")
Back to Journals » Orthopedic Research and Reviews » Volume 14
Where are We Now and What are We Hoping to Achieve with Robotic Total Knee Arthroplasty? A Critical Analysis of the Current Knowledge and Future Perspectives
Authors Mancino F , Jones CW , Benazzo F, Singlitico A, Giuliani A, De Martino I
Received 19 June 2022
Accepted for publication 29 September 2022
Published 17 October 2022 Volume 2022:14 Pages 339—349
DOI https://doi.org/10.2147/ORR.S294369
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Clark Hung
Fabio Mancino,1 Christopher W Jones,1,2 Francesco Benazzo,3,4 Alessandro Singlitico,5 Alessandro Giuliani,5 Ivan De Martino5,6
1Department of Orthopaedics, The Orthopaedic Research Foundation of Western Australia (ORFWA), Fiona Stanley Hospital, Perth, Western Australia, Australia; 2Curtin University, Perth, Western Australia, Australia; 3Sezione di Chirurgia Protesica ad Indirizzo Robotico, Unità di Traumatologia dello Sport, Fondazione Poliambulanza, Brescia, Italy; 4IUSS, Istituto di Studi Superiori, Pavia, Italy; 5Università Cattolica del Sacro Cuore, Roma, Italy; 6Unità di Ortopedia e Traumatologia, Dipartimento di Scienze dell’Invecchiamento, Neurologiche, Ortopediche e della Testa-Collo, Fondazione Policlinico Universitario Agostino Gemelli IRCCS, Roma, Italy
Correspondence: Ivan De Martino, Unità di Ortopedia e Traumatologia, Dipartimento di Scienze dell’Invecchiamento, Neurologiche, Ortopediche e della Testa-Collo, Fondazione Policlinico Universitario Agostino Gemelli IRCCS, Largo A. Gemelli 8, Roma, 00168, Italy, Tel +39 3512412491, Email [email protected]; [email protected]
Abstract: Robotic-assisted total knee arthroplasty (rTKA) has been developed to improve knee kinematics and functional outcomes, expedite recovery, and improve implants long-term survivorship. Robotic devices are classified into active, semi-active, and passive, based on their degree of freedom. Their capacity to provide increased accuracy in implants positioning with reduced radiographic outliers has been widely proved. However, these early advantages are yet to be associated with long-term survivorship. Moreover, multiple drawbacks are still encountered including a variable learning curve, increased setup and maintenance costs, and potential complications related to the surgical technique. Despite recent technologies applied to TKA have failed to prove substantial improvements, robotic-assisted surgery seems to be here to stay and revolutionize the field of TKA. To support its consistent usage on a daily basis, long-term results are still awaited, and further improvements are necessary to reduce the expenses related to it.
Keywords: robotic total knee arthroplasty, knee alignment, accuracy, robot, survivorship, clinical outcomes
Introduction
Even if the results of total joint arthroplasty (TJA) are amongst the greatest of modern surgery, the orthopaedic community is continuously looking for further innovations to reduce failure rates and increase patient satisfaction. With a survivorship at 10 years up to 98% and at 20 years up to 95%, the risk of failure is equaled to the chance of improvement.1,2 Indeed, many innovations introduced in the last 20 years have failed to achieve the expected improvements. As the level of technology increases hoping to lead to radiographic and clinical perfection, supporters of the conventional manual technique (mTKA) may say that today’s innovation is more driven by economic interests rather than by objective results.3 Big hopes are certainly riding on robotic total knee arthroplasty (rTKA), aiming to expedite recovery, improve kinematics and functional outcomes, and eventually increase implants long-term survivorship. The main goal of robotic-assisted surgery is to provide the technological support to precisely and accurately prepare the bone, making the ligaments as competent as before osteoarthritic changes, and restoring the limb alignment with a proper kinematic of the joint.
Despite being a topic already thoroughly studied with an exhaustive literature available, the authors wanted to focus on aspects not yet extensively analyzed, especially when talking about the drawbacks of rTJA. Therefore, the aim of this review is not only to highlight the different types of robotic devices available on the market for TKA and to report on their improved results in terms of increased accuracy and reduced radiographic outliers. But also, to report as these advantages come at a cost, including higher economic burden for the health systems, longer operative time (OR), learning curve for the surgeon and the team, and potential complications related to the technique.
Type of Robots
Robotic devices are classified according to the degree of freedom during the surgical procedure in autonomous (active), hands-on (semi-active) and passive. The passive systems are known as computer-assisted or navigation systems and do not perform independently the operation while providing the correct positioning for the cutting tool. Conversely, active robots hold the cutting tool and autonomously make the bone cuts reducing the level of human interaction. Lastly, semi-active robots combine both principles, the surgeon maintains the overall control over the bone resections under the surveillance of the robot that provides live intraoperative feedback with tactile, auditory, or visual signals, to limit deviation from the preoperative surgical plan. These systems are also known as “haptic” systems.4,5
In the last years, robotic surgery has gained increased interest and applications, driving the main companies to introduce these devices into their portfolio. Therefore, the level of quality, competitiveness, technology available, together with the amount of literature and publications, have risen at a fast pace.6 Robots can either be classified into open or closed platforms based on the possibility to have no limit on the pool of prosthesis models that can be used. Conversely, the latter forces to use only specific manufacturer’s implant designs, regardless of surgeon’s preference and patient’s needs. Further classification of robots is “image-based” or “image-less”. The former relies on preoperative second-level imaging to establish a preoperative plan, integrated intraoperatively with bony landmark registration. On the other hand, the image-less platforms are based on the direct registration of specific bony landmarks directly on the patient’s bone surface after exposure. Once registered, these landmarks are used to plan the surgical cuts intraoperatively.
The ROBODOC system (Curexo Technology, Fremont, CA, USA) was the first robotic device introduced in TJA in 1994 in Europe. It was an active system initially used for preparing the femur in total hip arthroplasty (THA). In 2014, THINK Surgical Inc (former Curexo Technology) introduced a new version for TKA named TSolution One surgical system. It is an image-based autonomous milling system characterized by being an open platform with an open library of legally available implants suitable for usage with this robotic device.7–11
The MAKO Robotic Arm Interactive Orthopaedic system (RIO; former MAKO Surgical Corp.®, FL, USA; now Stryker Ltd, Kalamazoo, MI, USA), firstly used in 2015 and now the most used robotic device. It is an image-guided semiactive robot system that requires a preoperative CT scan to generate a 3D model of the patient’s bone morphology. Then, the plan can be modified intraoperatively with data collected during the operation and the knee is brought through range of motion to assess deformity and ligament laxity.12
The NAVIO Surgical System (former Blue Belt Technologies; now Smith & Nephew, Andover, TX, USA), is an imageless robotic system that relies on haptic feedback equipped with a handheld end-cutting burr that can extend and retract during the procedure so that only the planned bone is removed. The system monitors the position of the burring tool with respect to the patient’s lower extremity, and when the edge of the desired bone resection volume is approached, the burr tip retracts to avoid over-resection.13 The recently introduced CORI surgical system (Smith & Nephew) is an imageless portable robotic system for use in TKA and unicompartmental knee arthroplasty (UKA) that has been developed to operate within a smaller footprint than earlier generations of robotic systems. Its efficiency in workflow has been improved through the adoption of high-speed cameras and high-speed burrs to increase the speed of surgical navigation and the rate of bone removal.
The ROSA® Knee System (Zimmer-Biomet, Warsaw, IN, USA) is a collaborative robot that can be used in image-based or image-less mode. After bony landmarks are recorded and intraoperative plan is validated, this system enables the surgeon to personalize in real time the surgical plan based on each patient’s individual characteristics and ligament compliance. The cutting jigs are positioned and hold by the robot (collaborative robotic system, a.k.a. cobot), while the surgeon performs the bone cuts through the slot, with no boundary protection.14
Orthotaxy (Johnson & Johnson, Fort Washington, PA, USA) is an image-less semi-active device characterized by being a small-size platform attached to the operating table and interestingly it is expected to drop the costs avoiding the use of disposable instruments and being designed to be used without the assistance of additional technicians.15 As another option, VELYS (DePuy Synthes, West Chester, PA, USA) was introduced in 2020 as an image-free operating room table bed-rail mounted device that allows intraoperative plan based on registration of specific bony landmarks and once accepted, positions an oscillating saw for the surgeon to perform the bone cuts with real-time cut-plane tracking to compensate for any leg movement.
OMNIBotics (OMNIlife Science Inc, East Taunton, MA, USA) is an imageless system characterized by a ligament balancing component (BalanceBot) used to measure ligament tension in both extension, flexion, and throughout the range of motion aiming to reduce the risk of mid-flexion instability. A single cutting guide is then positioned for each of the cuts to allow the surgeon to perform the bone resections.16,17
Other robotic devices are currently available with different characteristics as the commercial companies are trying to improve the technology levels and provide increased accuracy while providing a functional workflow and limited costs (Table 1).
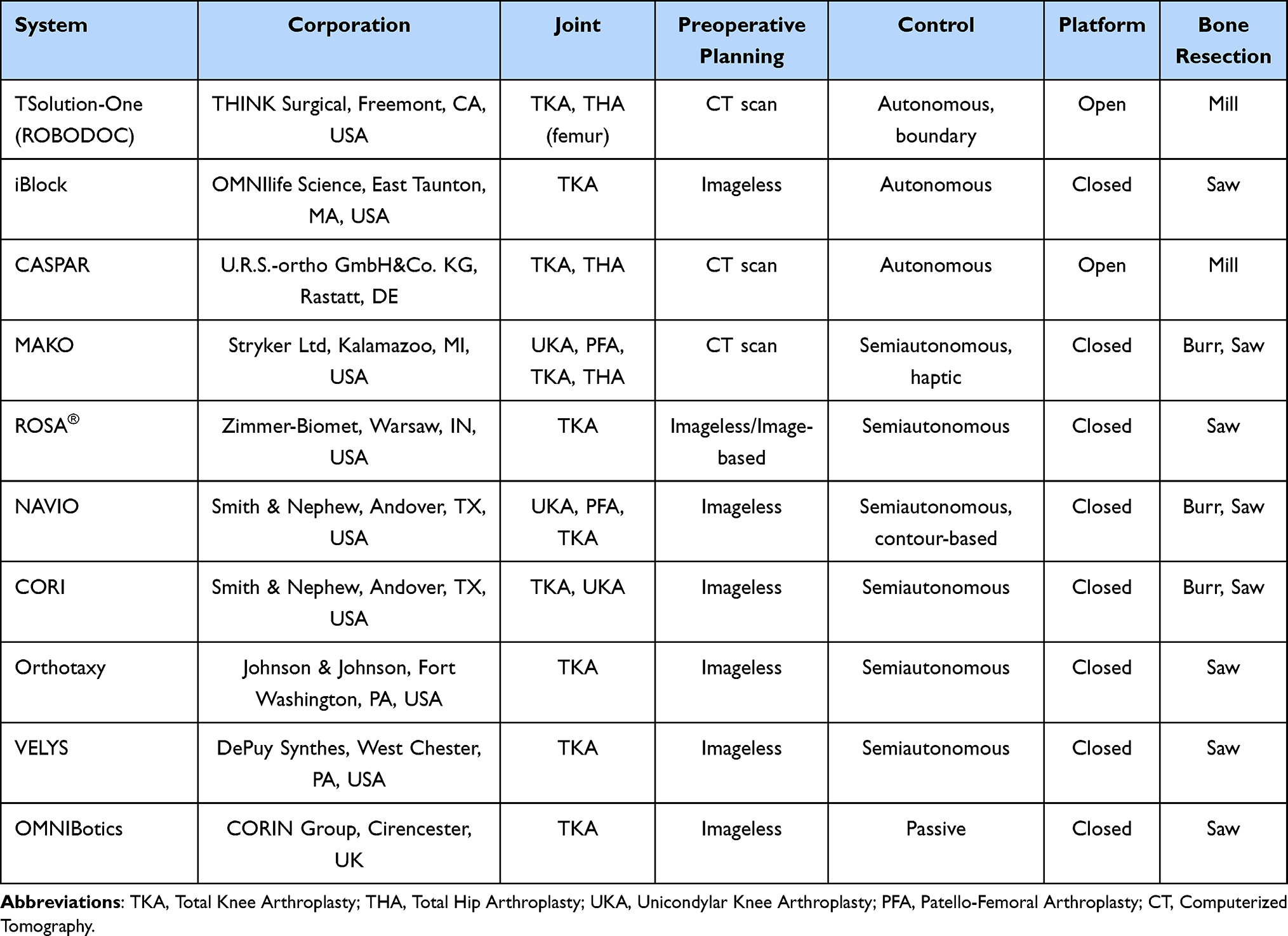 |
Table 1 Systems Available and Main Characteristics |
Advantages of Robotic-Assisted Technique
Accuracy and Radiographic Outliers
Accuracy and precision are two key concepts in TKA as the surgeon seeks to accurately position the implant components to produce a balanced and stable joint. Accuracy is usually intended as the ability to hit a planned target, while precision is the ability to reproduce the same result repeatedly over time. Robotic-assisted technique has proven reliable in improving the accuracy for component positioning and limb alignment compared to the conventional manual technique.7–9,11,12,14,16–26 Despite different alignment philosophies have been recently proposed, mechanical alignment (MA) remains the most frequently adopted and still considered the “safe-zone”.27 Target for MA have been typically considered within a cut-off of 2–3° from the neutral MA in the coronal plane, while errors >3° have been usually considered as radiographic outliers.28 However, the greater accuracy of robotic devices may be important as new alignment principles and new objectives for component positioning are developed to further individualize TKA (Table 2).
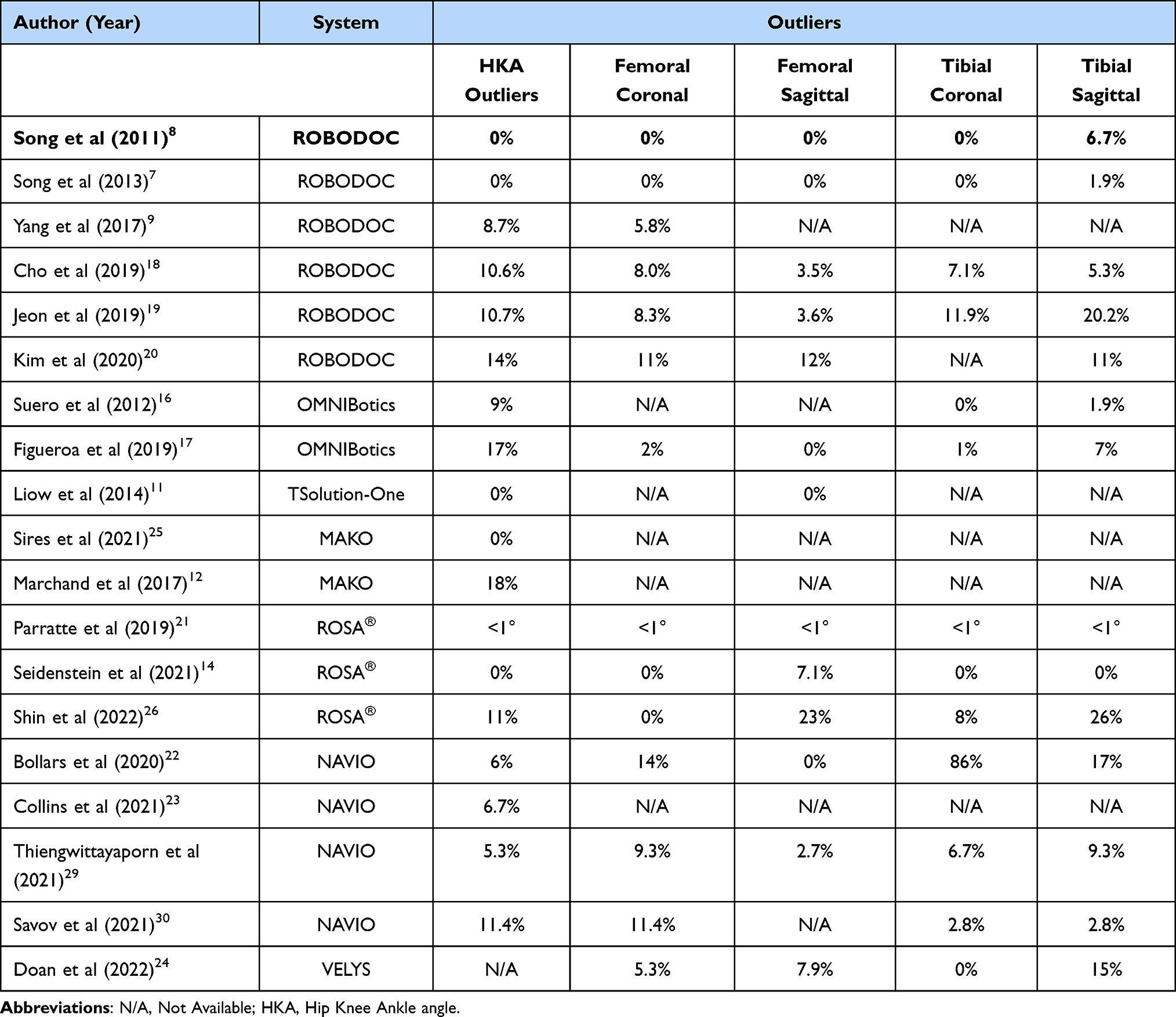 |
Table 2 Accuracy When Considering as Outliers Implant Aligned Out of ± 3 Degrees from Target Angle |
Thiengwittayaporn et al29 reported in a randomized controlled trial (RCT) on robotic vs manual TKA (NAVIO) that rTKA group was associated with higher accuracy with 94.7% (71 of 75 knees) of patients achieving an overall mechanical alignment within ±3° of a neutral mechanical axis compared with 84.4% (65 out of 77 knees, p = 0.035) in the conventional group. Moreover, the mean change in joint line was 3.6 mm in the rTKA group compared with 5.5 mm in the conventional (p = 0.004). Similarly, Liow et al11 reported that rTKAs were associated with a more accurate restoration of the joint line with only 3.2% of outliers (defined as >5 mm deviation) compared to a 20.6% in the conventional group. Savov et al30 reported an overall incidence of 11% outliers (8 cases out of 70; p = 0.002) when comparing NAVIO assisted TKA with conventional technique with a mean error from planned of 2±1.2° regarding HKA (p < 0.001), 1±0.8° regarding medial proximal tibial angle (MPTA, p = 0.002), 1.6±1.3° regarding lateral distal femoral angle (LDFA, p = 0.014), and 1.4±1.3° regarding posterior tibial slope (p = 0.038). The mean distalization values for the medial and lateral sides of the joint line (JL) in the valgus morphotype subgroup were approximately 2.6±1.6 mm and 3.7±1.8 mm, respectively; in the varus morphotype subgroup, the respective values were 0.9±1.7 mm and 1.9±2.3 mm while the JL was proximalized in the conventional cases. Clearly, the less change in joint line may contribute to a reduced incidence of knee instability and improved clinical outcomes for patients undergoing rTKA. On the other hand, Shin et al26 reported an accuracy of 77 and 74% when analyzing the sagittal femoral and tibial component alignment measured intraoperatively by the ROSA® knee system compared with the radiographic outcomes using a cutoff error of ±3°. However, high accuracy was noted when considering the HKA angle and the coronal components’ alignment.
Despite most of the studies reported results on the accuracy of component positioning based on the number of radiographic outliers, considering a cutoff of ±3°, Deckey et al,31 confirmed the increased accuracy of MAKO-assisted TKA compared to conventional technique proving that postoperative femoral and tibial components positioning, apart from overall alignment, deviated significantly less from the preoperative plan (p < 0.001) and that polyethylene thickness deviated less from planned in the robotic group (1.4 mm vs 2.7 mm; p < 0.001). These findings suggest that rTKA is significantly more accurate and precise in planning both components positioning and final polyethylene insert thickness.
Statistically significant improvements in accuracy and precision have been proven in these and other studies, however, questions remain that need to be answered. Indeed, increased accuracy and precision have to be proven effective in providing improved clinical outcomes and patient satisfaction. Therefore, future investigations are required to determine the potential effect of increased accuracy and precision on clinical outcomes.
Drawbacks of Robotic-Assisted Technique
Learning Curve
Increased operative time (OR) is considered one of the main problems related to robotic-assisted surgery as it is associated with potential increased complications and with additional costs. Different results have been reported in literature with a wide range of cases considered necessary for a proper learning phase, ranging from 7 to 43 cases.32,33 Kayani et al32 evaluated the learning curve in the haptic guided MAKO robotic-arm system reporting that robotic-assisted TKA was associated with a learning curve of seven cases to achieve OR times comparable with mTKA and “surgical team comfort” levels using a cumulative summation analysis but there was no learning curve for accuracy of implant positioning, limb alignment, posterior condylar offset ratio, posterior tibial slope, and joint line preservation. Conversely, a learning curve of 11–43 cases was reported by Vermue et al,33 over 386 patients for OR time (p < 0.001) using the same robotic device, however this was significantly affected by the surgical profile, while no learning curve was detected for implant positioning and gap balancing. On the other hand, Vanlommel et al34 reported a learning curve of 6–11 cases when using the imageless ROSA® Knee System. As both the systems use an optically guided robotic-arm, it therefore seems reasonable that the learning curves should approximate each other. However, when analyzing the differences between the two devices, the ROSA® Knee System showed a reduced initial setup time (8.9±1.9 min vs 14±4.3 min) and registration times. Conversely, bone preparation and implant trialing seemed to be longer with the ROSA® Knee System, probably related to the fact that being imageless free of preoperative planning, additional time was necessary intraoperatively to determine bone cuts, components position and size.
The learning curve of another imageless device, the NAVIO® system, was reported in a RCT by Thiengwittayaporn et al over 150 TKAs.29 The authors noted that the mean operative time of the rTKA group was significantly longer than the conventional one (70.1 min vs 61.9 min; p < 0.001) with bigger difference when comparing the first 10 robotic cases (95.0 min vs 61.9 min; p < 0.001). Conversely, no significant difference was detected when the last 10 cases were analyzed, despite being the rTKA procedures still slightly longer. However, their analysis revealed an inflection point after the initial seven cases, identifying an initial learning stage with mean 100 min per case and a proficiency stage with mean 67 min per case (p < 0.001). The learning curve associated with the same robotic system (NAVIO) was analyzed by Savov et al,30 on two groups of 70 consecutive patients operated with robotic and conventional technique, respectively. The authors reported that no significant difference was observed between the two techniques after 11 cases (69 min rTKA vs 67 min; p = 0.5). Conversely, Bell et al35 reported that 29 cases were necessary for a fellowship-trained senior surgeon to complete the learning curve using the NAVIO robotic system. The authors reported an overall 26% increase of efficiency throughout the learning curve mostly related to the so-called “review of intraoperative plan” phase, where the surgeon reviewed the cut suggested by the robotic system.
Similar findings were noted by Mahure et al36 in a multi-centre prospective study of over 115 patients with the TSolution One device. The authors reported a learning curve of 10–20 cases regarding OR time, while there was no learning curve associated with 3D component position or patient-reported outcome measures (PROMs). However, most of the studies on this topic have explored it with regard to fellowship-trained surgeons. To evaluate what that would be in general orthopaedic surgeons, Ali et al37 reported the learning curve of two non-fellowship-trained orthopaedic surgeons noting that it would require 40 cases, meaning that a non-fellowship-trained surgeon should be able to adequately perform a rTKA in a similar timeframe to mTKA within the first 40 cases (Table 3).
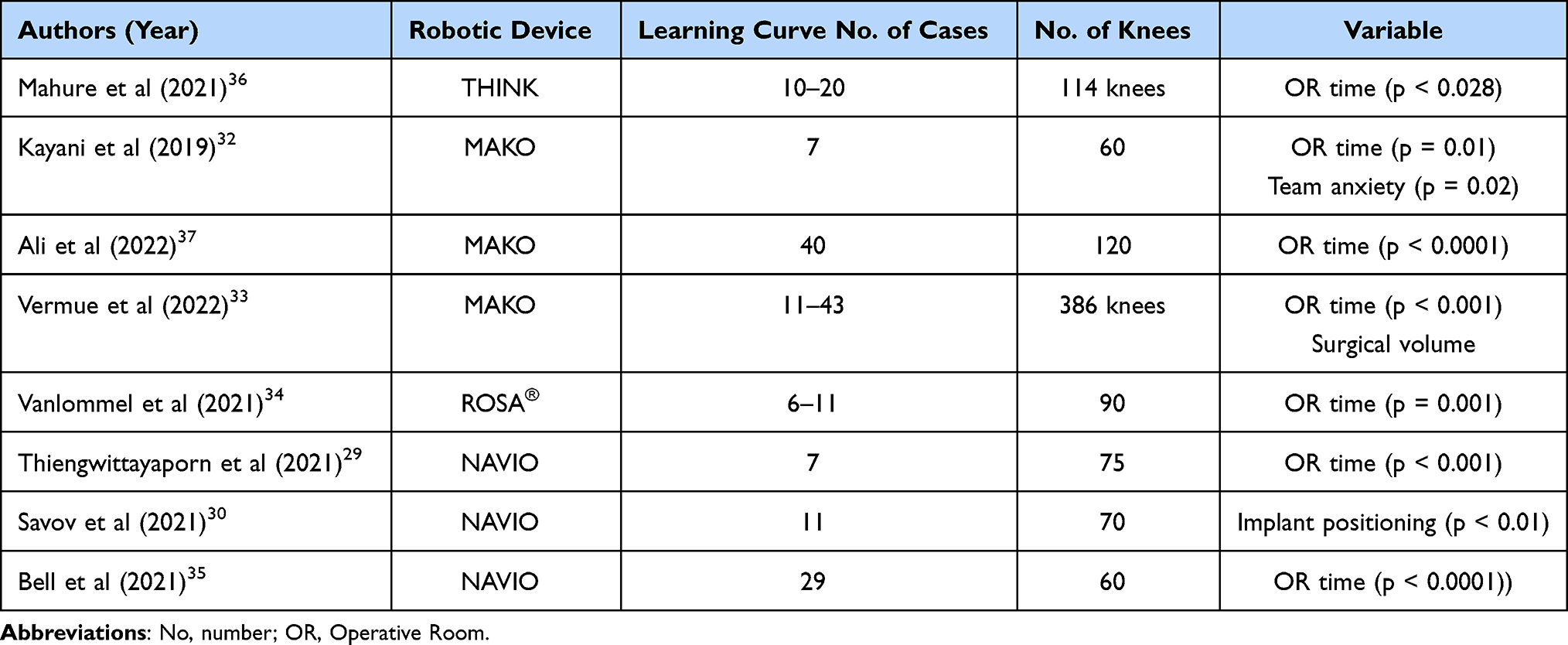 |
Table 3 Learning Curve of Different Robotic Systems |
Cost Effectiveness Analysis
Robotic systems are associated with high costs including the base system, operational costs, disposables, and pre-operative imaging with an estimated initial start-up cost of approximately US$ 800,000 and recurring cost of $ 1500 per patient to implement and carry out surgical procedures and with disposable costing approximately between $ 750 and $ 1300.10,38 Moreover, when image-based systems are used, preoperative imaging costs start from $ 260 and the annual maintenance costs for most robotic systems are between $ 40,000 and $ 150,000 and additional costs are required for the proper training of the surgical team.39
Moschetti et al39 reported that the robotic UKA system can be considered cost-effective in a high-volume setting of 100 cases annually, being case volume the most important determinant to the cost-effectiveness of the robotic system at the $ 50,000 willingness-to-pay (WTP) threshold, the most commonly used threshold used in the literature. However, the authors also suggest that robotic-assisted UKA must achieve a lower revision rate than traditional UKA for it to be cost-effective, even in high-volume centers. Similar results were reported by Vermue et al,40 reporting the number of annual cases necessary for rTKA to be theoretically cost-effective as 253 per year. Similarly, Cool et al41 utilized a large Medicare database to compare a short-term 90-day episode-of-care (EOC) costs between matched rTKA and mTKA patients operated between 1 January 2016 and 31 March 2017 including index costs, length-of-stay (LOS), discharge dispositions, and readmission rates. The authors reported that that rTKA patients had statistically significantly lower 90-day EOC costs (US$ 18,568 vs US$ 20,960; p < 0.0001) considering lower facility index costs, shorter LOS, higher likelihood that rTKA patients were discharged home (rTKA 57% vs mTKA 47%; p < 0.0001) and were less likely to be discharged to skilled nursing facility (SNF, rTKA 12% vs mTKA 22%; p < 0.0001), as well as having lower readmission rates.
By contrast to the limited 30- and 90-day EOC periods, the Markov model-based evaluation proposed by Rajan et al42 projected patient costs and outcomes over a lifetime and considered PROMs, and the potential future risk of arthroplasty revision. The authors reported that, despite improved PROMs and lower revision rates, rTKA is associated with higher capital equipment and surgical costs. As such, with incremental cost-effectiveness ratios (ICERs) of $ 15,685 and $ 2331/quality-adjusted-life (QALY) being less than the $ 50,000 and $ 100,000 WTPs, rTKAs were cost-effective for mid- and high-volume institutions, respectively. The authors used a comprehensive review of studies to determine optimal Quality of Life (QOL) values for a conventional TKA, estimated at 0.82 at 1 year and 0.84 thereafter. Therefore, rTKA remained cost-effective for a mid-volume institution as long as their annual revision rates were kept below 1.6% and the quality-of-life values were greater than 0.84, otherwise shifting the results in favor of mTKA.
Steffens et al43 compared the in-hospital costs between MAKO-assisted and computer-navigated TKA (nTKA) between October 2018 and June 2019 and reported that, when the upfront surgical equipment and maintenance costs were included to the in-hospital cost, rTKA was significantly more expensive than nTKA (+US$ 2359, CI95% 4359 to 656; p = 0.007). However, the authors affirmed that this was partly dependent on the relatively smaller number of cases performed with this technology during the study period and the per-case calculation method used.
Despite the promising results from projections model related with fewer readmission rates, shorter LOS, and less utilization of nursing services after discharge, robotic technology still has to prove its long-term efficacy in terms of PROMs and survivorship. Moreover, the volume of procedures remains a clear factor in determining the cost effectiveness of these devices. In order to establish rTKA as a daily standard of care baseline costs need to be reduced to avoid the results to be biased by the fact that only experienced/high volume surgeons or surgeons with potential conflict of interests are able to afford this interesting technology.
Complications Robot-Related
Despite being unusual, several complications have been associated with robotic-assisted technique including superficial pin site infections, pin-track osteomyelitis, pin-track site stress fracture, vascular injury, hematoma, myositis ossificans, and even mechanical failures related to pin-use. In order to reduce the risk of fractures at pin sites, Baek et al44 reported success on using unicortical pins in MAKO assisted TKA with 0 cases (out of 81 TKAs) of pin-related complications at 1-year follow-up. Thomas et al45 recently reported that the overall pin site complication rate was 1.4% over 7336 knees (range, 0.3% to 8%), with intraoperative and postoperative complications occurring at 1.4% and 1.1%, respectively. The most common intraoperative complications reported were pin dislodgement, breakage or loosening, eventually leading to abortion of the robotic technique in favor of the manual one (up to 40% of all intraoperative complications). On the other hand, among the postoperative complications, the most common were superficial infection, cellulitis, and pin site irritation in up to 83% of them. Moreover, the consequences may result in the need for secondary surgeries and increased EOC costs, increasing the notable economic burden related with this procedure.
Discussion
Robotic assistance in TKA was introduced to improve precision and accuracy, aiming at better outcomes, lower revision rates, and better patients’ satisfaction. Despite being considered still in its early phases, there are clearly some limitations with the available systems that need to be addressed to support definitive widespread and daily adoption of this technology.
Many authors have shown the increased costs related to robotic TKA including the initial capital investment, the yearly maintenance, and the per-case costs.4,40 Others have thoroughly described different learning curves with additional OR time required to correctly complete the surgical procedure.33 Both these downsides seem to be closely related to the volume-load and the experience of the surgeon and the surgical team, while none of the outcomes are affected during the learning curve, providing consistent results in terms of accuracy and precision to the preoperative plan since the very first cases. However, the more time-consuming procedure, associated with subsequent increased costs and reduced time-efficiency, limits the possibility of less experienced surgeons to adopt these platforms into their practice. Moreover, this technique is potentially associated with additional complications related to the longer OR-times and the tracker pins such as infection and fractures.5,45,46 Furthermore, despite the promising preliminary results, most of the available literature comparing robotic-assisted and conventional techniques in THA, TKA and UKA, involve financially conflicted authors; therefore, someone may consider the results to be biased. To further clarify the effects of robotic assistance, additional studies free from conflict of interests (COI) may be necessary to provide objective unbiased results.47
On the other hand, the benefits of rTKA include improved radiographic alignment and increased accuracy of component positioning and targeted alignment when compared with mTKA, among all the robotic platforms evaluated.48 Despite this was not believed to be clinically relevant until recently, it has now become apparent that component positioning has an important influence at least on short-term clinical outcomes.49 Indeed, several studies have reported on short-term improved functional outcomes, soft-tissue protection, patient satisfaction, and less surgeon and surgical team fatigue when comparing rTKA with conventional technique.50–52 However, further results to prove the effects on implant survivorship are still required.53 It is worth noticing that rTKA has proven increased accuracy in component positioning and soft tissue balance, however, whether this will be the holy grail in TKA there remains the question. Soft tissue and ligaments intraoperative evaluation still requires improvements considering that the systems available measure the kinematic response of the joint during application of set forces to restore the natural soft tissue tension avoiding soft tissue releases. However, joint loading is not standardized, leading to potential misinterpretation of the reported data.
In the compulsory search for novel devices and techniques, driven by the hope to solve the mystery of dissatisfaction after TKA and make the procedure as successful as THA, technologies are improving at a fast pace. Despite more than one has failed in the last 20 years, robotic-assisted TKA seems to be here to stay as more and more surgeons are willing to adopt this technology in their clinical practice. As clearly shown, the number of publications on robotic-assisted techniques experienced a high rise during the last decade and maintained interest year by year.54 Moreover, to further support that, the number of robotically-assisted procedures remains stable without facing any real decline and the wide implementation of robotic surgery will promptly provide additional data to better understand its applications and clinical outcomes. In the meanwhile, Artificial Intelligence (IA) is rapidly growing, and the first clinical studies have reported promising results when used in total joint arthroplasty.55 Modern robotic devices will continue to evolve eventually integrating Augmented Reality (AR) to visualize 3D images and use intra-operatively 3D planning through portable head mounted glasses avoiding the necessity to look at the screen.
Clearly, it is not a simple job to effectively define what the future perspectives and applications of robotic TKA will be. This is for several reasons: firstly, as most technologies available in 2022, its evolution is extremely fast with new designs, software, applications and updates being developed every year, putting a hard pressure on health systems to keep up with such innovations without being externally funded or financed. Secondly, these devices are currently strongly supported after promising short-term results obtained throughout the whole range of different machines. However, strong mid-term outcomes are available mainly for MAKO robotic system, while 5-year mark results are mostly still pending. Moreover, the enthusiasm over rTKA could diminish if the 10-years survivorship and patients’ satisfaction will not show the expected and hoped improvements compared with the conventional technique, as some authors have already reported with the old robotic systems.18 Moreover, the significancy of such improvements is still not clear if we are to expect higher survivorship rather than improved outcomes and patients’ satisfaction, or just more “aligned” knees. Thirdly, as previously reported, the big contradiction of rTKA is that it is mainly used by high volume – highly experienced orthopaedic surgeons with a sufficient caseload to provide publishable results, despite often reporting a conflict of interest. For all these reasons, we can imagine that strong of the early outcomes, the applications of robotic devices will lead to a new era of long-lasting TKAs; however, this is yet to be proven.
Conclusion and Future Direction
In conclusion, surgical robots for TKA might be in their infancy when considering their actual potential, but they are already demonstrating clear benefits when compared to conventional manual technique. As technology continues its evolution, a more streamlined, interactive, AR integrated robotic systems can be expected. As more surgeons support this technology and become more familiar with the surgical technique, it may be possible to reduce the costs and increase the theatre time efficiency, enabling a wider adoption of this powerful tool.
Abbreviations
TJA, total joint arthroplasty; mTKA, manual total knee arthroplasty; rTKA, robotic total knee arthroplasty; OR, operative room; UKA, unicompartmental knee arthroplasty; MPTA, medial proximal tibial angle; LDFA, lateral distal femoral angle; JL, joint line; PROMs, patient-reported outcome measures; EOC, episode-of-care; LOS, length-of-stay; QUALY, quality adjusted-life; WTP, willingness-to-pay; ICER, incremental cost-effectiveness ratio; nTKA, navigated total knee arthroplasty; THA, total hip arthroplasty; COI, conflict of interest; AI, artificial intelligence; AR, augmented reality; QOL, Quality of Life.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
FB declares a teaching contract with Zimmer Biomet (Warsaw, IN, USA). Dr Christopher W Jones reports personal fees from Johnson & Johnson, share holder in NavBit Pty Ltd, personal fees from Medacta, personal fees from MatOrtho, outside the submitted work. The other authors have no conflicts of interest to declare that are relevant to the content of this article. No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
References
1. Callaghan JJ, Bracha P, Liu SS, Piyaworakhun S, Goetz DD, Johnston RC. Survivorship of a Charnley total hip arthroplasty: a concise follow-up, at a minimum of thirty-five years, of previous reports*. J Bone Jt Surg. 2009;91(11):2617–2621. doi:10.2106/JBJS.H.01201
2. Jauregui JJ, Cherian JJ, Pierce TP, Beaver WB, Issa K, Mont MA. Long-term survivorship and clinical outcomes following total knee arthroplasty. J Arthroplasty. 2015;30(12):2164–2166. doi:10.1016/j.arth.2015.05.052
3. Booth RE, Sharkey PF, Parvizi J. Robotics in hip and knee arthroplasty: real innovation or marketing ruse. J Arthroplasty. 2019;34(10):2197–2198. doi:10.1016/j.arth.2019.08.006
4. Kayani B, Konan S, Ayuob A, Onochie E, Al-Jabri T, Haddad FS. Robotic technology in total knee arthroplasty: a systematic review. EFORT Open Rev. 2019;4(10):611–617. doi:10.1302/2058-5241.4.190022
5. Mancino F, Cacciola G, Malahias MA, et al. What are the benefits of robotic-assisted total knee arthroplasty over conventional manual total knee arthroplasty? A systematic review of comparative studies. Orthop Rev. 2020. doi:10.4081/or.2020.8657
6. Innocenti B, Bori E. Robotics in orthopaedic surgery: why, what and how? Arch Orthop Trauma Surg. 2021;141(12):2035–2042. doi:10.1007/s00402-021-04046-0
7. Song EK, Seon JK, Yim JH, Netravali NA, Bargar WL. Robotic-assisted TKA reduces postoperative alignment outliers and improves gap balance compared to conventional TKA. Clin Orthop. 2013;471(1):118–126. doi:10.1007/s11999-012-2407-3
8. Song EK, Seon JK, Park SJ, Jung WB, Park HW, Lee GW. Simultaneous bilateral total knee arthroplasty with robotic and conventional techniques: a prospective, randomized study. Knee Surg Sports Traumatol Arthrosc. 2011;19(7):1069–1076. doi:10.1007/s00167-011-1400-9
9. Yang HY, Seon JK, Shin YJ, Lim HA, Song EK. Robotic total knee arthroplasty with a cruciate-retaining implant: a 10-year follow-up study. Clin Orthop Surg. 2017;9(2):169. doi:10.4055/cios.2017.9.2.169
10. Liow MHL, Chin PL, Pang HN, Tay DKJ, Yeo SJ. THINK surgical TSolution-One ® (Robodoc) total knee arthroplasty. SICOT-J. 2017;3:63. doi:10.1051/sicotj/2017052
11. Liow M, Chin P, Tay K, Chia S, Lo N, Yeo S. Early experiences with robot-assisted total knee arthroplasty using the DigiMatchTM ROBODOC® surgical system. Singapore Med J. 2014;55(10):529–534. doi:10.11622/smedj.2014136
12. Marchand R, Sodhi N, Khlopas A, et al. Patient satisfaction outcomes after robotic arm-assisted total knee arthroplasty: a short-term evaluation. J Knee Surg. 2017;30(09):849–853. doi:10.1055/s-0037-1607450
13. Jacofsky DJ, Allen M. Robotics in arthroplasty: a comprehensive review. J Arthroplasty. 2016;31(10):2353–2363. doi:10.1016/j.arth.2016.05.026
14. Seidenstein A, Birmingham M, Foran J, Ogden S. Better accuracy and reproducibility of a new robotically-assisted system for total knee arthroplasty compared to conventional instrumentation: a cadaveric study. Knee Surg Sports Traumatol Arthrosc. 2021;29(3):859–866. doi:10.1007/s00167-020-06038-w
15. Han S, Rodriguez-Quintana D, Freedhand AM, Mathis KB, Boiwka AV, Noble PC. Contemporary robotic systems in total knee arthroplasty. Orthop Clin North Am. 2021;52(2):83–92. doi:10.1016/j.ocl.2020.12.001
16. Suero EM, Plaskos C, Dixon PL, Pearle AD. Adjustable cutting blocks improve alignment and surgical time in computer-assisted total knee replacement. Knee Surg Sports Traumatol Arthrosc. 2012;20(9):1736–1741. doi:10.1007/s00167-011-1752-1
17. Figueroa F, Wakelin E, Twiggs J, Fritsch B. Comparison between navigated reported position and postoperative computed tomography to evaluate accuracy in a robotic navigation system in total knee arthroplasty. Knee. 2019;26(4):869–875. doi:10.1016/j.knee.2019.05.004
18. Cho KJ, Seon JK, Jang WY, Park CG, Song EK. Robotic versus conventional primary total knee arthroplasty: clinical and radiological long-term results with a minimum follow-up of ten years. Int Orthop. 2019;43(6):1345–1354. doi:10.1007/s00264-018-4231-1
19. Jeon SW, Kim KI, Song SJ. Robot-assisted total knee arthroplasty does not improve long-term clinical and radiologic outcomes. J Arthroplasty. 2019;34(8):1656–1661. doi:10.1016/j.arth.2019.04.007
20. Kim YH, Yoon SH, Park JW. Does robotic-assisted TKA result in better outcome scores or long-term survivorship than conventional TKA? A randomized, controlled trial. Clin Orthop. 2020;478(2):266–275. doi:10.1097/CORR.0000000000000916
21. Parratte S, Price AJ, Jeys LM, Jackson WF, Clarke HD. Accuracy of a new robotically assisted technique for total knee arthroplasty: a cadaveric study. J Arthroplasty. 2019;34(11):2799–2803. doi:10.1016/j.arth.2019.06.040
22. Bollars P, Boeckxstaens A, Mievis J, Kalaai S, Schotanus MGM, Janssen D. Preliminary experience with an image-free handheld robot for total knee arthroplasty: 77 cases compared with a matched control group. Eur J Orthop Surg Traumatol. 2020;30(4):723–729. doi:10.1007/s00590-020-02624-3
23. Collins K, Agius PA, Fraval A, Petterwood J. Initial experience with the NAVIO robotic-assisted total knee replacement—coronal alignment accuracy and the learning curve. J Knee Surg. 2021;s-0040–1722693. doi:10.1055/s-0040-1722693
24. Doan GW, Courtis RP, Wyss JG, Green EW, Clary CW. Image-free robotic-assisted total knee arthroplasty improves implant alignment accuracy: a cadaveric study. J Arthroplasty. 2022;37(4):795–801. doi:10.1016/j.arth.2021.12.035
25. Sires JD, Craik JD, Wilson CJ. Accuracy of bone resection in MAKO total knee robotic-assisted surgery. J Knee Surg. 2021;34(07):745–748. doi:10.1055/s-0039-1700570
26. Shin C, Crovetti C, Huo E, Lionberger D. Unsatisfactory accuracy of recent robotic assisting system ROSA for total knee arthroplasty. J Exp Orthop. 2022;9(1):82. doi:10.1186/s40634-022-00522-7
27. Rivière C, Iranpour F, Auvinet E, et al. Alignment options for total knee arthroplasty: a systematic review. Orthop Traumatol Surg Res. 2017;103(7):1047–1056. doi:10.1016/j.otsr.2017.07.010
28. Kazarian GS, Haddad FS, Donaldson MJ, Wignadasan W, Nunley RM, Barrack RL. Implant malalignment may be a risk factor for poor Patient-Reported Outcomes Measures (PROMs) Following Total Knee Arthroplasty (TKA). J Arthroplasty. 2022;37(6):S129–S133. doi:10.1016/j.arth.2022.02.087
29. Thiengwittayaporn S, Uthaitas P, Senwiruch C, Hongku N, Tunyasuwanakul R. Imageless robotic-assisted total knee arthroplasty accurately restores the radiological alignment with a short learning curve: a randomized controlled trial. Int Orthop. 2021;45(11):2851–2858. doi:10.1007/s00264-021-05179-y
30. Savov P, Tuecking LR, Windhagen H, Ehmig J, Ettinger M. Imageless robotic handpiece-assisted total knee arthroplasty: a learning curve analysis of surgical time and alignment accuracy. Arch Orthop Trauma Surg. 2021;141(12):2119–2128. doi:10.1007/s00402-021-04036-2
31. Deckey DG, Rosenow CS, Verhey JT, et al. Robotic-assisted total knee arthroplasty improves accuracy and precision compared to conventional techniques. Bone Jt J. 2021;103-B(6 Supple A):74–80. doi:10.1302/0301-620X.103B6.BJJ-2020-2003.R1
32. Kayani B, Konan S, Huq SS, Tahmassebi J, Haddad FS. Robotic-arm assisted total knee arthroplasty has a learning curve of seven cases for integration into the surgical workflow but no learning curve effect for accuracy of implant positioning. Knee Surg Sports Traumatol Arthrosc. 2019;27(4):1132–1141. doi:10.1007/s00167-018-5138-5
33. Vermue H, Luyckx T, Winnock de Grave P, et al. Robot-assisted total knee arthroplasty is associated with a learning curve for surgical time but not for component alignment, limb alignment and gap balancing. Knee Surg Sports Traumatol Arthrosc. 2022;30(2):593–602. doi:10.1007/s00167-020-06341-6
34. Vanlommel L, Neven E, Anderson MB, Bruckers L, Truijen J. The initial learning curve for the ROSA® Knee System can be achieved in 6–11 cases for operative time and has similar 90-day complication rates with improved implant alignment compared to manual instrumentation in total knee arthroplasty. J Exp Orthop. 2021;8(1):119. doi:10.1186/s40634-021-00438-8
35. Bell C, Grau L, Orozco F, et al. The successful implementation of the Navio robotic technology required 29 cases. J Robot Surg. 2022;16(3):495–499. doi:10.1007/s11701-021-01254-z
36. Mahure SA, Teo GM, Kissin YD, Stulberg BN, Kreuzer S, Long WJ. Learning curve for active robotic total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2021. doi:10.1007/s00167-021-06452-8
37. Ali M, Phillips D, Kamson A, Nivar I, Dahl R, Hallock R. Learning curve of robotic-assisted total knee arthroplasty for non-fellowship-trained orthopedic surgeons. Arthroplast Today. 2022;13:194–198. doi:10.1016/j.artd.2021.10.020
38. St Mart JP, Goh EL. The current state of robotics in total knee arthroplasty. EFORT Open Rev. 2021;6(4):270–279. doi:10.1302/2058-5241.6.200052
39. Moschetti WE, Konopka JF, Rubash HE, Genuario JW. Can robot-assisted unicompartmental knee arthroplasty be cost-effective? A Markov decision analysis. J Arthroplasty. 2016;31(4):759–765. doi:10.1016/j.arth.2015.10.018
40. Vermue H, Tack P, Gryson T, Victor J. Can robot-assisted total knee arthroplasty be a cost-effective procedure? A Markov decision analysis. Knee. 2021;29:345–352. doi:10.1016/j.knee.2021.02.004
41. Cool CL, Jacofsky DJ, Seeger KA, Sodhi N, Mont MA. A 90-day episode-of-care cost analysis of robotic-arm assisted total knee arthroplasty. J Comp Eff Res. 2019;8(5):327–336. doi:10.2217/cer-2018-0136
42. Rajan PV, Khlopas A, Klika A, Molloy R, Krebs V, Piuzzi NS. The cost-effectiveness of robotic-assisted versus manual total knee arthroplasty: a Markov model–based evaluation. J Am Acad Orthop Surg. 2022;30(4):168–176. doi:10.5435/JAAOS-D-21-00309
43. Steffens D, Karunaratne S, McBride K, Gupta S, Horsley M, Fritsch B. Implementation of robotic-assisted total knee arthroplasty in the public health system: a comparative cost analysis. Int Orthop. 2022;46(3):481–488. doi:10.1007/s00264-021-05203-1
44. Baek JH, Lee SC, Kim JH, Ahn HS, Nam CH. Distal femoral tracker pin placement prevents delayed pin tract-induced fracture in robotic-assisted total knee arthroplasty: results of minimum 1-year follow-up. J Knee Surg. 2022. doi:10.1055/s-0042-1749605
45. Thomas TL, Goh GS, Nguyen MK, Lonner JH. Related complications in computer navigated and robotic-assisted knee arthroplasty: a systematic review. J Arthroplasty. 2022;S0883540322005447. doi:10.1016/j.arth.2022.05.012
46. Naranje S, Lendway L, Mehle S, Gioe TJ. Does operative time affect infection rate in primary total knee arthroplasty? Clin Orthop. 2015;473(1):64–69. doi:10.1007/s11999-014-3628-4
47. DeFrance MJ, Yayac MF, Courtney PM, Squire MW. The impact of author financial conflicts on robotic-assisted joint arthroplasty research. J Arthroplasty. 2021;36(4):1462–1469. doi:10.1016/j.arth.2020.10.033
48. Elliott J, Shatrov J, Fritsch B, Parker D. Robotic-assisted knee arthroplasty: an evolution in progress. A concise review of the available systems and the data supporting them. Arch Orthop Trauma Surg. 2021;141(12):2099–2117. doi:10.1007/s00402-021-04134-1
49. Siddiqi A, Horan T, Molloy RM, Bloomfield MR, Patel PD, Piuzzi NS. A clinical review of robotic navigation in total knee arthroplasty: historical systems to modern design. EFORT Open Rev. 2021;6(4):252–269. doi:10.1302/2058-5241.6.200071
50. Agarwal N, To K, McDonnell S, Khan W. Clinical and radiological outcomes in robotic-assisted total knee arthroplasty: a systematic review and meta-analysis. J Arthroplasty. 2020;35(11):3393–3409.e2. doi:10.1016/j.arth.2020.03.005
51. Khlopas A, Sodhi N, Sultan AA, Chughtai M, Molloy RM, Mont MA. Robotic arm–assisted total knee arthroplasty. J Arthroplasty. 2018;33(7):2002–2006. doi:10.1016/j.arth.2018.01.060
52. Mancino F, Rossi SMP, Sangaletti R, Lucenti L, Terragnoli F, Benazzo F. A new robotically assisted technique can improve outcomes of total knee arthroplasty comparing to an imageless navigation system. Arch Orthop Trauma Surg. 2022. doi:10.1007/s00402-022-04560-9
53. Mullaji AB, Khalifa AA. Is it prime time for robotic-assisted TKAs? A systematic review of current studies. J Orthop. 2022;34:31–39. doi:10.1016/j.jor.2022.07.016
54. Batailler C, Parratte S. Assistive technologies in knee arthroplasty: fashion or evolution? Rate of publications and national registries prove the Scott Parabola wrong. Arch Orthop Trauma Surg. 2021;141(12):2027–2034. doi:10.1007/s00402-021-04051-3
55. Rossi SMP, Mancino F, Sangaletti R, Perticarini L, Lucenti L, Benazzo F. Augmented reality in orthopedic surgery and its application in total joint arthroplasty: a systematic review. Appl Sci. 2022;12(10):5278. doi:10.3390/app12105278
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.