")
Back to Journals » Psychology Research and Behavior Management » Volume 13
Work-Related Stress and Associated Factors Among Textile Factory Employees in Northwest Ethiopia: A Cross-Sectional Study
Authors Belete H , Ergetie T, Ali T , Birhanu S , Belete T
Received 15 September 2020
Accepted for publication 11 November 2020
Published 27 November 2020 Volume 2020:13 Pages 1071—1078
DOI https://doi.org/10.2147/PRBM.S282061
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Igor Elman
Habte Belete,1 Temesgen Ergetie,1 Tilahun Ali,2 Simon Birhanu,3 Tilahun Belete1
1Department of Psychiatry, College of Medicine and Health Sciences, Bahir Dar University, Bahir Dar, Ethiopia; 2Department of Psychiatry, School of Nursing and Midwifery, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia; 3Department of Nursing, School of Nursing and Midwifery, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia
Correspondence: Tilahun Ali Email [email protected]
Background: Work-related stress is becoming an alarmingly growing public health concern worldwide. Textile factories are among the most common manufacturing industries that have a higher rate of work-related stress. Investigating the prevalence and factors associated with work-related stress will help planners and decision-makers at every level in planning, managing, and evaluating the health status of the employees. Research evidence is limited for work-related stress in Northwest Ethiopia. Therefore, this study was aimed to assess work-related stress and associated factors among textile factory employees in Northwest Ethiopia.
Methods: A cross-sectional study design was employed among 403 employees in Bahir Dar Textile Factory. Data were collected using an interviewer administered questionnaire, then entered into EpiData version 3.1, and analyzed using SPSS version 22 software. Descriptive statistics, bivariate and multivariate logistic regressions were carried out. In logistic regression analysis, adjusted odds ratio (AOR), along with 95% confidence interval (CI), was used to identify the associated factors of work-related stress. A P-value< 0.05 was considered as statistically significant.
Results: The prevalence of work-related stress was 45.2%, with 95% CI=40.0– 50.1%. Working in rotational shifts (AOR=2.33, 95% CI=1.34– 4.03), current substance use (AOR=5.67, 95% CI=3.38– 9.52), poor and medium social support (AOR=3.75, 95% CI=1.71– 8.21 and AOR=3.26, 95% CI=1.39– 7.64) were significantly associated factors with work-related stress, respectively.
Conclusion and Recommendation: Near to half of the study participants had work-related stress. Work shift, substance use, and social support were among the factors which affect work-related stress. Thus, interventions that could reduce work-related stress such as stress management programs should be considered.
Keywords: prevalence, work-related stress, textile factory, employee, Ethiopia
Introduction
Work-related stress is an alarmingly growing public health problem that could result in serious social and economic consequences that could be prevented if appropriate measures are taken.1,2 The World Health Organization (WHO) broadly defines work-related stress as
the reaction people may have when presented with work demands and pressures that are mismatched to their knowledge and abilities that challenges their ability to cope3.
The working environment has a major influence on the mental health and behavioral well-being of individual employees.4,5 In the current modern and turbulent working environment, making the employees work with high stress and pressurized conditions could lead to risk for a variety of mental health problems in which work-related stress is amongst the first line problem.6,7 Work-related stress is one of the leading contributors of global burden of disease in terms of its adverse emotional, psychological, and physiological impact of workers across the world and more impactful for those living in developing countries.1,7,8 Thus, work-related stress has resulted in a substantial multifaceted impact to employees and decrement in organizational productivities.9,10 Unless work-related stress (WRS) has been monitored at the beginning, it can lead to a considerable decrease in employee performance to the success of the organization in terms of higher turnover number, repeated absenteeism from duties, and link to misbehavior in employees such as psychoactive substance misuse and sleep disturbance.11,12 When an employee’s performance decreased, it resulted in reduction of productivity, accident and injury, compensation, and treatment costs for injured workers.13,14
The prevalence of work-related stress has been reported in a wide range of differences across the globe. It has been found to be 25% in India,15 27.5% in Thailand,16 21.3% in Iran,17 28% in the Democratic Republic of Congo,18 and 40.4% in Ethiopia among employees in a shoe manufacturing factory.19 Work-related stress is also common among healthcare professionals working in different public healthcare facilities in Mekele and Bahir Dar, Ethiopia that revealed the prevalence to be 48.6%20 and 46.9%,21 respectively.
Previous research findings reported that the risk of work-related stress, its severity, and impacts have been varied depending on cultural orientation, nature of the work, and working environments. Some of the factors that lead employees to WRS were working in shift,22 psychoactive substance use,23 social support,24,25 socio-professional factors, and demographic factors such as age.18
Although the impact and burden of WRS is huge, there is a limited study available in Ethiopia regarding magnitude and associated factors of WRS among employees in the textile factories.
Therefore, the aim of this study was to assess the prevalence and associated factors of work-related stress among Bahir Dar textile share company employees in Northwest Ethiopia.
Materials and Methods
Study Design and Period
An institutional-based cross-sectional study design was employed from March to April 2019, at Bahir Dar textile share company, Northwest Ethiopia.
Study Setting
The study was conducted in Bahir Dar city which is the capital city of Amara regional state. Bahir Dar is located 570 km Northwest of Ethiopia. Bahir Dar Textile Share Company was established in 1961 in Bahir Dar and it was a government owned integrated mill manufacturing 100% woven cotton fabric. In 1989, the factory rehabilitated its spinning and weaving section, replacing most of the machines and renovating the rest. As of September 30, 1999, the factory changed from a public enterprise to a share company. The share company comprises 480,000 square meters, of which 39,200 square meters are covered by buildings. The share company currently has 1,431 employees, of which 799 are males and 632 are females. Seventy-nine percent of the company employees work in the main product sections. The remaining 21% of employees are under support process sections.
Study Participants
All employees working in Bahir Dar textile factory were the source population. Employees who were available in their workplace during the study period and those included in the sample were the study population. Employees who were currently engaged in the textile factory and had worked for more than 6 months prior to the data collection were included in the study. Those employees who were seriously ill or on annual leave during the data collection period were excluded from the study.
Sample Size Determination and Sampling Procedure
The sample size required for the study was calculated using a single population proportion formula by considering an estimated prevalence of work-related stress to be 50% (since there is no previous published study among textile factory workers in Ethiopia), a 5% margin of error, a 95% confidence interval, and 10% non-response rate. The final calculated sample size was 423.
A simple random sampling technique was used to select all 423 samples which were proportionally allocated for each working section.
Data Collection Procedures and Tools
The data were collected using a structured interviewer-administered questionnaire adapted from previously conducted studies19,26 through a face-to-face interview to assess sociodemographic, perceived relative wealth, substance use, suicidal behavior, psychosocial and clinical factors, organization and job-related factors, and work-related stress. Other previously validated and reliable tools employed for the purpose were the workplace stress scale (WPSS), job content questionnaire (JCQ),27 and the National Institute for Occupational Safety and Health (NIOSH) generic job stress questionnaire,28 which were used to assess organizational and job content factors. Data on work-related stress was collected using the workplace stress scale (WPSS) which is a 20-item standard questionnaire with a 5-points Likert scale. The score ranges from 1 (never) to 5 (very often).26,29 These instruments were used in a previous study conducted among shoe factory employees in Ethiopia and it is valid and reliable.19
Operational Definition
Workplace stress scale: A sum score below 60 was classified as having a work-related stress among participants.20
The Oslo-3 Social Support Scale (OSS-3): A three-item scale exploring the number of close friends, perceived level of concern from others, and perceived ease of getting help from neighbors was used to assess the level of social support. A score 3–8, 9–11, and 12–14 was considered to have low, medium, and high social support, respectively.30
Suicidal behavior was assessed by using the mini international neuropsychiatric interview and was set based on Diagnostic and Statistical Manual of mental disorders-IV criteria. Based on the instrument, if the participant responded “yes” to one of the six questions, they were considered as a risk for suicidal behavior.24
Substance use: Current and ever substance uses were considered when participants had use of at least one of the specified substances in the last 3 months and use of at least one of the specified substances in a lifetime, respectively, by using the adopted alcohol, smoking, and substance involvement screening test (ASSIST).31
Perceived relative wealth: This was assessed by simply asking the participants what they perceived about their wealth to be in relation to other people in the neighborhood (poor, average, or well-off) and participants were asked to level their own income by comparing with others as less than others; similar to others and better than others. Following previously published work,32,33 we applied the method of principal component analysis to these variables.
Data Quality Control
The questionnaire was prepared in English and then translated into Amharic for data collection and re-translated back into English by language experts. Two days training was provided to the data collectors and supervisors on the data collection tools and the data collection procedures. After that, the questionnaire was pre-tested on 5% of the sample size out of the study area to ensure its validity. Data collectors were closely supervised by the supervisors and the principal investigator. Completeness of each questionnaire was checked on a daily basis. Double data entry was done by two data clerks and consistency of the entered data were cross-checked by comparing the two separately entered data.
Data Processing and Analysis
The collected data were checked for its completeness and cleaned before entry into the computer. Then, data were coded, cleaned, edited, and entered into EpiData version 3.1 and exported to SPSS window version 22 for analysis. Descriptive statistics were presented in frequency, tables, texts, and summary measures.
Bivariate and multivariate analysis were done to see the association between each independent variable and outcome variable by using binary logistic regression. The assumption for binary logistic regression were checked. The goodness of fit was checked by Hosmer-Lemeshow statistic at a P-value of greater than 0.05. All variables with P<0.25 in the bivariate analysis were included in the final model of multivariate analysis in order to control all possible confounders.34 The direction and statistical association were measured by odds ratio with 95% CI. Adjusted odds ratio along with 95% CI was estimated to identify the associated factors with work-related stress by using multivariate analysis in binary logistic regression. In this study, a P-value<0.05 was considered as statistically significant.
Ethical Approval and Consent to Participate
Ethical approval was obtained from the Institutional Health Research Ethics Review Committee (IRB) of Bahir Dar University, and ethical clearance was granted. In addition, a supporting letter was written to Bahir Dar textile share company. The objective and purpose of the study were verified briefly to the study participants and confidentiality was assured. Finally, written informed consent was obtained from the study participants before conducting the interview. This study was conducted in accordance with the Declaration of Helsinki.
Results
Socio-Demographic Characteristics
The response rate was 95.3% (403/423) and, of the 403 respondents, 220 (54.6%) were male. The majority of the participants (83.4%) were Orthodox Christians, and 45.7% of the respondents were married (see Table 1).
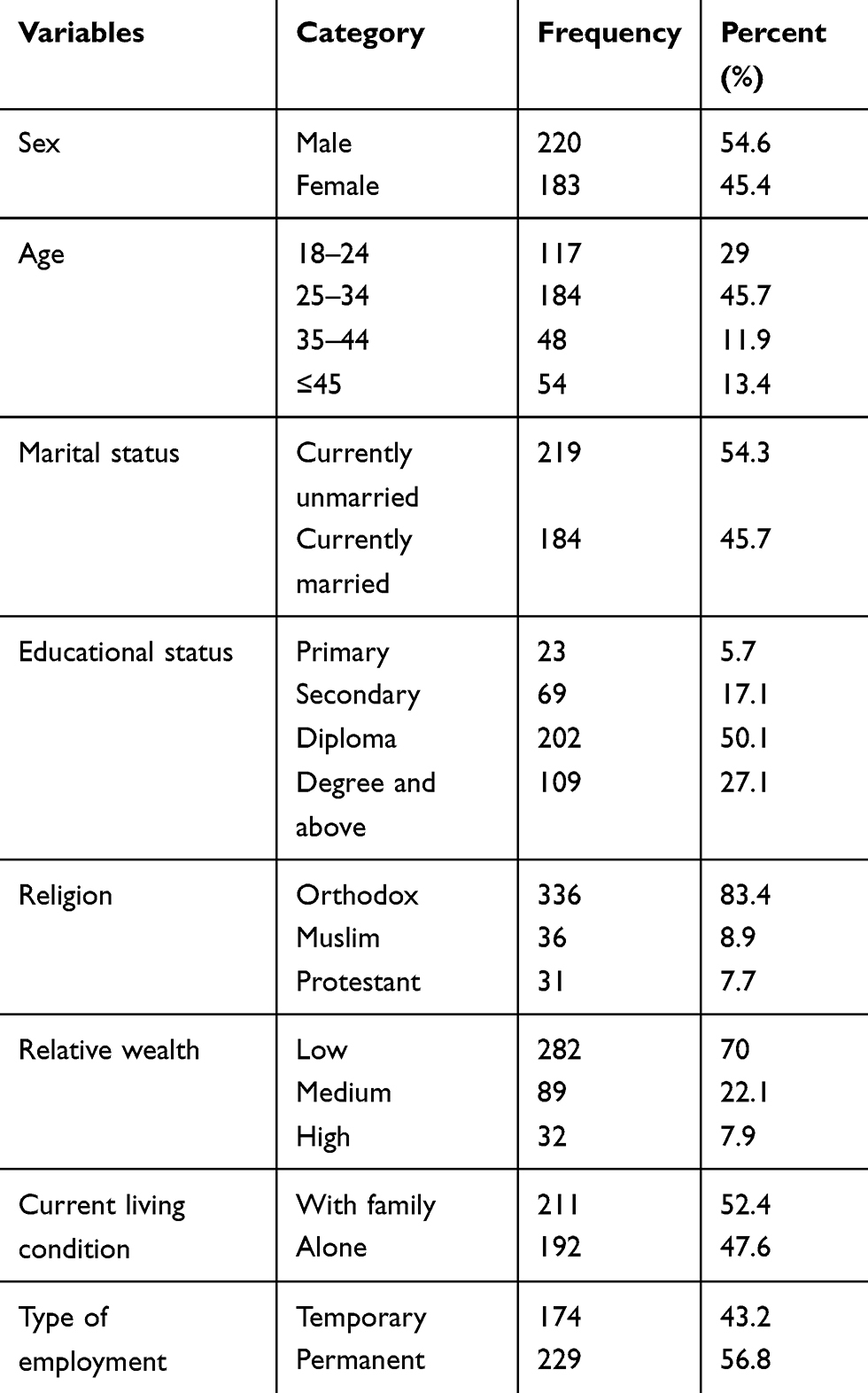 |
Table 1 Socio-Demographic Characteristics of Respondents in Bahir Dar Textile Factory, Ethiopia, 2019 (n=403) |
Substance Use, Suicidal Behavior, Psychosocial and Clinical Characteristics
Of the respondents, 178 (44.2%) had a history of any substance use at least once in their lifetime, while 117 (29.0%) were current substance users. Regarding social support, 251 (62.3%), 98 (24.3%), and 54 (13.4%) of the participants had poor, moderate, and strong support, respectively. The prevalence of suicidal behavior was 60 (14.9%) among the total participants and, of these, 23 (38.3%) had attempted, 41 (68.3%) had a suicidal plan, and 46 (76.7%) had suicidal ideation. One hundred and fifty-four (38.2%) participants had reported having chronic medical illnesses such as hypertension (n=87), tuberculosis (n=32), cardiac illness (n=9), diabetes mellitus (n=21), and kidney disease (n=5).
Organizational and Job-Related Characteristics
There were different work-related problems at the workplace and from the total 77 (19.1%) had reported injury at the workplace, 221 (54.8%) had reported uncomfortable working environment, and 161 (40%) had reported workplace violence (see Table 2).
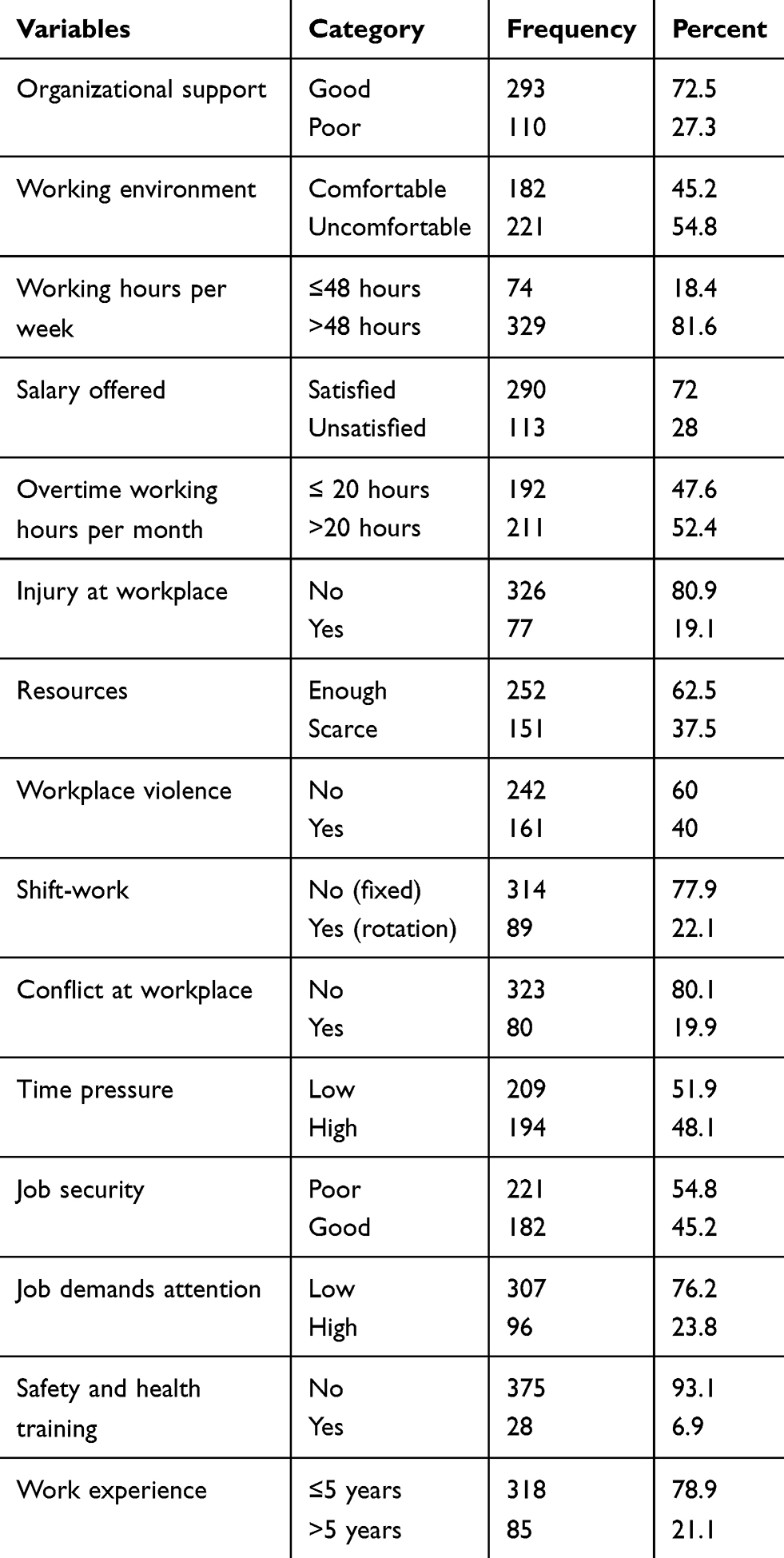 |
Table 2 Organizational and Job-Related Characteristics of Respondents in Bahir Dar Textile Factory, Ethiopia, 2019 (n=403) |
Prevalence of Work-Related Stress
The overall prevalence of work-related stress was 45.2% (95% CI=40.0–50.1%) among textile factory workers. From all the participants who had work-related stress, 46.2% of them had reported workplace violence, while 48.9% of them were current substance users.
Associated Factors of Work-Related Stress
Bivariate and Multivariate Analysis
Table 3 summarizes the results of bivariate and multivariable analyses for associations with work-related stress. In bivariate analysis, the factors that showed a significant association with work-related stress were perceived social support, workplace violence, shift-work, satisfaction with salary, overtime working hours per month, current substance use, injury at workplace, and organizational support (See Table 3).
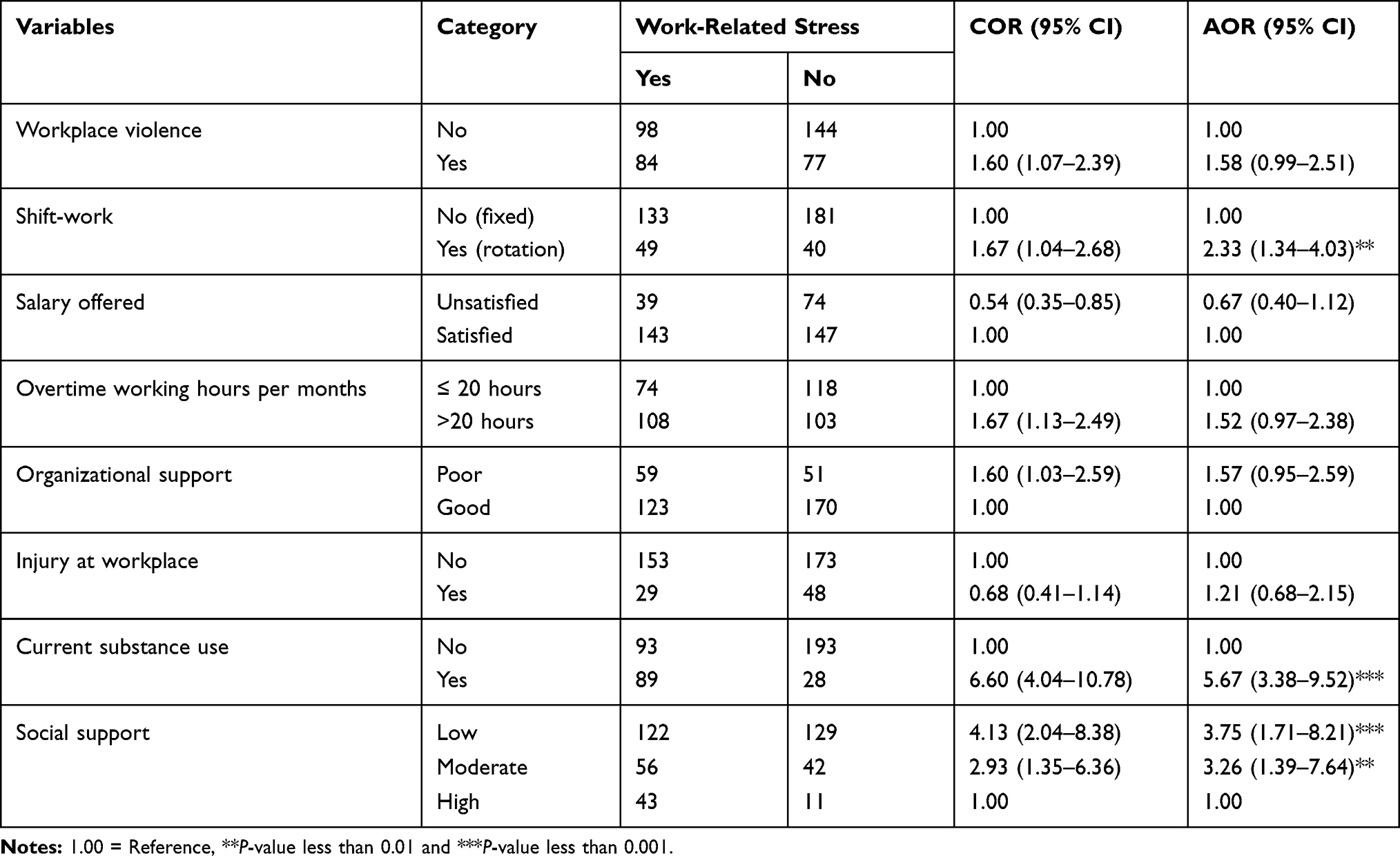 |
Table 3 Factors Associated with Work-Related Stress Among Textile Factory Workers in Bahir Dar Textile Factory, Ethiopia, 2019 (n=403) |
Finally, after multivariate analysis of work-related stress in relation to all independent variables, rotating shift-work, poor and moderate social support, and current substance use (khat, tobacco, alcohol, and caffeinated beverage like coffee) were found to be statistically significant.
The odds of work-related stress was 2-fold among rotating shift workers as compared to their counterparts (AOR=2.33, 95% CI=1.34–4.03). Current substance use (alcohol, khat, cigarette, and caffeinated beverages) was a risk to develop work-related stress as compared with non-users (AOR=5.67, 95% CI=3.38–9.52). Poor social support (AOR=3.75, 95% CI=1.71–8.21), and moderate social support (AOR=3.26, 95% CI=1.39–7.64) were higher risk factors for work-related stress than good social support.
Discussion
In this study, the overall prevalence of work-related stress was 45.2% (95% CI=40.0–50.1). The current study is consistent with previous studies done in West Sussex (43%),35 Dukem, Ethiopia among shoe manufacturing employees (40.4%),19 Bahir Dar, Ethiopia among healthcare professionals working in public health care facilities (48.6%),20 and Mekelle, Ethiopia (46.9%).21 However, it was found to be higher than those studies conducted in the Congo (28%),18 India (25%),15 Thailand (27.5%),16 Iran (21.3%),17 and Bangalore city (26%).36 The current finding was lower than a study conducted in Iran among Nurses (68%).37
The reason for this discrepancy might be explained by differences in the sample size, the study setting, the tools used, and the study populations. Moreover, the variation might be socio-economic status, organized safety precaution training, and access to a health facility in developed countries is better compared to in developing countries.38
The current study showed that work-related stress was associated with substance use and supported by similar studies on alcohol use39–41 and smoking cigarettes42,43 were found to be risk factors for work-related stress. It might be the fact that alcohol use has a strong association with mental distress and common mental disorders such as depressive symptoms and stress among factory workers.44 The other reason could be the direct effect of substances on the brain and the psychosocial effect of substance on individuals with work-related stress. In addition, unmatched work performance and related rewards can create unintended negative consequences in which these unintended consequences are particularly important to start substance use as coping with work-related stress.45
This study also revealed that poor and moderate social support were significantly associated with work-related stress, which is supported by other previous studies conducted in Thailand16 and Belgium.46 Organizational support and close supervisory support have a significant contribution for employees psychological wellbeing in the workplace and are related to job stress.47 This could be explained by the fact that poor social support is a determinant factor of psychopathology like stress and have negative impacts on the employees quality-of-life.48–50
Rotating shift work was associated with work-related stress with the odds of two times and which is supported by studies done in different countries such as Bangladesh,51 India,52 USA,53 Taiwan,54 and Ghana55 which have indicated that employees who worked rotating shifts were more stressed than employees who worked fixed shifts. Shift working has a higher stress level than fixed time workers,56 and this might be due to the fact that rotating shift work affects the normal human circadian rhythm and can lead to numerous psychological and physiological problems.57
Limitation and Strength of the Study
Though this study tried to assess work-related stress, which was not previously studied in this particular working environment, and use a validated and standardized tool to assess variables. One of the limitations of the study was that the nature of the study design could not establish a clear temporal relationship between significantly associated factors and work-related stress.
Conclusion
It has found that a substantial proportion of employees in a textile factory (45.2%) were suffering from work-related stress. Working on shift-work, substance use, and perceived social support were factors significantly associated with work-related stress. Interventions that focuses on reducing work-related stress due to shift work should be considered. Improving the social support status and preventing substance use among employees is important to reduce work-related stress.
Abbreviations
AOR, adjusted odd ratio; CI, confidence interval; JCQ, job content questionnaire; OSSS, Oslo social support scale; NIOSH, National Institute for Occupational Safety and Health; WHO, World Health Organization; WMH, World Mental Health; WPSS, workplace stress scale; WRS, work-related stress.
Data Sharing Statement
The datasets used and analyzed in the current study are included within the article.
Acknowledgments
We acknowledge the entire staff of Bahir Dar textile share company for their cooperation in making this study a success. Our sincere gratitude goes to Bahir Dar University, Research and Dissemination Office for funding the study. We also appreciate the study participants for their cooperation in providing the necessary information.
Author Contributions
HB, TE, TA, SB, and TB were involved in the conception and design of the study, acquisition of data, analysis and interpretation of data, drafting and revising the article, agreed to submit to the current journal, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
The study was funded by Bahir Dar University.
Disclosure
The authors declare that they have no competing interests.
References
1. Houtman I, Jettinghof K, Cedillo L. Raising Awareness of Stress at Work in Developing Countires: A Modern Hazard in a Traditional Working Environment: Advice to Employers and Worker Representatives. World Health Organization (WHO); 2007.
2. Akinboye J, Akinboye D, Adeyemo D. Coping with Stress in Life and Workplace. Ibadan: Stirling-Horden Publishers; 2002.
3. World Health Organization(WHO). Stress at the workplace 2019. Available from: https://www.who.int/occupational_health/topics/stressatwp/en/.
4. Gabriel P, Liimatainen M-R Mental health in the workplace: introduction, executive summaries. 2000.
5. Maulik PK. Workplace stress: a neglected aspect of mental health wellbeing. Indian J Med Res. 2017;146(4):441.
6. Tabassum S. Occupational stress among employees of public and private insurance sector: a comparative study. Amity Glob Bus Rev. 2013;8.
7. Chopra P. Mental health and the workplace: issues for developing countries. Int J Ment Health Syst. 2009;3(1):4.
8. Ratanasiripong P, Kaewboonchoo O, Bell E, et al. Depression, anxiety and stress among small and medium enterprise workers in Indonesia, Malaysia, Thailand, and Vietnam. Int J Occup Health Public Health Nurs. 2016;3(2):13–29.
9. Leka S, Griffiths A, Cox T, Organization WH. Work Organisation and Stress: Systematic Problem Approaches for Employers, Managers and Trade Union Representatives. World Health Organization; 2003.
10. Imtiaz S, Ahmad S. Impact of stress on employee productivity, performance and turnover; an important managerial issue. Int Rev Bus Res Papers. 2009;5(4):468–477.
11. Aderaw Z, Engdaw D, Tadesse T. Determinants of occupational injury: a case control study among textile factory workers in Amhara Regional State, Ethiopia. J Trop Med. 2011;2011.
12. Ongori H, Agolla JE. Occupational stress in organizations and its effects on organizational performance. J Manag Res. 2008;8(3):123–135.
13. Priyadharshini R, Pujar S, Sangeetha R The impact of occupational stress on employees in textile industry: a review. 2017.
14. Demeke A. Assessment of the Utilization of Personal Protective Equipment Among Textile Industry Workers in Dukem Town. Addis Ababa University; 2017.
15. Mohan GM, Elangovan S, Prasad P, Krishna PR, Mokkapati AK. Prevalence of job strain among Indian foundry shop floor workers. Work. 2008;30(4):353–357.
16. Sein MM, Howteerakul N, Suwannapong N, Jirachewee J. Job strain among rubber-glove-factory workers in central Thailand. Ind Health. 2010;48(4):503–510. doi:10.2486/indhealth.MS962
17. Soori H, Rahimi M, Mohseni H. Occupational stress and work-related unintentional injuries among Iranian car manufacturing workers. East Mediterr Health J. 2008;14(3):697–703.
18. Kitronza PL, Mairiaux P. Occupational stress among textile workers in the Democratic Republic of Congo. Trop Med Health. 2015;43(4):223–231. doi:10.2149/tmh.2015-24
19. Etefa MM, Teklu MG, Teshome DF. Work related stress and associated factors among Huajian shoe manufacturing employees in Dukem town, central Ethiopia. BMC Res Notes. 2018;11(1):610. doi:10.1186/s13104-018-3727-5
20. Gebeyehu S, Zeleke B. Workplace stress and associated factors among healthcare professionals working in public health care facilities in Bahir Dar City, Northwest Ethiopia, 2017. BMC Res Notes. 2019;12(1):249. doi:10.1186/s13104-019-4277-1
21. Godifay G, Worku W, Kebede G, Tafese A, Gondar E. Work related stress among health care workers in Mekelle City Administration Public Hospitals, North Ethiopia. Work. 2018;46.
22. von Treuer K, Fuller-Tyszkiewicz M, Little G. The impact of shift work and organizational work climate on health outcomes in nurses. J Occup Health Psychol. 2014;19(4):453. doi:10.1037/a0037680
23. Biron M, Bamberger PA, Noyman T. Work-related risk factors and employee substance use: insights from a sample of Israeli blue-collar workers. J Occup Health Psychol. 2011;16(2):247. doi:10.1037/a0022708
24. Tennant C. Work-related stress and depressive disorders. J Psychosom Res. 2001;51(5):697–704. doi:10.1016/S0022-3999(01)00255-0
25. Bartram T, Joiner TA, Stanton P. Factors affecting the job stress and job satisfaction of Australian nurses: implications for recruitment and retention. Contemp Nurse. 2004;17(3):293–304. doi:10.5172/conu.17.3.293
26. Attitudes in the American Workplace VII. The Workplace Stress Scale. Yonkers: Marlin Company and the American Institute of Stress; 2009.
27. Karasek R, Brisson C, Kawakami N, Houtman I, Bongers P, Amick B. The Job Content Questionnaire (JCQ): an instrument for internationally comparative assessments of psychosocial job characteristics. J Occup Health Psychol. 1998;3(4):322. doi:10.1037/1076-8998.3.4.322
28. NIOSH generic job stress questionnaire. Natl Inst Occup Saf Health. 2011;513:533–8165.
29. Salilih SZ, Abajobir AA. Work-related stress and associated factors among nurses working in public hospitals of Addis Ababa, Ethiopia: a cross-sectional study. Workplace Health Saf. 2014;62(8):326–332. doi:10.1177/216507991406200803
30. Abiola T, Udofia O, Zakari M. Psychometric properties of the 3-item oslo social support scale among clinical students of Bayero University Kano, Nigeria. Malays J Psychiatry. 2013;22(2):32–41.
31. Humeniuk R, Ali R, Babor TF, et al. Validation of the alcohol, smoking and substance involvement screening test (ASSIST). Addiction. 2008;103(6):1039–1047. doi:10.1111/j.1360-0443.2007.02114.x
32. Fekadu A, Medhin G, Selamu M, et al. Population level mental distress in rural Ethiopia. BMC Psychiatry. 2014;14(1):194. doi:10.1186/1471-244X-14-194
33. Filmer D, Pritchett LH. Estimating wealth effects without expenditure data—or tears: an application to educational enrollments in states of India. Demography. 2001;38(1):115–132.
34. Bendel RB, Afifi AA. Comparison of stopping rules in forward “stepwise” regression. J Am Stat Assoc. 1977;72(357):46–53.
35. Phillips S, Sen D, McNamee R. Prevalence and causes of self-reported work-related stress in head teachers. Occup Med (Chic Ill). 2007;57(5):367–376. doi:10.1093/occmed/kqm055
36. Anandi BS, Rajaram D, Aravind B, Sukumar GM, Radhika K. Work-related stress assessment among a garment factory employee in Bangalore suburban locality. Int J Community Med Public Health. 2017;4(10):3870–3876. doi:10.18203/2394-6040.ijcmph20174266
37. Poursadeghiyan M, Abbasi M, Mehri A, Hami M, Raei M, Ebrahimi MH. Relationship between job stress and anxiety, depression and job satisfaction in nurses in Iran. Soc Sci. 2016;11(9):2349–2355.
38. Jamison DT, Summers LH, Alleyne G, et al. Global health 2035: a world converging within a generation. Lancet. 2013;382(9908):1898–1955. doi:10.1016/S0140-6736(13)62105-4
39. Gimeno D, Amick BC, Barrientos-Gutiérrez T, Mangione TW. Work organization and drinking: an epidemiological comparison of two psychosocial work exposure models. Int Arch Occup Environ Health. 2009;82(3):305. doi:10.1007/s00420-008-0335-z
40. Heikkilä K, Nyberg ST, Fransson EI, et al. Job strain and alcohol intake: a collaborative meta-analysis of individual-participant data from 140 000 men and women. PLoS One. 2012;7(7):e40101. doi:10.1371/journal.pone.0040101
41. Kouvonen A, Kivimäki M, Cox SJ, Poikolainen K, Cox T, Vahtera J. Job strain, effort–reward imbalance, and heavy drinking: a study in 40,851 employees. J Occup Environ Health. 2005;47(5):503–513. doi:10.1097/01.jom.0000161734.81375.25
42. Heikkilä K, Nyberg ST, Fransson EI, et al. Job strain and tobacco smoking: an individual-participant data meta-analysis of 166 130 adults in 15 European studies. PLoS One. 2012;7(7):e35463. doi:10.1371/journal.pone.0035463
43. Kouvonen A, Kivimäki M, Virtanen M, Pentti J, Vahtera J. Work stress, smoking status, and smoking intensity: an observational study of 46 190 employees. J Epidemiol Community Health. 2005;59(1):63–69. doi:10.1136/jech.2004.019752
44. Do HN, Nguyen AT, Nguyen HQT, et al. Depressive symptoms, suicidal ideation, and mental health service use of industrial workers: evidence from Vietnam. Int J Environ Res Public Health. 2020;17(8):2929. doi:10.3390/ijerph17082929
45. Artz B, Green CP, Heywood JS. Does performance pay increase alcohol and drug use? J Popul Econ. 2020:1–34.
46. Moreau M, Valente F, Mak R, et al. Occupational stress and incidence of sick leave in the Belgian workforce: the Belstress study. J Epidemiol Community Health. 2004;58(6):507–516. doi:10.1136/jech.2003.007518
47. Lambert EG, Minor KI, Wells JB, Hogan NL. Social support’s relationship to correctional staff job stress, job involvement, job satisfaction, and organizational commitment. Soc Sci J. 2016;53(1):22–32. doi:10.1016/j.soscij.2015.10.001
48. Alsubaie MM, Stain HJ, Webster LAD, Wadman R. The role of sources of social support on depression and quality of life for university students. Int J Adolesc Youth. 2019;24(4):484–496. doi:10.1080/02673843.2019.1568887
49. Wang J, Mann F, Lloyd-Evans B, Ma R, Johnson S. Associations between loneliness and perceived social support and outcomes of mental health problems: a systematic review. BMC Psychiatry. 2018;18(1):1–16. doi:10.1186/s12888-018-1736-5
50. Ren P, Qin X, Zhang Y, Zhang R. Is social support a cause or consequence of depression? A longitudinal study of adolescents. Front Psychol. 2018;9. doi:10.3389/fpsyg.2018.01634
51. Ahasan R, Mohiuddin G, Khaleque A. Psychosocial Implications of Shift Work: A Case Study. Work Study. 2002;51(3):116–20. doi:10.1108/00438020210424244
52. Srivastava UR. Shift work related to stress, health and mood states: a study of dairy workers. J Health Manag. 2010;12(2):173–200. doi:10.1177/097206341001200205
53. Ma CC, Andrew ME, Fekedulegn D, et al. Shift work and occupational stress in police officers. Saf Health Work. 2015;6(1):25–29. doi:10.1016/j.shaw.2014.10.001
54. Lin PC, Chen CH, Pan SM, et al. The association between rotating shift work and increased occupational stress in nurses. J Occup Health. 2015;57(4):307–315. doi:10.1539/joh.13-0284-OA
55. Agyemang CB, Nyanyofio JG, Gyamfi GD. Job stress, sector of work, and shift-work pattern as correlates of worker health and safety: a study of a manufacturing company in Ghana. Int J Bus Manag. 2014;9(7):59. doi:10.5539/ijbm.v9n7p59
56. Sharma KS, Srivastava SP, Panchal PA, Kaur AM. The effect of shift work on lifestyle, mental health and physical health status of footwear factory workers: a comparison between night shifts and day shifts. Website: www ijpot com. 2017;11(4):434
57. James SM, Honn KA, Gaddameedhi S, Van Dongen HP. Shift work: disrupted circadian rhythms and sleep—implications for health and well-being. Curr Sleep Med Rep. 2017;3(2):104–112. doi:10.1007/s40675-017-0071-6
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.