")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 12
“We feel included”: education and inclusion of health care staff with minority language in elder care
Authors Krohne K, Døble B, Johannessen A , Thorsen K
Received 27 June 2018
Accepted for publication 15 October 2018
Published 20 December 2018 Volume 2019:12 Pages 9—19
DOI https://doi.org/10.2147/JMDH.S178458
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Kariann Krohne,1,2 Betty Døble,1,2 Aud Johannessen,1,3 Kirsten Thorsen1,2,4
1Norwegian Advisory Unit on Ageing and Health, Vestfold Hospital Trust, Tønsberg, Norway; 2Department of Geriatric Medicine, Oslo University Hospital, Oslo, Norway; 3Department of Nursing and Health Sciences, Faculty of Health and Social Sciences, University of South-Eastern Norway, Vestfold, Norway; 4Norwegian Social Research (NOVA), Oslo Metropolitan University, Oslo, Norway
Background: In Norwegian elder care, an increasing percentage of the health care staff has a migrant background. “The aging and nursing care ABC” educational program offers multicomponent training for municipal care staff to systematically improve their competence in elder care. The program consists of written material organized into booklets, regular multidisciplinary reflection group meetings, and a full-day workshop in each semester. In 2017, a Norwegian municipality included migrant health care personnel in an educational Minority ABC-model (Min. ABC), systematically focusing on processes relevant for interaction between majority and minority health care staff.
Aim: To investigate the experiences of the participants in the Min. ABC-model, focusing on the processes and relationships between native participants with Norwegian language and migrants with other lingual backgrounds.
Method: The study has a qualitative design, and draws on four focus group interviews, one group interview, and four individual interviews with a total of 23 female Min. ABC-model participants. Data were analyzed using an approach outlined by Corbin and Strauss.
Results: Our analysis resulted in six main themes: 1) reaching equality, 2) sharing experiences, 3) communication and language, 4) relations to the elderly, 5) differences and discrimination, and 6) lessons learnt.
Conclusion: Our findings indicate that the Min. ABC-model of the ABC program contributes to better the competence and interaction among personnel with migrant and native lingual backgrounds. The participants describe increased inclusion at work, as well as integration into a more holistic form of teamwork in elder care.
Keywords: educational program, elder care, health care professionals, integration, migrant and native personnel, staff training
Introduction
Two demographic trends dominate the industrialized societies today: aging of the population and increased migration.1 In Norway, like in other countries, these trends intersect in the welfare sector, especially concerning care for the elderly.2 The following vital questions arise: 1) how to develop qualitatively good person-centered care for the elderly in Norway? and 2) how to best educate and integrate health care personnel with a minority background in the elder care sector? There is a great need for studies combining gerontological and migration perspectives – a field that seems neglected.1,2
Migration implies both that migrants will age and become elderly people in need of services, and labor migration – people with migrant background working in elder care. Labor migration in elder care has become a global and multifaceted issue,3 a fast spreading phenomenon. Torres notes in a review that there is scarce research on migrant work in the public elder sector.4 Most of the migrant workers are women.5,6 There is a lack of models and methods, as well as knowledge on how to educate and increase the competence and inclusion of people with migrant backgrounds in the teams working in the public elder care. Norway has had a rapid increase in the number and percentage of inhabitants with immigrant backgrounds, and a corresponding increase in people with this background among personnel in the health care sector. In 2016, 6,98,500 people with immigrant backgrounds lived in Norway, out of a total population of 5.2 million.7 In the past four decades, the country has been transformed from having a rather homogenous population to becoming a multiethnic country, with inhabitants from 220 countries.8 In the next 40 years, the prognosis is that the immigrant population will increase from 13.4% to somewhere between 19% and 27%.9
About half of the migrant population is from European countries, the other half are mostly from Asia and Africa, specifically Somalia, Eritrea, Afghanistan, and Iraq.10 Their educational resources and competence vary greatly, from analphabets to people with academic degrees. Health personnel with a minority background risk meeting language prejudice and discrimination.11,12 They are hampered by their lack of fluency in the Norwegian language and knowledge of the society and may be met with distrust.12 The integration of migrant workers is a challenge. The Norwegian Minister of Trade, Industry and Fisheries at the time of this writing, Torbjørn Isaksen, refers to the urgency of the situation in general, when he exclaims that, “There is a pressing need to do something about integration, which seems to function miserably many places.”13 Also, the migrant population is aging, and they will increasingly need health care during this process.14–16 This influx of people – aging over time – has great implications for the welfare state, health and social care, and policy planning.17 The supply of necessary care will imply great challenges for the health care services in Norway within what is called the Nordic welfare system, which is dominated by public services.18,19
The aging of the migrant population parallels the rapid increase in the elderly population in total, especially among the eldest most in need of services. The number of people ≥80 years is estimated to increase from 2,20,000 to 4,40,000 in the next two decades.7,20 Obviously, the country will experience a great gap between needs and supply of services and care, which is in line with other “aging” European countries.1,15,21
At the same time, the migrant groups may potentially be an important personnel source for the elder care sector, both in home care services and long-term care. An increasing percentage of workers in elder care in Western Europe are migrants, both in the private and public sectors; however, the proportion varies greatly. In the home care sector, the proportion of migrant workers varies from 18% to 27% in English-speaking countries to >70% in Italy.22–24 In the Nordic countries, the proportion is smaller than in Southern European countries, like Italy, where most of the home care for the elderly is privately funded. The Nordic countries have a model of a dominating public welfare sector, including care for the elderly.3,19
In Norway, there are great challenges in the recruitment of certified health care personnel,21,25 and the Norwegian Government21 emphasizes the migrant resources in their policy guide for recruitment, increased competence and professional development in the health care and elder services, especially in the municipalities. Some Norwegian counties are providing financial support for the municipalities in order to qualify people with a migrant language background to become health workers. In 2015, 14% of all health workers in Norway had a migrant background.26 An important aim is to integrate them into well-qualified, well-coordinated, and well-functioning teams, stimulating the personnel group by giving holistic person-centered care. This article reports from a project examining the experiences of health care personnel in an educational program modified to systematically include participants with migrant backgrounds.
The ABC-model
The ABC-model is a national interdisciplinary educational program focusing on aging and the needs of the elderly, provided for personnel in the health care sector in the Norwegian municipalities.27 Since its beginning in 2007, 96% of all municipalities in Norway have had health care personnel participating in the ABC-model. ABC participants have a variety of educational backgrounds, positions, and employments (full time, part time, and temporary employees). There are several ABC programs in the ABC-model. A common denominator for these educational programs is that they present information about aging, age-related diseases and disabilities, prevention, treatments, services, and examples of practices to reflect upon and discuss, as well as principles for best practices. The model is used nationally; it is financed by the Norwegian Directorate of Health, a state level organization under the Ministry of Health, and is outsourced to the Norwegian National Advisory Unit on Aging and Health, which manages and implements the program.27,28 “The aging and nursing care ABC” consists of three parts. First, a collection of 13 booklets is distributed to each participant. Second, six to eight participants participate in monthly reflection groups, taking place at the workplace, to discuss the topics in the booklets after having read them beforehand. Empirical examples and questions are presented to discuss and reflect upon, and to relate to their own practice. Third, two workshops are offered annually. The core activity in the ABC-program is the self-run reflection groups. The management of the groups may differ out of convenience and preference; some groups appoint a leader, others rotate the leadership or pursue without a leader. The costs of the workshops, booklets, and work time used by the staff are covered by the municipalities.
The Minority ABC-model: the ABC-program adapted to migrant health care personnel
The Minority ABC (the Min. ABC), which this study concentrates on, was developed in a small rural municipality in Mid-Norway, where they had experienced difficulties with recruiting enough personnel to the health care services. The municipality administration decided to educate and employ migrant inhabitants. Many migrants wished for work and economic independence. The Resource Center for Adult Education at the county level firstly adapted the ordinary secondary education for health workers at the high school level to a special version for people with minority language and varying competence in Norwegian. The Resource Center deliberately focused on language and communication. The reason for this focus was an intention to address two general challenges for migrant health care workers: mastering of the Norwegian language and their ability to communicate adequately with native health care personnel.
After having completed this certified health care education for people with minority backgrounds, most of them gained employment in the municipal elder care. Gradually, challenges with language, communication, understanding, norms and interactions with colleagues, patients, and users, were exposed. The Resource Center administration recognized that health workers with a minority background needed further follow-up at their work place. They decided to modify the ordinary ABC-program to the Min. ABC-model and use it for development and education of the health workers, where the participants could discuss and reflect on the information and their own practices.
Special aspects of this model are that two persons in every ABC-group should have a minority language as their primary language. They received a pocket dictionary on Norwegian words/concepts used frequently in health care services and were offered reading support. The group leaders had a bachelor’s degree. The leaders were also given a special introduction to the Min. ABC-model and they received lectures on aspects of minority languages. The aim was to obtain better inclusion of personnel with minority language, and more well-functioning working groups. Increased knowledge and competence in elder care among the participants should lay the groundwork for a more shared and holistic understanding and practice. In January 2016, 34 participants in the municipality started up with a workshop and continued with the reflection group meetings in four ABC-groups using the Min. ABC-model. They had another workshop, and the education ended in Spring 2017.
Aim of the study
The aim of the study was to investigate the experiences of the participants in the Min. ABC-model focusing on the processes and relationships between participants with majority and minority lingual backgrounds.
Methods
Qualitative research methods are helpful in providing knowledge of phenomena in areas where little is known.29 Here, focus groups and individual interviews were performed with health care personnel who had participated in the Min. ABC-model in a small rural Norwegian municipality.
The participants in the study
The 34 participants in the Min. ABC-model were asked to participate in the present study. A total of 24 people, all women, aged 22–61 (mean 45) years, agreed to participate. The reasons for not participating are not known. The participants were interviewed in 2017 within a month after they had completed the year-long Min. ABC-model. The informants had worked in the health sector from 4 to 38 years. Four participants were nurses, 2 were social educators, and 18 were health workers. All were recruited from the rural municipality where the program was conducted by a leader.
In the study the recruited informants were interviewed in four focus groups with respectively six, five, three, and three informants, one group interview with two participants and five individual interviews.
The largest focus group (group 1) in the study consisted exclusively of migrant informants from three non-European countries. The informants in the other focus groups were native Norwegians. The reason for this was to give the participants an occasion to speak freely about their experiences.30 One interview was conducted as a group interview – with only two participants. In a group interview with few informants, like here, the moderator has a somewhat different role than in a larger focus group, where all participants should be included in a discussion.30 Five interviews were conducted individually by telephone, since some informants were not able to participate in the focus groups. One informant, a health worker who was interviewed individually, withdrew from the study after the interview was performed. This interview was erased and is not part of the study’s data. The total sample thus consists of 23 participants.
The focus group sessions and the group interview took place in a municipality meeting room in May 2017. AJ moderated these and encouraged participants to discuss the questions freely. The focus group sessions and the group interview were observed by KK, who also posed complementary questions toward the end of each session. AJ performed the individual interviews. The interviews were recorded and transcribed verbatim by secretarial staff. A quality control of the transcripts – relistening to the interviews and comparing them to the written transcripts – was performed by KK and AJ.
The interview guide for the focus groups and group interview had ten main questions (Table 1) concentrating on the informants’ experiences of participating in the program, and their reflections on how municipalities might organize future groups. Depending on the replies, the aspects and ideas raised by the informants led to probes – further questions to obtain additional information. The individual interviews lasted from 16 to 25 minutes, and the four focus group interviews and the group interview lasted from 55 to 77 minutes.
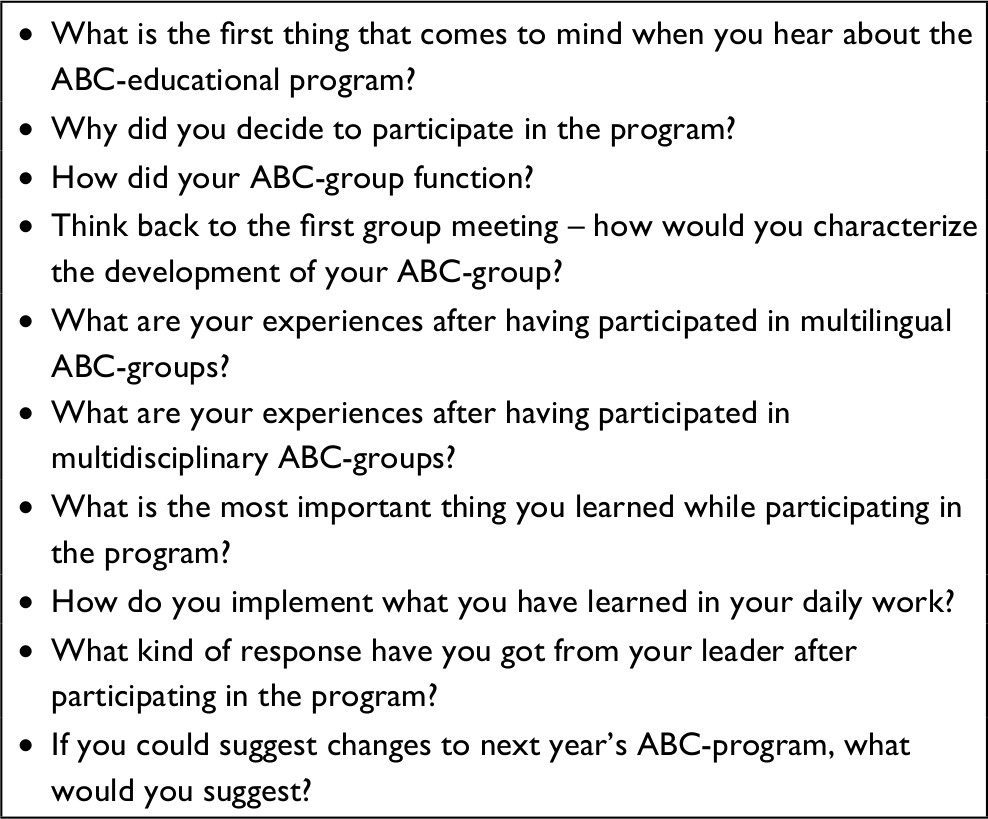 | Table 1 Questions for the interviews |
Analysis
The analysis was performed in line with the strategies for qualitative data analysis described by Corbin and Strauss.31 They underline in their book Basics of Qualitative Research that thick descriptions are valid and valuable reasons for doing qualitative research, searching for new knowledge, without intention of theory construction (p. ix). Our study is descriptive, exploring experiences of participation in an educational program.
Authors KK, AJ, and KT had principal responsibility for the analysis; however, the process was continuously discussed with BD. To get an overview, we condensed every interview, making a shorter version, showing the salient points in the discussions and accounts. The first analytical step (open coding) was to read all the condensed interviews open-mindedly for relevant codes. These were a mix of codes at different levels: emotions, reactions, actions, reflections, and narratives about processes, themes, and situations. Then, the codes were compared to find the most relevant higher level of codes (axial coding) for the whole group. At the same time, subcategories and variations were noted. At this stage of the analysis, an agreement on higher level codes was reached by discussions and reflections among the researchers. In the process, the researchers continuously related to the empirical material, analyzing it both vertically, going back and forth in the material of one informant, and horizontally, comparing the informants on different codes.
Ethics
This study follows the ethical principles outlined in the Declaration of Helsinki32 and was approved by the Norwegian Centre for Research Data. In line with instructions from the Norwegian Centre for Research Data, all informants were informed about the study’s purpose and the right to withdraw in writing and verbally, and prior to the interviews their written informed consent was collected.
Results
Six main categories summarize the participants’ most significant experiences of participating in the Min. ABC. The categories present the processes and thematic contents of the meetings, as the participants recount their experiences. These are as follows: 1) reaching equality, 2) sharing experiences, 3) communication and language, 4) relations to the elderly, 5) differences and discrimination, and 6) lessons learnt. In the presentation of the empirical results, the background of the participants will be denoted minority or migrants for the immigrants, and majority or native for those with Norwegian backgrounds.
Reaching equality
The participants appreciated the ideal of equal participation in the group and they all participated in the group’s strivings to achieve equality. Some of the Min. ABC-groups used the appointed group leader; intermittently, some group participants took turns functioning as group leaders. The participants valued having an experienced, educated, and prepared leader, taking responsibility for the interactions in the groups – for the talkative as well as the more silent participants, especially those with a minority background: “To have a group leader did function very well for us, really.”
They saw this leadership as being important for “balancing” the participants and to make sure that all members got their share of the time and expressed themselves. Some had to be nudged a bit to get on the stage. Members of the minority group tell how they started out being shy and silent. However, “Our leader, she is very direct, and said: ‘Don’t be afraid of giving your opinion!’ Then we all got confirmation. The leader was very OK, we were lucky!” Another minority participant pointed at “our culture” as a reason for being silent:
The leader said; “Just say your opinion!” But is about our culture, for we are not saying so much, “I admit that. It is culture. But the Norwegians are clever and just say what they mean, and present their opinion, just like that! We say little. We are very good at listening.”
One in the migrant group pointed out: “We sit still, and they ask: ‘What do you do in your country? What do you mean?’ and stare at us. And yes – we have to answer!” Another joined in: “Then we became… we became included more and more, and they were interested in what we thought. That was really good! We were not afraid of talking anymore.” To feel safe is fundamental for daring to express themselves and sharing experiences and opinions. As they report, the organizing of the Min. ABC-groups has given a platform of security to all participants, of special importance for caregivers with minority background. The interviewer asked: “How have the meetings evolved?” and received the following answer from a native participant: “We all participate more, and all are much more secure and have confidence in each other. Now no one finds it difficult to talk. All are engaged!” They have discovered that, “We are not so different, though we have separate roles, really.”
The leaders seem to have been essential for organizing and practicing the basic principles of equality – that all shall participate, all opinions are listened to, and all are taken seriously. The leaders have had the authority to support positive group processes and stimulate engagement and enthusiasm. The task is complicated and may take some time. The principles must be revitalized along the course.
Sharing experiences
The foundation for the participants’ feelings of satisfaction is the interactive, reflective learning processes that take place in the group while sharing experiences. In these groups, health care personnel from different sectors and working places in the municipality participate, with different educational background, positions, lengths of practice and experiences, within the same municipality. Some worked in home care, others in nursing homes.
As shown, a fundamental premise for sharing experiences in the group is the feeling of being a valuable group member, whatever their differences otherwise are, like in language and national/cultural background. Some are or have been leaders, some are veterans, others are newcomers; some feel they are experienced in elder care, others are still insecure after just having completed their education. The differences are appreciated as a source for sharing varied experiences, to learn from each other. One participant says
It was good that we represented different services, sectors, and places, then we got more experiences, and did learn much. Sharing experiences, both positive and negative. And we have discussed and reflected on many different topics. This is my first thought.
Another informant added: “The many different opinions on the themes were the most valuable for me.” To see issues from other perspectives, and hear the others propose varied and different solutions were greatly appreciated. The interdisciplinary participation was in accordance with how they normally worked. “It was positive, but nothing special.” “We are all colleagues, regardless of what title the person has.”
One important reason for the positive evaluation of the groups was the reflection time, since such occasions are rare and often nonexistent in their daily work because they often feel busy and sometimes overburdened. One informant told that they at her department had meetings where they discussed “Problems, challenges and solutions, and ethical dilemmas”, but later there was no more time for it. Another participant (minority background) remarks, “We need to get more knowledge, and have time to talk to each other, and discuss. Not only work and work! We do not have much time to talk when we are at work.” Not all departments have regular staff meetings, and the temporary employees rarely meet there.
To learn from older and more experienced colleagues is appreciated. A woman with a minority background underlines: “The older ones have worked many, many years and know how to react in different situations. We who are newcomers do not know what to do if the patients are restless and behave improperly.” The newcomers learn from the more experienced how to handle problematic situations. They tell that they have learned “tricks” to cope with demanding situations and get confidence and support from the group members to just do it. They acquire more authority, self-confidence, as well as cleverness and imagination.
Communication and language
Both colleagues and patients are dependent on competent and correct communication so that messages are understood, and requests carried out. An overall experience among the participants with a native background, and one of the main reasons the program was started, is that the migrants’ qualifications in native language are more lacking than it should be. Also, the migrant workers admitted they can have “problems with the language, the culture and various things”. Before the Min. ABC, these themes had been muted and were difficult to touch upon for all involved. That the people with migrant backgrounds were certified health workers should guarantee that they mastered the Norwegian language at an acceptable level. This is not so, and to admit it is not easy. The native participants have avoided criticizing the migrants’ work and their language skills directly, and this might have silenced communication about care practice between them. Feeling the acceptance and the security in the group, the members have together discussed the communication and language challenges, the implications and consequences, and how to handle them.
The language problems interact with other aspects of the migrants’ cultural background and minority status in Norway. At home, the migrants usually speak English or their native language and adhere to their national media; at work they may join minority groups speaking their native language. To be a temporary employee makes it even more difficult to learn Norwegian; they do not feel secure enough to ask about what they do not understand. Their accent sometimes causes great difficulties, especially for the patients. The migrant participants have learnt Norwegian with the local dialect (even difficult to understand for native people from other regions in Norway), and they speak this dialect with an accent from their homeland. The resulting accent seems to be difficult to understand for other people, especially the elderly, often with reduced hearing capacity. One migrant participant underlines the importance of speaking clearly to people with dementia:
When we are with people with dementia, it is absolutely necessary that we speak Norwegian. If we speak another language, it stirs anxiety and agitation. For they do not understand, they do not understand what I mean and what we are talking about. So that is very important in my job: Language. Language. Language!
Many elderly patients and their families prefer to talk to personnel speaking the Norwegian language well, which favors the natives. The line between rational behavior and discrimination becomes blurred. One participant reported on what she has learnt: “Now we show our knowledge and what we shall do, and we do talk distinctly when we talk to them. We try to speak slowly, and if they do not understand, we repeat. But we do have to take time and listen.”
What was discussed in all groups was the migrants’ tendency to respect authorities. The participants agree that the minority health workers often consent to what the leaders say, or what they think they have said. They are not habituated to ask a superior to repeat the message more clearly, to voice another opinion, to be in dialog or to oppose those more educated and experienced. They are timid and reluctant to show what they do not understand and know. In communication, they conceal their lacking language skills. At the same time, they feel overlooked. For their native colleagues, the lacking language competence and tendency to consent imply that they feel they cannot trust that information is correctly understood, and tasks successfully performed. They often follow up the migrants’ work, control, educate, and take on extra responsibility, which is felt as a burden in busy daily work. Often, the migrants do not feel able to take phone calls, or the native health workers do not trust them to do so, causing them to prefer having one native and one migrant health worker together when there are only two on duty. A participant (minority background) voices their collective learning from the course: “We must ask, if we do not understand. Ask and repeat!”
Relations to the elderly
In the groups, the participants reflect upon variations in the health system and old age care, and fundamental differences in the way the elderly are seen and respected. Since they all share knowledge about the Norwegian elder care from former education, practice, and the Min. ABC-program, the migrant participants are stimulated to tell about relationships with the elderly, norms and practices from their homeland – silenced stories. The supportive and sharing atmosphere in the group encourages them to share their experiences.
We want them (the elderly) at home, see? It is not only about money, that we cannot afford to buy nursing home care for them. We have learnt that we should be fond of our parents, we must have respect for elderly people. When we were small, they looked after us. And in old age we have to look after them.
Another reformulates: “When we were young, they changed diaper on us, when they are old, we change diaper on them.” (They all laugh). A participant summarizes their norms and feelings: “They (the elderly) have supported us throughout life and helped us as a family, so we enjoy that they live together with us.”
One migrant informant reflects on the individualistic lifestyle she sees in Norway: “I just have to say it. I think there are many lonely people here in this country.” She observes the differences: “Even if there are many neighbors, they are busy working, or going to their cottages, or travelling. Here people are very preoccupied with themselves, but in my country, we can visit neighbors and talk to them.”
That they have internalized a respect for elderly people brings about some consequences in care situations. “We have much respect for elderly people. We are …a little bit cautious.” Some majority informants tell that personnel with minority backgrounds have difficulties refusing to do what old people ask for, even if it is unreasonable. To say “no” becomes a problem. The Min. ABC-groups give them support to set professional limits to overwhelming demands – a no is allowed.
Differences and discrimination
Getting to know each other in the group – “When they know us, and we know them” – gives a safe platform of trust to discuss experiences related to ethnic differences and discrimination. The minority group tells how they are met by the patients. The first meeting clearly is a situation where their differences are seen face to face. Both parts may be insecure. One participant with a minority background mentions: “Maybe the first time when we come to a patient, when we are at their home, maybe they feel that the language is unknown, the culture, the face or something. Maybe they feel anxiety. But it becomes better and better.” Another participant underlines the color of their skin. “The first thing is our outlook. We are dark, true? They are elderly people, but we are different anyway.” They tell how they gradually get used to and accept each other.
However, many instances of badgering and racial discrimination were reported in the groups. One informant with a native background explains:
We do hear directly from them how they are met with negative attitudes, abuses and words. It is so heartbreaking that you just must do something about it. Of course, if the patient is not demented, or psychotic. But if they are normal, you can’t just disregard it, you must act. We teach them that they must set limits.
One from the majority group adds that they also meet abuses from the patients, “You are not alone,” but the content of the abuse differs.
The Min. ABC-groups have supported people with minority backgrounds to mark limits to abuses and discrimination, and colleagues have also interfered directly. A migrant participant tells about her tactic to handle initial skepticism:
I have tried to go to a ninety-year-old lady. She asks: “Who are you? You are not from this country?” I say “No, but I have lived here for many years. I am a local.” I then ask: “Where do you come from?” I can hear from her dialect that she is not a local. “Then we are migrants both of us,” I say. Then I may come in.
She has ingeniously transformed the situation and evoked common identities as a basis for a good relationship.
Lessons learnt
The participants were unanimously positive about the program, and their evaluations were dominantly on the very positive side. They expressed that the program was “seriously good”, “very interesting”, “very good”, repeated and reported with references to different aspects of the course. One participant remarked how the course has given “vitamin for our practice”. A participant with a minority background underlined that the Min. ABC-model has been of special value for them. To demonstrate their enthusiasm, they often added that they missed the group, and wished they could attend a new one the next year, saying “The time passed so quickly.” Looking back, some mentioned that the meetings could have been more frequent, “because it was such an enjoyable time”.
What do the interviewees see as results from the Min. ABC-program? At the end of the focus groups, the informants in the study were asked: “What is the most important thing you have learnt through the Min. ABC-program?” One from the migrant group formulated their shared experience: “We in the same group know each other very well. They are very clever, we do not feel left out. For I am not a Norwegian.” Another filled in: “We feel included.”
Several informants mentioned that they now reflect much more over decisions they make: “It is a feeling I have, realizing that I now do understand more.” One mentions that “The primary (result) seems to be that I feel more secure in what I do.” They value that they have increased in knowledge, support to reflect and discuss, and more security to act. They underline that the personnel now have been provided a common ground for their work practices and for implementing changes. They have a shared understanding. “You get a more positive approach when so many have been through the same. You work more together, draw the carriage together, in a way.” The participant contrasts this experience with her situation when she individually had taken advanced health education. “It was difficult to initiate changes since I was the only one who had learnt it. Now it is much easier to make changes since many take part.”
One of the effects is more self-confidence for all Min. ABC-participants, which spill over into daily work, most markedly for the migrants. A participant with a native background describes this effect:
We see that they dare to talk more when we have had this course. It has easily been so that they do not dare to ask and repeat the question, and they gloss over, even if they should have heard it (missed the instructions). But now they are more confident, and dare to speak, and speak up!
A participant with a minority background remarks: “We have a lot of good chemistry, you see. Getting to know each other, and we talk and feel safe, and then we talk. Yes!” In addition, they saw that the milieu at their working place had been affected in a positive way, with more openness and confidence between the staff members.
Discussion
The study has established that the participants unanimously find that participating in the Min. ABC-program has been successful and satisfying. This positive evaluation seems to come from the “whole package” – a totality of well-planned integrated elements. Firstly, the structural part: the size of the group, six to eight members, seems to be optimal for including many positions and experiences and allowing all participants to have a voice. Then the processes: the sharing of experiences and striving toward equality in the interaction. And the content: giving a platform to discuss silenced themes in the interaction between majority and minority workers, and the relationships with the patients. According to Schön,33 the development of practice skills depends on the capacity for reflection-in-action as well as reflection-on-action. The groups have been presented updated knowledge on aging and elder care, as well as information about aspects of languages of importance for communication. Participants have reflected together, and reflection time is scarce in daily practice. The groups have adhered to the principle of equality, overcoming their differences in background. To be treated as equal provides self-confidence and supports participation, which is vital for minority workers. In this way, the groups aim to repair the division between “we” and “them”,5,34 the majority and the minority, which defines “Otherness”.35 This study has found that a “we–them” division has existed in former work situations.
The leader of the group has been vital for all aspects: educated, prepared, focused, and responsible for the processes in the group, with authority to stimulate, direct, and “balance” the members. Thaler and Sunstein36 has examined the everyday word nudge as a scientific concept, referring to that many (people, organizations) must be directed a little (by “choice architecture”) to make wise decisions. More generally, nudge indicates influencing behavior. Applying the concept, we have seen that nudging is necessary to push the modest participants, particularly those with a minority background, to tell their experiences and voice their opinions.
Focus groups based on community and solidarity can be suited for sensitive subjects,30 like the majority and minority relations in our study. The dynamic evoked in the focus group will, many times, surpass the ability of an interviewer to raise good questions.37,38 The moderator’s role varies with the purpose of the focus group.30,39 In the Min. ABC-groups as well as in the focus groups of the study, the leader shall guide the participants through the course with the included themes and questions. Generally, a moderator shall show empathy, sympathy, and be understanding, engaged, and impartial. A question is how much direction should be applied. As shown, nudge had been used directly to push the silent ones to talk and participate. The other way, pauses can also be “pushing”. After a long pause, group members may introduce new themes and new thoughts.30
These aspects are particularly decisive for personnel with a minority background who admit that they are “good at listening”. The interactive group processes have given them a new role as more active participants and a new strategy: not accepting authority’s or elderly’s requests unconditionally, but standing up for themselves and voicing their viewpoints. The silent role seems easily adapted for a migrant health worker, not mastering the language, a newcomer in the health care system, insecure about national rules and cultural codes, and filled with respect for authorities and the elderly. Female workers may be especially prone to subordination, habituated by their traditional gender roles. A tendency to consent covers up their difficulties and protects against shame. Shame is the internalized anxiety for others’ disrespect and discrimination.40 Shame hinders integration, making outsiders. Many are also foreign to the national egalitarian ideal of participation of all the professionals in teams, even if rank matters in the end.
The Min. ABC-groups have been, as in the other ABC-groups, composed of people from various health sectors in the municipality. We find this structure seems to be well suited to discuss openly majority/minority relations, and the problems experienced with communication and language, abuse and discrimination. In small personnel groups at small working places, such problems may be personalized, stirring conflicts and personal accusations. Also, the strategy that the groups shall concentrate on challenges with language, not on cultural diversity in general, seems to be fruitful. To learn better language is an “ordinary” concrete task, with measures and methods recognized in the groups. Relevant aspects of culture concerning different attitudes toward the elderly, and variations on the care systems for the elderly – private family care or public welfare – are touched upon. Interestingly, it is the minority participants who raise the matter of “our culture”, to explain their position. The “culture” of the majority workers seems to be self-evident and unreflected upon. It is presented as “best practice” of public services in the course and implied in the concept of person-centered care.41,42 The individualistic focus is commented upon by the minority workers, because it contrasts the familistic care in their homeland. Studies38,43 reveal different conceptions of filial obligations among immigrants and natives.
What may be the effects of the ABC-course, when enthusiasm is replaced by mundane, everyday work? A large longitudinal study of the participants’ experiences of partaking in the Dementia ABC educational program found that person-centered care and job satisfaction increased over the period.44 However, the organizational support tended to decrease. In our study, the Min. ABC was supported by the political and administrative leaders in the municipality, which may have been vital for the success of the course and the satisfaction among the participants. The influences of the organizational structure on the effects of educational programs seem to be underrated.42,45 Changing attitudes among staff, like person-centered care, may not be established in practice, until organizational changes have been met.27,46
Our results, based on the informants’ reports, indicate that their practices after the course have changed. However, the study was performed shortly after the course, and the effect may fade away in daily routines. Hopefully, the lessons and the support for the minority health workers to ask and ask again may be a permanent change, spilling over to newcomers who see them as role models.
It is relevant to relate a small municipality, as well as larger health institutions like nursing homes and hospitals, to the concept of “learning organization”.47 The characteristics are systems thinking, personal mastery, mental models, shared visions, and team learning. The processes during the Min. ABC-model have included all these aspects. Team learning requires individuals to engage in dialog and discussion. Principal elements are boundary crossing, open communications, shared meaning, and shared understanding. The problem-solving capacity of the organization improves through better access to knowledge. We find that the Min. ABC-model has performed these aims and functions.
Methodological considerations
We suggest that our results concerning the Min. ABC-model might be transferable to other local contexts with an aging population, and interdisciplinary health care personnel with minority and majority backgrounds. However, more detailed studies performed in other contexts are necessary, with differences among personnel in language, health and social caring systems, views on elderly people, and religion and cultural background. Focusing on language and communication seems to be a fruitful strategic road to education and better integration in holistic teamwork.
Conclusion
The Min. ABC-groups seem to be very much adequate for transforming the roles of minority members of the staff, giving them more competence and self-confidence. The Min. ABC-model seems to contribute to better competence, interaction, and development among migrant personnel in the health services for the elderly, increased inclusion and integration, and support of a more holistic care system.
Acknowledgments
First, the authors wish to thank the participants for sharing their experiences, along with the Norwegian National Advisory Unit on Ageing and Health, who supported the study.
Author contributions
BD and KK designed the study. KK and AJ collected the data. All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Torres S, Karl U. A migration lens on inquiries into ageing, old age and elderly care: carving a space while assessing the state of affairs. In: Karl U, Torres S, editors. Ageing in Contexts of Migration. Oxon: Routledge; 2016:1–12. | ||
Torres S. Etnicitet och invandrarskap: relevanta begrippsliga och teoretiska perspektiv för äldrevård och omsorgsforskning [Ethnicity and migration: relevant conceptual and theoretical perspectives for elder care research]. In: Torres S, Finnur M, editors. Innvandrarskap, äldrevård och omsorg [Migration and Elder Care]. Malmö: Gleerups; 2010:222–243. Swedish. | ||
Iecovich E. Migrant homecare workers in elder care: the state of art. In: Karl U, Torres S, editors. Ageing in Contexts of Migration. Routledge: New York; 2016:147–158. | ||
Torres S. At the intersection between an elderly care regime and a migration regime: the swedish case as an example. In: Karl U, Torres S, editors. Ageing in Contexts of Migration. London: Routledge; 2016:35–46. | ||
Rostgaard T. More diversity, better quality of care: constructions of professional identity and work culture among migrant care workers in Denmark. In: Karl U, Torres S, editors. Ageing in Contexts of Migration. New York: Routledge; 2016:172–186. | ||
Browne CV, Braun KL. Globalization, women’s migration, and the long-term-care workforce. Gerontologist. 2008;48(1):16–24. | ||
Statistics Norway. Immigration and immigrants. Statistics Norway. Available from: https://www.ssb.no/en/innvandring-og-innvandrere. 2018.Accessed June 17, 2018. | ||
Østby L. Hvor i landet betyr EU-innvandringen mest? [Where in the country is EU-immigration most important?] Samfunnsspeilet. 2013;5:20–26. Norwegian. | ||
Brunborg H. Hvor mange innvandrere er det - og blir det - i Norge?; framskrivning av innvandrere og norskfødte barn av innvandrere [How many immigrants are there – and will there be – in Norway? Population projections of immigrants and Norwegian born children of immigrants.].Samfunnsspeilet. 2013;27(3):2–9. Norwegian. | ||
Statistics Norway. Landbakgrunn for innvandring i Norge [Country background of immigrants in Norway]. Available from: www.ssb.no/innvandring-og-innvandrere/faktaside/innvandring. 2018. Accessed June 17, 2018. Norwegian. | ||
Johnstone M-J, Kanitsaki O. Cultural racism, language prejudice and discrimination in hospital contexts: an Australian study. Divers Equal Health Care. 2008;5(1):19–30. | ||
Raatiniemi J, Mehus G. Språkvansker skaper stress på jobb [Language difficulties causes work stress]. Sykepleien. 2012;13. Norwegian. | ||
Sørenes K. Tvinger AP til venstre [Forcing AP to the left]. Klassekampen. 2018. Norwegian. | ||
Lanari D, Bussini O. International migration and health inequalities in later life. Ageing Soc. 2012;32(06):935–962. | ||
Forland F, Helsedirektoratet. Migrasjon og helse: utfordringer og utviklingstrekk [Migration and Health: Challenges and Development].Oslo: Helsedirektoratet; 2009. Norwegian. | ||
Dalgard OS, Thapa SB. Immigration, social integration and mental health in Norway, with focus on gender differences. Clin Pract Epidemiol Ment Health. 2007;3(1):24. | ||
Forssell E. Transnational aging, care and the welfare State. Transnational Soc Rev. 2013;3(1):83–99. | ||
Scruggs LA, Allan JP. Social stratification and welfare regimes for the twenty-first century: revisiting the three worlds of welfare capitalism. World Politics. 2008;60(4):642–664. | ||
Esping-Andersen G. The Three Worlds of Welfare Capitalism. Cambridge: Polity Press; 1990. | ||
Tønnessen M, Lekne S, Syse A. Befolkningsframskrivninger 2016–2100: Hovedresultater [Population Projections in Norway]. Oslo: Statistics Norway; 2016. Norwegian. | ||
Kunnskapsdepartementet. Meld. St. 13 (2011–2012) Utdanning for velferd. Samspill i praksis [Education for Welfare. Interaction i Practice]. Oslo: Kunnskapsdepartementet; 2012. Norwegian. | ||
Alessio C. Ageing, demand for care and the role of migrant care workers in the UK. J Popul Ageing. 2010;3(1):39–57. | ||
Di Rosa M, Melchiorre MG, Lucchetti M, Lamura G. The impact of migrant work in the elder care sector: recent trends and empirical evidence in Italy. Eur J Soc Work. 2012;15(1):9–27. | ||
Lowell BL, Martin S, Stone R. Ageing and care giving in the United States: policy contexts and the immigrant workforce. J Popul Ageing. 2010;3(1–2):59–82. | ||
Skålholt A, Høst H, Nyen T, Tønder AH. Å bli helsefagarbeider: en kvalitativ undersøkelse av overganger mellom skole og læretid, og mellom læretid og arbeidsliv blant ungdom i helsearbeiderfaget [Becoming a Health Worker: A Qualitative Study of Transitions between School and Apprenticeship, and between Apprenticeship and Work Life]. Oslo: NIFU; 2013. Norwegian. | ||
Statistics Norway. Health care personnel. Available from: https://www.ssb.no/en/arbeid-og-lonn/statistikker/hesospers/aar. 2018. Accessed June 17, 2018. Norwegian. | ||
Fossli KR, Døble BS, Kirkevold Ø. Kompetanseløft på arbeidplassen: kommunenes erfaringer med ABC modellen [Lifting Competency at the Workplace: The Municipalities Experiences with the ABC-Model].Tønsberg: Forlaget Aldring og helse; 2011. Norwegian. | ||
Døble BS, Kirkevold Ø. Virksomhetsintern opplæring i kommunene: erfaringer med gjennomføring av Demensomsorgens ABC og Eldreomsorgens ABC som del av kompetansesatsingen i Demensplan 2015 og Komeptanseløftet 2015 [Workplace Education in the Municipalities: Experiences with the Dementia Care ABC and the Aging and Nursing Care ABC as Part of the Dementia Plan 2015 and Competency Lift 2015]. Tønsberg: Forlaget Aldring og helse; 2015. Norwegian. | ||
Patton MQ. Qualitative Research & Evaluation Methods. Thousand Oaks, CA: Sage Publications; 2002. | ||
Wibeck V. Fokusgrupper: om fokuserade gruppintervjuer som undersökningsmetod [Focus Groups: On Focused Group Interviews as Research Method]. 2nd ed. Lund: Studentlitteratur; 2010. Swedish. | ||
Corbin JM, Strauss AL. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory. 3rd ed. Thousand Oaks, CA: Sage Publications; 2008. | ||
World Medical Association (WMA). WMA Declaration of Helsinki. Ethical principles for medical research involving human subjects. Available from: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/. 2018. Accessed June 17, 2018. | ||
Schön DA. Educating the Reflective Practitioner. San Francisco, California: Jossey-Bass; 1987. | ||
Lill L. Att göra etnicitet - inom äldreomsorgen [Doing Ethnicity in Elder Care. International Migration and Ethnic Relations]. Malmö: Malmö högskola; 2007. Swedish. | ||
Prasad A, Prasad P. Otherness at large: identity and differences in the new globalization organizational landscape. In: Mills AJ, Aaltio I, editors. Gender, Identity and the Culture of Organizations. London: Routledge; 2002:57–71. | ||
Thaler RH, Sunstein CR. Nudge: Improving Decisions about Health, Wealth, and Happiness. New Haven, CT: Yale University Press; 2008. | ||
Hamran T, Moe S. Yngre og eldre brukere i hjemmetjenesten – ulike behov eller forskjellsbehandling : flerfaglig praksis i et interaksjonsteoretisk perspektiv [Younger and Older Clients in Home Care Services – Different Needs or Discrimination: Multidisciplinary Practice in an Interactional Perspective]. Gjøvik: Høgskolen i Gjøvik; 2012. Norwegian. | ||
Ingebretsen R, Thorsen K, Myrvang VH. Livsmot og mismot blant aldrende kvinner med innvandrerbakgrunn : “Møteplasser er viktig! Det er kjempeviktig!” [Courage and Discourage amongst Older Women with a Migrant Background: “It Is Really Important to Have a Place to Meet!”].Tønsberg: Forlaget Aldring og helse; 2015. Norwegian. | ||
Morgan D, Krueger R. The Focus Group Kit. London: Sage Publications Ltd.; 1998. | ||
Taylor G. Pride, Shame, and Guilt: Emotions of Self-Assessment. Oxford: Clarendon Press; 1985. | ||
Edvardsson D, Winblad B, Sandman PO. Person-centred care of people with severe Alzheimer’s disease: current status and ways forward. Lancet Neurol. 2008;7(4):362–367. | ||
McCormac B, McCance TV. Development of a framework for person-centred nursing. J Adv Nurs. 2006;56(5):472–479. | ||
De Valk H, Schans D. “They ought to do this for their parents”: perceptions of filial obligations among immigrant and Dutch older people. Age Soc. 2008;28(1):49–66. | ||
Rokstad AMM, Døble BS, Engedal K, Kirkevold Ø, Benth JŠ, Selbaek G. The impact of the Dementia ABC educational programme on competence in person-centred dementia care and job satisfaction of care staff. Int J Older People Nurs. 2017;12(2):10. | ||
McCormack B, Kitson A, Harvey G, Rycroft-Malone J, Titchen A, Seers K. Getting evidence into practice: the meaning of “context”. J Adv Nurs. 2002;38(1):94–104. | ||
Dichter MN, Trutschel D, Schwab CGG, Haastert B, Quasdorf T, Halek M. Dementia care mapping in nursing homes: effects on caregiver attitudes, job satisfaction, and burnout. A quasi-experimental trial. Int Psychogeriatr. 2017;29(12):1993–2006. | ||
Senge PM. The Fifth Discipline: The Art and Practice of the Learning Organization. New York: Doubleday; 1990. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.