")
Back to Journals » Risk Management and Healthcare Policy » Volume 15
What are the Bad Habits and Behaviors of Inconsiderate Doctors in Chinese Inhabitants’ Mind? A Cross-Sectional Study
Authors Wang HN, Wang JH, Zhao X, Wang XH, Zhang M, Shi Y, Zhang SE , Sun T , Liu B
Received 24 January 2022
Accepted for publication 18 March 2022
Published 6 April 2022 Volume 2022:15 Pages 583—595
DOI https://doi.org/10.2147/RMHP.S358680
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Hong-Ni Wang,1 Jing-Hui Wang,2 Xin Zhao,1 Xiao-He Wang,1 Meng Zhang,1 Yu Shi,3 Shu-E Zhang,2 Tao Sun,1 Bei Liu4
1Department of Health Management, School of Public Health, Hangzhou Normal University, Hangzhou, People’s Republic of China; 2School of Bioinformatics Science and Technology, Harbin Medical University, Harbin, People’s Republic of China; 3Department of Health Management, School of Vanke Public Health, Tsinghua University, Beijing, People’s Republic of China; 4School of Public Health, Peking University, Beijing, People’s Republic of China
Correspondence: Tao Sun; Bei Liu, Email [email protected]; [email protected]
Purpose: This study aims to 1) investigate inhabitants’ perceptions of doctors’ inconsiderate behaviors during diagnosis and treatment, 2) explore the factors influencing inhabitants’ attitudes toward doctors’ professional reputation, and 3) examine the status of doctors’ inconsiderate behaviors and inhabitants’ attitudes and behaviors toward these doctors in China.
Patients and Methods: A cross-sectional online survey was conducted with 2050 participants from over 30 Chinese cities, from March to June 2018. In total, 1598 valid questionnaires were obtained (with an effective response rate of 77.95%). Data were analyzed using descriptive statistics, exploratory factor analysis, and logistic linear regression analysis.
Results: We developed a questionnaire comprising of 15 items regarding doctors’ inconsiderate behaviors based on inhabitants’ perspectives (Cronbach’s alpha was 0.944). Additionally, we identified the factors that influence the attitudes of inhabitants regarding doctors’ professional reputation, such as frequency of medical consultations, medical expenses, education catalog, and type of medical insurance. A majority of the participants highly valued Chinese doctors’ professional reputation (87.55%), and trusted them (86.29%). However, about 60.27% of the participants reported a pessimistic-like judgment on the current doctor–patient relationship (DPR) in China. Participants believed that Chinese doctors received a high income (20.47%), maintained a high social status (23.46%), and had a heavy workload (59.95%). Furthermore, about 54.88% of participants reported that they would not engage in aggressive behaviors against doctors during a dispute. Lastly, about 26.66% of participants reported that they would act rationally when they were dissatisfied with their doctors.
Conclusion: Impassive emotions and improper actions of doctors toward patients jointly contributed to the disrepute of Chinese doctors. Although DPR was becoming tense, Chinese inhabitants held a positive evaluation of doctors’ professional reputation. While an improvement in the economic situation and reputation of doctors enhanced the DPR, there remains an urgent need to improve the working environment in regard to future Chinese health reforms.
Keywords: Chinese doctors, inconsiderate behaviors, inhabitants’ perspective, doctor–patient relationship
Introduction
After a series of reforms, China’s healthcare system has achieved considerable success in the last decade. The fairness and accessibility of various health care services provided for inhabitants has improved drastically,1 particularly regarding the increase in health care utilization, and the reduced rate of catastrophic health expenditure.2 However, all forms of achievements driven by the health system reform do not yield a harmonious doctor–patient relationship (DPR). Contrary to public expectations, the Chinese DPR continuously appears to deteriorate. In particular, workplace violence against medical professionals is particularly serious in China, with a large number of victims, and high frequency and viciousness of attacks.3 A recent survey conducted with 2617 doctors from across 30 provinces in China revealed that 83.4% of doctors had experienced at least one type of workplace violence within the past year.4 Similarly, a previous study indicated that doctors who experienced high-frequency workplace violence were more likely to have decreased job satisfaction and subjective well-being, and increased turnover intention in hospital settings.5 The Chinese Physicians’ Practice Status White Paper published by the Chinese Medical Doctor Association in 2018 revealed that three-quarters of interviewed doctors had experienced different extents of doctor–patient conflict (DPC), while 62% reported having a poor practice environment. Approximately half of the participants believed that society had not recognized their professional value, and their job satisfaction was significantly lower than that of other professionals.6 Workplace violence initiated by patients or their relatives has significantly increased the level of tension in DPRs in China in recent years. Further, a high quality DPR is conducive to patients’ treatment compliance.7 Therefore, in the field of health policy and hospital management in China, poor DPRs have attracted attention from scholars and practitioners.8
A majority of previous studies on DPRs have only examined the perspective of medical professionals, elucidating the reasons behind frequent workplace violence from patients, leading to a biased understanding of Chinese DPRs among the public.9 The inhabitants’ perceptions of DPRs has received little academic attention in China. Consequently, the receivers’ viewpoints and suggestions on health services have been insufficiently discussed, which likely causes a biased portrayal of the issues related to Chinese DPRs. Previous studies have infrequently mentioned how inhabitants perceive the inconsiderate behaviors of doctors,10 the types of behaviors of doctors that offend the service receivers, and the factors that influence inhabitants’ attitudes toward Chinese doctors. Improving the DPR in China will improve the medical experience of one fifth of the world’s population. While communication varies in countries and nationalities based on language and cultural environments, in the medical field, the psychological processes between doctors and patients remain the same.11 China’s efforts to improve the DPR will also provide reform experience for other countries in the world to review and implement.
Therefore, this study was conducted to augment a more comprehensive understanding of Chinese DPRs. This study proposed 1) to investigate the current status of the doctor’s inconsiderate behaviors from the perspective of inhabitants, 2) to explore the factors influencing inhabitants’ attitudes regarding doctors’ professional reputation, and 3) to identify the inhabitants’ general evaluation tendency toward the current status of the DPR, as well as the attitudes, extent of trust, and behavior tendencies toward Chinese doctors.
Materials and Methods
Participants and Procedures
We conducted a cross-sectional study to collect data using an anonymously online questionnaire. A total of 2050 inhabitants from different regions and occupational groups within China were recruited using convenient sampling between March and June 2018. First, we created a questionnaire on an online survey platform utilizing a reward mechanism, wherein the website would provide some amount of money as a bonus to the respondent upon completion of the questionnaire. Second, in order to make up for the representativeness of the snowball sampling approach, we carefully selected 50 original deliverers, and strived to ensure heterogeneity in their personality traits and living environments. Third, a questionnaire web link was delivered to the participants. This link was then sent to additional individuals by the original deliverers. The survey’s progress was monitored daily. After the survey deadline, the accuracy of the data was evaluated. The inclusion criteria of the study were as follows: 1) voluntary participation, 2) informed consent on the front page of the online questionnaire had been checked by the participant, and 3) the individual’s assurance about the accuracy of the information was provided. The exclusion criteria were as follows: 1) multiple missing item responses in the questionnaire, 2) contradictory answers, and 3) the time to in the in the questionnaire was less than 3 minutes. Finally, 1598 valid questionnaires were included for analysis. The effective response rate was 77.95%. All data were checked for consistency between the two authors.
Patient and Public Involvement
Verbal informed consent for the investigation was obtained from the participants with the approval of the Ethics Committee of Harbin Medical University (ECHMU). Additionally, the informed consent, presented at the beginning of our questionnaire, was personally confirmed by the interviewees. The collected data were only utilized by academic researchers, and the confidentiality of participant information was guaranteed. The guidelines outlined in the Declaration of Helsinki were followed in the study.
Measures
Development of the Doctor’s Inconsiderate Behaviors from the Inhabitants’ Perspective
The questionnaire utilized in this study was developed by the authors. Using a mixed-method evaluation, the questionnaire was designed to measure doctors’ inconsiderate behaviors perceived by inhabitants and was developed in two stages. In the first stage, two authors conducted individual unstructured interviews with inhabitants to identify their perspectives on the inconsiderate behaviors of doctors. When the number of interviewees reached 10, the authors were not able to obtain any new information; thus, the interview was concluded. Interview questions included, but were not limited to the following: 1) In general, when you choose to see a doctor, what are the main factors that you consider? 2) What is the current social image of the doctor in your mind? and 3) Has the DPR changed in recent years? Using interview data, the factors influencing the inhabitants’ social impression/image and attitude toward Chinese doctors were identified. Further, the authors organized the formation and description of an inconsiderate doctor’s social impression and evaluation in the minds of an inhabitant. On this basis, the initial item pool was established. Subsequently, the qualitative interview data collection began (ie, an expert-led discussion group was formed comprising one professor, one doctor, and four graduate students focused on the topic of DPR). Finally, 17 definitive questions were determined.
Next, the determined questions were modified in order to remain distinct from one another, and to provide a basic reference for item rhetoric in the process of the formal questionnaire design. Finally, all items were preliminarily divided into two dimensions. One dimension, termed “behavioral biases,” comprised 10 items on the improper behaviors of doctors. The second dimension, labeled “emotional alienation,” comprised seven items representing the doctors’ negative emotional expressions from the patients’ perspective. The responses were evaluated using a 5-point Likert scale12 (“1=very inconsistent,” “2=inconformity,” “3=ordinary,” “4=consistent,” and “5=very consistent”). Cronbach’s alpha coefficient of the doctor’s bad habit or behaviors from inhabitants’ perspective (BHB) questionnaire was 0.944.
Inhabitants’ Dual-Dimension General Evaluation Tendency Toward Chinese Doctors
As the outcome variable in the regression analysis, one question was used to verify inhabitants’ general evaluation tendency on doctors. The answers were coded on a dual-dimension, including positive general evaluation tendency and negative general evaluation tendency. In the single choice question (ie, “What is your general evaluation about Chinese doctors?”) the following answers were considered to be a negative evaluation and were coded as a “0”: “All the doctors are unqualified,” “There are more bad doctors, and very few good doctors,” and “Good doctors and bad doctors are equal in number.” Two answer options, “There are more good doctors and a few bad doctors” and “All the doctors are good,” were treated as a positive evaluation and coded as “1.”
Inhabitants’ Extent of Trust in Chinese Doctors
Referring to Bova et al.13 Doctor–Patient Trust Scale and considering the differences between Chinese and Western cultures, we used a representative question (ie, “Considering your trust in the doctor, what is your opinion about the doctor’s diagnosis and treatment plan?”) to test the extent of trust that participants held in their doctors. The question corresponded well with the Chinese medical and health industry in our study in investigating participants’ extent of trust in Chinese doctors. The response options included: “I do not believe doctors at all,” “I do not believe doctors very much, and I think I should find more doctors for help,” “I have doubts, but I trust the doctor and will follow the doctor’s plan,” and “I trust doctors very much and I firmly implement the doctor’s treatment plan.” The respondents’ degree of trust in doctors expressed by these options differed. The frequency of participants’ choice of each option relatively reflects the overall situation of their trust in doctors.
Inhabitants’ Perspective Regarding the Chinese DPR
The Patient-Doctor Relationship Questionnaire-15 (PDRQ-15; Chinese version), revised by Hui and Hongqi,14 was used to assess the inhabitants’ perspectives of DPRs in China. Of these, two questions were selected to describe the condition of DPRs. One question, “What do you think about the quality of the current DPR?” included five response options of, “very bad,” “bad,” “neither good nor bad,” “good,” and “very good.” Based on the participants’ responses, the frequency percentage of each option reflected the current DPR status. The second question was, “What do you think about the probability of doctors experiencing DPC in the future?” The probability of doctors experiencing a DPC was measured by 10-point Likert scale, and the score ranged from 1 (low) to 10 (high).
Inhabitants’ Perspectives About the Work Environment of Chinese Doctors
Three indices—doctors’ income, social status, and workload—were used to measure the work environment of Chinese doctors. Each index was measured using a 10-point Likert scale,12 with responses for the three questions ranging from 1 to 10. Based on the final scores, the data of each index were divided into three groups: a low-score group (score of 1 to 4), a medium-score group (score of 5 to 8 score), and high-score group (score of 9 or 10).
Inhabitants’ Behavior Tendency Toward Doctors in a DPC Situation
We examined the inhabitants’ behavior tendency toward doctors facing a DPC situation. First, we used the question, “Will you take aggressive actions against Chinese doctors in a DPC?” to assess the participants’ aggressive intentions. There were three response options. The first response, “I will never attack the doctors in a DPC,” indicated that participants were not aggressive toward doctors. The second response, “Whether I will attack the doctor in a DPC depends on the circumstance,” indicated that participants held moderate aggressiveness toward doctors. The third response, “I would attack the doctor in a DPC,” indicated that participants were highly likely to attack doctors. The overall status of the inhabitants’ aggressive intentions toward doctors was measured using the participants’ option selection frequency. Then, the multiple-choice question “What would you do if you are dissatisfied with doctors?” was asked to investigate the participants’ specific behaviors in a DPC situation. The multiple choices included “Telling people nearby to discredit doctors,” “Abusing doctors on the Internet,” “Attacking doctors with words and actions,” “Complaining about doctors to relevant departments or institutions,” “Tolerating the doctor’s accidental mistake,” and “Wanting to complain, but not yet acted on it.” The respondents’ selection frequency of each option was used to inspect their specific behaviors in a DPC.
Results
Participants’ Demographic Information
A total of 1598 valid questionnaires were included in the final analysis. The average age of the participants was 25±10 years, ranging from 17 to 63 years. About 63.8% of the participants were women. The majority of the participants (74.8%) had social medical insurance. Table 1 presents the participants’ sociodemographic information.
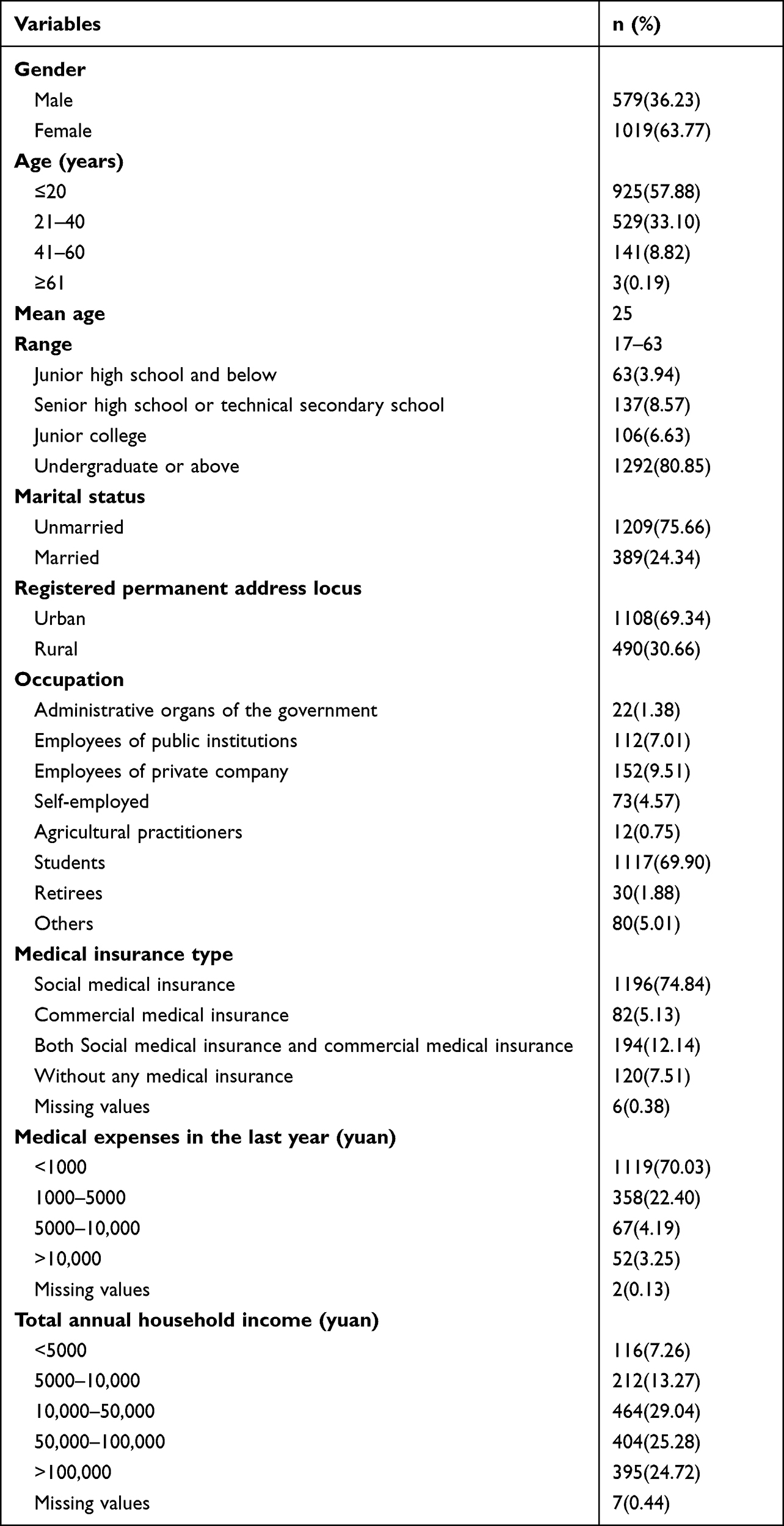 |
Table 1 Characteristics of the Sampling Inhabitants (n = 1598) |
Exploratory Factor Analysis and Reliability Analysis of the Doctors’ Inconsiderate Behaviors as Perceived by the Inhabitants
In this study, 1598 valid questionnaires were collected. The valid data were analyzed using an exploratory factor analysis. The results of the statistical measures employed were as follows: the Kaiser-Meyer-Olkin value was 0.960>0.7, and Bartlett’s test of sphericity was p<0.001. The data analyses suggested that 17 items in this questionnaire were suitable for a factor analysis.15 Further, a principal component analysis (PCA) under the method of maximum orthogonal rotation of variance was used, and the common factors of measurement items were extracted according to the standard of eigenvalue >.16 According to the PCA, “deviant item-9 and-10” had severe cross-loading, which needed to be eliminated. Finally, the BHB questionnaire contained 15 items from which two common factors were extracted, and the total explained variation was 64.85%. After rotation, the dimensions of each item belonged to a clear structure. Table 2 presents the factor loading after rotation.
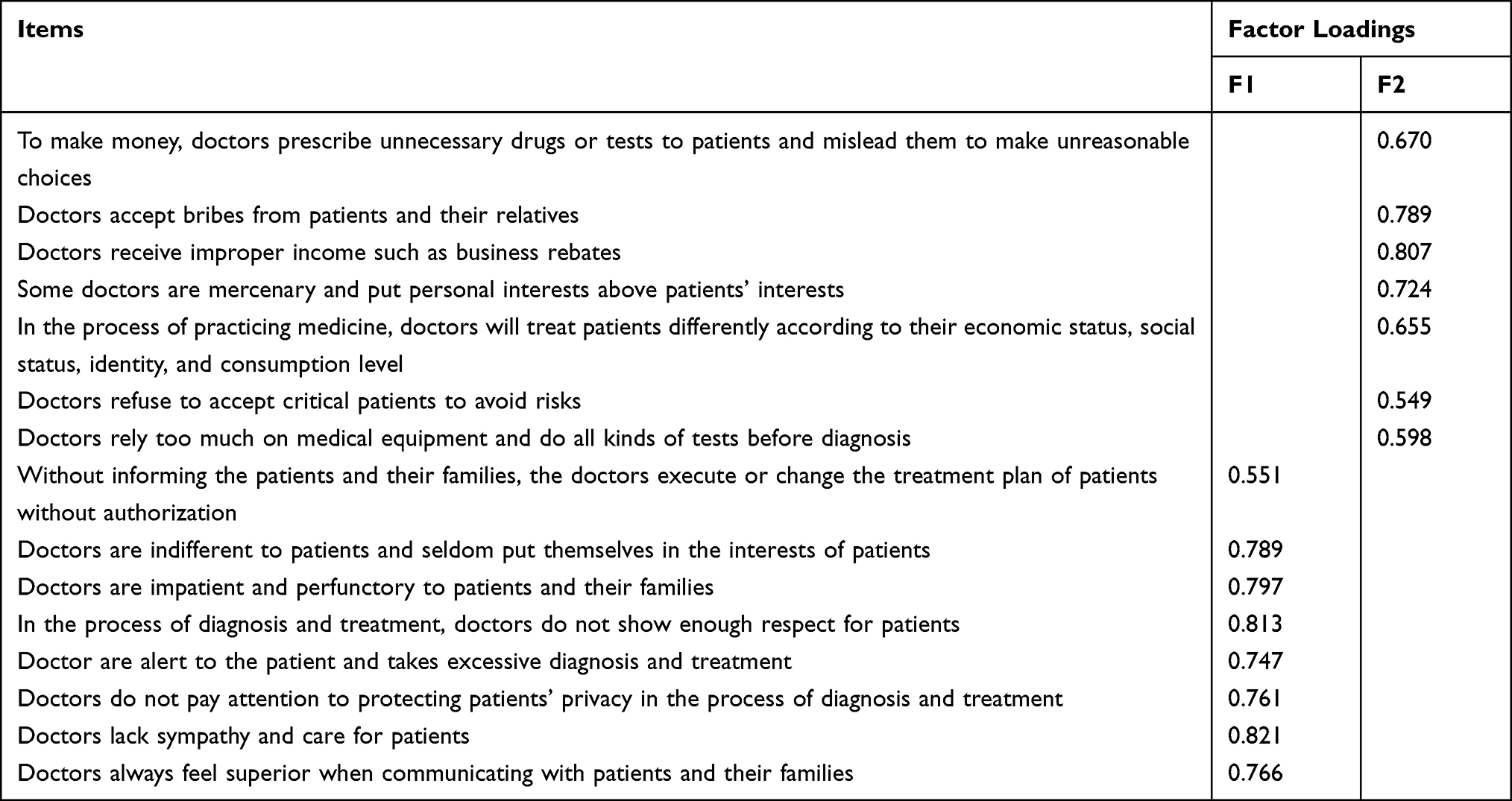 |
Table 2 The Rotated Factor Loading Matrix of All Items (n = 1598) |
Based on the results, we found that the first factor focused on doctors’ impassive emotion, and the second factor encompassed doctors’ improper actions. Therefore, we named the two factors as “human alienation” and “deviant behavior,” respectively.
In this study, Cronbach’s alpha was used to test the reliability of the scale of doctors’ inconsiderate behaviors.17 Factor 1 of the BHB consisted of seven items with a Cronbach’s alpha of 0.880. Cronbach’s alpha for factor 2 was 0.938 and with eight items. The overall Cronbach’s alpha for the scale of doctors’ inconsiderate behaviors was 0.944. Therefore, the new scale was found to have good reliability.
Univariate Logistic Regression Analysis
Inhabitants’ dual-dimension general evaluation tendency (DET) toward doctors was taken as the outcome variable. Independent variables included demographic variables, such as education catalog, medical insurance type, frequency of medical consultations, medical expenses, annual family income, age, and occupation. Through a univariate logistic regression analysis, the factors influencing inhabitants’ perspectives of the DET were extracted from numerous demographic variables and included education catalog, medical insurance type, frequency of receiving medical services, and medical expenses. Among the categorical variables, education catalog and type of medical insurance, one group was chosen as the control group from each variable, and regarded as a dummy variable. Regarding the education catalog, the group “junior high school and below” was treated as the control group. Regarding medical insurance type, as shown in Table 3, the group “social medical insurance” was treated as the control group.
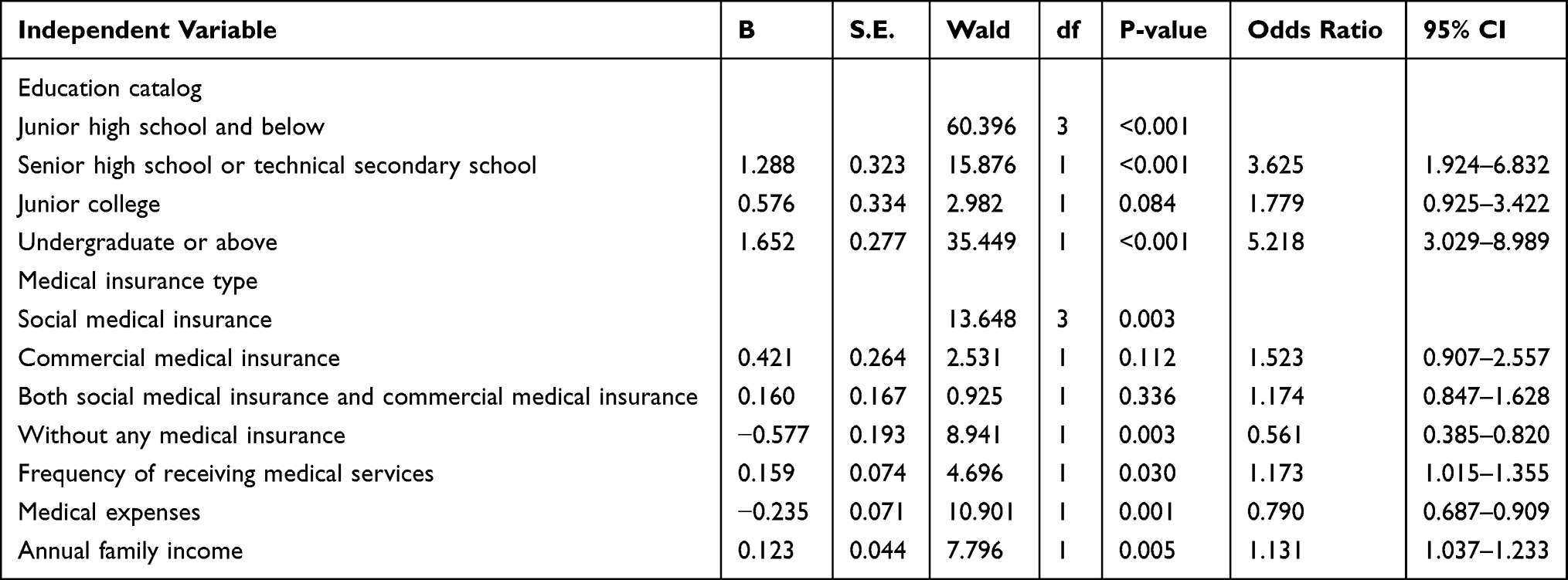 |
Table 3 The Results of Univariate Logistic Regression Analysis on the Factors Influencing the Inhabitants’ General Evaluation Tendency Toward Doctors (n = 1598) |
Multivariate Logistic Regression Analysis
The multivariate logistic regression analysis model included the independent variables, such as education catalogs, medical insurance types, frequency of medical consultations, and medical expenses; and it was identified using the univariate logistic regression analysis. The DET was used as a binary outcome variable. The results showed that the frequency of medical consultations, medical expenses, education catalog, and medical insurance type had a statistically significant impact on the DET (p<0.05; Table 4). The frequency of medical services received by participants (Wald χ2=6.252, p<0.01, OR>1) had a significantly positive impact on the DET, indicating that inhabitants with a high frequency of medical consultations had a higher DET score. Furthermore, participants’ medical expenses (Wald χ2=613.205, p<0.01, OR<1) negatively affected the DET. The results showed that, compared with the “junior high school and below” group, the participants who graduated from senior high School or technical secondary school (Wald χ2=15.545, p<0.01, OR>1), and undergraduate college or above (Wald χ2=1.623, p<0.01, OR>1), had a statistically significant impact on the DET. Additionally, compared to the participants with social medical insurance, participants with commercial medical insurance (Wald χ2=5.869, p<0.01, OR>1) tended to evaluate doctors more positively, and participants without any medical insurance (Wald χ2=8.045, p<0.01, OR<1) tended to evaluate doctors more negatively. The significance test of the whole regression model showed that χ2 = 95.344 (p=0.001, p<0.01), Hosmer-Lemeshow = 4.093 (p=0.769, p>0.05), Cox-Snell R2 = 0.058, and Nagelkerke R2 = 0.081, indicating that the goodness of fit of the regression model was acceptable.
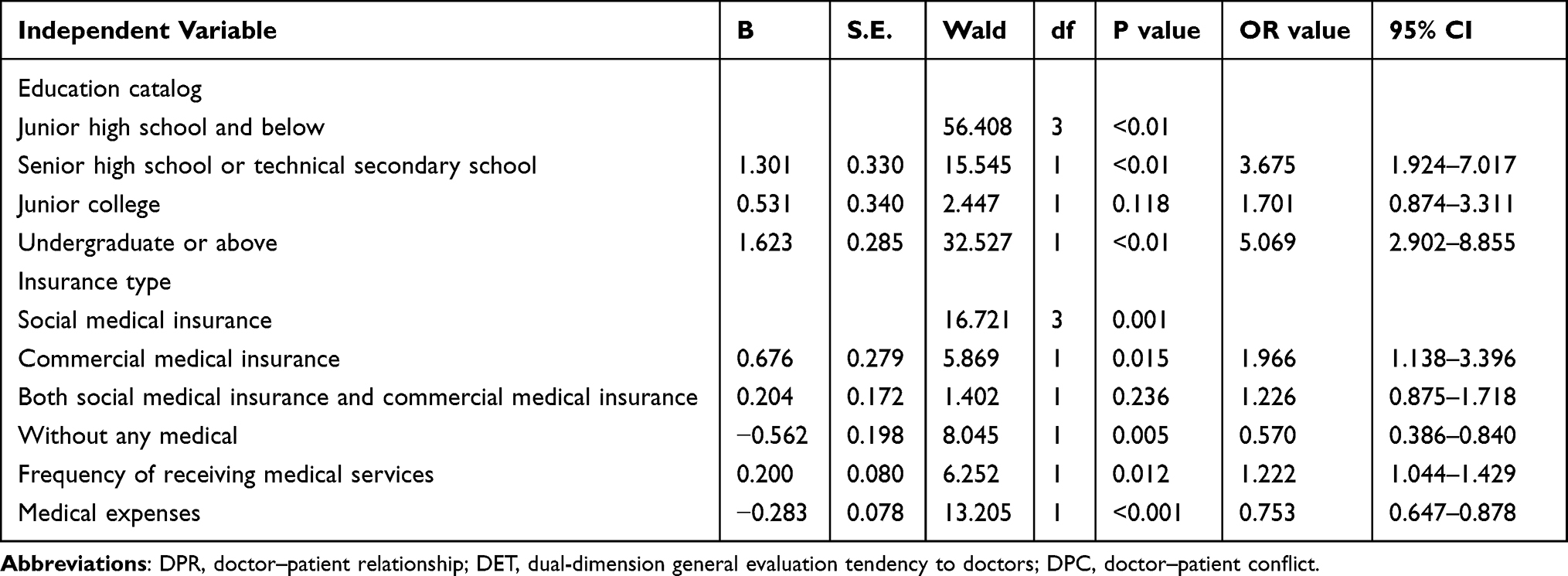 |
Table 4 The Results of Multivariate Logistic Regression Analysis on the Factors Influencing the Inhabitants’ General Evaluation Tendency Toward Doctors (n = 1598) |
Descriptive Statistical Analysis of Status Indicators
Inhabitants’ General Evaluation of DPRs and Their Extent of Trust on Doctors
I in Figure 1 shows that more than three-fifths of the participants tended to evaluate Chinese doctors positively. Additionally, over three-fifths of participants reported greater trust in doctors (II in Figure 1). However, III in Figure 1 clearly indicates that over three-fifths of the participants admitted that the current DPR in China is bad, as reported from the inhabitants’ perspectives.
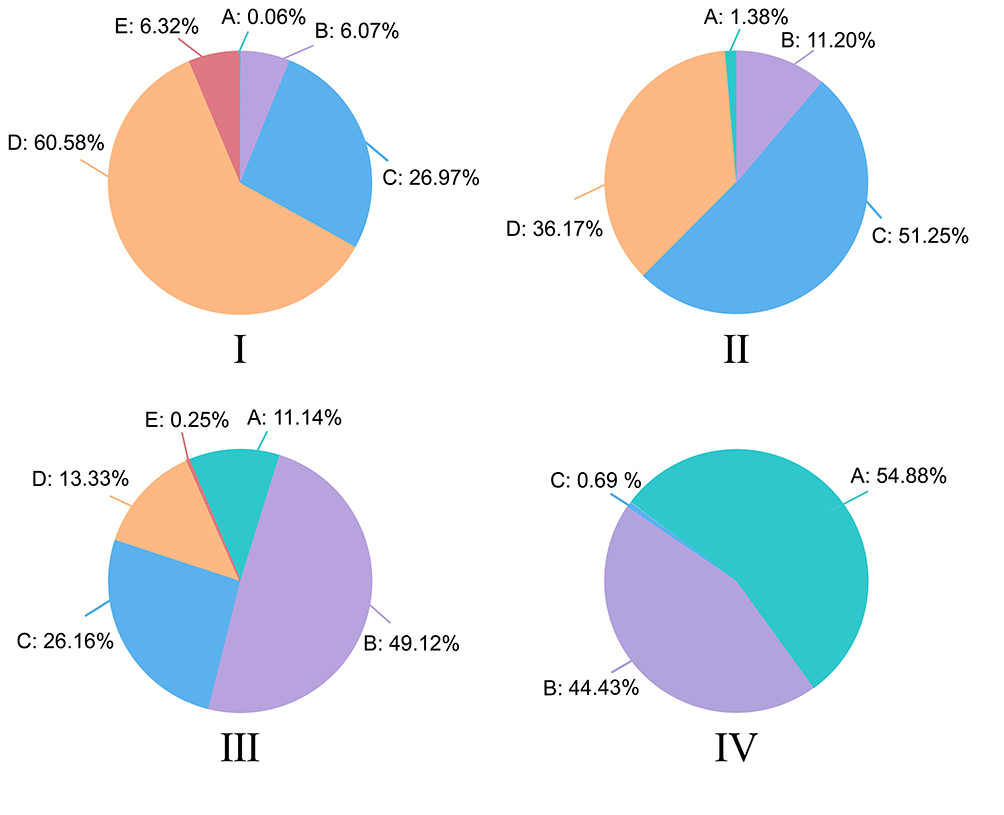 |
Figure 1 Inhabitants’ overall perception of doctor–patient relationship. Notes: (I) In the single choice question “What is your general evaluation about Chinese doctors?” the answers “A. All the doctors are bad,” “B. There are more bad doctors, a few good doctors,” and “C. Good doctors and bad doctors are equal in number” were considered as a negative evaluation tendency. Additionally, two options, “D. There are more good doctors and a few bad doctors” and “E. All the doctors are good,” were treated as a positive general evaluation tendency. (I) shows that more than three-fifth of the participants tended to evaluate Chinese doctors positively. (II) A representative question “Considering your trust in the doctor, what is your opinion about the doctor’s diagnosis and treatment plan?” was used to test the trust extent of participants to doctors. The response options included “A. I do not believe doctors at all,” “B. I do not believe doctors very much, and I think I should find more doctors for help,” “C. I have doubts, but I trust the doctor and will follow the doctor’s plan,” and “D. I trust doctors very much and I firmly implement the doctor’s treatment plan.” The respondents’ degree of trust in doctors expressed by these options was different. The frequency of participants’ choice of each option relatively reflects the overall situation of their trust in doctors. More than three-fifth participants reported greater trust in doctors. (III) “How do you think is the quality of the current DPR?” included five response options of “A. Very bad,” “B. Bad,” “C. Not bad and not good,” “D. Good,” and “E. Very good.” was used to assess the inhabitants’ perspective on DPRs in China. Based on the participants’ responses, the frequency percentage of each option reflected the current DPR status. (III) clearly shows that over three-fifth of the participants admitted that the current DPR in China is bad. (IV) The question “A. Will you take aggressive actions against Chinese doctors in a DPC?” was used to assess the participants’ aggressive intentions. There were three response options. The first response, “B. I will never attack the doctors in a DPC,” indicated that participants were not aggressive toward doctors. The second response, “C. Whether I will attack the doctor in a DPC depends on the circumstance,” indicated that participants held moderate aggressiveness toward doctors. The third response, “I would attack the doctor in a DPC,” indicated that participants were highly likely to attack doctors. As shown in (IV), when doctors ignored the inhabitants, about 54.88% of the participants reported that they would never attack or abuse doctors, and 44.43% would respond depending on the temporal situation; however, 0.69% of the participants reported that they would absolutely attack or abuse doctors. |
Inhabitants’ Perspective About the Practice Conditions of Chinese Doctors
II and III in Figure 2 present a strong similarity in the inhabitants’ evaluation tendency toward Chinese doctors’ income and social status. More than one-fifths of the participants formed the high-score group, indicating their agreement that Chinese doctors’ income and social status were important. Approximately one-fifth of participants, falling in the low-score group, indicated that doctors’ income and social status were not significant from the inhabitants’ perspectives. The high rate of the high-score group is prominent in IV in Figure 2, and almost three-fifths of the participants believed that Chinese doctors’ workload was extremely heavy. About 3.25% of the participants fell in the low-score group.
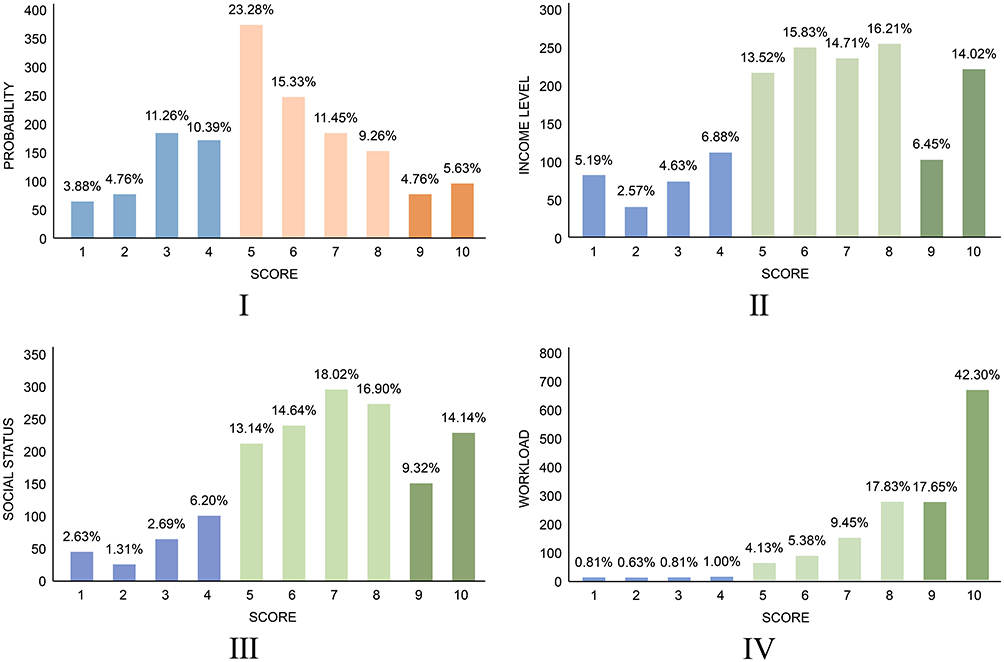 |
Figure 2 Inhabitants’ overall perception of doctor profession. Notes: (I) The probability of doctors experiencing a DPC was measured by a score ranging from 1 (low) to 10 (high). The groups of 1 to 4 score means low score group, the groups of 5 to 8 score means medium score group, and the groups of 9 to 10 score means high score group. The scoring trend of the probability of doctors suffering from a DPC speculated by the participants was similar to a normal distribution. The number of participants who gave a score of 1-2 and 9-10 was similar (about 10%, respectively). The majority of the participants (about two-fifth) concentrated on 5-6 points. (II) The income level of doctors was measured by a score ranging from 1 (low) to 10 (high). The groups of 1 to 4 score means low score group, the groups of 5 to 8 score means medium score group and the groups of 9 to 10 score means high score group. More than one-fifth of the participants formed the high score group, indicating their agreement that Chinese doctors’ income was high. Approximately one-fifth of participants, falling in the low score group, indicated that doctors’ income was not significant from the inhabitants’ perspective. (III) The social status of doctors was measured by a score ranging from 1 (low) to 10 (high). The groups of 1 to 4 score means low score group, the groups of 5 to 8 score means medium score group and the groups of 9 to 10 score means high score group. More than one-fifth of the participants formed the high score group, indicating their agreement that Chinese doctors’ social status was high. Approximately one-fifth of participants, falling in the low score group, indicated that doctors’ social status was not significant from the inhabitants’ perspective. (IV) The workload of doctors was measured by a score ranging from 1 (low) to 10 (high). The groups of 1 to 4 score means low score group, the groups of 5 to 8 score means medium score group and the groups of 9 to 10 score means high score group. The high rate of the high score group is prominent in Figure 7, and almost three-fifths of the participants believed that Chinese doctors’ workload was extremely heavy. About 3.25% of the participants fell in the low score group. |
Inhabitants’ Behavior Tendency Toward Doctors in a DPC Situation
As shown in IV in Figure 1, when doctors ignored the inhabitants, about 54.88% of the participants reported that they would never attack or abuse doctors, and 44.43% reported that would respond depending on the temporal situation; however, 0.69% of the participants reported that they would definitely attack or abuse doctors.
In the multiple-choice question “When you are dissatisfied with the doctor, what will you do,” about 7.51% of participants stated that they would “Tell people around them to discredit doctors,” while only 1.75% and 1.63% would “Abuse doctors on the Internet” and “Attack doctors with words and actions,” respectively. About 57.76% of the inhabitants reported that they would “Complain about doctors by resorting to relevant departments or institutions,” half of the participants expressed that they would tolerate the doctor’s accidental mistake, and 26.66% of the participants reported that they would complain but had not approached to seek help.
Discussion
In this study, we developed a questionnaire on doctors’ inconsiderate behavior from the perspective of inhabitants. We found that education level, frequency of medical treatment, medical insurance, and medical expenses affected inhabitant’s’ evaluation of doctors’ professional reputation. Although the current situation of DPR is strained in China, there appears to be feasible methods to reduce this tension.
From the inhabitants’ perspective, 15 inconsiderate behaviors initiated by Chinese doctors were listed and divided into two dimensions (ie, “human alienation” and “deviant behavior”) (see Table 2). In previous research, Zhang et al18 summarized four main inconsiderate behaviors of doctors based on the patients’ negative general evaluation, including impatience, disrespect, exclusion of patients from decision-making, and disregard of patients’ disease or symptoms. Doctors’ inconsiderate behaviors toward the patients and inhabitants’ perspectives in this study also show similar characteristics. Doctors’ behaviors, services, or practiced habits during diagnosis and treatment, whether good or bad, emphasize the importance of their interpersonal communication ability. For patients in the United States,19 doctors’ honesty, openness, and timely communication are the most important aspects for assessing a good DPR. According to the satisfaction survey, most patients claimed that doctors should provide them with sufficient information and participation rights in the treatment process.20 From the patients’ perspectives, it is insufficient for a good doctor to exhibit excellent professional skills in the workplace while neglecting patients’ emotional needs. Thus, it is essential to ask doctors to reduce “human alienation” and “deviant behaviors.” Generally, doctors have to offer advanced medical technology services to patients with compassionate care and regular inspection of their professional behaviors based on patient-centered principles, such as the Socratic maxim “Know Yourself”.21
The current study found that multiple factors involving inhabitants’ educational level, medical insurance type, frequency of medical consultations, and medical expenses affected inhabitants’ attitudes regarding doctors’ professional reputation. Inhabitants with high-level education, high frequency of medical consultations, and high-quality medical insurance tended to evaluate the doctors’ professional reputation positively. Participants experiencing high medical expenses generally tended to evaluate doctors negatively. These findings are consistent with those of Shi et al,22 who found that the patients’ satisfaction with DPR differed statistically based on age, living area, education catalog, occupation, and medical expenses incurred. Moreover, people with high-level education and greater frequency of medical consultations have the advantage of providing sufficient information about doctors’ profession owing to better individual understanding and frequent interaction, further enhancing their positive emotions toward the hospital industry. Typically, inhabitants having competency in purchasing medical insurance and those with good financial conditions often possess adequate ability to resist risks and are not as vulnerable to the high medical cost burden. On the contrary, inhabitants with an experience of high medical expenses are more likely to divert their dissatisfaction toward doctors and even the hospital industry as a whole. The above findings indicate that the deterioration of the DPR cannot be completely attributed to “bad doctors” or “inconsiderate services” as individual differences in the evaluator group with disparate experiences are relatively large.
We found that 87.55% of the participants considered the social image of doctors to be good, and approximately 87.42% trusted Chinese doctors. However, 60.26% of the participants admitted that the current Chinese DPR was tense, which is similar to Zhang et al’s15 findings (48.89%). In general, our findings suggest that inhabitants held a positive general evaluation tendency toward Chinese doctors, while they had a negative attitude toward Chinese DPR. The reasons why inhabitants hold a contradictory view on the general impression about doctors and the DPR is worth further exploration using an empirical study. Some Chinese media failed to report DPR events from a profound, professional, and objective perspective, which led to the deviation of inhabitants’ cognition toward the hospital industry.23 Yang’s research suggested that media reports had little influence on the perceptions of the causes of tense DPRs, but influenced the inhabitants’ perceptions of the number of DPCs. Hence, media reports significantly influence DPRs. Second, according to the stakeholder theory,24 deteriorating DPRs is not only caused by doctors and patients, but is also greatly influenced by other stakeholders, including hospitals, governments, societies, and businesses. For instance, the price of Chinese medical equipment has been increasing unreasonably owing to business stakeholders. Consequently, patients’ financial burden increases, which deepens their dissatisfaction with doctors and worsens the DPR.25 The causes of the deteriorating DPR should be discussed not only among doctors and patients but also across the medical system and society,26 considering the participation of all stakeholders, which is critical for bottom-up health reforms to improve DPRs in China.27
The present study found that about one-fifth of the inhabitants believed that doctors’ income and social status were considerably high. However, this was found to be disproportionate to the doctors’ heavy workload and high risks of DPCs. Furthermore, about three-fifths of the participants thought that the Chinese doctors’ workload was extremely heavy. Likewise, nearly one-tenth of the participants considered doctors to be at-risk of suffering DPCs. Participants reported that doctors’ work environments were terrible, which is consistent with the doctors’ self-perceptions. Indeed, doctors’ job burnout is strongly related to the deterioration of the work environment.28 A recent study in 2019 indicated that the overall prevalence of burnout symptoms among Chinese doctors was 85.79%.29 Many factors could cause the poor professional environment of Chinese doctors. For instance, some of the main reasons are that China’s high-quality health resources are relatively weak and regional inequality30 results in a huge per capita workload of doctors. Other reasons include the backward salary mechanism of doctors, and the serious outflow of talent.31 The reform of China’s health system is not thorough due to the existence of bureaucratization and fragmentation.32 Fortunately, the current inferior working environment of doctors has not only been recognized by Chinese doctors,33 but has also been acknowledged by Chinese inhabitants according to the current study findings. Thus, the current findings strongly indicate that the Chinese doctors’ working environment requires improvement, and that only focusing on external economic incentives is inadequate. Thus, it is imperative to improve doctors’ internal motivation and intrinsic satisfaction.34
In our study, 54.88% of the participants reported that they would never attack doctors if they were irritated by them in the hospital. About 44.43% of the participants reported being uncertain of whether they would exhibit temporary responses depending on the specific situation at that time. However, only 0.69% of the participants reported that they would choose to take aggressive actions against doctors if they were angered. According to the participants’ self-predicted intention data, we can speculate that Chinese doctors are exposed to a high personal risk environment. The deterioration of DPRs is mainly reflected in the rejection, opposition, and conflict between the relationship status of doctors and patients.35 Thus, poor DPRs can be initiated by emotions or behaviors.36 Patients’ aggressive behavior contributes to the deterioration of DPR in the most severe and violent style. In a DPCs, patients who engage in aggressive behaviors against doctors are directly reacting to a personal safety situation. In a vicious circle, aggressive behaviors initiated by patients toward doctors has become a leading cause of inferior public perception of DPRs.37 Meanwhile, about 57.76% of participants reported that they would initially seek help by appealing to a third party when they encounter a doctor’s unconscionable behavior, which shows that most participants were likely to take an appropriate rational approach to tackle their dispute with doctors. Using third-party intervention appears to be the best way to deal with DPCs based on our findings. However, about 26.66% of the participants reported that they wanted to mediate the dispute in the DPC situation but were unaware of the department from which they could seek help. This contradiction highlights the important role of third-party institutions in the doctor–patient contradiction. As a strong information asymmetry exists in the relationship between doctors and patients,38 it often requires a third party to intervene and settle medical disputes.39 For example, Rui et al40 discussed the important role of medical social workers in third-party mediation organizations for the purpose of managing medical disputes.
Limitations
Although this paper has several contributions, some limitations must be mentioned. First, we used a self-developed and self-administered questionnaire. Although the scientific nature of the questionnaire has been verified with acceptable statistical results, it still has a certain extent of subjectivity without repeated verification by other studies. Second, the cross-sectional nature of the study cannot indicate a causal relationship. Third, by utilizing an online survey, completion of the questionnaire is carried out through the network, which will affect the distribution structure of participants in the population and interfere with the quality of the questionnaire. Fourth, a convenience sample was adopted, which tends to increase the potential sampling bias. Fifth, we used a non-random sampling method, which has certain subjectivity, and does not allow the data to be analyzed by inferential statistics. Therefore, random sampling and longitudinal research designs are necessary in future studies.
Conclusion
This study investigated the status of the overall evaluation of doctors’ professional reputation in China based on the inhabitants’ perspectives. From the two dimensions of “deviant behavior” and “human alienation” in our research, we listed 15 inconsiderate behaviors of doctors based on the perspectives of Chinese inhabitants and developed a questionnaire. Additionally, we found that inhabitants with a high education level, high frequency of medical consultations, high quality of medical insurance, and high medical expenses were more likely to evaluate doctors’ professional reputation positively. Moreover, the findings revealed that inhabitants held positive general evaluations of doctors and a high degree of trust in them; however, the Chinese inhabitants acknowledged the terrible working environment of doctors and tense DPRs. Doctors’ high income and social status obtained broad acceptance from inhabitants. Concurrently, the findings revealed that the Chinese doctors’ workload was extremely heavy, which was observed by inhabitants. Although the inhabitants expressed sympathy for the professional environment of doctors, some inhabitants claimed that they would behave aggressively if they were dissatisfied with their doctor. These findings seem to imply that inhabitants hold complex and contradictory attitudes toward and perceptions of Chinese doctors. Fortunately, most inhabitants were rational and asserted that they would seek help from third-party organizations in a DPC situation.
Acknowledgments
The authors would like to thank all individuals who voluntarily participated in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zhang L, Cheng G, Song S, et al. Efficiency performance of China’s health care delivery system. Int J Health Plann Manage. 2017;32(3):254–263. doi:10.1002/hpm.2425
2. Yip W, Fu H, Chen AT, et al. 10 years of health-care reform in China: progress and gaps in Universal Health Coverage. Lancet. 2019;394(10204):1192–1204. doi:10.1016/S0140-6736(19)32136-1
3. The Lancet. Protecting Chinese doctors. Lancet. 2020;395:90. doi:10.1016/S0140-6736(20)30003-9
4. Sun T, Gao L, Li F, et al. Workplace violence, psychological stress, sleep quality and subjective health in Chinese doctors: a large cross-sectional study. BMJ Open. 2017;7. doi:10.1136/bmjopen-2017-017182
5. Zhang S-E, Liu W, Wang J, et al. Impact of workplace violence and compassionate behaviour in hospitals on stress, sleep quality and subjective health status among Chinese nurses: a cross-sectional survey. BMJ Open. 2018;8. doi:10.1136/bmjopen-2017-019373
6. Chinese Medical Doctor Association. Chinese physicians’ practice status white paper. Beijing, China; 2018.
7. Zolnierek KBH, DiMatteo MR. Physician communication and patient adherence to treatment: a meta-analysis. Med Care. 2009;47(8):826. doi:10.1097/MLR.0b013e31819a5acc
8. Tucker JD, Wong B, Nie J-B, Kleinman A. Rebuilding patient-physician trust in China. Lancet. 2016;388(10046):755. doi:10.1016/S0140-6736(16)31362-9
9. Lv H, Wang J, Xing X, et al. Prevalence and influencing factors of medical dissatisfaction experiences in Chinese hospitals: a cross-sectional study. Patient Prefer Adherence. 2021;15:523–532. doi:10.2147/PPA.S290651
10. Qiao T, Fan Y, Geater AF, Chongsuvivatwong V, McNeil EB. Factors associated with the doctor-patient relationship: doctor and patient perspectives in hospital outpatient clinics of Inner Mongolia Autonomous Region, China. Patient Prefer Adherence. 2019;13:1125–1143. doi:10.2147/PPA.S189345
11. Schouten BC, Meeuwesen L. Cultural differences in medical communication: a review of the literature. Patient Educ Couns. 2006;64(1–3):21–34. doi:10.1016/j.pec.2005.11.014
12. Dawes J. Do data characteristics change according to the number of scale points used? An experiment using 5-point, 7-point and 10-point scales. Int J Market Res. 2008;50(1):61–104. doi:10.1177/147078530805000106
13. Bova CA, Fennie KP, Watrous E, et al. The health care relationship (HCR) trust scale: development and psychometric evaluation. Res Nurs Health. 2006;29(5):477–488. doi:10.1002/nur.20158
14. Hui Y, Hongqi W. Reliability and validity evaluation of the Chinese version of PDRQ-15. Chin Med Ethics. 2011;24(03):350–353.
15. Costello AB, Osborne J. Best practices in exploratory factor analysis: four recommendations for getting the most from your analysis. Pract Assess Res Eval. 2005;10(1):7.
16. Shlens J. A tutorial on principal component analysis. arXiv preprint arXiv:14041100. 2014. doi:10.13140/2.1.1593.1684
17. Tavakol M, Dennick R. Making sense of Cronbach’s alpha. Int J Med Educ. 2011;2:53. doi:10.5116/ijme.4dfb.8dfd
18. Zhang W, Deng Z, Hong Z, et al. Unhappy patients are not alike: content analysis of the negative comments from China’s good doctor website. J Med Internet Res. 2018;20:e8223. doi:10.2196/jmir.8223
19. Mechanic D, Meyer SD. Concepts of trust among patients with serious illness. Soc Sci Med. 2000;51(5):657–668. doi:10.1016/S0277-9536(00)00014-9
20. Coulter A, Fitzpatrick R. The patient’s perspective regarding appropriate health care. In: The Handbook of Social Studies in Health and Medicine. London: Sage; 2000:454–464.
21. Hurwitz B, Vass A. What’s a good doctor, and how can you make one? BMJ. 2002;325(7366):667–668. doi:10.1136/bmj.325.7366.667
22. Shi J, Jiang Y, Pei H, et al. A surveying study on social satisfaction to current doctor-patient relationship in China. J Serv Sci Manage. 2015;08(5):695–702. doi:10.4236/jssm.2015.85071
23. Zhang T, Xu Y, Ren J, et al. Inequality in the distribution of health resources and health services in China: hospitals versus primary care institutions. Int J Equity Health. 2017;16(1):42. doi:10.1186/s12939-017-0543-9
24. Wu LX, Qi L, Li Y. Challenges faced by young Chinese doctors. Lancet. 2016;387(10028):1617. doi:10.1016/S0140-6736(16)30202-1
25. He AJ. Maneuvering within a fragmented bureaucracy: policy entrepreneurship in China’s local healthcare reform. China Q. 2018;236:1088–1110. doi:10.1017/S0305741018001261
26. Wang J, Xie F, Yin D, et al. A cross-sectional study of job burnout, psychological attachment, and the career calling of Chinese doctors. BMC Health Serv Res. 2020;20(1):1–11. doi:10.1186/s12913-020-4996-y
27. Ma S, Xuehu X, Trigo V, Nelson JC. Curing doctor-patient relationships (DPR) in China. J Health Organ Manag. 2017;31(1):110–124. doi:10.1108/JHOM-09-2016-0165
28. Sun J, Liu S, Liu Q, et al. Impact of adverse media reporting on public perceptions of the doctor–patient relationship in China: an analysis with propensity score matching method. BMJ Open. 2018;8(8):e022455. doi:10.1136/bmjopen-2018-022455
29. Mitchell RK, Agle BR, Wood DJ. Toward a theory of stakeholder identification and salience: defining the principle of who and what really counts. Acad Manage Rev. 1997;22(4):853–886. doi:10.2307/259247
30. Wall LL, Brown D. Pharmaceutical sales representatives and the doctor/patient relationship. Obstet Gynecol. 2002;100(3):594–599. doi:10.1016/S0029-7844(02)02150-6
31. Liu Y, Bai J. The research or current status and causes of medical disputes in part of hospitals in Urumqi. J Xinjiang Med Univ. 2010;33(5):554–575.
32. The Lancet. Violence against doctors: Why China? Why now? What next? Lancet. 2014;383:1013. doi:10.1016/S0140-6736(14)60501-8
33. Swider BW, Zimmerman RD. Born to burnout: a meta-analytic path model of personality, job burnout, and work outcomes. J Vocat Behav. 2010;76(3):487–506. doi:10.1016/j.jvb.2010.01.003
34. Zhang S, Wang J, Xie F, et al. A cross-sectional study of job burnout, psychological attachment, and the career calling of Chinese doctors. BMC Health Serv Res. 2020;20(1):1–11. doi:10.1186/s12913-020-4996-y
35. Jing W, Otten H, Sullivan L, et al. Improving the doctor-patient relationship in China: the role of Balint groups. Int J Psychiatry Med. 2013;46(4):417–427. doi:10.2190/PM.46.4.g
36. He AJ, Qian J. Explaining medical disputes in Chinese public hospitals: the doctor–patient relationship and its implications for health policy reforms. Health Econ Policy Law. 2016;11(4):359–378. doi:10.1017/S1744133116000128
37. Schouten BC, Meeuwesen L. Cultural differences in medical communication: a review of the literature. Patient Educ Couns. 2006;64(1–3):21–34. doi:10.1016/j.pec.2005.11.014
38. Barile S, Saviano M, Polese F. Information asymmetry and co-creation in health care services. Australas Mark J. 2014;22(3):205–217. doi:10.1016/j.ausmj.2014.08.008
39. Zhao M. Evaluation of the third-party mediation mechanism for medical disputes in China. Med & L. 2011;30:401.
40. Rui H, Lin W, Jingping L, et al. The mediating effects of job satisfaction on the association between doctor-patient relationship and OCB among physicians in China. Iran J Public Health. 2018;47(5):698.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.