")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 14
When Inappropriate Use of Insulin is Dangerous: The Utility of C-Peptide Assay in the Era of Cardioprotective Antidiabetic Drugs
Authors Volpe S, Tortorella C, Solfrizzi V, Piazzolla G
Received 22 May 2021
Accepted for publication 26 June 2021
Published 5 August 2021 Volume 2021:14 Pages 3517—3521
DOI https://doi.org/10.2147/DMSO.S321340
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Konstantinos Tziomalos
Sara Volpe, Cosimo Tortorella, Vincenzo Solfrizzi, Giuseppina Piazzolla
Interdisciplinary Department of Medicine, University of Bari “Aldo Moro” Medical School, Bari, 70124, Italy
Correspondence: Giuseppina Piazzolla
Interdisciplinary Department of Medicine, University of Bari “Aldo Moro” Medical School, Policlinico, Piazza G. Cesare 11, Bari, 70124, Italy
Fax +39 080 5478126
Email [email protected]
Introduction: New antidiabetic drugs have simplified treatment regimens in patients with type-2 diabetes (T2D). More importantly, they have proven to reduce cardiovascular risk by lowering insulin-resistance, blood pressure and body weight, in addition to avoiding inappropriate insulin therapy, responsible for hypoglycemic episodes and weight gain. In this context, accurate assessment of the metabolic status of T2D patients becomes essential. The C-peptide assay is a simple but often overlooked test that can provide a fundamental contribution to the correct disease classification and optimal therapeutic management of diabetic patients.
Clinical Case: We report the case of a 72-year-old patient, treated with insulin for 26 years after a diagnosis of type-1 diabetes (T1D), resulting in inadequate glycemia control and a severe evolution of cardiovascular complications. After an accurate evaluation of the clinical history, phenotype and laboratory data, including the determination of C-peptide serum levels, a diagnosis was made of T2D not T1D. Considering the patient’s very high cardiovascular risk and dysmetabolic profile, insulin therapy was discontinued and more appropriate therapy with dulaglutide and metformin was instituted. These overall therapeutic modifications yielded remarkable clinical advantages in terms of the glycometabolic profile, weight reduction, abdominal circumference and body mass index decrease, as well as a better quality of life, with complete resolution of the dangerous hypoglycemic episodes.
Conclusion: In the era of new cardioprotective antidiabetic drugs, we believe the importance of the C-peptide assay should be re-evaluated in order to avoid misdiagnosis and to improve the therapeutic approach to T2D.
Keywords: diabetes, metabolic syndrome, hypoglycemia, obesity, dulaglutide, quality of life
Introduction
Type-2 diabetes (T2D) is becoming more prevalent in the general population, especially in individuals over the age of 65 years, and is closely linked to cardiovascular diseases (CVDs). The treatment of diabetes is challenging, since the aims addressed are to achieve metabolic compensation and to reduce micro and macrovascular complications.1,2 Cardiovascular outcome trials (CVOTs) have provided useful information on the cardiovascular safety and cardio- and nephro-protection achieved with the new anti-diabetes drugs, namely Glucagon-like-peptide-1 receptor agonists (GLP-1 RA) and sodium-glucose transporter-2 inhibitors (SGLT2i). These are both very effective pharmacological approaches, currently recommended for T2D, particularly in patients with established heart disease or at high risk for cardiovascular events. Nowadays, since the emergence of these revolutionary drugs for the treatment of T2D, routine determination of the pancreatic β cells reserve has become essential. C-peptide is a biomarker of residual β-cell function and can provide valuable clinical information, but it is rarely used to classify the diabetes type in clinical practice or to manage T2D.3,4 While type-1 diabetes (T1D) is an autoimmune process leading to the loss of pancreatic β-cell function, T2D is a heterogeneous disease characterized by a combination of varying degrees of relative insulin secretory deficiency and insulin-resistance linked to the metabolic syndrome, featuring a slower, more protracted course. We report the case of a 72-year-old dysmetabolic patient, treated with insulin for 26 years after a diagnosis of T1D, who developed severe CVDs. An accurate evaluation of the clinical history, phenotype and especially the measurement of C-peptide levels allowed us to correct the T1D misdiagnosis to T2D, and set up a more appropriate therapy resulting in metabolic and glycemic advantages and a marked improvement of the patient’s quality of life. Regular use of the C-peptide assay in clinical practice, particularly at the time of first diagnosis, might help clinicians to avoid inappropriate use of insulin and prevent a detrimental delay in the introduction of new cardioprotective antidiabetic drugs.
Clinical Case
A 72-year-old man with a history of T1D was admitted to the Department of Internal Medicine complaining of alternating hyperglycemia and numerous hypoglycemic episodes.
The patient signed the informed consent for the acquisition, analysis, and publishing of the anonymized data collected. Since no personal identification data were used in this manuscript, the ethics committee approval is not needed.
The patient had been diagnosed with T1D in 1994 at a diabetes center and treated with insulin thereafter, continuing follow-up at an endocrinology department. He was a former smoker (15 pack-years), non-drinker, and reported a family history of diabetes and cardiovascular diseases. After the T1D diagnosis, his clinical course was complicated by peripheral neuropathy, arterial hypertension, OSAS (obstructive sleep apnea syndrome) and multiple episodes of angina, requiring placement of intracoronary stents for an N-STEMI (non-ST-segment elevation myocardial infarction) in 2011. At the time of our first observation, the patient’s medications included a β-blocker, an angiotensin-converting enzyme (ACE)-inhibitor, double antiplatelet therapy, ranolazine, statins, furosemide and pregabalin. Diabetes medications consisted of basal-bolus insulin therapy, in the form of long-acting insulin glargine 30 I.U. at bedtime, and short-acting insulin lispro at meals (8 I.U. at breakfast and dinner, 15 I.U. at lunch). Last year, his family doctor had recommended increasing the doses of short-acting insulin at meals, in order to improve the glycemic control, but his conditions were deteriorating due to the onset of numerous hypoglycemic episodes (up to 4 per day) and an increased appetite. At physical examination, the patient had a high body mass index (BMI) and abdominal circumference, and his condition was classified as metabolic syndrome with class I obesity (Table 1). The laboratory tests showed unsatisfactory glycemic compensation and a suboptimal lipid profile but preserved renal function (see Table 1). Serum C-peptide levels had never been determined in any of the patient’s clinical records. Nor had the presence of autoantibodies to diabetes-associated antigens ever been evaluated since the T1D diagnosis. The fasting serum C-peptide assay was performed and resulted within the normal range. The patient’s clinical history, as well as his phenotype, suggested a diagnosis of T2D rather than T1D. This view was confirmed by the finding of normal C-peptide levels. Ezetimibe and metformin were added to the therapy, and the short-acting insulin dose was tapered until complete discontinuation at 10 days. Owing to the patient’s very high cardiovascular risk, either an SGLT2i or a GLP-1RA was particularly indicated.5–8 His obesity status and referred increase in appetite led us to institute therapy with dulaglutide, a long-acting GLP-1RA. Over the next 4 weeks, the long-acting insulin doses were also completely discontinued. After 4 weeks of treatment, the patient’s glycated hemoglobin values had normalized and no further hypoglycemic episodes occurred. After 2 months of dulaglutide treatment, and the insulin discontinuation, the patient achieved 10 kg of weight loss and a reduction in abdominal circumference by 13 cm.
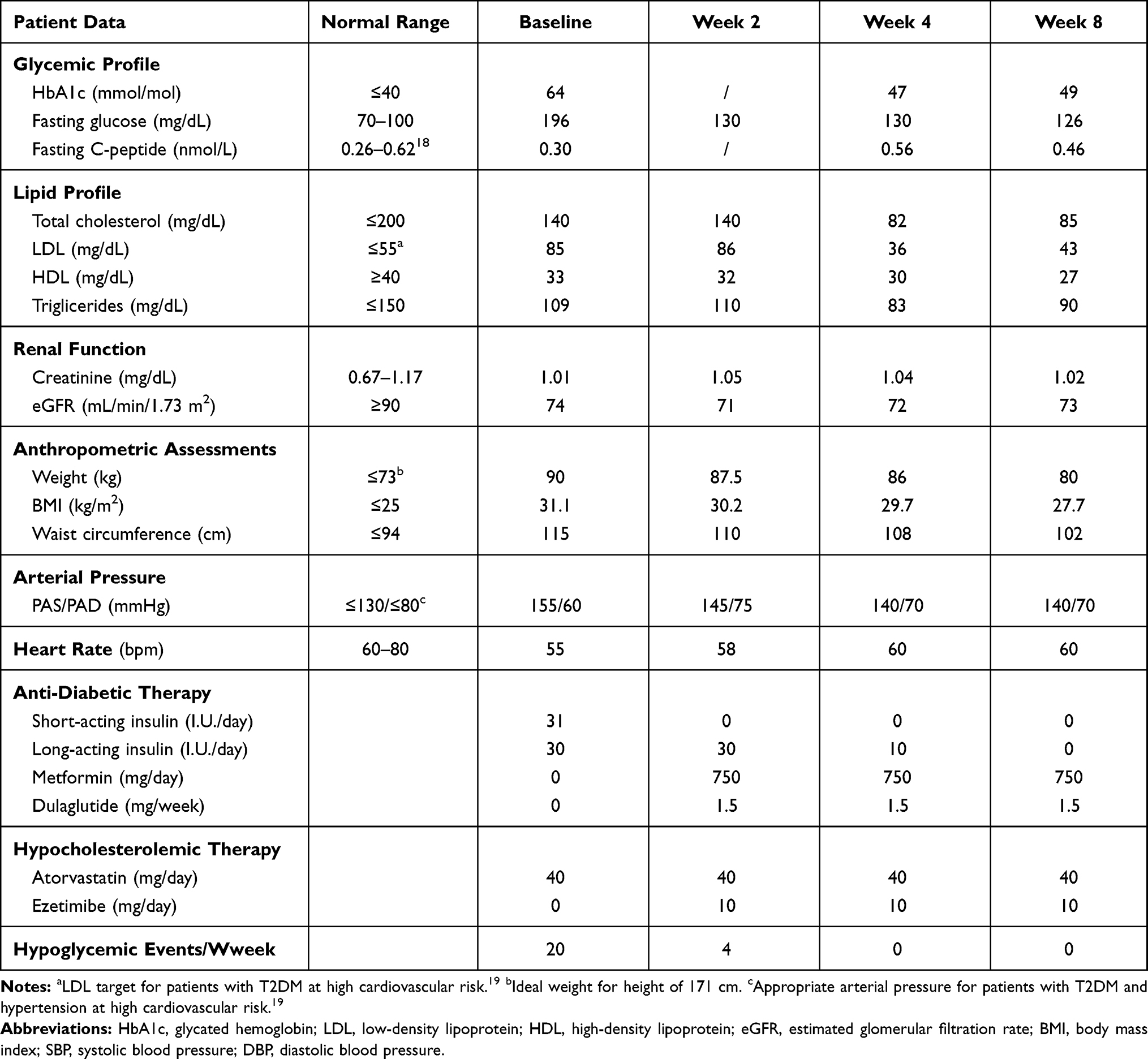 |
Table 1 Relevant Patient Data Before (Baseline) and 2, 4 and 8 Weeks After Instituting the New Therapy |
Discussion
In past decades, randomized trials compared the effect of more versus less intensive glycemic control, showing that the potential benefit of strict glycemic control on microvascular diabetes complications was counteracted by the increased risk of cardiovascular disease and mortality.9 In contrast to the more traditional focus on glycemic control, new diabetes guidelines increasingly highlight the importance of multifactorial management focused on cardiovascular risk benefits. Recent CVOTs have provided useful information on cardio- and nephro-protection conferred by the new antidiabetic drugs.6,10 In this context, an accurate evaluation of the diabetic disease and correct determination of pancreatic reserves are crucial to ensure optimal care. C-peptide is the part of pro-insulin cleaved prior to co-secretion with insulin by pancreatic β-cells. It is produced in equimolar amounts to endogenous insulin and provides the best gauge of β-cells’ ability to produce insulin in diabetic patients, including those treated with exogenous insulin.3,11,12 The determination of serum C-peptide levels can help to identify subjects whose residual β-cell function is still sufficient to indicate the use of emerging antidiabetic drugs, avoiding the administration of exogenous insulin. Instead, very low C-peptide levels, suggestive of a defective β-cell secretory function, have been indicated as predictors of poor response to GLP-1 RA.13 Serious errors may arise when T1D is diagnosed later in life; in fact, more than 50% of the patients diagnosed with T1D after age 35 have been found to have T2D at long-term follow-up.14 Furthermore, among T2D patients, too often the timing of insulin administration is anticipated due to suboptimal glycemic control, potentially leading to hypoglycemic episodes, weight gain and increased cardiovascular risk. In this context, the C-peptide assay is a simple, inexpensive but often overlooked laboratory test that can provide an essential contribution to the differential diagnosis between T1D and T2D and to a correct determination of pancreatic reserves in T2D.15,16 This patient did not have the typical hallmarks of immune-mediated T1D and his normal C-peptide value was poorly compatible with a diagnosis of T1D 26 years after the disease onset. The patient’s complaint of an increased appetite, the absence of clinical evidence of heart failure, as well as our aim to simplify the therapeutic schedule, constituted the rationale for prescribing metformin and dulaglutide and discontinuing exogenous insulin therapy. After only 4 weeks of treatment the C-peptide levels had further increased, indicating a satisfactory residual β-cell function. Following these therapeutic changes, the patient’s quality of life significantly improved, thanks to the reduced subcutaneous administration of drugs (from 4 per day to 1 per week) and resolution of the frequent hypoglycemic episodes. Hypoglycemia has long been recognized as a dangerous side effect of treating diabetes with insulin or insulin secretagogues. Indeed, hypoglycemia is associated with negative life consequences, ranging from the disruption of daily activities to psychosocial problems for both patients and their family members, in addition to increasing cardiovascular risk and mortality.9,17 After a few days of treatment with dulaglutide and insulin discontinuation, the quality of life of our patient had improved considerably, as also his therapeutic compliance. Other clinical advantages included the normalization of glycated hemoglobin values, a decreased appetite, 10 kg of weight loss in only 2 months and a 13 cm reduction in abdominal circumference, all yielding unquestionable health benefits.
The study's strong point lies in the evidence that C-peptide evaluation changed the diagnosis and therapeutic management of our patient. Accordingly, the use of C-peptide as a preliminary test in clinical practice may help clinicians to institute the most suitable antidiabetic therapy as early as possible, and also encourage them to refrain from prescribing insulin at all, when it may actually be useless.
The main limitation is that the c-peptide assay is a well-known but overlooked test and the official guidelines on medical care in diabetes and pre-diabetes do not exploit it for the correct classification of patients. For this reason, there are not yet data in the literature to support our view that re-evaluating c-peptide dosage as a key tool may offer a novel approach to diabetic disease management.
Conclusion
We believe that in the era of the new cardioprotective antidiabetic drugs, the C-peptide assay may be the natural laboratory complement to clinical signs and symptoms in T2D patients, offering the advantage of avoiding inappropriate prescription of insulin to dysmetabolic and insulin-resistant patients. A correct clinical classification of our patient and the determination of a preserved pancreatic β-cell function with this simple test led us to introduce a more beneficial and appropriate antidiabetic therapy. The application of this test in clinical practice might have important implications on cardioprotection and body wellness in diabetic patients. Certainly, inappropriate or overuse of insulin in dysmetabolic and high cardiovascular risk patients is no longer acceptable, and should be considered deleterious to their health and quality of life. This strongly suggests that the C-peptide assay needs to be re-evaluated as a key tool for use in daily clinical practice.
Abbreviations
T2D, type-2 diabetes; T1D, type-1 diabetes; CVD, cardiovascular disease; CVOTs, cardiovascular outcome trials; GLP-1RA, glucagon-like-peptide-1 receptor agonists; SGLT2i, sodium-glucose transporter-2 inhibitors; OSAS, obstructive sleep apnea syndrome; N-STEMI, non-ST-segment elevation myocardial infarction; ACE, angiotensin-converting enzyme; I.U., International Units; BMI, body mass index; HbA1c, glycated hemoglobin; LDL, low-density lipoprotein; HDL, high-density lipoprotein; eGFR, estimated glomerular filtration rate; SBP, systolic blood pressure; DBP, diastolic blood pressure.
Acknowledgments
We are grateful to Mary Pragnell for language revision.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no actual or potential conflicts of interest in relation to this work.
References
1. Beckman JA, Paneni F, Cosentino F, et al. Diabetes and vascular disease: pathophysiology, clinical consequences, and medical therapy: part II. Eur Heart J. 2013;34:2444–2452. doi:10.1093/eurheartj/eht142
2. Low Wang CC, Hess C, Hiatt WR, et al. Clinical update: cardiovascular disease in diabetes mellitus: atherosclerotic cardiovascular disease and heart failure in type 2 diabetes mellitus - mechanisms, management, and clinical considerations. Circulation. 2016;133:2459–2502. doi:10.1161/CIRCULATIONAHA.116.022194
3. Jones AG, Hattersley AT. The clinical utility of C-peptide measurement in the care of patients with diabetes. Diabet Med. 2013;30:803–817. doi:10.1111/dme.12159
4. Hope SV, Wienand-Barnett S, Shepherd M. Practical Classification Guidelines for Diabetes in patients treated with insulin: a cross-sectional study of the accuracy of diabetes diagnosis. Br J Gen Pract. 2016;66:E315–E322. doi:10.3399/bjgp16X684961
5. Gerstein HC, Colhoun HM, Dagenais GR, et al. Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): a double-blind, randomized placebo-controlled trial. Lancet. 2019;394:121–130.
6. Giorgino F, Caruso I, Moelimann J, et al. Differential indication for SGLT-2 inhibitors versus GLP-1 receptor agonists in patients with established atherosclerotic heart disease or at risk for congestive heart failure. Metabolism. 2020;104:154045. doi:10.1016/j.metabol.2019.154045
7. Cosentino F, Grant PJ, Aboyans V, et al. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular disease developed in collaboration with the EASD. Eur Heart J. 2020;41(2):255–323.
8. Standards of medical care in diabetes 2021 ADA (American Diabetes Association). Diabetes Care. 2021;44(Suppl1):S111–S124. doi:10.2337/dc21-S009
9. Gerstein HC, Miller ME, Byington RP, et al. Effect of intensive glucose lowering in type 2 diabetes. N Engl J Med. 2008;358(24):2545–2559.
10. Zelniker TA, Wiviott SD, Raz I, et al. SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials. Lancet. 2019;393:31–39. doi:10.1016/S0140-6736(18)32590-X
11. Becht FS, Walther K, Martin E, et al. Fasting C-peptide and related parameters characterizing insulin secretory capacity for correctly classifying diabetes type and for predicting insulin requirement in patients with type 2 diabetes. Exp Clin Endocrinol Diabetes. 2016;124:148–156. doi:10.1055/s-0035-1565177
12. Ludvigsson J. C-peptide in diabetes diagnosis and therapy. Front Biosci. 2013;5:214–223. doi:10.2741/E609
13. Jones AG, McDonald TJ, Shields BM, et al. Markers of β-cell failure predict poor glycemic response to GLP-1 receptor agonist therapy in type 2 diabetes. Diabetes Care. 2016;39:250.
14. Thomas NJ, Jones SE, Weedon MN, et al. Frequency and phenotype of type 1 diabetes in the first six decades of life: a cross-sectional, genetically stratified survival analysis from UK Biobank. Lancet Diabetes Endocrinol. 2018;6:122–129. doi:10.1016/S2213-8587(17)30362-5
15. Munshi MN, Hayes M, Sternthal A, et al. Use of serum C-peptide level to simplify diabetes treatment regimens in older adults. Am J Med. 2009;122:395–397. doi:10.1016/j.amjmed.2008.12.008
16. Nathan D. The diabetes control and complications trial/epidemiology of diabetes interventions and complications study at 30 years: overview. Diabetes Care. 2014;37:9–16. doi:10.2337/dc13-2112
17. Rossi MC, Nicolucci A, Ozzello A, et al. Impact of severe and symptomatic hypoglycemia on quality of life and fear of hypoglycemia in type 1 and type 2 diabetes. Results of the Hypos-1 observational study. Nutr Metab Cardiovasc Dis. 2019;29(7):736–743. doi:10.1016/j.numecd.2019.04.009
18. Pagana KD, Pagana TJ, Pagana TN. Mosby’s Diagnostic & Laboratory Test Reference.
19. Mach F, Baigent C, Catapano AL, et al. 2019 ESC/EAS Guidelines for the management of dyslipidemia: lipid modification to reduce cardiovascular risk. Eur Heart J. 2020;41(1):111–188.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.