensive review of rapid-onset opioids for breakthrough pain. CNS Drugs. 2012;26(6):509–535. doi:10.2165/11630580-000000000-00000
22. Mercadante S, Portenoy RK. Breakthrough cancer pain: twenty-five years of study. Pain. 2016;157(12):2657–2663. doi:10.1097/j.pain.0000000000000721
23. Zeppetella G. Breakthrough pain in cancer patients. Clin Oncol (R Coll Radiol). 2011;23(6):393–398. doi:10.1016/j.clon.2010.12.002
24. Boceta J, De la Torre A, Samper D, Farto M, Sanchez-de la Rosa R. Consensus and controversies in the definition, assessment, treatment and monitoring of BTcP: results of a Delphi study. Clin Transl Oncol. 2016;18(11):1088–1097. doi:10.1007/s12094-016-1490-4
25. Escobar ÁY. Diagnóstico y tratamiento del dolor irruptivo oncológico: recomendaciones de consenso. Revista de la Sociedad Española del Dolor 2013;20(2):61–68.
26. Porta-Sales J, Perez C, Escobar Y, Martinez V. Diagnosis and management of breakthrough cancer pain: have all the questions been resolved? A Delphi-based consensus assessment (DOIRON). Clin Transl Oncol. 2016;18(9):945–954. doi:10.1007/s12094-015-1468-7
27. Webber K, Davies AN, Cowie MR. Accuracy of a diagnostic algorithm to diagnose breakthrough cancer pain as compared with clinical assessment. J Pain Symptom Manage. 2015;50(4):495–500. doi:10.1016/j.jpainsymman.2015.05.006
28. Mercadante S, Adile C, Torta R, et al. Meaningful cut-off pain intensity for breakthrough pain changes in advanced cancer patients. Curr Med Res Opin. 2013;29(1):93–97. doi:10.1185/03007995.2012.755120
29. Jara C, Del Barco S, Gravalos C, et al. SEOM clinical guideline for treatment of cancer pain (2017). Clin Transl Oncol. 2018;20(1):97–107. doi:10.1007/s12094-017-1791-2
30. Fallon M, Giusti R, Aielli F, et al. Management of cancer pain in adult patients: ESMO clinical practice guidelines. Ann Oncol. 2018;29(Supplement_4):iv166–iv191. doi:10.1093/annonc/mdy152
31. Escobar Alvarez Y, Rodriguez Sanchez CA, Caballero Martinez F, Recuero Cuervo V, Camps Herrero C. Professional survey on knowledge and clinical patterns of pain management in Spanish medical oncology. Clin Transl Oncol. 2010;12(12):819–824. doi:10.1007/s12094-010-0603-8
32. Breuer B, Chang VT, Von Roenn JH, et al. How well do medical oncologists manage chronic cancer pain? A national survey. Oncologist. 2015;20(2):202–209. doi:10.1634/theoncologist.2014-0276
33. Kim YC, Ahn JS, Calimag MM, et al. Current practices in cancer pain management in Asia: a survey of patients and physicians across 10 countries. Cancer Med. 2015;4(8):1196–1204. doi:10.1002/cam4.471
34. American Pain F. Breakthrough cancer pain: mending the break in the continuum of care. J Pain Palliat Care Pharmacother. 2011;25(3):252–264. doi:10.3109/15360288.2011.599920
35. Carulla Torrent J, Jara Sanchez C, Sanz Ortiz J, et al. Oncologists’ perceptions of cancer pain management in Spain: the real and the ideal. Eur J Pain. 2007;11(3):352–359. doi:10.1016/j.ejpain.2006.05.006
36. Perez-Hernandez C, Jimenez-Lopez AJ, Sanz-Yague A, Mar-Medina J, Larranaga I, Soler-Lopez B. Observational study evaluating the economic impact of breakthrough pain in cancer patients in clinical practice in Spain: the IMDI study. Pain Ther 2018;7(2):227–240. doi:10.1007/s40122-018-0102-0
37. Cortesi PA, D’Angiolella LS, Vellucci R, et al. Cost-effectiveness analysis of oral fentanyl formulations for breakthrough cancer pain treatment. PloS One 2017;12(6):e0179523.
38. Janknegt R, van den Beuken M, Schiere S, et al. Rapid acting fentanyl formulations in breakthrough pain in cancer. Drug selection by means of the system of objectified judgement analysis. Eur J Hosp Pharm. 2018;25(3):e2. doi:10.1136/ejhpharm-2016-001127
39. England R, Maddocks M, Manderson C, Zadora-Chrzastowska S, Wilcock A. How practical are transmucosal fentanyl products for breakthrough cancer pain? Novel use of placebo formulations to survey user opinion. BMJ Support Palliat Care. 2011;1(3):349–351. doi:10.1136/bmjspcare-2011-000037
40. Moore N, Darwish M, Amores X, Schneid H. A review of the pharmacokinetic profile of transmucosal fentanyl formulations. Curr Med Res Opin. 2012;28(11):1781–1790. doi:10.1185/03007995.2012.735227
41. Zucco F, Bonezzi C, Fornasari D. Breakthrough cancer pain (BTcP): a synthesis of taxonomy, pathogenesis, therapy, and good clinical practice in adult patients in Italy. Adv Ther. 2014;31(7):657–682. doi:10.1007/s12325-014-0130-z
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.