")
Back to Journals » International Medical Case Reports Journal » Volume 15
Wandering Spleen with Splenic Torsion: Unusual Cause of Acute Abdomen
Authors Ahmed M , Nasir M , Negash A, Haile K
Received 31 August 2022
Accepted for publication 26 October 2022
Published 4 November 2022 Volume 2022:15 Pages 625—630
DOI https://doi.org/10.2147/IMCRJ.S388271
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ronald Prineas
Muluken Ahmed,1 Mohammed Nasir,2 Ashenafi Negash,3 Kidist Haile1
1Pediatrics Department, Arba Minch University, Arba Minch, Ethiopia; 2Pediatrics Department, Saint Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia; 3Surgery Department, Arba Minch University, Arba Minch, Ethiopia
Correspondence: Muluken Ahmed, Pediatrics Department, Arba Minch University, PO Box: 021, Arba Minch, Ethiopia, Tel +251932152342, Email [email protected]
Introduction: Wandering spleen is a rare condition characterised by laxity or lack of splenic ligaments as a result of acquired or congenital causes. There is a possibility of misdiagnosis due to its vague symptoms. In order to make a proper diagnosis, imaging techniques including abdominal ultrasonography and CT scanning are essential. Surgery is the main option of management. If the spleen is viable and there is no thrombosis in the splenic veins, splenopexy is the preferred surgical procedure. Alternatively, splenectomy plus prophylactic antibiotic and vaccination usage may be employed if spleen has infarction.
Case Presentation: A 12-year-old male child who had previously experienced constipation, mucoid diarrhoea, and abdominal distention arrived with crampy abdominal pain that had lasted for four days. The patient was tachycardic with abdominal tenderness. Whirlpool sign and lack of a spleen in its normal position were visualized on an abdominal ultrasound. The spleen was located intraoperatively in the lower abdomen, adhered to the ileum and appendix. It was 720° twisted and had necrotic areas. The patient underwent an appendectomy with splenectomy with a smooth post-operative course; combination meningococcal and pneumococcal vaccines were administered; and antibiotic prophylaxis was started for the patient.
Conclusion: High clinical suspicion and the use of imaging modalities like ultrasound and CT scan are extremely crucial to diagnose wandering spleen and perform splenic salvage surgery because its clinical diagnosis is challenging.
Keywords: wandering spleen, torsioned spleen, splenopexy, splenectomy
Background
The term “wandering spleen” refers to splenic hypermobility and loss of fixation brought on by the laxity or underdevelopment of the suspensory ligaments in the spleen.1,2 The ligaments stretching and, frequently, the spleen’s axial rotation is linked to this loss of fixation.3 This propensity can be amplified by additional acquired and congenital factors.1 Congenital causes such as abnormal mesogastrium development have been proposed.4,5 However, pregnancy is mentioned as an acquired cause.6
It is a rare disease in children that has only sometimes been documented. It can be asymptomatic or can cause chronic symptoms from an abdominal mass in addition to sudden surgical emergencies with splenic infarction due to torsion.7,8 About 0.2–0.3% of individuals who need a splenectomy had wandering spleens detected.8 Due to the symptoms’ lack of specificity, diagnostic modalities like ultrasound and Computed Tomography scan are crucial for the diagnosis.2,9,10 Splenic torsion may be misdiagnosed as acute cholecystitis, appendicitis, gastric hemorrhage, intestinal obstruction, colon cancer, urine retention, and torsed ovarian cyst.3,8 Surgery is one of the treatment choices for wandering spleen, and laparotomy or laparoscopy methods can be used to perform splenectomy, or splenopexy.2
The purpose of this case report is to discuss a 12-year-old male child who appeared with an acute abdomen caused by a wandering spleen, along with acute appendicitis and splenic torsion.
Case Presentation
A 12-year-old male boy complained of crampy, lower abdominal pain that had been going on for four days. Additionally, he had a history of appetite loss, constipation, and mucoid diarrhoea. He also expressed abdominal distension, however, he had never vomited. No family history of similar symptoms was identified. He resides with his parents, three siblings, and grandparents. There were no recognized medical conditions in the child or his family.
On evaluation, the patient was acutely sick looking, appeared to be in severe agony. His vital sign was remarkable for tachycardia (pulse rate of 134 beats per minute), a respiratory rate of 22 breaths per minute, a temperature of 36.40°C, and a blood pressure of 110/75 millimetre of mercury. He lacked a depressed eyeball and had moist buccal mucosa. His abdomen was distended, moves with respiration, and tender everywhere else but the epigastrium. An 8 cm by 5 cm firm, tender mass across the left lower quadrant (Figure 1) with the lowest boundary out of reach, and no evidence of fluid accumulation. The assessment of other systems was normal.
 |
Figure 1 Visible lower abdominal mass on abdominal examination. |
Investigations
Blood tests were conducted which revealed a white blood cell count 10,300/micL with a neutrophilia of 78.5%, with moderate anemia (Hg 8.6 g/dl, Hct 28%), MCV 86 fl and platelet 775x103/micL. Ultrasound investigation identified a whirlpool sign at the splenic vessel, and the spleen is held in place in the lower abdomen with change in echogenicity. Wandering spleen with focal area infarction was the ultrasound diagnosis.
Treatment and Outcome
The patient was kept nil by mouth and was put on maintenance fluid. He was started on broad-spectrum antibiotics and analgesia. After stabilizing the patient an emergency laparotomy was done. Intraoporately slightly enlarged spleen located intraperitoneally below the level of umbilicus. Vascular pedicle torsioned 720° was found unusually entering via the convexity of the spleen (Figure 2). Areas of necrosis apparent as soft pale patchy areas were noted (Figure 3). There was adhesion to the tip to appendix and loop of terminal ileum (Figure 4). There was no accessory spleen. Appendix tip was erythematous with petechial bleeding up on releasing from its adhesion to the spleen but the ileum was released from the adhesion uneventfully. With an intraoperative diagnosis of wandering spleen with multifocal infarction secondary to splenic volvulus plus secondarily inflammed appendix, splenectomy and appendectomy was done. Post-operative period is uneventful. He stayed for 2 hours in recovery and was then transferred to a surgical ward and stayed for seven days. After seven days stay, the patient was discharged with PO amoxicillin prophylaxis and appointed after a week for pneumococcal conjugate vaccine.
 |
Figure 2 Intra operative finding shows torsioned spleen along mesentery. |
 |
Figure 3 Intra operative finding shows focal infarct of spleen. |
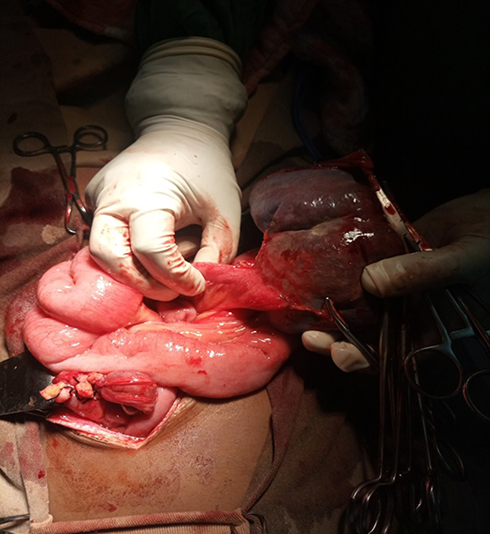 |
Figure 4 Intra operative finding shows adherence of ileum and appendix with spleen. |
Discussion
The spleen is a vital organ in both newborns and prepubescent children. It is a pulpy organ about the size of a fist that holds the body’s largest single collection of lymphoid tissue. It is located obliquely in the left hypochondrium and consists of ligaments, which are peritoneal attachments named after the organs to which they attach. These ligaments, which include the lienorenal, splenocolic, splenophrenic, gastrosplenic, and phrenicocolic ligaments, keep the spleen in the left hypochondrium where it normally occupies an anatomical position.11,12 Consequently, the lack or laxity of the aforementioned ligaments enables the spleen to be freely mobile in the abdominal cavity and to be mostly found in the pelvis, causing a condition called wandering spleen.13 Dorsal mesogastrium is also responsible for the formation of the peritoneum, the greater omentum and several peritoneal folds. Embryologically, Congenital defects of the mesogastrium are the cause of the spleen’s excessive motility.7,14 All cases of wandering spleen have been found associated with long splenic pedicle which contains splenic vessels and pancreas.15–17
This uncommon condition also known as splenoptosis, is most frequently found in children and women of childbearing age.6 Children account for one-third of instances, with most (70%) being older than 10 years.5 Fewer than 500 cases are reported with incidence of less than 0.2%.17
The clinical presentation of a wandering spleen is variable. It may pass asymptomatically throughout life.18 Despite the fact that the majority are probably asymptomatic, some require surgical intervention because to acute or chronic torsion, which can result in symptoms including abdominal discomfort, a mass in the abdomen, symptoms of splenic infarction, or left side portal hypertension.14,19 Wandering spleen can also cause intestinal obstruction which can be the initial presentation.20 Potential complications of wandering spleen includes sepsis, splenic rupture, and acute pancreatitis.21 Patients with splenic torsion may appear with an acute abdomen from an infarction. Reports showed that Spleen weight larger than 500gm and prolonged twisting greater than 180° predispose to splenic infarction.6,15 Similarly, in our case, the spleen had a 720° twist and was grossly enlarged.
Absence of spleen in its location and finding of spleen in other site is confirmatory sonographic diagnostic modality for wandering spleen. Doppler and color flow sonography were also used in the diagnostic evaluation because of their capacity to noninvasively evaluate splenic parenchymal flow and flow in major splenic vessels; however, Contrast-Enhanced Tomography (CECT) scan may be required if bowel gas obscures visualization of spleen.1,3,22 Other diagnostic modalities are Magnetic Resonance Imaging (MRI), splenic angiogram and scintigraphy.20
Splenectomy, which involves removing the entire spleen, and splenopexy, which involves preserving the spleen, are two surgical treatments for managing a wandering spleen.4 One of the main dangers of having the spleen removed is post-splenectomy septicemia, and patients who have had the procedure are more susceptible to infection, particularly from encapsulated pathogens such Streptococcus pneumoniae, Neisseria meningitidis, and Hemophilus influenzae.23 Overwhelmingly,post-splenectomy sepsis has a mortality rate between 30 and 60%.24 Therefore in patients with a viable spleen, splenopexy is the surgical procedure of choice in order to preserve the spleen, regardless of the presence of symptoms.25,26 Only splenic torsion patients with significant infarction and thrombosis of the splenic vessels should undergo splenectomy.1,19
Even though it has a strong immune function, the absence of a functioning spleen very slightly increases the risk of fulminant infection in otherwise healthy adults. However, the spleen’s capacity to phagocytose and destroy organisms is crucial for the host’s resistance against severe bacterial sepsis in the very young and in people with very major underlying illnesses.11 The use of combination vaccines against Hemophilus influenzae, polyvalent pneumococcal, and Neisseria meningitidis is advised at least three days prior to an elective splenectomy if performing one is necessary.27 Prophylactic penicillin in addition to pneumococcal and meningococcal vaccines should be administered to all patients who have had splenectomy.4,28
Conclusion
Clinically, wandering spleen is quite challenging to diagnose, thus it’s essential to use diagnostic tools like ultrasound or CECT scan to identify the condition early. If the spleen is viable and there is no thrombosis, splenopexy is advised. Splenic torsion with infarction should be treated with a splenectomy, and with provision prophylactic antibiotics, and a pneumococcal and meningococcal vaccine combination to prevent post splenectomy sepsis.
Ethical Clearance
Ethical clearance was obtained from Arba Minch University Research Ethics Review Board. The protocol No MA9. Arba Minch University, Arba Minch, Ethiopia.
Consent
Verbal informed consent was taken from both parents and the child to use patient medical information and images for the publication. Both parents and the child gave the consent. Consent was witnessed and verified by research ethics review board chair person. The address of mentioned person is stated on ethical clearance letter submitted with the manuscript.
Acknowledgment
We would like to acknowledge the patient for providing us consent to share his history as a case report and Arba Minch general hospital and Arba Minch University for evaluating the case and giving us ethical clearance.
Funding
No specific grant was obtained for this case report from any funding agency.
Disclosure
The authors declare that there is no conflict of interest regarding the publication of this article.
References
1. Nemcek AA, Miller FH, Fitzgerald SW. Acute torsion of a wandering spleen: diagnosis by CT and duplex Doppler and color flow sonography. Am J Roentgenol. 1991;157(2):307–309. doi:10.2214/ajr.157.2.1853811
2. Fiquet-Francois C, Belouadah M, Ludot H, et al. Wandering spleen in children: multicenter retrospective study. J Pediatr Surg. 2010;45(7):1519–1524. doi:10.1016/j.jpedsurg.2010.03.003
3. Dawson JM, Roberts NG. Management of the wandering spleen. Austral NZ J Surg. 1994;64(6):441–444. doi:10.1111/j.1445-2197.1994.tb02249.x
4. Stringel G, Soucy P, Mercer S. Torsion of the wandering spleen: splenectomy or splenopexy. J Pediatr Surg. 1982;17(4):373–375. doi:10.1016/S0022-3468(82)80492-2
5. Steinberg R, Karmazyn B, Dlugy E, et al. Clinical presentation of wandering spleen. J Pediatr Surg. 2002;37(10):1–4. doi:10.1053/jpsu.2002.35443
6. Faridi MS, Kumar A, Lubna IN, Shahid R. Wandering spleen-a diagnostic challenge: case report and review of literature. Malay J Med Sci. 2014;21(6):57.
7. Allen KB, Andrews G. Pediatric wandering spleen—the case for splenopexy: review of 35 reported cases in the literature. J Pediatr Surg. 1989;24(5):432–435. doi:10.1016/S0022-3468(89)80395-1
8. Kapan M, Gümüş M, Önder A, Gümüş H, Aldemir M. A wandering spleen presenting as an acute abdomen: case report. J Emerg Med. 2012;43(5):e303–5. doi:10.1016/j.jemermed.2010.06.029
9. Assaf R, Shebli B, Alzahran A, et al. Acute abdomen due to an infarction of wandering spleen: case report. J Surg Case Rep. 2020;2020:rjz378. doi:10.1093/jscr/rjz378
10. Schaarschmidt K, Lempe M, Kolberg-Schwerdt A, Schlesinger F, Hayek I, Jaeschke U. The technique of laparoscopic retroperitoneal splenopexy for symptomatic wandering spleen in childhood. J Pediatr Surg. 2005;40(3):575–577. doi:10.1016/j.jpedsurg.2004.11.020
11. Bowdler AJ. The Complete Spleen: Structure, Function, and Clinical Disorders. Springer Science & Business Media; 2001.
12. Taher H, Abdellatif M, Tarek M, El Tagy G. Torsion of wandering spleen in an infant associated with hamartomatous vascular malformation. J Pediatr Surg Case Rep. 2019;40:13–16. doi:10.1016/j.epsc.2018.10.001
13. Viana C, Cristino H, Veiga C, Leão P. Splenic torsion, a challenging diagnosis: case report and review of literature. Int J Surg Case Rep. 2018;44:212–216. doi:10.1016/j.ijscr.2018.02.032
14. Schmidt SP, Andrews HG, White JJ. The splenic snood: an improved approach for the management of the wandering spleen. J Pediatr Surg. 1992;27(8):1043–1044. doi:10.1016/0022-3468(92)90555-L
15. Buehner M, Baker MS. The wandering spleen. Surg Gynecol Obstet. 1992;175(4):373–387.
16. Desai DC, Hebra A, Davidoff AM, Schnaufer L. Wandering spleen: a challenging diagnosis. South Med J. 1997;90(4):439–443. doi:10.1097/00007611-199704000-00017
17. Satyadas T, Nasir N, Bradpiece HA. Wandering spleen: case report and literature review. J R Coll Surg Edinb. 2002;47(2):512–514.
18. Hamdy O, Yousry M, Saleh GA. An infarcted wandering spleen leading to a sigmoid volvulus presenting with acute large bowel obstruction: a case report. Ann R Coll Surg Engl. 2021;103(4):e127–30. doi:10.1308/rcsann.2020.7144
19. El Bouhaddouti H, Lamrani J, Louchi A, et al. Torsion of a wandering spleen. Saudi J Gastroenterol. 2010;16(4):288. doi:10.4103/1319-3767.70618
20. Bairwa BL, Gupta S, Singh AK, Gupta P. Wandering spleen with torsion: a rare cause of acute abdomen in a 14-year-old girl. Arch Clin Cases. 2022;9:56–61. doi:10.22551/2022.35.0902.10204
21. Lugo-Fagundo E, Fishman EK. Wandering spleen with torsion and infarction: a case report. Radiol Case Rep. 2022;17:3377–3379. doi:10.1016/j.radcr.2022.06.073
22. Tang PH, Tangaperumal A, Ahmad NA, Bahari M, Mra A, Teh YG. Torsed wandering spleen as a cause of recurrent abdominal pain in a child. Radiol Case Rep. 2022;17(5):1794–1797. doi:10.1016/j.radcr.2022.03.017
23. Zarrintan S, Jamali F, Tubbs RS, Khaki AA, Salavati A, Tanoomand A. A wandering spleen presenting as a pelvic mass: case report and review of the literature. Folia Morphologica. 2007;66(2):152–154.
24. Seashore JH, Mclntosh S. Elective splenopexy for wandering spleen. J Pediatr Surg. 1990;25(2):270–272. doi:10.1016/0022-3468(90)90438-F
25. Awan M, Gallego JL, Al Hamadi A, Vinod VC. Torsion of wandering spleen treated by laparoscopic splenopexy: a case report. Int J Surg Case Rep. 2019;62:58–61. doi:10.1016/j.ijscr.2019.06.040
26. Najid F, Sandrasecra S, Asyraf MZ, et al. Wandering spleen as a cause of acute abdomen: a surgical conundrum from acute appendicitis to splenic torsion and ischemic small bowel volvulus. Mal J Med Health Sci. 2020;16(1):33.
27. Soleimani M, Mehrabi A, Kashfi A, Fonouni H, Büchler MW, Kraus TW. Surgical treatment of patients with wandering spleen: report of six cases with a review of the literature. Surg Today. 2007;37(3):261–269. doi:10.1007/s00595-006-3389-0
28. Sharma A, Salerno G. A torted wandering spleen: a case report. J Med Case Rep. 2014;8(1):1–4. doi:10.1186/1752-1947-8-133
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.