")
Back to Journals » Risk Management and Healthcare Policy » Volume 15
Work Motivation of Primary Health Workers in China: The Translation of a Measurement Scale and Its Correlation with Turnover Intention
Authors Li H, Yuan B, Yu Y, Li J, Meng Q
Received 14 March 2022
Accepted for publication 29 June 2022
Published 17 July 2022 Volume 2022:15 Pages 1369—1381
DOI https://doi.org/10.2147/RMHP.S366389
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Huiwen Li,1 Beibei Yuan,2 Yahang Yu,3 Jia Li,4 Qingyue Meng2
1China Population and Development Research Center, Beijing, People’s Republic of China; 2China Center for Health Development Studies, Peking University, Beijing, People’s Republic of China; 3School of Public Health, Peking University, Beijing, People’s Republic of China; 4Department of Health Policy and Management, School of Public Health, Peking University, Beijing, People’s Republic of China
Correspondence: Beibei Yuan, China Center for Health Development Studies, Peking University, 38 Xuan Yuan Road, Haidian District, Beijing, 100191, People’s Republic of China, Tel +86 01 82805703, Fax +86 01 82805695, Email [email protected]
Background: High turnover intention, as a manifestation of low work motivation, is a crucial barrier to strengthening primary health systems worldwide, including in China. Targeting those being less motivated will be a realistic choice to retain primary health workers. This study translate, adapt, and validate the Work Motivation Scale for Health Workers (WMSHW) scale to directly measure and rate health workers’ motivation composition based on Self-Determination Theory, and assessed how health workers with different levels of motivation being associated with the turnover intention.
Methods: The process of translation and cross-cultural adaptation followed the recommendations of international guidelines. Participants include 1341 health workers within 75 primary health institutions from 6 provinces in China. The reliability and validity of the scale was analyzed. Cluster analysis in a person-centered approach and logistic regression analysis was used to understand how different combinations of motivations related to intention to leave.
Results: Confirmatory factor analysis indicated that the modified five-factor model had a better fit than the other models in accordance with the original English version. The factor loads were high and ranged from 0.70 to 0.9. Cronbach’s alpha coefficients for five dimensions of the Chinese WMSHW ranged from 0.81 to 0.94, indicating the scale’s high internal consistency. Four distinct clusters of work motivation were found in this study, representing low motivated, highly controlled, highly autonomous and highly motivated primary health workers. Compared with low motivation group, both controlled and autonomous motivation groups were more likely to have lower turnover intention. The negative relationship between motivation and intention to leave became stronger with the level of motivation increasing: highly controlled cluster (OR: 0.47; 95% CI: 0.35– 0.63), highly autonomous (OR: 0.27; 95% CI: 0.18– 0.41) and highly motivated (OR: 0.20; 95% CI: 0.15– 0.27).
Conclusion: The Chinese version of WMSHW showed satisfactory reliability and validity and can be used as an instrument for measuring and rating the work motivation of Chinese health workers. The primary health workers were grouped into four motivation levels based on this scale. Both controlled and autonomous motivation could work in reduce the turnover intention, and the influence of autonomous motivation on retaining was stronger.
Keywords: work motivation, health worker, self-determination theory, validation, turnover intention
Introduction
The availability of motivated health human resources is critical for the health system to high-quality health care.1 Just as a common problem worldwide, the low performance of primary health system has been recognized as the bottleneck problem in improving the overall health system performance in China.
Work motivation is defined as the drivers of workers for choice of action and persistence in doing it.2 The drivers working with environmental factors determined a psychological process that energizes, directs and sustains work behaviors,3,4 and “be motivated” manifests as a status “the willingness to exert efforts at work towards certain goals”.5 In health sector researches, it is widely accepted that the health workers’ motivation was significantly related to the choice of work behaviours, including whether to retain in existing position and whether to perform as the desire of managers or supervisors.6–8 In China’s primary health system, attraction and retaining of primary health workers (PHWs) is always a challenge, and turnover intention of PHWs is higher than that in hospital health workers.9 One systematic review showed that the pooled prevalence of turnover intention was 30.4%,10 and the Health Workers Survey under the Sixth National Health Service Survey in 2018 showed that 55.3% of the investigated primary health workers have a middle or higher level of intention to leave.9 Turnover intention is one predictor of turnover behaviour so it was reported that the mobility of health workers in primary health institutions (PHIs) is high and those leaving PHIs are more likely to be those with higher professional title level and longer working experience.11
Health workers’ willingness to stay is the basis for better performance. Studying the relationship between intention to leave and its predictor - motivation, will be closely relevant to health policy makers and managers of PHIs to take more targeted interventions to retain health workers. There have been some studies exploring the relationship between determinants of motivation and the attrition or retention of health workers in different countries,6,12,13 and from investigations in rural and urban PHIs in China, these factors included income and payment methods, learning and training opportunities, promotion and personal development space.14 These findings can potentially help policy makers to provide relevant incentives for retaining PHWs. However, providing these incentive factors usually involves extra resources or system reforms, which may not be applicable.
An alternative is to transfer the focus of interventions from factors to individuals, to measure the individual motivation level and composition, and then to help with the design of incentive tailored to individuals.15,16 However, studies directly analyzing the relationship between health workers with different level of motivation and intention to leave are still lacking. The key reason is the lack of measurement tools for work motivation.17 Most of the existing measurements of motivation are to indirectly measure the external or internal influencing factors of motivation,18 or measure the affective or cognitive outcomes of motivation as a proxy, like job satisfaction.19,20 There are few tools to directly measure the drivers of work behavior. Based on the definition of motivation as a driver of behavior, some people may more likely be motivated by the enthusiasm and interest of the task, while others may more likely be motivated by external pressure and benefits. Different sources and levels of motivation may contribute to completely different outcomes.
This study aims to use a scale to measure motivation directly and assess relations between the PHWs with different motivation levels and intention to leave in China. This study will contribute to existing knowledge in two aspects. Firstly, a well-structured and psychometrically sound tool to measure the work motivation of Chinese health workers could help further studies on predictors and outcomes of motivation in Chinese health care settings. To our knowledge, there are no validated instruments in China to measure health motivation among health workers. Secondly, this study will find the relationship between different compositions of motivation and intention to leave of PHWs, which is of great value to policy makers in designing targeting strategies for health workers with different drivers.
Methods
Theoretical Basis
Self-Determination Theory (SDT) provides a way to measure motivation itself and distinguish different motivation compositions. This theory was first described by Edward Deci and Richard Ryan in the mid-1980s, who conceptualized motivation as a continuum of self-determination representing different motivation dimensions with regulatory styles.21,22 The first dimension of motivation, which is labelled as intrinsic motivation, mainly relates to pure enjoyment inherent in the activity itself. The second dimension of motivation is labelled as integrated regulation, which is driven by the congruence between one’s behavior and values, identity and needs. The third dimension of motivation is labelled as identified regulation, which is derived from a conscious valuing of goals and values. The fourth dimension of motivation is labelled as introjected regulation, in which behaviors are undertaken to attain ego involvement or to avoid guilt such as pride. The fifth dimension of motivation is labelled as external regulation, which occurs when behaviors are performed for external rewards or punishments.23
SDT has become the mainstream motivation theory in the fields of education and sports and other life domains accompanied by the booming of well-validated motivation scales development based on SDT.24–27 In terms of work domain, the first motivation scale —“L’ Inventaire des Motivations au Travail de Blais” (Blais Inventory of Work Motivation) based on SDT was developed in France.28 There has been a growing trend in the development and evaluation of work motivation measurement such as Work Extrinsic and Intrinsic Motivation Scale29 and Multidimensional Work Motivation Scale.30 Most recent studies focus on the whole employees, while less attention is paid to the occupational particularity of health workers. The Work Motivation Scale for Health Workers (WMSHW) is a 15-item multidimensional scale developed to measure work motivation composition, which has been explicitly designed for use in the medical context.31
Measurement of Motivation
Considering the specialty in healthcare contexts, WMSHW has been developed tailored for health workers and has previously been applied and tested in 1142 nurses from government health institutions.31 All respondents were asked to answer the guiding question: “Why are you motivated to work?”, to capture their underlying motivation composition for hardworking. The original version of the WMSHW is a 15-item inventory that covers and assesses five dimensions of work motivation: 3 pertaining to intrinsic motivation (eg “Because I enjoy doing what I do at work every day”); 1 to integrated regulation (eg “Because being a health worker is a fundamental part of who I am.”); 2 to identified regulation (eg “Because my work is extremely important for my patients.”), 2 to introjected regulations (eg “In order to feel good about me.”) and 7 external regulations (eg “Because my supervisor recognizes and appreciates me.” or “In order to earn money”). All items are rated on an 11-point Likert scale ranging from 0 (“No, I disagree completely”) to 10 (“Yes, I agree”). The five types of regulation represent different levels of motivation sources, which were distinguished by the extent to which they stem from contingencies outside the person (controlled motivation) or originate within the person (autonomous motivation).32
The WMSHW has only been available in the English language to date, there is a need to adapt and validate this tool within a Chinese-speaking population to investigate different compositions of work motivation of health workers.
Translation and cross-cultural adaptation were carried out following the previously published international common guidelines.33 To ensure an accurate translation process, the scale was translated in 4 steps: forward translation from English into Chinese, achieving consensus, back-translation into English, and pretesting on health workers. Firstly, two bilingual academics who are familiar with health human resource management translated the original English version into Chinese respectively. Secondly, the English and the Chinese versions were discussed by the expert committee to obtain an exact translation. Thirdly, two language specialists who were blinded to the original English version translated the Chinese version into English respectively. Then, a panel of experts experienced in pediatric nursing was then asked to compare and examine discrepancies between these two versions (original English and back-translated English versions) until a unified Back translation scale formed through consensus discussion. Lastly, the Chinese version of the WMSHW was finalized after being well-tested in a representative piloted group of forty health workers.
Measurement of Turnover Intention
The turnover intention of health workers was measured by the scale developed by Mobley et al34 and Cammannet et al35 and has been widely used in the National Health and Services Survey in China.36 This Turnover Intention Scale consisted of four items including thoughts of leaving the organization you served now; thoughts of leaving a career in the medical profession; the possibility of finding other jobs recently; and the possibility of looking for new jobs next year. All items are rated on a 6-point Likert scale ranging from 1 (“No, I disagree completely”) to 6 (“Yes, I agree”), with a higher score indicating stronger intention to leave. The total score of turnover intention was rated by adding the scores in all 4 items ranging from 4 to 24. Additionally, the internal consistency of the Turnover Intention Scale was tested using Cronbach’s alpha coefficient (α = 0.90).
Study Design and Participants
A cross-sectional study was conducted for data collection in six provinces throughout the eastern, central and western regions of mainland China between April and October 2019. A stratified cluster sampling method was applied in this study. Data were collected from 76 primary health institutions (47 in urban area and 28 in rural areas). All health workers present on the day of the investigation were invited to participate. Participation was informed that they were voluntary to participate in the study and their responses were anonymous questionnaires. The final sample was made up of 1341 health workers comprising 60.2% of health workers were selected from the eastern region, 9.9% from central and 29.9% from the western region of China, which was far more than the recommended sample size of at least 10 subjects per item of the scale. Informed consent from PHWs was obtained.
Statistical Analysis
Quantitative variables for scale description were expressed as item means, standard deviations (SDs), skewness, and kurtosis. The structural validity and internal consistency of the WMSHW Chinese version were carried out to assess the psychometric properties of the tool. Confirmatory factor analysis (CFA) with maximum likelihood was conducted to test how well the items adequately represented their intended dimensions of the work motivation. Goodness-of-fit indices were assessed using the chi-square (χ2), degrees of freedom (df), the comparative fit index (CFI), the root mean square error of approximation (RMSEA), standardized root mean square residual (SRMR), and Akaike information criterion (AIC). For the CFI indices, values close to or greater than 0.95 are taken to reflect a good fit to the data. RMSEA values of less than 0.08 indicate a satisfactory fit, with values ranging to 0.10 representing a mediocre fit.37 SRMR values of less than 0.08 indicate a good fit.38 Pearson correlation coefficients were referred to in order to explore intercorrelations among subscales. Internal consistency estimates for both total scale and subscales were evaluated using Cronbach’s alpha. An alpha value between 0.70 and 0.90 was considered good and values greater than 0.90 were considered excellent.39
Due to the scarcity of studies on the motivation level category of health workers, cluster analysis, an analytic tool of person-centered approach was applied to explore the motivation profiles of PHWs in China. In contrast to the variable-centered approach, this approach aimed to understand how a health worker standing on multiple motivations might be related to turnover intention, instead of how particular work motivations relate to turnover intention. We used logistic regression models to explore the influence of work motivation on turnover intention among primary health workers in China.
Statistical analysis was conducted using STATA 14.0 for Windows, while CFA was performed through Mplus software version 7.0.40 All two-tailed p values less than 0.05 are considered statistically significant.
Results
Description of Participants in This Study
The demographic and job characteristics of 1341 participants are presented in Table 1. Overall the participants were predominantly female (75.8%) and married (77.0%). The majority were between 35 to 39 years old (45.2%) and 30.2% were under 35 years old. Approximately 65% of them had a bachelor’s or higher degree and 58.8% held a junior technical title. The respondents included 343 (25.6%) doctors, 317 (23.6%) nurses, 339 (25.3%) public health workers and 342 (25.5%) other medical technicians. About 35.0%, 44.6%, and 20.4% PHWs experienced a low, moderate, and high level of turnover intention, respectively.
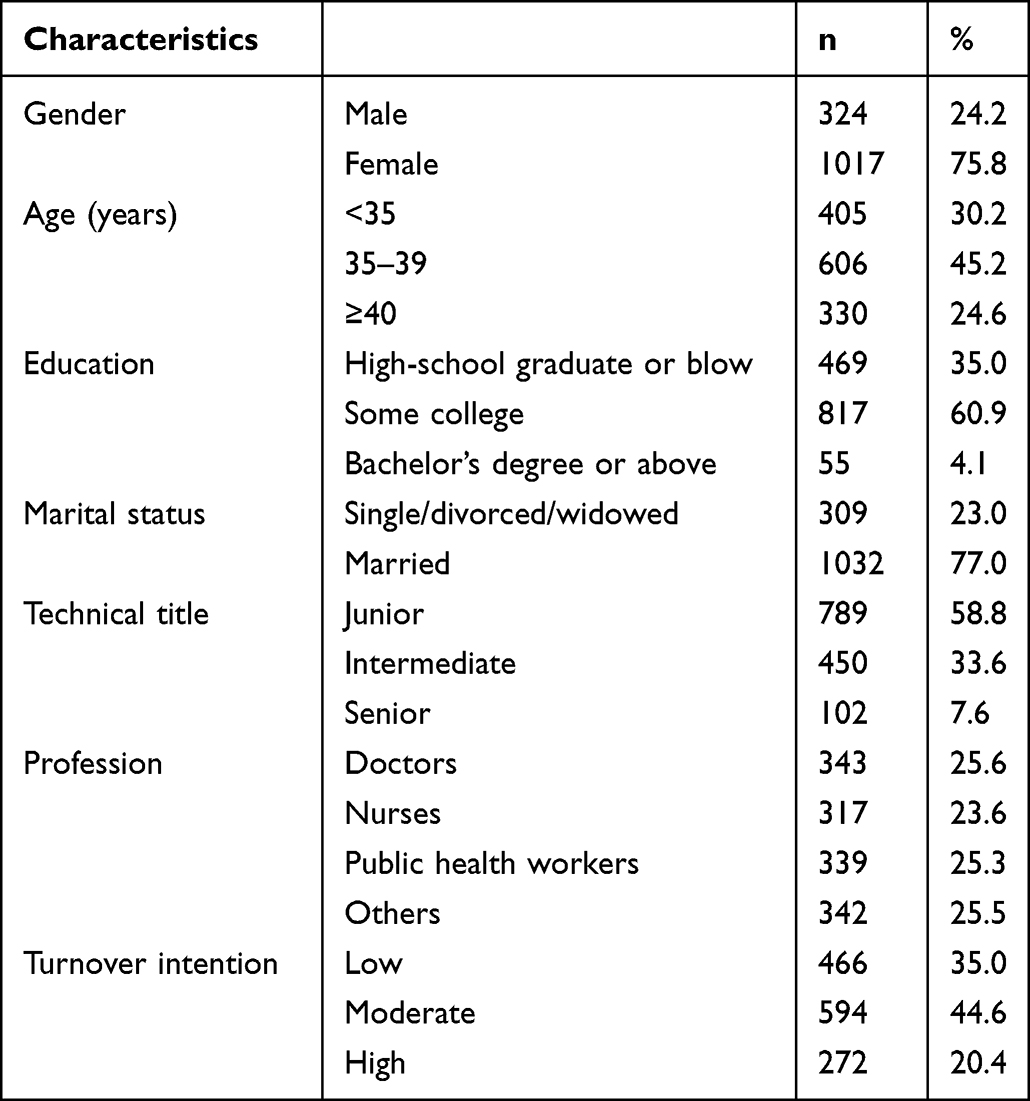 |
Table 1 Participant Characteristics |
Description of Scale Measuring Work Motivation
Table 2 presents the mean scores, SDs, skewness, kurtosis, and range of 15 scale items. All mean scores were above 5 (range=6.39 to 8.13). The highest mean score was found for items Ext6 (8.13±2.19) of external regulation-economic. However, all three items of intrinsic motivation (Im1-Im3) were found to be the lowest mean scores among 15 items. Skewness values ranged from −0.36 to −1.24, indicating that all items were negatively skewed. None of the items showed extremely leptokurtic distribution as the kurtosis values ranging from 2.37 to 4.13.
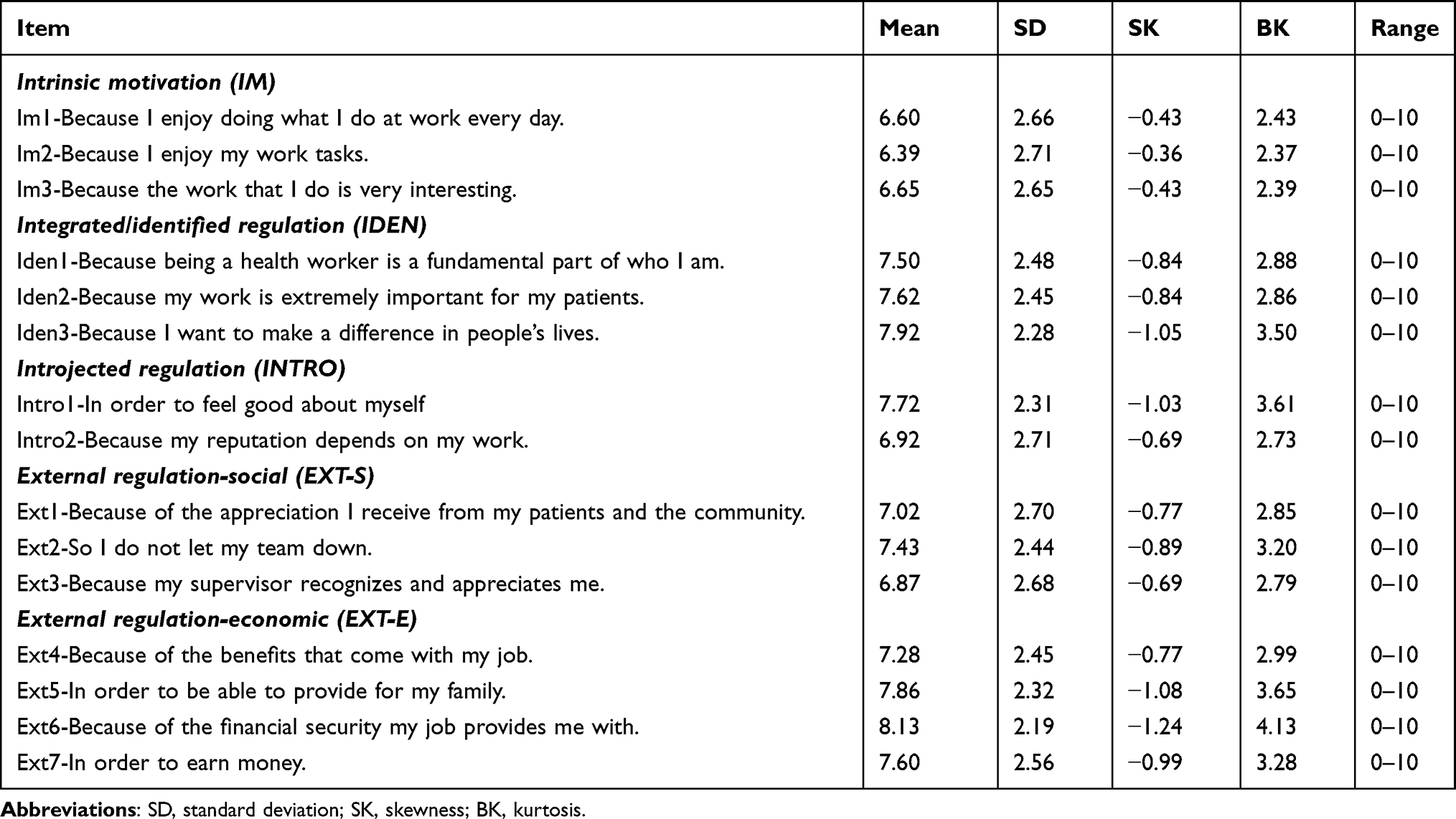 |
Table 2 Item Mean Scores, Standard Deviations, Ranges, Skewness, and Kurtosis |
Structural Validity of Scale Measuring Work Motivation
Five subscales including intrinsic motivation (IM), integrated regulation, identified regulation, introjected regulation (INTRO), and external regulation (EXT), are supposed to be included in the WMSHW, which correspond to the five motivation dimensions postulated by SDT. As there is only one integrated regulation item (Iden1), a four-factor model was created which combines the integrated and identified regulation dimensions as integrated/identified regulation (IDEN). In addition, two other alternative models were also tested for structural validation. The first alternative model dividing external regulation into a social and an economic sub-component consists of five factors. The second alternative model consists of two factors where autonomous motivation (AUT) was a combination of IM and IDEN and controlled motivation (CTRL) was a combination of INTRO and EXT.
CFA was conducted to assess how well the three hypothesized models represented the data using the maximum likelihood estimation method. The goodness-of-fit indices for the three models are present in Table 3. We found low goodness-of-fitness indices for both four-factor structure and two-factor structure, while the five-factor model yielded acceptable fit indices: χ2 (80) = 1015, p < 0.001, CFI = 0.94, RMSEA = 0.093, and SRMR = 0.059. The result revealed that five-factor model proposed by the original authors31 was accepted as the best-fitting model compared to the other two models.
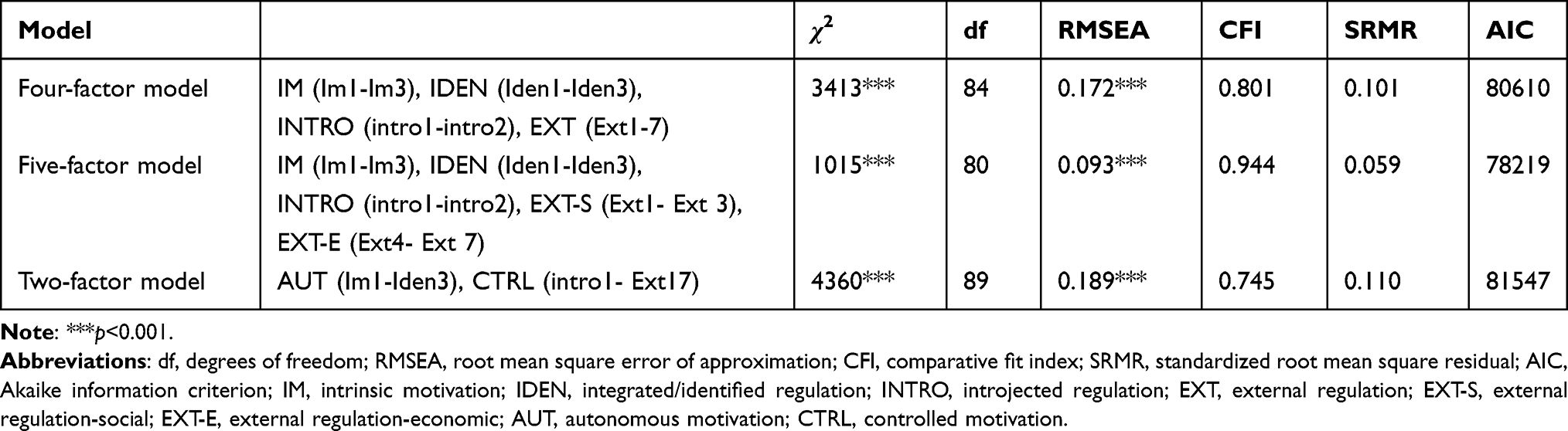 |
Table 3 Goodness-of-Fit Indices for Different Models |
As seen in Figure 1, all standardized factor loadings were over 0.5 and statistically significant, ranging from 0.69 to 0.94. The correlation among five factors ranged from 0.31 to 0.81, indicating that they are related, but measure different dimensions of work motivation. More specifically, the correlations between each subscale followed the theory hypothesized as the less nonadjacent subscales are less strongly positively related.
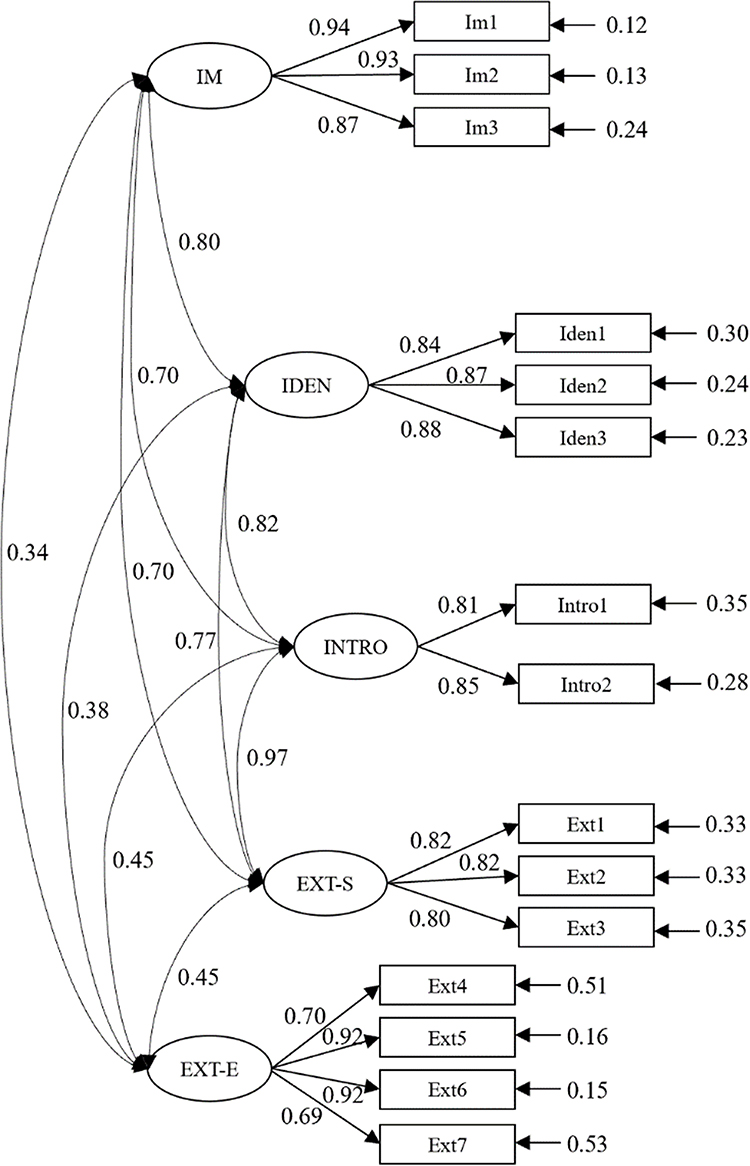 |
Figure 1 Standardized parameter estimates for five-factor model. Notes: Coefficients attached to arrows pointing at items from the right: residual variances (ie non-explained item variance, error terms); coefficients attached to arrows from factors to items: factor loadings; factor variances were fixed to 1 for model identification; coefficients attached to curved arrows represent factor correlations. |
Reliability of Scale Measuring Work Motivation
Cronbach’s alpha coefficients were 0.93 for the total scale, 0.94 for the IM subscale, 0.89 for the IDEN subscale, 0.81 for the INTRO subscale, 0.82 for the external regulation-social (EXT-S) subscale, and 0.88 for the external regulation-economic (EXT-E) subscale, showing that the Chinese version of the WMSHW demonstrated strong internal consistency.
The Correlation Between Work Motivation and Turnover Intention
We used cluster analysis to group PHWs based on the composition of regulation types. The result of cluster analysis was shown in Figure 2. To facilitate the naming of different groups, we grouped IM and IDEM as autonomous motivation, and group INTRO, EXT-S and EXT-E as controlled motivation. Participants in cluster 1 presented low levels on all dimensions of work motivation compared with other clusters, which could be described as “low motivated” workers. Participants in cluster 2 presented low levels of autonomous motivation and middle levels of controlled motivation, which could be described as “highly controlled” workers. Participants in cluster 3 presented middle levels of autonomous motivation and low levels of controlled motivation, which could be described as “highly autonomous” workers. Participants in cluster 4 presented high levels on all dimensions of work motivation, which could be described as “highly motivated” workers. Each cluster accounted for 19.6%, 32.2%, 10.1% and 38.1% of the PHWs respectively.
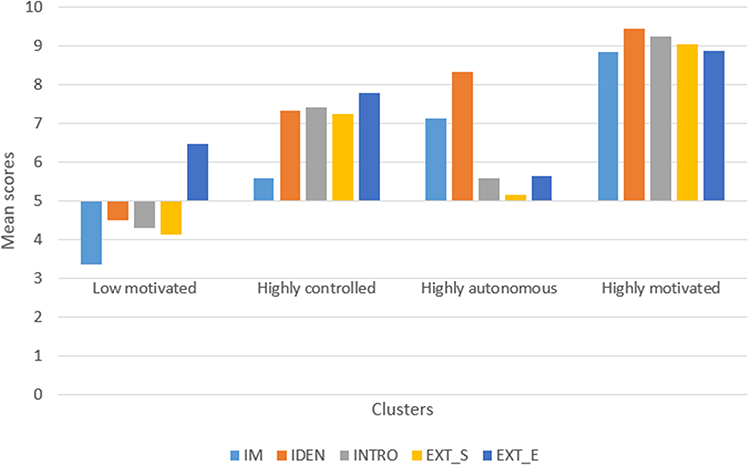 |
Figure 2 Mean scores of four cluster of motivation. Abbreviations: IM, intrinsic motivation; IDEN, integrated/identified regulation; INTRO, introjected regulation; EXT, external regulation; EXT-S, external regulation-social; EXT-E, external regulation-economic. |
In Table 4, the relationships between the work motivation and outcomes turnover intention were tested. It was found that was four distinct clusters of work motivation differently related to turnover intention. The highly autonomous (OR: 0.27; 95% CI: 0.18–0.41) and highly motivated (OR: 0.20; 95% CI: 0.15–0.27) clusters were strongly related to low level of turnover intention, while highly controlled cluster (OR: 0.47; 95% CI: 0.35–0.63) had less favorable levels of correlates.
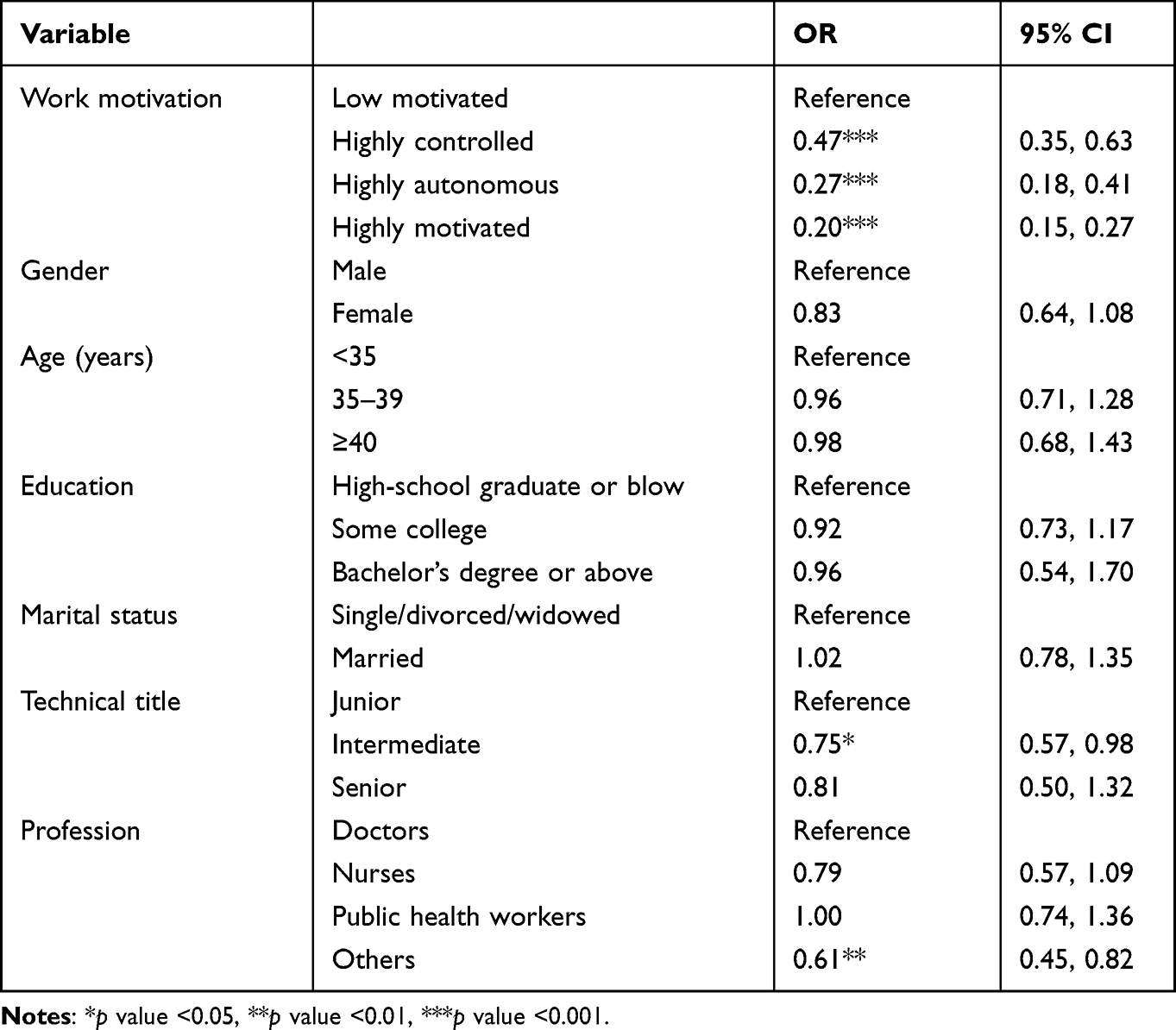 |
Table 4 Logistic Regression Between Work Motivation and Turnover Intention |
Discussion
In the present study, we sought to examine the correlation between the motivation of PHWs and their intention to leave, at the same time to examine the psychometric properties of a Chinese translation of the WMSHW. The current results provide supportive evidence regarding the cross-cultural reliability and validity of the inventory implying that WMSHW opens a new field of research in relation to work motivation of Chinese health workers by introducing a scale that measures motivation compositions and levels. The data show that the majority of PHWs investigated had a moderate level of motivation with controlled motivation dominantly existed, and 65% of PHWs were with moderate or high level of turnover intention. It is also found that higher autonomous motivation and those being highly motivated by all types of drivers are more likely to be with lower turnover intention.
This study is the first time to measure the work motivation of PHWs in China as the drivers of working hard and ensuring the validation of scale is the basis for further exploration of the correlation between motivation and intention to leave. The translated and cross-culturally adapted WMSHW demonstrated good structural validity and internal consistency among Chinese sample. We used the well-established translation and back-translation guidelines to assure equivalence in varied aspects between source and target versions. During the translation of the English WMSHW into Chinese, a minor cultural discrepancy was encountered and one item of the WMSHW has been modified accordingly: “supervisor” was replaced with “leader” as this word is closer to Chinese culture. Compared with previous studies that measure work motivation, this is the first study to confirm the structure of WMSHW with the population working at health institutions in China without sacrificing any item.
The result of CFA showed that the modified five-factor model had a better fit than the other models and was selected as the best-fitting model, which was consistent with the original scales. In line with a previous study testing the latent structure of work motivation based on SDT in seven languages,30 fit indices in the Chinese version demonstrated slightly lower than the original English version. Culture may have played a role in shaping the understanding of work motivation. Although values of RMSEA are barely within the scope of adequate model fit, our option was not to modify the model considering that the current results suggest that the five-factor model may be a theoretically adequate model for the data based on SDT. Therefore, the current results showed that a Chinese translation of the WMSHW demonstrates a five-dimensional factor structure representing IM, IDEN, INTRO, EXT-S, EXT-E as hypothesized. Specifically, the IDEN dimension combines integrated regulation and identified regulation which has proven difficult to separate in previous research.30,41
In line with previous studies,29,42 the correlation between the two factors was identified as moderate, indicating that they are related although they measure different compositions of work motivation. Furthermore, strong internal consistency of the Chinese WMSHW was demonstrated, as evidenced by all Cronbach’s alpha coefficients over 0.8. In the Chinese WMSHW, the Cronbach’s alpha for the total scale (0.94) was much higher than in the English (0.89) versions, and Cronbach’s alpha for the five subscales was also higher than in the English version (0.92).31
This study firstly used the WMSHW to measure and categorized PHWs into four types based on motivation composition. As explained by SDT, the self-determination continuum of motivation includes five major dimensions of drivers covering from controlled motivation to autonomous motivation. So we rated four types of groups as PHWs without any controlled or autonomous drivers for work (low motivation), PHWs with more external controlled drivers (controlled motivation), PHWs with more internal autonomous drivers (autonomous motivation), PHWs with strong drivers from both controlled and autonomous factors (highly motivated). Previous studies43,44 mainly used job satisfaction as a proxy to measured and categorized the motivation of PHWs. The boundaries between motivation and job satisfaction measurements are blurred in existing studies. The reasons include: firstly, the influencing factors of job satisfaction have a lot of overlap with determinants of motivation;17,45 secondly, job satisfaction is an effective consequence of motivation, and a status of harmony between drivers’ of health workers and organization environments;5 lastly, scales directly measuring motivation per se as the drivers of working hard are lacking. The measurement of job satisfaction cannot substitute the measurement of motivation. Compared with the category of being satisfied or dissatisfied, category-based WMSHW can identify complex compositions of drivers and diverse levels of motivation.
It was found that the health workers with low motivation, controlled motivation, autonomous motivation and highly motivated (higher scores on both autonomous and controlled drivers) took 19.6%, 32.2%, 10.1% and 38.1% of the total number of participants respectively. Based on the assumption of STD, human beings tend to make decisions by themselves and health workers with autonomous drivers, ie doing what they love and can make decisions for themselves, so those with the highest autonomous motivation are the most motivated compared with health workers with other drivers or those without drivers.7 So the four groups of health workers provide a possible method to order the motivation level from the lowest level (low motivation group) to the highest level (highly motivated group). We found that 38.1% of PHWs have the strongest driving forces from both external incentives and enjoyment of work, and this group had a relatively well motivation status. There were still 19.6% of PHWs in the investigated area being rated as low motivation, and 32.2% of PHWs being dominantly driven by controlled factors, like monetary incentives or avoidance of punishment. These two groups took more than half (51.5%) of investigated PHWs, so overall the motivation of PHWs still was at a moderate level. Existing studies on work motivation of health workers working in China PHIs all used job satisfaction17,46 or perception of health workers as determinants of motivation47 to assess the motivation status and all have the similar findings, ie 74% of PHWs were satisfied with present work.17 This study also found that only 10.1% of PHWs are dominantly driven by passion and enjoyment at work. For PHWs in China, a large number of studies have reported the low level of income level and poor work environment. Under this context the existing needs cannot be fully met, it is less likely for PHWs to have the pursuit for enjoyment of work tasks.48 The dominant role of existence need can also be reflected by the findings of this study: health workers mainly driven by controlled factors took 32.2% of investigated PHWs in this study; at the same time, in the driving forces of highly motivated participants (38.1%), the impetus of controlled factors was also as strong as the forces of autonomous factors; the sum of the above two groups means that the majority of participants are in the stage being driven by monetary rewards and other forms of material benefits.
The data analysis showed that compared with the “low motivation” group (those having no drivers to work hard), the groups with any type of motivation, including controlled, autonomous, both controlled and autonomous, were all more likely to have lower turnover intention. Though there are no studies that directly measure motivation for PHWs in China, previous studies using job satisfaction as a proxy to measure reported similar findings: lower satisfaction as an important indicator of low motivation, was correlated with higher turnover intention no matter in China and other LMICs.10,49,50
The negative relationship between motivation and intention to leave was found to become stronger with the level of motivation increasing: highly controlled cluster (OR: 0.47; 95% CI: 0.35–0.63), highly autonomous (OR: 0.27; 95% CI: 0.18–0.41) and highly motivated (OR: 0.20; 95% CI: 0.15–0.27). Autonomous motivation is more effective in reducing turnover intention compared with controlled motivation, and this result implies those PHWs with real interest or pure enjoyment in the activities related to primary health care have less intention to leave the existing work position. As agreed by SDT and other motivation theories, being motivated is a status of harmony between personnel goals and organization goals, so those PHWs with natural enthusiasm on their tasks are nearer to the status of harmony even under disadvantaged environments. Autonomous motivation can help health workers keep optimistic in work, and cope with the feelings of dissatisfaction, stress, and burnout. Though there are no similar studies on the relationship between different compositions of motivation and turnover intention of health workers, the studies in other industries have found that employees with the pursuit of individual development, interests and achievement were more likely to have positive feelings compared with those with financial benefits and prestige as major drivers.51,52
We also found that controlled motivation can work in reducing the extent of turnover intention compared with those without any driving forces. In this study, the PHWs in the “low motivation” group are those having the lowest score on any drivers of working hard, which means those people having no purposes or desires, thus they usually do not expect any achievements from their efforts or do not have confidence on the competency of themselves. The PHWs with no motivation usually perform as having no willingness to make efforts in work and responding passively to external environments. PHW workers with controlled motivation, though they are rated as the lower level of motivation in the STD continuum of motivation, their pursuit for the basic living substances can work to some extent in retaining them in the existing work position.
The present study has several limitations that should be noted. First, the Chinese WMSHW has been tested only among health workers working at primary health care facilities, so further psychometric testing in secondary-level and third-level hospitals and other health settings would contribute to reject or confirm the generalizability of the instrument. Secondly, although our study translated and adapted the English-language scale into the Chinese language using standard procedures, the cultural differences between Western countries and China may limit the ability to measure work motivation in Chinese cultural contexts. Thirdly, because limited studies assessing the motivation level directly are published for us to compare, our findings on categories of PHWs based on motivation level, and the relationship between motivation and turnover intention are mainly discussed based on motivation theories.
Conclusion
In general, cross-cultural translation was completed, and the Chinese version of WMSHW showed good reliability and validity. The self-determinant perspective provided insights into a broader set of measure work motivation composition that are associated with work behavior. Specifically for turnover intention, we found that both controlled and autonomous motivation can work in reducing turnover intention, and the influence of autonomous motivation on retention was stronger. To retaining PHWs, the interventions should be tailored to different workers with varied motivation compositions, those measures inspiring the interests and enthusiasm of primary health workers may have stronger effects.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author, Beibei Yuan, upon reasonable request.
Ethics Approval and Consent to Participate
The study has been approved by the Ethics Review Board of the School of Public Health, Peking University (code of ethics: PKU201412128). Informed consent was obtained from all participants prior to questionnaire administration.
Acknowledgments
The authors would like to thank Feng Yan and her research team from Fudan University for their assistance in data collection.
Funding
This research was supported by Beijing Natural Science Foundation (No. 9202007).
Disclosure
The authors declared no potential conflicts of interest.
References
1. Pinder CC. Work Motivation in Organizational Behavior. NJ: Prentice-Hall; 1998.
2. Erickson JI, Duffy ME, Gibbons MP, Fitzmaurice J, Jones D. Development and psychometric evaluation of the Professional Practice Environment (PPE) scale. J Nurs Scholarship. 2010;36(3):279–285. doi:10.1111/j.1547-5069.2004.04050.x
3. Kanfer R. Measuring Health Worker Motivation in Developing Countries. Bethesda Maryland: Abt Associates Partnerships for Health Reform; 1999.
4. Mathauer I, Imhoff I. Health worker motivation in Africa: the role of non-financial incentives and human resource management tools. Hum Resour Health. 2006;4(1):24. doi:10.1186/1478-4491-4-24
5. Dolea C, Adams O. Motivation of health care workers-review of theories and empirical evidence. Cah Sociol Demogr Med. 2005;45(1):135–161.
6. Bonenberger M, Aikins M, Akweongo P, Wyss K. The effects of health worker motivation and job satisfaction on turnover intention in Ghana: a cross-sectional study. Hum Resour Health. 2014;12:43. doi:10.1186/1478-4491-12-43
7. Deci EL, Olafsen AH, Ryan RM. Self-determination theory in work organizations: the state of a science. Annu Rev Organ Psychol Organ Behav. 2017;4:19–43. doi:10.1146/annurev-orgpsych-032516-113108
8. Alhassan RK, Spieker N, van Ostenberg P, Ogink A, Nketiah-Amponsah E, de Wit TF. Association between health worker motivation and healthcare quality efforts in Ghana. Hum Resour Health. 2013;11:37. doi:10.1186/1478-4491-11-37
9. Center for Health Statistics and Information. Special Report on the Sixth National Health Service Survey (Second Series). Beijing: Peking Union Medical College Press; 2021.
10. Rongxin H, Liu J, Zhang WH, Zhu B, Mao Y. Turnover intention among primary health workers in China: a systematic review and meta-analysis. BMJ Open. 2020;10:37117.
11. Meng Q, Yuan J, Jing L, Zhang J. Mobility of primary health care workers in China. Hum Resour Health. 2009;7(1):24. doi:10.1186/1478-4491-7-24
12. Blaauw D, Ditlopo P, Maseko F, et al. Comparing the job satisfaction and intention to leave of different categories of health workers in Tanzania, Malawi, and South Africa. Glob Health Action. 2013;6:19287.
13. Fogarty L, Kim YM, Juon HS, Tappis H, Rozario A. Job satisfaction and retention of health-care providers in Afghanistan and Malawi. Hum Resour Health. 2014;12(1):11. doi:10.1186/1478-4491-12-11
14. Wen T, Zhang Y, Wang X, Tang G. Factors influencing turnover intention among primary care doctors: a cross-sectional study in Chongqing, China. Hum Resour Health. 2018;16(1):10. doi:10.1186/s12960-018-0274-z
15. Graves LM, Cullen KL, Lester HF, Ruderman MN, Gentry WA. Managerial motivational profiles: composition, antecedents, and consequences. J Vocat Behav. 2015;87:32–42. doi:10.1016/j.jvb.2014.12.002
16. Howard J, Gagne M, Morin A, Anja V. Motivation profiles at work: a self-determination theory approach. J Vocat Behav. 2016;95–96:74–89. doi:10.1016/j.jvb.2016.07.004
17. Li H, Yuan B, Wang D, Meng Q. Motivating factors on performance of primary care workers in China: a systematic review and meta-analysis. BMJ Open. 2019;9(11):e028619.
18. Bennett S, Franco LM, Kanfer R, Stubblebine P. The development of tools to measure the determinants and consequences of health worker motivation in developing countries. Major Appl Res Tech Paper. 2001;4:63.
19. Mbindyo PM, Blaauw D, Gilson L, English M. Developing a tool to measure health worker motivation in district hospitals in Kenya. Hum Resour Health. 2009;7(1):40. doi:10.1186/1478-4491-7-40
20. Mutale W, Ayles H, Bond V. Measuring health workers’ motivation in rural health facilities: baseline results from three study districts in Zambia. Hum Resour Health. 2013;11(1):8. doi:10.1186/1478-4491-11-8
21. Deci EL, Ryan RM. Intrinsic Motivation and Self-Determination in Human Behavior. US: Springer; 1985.
22. Gagne M, Deci EL. Self-determination theory and work motivation. J Organ Behav. 2005;26(4):331–362. doi:10.1002/job.322
23. Ryan RM, Deci EL. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am Psychol. 2000;55(1):68–78. doi:10.1037/0003-066X.55.1.68
24. Grolnick WS, Ryan RM. Autonomy in childrens learning - an experimental and individual difference investigation. J Pers Soc Psychol. 1987;52(5):890–898. doi:10.1037/0022-3514.52.5.890
25. Guay F, Vallerand RJ, Blanchard C. On the assessment of situational intrinsic and extrinsic motivation: the Situational Motivation Scale (SIMS). Motiv Emotion. 2000;24(3):175–213. doi:10.1023/A:1005614228250
26. Pelletier LG, Tuson KM, Fortier MS, Vallerand RJ, Briere NM, Blais MR. Toward a new measure of intrinsic motivation, extrinsic motivation, and amotivation in sports: the Sport Motivation Scale (SMS). J Sport Exercise Psy. 1995;17(1):35–53. doi:10.1123/jsep.17.1.35
27. Vallerand RJ, Pellerier LG, Blais MR, Briere NM, Senecal C, Vallieres EF. The academic motivation scale: a measure of intrinsic, extrinsic, and amotivation in education[J]. Educ Psychol Meas. 1992;52(4):1003–1017. doi:10.1177/0013164492052004025
28. Blais MR, Brière NM, Lachance L, Riddle AS, Al E. L’inventaire des motivations au travail de Blais [The Blais Inventory of Work Motivation]. Revue québécoise de psychologie. 1993;14:185–215.
29. Tremblay MA, Blanchard CM, Villeneuve M, Taylor S, Pelletier LG. Work extrinsic and intrinsic motivation scale: its value for organizational psychology research. Can J Behav Sci. 2009;41(4):213–226. doi:10.1037/a0015167
30. Gagne M, Forest J, Vansteenkiste M, et al. The multidimensional work motivation scale: validation evidence in seven languages and nine countries. Eur J Work Organ Psy. 2015;24(2):178–196. doi:10.1080/1359432X.2013.877892
31. Lohmann J, Souares A, Tiendrebeogo J, et al. Measuring health workers’ motivation composition: validation of a scale based on Self-Determination Theory in Burkina Faso. Hum Resour Health. 2017;15(1):33. doi:10.1186/s12960-017-0208-1
32. Deci EL, Ryan RM. The “What” and “Why” of goal pursuits: human needs and the self-determination of behavior: psychological inquiry. Psychol Inq. 2000;11(4):227–268. doi:10.1207/S15327965PLI1104_01
33. Brislin RW. Comparative research methodology: cross-cultural studies. Int J Psychol. 1976;11(3):215–229. doi:10.1080/00207597608247359
34. Mobley WH. Intermediate linkages in the relationship between job satisfaction and employee turnover. J Appl Psychol. 1977;62(2):237–240. doi:10.1037/0021-9010.62.2.237
35. Cammann C, Fichman M, Jenkins D, Klesh JR. The michigan organizational assessment questionnaire. In: Assessing Organizational Change a Guide to Methods Measures & Practices. University of Michigan; 1983.
36. Center for Health Statistics and Information. Research on Relationship Between YI and HUAN in China, 2008.
37. Hoyle RH. The Structural Equation Modeling Approach: Basic Concepts and Fundamental Issues. Sage Publications; 1995.
38. Hu LT, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Model. 1999;6(1):1–55. doi:10.1080/10705519909540118
39. Terwee CB, Bot SD, de Boer MR. Quality criteria were proposed for measurement properties of health status questionnaires. J Clin Epidemiol. 2007;60:34–42.
40. Muthén L, Muthén B, Muthén LK, et al. Mplus User’s Guide. Los Angeles: Muthén & Muthén; 1998.
41. Gagne M, Forest J, Gilbert M, Aube C, Morin E, Malorni A. The motivation at work scale: validation evidence in two languages. Educ Psychol Meas. 2010;70(4):628–646. doi:10.1177/0013164409355698
42. Moran CM, Diefendorff JM, Kim TY, Liu ZQ. A profile approach to self-determination theory motivations at work. J Vocat Behav. 2012;81(3):354–363. doi:10.1016/j.jvb.2012.09.002
43. Kudo Y, Satoh T, Hosoi K, et al. Association between intention to stay on the job and job satisfaction among Japanese nurses in small and medium-sized private hospitals. J Occup Health. 2006;48(6):504–513.
44. Dieleman M, Cuong PV, Le VA, Martineau T. Identifying factors for job motivation of rural health workers in North Viet Nam. Hum Resour Health. 2003;1(1):10. doi:10.1186/1478-4491-1-10
45. Peters DH, Chakraborty S, Mahapatra P, Steinhardt L. Job satisfaction and motivation of health workers in public and private sectors: cross-sectional analysis from two Indian states. Hum Resour Health. 2010;8(1):1–11. doi:10.1186/1478-4491-8-27
46. Hung L-M, Shi L, Wang H, Nie X, Meng Q. Chinese primary care providers and motivating factors on performance. Fam Pract. 2013;30(5):576–586. doi:10.1093/fampra/cmt026
47. Wang H, Shi L, Meng Q. Comparatively studying the job incentive factors for urban and rural grass-roots health professionals. Chinese Health Serv Manage. 2013;30(011):863–865.
48. Maslow AH. A theory of human motivation. Psychol Rev. 1943;50:370–396. doi:10.1037/h0054346
49. Wang H, Jin Y, Wang D, Zhao S, Yuan B. Job satisfaction, burnout, and turnover intention among primary care providers in rural China: results from structural equation modeling. BMC Fam Pract. 2020;21(1). doi:10.1186/s12875-020-1083-8
50. Shen X, Jiang H, Xu H, Ye J, Gan Y. The global prevalence of turnover intention among general practitioners: a systematic review and meta-analysis. BMC Fam Pract. 2020;21(1). doi:10.1186/s12875-020-01309-4
51. Deci EL, Connell JP, Ryan RM. Self-determination in a work organization. J Appl Psychol. 1989;74(4):580–590. doi:10.1037/0021-9010.74.4.580
52. Vansteenkiste M, Neyrinck B, Niemiec CP, Soenens B, Witte HD, Broeck A. On the relations among work value orientations, psychological need satisfaction and job outcomes: a self-determination theory approach. J Occup Organ Psychol. 2011;80:251–277.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.