")
Back to Journals » International Journal of Women's Health » Volume 6
Women’s perception of accuracy of ultrasound dating in late pregnancy: a challenge to prevention of prolonged pregnancy in a resource-poor Nigerian setting
Authors Ugwu EO , Odoh G, Dim C, Obi S, Ezugwu E, Okafor I
Received 21 October 2013
Accepted for publication 17 December 2013
Published 10 February 2014 Volume 2014:6 Pages 195—200
DOI https://doi.org/10.2147/IJWH.S56321
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Emmanuel O Ugwu,1 Godwin U Odoh,1 Cyril C Dim,1 Samuel N Obi,1 Euzebus C Ezugwu,1 Innocent I Okafor2
1Department of Obstetrics and Gynaecology, University of Nigeria Teaching Hospital, Ituku/Ozalla, Enugu, Nigeria; 2Department of Obstetrics and Gynaecology, Enugu State University Teaching Hospital, Parklane, Enugu, Nigeria
Background: Expected date of delivery (EDD) is estimated from the last menstrual period (LMP) or ultrasound scan. Conflicts between these estimates especially on the part of the physician and his/her patient could pose a challenge to prevention of prolonged pregnancy. The objective of this study was to determine the perception and acceptability of menstrual dating (EDD derived from LMP) with regard to timing of labor induction for postdatism by pregnant women who have a late pregnancy (≥23 weeks’ gestation) ultrasound scan.
Methods: This cross-sectional study included 443 consecutive pregnant women receiving antenatal care at two tertiary health institutions in Enugu, Nigeria, from January 1, 2013 to March 31, 2013.
Results: The mean age of the women was 27.9±2.41 (range 17–45) years. Most ultrasound scans (90.8%, 357/389) were carried out in late pregnancy, and 41.9% (167/389) were self-referred. The majority of the respondents (51.7%, 229/443) did not accept induction of labor for postdatism at a certain menstrual dating-derived gestational age of 40 weeks plus 10 days if the late pregnancy ultrasound scan dating was less. Predictors of this poor attitude to timing of induction of labor for postdatism included low educational level, low social class, and poor knowledge of the limitations of ultrasound scan dating in late pregnancy (P<0.05).
Conclusion: The worrisome confidence in ultrasound scan dating is a challenge to the prevention of prolonged pregnancy and its complications in our environment. Antenatal health education should discourage self-referral for ultrasound scan dating and emphasize its limitations in late pregnancy as well as the perinatal effects of prolonged pregnancy.
Keywords: ultrasound dating, prolonged pregnancy, Nigeria
Introduction
Knowledge of the expected date of delivery (EDD) and gestational age is essential in the management of pregnant women. Both are important for optimal prenatal, intrapartum, and postnatal care. For instance, reliable information about gestational age and EDD is useful in assessment of fetal growth during the antenatal period.1,2 Two independently derived estimates are often used in the determination of the delivery date, ie, calculation based on the last menstrual period (LMP) and a prediction from obstetric ultrasound scan.
In clinical practice, the gestational age and EDD are often determined using the LMP, except when the discrepancy between the LMP-derived gestational age or EDD and that of early pregnancy ultrasound scan exceeds 1 week; in this situation, the ultrasound scan estimates are more reliable and should be used.3,4 A valid date of delivery can only be estimated from the first day of the LMP if the menstrual date is definite and accurate. However, the unreliability of this method has been demonstrated by various authors,2,5 who observed that 10%–45% of women did not have a reliable date for their LMP as a result of an irregular menstrual cycle, use of oral contraceptive pills, or bleeding during pregnancy. Further, the rate of post-term pregnancy has been shown to decrease when early ultrasound scan is used in estimating the gestational age and EDD.5 Therefore, ultrasound scan is considered the gold standard for estimation of gestational age and EDD when carried out in the first half of pregnancy.2,6 This is because the biological variations in biometric measurements of the fetus with respect to fetal size and effects of growth restriction are still minimal at these early gestational ages.2 In view of this proven accuracy, a first trimester or an early second trimester (15–22 weeks) ultrasound scan is an essential part of routine antenatal care in many high-resourced countries so as to establish a reliable gestational age and EDD.2 Nevertheless, the accuracy of ultrasound scan in estimating the EDD during the late second trimester/third trimester is low, and hence EDD derived from a certain LMP is generally preferred in this period.2
The error margin of EDD estimated by ultrasound scan increases as the pregnancy advances, reaching up to ±3 weeks in the third trimester.7,8 It has been observed that, despite this high error margin, pregnant Nigerian women often make their birth plans based on the ultrasound EDD irrespective of the gestational age at estimation, and regardless of the LMP-derived EDD. The uncontrolled proliferation of ultrasound in Nigeria has further heightened the conflict between these two estimates of delivery date because pregnant women are increasingly having access to ultrasound scanning manned by various cadres of health workers, without information on its known limitations. This scenario is a big challenge in terms of prevention of prolonged pregnancy in our environment where women register late for antenatal care9 and rarely have reliable early ultrasound scan results. A scenario is often created where the attending medical practitioner feels the pregnancy is prolonged based on a certain LMP-derived EDD while the client holds a different view based on her ultrasound scan-derived EDD, and therefore refuses to accept induction of labor despite counseling. The aim of this study was to determine the perception and acceptability of menstrual dating (EDD derived from LMP) for timing of labor induction for postdatism by pregnant women who have a late pregnancy ultrasound scan.
Materials and methods
Study area
Enugu State is one of the five states in the southeast geopolitical zone of Nigeria, and its capital city is Enugu. It lies within the West African rainforest region (latitude 5°55′ and 7°10′ North and longitude 6°50′ and 7°55′ East), with a land area of approximately 8,727.1 km2. It has an average annual temperature of 23.1°C–31°C and a rainfall of 1,520–2,030 mm. The state covers a land area of approximately 8,727.1 km2. It has a mixed rural and urban population of about 464,514 inhabitants, with the majority being Igbo and 52% being female.
The University of Nigeria Teaching Hospital, Ituku-Ozalla, Enugu, is owned by the federal government of Nigeria and located on the outskirts of Enugu City. The Enugu State University Teaching Hospital, Parklane, is a state-owned teaching hospital located in the center of the Enugu metropolis. Both centers provide antenatal and postnatal care services to pregnant women in Enugu State. Further details of the study area/centers are described in a recent study published elsewhere.10 The protocols of both these tertiary health centers recommend routine induction of labor at a gestational age of 40 weeks plus 10 days for eligible postdate pregnancies to minimize the risks of prolonged pregnancy, which include placental insufficiency, fetal oligohydramnios, intrauterine fetal death, macrosomia, increased cesarean and instrumental deliveries, and birth injuries, as well as birth asphyxia, neonatal jaundice, and perinatal death. The commonest indication for induction of labor in the two hospitals (and in our environment) is prolonged pregnancy.11 Other common indications include hypertensive disorders in pregnancy, intrauterine growth restriction, and diabetes mellitus in pregnancy.11
Study design and sample selection
This was a cross-sectional study of consecutive pregnant women attending for antenatal care at the antenatal clinics of the University of Nigeria Teaching Hospital, Ituku-Ozalla, Enugu, and the Enugu State University Teaching Hospital, Parklane, from January 1, 2013 to March 31, 2013. Every singleton pregnant woman due for a routine delivery planning discussion at a gestational age of 36 weeks and beyond was eligible for the study. Exclusion criteria included uncertainty of date, presence of contraindications to vaginal delivery, irregular menstrual cycle prepregnancy, use of hormonal contraceptives prior to pregnancy, or bleeding during pregnancy.
After individual counseling of eligible participants, pretested structured questionnaires were administered to consecutive consenting women by trained medical interns. Ethical clearance for the study was obtained from the institutional review board of the University of Nigeria Teaching Hospital, Enugu. Data collected included the sociodemographic characteristics of the respondents (age, marital status, tribe, level of education, occupation, parity), opinions and preferences regarding LMP and ultrasound scan dates, and their attitudes toward postdatism and induction of labor in relation to estimated dates. The primary outcome measure was willingness to accept induction of labor at an LMP-derived gestational age of 40 weeks plus 10 days (when late pregnancy ultrasound scan-derived gestational age was less than 40 weeks plus 10 days).
The first trimester was defined as a gestational age of 1–13 weeks, the second trimester as 14–27 weeks, and the third trimester as 28–42 weeks. Further, the early second trimester was defined as a gestational age of 15–22 weeks and the late second trimester as 23–27 weeks.7 For the purpose of this study, pregnancy was deemed to be prolonged if it had exceeded 40 weeks plus 10 days.11
As described in a previous study,12 the social class of the respondents was defined using a scoring system based on the educational level of the woman and her husband’s occupation or that of the caregiver (for unmarried women). Thus, high social class was defined as belonging to class I or II while low social class was defined as belonging to class III, IV, or V.
Respondents who were aware that LMP-estimated EDD was more accurate than ultrasound scan-estimated EDD in the late second trimester/third trimester were deemed to have “good knowledge” of the limits of accuracy of ultrasound scan dating, while those who thought that ultrasound scan-estimated EDD was more accurate than LMP-estimated EDD, irrespective of the woman’s gestational age at estimation, were said to have “poor knowledge” of the limits of accuracy of ultrasound dating.
Statistical analysis
Using an assumed willingness rate of 50% at a confidence interval (CI) of 95% and an error margin of 5%, the minimum sample size for the study was 385, although 460 questionnaires were administered to consenting women. The statistical analysis was both descriptive and inferential at a 95% CI using Statistical Package for Social Sciences computer software version 16 (SPSS Inc., Chicago, IL, USA). Frequency tables were generated for relevant variables. Proportions were compared using the Pearson’s chi-squared test, and relationships were expressed using odds ratios and CIs. A P-value of less than 0.05 was considered to be statistically significant.
Results
A total of 460 questionnaires were administered, but only 443 were completed correctly, giving a response rate of 96.3%. The mean age of the respondents was 27.9±2.41 (range 17–45) years. Most of the women (96.8%, 429/443) were married. Four hundred and thirty-one respondents (97.3%) were from the Igbo tribe and the remaining 12 (2.7%) were from the Yoruba tribe. The majority of respondents were multiparous (56.7%, 251/443) and had tertiary education (79.5%, 352/443). Further details of the sociodemographic characteristics of the respondents are shown in Table 1.
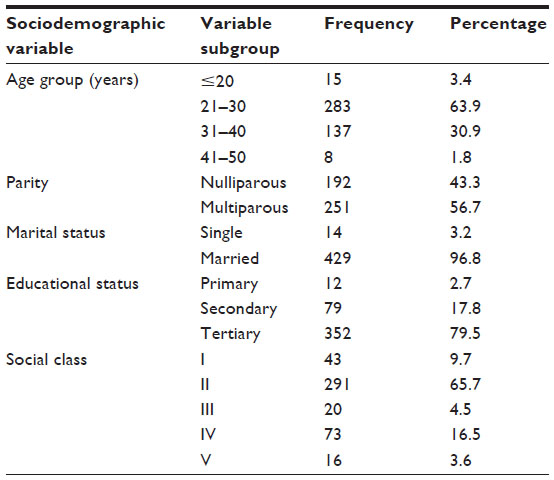 | Table 1 Sociodemographic characteristics of respondents |
The mean gestational age at recruitment and antenatal booking for respondents was 38.7±5.8 (range 36–41) weeks and 26.4±5.82 (range 13–41) weeks, respectively. Forty-one women (9.3%) booked in the first trimester, 190 (42.9%) in the second trimester, and 212 (47.8%) in the third trimester. A majority (87.8%, 389/443) of the respondents had had an ultrasound scan in the index pregnancy, ie, 32 (7.2%) in the first/early second trimester, 51 (11.5%) in the late second trimester, and 306 (69.1%) in the third trimester. One hundred and sixty-seven (42.9%) of 389 women had self-referred for their ultrasound scan.
One hundred and ninety-one (43.1%) respondents knew that LMP-estimated EDD was more accurate than ultrasound scan-estimated EDD in the late second trimester/third trimester, while 244 (55.1%) thought that ultrasound scan-estimated EDD was more accurate than LMP-estimated EDD, irrespective of the woman’s gestational age at estimation. The remaining eight women (1.8%) had no idea as to which of the estimates was more accurate. When respondents were asked whether they would accept induction of labor if the LMP-estimated EDD was exceeded by 10 days but a late second trimester/third trimester ultrasound-estimated EDD was not exceeded, 48.3% (214/443) of the women responded positively. Specifically, 97.9% (187/191) of those who knew that LMP-estimated EDD was more accurate than late pregnancy ultrasound scan-estimated EDD responded positively, while the remaining 2.1% (4/191) of women responded negatively. On the other hand, 88.9% (217/244) of those who thought that ultrasound scan-estimated EDD was more accurate throughout the pregnancy responded negatively, while the remaining 11.1% (27/244) responded positively. All the women who responded positively (48.3%) stated that they would present to hospital for induction on the date set by their attending physicians. Likewise, all the women who responded negatively (51.7%) stated that they would not present to hospital for induction until the ultrasound-estimated EDD was exceeded. The proportion of respondents who would accept induction of labor when LMP-estimated EDD was exceeded by 10 days, but a late second trimester/third trimester ultrasound scan-estimated EDD had not been exceeded, was significantly higher among women who knew that LMP-estimated EDD was more accurate than ultrasound scan-estimated EDD in the late second trimester/third trimester, than in women who did not have this knowledge (97.9% [187/191] versus 11.1% [27/244]; odds ratio 375.73, 95% CI 129.12–1,093.37; P<0.001). Women who had tertiary education were significantly more likely to accept induction of labor after the LMP-estimated EDD had been exceeded by 10 days (and the late second trimester/third trimester ultrasound scan-estimated EDD had not been exceeded) than women who had primary/secondary education (56.0% [197/352] versus 18.7% [17/91]; odds ratio 5.53; 95% CI 3.14–9.76; P<0.001). Similarly, women of high social class were significantly more likely to accept induction of labor after the LMP-estimated EDD had been exceeded by 10 days (and the late second trimester/third trimester ultrasound scan-estimated EDD had not been exceeded) than women of low social class (54.5% [183/336] versus 29.0% [31/107]; odds ratio 2.93; 95% CI 1.83–4.69; P<0.001). However, the age of the women and their parity had no significant association with acceptance of induction of labor after the LMP-estimated EDD had been exceeded by 10 days and the late second trimester/third trimester ultrasound scan-estimated EDD had not been exceeded (P>0.05, see Table 2).
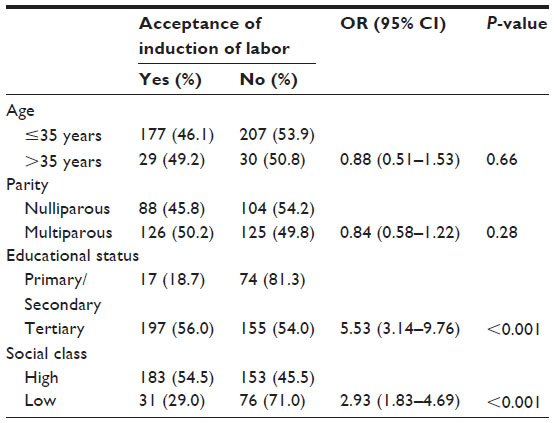 | Table 2 Characteristics of respondents versus acceptance of labor induction for postdatism using menstrual dating |
Discussion
This study demonstrates that pregnant women in Enugu, Nigeria, have poor knowledge of the limits of accuracy of late pregnancy ultrasound scan in estimating the delivery date. This poor knowledge invariably translated into the observed perception of respondents toward induction of labor for postdatism, as more than half of the women (51.7%) would not accept induction of labor until the ultrasound scan-estimated date of delivery had been exceeded, irrespective of the gestational age at which the ultrasound scan estimation was done. This attitude poses a great challenge to perinatal care in our environment because an ultrasound scan is usually carried out in the third trimester when the margin of error is up to 3 weeks.7,13 Further, in keeping with the findings reported by Nwagha et al in 2008,9 this study demonstrates that pregnant Nigerian women in the study area book late for antenatal care. Late booking for antenatal care might have strongly contributed to the poor uptake (7.3%) of early ultrasound scanning observed in this report. The clinical implication of the respondents’ poor uptake of early ultrasound scanning and their poor attitude to induction of labor for postdatism is that they are at risk of post-term pregnancy complications, including placental insufficiency, fetal oligohydramnios, intrauterine fetal death, macrosomia, increased risk of cesarean and instrumental deliveries, and birth injuries, as well as birth asphyxia, neonatal jaundice, and perinatal death.14
The recent proliferation of ultrasound scan services in our environment came with a wave of optimism that ultrasound scanning could accurately determine all aspects of fetal well-being, hence only the well-educated or informed could question or resist its results. This misconception is further worsened by uncontrolled purchasing and use of ultrasound scanning machines by poorly trained personnel who advertise themselves as sonologists or sonographers. Consequently, an unreliable gestational age/EDD may be provided to the pregnant woman, who often undergoes such an investigation on her own without a request from her attending physician. What is even more worrisome is the increasing number of self-referrals for ultrasound by our pregnant women merely to know the EDD which they usually hold on to. Legislation to regulate the acquisition and use of ultrasound by health professionals in the country may help to keep this problem in check. Only qualified/certified health personnel with the requisite knowledge of obstetric ultrasound should be allowed to offer ultrasound scan services. Such legislation should also discourage self-referral by pregnant women for ultrasound. This will further help to prevent our women from visiting poorly trained sonologists and guard against the possible effects of unreliable ultrasound scan results on maternal and neonatal health.
Tertiary education was identified in this report as a strong determinant of acceptance of induction of labor for postdatism using the last menstrual date. This may be explained by the expected impact of education on uptake of maternal and neonatal health services, as observed by previous authors.10 It is expected that the well-educated are more likely to appreciate the limits of any technologic advancements, ultrasound inclusive, unlike the poorly educated who may see ultrasound as an inviolable machine and thus view its results sacrosanct. Also, the lesser educated are more likely to rely more on the impression created outside about a procedure like ultrasound, whether right or wrong. As pointed out by Olusanya et al,12 the higher the educational status of the woman, the higher the social class, and this no doubt may explain the higher acceptance rate among women of higher social class than among women of lower social class. Given that women with a better knowledge of the limits of accuracy of late ultrasound scan dating are more likely to accept induction for postdatism when a certain LMP-estimated EDD is exceeded by 10 days, but a late second trimester/third trimester ultrasound scan-estimated EDD has not been exceeded, educating our women via antenatal health talks and other public health enlightenment campaigns in this direction will ultimately improve their perception of the accuracy of ultrasound scan dating in late pregnancy. This will help to reduce the incidence of prolonged pregnancy and its complications in our environment.
The limitation of this study is that the willingness to accept labor induction was assumed to mean acceptance of induction of labor. It is likely that some of the respondents might have responded differently if their pregnancies were actually prolonged. However, the effect of this limitation on the study estimates is likely to be minimal. Further studies using a population of women with prolonged pregnancy (>40 weeks plus 10 days) are recommended. Selection of respondents for this study was consecutive considering the short study period, and selection bias cannot be ruled out; a longer study period and use of probability sampling would have been more appropriate. The strength of the study is that it is a novel effort toward stimulating the interest of physicians involved in maternal care regarding the increasing wave of self-referral for ultrasound scan in pregnancy in our environment, and the strong value mothers attach to ultrasound scan dating.
In conclusion, this study shows that in cases where late pregnancy ultrasound scan-derived EDD is further on than the menstrual dating, most women seen in the antenatal clinics at the teaching hospitals in Enugu would not be willing to accept labor induction for postdatism based on their menstrual dating. This worrisome attachment to ultrasound scan dating is a challenge to the prevention of prolonged pregnancy and its complications in our environment. Predictors of this attitude in our study were low educational status, low social class, and poor knowledge of the limitations of late pregnancy ultrasound scan dating. Antenatal health education should discourage self-referral for ultrasound scanning and emphasize the limitations of late ultrasound scan dating as well as the perinatal effects of prolonged pregnancy. Educational campaigns are also encouraged regarding the need for early antenatal booking and accurate determination of EDD and gestational age during pregnancy. Further, there is a need for urgent legislation regarding the acquisition/use of ultrasound in our environment in order to check the recent uncontrolled proliferation of ultrasound services and its adverse effects on maternal and neonatal health.
Disclosure
The authors report no conflicts of interest in this work.
References
Lynch CD, Zhang J. The research implications of the selection of a gestational age estimation method. Paediatr Perinat Epidemiol. 2007;21:86–96. | |
Jehan I, Zaidi S, Rizvi S, et al. Dating gestational age by last menstrual period, symphysis-fundal height, and ultrasound in urban Pakistan. Int J Gynecol Obstet. 2010;110:231–234. | |
Hunter LA. Issues in pregnancy dating: revisiting the evidence. J Midwifery Womens Health. 2009;54:184–190. | |
Abuhamad AZ; ACOG Committee on Practice Bulletins-Obstetrics. ACOG Practice Bulletin, clinical management guidelines for obstetricians-gynecologists number 98, Oct 2008 (replaces Practice Bulletin number 58, Dec 2004). Ultrasonography in pregnancy. Obstet Gynecol. 2008;112:951–961. | |
Tailpale P, Hiilesmaa V. Predicting delivery date by ultrasound and last menstrual period in early gestation. Obstet Gynecol. 2001;97:189–194. | |
Olesen AW, Thomsen SG. Prediction of delivery date by sonography in the first and second trimesters. Ultrasound Obstet Gynecol. 2006;28:292–297. | |
Mongelli M, Ramus RM. Evaluation of gestation: combining menstrual and ultrasonographic dates [Updated March 29, 2012]. Available from: http://emedicine.medscape.com/article/259269-overview#a30. Accessed July 25, 2013. | |
Mongeli M, Wilcox M, Gardosi J. Estimating the date of confinement: ultrasonographic biometry versus certain menstrual dates. Am J Obstet Gynecol. 1996;174:278–281. | |
Nwagha UI, Ugwu OV, Nwagha TU, Anyaehie US. The influence of parity on the gestational age at booking among pregnant women in Enugu, South East Nigeria. Niger J Physio Sci. 2008;23:67–70. | |
Ugwu EO, Ezechukwu PC, Obi SN, Ugwu AO, Okeke TC. Utilization of insecticide treated nets among pregnant women in Enugu, South Eastern Nigeria. Niger J Clin Pract. 2013;16:292–296. | |
Ugwu EO, Obi SN, Iferikigwe ES, Dim CC, Ezugwu FC. Membrane stripping to prevent post-term pregnancy in Enugu, Nigeria: a randomized controlled trial. Arch Gynecol Obstet. June 14, 2013. [Epub ahead of print.] | |
Olusanya O, Okpere EE, Ezimokhai M. The importance of social class in voluntary fertility control in a developing country. West Afr J Med. 1985;4:205–212. | |
Kalish RB, Chervenak FA. Sonographic determination of gestational age. Ultrasound Rev Obstet Gynecol. 2005;5:254–258. | |
Chantry AA, Lopez E. Fetal and neonatal complications related to prolonged pregnancy. J Gynecol Obstet Biol Reprod (Paris). 2011;40:717–725. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.