")
Back to Journals » Journal of Pain Research » Volume 12
Where should analgesia lead to? Quality of life and functional recovery with tapentadol
Authors Panella L, Rinonapoli G , Coaccioli S
Received 8 October 2018
Accepted for publication 27 February 2019
Published 16 May 2019 Volume 2019:12 Pages 1561—1567
DOI https://doi.org/10.2147/JPR.S190158
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Katherine Hanlon
Lorenzo Panella,1 Giuseppe Rinonapoli,2 Stefano Coaccioli3
1Rehabilitation Department, ASST Pini-CTO, 20100 Milan, Italy; 2Dipartimento di Scienze Chirurgiche, s.c. Ortopedia e Traumatologia Università di Perugia. Ospedale S.Maria della Misericordia, 06100 Perugia, Italy; 3Department of Medicine, Sezione di Clinica Medica e Anatomia Patologia, 05100 Terni, Italy
Abstract: Chronic pain is a major health-care problem worldwide, affecting more than one out of five adults in Europe. Although multiple analgesic agents have been extensively investigated in terms of clinical response and tolerability profile, few studies have focused on the impact of these therapies on patients’ quality of life (QoL). Of note, improvement in QoL, together with functional recovery, has been recognized since the late 1990s as two main goals of analgesic therapy. Tapentadol is a novel analgesic molecule that synergistically combines two mechanisms of action, μ-opioid receptor agonism and norepinephrine reuptake inhibition, and for which multiple literature data are available that confirm its efficacy and safety in controlling pain. This narrative review summarizes the information available on the impact of tapentadol on QoL, with the aim to provide clinicians with a comprehensive overview of the analgesic effects of tapentadol prolonged release beyond the reduction of pain.
Keywords: pain, quality of life, tapentadol
Introduction
Chronic pain remains a major health-care problem worldwide, affecting more than one out of five adults in Europe.1 Clinical outcomes of pain therapy, including reduction of pain and adverse event profiles, have been extensively investigated for a variety of analgesic agents.2 However, the impact of different analgesic therapies on the quality of life (QoL) needs further investigation.3–5 Improvement in QoL and functional recovery is to be considered the main goal of analgesic therapies, although this has been recognized since the late 1990s.2,6 In this line, other outcomes, including functional recovery, maintenance of work productivity, and pharmacoeconomic considerations should be taken into account in the selection of analgesic therapy.7
Tapentadol is a dual μ‐opioid receptor (MOR) agonist and noradrenaline reuptake inhibitor (NRI), considered as the first and unique member of a new class of analgesic agents, namely MOR-NRI.8 The so-called “µ-load” of tapentadol is ≤40% relative to pure MOR agonists, thus resulting in a more favorable tolerability profile compared with strong opioids.9 Moreover, tapentadol shows minimal serotoninergic activity, with long-term safety advantages (eg, reduced emesis).10 The efficacy and safety of tapentadol, in its prolonged release (PR) formulation, have been evaluated in several pivotal trials and observational experiences, the presentation of which goes beyond the scopes of the present paper. Remarkably, tapentadol has been proposed to be different from classical opioids and may therefore represent an a priori choice for the treatment of chronic, neuropathic, and mixed pain.11 This concept has been strengthened and expanded to other drugs – eg, tramadol, buprenorphine, loperamide, cebranopanol – since current evidence shows that the inclusion of all analgesics that share the opioid mechanism of action into the same class is anachronistic and misleading. The recognition of subclasses of opioids may be highly beneficial to health-care providers, payers and regulators; to date, some definitions have been proposed such as atypical or multigesic.9,12
The impact of tapentadol on the QoL has been investigated in several studies, also specifically conducted to address this issue. Moreover, evidence is available on functional recovery with tapentadol. This narrative, non-systematic review addresses the above, with the aim to provide clinicians with an overview of what “follows” the analgesic efficacy of tapentadol PR.
Tapentadol and QoL: available evidence
Several studies have comprised, among their outcomes, the evaluation of QoL in patients with chronic pain treated with tapentadol PR.
In our opinion, three different pooled analyses are specifically worth mentioning.2,13,14 Moreover, another study specifically investigated QoL in patients treated with tapentadol.15 We have decided to focus on these papers since they were specifically designed to investigate QoL in tapentadol-treated patients with pain of non-oncological etiology. Table 1 summarizes the main studies on this topic, as described below.
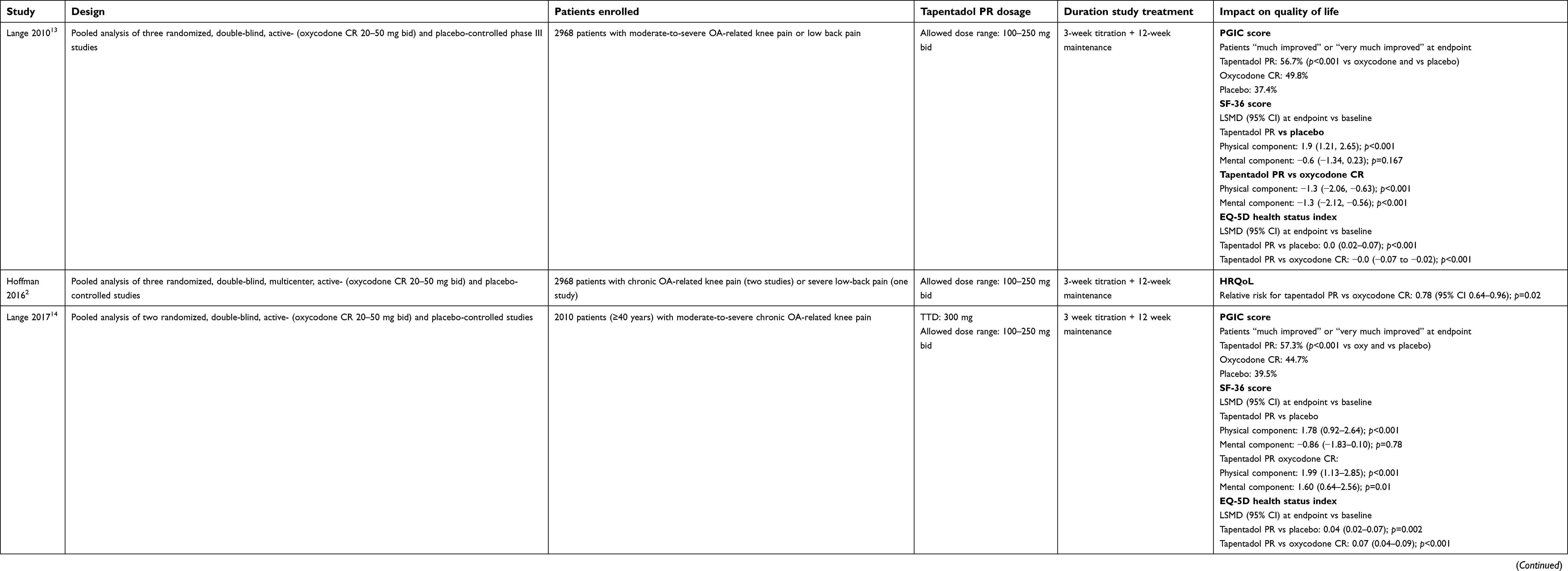 | Table 1 Key elements from studies on the impact of tapentadol prolonged release on patients’ quality of life in non-oncological patients |
In 2010, Lange et al, performed a pooled analysis of data from three Phase III randomized studies in patients with chronic osteoarthritis of the knee or low back pain, which evaluated tapentadol PR (100–250 twice daily) compared with placebo or oxycodone controlled release (CR; 20–50 mg twice daily).13 Data on QoL were collected using patient-reported outcomes, namely the patient global impression of change (PGIC), the Short Form-36 (SF-36) health survey,16 and the EuroQol 5-Dimension (EQ-5D) health survey.17 On the PGIC, patients rated their overall status on a scale from 1 to 7 (1=“ very much improved” to 7=“ very much worse”). The SF-36 evaluated patient health status in eight domains (physical functioning, role-physical, bodily pain, general health, vitality, social functioning, role-emotional, and mental health) on a scale from 0 to 100 (0=“poor health” to 100=“good health”) and two summary scales (the physical and mental component summaries). The EQ-5D health survey consisted of five dimensions (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression) rated by patients on a 3-point scale (1=“no problems”, 2=“some problems”, 3=“extreme problems”), an overall health state measure that was rated by patients on a 100 mm visual analog scale (VAS; 0=“worst imaginable health state” to 100=“best imaginable health state”), and a health status index, which calculated from the individual dimensions. On the PGIC, 56.7% treated with tapentadol PR (421/742) reported that their overall status was “much improved” or “very much improved” at endpoint, compared with 37.4% of patients in the placebo group (304/812) and 49.8% (310/622) of those in the oxycodone CR group. The advantage of tapentadol PR reached statistical significance compared with both controls (p<0.001). When the SF-36 questionnaire was evaluated, significant improvements from baseline to endpoint were observed with tapentadol PR compared with placebo in the physical functioning, role-physical, bodily pain and vitality scores (p<0.05 for all comparisons), and with oxycodone CR in all domains except general health. On the other hand, the results observed with oxycodone were similar, or even worse, to those reported with placebo. On the EQ-5D questionnaire, a greater improvement from baseline to endpoint was observed in the health status index score with tapentadol PR compared with placebo (LSMD vs placebo 0.0, 95% CI: 0.02–0.07; p<0.001), while the difference between oxycodone CR and placebo was not significant (−0.0, 95% CI: −0.02–0.02; p=0.867). A significantly greater improvement from baseline to endpoint in the health status index score was observed with tapentadol PR compared with oxycodone CR (LSMD between tapentadol PR and oxycodone CR −0.0, 95% CI: −0.07 to −0.02; p<0.001).
In 2016, Hofmann et al, performed a systematic comparison of three randomized trials on tapentadol PR and oxycodone CR in the treatment of chronic osteoarthritis pain (two studies) and severe low back pain (one study) using patient-relevant endpoints of efficacy, safety and health-related QoL (HRQoL).2 In total, 2,968 patients were evaluated (tapentadol PR: 978, oxycodone CR: 999, placebo arms: 991). QoL was assessed by PCIG and EQ-5D, using sophisticated methods derived from health-technology assessment. Overall, statistical analysis showed superior treatment effects of tapentadol PR in HRQoL compared with oxycodone CR and placebo (Figure 1). In addition, given the more evident efficacy and more favorable safety of tapentadol PR over oxycodone shown in the same analysis, the investigators concluded that it may be beneficial to initiate treatment of chronic severe nonmalignant pain with tapentadol PR rather than oxycodone.
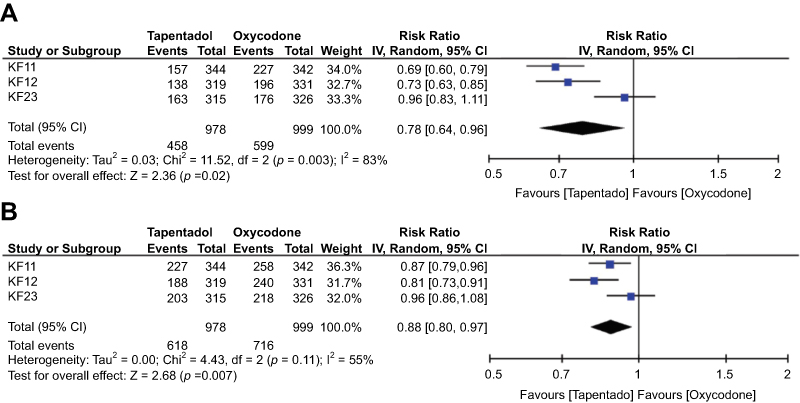 | Figure 1 Meta-analysis of treatment effects for the EQ-5D comparing tapentadol PR versus oxycodone CR (ITT population). (A) Responders were defined using the anchor-based minimal important difference (MID) (0.036). (B) Responders were defined using a distribution-based MID (0.154). Copyright © 2016. Prime National Publishing Corp. Reproduced from Hofmann JF, Lal A, Steffens M, Boettger R. Patient-relevant outcomes and health-related quality of life in patients with chronic, severe, noncancer pain treated with tapentadol prolonged release-using criteria of health technology assessment. J Opioid Manag. 2016;12(5):323–331.2 |
These findings were corroborated by those of another pooled analysis of two double-blind, randomized, placebo- and oxycodone CR-controlled studies in patients with moderate-to-severe chronic osteoarthritis knee pain.14 In total, 2010 patients were evaluated. At analysis of PGIC, more patients in the tapentadol PR group (57.3%) compared with oxycodone CR (44.7%) and placebo patients (39.5%) rated their overall health status at the end of treatment as “very much improved” or “much improved” (p<0.001 for tapentadol PR vs both oxycodone and placebo; no differences between oxycodone and placebo were reported).14 A significant advantage was also observed for tapentadol PR over oxycodone CR in terms of physical and mental SF-36 dimensions, while the mental component score significantly worsened with oxycodone treatment when compared with placebo. Increases in the weighted EQ-5D health status compared with baseline were reported in all groups but were highest for tapentadol PR (LS mean=0.04 [95% CI: 0.02–0.07] vs placebo and =0.07 [95% CI: 0.04–0.09]; p<0.001 vs oxycodone). The comparison between oxycodone and placebo was significantly in favor of placebo.
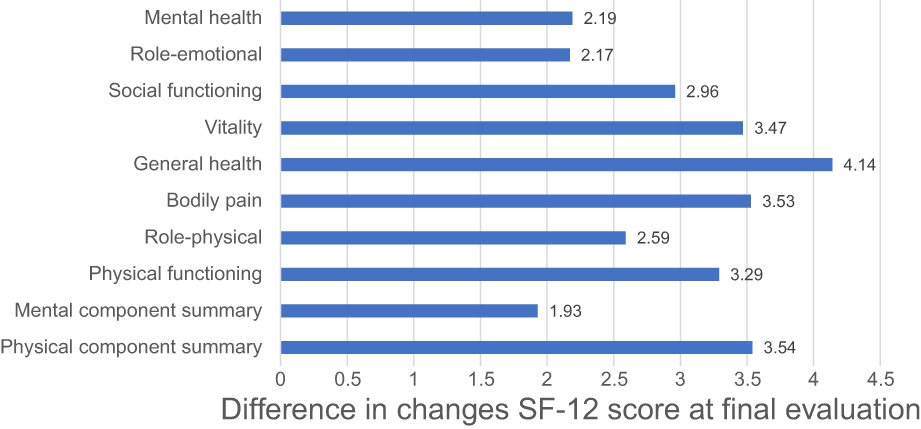 | Figure 2 Difference in changes in SF-12 score at final evaluation, as compared with baseline, in patients treated with either tapentadol PR (N=129) or oxycodone/naloxone PR (N=125). Difference is expressed as change in the tapentadol group (final evaluation-baseline)-change in the oxycodone/naloxone group. Data from Baron et al.15 |
In a randomized, controlled, open-label, Phase IIIb/IV trial, Baron et al, evaluated the QoL in opioid-naive patients with severe chronic low back pain with a neuropathic component treated with tapentadol PR (n=129) or oxycodone/naloxone PR (n=125) (Figure 2).15 QoL was assessed by the SF-12 and the EQ-5D questionnaires. Moreover, the Hospital Anxiety and Depression Scale (HADS) was used to evaluate symptoms of anxiety and depression.18 After 12-week treatment, significant improvements versus baseline were observed in the SF-12 total score and in all subdomains (p<0.001 vs baseline); in the oxycodone/naloxone PR group, significant improvements were observed only in the mean SF-12 physical component summary score and 7 SF-12 domain scores (all p≤0.012). Remarkably, significantly greater improvements from baseline to final evaluation were observed in the tapentadol PR group compared with the oxycodone/naloxone PR group for the mean physical component summary score and six domain scores (all p≤0.017). In addition, the EQ-5D health status improved in both groups, with a significant advantage for tapentadol over oxycodone/naloxone (p=0.010). Significant decreases from baseline to final evaluation were observed in the mean HADS anxiety and depression subscale scores in both treatment groups, with an advantage for tapentadol (p=0.032). These improvements in QoL were paralleled by an improvement in sleep quality: overall sleep quality was judged to be improved from baseline to final evaluation in 50.0% of patients in the tapentadol PR group and 37.7% of patients in the oxycodone/naloxone PR group.
Tapentadol and functional recovery
In the pooled analysis by Lange et al, which evaluated two double-blind, placebo- and oxycodone CR-controlled studies in patients with chronic osteoarthritis of the knee,15 pain, disability, and joint stiffness were assessed by the WOMAC questionnaire (Likert scale from 0 to 4 lower scores indicate lower levels of symptoms).19 Overall, there were no significant differences in mean changes from baseline to week 12 of the maintenance period in the WOMAC sub-scales and global scores between tapentadol PR and oxycodone CR (pain: −0.01, 95% CI: −0.13–0.12; physical functioning: −0.01, 95% CI: −0.13–0.12; stiffness: −0.05, 95% CI: −0.19–0.09; global score: 0.0, 95% CI: −0.12–0.12). However, tapentadol PR was significantly more effective than placebo in all four WOMAC scales, whereas a significant advantage for oxycodone versus placebo could not be shown for stiffness and the global WOMAC score.
Implications for clinical practice
Pain reduction remains the immediate outcome of analgesic therapy. However, in the last 20 years, mounting attention has been given to outcomes that go beyond the reduction of pain intensity, namely QoL and functional recovery. Indeed, a patient with reduced pain will likely experience an improvement of QoL and a recovery of the function of the affected area(s) in the case of musculoskeletal pain. Improved QoL and functionality will also turn into increased productivity of the patient – thus, further contributing to better QoL, in a vicious circle – and reduced need of other medical therapies, with a potential beneficial impact on the healthcare system. These improvements, however, may become less evident for some analgesic therapies, due to lack of efficacy or the onset of drug-associated adverse events.
Remarkably, despite its importance, the impact of different analgesic therapies on QoL and functional recovery has been poorly assessed to date,3–5 whereas these evaluations may greatly help clinicians in the selection of treatment.
The impact of tapentadol PR on QoL and functional recovery have been assessed in pooled analyses of randomized trials of non-oncological pain with oxycodone CR as a comparator. Overall, these well-grounded pieces of evidence consistently show that therapy with tapentadol PR does improve all dimensions of QoL, often with a significant advantage over oxycodone. Enhanced QoL is associated with more evident functional recovery and improved sleep quality. This beneficial action of tapentadol PR can likely be due to its peculiar pharmacological action, which is characterized also by a marked noradrenergic activity. Further studies on this topic are, however, also warranted in other settings. For instance, an explorative study in patients with cancer pain showed improvement of QoL with tapentadol PR,20 and additional evidence in this specific setting would be welcomed.
Some preliminary studies have also assessed whether the impact of tapentadol PR on QoL translates into improved productivity. In addition, a Bayesian Markov chain analysis showed that tapentadol was associated with less time missed from work, less impairment while working, and a lower overall loss in work productivity compared with oxycodone CR.21 In a pharmacoeconomy analysis, tapentadol PR showed more favorable results over oxycodone/naloxone, since in 65% of cases it was less costly and produced a considerable quality-adjusted life years gain.22 This more favorable cost-effectiveness was likely due to the price and the lower incidence of adverse events and related discontinuation rate, thus leading to a further economic advantage.
In conclusion, we believe that QoL and functional recovery should be better investigated in clinical trials on analgesic therapy. While results of dedicated studies appear awaited, current evidence specifically collected on tapentadol PR unequivocally shows its beneficial effect on QoL and functionality, thus contributing to a comprehensive recovery of the patient, and not only to pain reduction.
Key points
- Different analgesic therapies provide a reduction of pain and a good safety profile in the treatment of chronic pain, a condition that still represents a major health-care problem worldwide.
- In the last decades, quality of life (QoL) and functional recovery have emerged as two important goals of analgesic therapy; however, only few studies have investigated these aspects.
- Some pooled analyses have assessed the impact of tapentadol prolonged release (PR), a novel analgesic molecule acting on both µ-opioid receptor (MOR) agonism and norepinephrine reuptake inhibition (NRI), on QoL and functional recovery in patients with chronic pain related to knee osteoarthritis or low back pain.
- Literature data consistently show that tapentadol PR is associated with improvements in all dimensions of QoL (with superior results if compared with oxycodone CR), which in turns exerts a positive effect on functional recovery and sleep quality.
- Based on preliminary studies, tapentadol PR may have a positive impact also on patient’s productivity.
Acknowledgments
Editorial assistance was provided by Luca Giacomelli, Ph.D., Ambra Corti, and Aashni Shah. This assistance and fees for publications were supported by Grunenthal.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Breivik H, Collett B, Ventafridda V, et al. Survey of chronic pain in Europe: prevalence, impact on daily life, and treatment. Eur J Pain Lond Engl. 2006;10(4):287–333. doi:10.1016/j.ejpain.2005.06.009
2. Hofmann JF, Lal A, Steffens M, Boettger R. Patient-relevant outcomes and health-related quality of life in patients with chronic, severe, noncancer pain treated with tapentadol prolonged release-using criteria of health technology assessment. J Opioid Manag. 2016;12(5):323–331. doi:10.5055/jom.2016.0349
3. Devulder J, Richarz U, Nataraja SH. Impact of long-term use of opioids on quality of life in patients with chronic, non-malignant pain. Curr Med Res Opin. 2005;21(10):1555–1568. doi:10.1185/030079905X65321
4. Noble M, Treadwell JR, Tregear SJ, et al. Long-term opioid management for chronic noncancer pain. Cochrane Database Syst Rev. 2010;(1):CD006605.
5. Whittle SL, Richards BL, Husni E, et al. Opioid therapy for treating rheumatoid arthritis pain. Cochrane Database Syst Rev. 2011;(11):CD003113.
6.
7. Stanos S, Brodsky M, Argoff C, et al. Rethinking chronic pain in a primary care setting. Postgrad Med. 2016;128(5):502–515. doi:10.1080/00325481.2016.1188319
8. Kress HG. Tapentadol and its two mechanisms of action: is there a new pharmacological class of centrally-acting analgesics on the horizon? Eur J Pain. 2010;14(8):781–783. doi:10.1016/j.ejpain.2010.06.017
9. Raffa RB, Elling C, Tzschentke TM. Does ‘strong analgesic’ equal ‘strong opioid’? Tapentadol and the concept of ‘µ-load’. Adv Ther. 2018;35:1471–1484. doi:10.1007/s12325-018-0778-x
10. Tzschentke TM, Folgering JH, Flik G, De Vry J. Tapentadol increases levels of noradrenaline in the rat spinal cord as measured by in vivo microdialysis. Neurosci Lett. 2012;507(2):151–155. doi:10.1016/j.neulet.2011.12.008
11. Langford RM, Knaggs R, Farquhar-Smith P, Dickenson AH. Is tapentadol different from classical opioids? A review of the evidence. Br J Pain. 2016;10(4):217–221. doi:10.1177/2049463716657363
12. Pergolizzi JV
13. Lange B, Kuperwasser B, Okamoto A, et al. Efficacy and safety of tapentadol prolonged release for chronic osteoarthritis pain and low back pain. Adv Ther. 2010;27(6):381–399. doi:10.1007/s12325-010-0036-3
14. Lange B, von Zabern D1, Elling C1, Dubois C1. Efficacy and safety of tapentadol prolonged release for moderate-to-severe chronic osteoarthritis knee pain: a pooled analysis of two double-blind, randomized, placebo- and oxycodone controlled release-controlled studies. Curr Med Res Opin. 2017;33(8):1413–1422. doi:10.1080/03007995.2017.1335188
15. Baron R, Jansen JP, Binder A, et al. Tolerability, safety, and quality of life with tapentadol prolonged release (PR) compared with oxycodone/naloxone pr in patients with severe chronic low back pain with a neuropathic component: a randomized, controlled, open-label, phase 3b/4 trial. Pain Pract. 2016;16(5):600–619. doi:10.1111/papr.12361
16. Ware JE
17.
18. Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J Psychosom Res. 2002;52:69–77. doi:10.1016/S0022-3999(01)00296-3
19. Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW. Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol. 1988;15:1833–1840.
20. Mercadante S, Porzio G, Ferrera P, et al. Tapentadol in cancer pain management: a prospective open-label study. Curr Med Res Opin. 2012;28(11):1775–1779. doi:10.1185/03007995.2012.739151
21. Cepeda MS, Sutton A, Weinstein R, Kim M. Effect of tapentadol extended release on productivity: results from an analysis combining evidence from multiple sources. Clin J Pain. 2012;28(1):8–13. doi:10.1097/AJP.0b013e3182201983
22. Coluzzi F, Ruggeri M. Clinical and economic evaluation of tapentadol extended release and oxycodone/naloxone extended release in comparison with controlled release oxycodone in musculoskeletal pain. Curr Med Res Opin. 2014;30(6):1139–1151. doi:10.1185/03007995.2014.894501
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.