")
Back to Journals » Nutrition and Dietary Supplements » Volume 12
Women’s Involvement in Household Decision-Making and Nutrition Related-Knowledge as Predictors of Child Global Acute Malnutrition in Southwest Ethiopia: A Case–Control Study
Received 3 March 2020
Accepted for publication 10 June 2020
Published 22 June 2020 Volume 2020:12 Pages 87—95
DOI https://doi.org/10.2147/NDS.S252342
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Chandrika J Piyathilake
Shimelis Girma, Arefayne Alenko
Department of Psychiatry, Faculty of Medicine, Institute of Health, Jimma University, Jimma, Oromia, Ethiopia
Correspondence: Shimelis Girma
378, Jimma University, Jimma, Ethiopia
Tel +251 911721438
Email [email protected]
Background: Global acute malnutrition is one of the major contributors to the death of young children. It accounts for about 35% to 55% of all childhood deaths in low- and middle-income countries. However, there have been limited studies examining the relationship between global acute malnutrition and women’s involvement in decision-making, and nutrition-related knowledge in the locality.
Patients and Methods: A case–control study was conducted from March to April 2018. The sample size was determined using Epi Info statistical software, and a total of 234 children with their parents involved in the study. Childs’ height was measured using a stadiometer, and a digital weight scale was used to measure child weight. Weight-for-height Z-score (WHZ) was computed using the World Health Organization (WHO) Anthro Software. Women’s involvement in household decision-making was assessed using the household decision-making index. Socio-demographic and maternal nutrition-related knowledge were assessed using a structured questionnaire. Data entry and statistical analysis were done using EpiData 3.1 and Statistical Package for Social Science 24.0 (SPSS). Statistically, a significant association was declared by adjusted odds ratio (AOR), 95% confidence interval (CI), and P-value less than or equal to 0.05.
Results: About three-fifths of mothers whose children were cases had poor nutrition-related knowledge regarding optimal child feeding. The study found poor maternal nutrition-related knowledge (AOR 5.16, 95% CI (1.9, 13.96)), not attending formal education (AOR 4.98, 95% CI (2.09, 11.82)), lack of maternal involvement in household decision-making (AOR 4.68, 95% CI (1.99, 10.97)), and lowest wealth index (AOR 3.76, 95% CI (1.24, 11.38)) as independent predictors.
Conclusion and Recommendation: Maternal nutrition-related knowledge, maternal educational status, and involvement in household decision-making were found to be independent predictors of child global acute malnutrition. Emphasis needs to be given in strengthening girls’ education, nutrition education, household economic strengthening activities, and women empowerment in decision-making.
Keywords: global acute malnutrition, Southwest Ethiopia, household-related factors
Introduction
Adequate child nutrition is essential to ensure survival, healthy growth, and proper development. Childhood malnutrition is a major global health problem contributing to increased morbidity and mortality.1,2 Worldwide, 55 million children younger than age five are affected by global acute malnutrition (GAM) and 19 million affected by severe GAM.3 The Joint United Nations International Children’s Emergency Fund (UNICEF), World Health Organization (WHO), and World Bank (WB) group report indicated that GAM continued to threaten the lives of an estimated 7.5% or nearly 51 million young children. As per the report, the problem is even more severe in Africa, where more than one quarter lived in Africa, and in Eastern Africa, about 13.8% of children are affected by GAM.4 Ethiopia has the highest rates of malnutrition in Sub-Saharan Africa.5 A nationwide survey in Ethiopia indicated that 10% of children wasted and 3% severely wasted.6,7
It is recommended that infants should exclusively be breastfed during the first 6 months of life and thereafter supplementation of nutritionally adequate and safe complementary foods.8 However, optimal child feeding and caring practices are a major immediate factor for malnutrition. Human resource determinants take major consideration for the fulfillment of optimal child nutrition. Parental education and parental nutrition-related knowledge are key factors in maintaining optimal child nutrition.9–12
Analysis of the study conducted in 63 countries indicated that women’s education was strongly associated with child malnutrition in developing countries.13 A study conducted in rural Uganda14 and Nigeria15 revealed a significant statistical association between maternal educational status and nutritional-related knowledge and child nutritional status. The results of the Ethiopian Demographic Health Survey (EDHS) showed a positive relationship between mothers’ education and the nutritional status of their children.16 Similar findings were reported in Southern Ethiopia,17 Ghana,18 and Nairobi.19
In low-resource settings where women invest more in the welfare of their children, women’s ability in decisions is quite important for the nutritional outcome of children. A review of previous studies from LAMICs reported the effect of women empowerment on child nutritional status.20,21 Women’s decision-making roles were significantly compromised in a household earning lower income and those in the lowest quartile of wealth index. This, in turn, has been found a risk factor for child malnutrition.16,22 Furthermore, maternal hand-washing practice and large family size with overcrowding and inadequate spacing have been implicated as risk factors for acute malnutrition.23 Overall, several studies have examined the determinant factors of acute malnutrition. These studies are limited in examining the relationship between global acute malnutrition and maternal nutrition-related knowledge and decision-making roles. Most of the studies focused on either of the parents’ and often did not address women’s involvement in intra-household decision-making. Thus, the study was designed to assess predictors of global acute malnutrition focusing on maternal education, nutrition-related knowledge, and decision-making roles.
Patients and Methods
Study Design and Period
The institution-based age-matched case–control study design was conducted from March to April 2018.
Study Area and Setting
This study was conducted in all public health facilities in Jimma city, Ethiopia. The city has thirteen administrative Kebeles. Four public health centers are delivering primary health care services for the community: Jimma Health Center, higher two Health Center, Mandera Koche Health Center, and Bacho Bore Health Center. The city has one zonal hospital and one medical center which are namely Shenan Gibe Hospital and Jimma Medical Center (JMC), which delivers advanced medical services for approximately fifteen million people in Southwest Ethiopia.
Measuring Tools
Childs anthropometry was collected using a stadiometer, digital weight scale, and Salter scale. Parental nutrition-related knowledge was assessed using a structured questionnaire that included 13-items. The questionnaire has three main components: breastfeeding, complementary feeding, and feeding during difficult situations. The percentage score for each study participant was determined by the sum of correct responses given divided by the total number of questions. The overall composite score was categorized into three: score of less than 60% considered as poor knowledge, a score of 60–75% fair knowledge, and a score greater than 75% good knowledge. Women’s involvement in decision-making was assessed by the household decision-making index. The questionnaire contains women’s decisions regarding the use of once-earning, health care, major household purchase, and a visit to family or relatives. Each question had five responses: (1) respondent alone, (2) respondent and husband/partner jointly, (3) husband/partner alone, (4) someone else, and (5) others. The index was dichotomized for analysis, and we grouped one and two as women involved in decision-making, and responses 3–5 as women have no say in the decision.16 The food security status of the households was determined by the household food insecurity scale (HFIAS) developed by food and nutrition technical assistance (FANTA) in 2007.24 Wealth index was assessed using a structured questionnaire adapted from EDHS, and the scoring was based on ownership of fixed assets, and ownership of each fixed asset given a value of one, and non-ownership a value of zero.16 Other socio-demographic and environment-related factors were assessed using a structured questionnaire.
Population
Cases were all randomly selected children aged 6 to 59 months attending public health facilities in Jimma city during the data collection period, and who were found to have global acute malnutrition (WHZ-score less than −2 standard deviations (SD)).25 Controls were age-matched children visiting the same health facility with cases, and who were found to be without global acute malnutrition (WHZ-score above and equal to −2SD). Age intervals used for matching: 6–11 months, 12–23 months, 24–35 months, 36–47 months, and 48–59 months.
Sample Size Determination and Sampling Techniques
The sample size required for the study was determined using Epi Info statistical software version 7. The following assumptions were considered: the percentage of children with global acute malnutrition (cases) among households’ having fewer than five family members was 68.14%;26 the percentage of children without acute malnutrition (controls) among households’ having more than five family members was 46.9%;26 95% CI, 80% power, case to control ratio of 1:2 to detect an odds ratio of 2.4 and 10% of non-response rate. Thus, 234 children and their corresponding parents were included in the study. All public health facilities that were found in Jimma town and delivering medical services for children were identified and approached. The health facilities were Jimma Health Center, higher two Health Center, Mandera Koche Health Center, Bacho Bore Health Center, Shenan Gibe Hospital, and Jimma Medical Center (JMC). Retrospective data of 6 months regarding patient flow were obtained prior to data collection to be used as a base for proportional allocation to study subjects. Accordingly, study participants were proportional allocated to health facilities. A systematic random sampling technique was used to select cases, and every 2nd child from each health facility was recruited into the study. Controls were selected from the same health facility from which cases were selected (Figure 1).
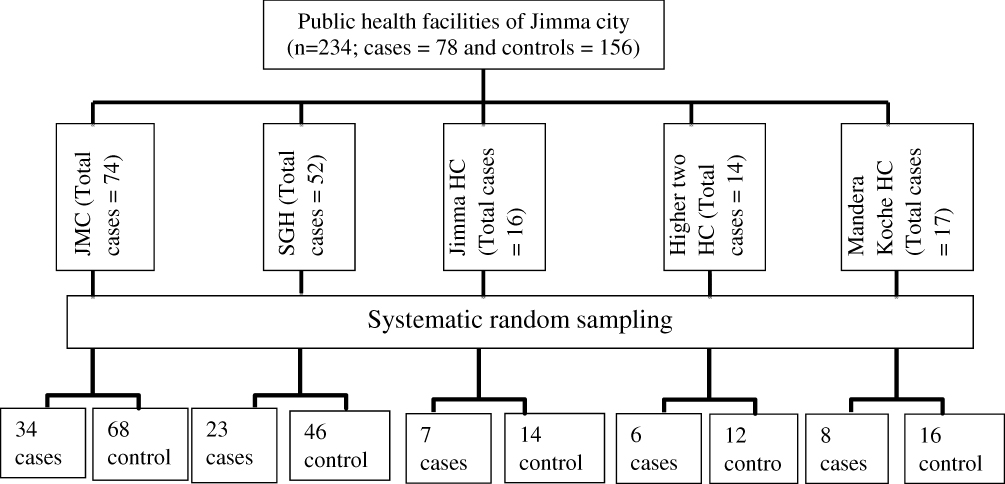 |
Figure 1 Flow chart of the sampling procedure of study participants attending public health facilities in Jimma city, Southwest Ethiopia (n = 234). |
Data Collection Procedure and Statistical Analysis
All children visiting public health facilities were screened for global acute malnutrition by the research team. A semi-structured interviewer-administered questionnaire was used to collect data related to the objectives of the study. The questionnaires were prepared in English, translated to Afaan Oromo and Amharic, and finally back translated into English language by other person who has good command of English, Afaan Oromo, and Amharic to check for its consistency. The questionnaire covered a range of topics including socio-demographic factors, child characteristics, and parental child feeding and caring knowledge. It took an average of 30–45 minutes to be filled. Height measured in standing position for children aged 24 months and older in a standard Frankfurt position. Weight was measured using a digital weight scale (SECA made in Germany) while a child dressed in a light cloth. Height and weight measurements were taken to the nearest 0.1cm/kg. Measurements’ taken twice, and the mean score was used in case of a significant difference between measurers during analysis. Following measurement, individual anthropometric data were entered into the WHO Anthro software version 3.2.2 to compute WHZ. Once a case of global acute malnutrition was identified, parents approached to collect the necessary data. For every case, respective two age-matched controls were identified. Data were entered into EpiData version 3.1 and exported into SPSS version 24.0 for analysis. Logistic regression analysis was used to determine factors that were independently associated with global acute malnutrition. AOR, 95% CI, and P-value less than or equal to 0.05 were used to decide statistically significant associations with the outcome variable. Seven nurses were recruited as data collectors, five nurses with their assistance were recruited as measurers, and two Nutritionists were recruited as supervisors. Training was given to data collectors, measurers, and supervisors for two days on the overall procedure of the study.
Result
Characteristics of the Study Participants
The mean ages of mothers and fathers were 25.74 ± 4.75 and 35.05 ± 6.15, respectively. More than two-thirds (69.7%) and (68.4%) parents were Muslim by religion and Oromo by ethnicity. The mean age of children with global acute malnutrition was 18.29 ± 10.23 months. Close to two-fifths of study participants, ie, 43.6% of mothers and 38.9% of fathers of children had no formal education (Table 1).
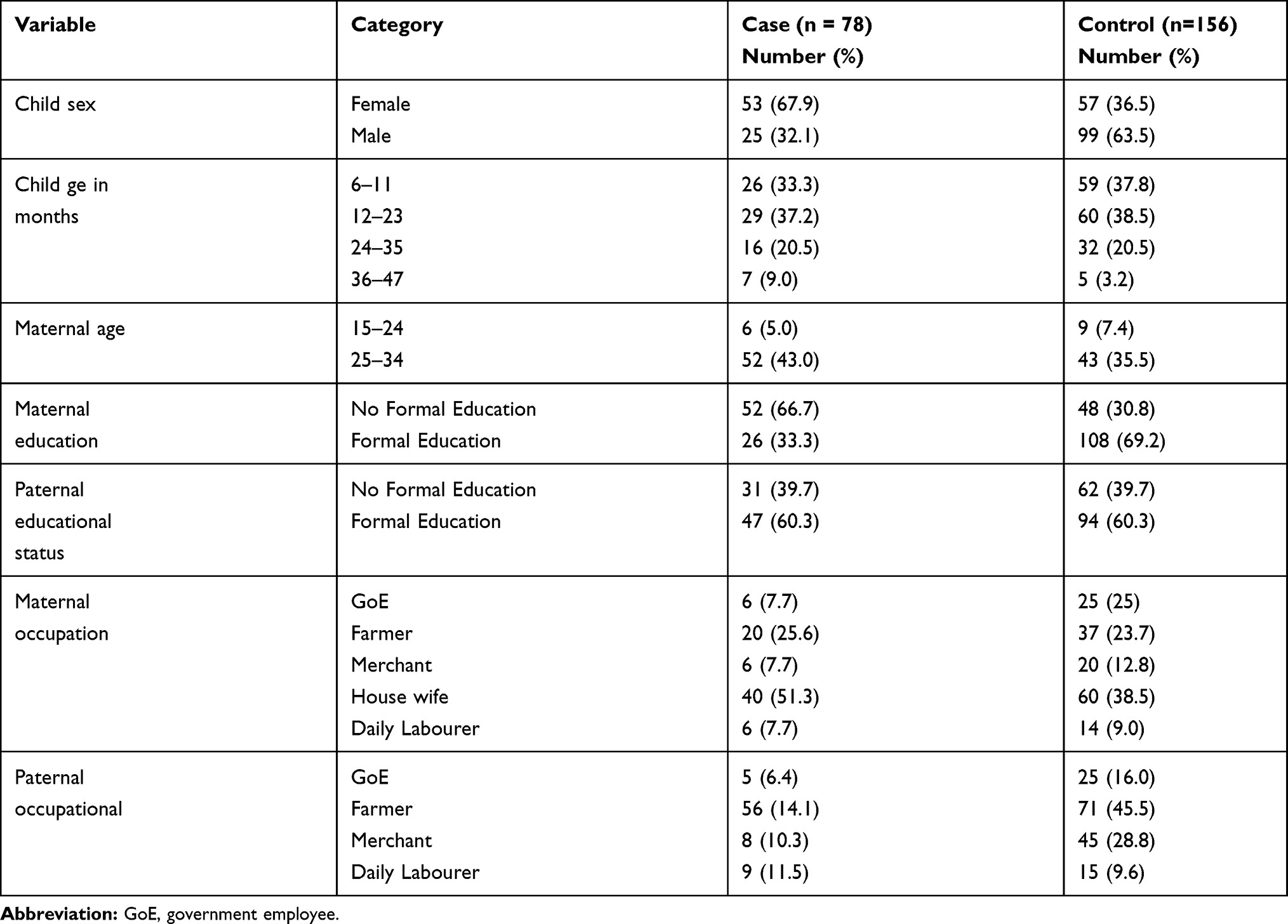 |
Table 1 Socio-Demographic Characteristics of Study Participants Attending Public Health Facilities in Jimma City, Southwest Ethiopia (n = 234) |
Parental Nutrition-Related Knowledge and Maternal Decision-Making Role
Two-fifths of women and about half of fathers scored poor for child nutrition-related knowledge. Regarding maternal involvement in decision-making roles, two-thirds (63.5%) of controls’ mothers and one-third (32.1%) of cases’ mothers had a say in making decisions on their own health care. Similarly, three-fourth (77.6%) of controls’ mothers and more than half (52.6%) of cases’ mothers were involved in decision-making regarding family visits. Regarding decisions regarding major household purchases, three-fourth (75%) of controls’ mothers and more than one-third (38.5) of cases’ mothers had active involvement in joint decision-making with their partner (Table 2).
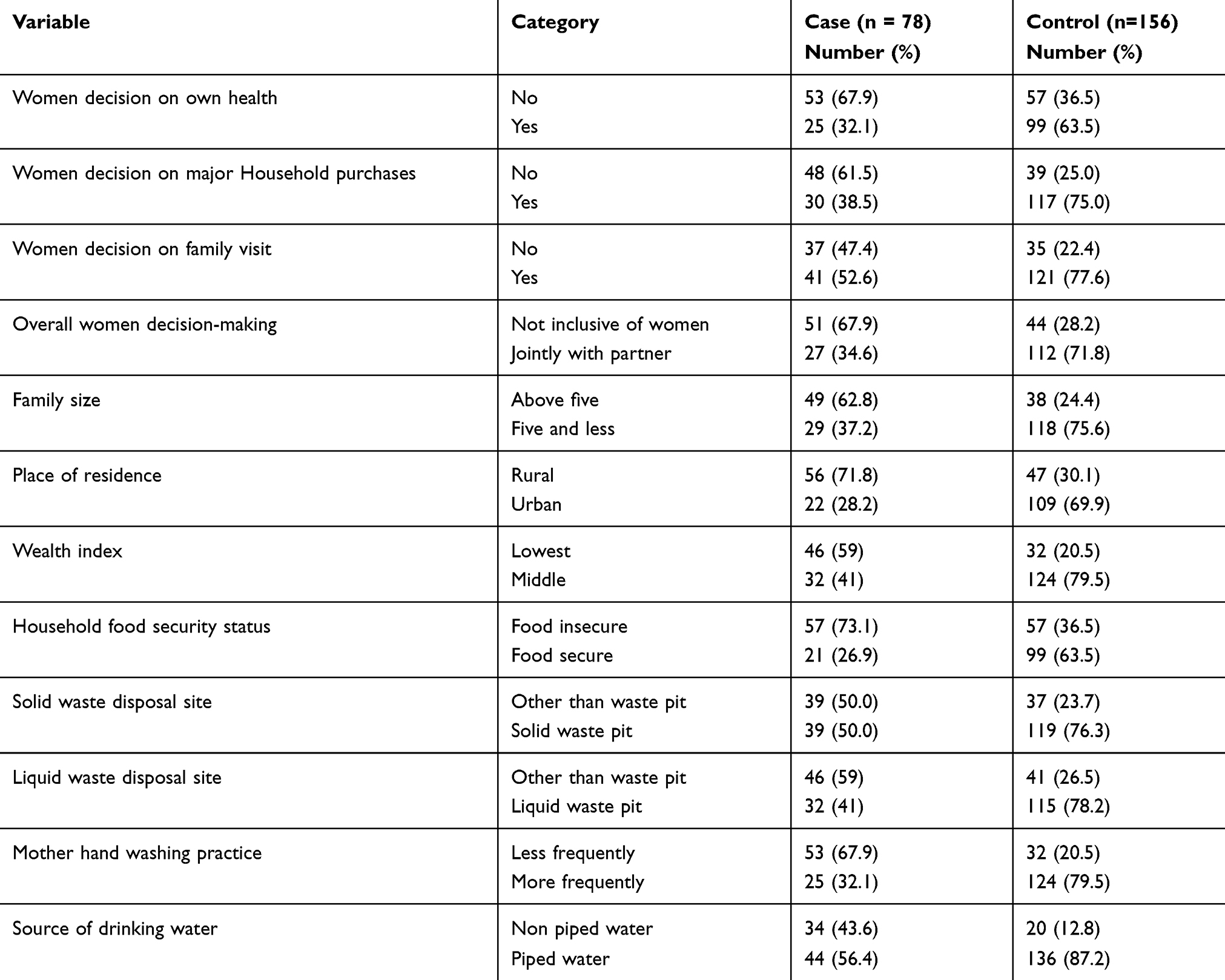 |
Table 2 Maternal Decision-Making Role and Other Household-Related Factors of Study Participants Attending Public Health Facilities of Jimma City, Southwest Ethiopia (N= 234) |
Other Co-Variables
The wealth index of the household was determined based on the ownership of fixed assets by householders. Principal component analysis was used to generate factors and components that define the index. Finally, the factors that fulfilled the assumption for the analysis and computed to generate the index were ownership of mobile phone, bed with mattress, chair, and having electricity. Accordingly, more than half (57.7%) of cases and about two-third (64.7%) of control households were found to have the lowest and highest wealth index, respectively. About 73% of cases and 36% of controls had reported food insecurity in the last one month prior to the data collection period (Table 2).
Multivariable Analysis
The final logistic regression model indicated that children whose mothers had poor nutrition-related knowledge were six times more likely to be acutely malnourished than their counterparts (AOR 6.23, 95% CI (2.49, 15.57)). Similarly, children whose mothers had fair nutrition-related knowledge were found to be four times more likely to be acutely malnourished than mothers who had good knowledge (AOR 3.59, 95% CI (1.21, 12.80)). Regarding women involvement in decision-making, children living in households in which women have no say in decision-making were five times more likely to be acutely malnourished than in households where women involved in joint decision-making (AOR 4.68, 95% CI (1.99, 10.97)). Furthermore, the lowest wealth index (AOR 3.76, 95% CI (1.24, 11.38)) and maternal hand-washing practice (AOR 4.51, 95% CI (1.99, 10.19)) were found to be independent predictors of GAM (Table 3).
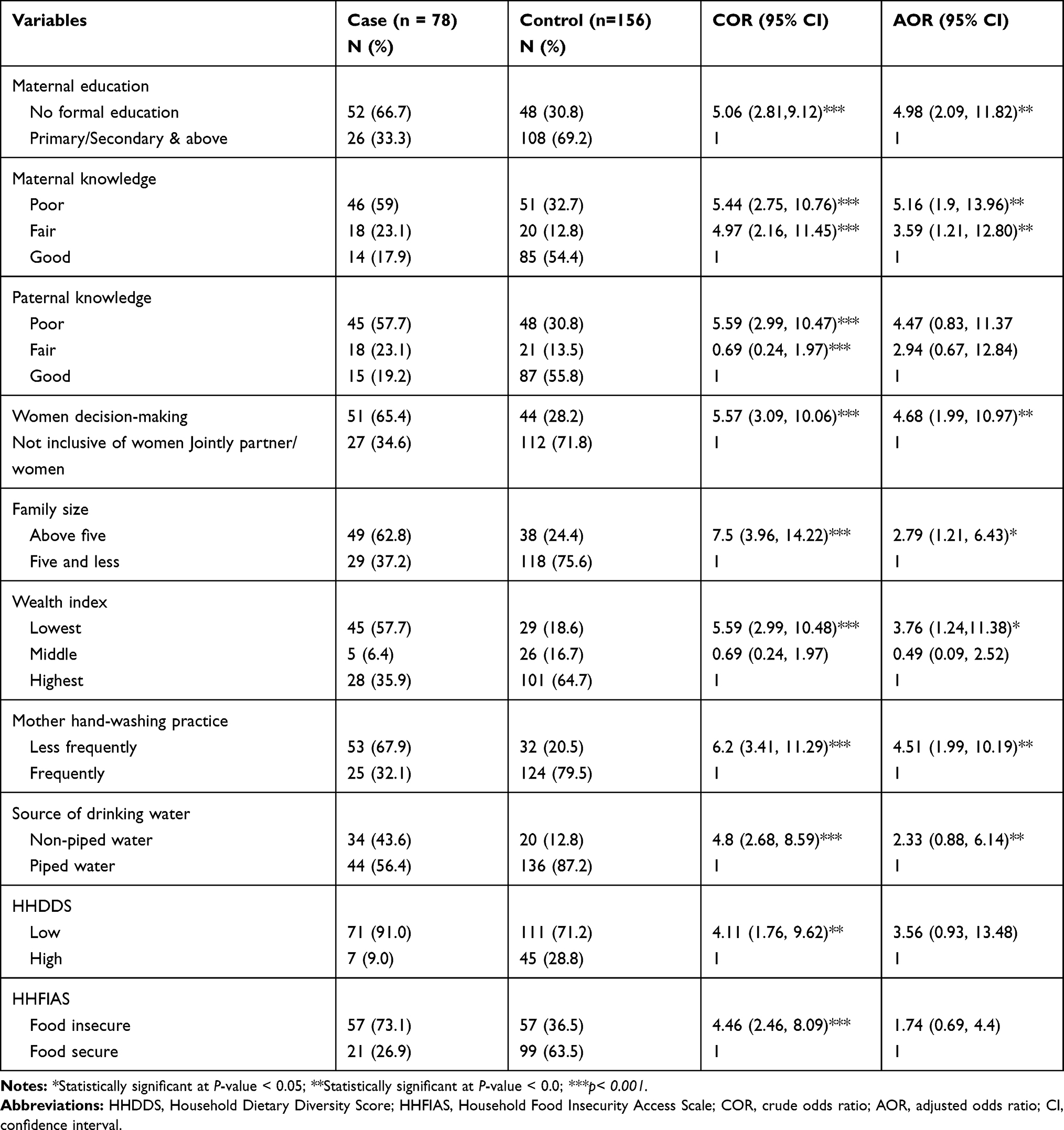 |
Table 3 Independent Predictors of Global Acute Malnutrition of Study Participants Attending Public Health Facilities in Jimma City, South West Ethiopia (n = 234) |
Discussion
The major finding of our study was maternal nutrition-related knowledge, maternal educational status, and women involvement in decision-making strongly predicts global acute malnutrition. Children whose mothers had poor nutrition-related knowledge were six times more likely to be acutely malnourished than their counterparts. This result is consistent with a study conducted in Nigeria, which revealed that mother’s nutrition and health-related knowledge safeguard young children from occasions that reduce height-for-age z-score (HAZ) and WHZ scores.18 Other studies report an independent association between maternal nutrition-related knowledge and global acute malnutrition.27,28 Regarding parental educational status, maternal educational status was found to be an independent predictor of acute malnutrition. A review of a demographic health survey of 62 low - and middle-income countries (LAMICs) revealed a stronger protective effect of maternal education.20 Similarly, several studies reported the same finding.29–32 Research findings indicated that an increased level of maternal education enhances higher health-seeking behavior for her childhood illness, and this helps the child in regain health shortly. The other possible reason might be that education generates confidence and allows women to be strongly involved in joint decision-making. This is supported by the current finding which found out women’s involvement in decision-making increases with the level of education.
Evidence from low-resource settings indicated the differential in preferences between men and women in channelling resources towards the welfare of the child.33,34 This depends on partners’ ability to negotiate, which contributes to women involvement in decision-making.35 In this study, data regarding women involvement in decision-making were collected on women’s involvement in their own health care, making major household purchases, and visits to family or relatives. Accordingly, the results of this study indicated that children whose mothers had no say in the intra-household decision were found to be four times more likely to be acutely malnourished than their counterparts. This study finding is in line with the study done in low-resource settings in which it is identified that lack of women’s decision-making as a predictor of child malnutrition.20,36 A study conducted in Benin found out that women decision-making autonomy was independently associated with WHZ-score of male children and WHZ and WAZ-scores of female children.20 A similar finding was also reported in Nepal37 and Southwest Ethiopia.38 The status of women in a society is also an important determinant of the nutritional status of women and children.
A previous study finding indicated that women’s low social status affects their autonomy in decision-making regarding family size, health-care-seeking behavior, child-feeding, support, and care.39 Furthermore, male dominance in Ethiopia poses difficulty in ensuring women independent decision-making in individual and household issues, which can affect the health and nutritional status of the child.40 Children from the lowest wealth index households were found to be four times more likely to be acutely malnourished. A study done in Ethiopia indicated that children belonging to the low-income group were at a higher risk of being wasted than children of better income families.41 The economic constraint in LAMICs limits the quality of food consumption and increases the likelihood of infection. In addition to this, a high socioeconomic status allows greater purchasing power for food and other goods that ensure the health of children.42 Family size in the study was found to be associated with global acute malnutrition, and a similar relationship was reported by previous studies.26,43 The inadequate allocation of household resources among many children may lead to a low nutritional status. The other possible explanation might be due to resource depletion, which is exposed to poverty and decrement in health care seeking practice, household environmental sanitation, food availability, and nutrition insecurity.
Strengths and Limitation of the Study
The main strength of our study was that two separate measurements were engaged to measure child anthropometry to minimize variability. Calibration of the anthropometric tool was given high emphasis, and factors like women decision-making role were addressed in this study. Measurement tools used to measure some explanatory variables relied on participants’ self-reported data, which were prone to recall bias and social desirability bias.
Conclusion
The study found out maternal education, maternal nutrition-related knowledge, women involvement in decision-making, maternal hand-washing practice, and family size as independent determinants of global acute malnutrition in children. Thus, concerned responsible bodies need to invest more in girls' education and women empowerment in decision-making.
Abbreviations
AOR, adjusted odds ratio; CI, confidence interval; EDHS, Ethiopian Demographic Health Survey; GAM, global acute malnutrition; HAZ, height-for-age z-score; HC, health center; JMC, Jimma medical Center; LAMICs, low and middle income countries; SD, standard deviation; SGH, Shenan Gibe Hospital; SPSS, Statistical Package for Social Sciences; UNICEF, United Nations International Children’s Emergency Fund; WB, World Bank; WHO, World Health Organization; WAZ, Weight-for-age z-score; WHZ, Weight-for-height z-score.
Data Sharing Statement
Data generated for this study are included in the article. The data set available upon request from the author in charge.
Ethics Approval and Consent to Participate
Ethical approval was obtained from the Institute of Ethical Review Board of Jimma University. Written informed consent was taken from the study participants, and parents provided written informed consent for their child participation. The study was conducted according to the Declaration of Helsinki.
Consent for Publication
Not applicable
Acknowledgments
The authors would like to acknowledge Jimma University, data collectors, supervisors, and study participants.
Author Contributions
Authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
We approve that there is no conflict of interest.
References
1. Black REAL, B Z, Caulfield LE, et al.; for the Maternal and Child Undernutrition Study Group. Maternal and child undernutrition: global and regional exposures and health consequences. Lancet. 2008;371:243–260. doi:10.1016/S0140-6736(07)61690-0
2. Liu LJH, C S, Perin J, et al.; for the Child Health Epidemiology Reference Group of WHO and UNICEF. Global, regional, and national causes of child mortality: an updated systematic analysis for 2010 with time trends since 2000. Lancet. 2012;379:2151–2161. doi:10.1016/S0140-6736(12)60560-1
3. ACF. What is acute malnutrition? Action against hunger. Available from: http://actioncontrelafaim.ca/what-is-acute-malnutrition/what-is-acute-malnutrition. Accessed June 17, 2020.
4. UNICEF W, World B. Levels and trends in child malnutrition: UNICEF/WHO/World Bank Group joint child malnutrition estimates key findings. New York. 2018.
5. MoH. Protocol for the Management of Severe Acute Malnutrition. Addis Ababa.
6. CSA. Ethiopia Mini Demographic and Health Survey. Addis Ababa; 2014.
7. CSA ICF. Ethiopian Demographic and Health Survey. Addis Abeba, Ethiopia and Rockville, Maryland, USA: Central Statistical Agency and ICF International; 2016.
8. UNICEF. Infant and young child feeding. 2011. Available from: https://www.unicef.org/nutrition/files/Final_IYCF_programming_guide_2011.pdf. Accessed June 17, 2020.
9. Kuzma J. Knowledge, attitude and practice related to infant feeding among women in rural Papua New Guinea: a descriptive, mixed method study. Int Breastfeed J. 2013;8:16. doi:10.1186/1746-4358-8-16
10. Karnawat DKB, J A, Kohli GK. Knowledge, attitude and practices about infant feeding among mothers of urban and rural area of Ajmer district. J Med Res. 2015;1(3):90–94.
11. Ekwochi UNI, O C, Amadi OF, et al. Knowledge of danger signs in new borns and health seeking practices of mothers and caregivers in Enugu state, South-East Nigeria. Ital J Pediatr. 2015;41(1):18. doi:10.1186/s13052-015-0127-5
12. Al-Ayed IH. Mothers’ knowledge of child health matters: are we doing enough? J Family Community Med. 2010;17(1):22–28. doi:10.4103/1319-1683.68785
13. Smith LC, Haddad LJ. Explaining child malnutrition in developing countries: a cross-country analysis. Int Food policy res Inst. 2000.
14. Wamani HAA, P S, Tumwine J, Tylleskar T. Predictors of poor anthropometric status among children under 2 years of age in rural Uganda. Public Health Nutr. 2006;9(3):320–326. doi:10.1079/PHN2006854
15. Akeredolu A, JOO JS; Seriki-Mosadolorun and U. Okorafor. Mothers’ nutritional knowledge, infant feeding practices and nutritional status of children (0–24 Months) in Lagos state. Nigeria; Eur J Nut Food Safety. 2014;4(4):364–374. doi:10.9734/EJNFS/2014/7604
16. CSA, ICF. Ethiopia Demographic and Health Survey 2011. Addis Ababa, Ethiopia and Calverton, Maryland, USA: Central Statistical Agency and ICF International; 2012.
17. Dereje N. Determinants of severe acute malnutrition among under five children in Shashogo Woreda, Southern Ethiopia; a community based matched case control study. Int J Res. 2014;1:6.
18. Saaka M. Relationship between mothers’ nutritional knowledge in childcare practices and the growth of children living in impoverished rural communities. J Health Popul Nutr. 2014;32(2):
19. Benta AJC, Elizabeth K. Effect of mother’s education on child’s nutritional status in the slums of Nairobi. BMC Pediatr. 2012;12:80.
20. Alaofe H, Zhu M, Burney J, Naylor R, Douglas T. Association between women’s empowerment and maternal and child nutrition in Kalalé district of Northern Benin. Food Nutr Bull. 2017;38(3):302–318. doi:10.1177/0379572117704318
21. Rabaoarisoa C, Rakotoarison R, Rakotonirainy NH, et al. The importance of public health, poverty reduction programs and women’s empowerment in the reduction of child stunting in rural areas of Moramanga and Morondava, Madagascar. PLoS One. 2017;12(10):10. doi:10.1371/journal.pone.0186493
22. Egata G, Berhane Y, Worku A. Predictors of acute under nutrition among children aged 6 to 36 months in east rural Ethiopia: a community based nested case-control study. BMC Pediatr. 2014;14:91. doi:10.1186/1471-2431-14-91
23. Haidar J, Abate G, Koqi-Makau W, Sorensen P. Risk factors for child under nutrition with a human rights edge in rural villages of North Wollo, Ethiopia. East Afr Med J. 2005;82(12):625–630. doi:10.4314/eamj.v82i12.9367
24. Coates J, Swindale A, Bilinsky P. Household Food Insecurity Access Scale (HFIAS) for Measurement of Household Food Access: Indicator Guide. 3. Washington D.C: Food and Nutrition Technical Assistance Project. Academy for Educational Development; 2007.
25. CDC WFP. A Manual for Measuring and Interpreting Malnutrition and Mortality. 2005.
26. Bokore A, Woldemariam T, Sufa A. Determinants of acute malnutrition among children aged 6–59 months in public hospitals, Oromia region. West Ethiopia. 2015;1:34.
27. Webb P, Block S. Nutrition information and formal schooling as inputs to child nutrition. Econ Dev Cult Change. 2004;52(4):801–820. doi:10.1086/420901
28. Appoh LY, Krekling S. Maternal nutritional knowledge and child nutritional status in the Volta region of Ghana. Matern Child Nutr. 2005;1(2):100–110. doi:10.1111/j.1740-8709.2005.00016.x
29. A LA A, Fouad H, Sadeq A, Saif A. Effect of mothers’ nutritional knowledge and attitudes on Omani children’s dietary intake. Oman Med J. 2011;26(4):253.
30. Frost MBFR, Haas DW. Maternal education and child nutritional status in Bolivia: finding the links. Soc Sci Med. 2005;60(2):395–407. doi:10.1016/j.socscimed.2004.05.010
31. Glewwe P. Why does mother’s schooling raise child health in developing countries? Evidence from Morocco. J Human Res. 1999;34:124. doi:10.2307/146305
32. Desai S, Alva S. Maternal education and child health: is there a strong causal relationship? Demography. 1998;35(1):71–81. doi:10.2307/3004028
33. FAO. Women in Agriculture: Closing the Gender Gap for Development. Rome, Italy: Food and Agriculture Organization of the United Nations; 2011.
34. UNICEF. Gender Influences on Child Survival, Health and Nutrition. A Narrative Review Geneva: United Nations Children’s Fund (UNICEF); 2011.
35. Sen A. Gender and cooperative conflicts. In: Tinker I, editor. Persistent Inequalities: Women and World Development. Oxford: Oxford University Press; 1990.
36. Cunningham K, Ruel M, Ferguson E, Uauy R. Women’s empowerment and child nutritional status in South Asia: a synthesis of the literature. Matern Child Nutr. 2015;11:1–19. doi:10.1111/mcn.12125
37. Dancer D, Rammohan A. Maternal autonomy and child nutrition: evidence from rural Nepal. Indian Growth Develop Rev. 2009;2(1):18–38. doi:10.1108/17538250910953444
38. Abate KH, Belachew T. Women’s autonomy and men’s involvement in child care and feeding as predictors of infant and young child anthropometric indices in coffee farming households of Jimma Zone, South West of Ethiopia. PLoS One. 2017;12(3):e0172885. doi:10.1371/journal.pone.0172885
39. Heaton TB, Forste R.(2007). Domestic violence, couple interaction and children’s health in Latin America. Springer science and business media. J Fam Viol.2008;23:183–193. doi:10.1007/s10896-007-9142-7
40. Alemu B, Asnake M. Women’s Empowerment in Ethiopia: New Solutions to Ancient Problems. Ethiopia: Pathfinder International; 2007.
41. Abate A, Bayissa D, Belachew T. Predictors of acute malnutrition among 6–23 months children in Hidhebu Abote Woreda, Oromi, Ethiopia. J Health, Med Nursing. 2016;24.
42. de Poel E, Hosseinpoor A, Speybroeck N, Ourtia T, Vegab J. Socioeconomic inequality in malnutrition in developing countries. Bull World Health Organ. 2008;86:282–291. doi:10.2471/BLT.07.044800
43. Fazlur R, Islam G, Jan MA. Association of risk factors with severe malnutrition in children under five years of age in Peshawar, Pakistan. J Med Sci. 2013;21(4):180–182.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.