")
Back to Journals » Risk Management and Healthcare Policy » Volume 15
Water, Sanitation, and Hygiene and Infection Prevention and Control in Jordanian Hospitals in the Context of COVID-19: A National Assessment
Authors Saadeh R, Khader Y , Alyahya M , Al-Samawi M, Allouh MZ
Received 15 January 2022
Accepted for publication 26 March 2022
Published 5 April 2022 Volume 2022:15 Pages 571—582
DOI https://doi.org/10.2147/RMHP.S358600
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Rami Saadeh,1 Yousef Khader,1 Mohammad Alyahya,2 Majid Al-Samawi,1 Mohammed Z Allouh3,4
1Department of Public Health and Community Medicine, Faculty of Medicine, Jordan University of Science and Technology, Irbid, Jordan; 2Department of Health Management and Policy, Faculty of Medicine, Jordan University of Science and Technology, Irbid, Jordan; 3Department of Anatomy, College of Medicine and Health Sciences, United Arab Emirates University, Al Ain, United Arab Emirates; 4Department of Anatomy, Faculty of Medicine, Jordan University of Science and Technology, Irbid, Jordan
Correspondence: Mohammed Z Allouh, Department of Anatomy, College of Medicine and Health Sciences, United Arab Emirates University, P. O. Box: 15551, Al Ain, United Arab Emirates, Tel +97 137 137 551, Email [email protected]
Purpose: To identify areas that need improvement in Jordanian health centers regarding infection prevention and control (IPC) programs; water, sanitation, and hygiene (WASH) services; and other protective measures, especially in the context of coronavirus disease (COVID-19).
Methods: This is a national assessment study that comprised hospitals of different sectors in Jordan, including, Ministry of Health (MoH), private, and military hospitals. The study included 23 Jordanian hospitals. Assessment tools were developed and adapted mainly from the WASH Facility Improvement Tool (WASH FIT) and other tools. Hospitals were assessed to meet targets based on whether indicators were fully met, partially met, or not met.
Results: The mean percentage of the 150 indicators that met the standards was 83.2% (72.6% for MoH, 84.5% for private, and 90.4% for military hospitals). The percentage of indicators, both WASH/IPC and training and education indicators, that met the targets were higher in military hospitals than in MoH and private hospitals. However, in context of COVID-19, only 64.7% of indicators related to precautionary measures were met by all hospitals.
Conclusion: The data available on WASH/IPC in Jordan are scarce, and the study findings will help in preventing severe consequences of the COVID-19 pandemic. There is scope for improvement in many WASH/IPC aspects, and urgent actions should be taken, especially to fill the gaps in COVID-19 precautionary measures.
Keywords: COVID-19, healthcare, hospitals, infection control, waste management
Introduction
Infection prevention and control (IPC) is a scientific approach designed to prevent harm caused by infection in patients and healthcare workers. In health facilities, water, sanitation, and hygiene (WASH) services provide the basis for adequate IPC. Poor and inadequate WASH and IPC services lead to transmission of coronavirus disease (COVID-19) from health facilities to communities and exacerbate the outbreak.
WASH has a major impact on public health, and its importance is globally recognized. In 2015, members of the United Nations agreed on 17 sustainable development goals, which require urgent actions from all countries (developed and developing).1 The first two targets in goal number 6 are focused on the availability of clean, affordable water and proper sanitation and hygiene conditions.2 These proper WASH conditions are essential for protecting human health during all outbreak types, including the recent COVID-19 pandemic. According to the World Health Organization (WHO), routine application of WASH and waste management in homes, communities, schools, marketplaces, and healthcare facilities help in preventing viral transmission that causes COVID-19.3 Prüss et al estimated the global disease burden from water, sanitation, and hygiene to be 4.0% of all deaths and 5.7% of the total disease burden in DALYs (Disability-Adjusted Life Years).4 WASH services strengthen the resilience of healthcare systems to prevent disease outbreaks, allow effective responses to emergencies (including natural disasters and outbreaks), and control emergencies.5,6
IPC has an immense role in reducing disease transmission generally and in health facilities specifically. Studies have concluded that several IPC measures significantly reduce the incidence of nosocomial infections and antibiotic resistance.7 One study on nosocomial IPC among radiographers in Jordan reported moderate knowledge of IPC practices and revealed that future trainings and improvements were needed.8 Another study conducted among nurses from nine different hospitals in Jordan regarding safe injection handling recommended focused and effective infection control educational programs in Jordanian hospitals.9 According to Khader, in the Jordanian healthcare setting, despite major advancements in IPC by providing access to drinking water and improving sanitation and waste management, several areas remain to be improved.5 It is also advisable to establish and implement a WASH monitoring system for healthcare systems.5
Conducting evaluation studies for IPC in health facilities helps find gaps that should be corrected for efficiency. In Jordan, such types of studies are limited. Thus, this study aimed to identify strengths and gaps in the WASH and IPC practices, activities, and resources in Jordanian hospitals in the context of COVID-19 and identified areas for quality improvement.
Materials and Methods
Study Design
A national assessment of WASH and IPC practices in hospitals was conducted in Jordan from October to December 2020 using a structured assessment tool. The assessment was performed in a cross-sectional study design.
Sampling
A multistage cluster sampling technique proportional to the size was used for selecting hospitals. The sampling frame was developed to include all hospitals in different sectors, including Ministry of Health (MoH), private, and military hospitals. The hospitals were stratified according to the region, sector, and facility size based on patients’ load (small, medium, and large). A random sample was selected from each stratum, and a total of 23 hospitals were selected for this study.
Assessment Tools and Study Questionnaires/Checklists
An assessment tool was developed for hospitals (inpatient wards and outpatient clinics) based on the review and adaptation of several tools. The main tool used was the Water and Sanitation for Health Facility Improvement Tool (WASH FIT).6 The WASH FIT covers four broad domains with 65 indicators and targets to achieve minimum standards for maintaining safe and clean environments. Some indicators were developed from other tools, including the Infection Prevention and Control (IPC) Assessment Framework (IPCAF),10 Guide to Infection Prevention for Outpatient Settings: Minimum Expectations for Safe Care,11 Systems for Improved Access to Pharmaceuticals and Services (SIAPS) tool, and COVID-19 technical guidance by the WHO.3
There were eight domains covered in this tool: water, medical waste and sanitation facilities, hygiene, management, IPC program, training and education, evaluation and feedback, and COVID-19 precautionary measures. The hygiene domain covered areas related to hand hygiene and facility environment, cleanliness, and disinfection. The IPC program domain was divided into subareas, including basic indicators, guidelines of IPC,10,11 training and education for the IPC unit, healthcare-associated infection monitoring, monitoring/auditing of infection control practices and outcomes, personal protective equipment (PPE), and availability of hygiene materials. Evaluation and feedback covered subareas were basic indicators, respiratory safety, environmental cleaning, and sterilization of reusable devices.
Each area/subarea included indicators and targets to achieve minimum standards for maintaining safe and clean environments. These were global standards as illustrated in the WHO essential environmental health standards in health care12 and the WHO Guidelines on core components of IPC programs at the national and acute health care facility level.10 The assessment tool included WASH FIT indicators besides other indicators identified from the available tools. Indicators were adapted to the needs, local priorities, and national standards to meet quality, and mechanisms were implemented for improvement. Irrelevant indicators were excluded, and few were added as necessary to represent the service levels.
Assessment Team
A committed team trained on WASH and IPC was established. The assessment team comprised 12 assessors with each assessor having a minimum B.Sc. degree and holding an administrative position in MoH. The assessors were divided into three teams: one team for each region (north, central, and south of Jordan). The team was supported by the MoH leadership and the facility’s administration. A training workshop was held to train the assessment team on the assessment process, data collection, and use of assessment tool.
Assessment Process
The assessment teams planned their visits to hospitals with the senior facility managers. During the facility visit, the assessment team worked with a facility team, including those with an in-depth understanding and knowledge of WASH and IPC activities at the facility level to complete the assessment tool. If there were no professionals in charge of WASH and IPC or if an IPC program was not yet established, the tool was completed by the assessment team while consulting the senior facility manager.
A comprehensive facility assessment was conducted using the approved list of indicators, and each indicator was recorded as whether it met, partially met, or did not meet the minimum standards. The assessment forms were reviewed by supervisors to ensure that all information was clear and correct, and all team members agreed on the findings of each assessment. During assessment, hygiene promotion materials, WASH and IPC guidelines, and budget were also reviewed and observed.
Analysis
The percentage of indicators that met or partially met the standards was calculated for each facility. The overall facility score (percentage of all indicators meeting the standards) was calculated to compare over time when future assessments were conducted. Data are described as mean percentages in the text, and as median, range, and mean ± SD in the tables.
Ethical Consideration
This study was approved by Jordan University of Science and Technology and the Jordanian MoH.
Results
Hospitals’ Characteristics
Overall, 23 hospitals distributed across the three regions of the country (11 in the north, 13 in the central, and three in the south) were assessed. Among all hospitals, seven were MoH, nine were military, and seven were private. Table 1 shows the characteristics of the 23 hospitals assessed for WASH and IPC. The total number of beds in all hospitals ranged from 58 to 494, and the annual occupancy rate ranged from 30% to 97% (median, 67%). The median number of emergency room and intensive care unit beds was 55 and 50, respectively. The median number of ventilators in the hospitals was 49. The number of doctors ranged from 5 to 374, and the number of nurses ranged from 80 to 934. Some military settings included tertiary health facilities. Thus, some facilities did not have emergency room and intensive care unit beds, isolation rooms, or ventilators. All hospitals in all sectors had laboratory and X-ray imaging facilities.
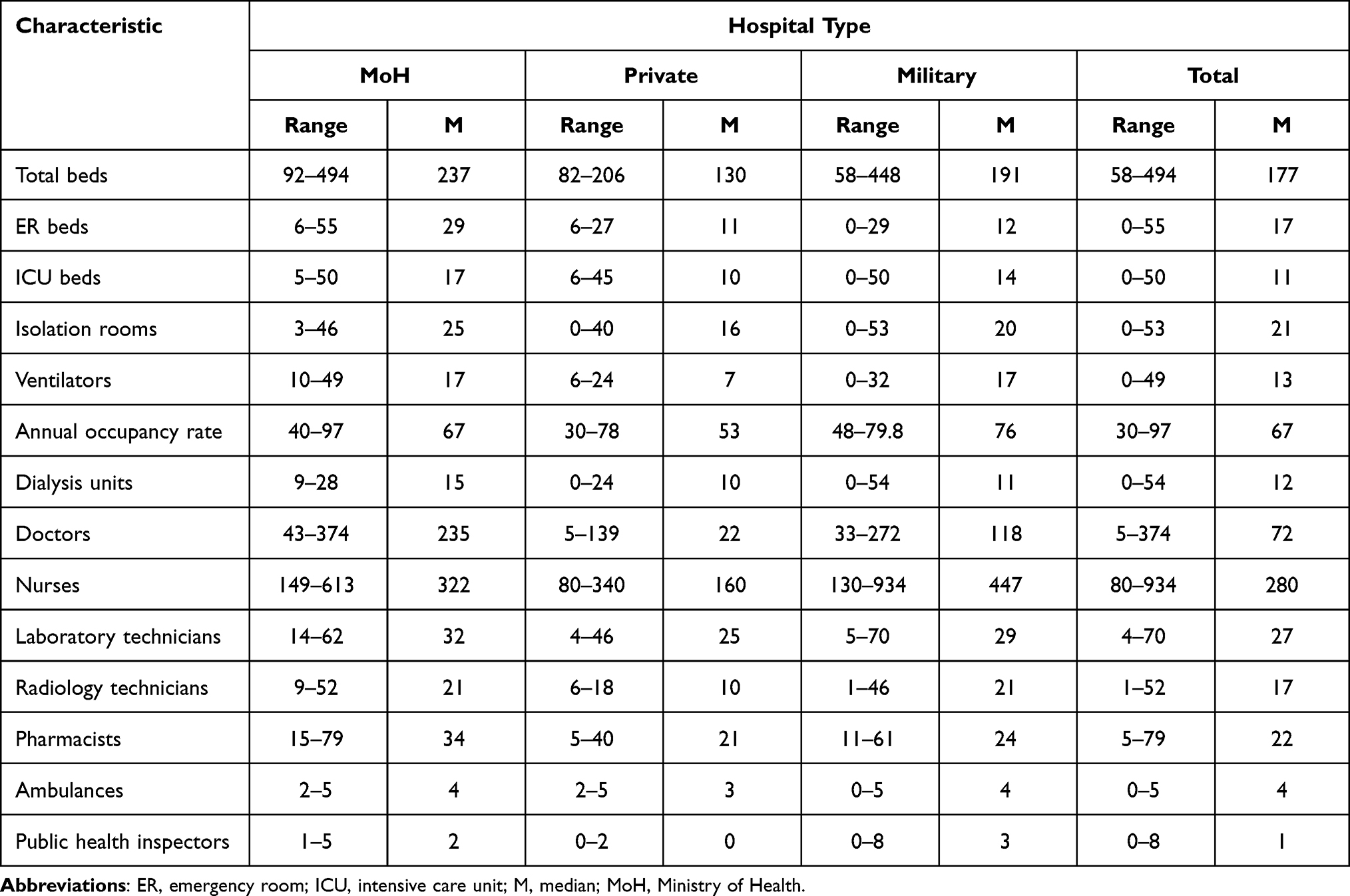 |
Table 1 Characteristics of 23 Hospitals Assessed for Water, Sanitation and Hygiene (WASH) and Infection Prevention and Control (IPC) Indicators |
WASH and IPC Indicators
Table 2 shows the mean percentages of WASH and IPC indicators that met targets across all participating hospitals. Overall, 150 indicators were assessed for each facility. The mean percentage of the 150 indicators that met the standards was 83.2% (72.6% for MoH hospitals, 84.5% for private hospitals, and 90.4% for military hospitals). The percentage of indicators that met targets in all hospitals varied according to the assessed WASH and IPC domains and ranged from 64.7% to 100%. Only 64.7% of indicators related to COVID-19 precautionary measures were met by all hospitals. The percentage of indicators that met the targets was higher in military hospitals in 14 out of 18 WASH/IPC areas than in MoH and private hospitals (Table 2). Furthermore, military hospitals met all indicators (100%) in seven areas. Only 35.7% of basic evaluation and feedback indicators were met in MoH hospitals, while 100% of these indicators were met in military hospitals. Almost 94.4% of training and education indicators were met in military settings, whereas only 57.1% and 60.7% of these indicators were met in MoH and private hospitals, respectively. All hospitals met all sterilization of reusable device indicators.
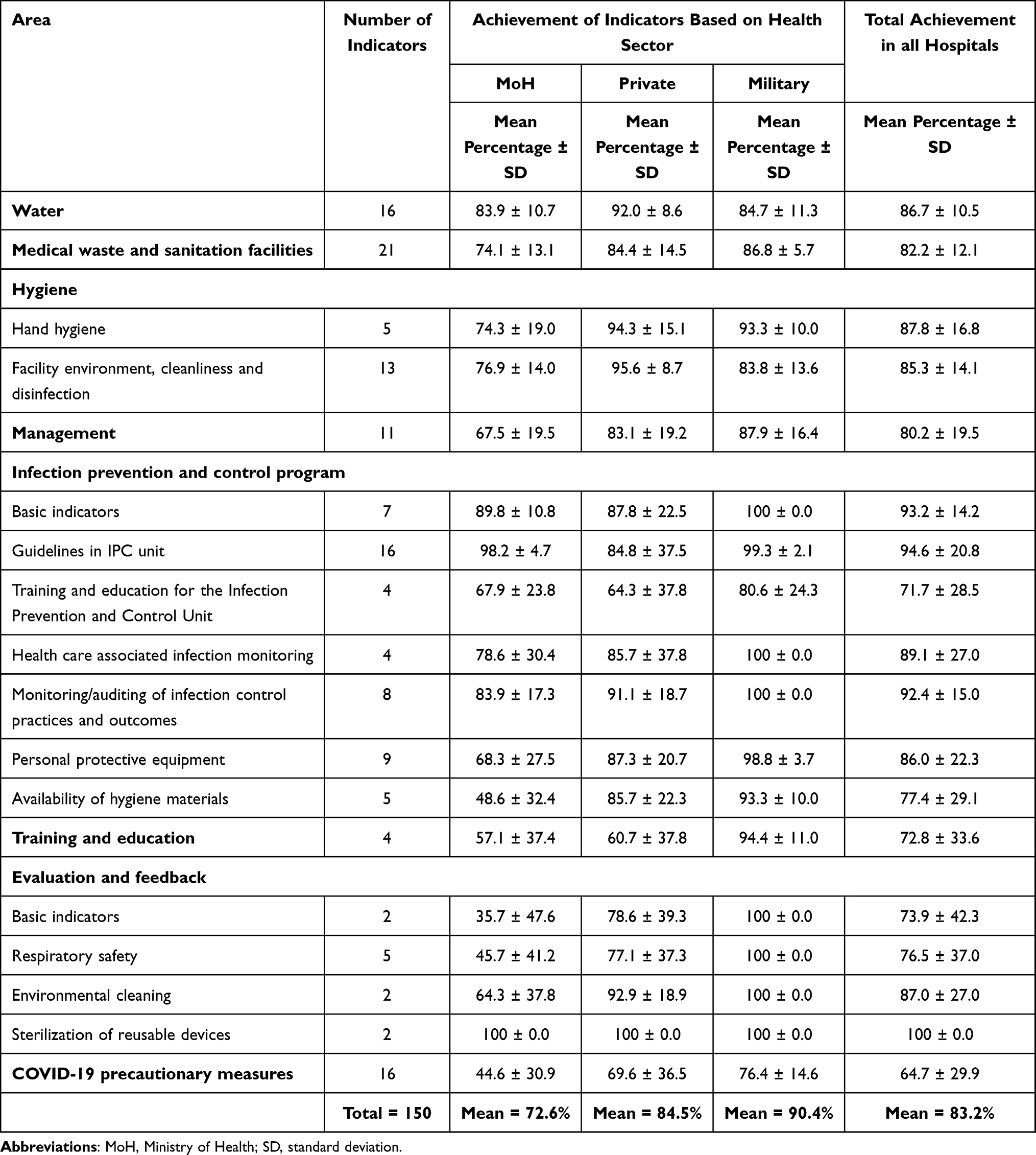 |
Table 2 Mean Percentages of Water, Sanitation and Hygiene (WASH) and Infection Prevention and Control (IPC) Indicators That Met Targets in All Participating Hospitals |
Water Indicators
Overall, 16 “Water” indicators were assessed. Among them, 86.7% met the targets (83.9% in MoH, 92.0% in private, and 84.7% in military hospitals). Most hospitals (>70%) met most “Water” indicators. However, some indicators such as “Improved drinking water supply is piped into the facility” and “A clean drinking water is available and accessible for staff, patients and health care providers always and in all locations/wards” were met in 69.9% and 60.9% of hospitals, respectively. Only 14.3% of MoH hospitals had improved drinking water supply piped into the facility, and only 22.2% of military hospitals always had available clean water in all locations/wards. Conversely, meeting the target for indicators related to storage, functionality, and quality of water was high in all hospitals, reaching 100% in four indicators. All private hospitals (100%) fully met the targets of 10 of the 16 water indicators. However, only 42.9% of private hospitals had available emergency water tanks.
Medical Waste and Sanitation Facilities
In total, 21 “Medical waste and sanitation facility” indicators were assessed. Among them, 82.2% met the targets (74.1%, 84.4%, and 86.8% in MoH, private, and military hospitals, respectively). The targets of many indicators related to toilets and waste management were met by most hospitals. More than two-thirds of hospitals met 18 of 21 indicators, and >95% of hospitals met eight indicators. All hospitals (100%) had adequate toilets and functional waste collection containers. However, only 43.5% of all hospitals had records of cleaning toilets; only one MoH hospital had such records. Almost half of the hospitals, especially MoH (42.9%) and military hospitals (44.4%), did not have toilets serving people with special needs. Moreover, less than one-third of MoH hospitals had functioning hand hygiene stations within 5 m of the toilets, and only 14.3% of private hospitals had a greywater (ie, rainwater or wash water) drainage system.
Hygiene
Hand Hygiene
Overall, five “Hand hygiene” indicators were assessed. Among them, 87.8% met the targets (74.3% in MoH, 94.3% in private, and 93.3% in military hospitals). Most hospitals met the indicators of hand hygiene. However, over half of the MoH hospitals (57.1%) had clearly displayed sign boards for hand hygiene (poster), and 66.7% of military hospitals had functioning hand hygiene stations adequately available at all care points (in wards and outpatient clinics).
Facility Environment, Cleanliness, and Disinfection
Overall, 13 “Facility environment, cleanliness and disinfection” indicators were assessed. Among them, 85.3% met the targets (76.9% in MoH, 95.6% in private, and 83.8% in military hospitals). All MoH, military, and private hospitals met 6, 5 and 9 indicators, respectively. However, only 47.8% of hospitals had cleaning records visible and signed by cleaners each day. Only 42.9% of MoH hospitals provide at least two pairs of household cleaning gloves, one pair of overalls or aprons, and boots for each cleaning and waste disposal staff member. Moreover, only 42.9% of MoH hospitals had a mechanism to track the supply of IPC-related materials (eg, gloves and protective equipment) to identify stock-outs.
Management
In total, 11 “Management” indicators were assessed. Among them, 80.2% met the targets (67.5% in MoH, 83.1% in private, and 87.9% in military hospitals). The targets of indicators related to the management of WASH/IPC were met by most hospitals, except for one indicator “Health care staff trained on WASH/IPC each year.” Only 28.6% of MoH hospitals reported that healthcare staff received training on WASH/IPC programs every year. Less than half of the MoH hospitals were committed to have an annual planned budget, a regular ward-based audit system, and a performance appraisal system to recognize and reward high-performing staff. Nonetheless, military settings met most management indicators.
IPC Program
Basic Indicators
Among seven basic indicators, 93.2% of hospitals met the targets (89.8% in MoH, 87.8% in private, and 100% in military hospitals). Most hospitals in all sectors successfully met the IPC basic indicators. However, only 57.1% of MoH hospitals had an early detection system and dealt with potential contagious individuals at early meeting points.
Guidelines of IPC
Sixteen indicators related to guidelines in the IPC unit were assessed. Most MoH and military hospitals successfully achieved the 16 indicators. The percentage of all hospitals that met the target was 94.6% (98.2% in MoH, 84.8% in private, and 99.3% in military hospitals).
Training and Education for the IPC Unit
Among four indicators, 71.7% of hospitals met the targets (67.9% in MoH, 64.3% in private, and 80.6% in military hospitals). Although most hospitals (95.7%) had an employee who led the IPC training, only half of the hospitals had healthcare workers and other personnel trained on IPC. Interestingly, >91% of hospitals had regular and ongoing development/education programs offered to IPC staff.
Health Care-Associated Infection Monitoring
Among four indicators, 89.1% of hospitals met the targets (78.6% in MoH, 85.7% in private, and 100% in military hospitals). Health care-associated infection monitoring targets were met by most hospitals. All military settings (100%) and more than 85% of private hospitals met the four monitoring indicators. Surveillance was conducted for epidemic-prone infections in only 57.1% of MoH hospitals.
Monitoring/Auditing of Infection Control Practices and Outcomes
All indicators of infection control practices and outcomes were met by most hospitals. Among eight indicators, 92.4% of hospitals met the targets (83.9% in MoH, 91.1% in private, and 100% in military hospitals). All military settings successfully achieved the targets, and all private hospitals met half of the indicators. All hospitals in the three sectors reported that the updated list of reported diseases was made available to all of their employees. However, only 57% of MoH hospitals had a regular monitoring program for transmission-based precautions and isolation to prevent the spread of multidrug-resistant organisms.
Personal Protective Equipment (PPE)
Among nine indicators, 86% of hospitals met the targets (68.3% in MoH, 87.3% in private, and 98.8% in military hospitals). Although most hospitals achieved PPE indicators, there was a considerable difference in most indicators between military settings and MoH hospitals. The target was achieved in a higher percentage in military and private hospitals than the MoH hospitals for almost all indicators. All military settings met all PPE indicators. Two indicators, namely “Compliance in using PPE is routinely reviewed and monitored” and “Healthcare providers (HCPs) do not wear the same gown for the care of more than one patient” were met by only 42.9% at MoH hospitals. Moreover, the two indicators “HCPs wear proper gowns to protect skin and clothing during procedures or activities where contact with blood or body fluids is anticipated” and “HCPs wear mouth, nose, and eye protection during procedures that are likely to generate splashes or sprays of blood or other body fluids” were met by only 54.1% at MoH hospitals.
Availability of Hygiene Materials
Among five indicators, 77.4% of hospitals met the targets (48.6% in MoH, 85.7% in private, and 93.3% in military hospitals). A higher percentage of military and private hospitals met the targets than MoH hospitals for all indicators. The targets for indicators of hygiene materials were met by most hospitals, except for one indicator “Single-use towels are available at each sink.” Only one MoH hospital (14.3%) reported the availability of single-use towels at each sink. All military and private facilities (100%) had supplies needed for adherence to hand hygiene, while only 42.9% of MoH hospitals had them.
Training and Education
Among the four indicators, 72.8% of all hospitals met the targets (57.1% in MoH, 60.7% in private, and 94.4% in military hospitals). Military hospitals achieved the highest percentage of all training and education indicators. The target of the indicator “Healthcare workers receive training regarding hand hygiene” was met by 57.1% of MoH hospitals and 42.9% of private hospitals. Similarly, the “Instructions on hand hygiene” indicator was met by 57.1% in both MoH and private hospitals.
Evaluation and Feedback
Basic Indicators and Respiratory Safety
Among two basic evaluation and feedback indicators, 73.9% of hospitals met the targets (35.7% in MoH, 78.6% in private, and 100% in military hospitals). Regarding five respiratory safety indicators, 76.5% of hospitals met the targets (45.7% in MoH, 77.1% in private, and 100% in military hospitals). All military hospitals (100%) met seven evaluation and feedback indicators. Unfortunately, less than half of the MoH sector hospitals met the target for the evaluation and feedback indicators, except for “Signboards and posters are spread on entrances with instructions,” which was met by 71.4% of private and MoH hospitals. Moreover, the targets of two evaluation and feedback indicators “At department level, regular reviews are conducted at least annually” and “Had face masks offered to cough patients and other people with symptoms upon admission” were met by about one-quarter (28.6.3%) of MoH hospitals.
Environmental Cleaning and Sterilization of Reusable Devices
Almost all (95.7%) hospitals met the target for disinfectant use according to the manufacturer’s instructions, and 78.3% of hospitals met the target for wearing PPE by HCPs. However, wearing appropriate PPE by HCPs to prevent the exposure of infectious agents or chemicals was achieved in only 42.9% of MoH hospitals Furthermore, all hospitals met the target of the two indicators about the sterilization of reusable devices.
COVID-19 Precautionary Measures
The average percentage of COVID-19 precautionary measures that met the targets across all hospitals was 64.7% (44.6% in MoH, 69.6% in private, and 76.4% in military hospitals). This percentage varied widely among the target indicators (Figure 1). Only about one-third (30.4%) of all hospitals regularly checked healthcare workers for COVID-19. Less than half of the hospitals (47.8%) checked temperature and breathing problems in all patients before entering the hospital. Likewise, less than half (47.8%) of the hospitals had spacing in time and appointments of patients owing to the COVID-19 outbreak.
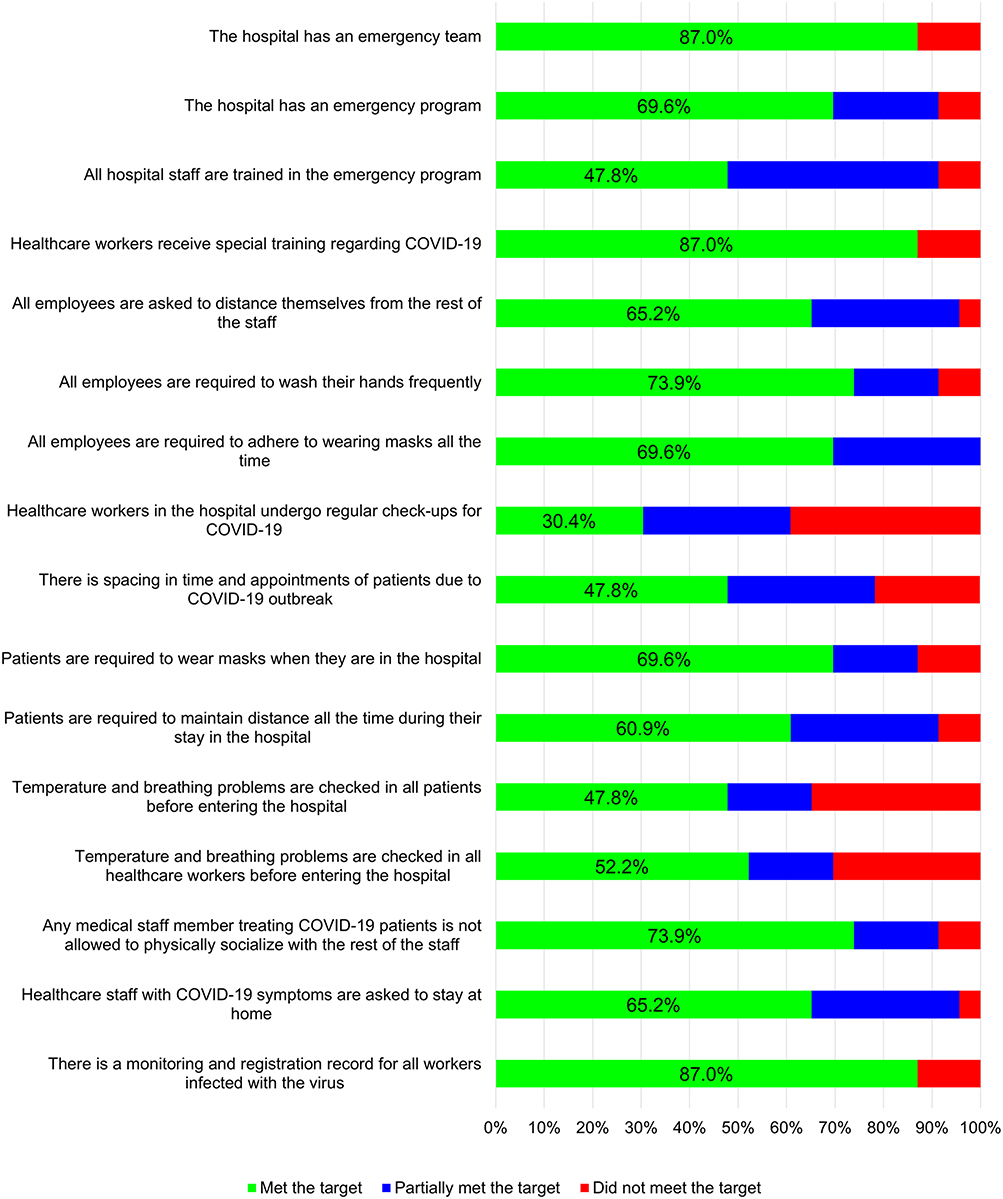 |
Figure 1 Percentage of hospitals that met the target, partially met the target, or did not meet the target for indicators related to COVID-19. |
Military settings performed better for most indicators of COVID-19, yet healthcare workers receiving regular checks for COVID-19 were reported in only one military hospital. Private hospitals performed better for most indicators than MoH hospitals.
Discussion
In Jordan, the first COVID-19 case was registered in March 2020, which reached its peak in the same month in 2021. Data collection for this national study was conducted from October to December 2020, which was the time when all precautions and protective measures against communicable diseases should have been at their maximum levels. The inclusion of hospitals from all health sectors in the country was useful in identifying gaps and areas of improvement in IPC and WASH services, with special attention to COVID-19. To our knowledge, this is the first national study to provide valuable descriptions of the current WASH and IPC practices, activities, and resources in Jordanian hospitals.
Although the mean percentage of 150 indicators that met the standards was 83.2% for all evaluated hospitals, there were gaps in some areas, especially among MoH hospitals, which had an overall mean percentage of 72.6%. Khader et al indicated the need for enhancement in several WASH areas in Jordan.5 A recent assessment of WASH in Uganda’s health facilities revealed similar conclusions as it mentioned that institutional and performance obstacles are underlying causes for deteriorated levels of several WASH indicators, including water, sanitation, environmental cleanliness, and waste management.13 Meeting the targets for all WASH indicators is difficult with a limited or planned budget. Less than half of the MoH hospitals were committed to have an annual planned budget, and the opposite was true for military hospitals; therefore, the difference in meeting WASH targets was found between these two hospital sectors. Moreover, clean water provision is a common problem among many developing countries, as reported in a systematic review that described water availability in 420 hospitals located in 19 low- and middle-income countries. The study reported that more than one-third of assessed hospitals did not have dependable water sources.14 Another common problem in developing countries is wastewater management, which is a relatively new discipline mainly used to detect drugs in wastewater to estimate drug use in a population. However, it is now used to detect pathogens, including SARS-CoV-2, as the first report of its detection in an Australian study by Ahmed et al 2020 was followed by several studies that all recommended a safe wastewater management to help fight the pandemic.15
Since the beginning of the COVID-19 pandemic, medical waste has considerably increased, and its management has become more difficult.15 Therefore, it is important to evaluate waste management for accurate infection prevention assessment. In Jordan, <78% of sanitation systems are safely managed, and one-third of schools have basic sanitation services.16 Several studies reported that viral materials of SARS-CoV-2 (RNA) can be found in human wastes, including blood and stool,17,18 and infection can spread quickly through hospitals if any IPC indicator is severely breached. An example was the outbreak of MERS-COV infection in a Jordanian hospital, wherein a 10% attack rate was noted among potentially exposed groups.19 However, hospitals sampled in this study scored low on the number of toilets available for special needs and the cleaning strategy, which jeopardized the integrity of IPC and made the hospital a possible source of infection, including SARS-CoV-2 transmission.
A situational analysis study assessed IPC programs in 88 countries, including high-, upper middle-, lower middle-, and low-income countries, according to the World Bank classification. This global assessment showed that most countries have IPC guidelines but varied significantly in their implementation and evaluation strategies.20 High-income countries had higher implementation and compliance rates.20 Fortunately, most Jordanian hospitals assessed in this report met the target for IPC scores, which indicates that implementation strategies in Jordan are comparable to those of high-income countries. However, many MoH and private hospitals did not meet the target for IPC training and education, which is similar to other low- to upper middle-income countries included in the study.20 Conversely, developed countries, including the USA and Europe, have already acknowledged the importance of training and education in IPC. For example, the next goal for the European Union is to unify the training and education system for IPC across Europe as the commitment to IPC training and education has mostly been achieved.21,22 However, it is not always possible for high-income countries to score high for all IPC indicators. For example, Austrian acute care hospitals yielded a low score on an IPC national assessment.23
In our study, the scores for hand hygiene were remarkable, except for the lack of adequate hand hygiene stations, which were slightly lower, especially among MoH hospitals. In general, hand hygiene compliance is a global problem, as indicated in a systematic review study assessing hand hygiene compliance in health facilities.24 The review reported an overall median hand hygiene compliance rate of 40%. The study also showed lower compliance rates in intensive care units, and among doctors.24 Conversely, Kilpatrick et al presented the results of two surveys that used the global Hand Hygiene Self-Assessment Framework conducted by the WHO in 2011 and 2015 in 86 health facilities. The scoring system of the surveys comprised five main areas, each with a score of 100. The mean score of the studied facilities in 2011 was 335.1, which was significantly improved to reach 374.4 in 2015 (p<0.001).25
In this study, there was some areas of IPC, including environmental cleanliness and disinfection, where a large variation in mean scores was noticed among indicators and hospital types. For instance, military hospitals scored lower than MoH and private hospitals for floor cleaning and municipal trash containers but scored higher for the availability of IPC materials and supplies. These outcomes show that there is a room for improvement in all types of hospitals. The findings of environmental cleaning were similar to those of an assessment conducted in 23 hospitals in the USA.26 This study reported a total percentage score of 49% for environmental cleaning in terminal rooms but ranged between 35% and 81% based on the types of hospitals assessed. The study mentioned that there was a scope for environmental cleaning improvement in all evaluated hospitals, especially in patient’s surrounding areas.26
Maintaining strong IPC strategies is required to protect health facilities from different hazards, including COVID-19. Nonetheless, some indicators that are important for COVID-19 prevention, such as regular check-ups for healthcare workers, including temperature checks or regular COVID-19 testing, were not met by most hospitals. Furthermore, certain indicators need immediate improvement, including staff emergency training, routine checks for everyone who enters the hospitals, and infected staff monitoring system. A recent WASH assessment in Zimbabwe used the WASH FIT to assess the adherence of 50 health centers during the COVID-19 pandemic. The study reported that 25% of facilities scored an inadequate level in the main WASH domains, including sanitation, water, waste management, cleanliness, and management. Only 8% of the facilities scored good and 42% scored poor in WASH domains.27 However, some studies in developed countries, including the United States, reported the need for improvement in adherence to COVID-19 IPC measures. For instance, a study in the state of Georgia assessed adherence to IPC guidelines in 24 health facilities and classified them into higher and lower prevalence facilities depending on the prevalence of COVID-19 cases. The study reported low adherence in the area of disinfection (32%). There were also significant differences between high- and low-prevalence facilities in areas such as PPE and social distancing.21
Certain limitations to our study include that the design consists of a one–time assessment of the facility, which does not necessarily represent the hospitals’ IPC/WASH conditions at all times. Additionally, despite the assessment being built on an objective tool, there could be a subjective estimation for items that partially rather than fully meet the target, especially if the evaluation was performed during some administrative and managerial transitions.
Conclusion
There are some gaps in IPC and WASH procedures in Jordanian hospitals, which were largely noticed among MoH hospitals. Some areas that scored low need improvement but might not seem urgent, especially with budget constraints in governmental settings. However, the current offensiveness of the COVID-19 pandemic reassures its urgency, and all indicators measured in this assessment are highly valuable in breaking the transmission chain of this disease. Ensuring the functionality and applicability of IPC and WASH measures in all health and public sectors is inevitable to avoid another fierce outbreak that could damage the healthcare system. A major area of improvement is the training and education of healthcare workers who have prompt and prudent responses during the fluctuating courses of the pandemic.
Acknowledgments
The authors appreciate the help of research assistants and the support of hospital administrators during the collection of data.
Funding
This study was funded by a grant from the United Nations Children’s Fund (UNICEF). Article editing and publication charges were provided by a grant from the College of Medicine and Health Sciences at the United Arab Emirates University (grant # 00003395).
Disclosure
All authors report no conflicts of interest in this work.
References
1. Sustainable Development Goals. Available from: https://sdgs.un.org/goals.
2. Goal 6: ensure availability and sustainable management of water and sanitation for all. Available from: https://sdgs.un.org/goals/goal6.
3. Interim guidance. Water, sanitation, hygiene, and waste management for SARS-CoV-2, the virus that causes COVID-19; 2020. Available from: https://www.who.int/publications/i/item/WHO-2019-nCoV-IPC-WASH-2020.4.
4. Prüss A, Kay D, Fewtrell L, Bartram J. Estimating the burden of disease from water, sanitation, and hygiene at a global level. Environ Health Perspect. 2002;110(5):537–542. doi:10.1289/ehp.110-1240845
5. Khader YS. Water, sanitation and hygiene in Jordan’s healthcare facilities. Int J Health Care Qual Assur. 2017;30(7):645–655. doi:10.1108/IJHCQA-10-2016-0156
6. Water and Sanitation for Health Facility Improvement Tool (WASH FIT); 2017. Available from: https://apps.who.int/iris/bitstream/handle/10665/254910/9789241511698-eng.pdf;jsessionid=CBA30FFCCFC3CD66C0827B5C38BCDDF9?sequence=1.
7. Ershova K, Savin I, Kurdyumova N, et al. Implementing an infection control and prevention program decreases the incidence of healthcare-associated infections and antibiotic resistance in a Russian neuro-ICU. Antimicrob Resist Infect Control. 2018;7:94. doi:10.1186/s13756-018-0383-4
8. Abdelrahman MA, Alhasan M, Alewaidat H, Rawashdeh MA, Al Mousa DS, Almhdawi KA. Knowledge of nosocomial infection control practices among radiographers in Jordan. Radiography. 2017;23(4):298–304. doi:10.1016/j.radi.2017.07.005
9. Al-Rawajfah OM, Tubaishat A. A concealed observational study of infection control and safe injection practices in Jordanian governmental hospitals. Am J Infect Control. 2017;45(10):1127–1132. doi:10.1016/j.ajic.2017.04.293
10. Infection Prevention And Control Assessment Framework At The Facility Level; 2018. Available from: https://www.who.int/infection-prevention/tools/core-components/IPCAF-facility.PDF.
11. Guide To Infection Prevention For Outpatient Settings: minimum Expectations For Safe Care; 2016. Available from: https://www.cdc.gov/infectioncontrol/pdf/outpatient/guide.pdf.
12. Adams J, Bartram J, Chartier Y. Essential Environmental Health Standards in Health Care. World Health Organization (WHO); 2008. https://books.google.ae/books?hl=en&id=QwVj87Mmz4sC&oi=fnd&pg=PA3&dq=Chartier+Y,+Adams+J,+Bartram+J.+Essential+environmental+health+standards+in+health+care.+Geneva:+WHO.+2008.&ots=qCPghPGuJR&sig=PmCHhpSNyQARMFV7v2mCgBA5C68&redir_esc=y#v=onepage&q&f=false.
13. Kayiwa D, Mugambe RK, Mselle JS, et al. Assessment of water, sanitation and hygiene service availability in healthcare facilities in the greater Kampala metropolitan area, Uganda. BMC Public Health. 2020;20(1):1767. doi:10.1186/s12889-020-09895-9
14. Chawla SS, Gupta S, Onchiri FM, Habermann EB, Kushner AL, Stewart BT. Water availability at hospitals in low- and middle-income countries: implications for improving access to safe surgical care. J Surg Res. 2016;205(1):169–178. doi:10.1016/j.jss.2016.06.040
15. Ahmed W, Angel N, Edson J, et al. First confirmed detection of SARS-CoV-2 in untreated wastewater in Australia: a proof of concept for the wastewater surveillance of COVID-19 in the community. Sci Total Environ. 2020;728:138764. doi:10.1016/j.scitotenv.2020.138764
16. Water, sanitation and hygiene Access to safe water and sanitation for every child. Available from: https://www.unicef.org/jordan/water-sanitation-and-hygiene.
17. Young BE, Ong SWX, Kalimuddin S, et al. Epidemiologic Features and Clinical Course of Patients Infected With SARS-CoV-2 in Singapore. JAMA. 2020;323(15):1488–1494. doi:10.1001/jama.2020.3204
18. Zhang J, Wang S, Xue Y. Fecal specimen diagnosis 2019 novel coronavirus-infected pneumonia. J Med Virol. 2020;92(6):680–682. doi:10.1002/jmv.25742
19. Al-Abdallat MM, Payne DC, Alqasrawi S, et al. Hospital-associated outbreak of Middle East respiratory syndrome coronavirus: a serologic, epidemiologic, and clinical description. Clin Infect Dis. 2014;59(9):1225–1233. doi:10.1093/cid/ciu359
20. Tartari E, Tomczyk S, Pires D, et al. Implementation of the infection prevention and control core components at the national level: a global situational analysis. J Hosp Infect. 2021;108:94–103. doi:10.1016/j.jhin.2020.11.025
21. Telford CT, Bystrom C, Fox T, et al. COVID-19 Infection Prevention and Control Adherence in Long-Term Care Facilities, Atlanta, Georgia. J Am Geriatr Soc. 2021;69(3):581–586. doi:10.1111/jgs.17001
22. Zingg W, Mutters NT, Harbarth S, Friedrich AW. Education in infection control: a need for European certification. Clin Microbiol Infect. 2015;21(12):1052–1056. doi:10.1016/j.cmi.2015.09.001
23. Aghdassi SJS, Hansen S, Bischoff P, Behnke M, Gastmeier P. A national survey on the implementation of key infection prevention and control structures in German hospitals: results from 736 hospitals conducting the WHO Infection Prevention and Control Assessment Framework (IPCAF). Antimicrob Resist Infect Control. 2019;8:73. doi:10.1186/s13756-019-0532-4
24. Erasmus V, Daha TJ, Brug H, et al. Systematic review of studies on compliance with hand hygiene guidelines in hospital care. Infect Control Hosp Epidemiol. 2010;31(3):283–294. doi:10.1086/650451
25. Kilpatrick C, Tartari E, Gayet-Ageron A, et al. Global hand hygiene improvement progress: two surveys using the WHO Hand Hygiene Self-Assessment Framework. J Hosp Infect. 2018;100(2):202–206. doi:10.1016/j.jhin.2018.07.036
26. Carling PC, Parry MF, Von Beheren SM; Healthcare Environmental Hygiene Study Group. Identifying opportunities to enhance environmental cleaning in 23 acute care hospitals. Infect Control Hosp Epidemiol. 2008;29(1):1–7. doi:10.1086/524329
27. Hirai M, Nyamandi V, Siachema C, et al. Using the Water and Sanitation for Health Facility Improvement Tool (WASH FIT) in Zimbabwe: a Cross-Sectional Study of Water, Sanitation and Hygiene Services in 50 COVID-19 Isolation Facilities. Int J Environ Res Public Health. 2021;18(11):5641. doi:10.3390/ijerph18115641
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.