")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 11
Vulnerability to HIV infection among the Borana pastoral community of Southern Ethiopia: a persisting challenge
Authors Serbessa MK
Received 1 November 2018
Accepted for publication 5 February 2019
Published 18 April 2019 Volume 2019:11 Pages 69—76
DOI https://doi.org/10.2147/HIV.S193035
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Bassel Sawaya
Video abstract presented by Dr Serbessa.
Views: 1271
Mirgissa Kaba Serbessa
Department of Preventive Medicine, School of Public Health, Addis Ababa University, Addis Ababa, Ethiopia
Background: Vulnerability to HIV infection is a major concern in an effort to control further infections. What drives vulnerability among pastoral settings of Ethiopia is not well documented.
Objectives: This study aims to identify drivers of vulnerability to HIV infection among the Borana pastoral community of Ethiopia.
Methods: Data were collected during 2008–2009 as part of a PhD work and subsequently in 2014 and 2016, during a follow-up visit to Borana. Data on perceived threats of HIV, facilitators of vulnerability, coping mechanisms and perceived consequences were collected by trained research assistants using topic guides developed for this purpose. In-depth and key informant interviews and Focus Group Discussions (FGDs) with selected married men and women, opinion leaders, and HIV focal persons of public sectors and Non Governmental Organizations in Teltele, Arero, Yabelo and Moyale were carried out. Sample transcripts were checked for consistency and completeness before data collection was completed. Two qualitative researchers read transcripts and suggested themes and subthemes in reference to the objective of the study. Transcripts were imported to MAXQDA software. Thematic analysis was applied to reduce data into defined themes. Findings were interpreted following the objective of the study.
Findings: The results show that HIV is a major threat in Borana with individual and community level consequences. Concurrent extramarital sexual practices, men’s role in the selling of livestock and consequent encounters with “other” women facilitate vulnerability to HIV. Lack of information about HIV, availability and use of condoms, and failure to use local resources for HIV prevention were key limitations to coping with the problem. After nearly 40 years of HIV intervention in Ethiopia, coping mechanisms are not exploited in Borana.
Conclusion: Vulnerability to HIV among the Borana pastoral community is facilitated by multiple factors that work in tandem, thus calling for interventions that address the different factors at the same time.
Keywords: pastoral community, HIV and AIDS prevention, vulnerability, coping mechanisms, threats of HIV, perceived consequences of HIV, facilitators of HIV, pastoral community
Introduction
Available evidence on HIV and AIDS tends to be related to risk and vulnerability interchangeably. While risk is an outcome of threats/hazards/stressors, vulnerability is the potential to be exposed to but lack of means to cope with threats/hazards/stressors.1,2
According to Chambers,3 vulnerability is defenselessness against threat due to exposure to shocks, stress and risk, but lacking the means to cope with the factors facilitating vulnerability. Failure to cope with factors of vulnerability could be attributed to physical weakness, economic impoverishment and poor social support mechanisms. Guided by Chamber’s definition of vulnerability, Watts and Bohle4 suggested three factors that are believed to facilitate the understanding of vulnerability. These are risk of exposure, lack of necessary resources to cope and being subjected to the consequences. Several reports in the literature have since been published to study how these factors together facilitate vulnerability to HIV infection.5–7
An individual’s behavior has long been documented as a major risk factor contributing to vulnerability to HIV infection.8,9 Such an emphasis on risk neglects the broader context underlying the risk and creates a favorable opportunity for the spread of HIV infection. In this regard, it is documented that due to their unique biological features, socio-cultural subordination and relative lack of the means to cope with HIV infection, women in Sub-Saharan Africa are 2.5 times more at risk of HIV infection as compared to men.10 As a result, design of responses against HIV is often guided by the notion of women as the most affected group although such arguments appear to neglect cultural, social and economic domains of women and HIV as a problem.11
In Ethiopia, there are limited studies on vulnerability particularly in connection to the epidemic of HIV. However, there are reports from epidemiological synthesis that documented market places, urban settings, prisons etc as hotspots.12 The same report and some others have further documented that female sex workers, mobile workers, in and out of school youth, uniformed services, widows, divorcees and separated women are most at risk.12–14 Furthermore, concurrent extramarital sexual practices, polygamy and marrying a sister of a deceased wife are documented as facilitators of HIV infection.15,16 Although it is not well documented, the tradition of keeping an extramarital sexual partner by men as well as women, widow inheritance and polygamy appears to have declined although they are still there in secret.15 Despite lack of studies on vulnerability to among the Borana population, a few behavioral and biological studies show relatively high HIV prevalence in the region as compared to similar settings.17,18
Informed by Watts and Bohle’s vulnerability framework,4 this paper aims to explore if the Borana pastoral community consider HIV as a threat, available means to cope with the threat and identify factors facilitating vulnerability and consequences of HIV infection. The finding from this study may help to challenge the long-established risk-focused studies on HIV infections and its compromised programmatic implication. In addition, the result from this study will inform HIV programming and intervention particularly in Borana’s pastoral community and may also inform HIV intervention in pastoral settings.
Materials and methods
Study area
The Oromo occupy about 40% of the land surface of Ethiopia and constitutes the same proportion of the Ethiopian population.20 The Borana community is considered as a senior Oromo clan which has long maintained the Gada system of social and political organization of the Oromo.19 The Gada system has been the basis of social, cultural and political Organization of the Oromo society since the early 13th century with elections of their leader Abba Gadaa to the highest political position for the last 8 years.19 The Gada system has been maintained by the Borana and neighboring Guji despite pressure from the central government over a long period.
Geographically, Borana is one of the 18 administrative zones in Oromia regional state. Borana zone is situated in a relatively arid area of the southern part of Ethiopia bordering with Somalia to the east and Kenya to the south. In addition, the zone borders with Gujii and Bale zones of the Oromia region to the north and northeast and Konso district of the Southern National Regional state to the west. The most recent census estimates the Borana population at a little over 1 million. The zone is divided into 13 districts. Characteristically livestock rearing is the major economic mainstay and people in all districts share common social and cultural features. Initially, three districts (Teltele, Arero and Liben) were arbitrarily chosen for the study although participants in subsequent key informant interviews were drawn from Moyale and Yabelo districts of the zone guided by the snowball technique and based on the investigator’s previous orientation of people in the zone.
Methods of data collection and analysis
A topic guide was developed following the objectives of the study. Accordingly key discussion points and probes were developed with a focus on whether HIV is perceived as a threat, facilitators of vulnerability, means to cope with the problem and perceived consequences of HIV. Using the guide, initial data were collected during October 2008 and April 2009 as part of a PhD dissertation. The same topic guide was used to generate evidence under the same theme during a follow-up visit to the study setting twice in 2014 and 2016. During the initial visit in 2008–2009, a total of 69 in-depth interviews and eight Focus Group Discussions (FGDs), four with sexually active women and men, were completed. A total of 12 key informant interviews were completed with local traditional leaders (Abba Gadaa), prominent women who are known to be role models as a mother and wife, HIV focal persons of the zonal health department and representatives of NGOs with HIV and AIDS programs that have offices in Yabelo (Capital of the Borana zone) during subsequent visits. While in-depth interviews were used to generate evidence on participant’s perceptions of HIV as a threat, experiences of concurrent multiple sexual activities and perceived consequences of HIV infection, FGD and key informant interviews were used to explore the local understanding of HIV as a threat and its consequences, facilitators of HIV infection, and local coping resources. While snowballing was used to identify FGD and key informant participants, in-depth interview participants were purposefully selected based on information generated from reliable local sources. The number of study participants was determined on the basis of saturation of information where no new information is forthcoming after a couple of subsequent interviews at all the different study settings.
Trained research assistants collected data using the local language (Afaan Oromo). Topic guide with probes was developed to guide data collection. In addition to scribbles taken during the interview and discussions, voice recordings were made to capture all the information. At the end of every day, notes were exchanged and discussions were held with assistants to identify gaps that needed to be addressed the next day. In order to reduce raw data to meaningful categories, relevant sections of the recordings were transcribed first into local language and translated into English and samples of these were back translated into Afaan Oromo to ensure accuracy and consistency of transcription.
Two independent experts of qualitative research were given the transcribed document along with the objectives of the study to define major themes and subthemes. A few differences of the themes from the two experts were clarified through phone discussion. Thematic analysis was used to analyze the data. The analysis was facilitated by application of qualitative data analysis software, MAXQDA 10. Interpretation of the findings followed the objective of the study. Pseudonyms were used to maintain anonymity of research participants. Widely shared views were quoted to substantiate findings. Age, sex and method used to generate that evidence and residence of the participant are shown in parentheses for easy reference.
Ethics statement
The Swiss Tropical and Public Health Institute of the University of Basel ethically cleared the PhD proposal of this study. A letter of ethical clearance from the university was submitted and the purpose of the study was explained to the zonal administration and health department of Borana. The zonal health department subsequently facilitated entry into the study community. Permission to collect additional data in 2014 and 2016 was obtained from the Borana Zone Health Department. During data collection, individual participants were provided with information on the purpose of the study, type of data to be collected, use of the result to the community and the country at large. In addition, participants were informed that there would be no harm in connection to their participation in the study and information they provide remains anonymous. Furthermore, participants were informed that participation is voluntary and the interview would take a maximum of an hour. Accordingly, in line with the IRB provisions, informed oral consent was obtained from all the participants except three who were not available for interview after repeated visits.
Findings
Profile of participants
The participant’s age profile shows that two out of three men and women who participated in the FGDs and in-depth interviews were in the age range of 30–39 years. Participants were found to be followers of either the local religion (Waaqefanaa) or Islam. All participants were married with stable marital relations and had children. Economically, those in Yabello and Teltele mainly practice agriculture and livestock rearing combined while those in the rest of the weredas are mainly pastoralists.
Findings from the two phases were entirely the same with no difference including the way explanations were made. Details of the findings are presented following themes and sub-themes as elaborated in Table 1 and further detailed below.
 | Table 1 Themes developed according to the objectives of the study |
Perception of HIV as a threat
Study participants unanimously argued that HIV is a “disease” with no cure (dhibee qorsa hinqabne) and is considered a major health challenge in Borana. One in three participants felt this problem is a curse for people who broke agreed socio-cultural values and religious principles among which respect for elders, contributing to the good of Borana and keeping Borana culture alive are just a few. Two-thirds of participants reported that they had heard that the “disease” prevails more seriously in towns where Borana people are not dominant. Participants unanimously argued that HIV has killed several people and is still continues to do so. One of the participants explained, “HIV is a disease that forces people to lose their loved ones to death, like a tree releases its leaves during the dry season” [79M, II Arero]. Although Borana has local resources for sexually transmitted infections, HIV remains to threaten life with no solution in sight. It was emphasized that:
Gonorrhea has been and is a common sexual health problem in Borana and yet it has never been scary since we have locally prepared medicines from such plants as awachoo [Albeizaanthelimentic] and if it becomes chronic, soup made from the bone of an ostrich will absolutely cure the problem. However, this new disease called HIV remains a challenge for which we cannot do anything. For us, HIV is a curse and Waaqaa (omnipresent supernatural force believed as creator of both living and non-living things) has left us to be punished. [35M, II Liban]
Further arguments revealed that HIV is a major threat in Borana for those who engage in sexual activity with non-regular sexual partners. One of the participants elaborates that: “In Borana, we suspect those who maintain sexual affairs with more men or women other than spouse and their regular sexual partner (Jaalaa or Jaalto) are most affected by HIV infection” [57M, FGD Teltele]. The question about who is more threatened by HIV infection revealed that both men and women are equally vulnerable to HIV infection. However, women informants commonly argued that, “Although men are more mobile and encounter “other women” than their regular partner which may expose them to HIV, they bring it back to us. Thus, men may get it first but his wife and jaaltos (regular girlfriends) will get it from them” [37W, II Dida Hara]. On the other hand, other women participants emphasized that, “Men and those who are in towns are more affected. Yet, it is a “disease” for everyone in Borana due to rural-urban connection mainly through market and no one is spared” [42W, FGD Arero].
Facilitators of HIV infection as a threat
Gender roles
In Borana, the spread of HIV infection is attributed to different locally established socio-cultural roles. Men and women in Borana have roles and expectations both at family and community levels. It was gathered that men have out of house (external) roles such as hunting, pasturing and watering livestock and representation of the family and sometimes the clan at public forums. Women’s role on the other hand is limited to in house (internal) and homestead with such responsibilities as house construction, caring for children and the elderly, and household chores. In connection to such roles, women stay around the home while men always stay out of the home and away from his wife(s) and jaaltos. One in three women and slightly less men reported that in connection to their mobility men are more vulnerable to HIV infection. As men travel away from home, it was argued that they may meet “other women,” who are not their regular sexual partners (marital and jaaltos). This is argued to facilitate exposure of such men to HIV infection. Women informants stressed that, “HIV is a problem that prevails in urban settings where women who work in bars are found and our men may have sexual relations with such women when they visit towns” [37W KII, Moyale]. Both men and women unanimously argued that men are exposed to HIV in connection with their socio-culturally sanctioned role. One of the participants stressed that, “No woman is vulnerable to HIV infection by their own action since they remain loyal to their husband and regular sexual partner and do not have other exposure (jaalaa)” [W56, II Arero].
Market places
The livestock markets are famous in Borana. There are four big markets (Harobake, Dida Hara, Dubuluk and El-waye) all of which are found within 50 kilometers radius from Yabelo. These markets draw business people and commercial sex workers from across Ethiopia. One of the participants pointed out that:
Sale of livestock is the responsibility of men. As such men take livestock for sale to the markets when they temporarily met “other women” who come to market places to earn money from our men. Although we [women] also meet our jaala at the market places, this is not a problem since we know each other for long. [W42, II Liben]
Another informant emphasized that, “Men do not only meet their extramarital partner (jaaltoo) at market places but also have encounters with other women who come from out of Borana. This is the source of concern for most of us since they may bring HIV to us” [W37, II Dida Hara].
One in six men admits that sexual encounter with other women during market days is an exception. One of the participants explained that:
I come to market to sell cattle to pay various fees. Once I sell, I would invite my jaalto and buy her gift. This is common in Borana. There are, of course, few other men who run with women who come from other places only on the market days to make money. This is indeed our concern. [M45, KII Liben]
Market centers in Borana are generally considered by women research participants as centers of sexual negotiation and encounters and consequently an opportunity for the spread of HIV.
Extramarital sexual partnership
Historically, extramarital-concurrent sexual engagement is common among the Borana. There are various reasons that have social, cultural and economic basis for such practices complementing biological drive. There is a separate article published on this.15 It is however relevant to recognize that such a practice has been widely practiced in the past although this practice (and others) is not as open and wide a practice as it used to be. Yet, participants argued that the practice is still recognized among the Borana and it is believed to facilitate HIV infection. One in three participants irrespective of their sex unanimously argued “While we recognize HIV exists and it is with us and worries us, jaalaa-jaaltoo is still practiced although in much more secret” [W 37, II Liben]. Local community’s practice of jaalaa-jaaltoo is far from mere sexual engagement. One of the participants emphasized that, “Keeping regular sexual partner is not about just sex, but it is about social, economic and cultural support mechanisms” [37W, II Teltele].
Coping with HIV infections
Coping is the reflection of various factors related to personal capabilities to protect oneself. This is the reflection of factors elaborated as below.
Awareness about HIV
Our findings show that one in four participants reported to have heard about HIV and its mode of transmission. Further query on the modes of transmission reveals that belief on sharing skin piercing objects such as needles and blades and sexual engagement with nonregulars facilitate HIV transmission from one person to the other.
In as much as translating the information gained is not straightforward for various reasons, those who provided such information were found to cast doubt on the authenticity of the message itself. Local health extension workers, schoolchildren, teachers and NGO officers working on HIV in Borana were found to be sources of information on HIV. Study participants, however, unanimously doubted the credibility of information received from such sources. One of the informants emphasized that:
I think we [community members] are not getting reliable information about how HIV is transmitted and means of prevention. Normally the community do not trust health extension workers, school children and school teachers, who are too young themselves to provide reliable information to the community about the disease. [W52, II Liban]
We found that in Borana, important information comes from the Gada leader and his messenger (maakala) and young people are considered as learners. The fact that messages failed to recognize the realities on the ground where abstinence before marriage is unquestionable and faithfulness after marriage may not be enforced. This was underscored by one of the participants:
In principle chastity is normal expectation in Borana and family members as well as the community is expected to ensure this to be observed. However, following marriage we used to keep extramarital partner not only for sexual interest but socio-economic reasons. [49M, KII Mega]
Although there was limited evidence, some participants expressed concern over lack of awareness and skill on how to care for those who are bed ridden.
There was this women who have got children and her husband died some years back. She was busy caring for her children and at times clan members used to help her. She got sick and remained on bed. Although she was taken to health facility, her health deteriorated. As neighbors we did not know how to care for this women and whom to talk to. [W30, KII, Yabelo]
There were repeated questions participants asked the research team on how condoms work in preventing HIV infection. “How does condom help to prevent HIV infection? We do not know much about this. It would be good if we are given information as well as the condom” [M32, Dubluk, FGD].
Condom use
Study participants invariably argued that usually the Borana community felt helpless with regard to prevention of HIV. Participants commonly expressed concern that “One who got it ultimately dies for there is no cure.”
At least one in three male and one in five female research participants reported to have heard that condom prevents HIV infection. A participant pointed out that, “I heard that condom prevents HIV infection, but I do not know how it works. I would love to know how it work and where to obtain it” [W39, FGD, Harobake]. Research participants expressed concern about potential problems that may be associated with condom use as well.
[…] in our community, people talk about condoms preventing HIV infection. The problem however is that it may prevent seminal fluids from passing in and may affect conception or it may remain in woman’s body after sexual activity that may create health problems to the woman. We would like to learn more about it and how it. [W57, FGD Harobake]
HIV intervention program
It was obvious that there is no organized and clear response against HIV. Discussion with the HIV focal person at the Zonal Health Department revealed that due to limited financial and human resources, there is limited response at health facility level, especially in accessing information by the community. The focus now is on provision of services such as HCT and ART. Equally important is the fact that non-governmental- and community-based organizations with an HIV program in the zone do not have services that meets the interests of the community. One of the participants argued that, “It looks like HIV is no more a major problem. What used to be a concern by local authorities and NGOs is no more there. This gave an impression that the disease is no more there” [M38, KII, Yabelo]. Unlike a few years back, currently, there is no HIV prevention and control program running at community and school level nor has there been any effort to use local influential people to share information.
Perceived consequences of HIV in Borana
It was discovered that the consequences of HIV in Borana is widespread. The findings show that consequences are perceived to prevail at individual, family and community levels.
Perceived consequences at individual level were argued in terms of what happens to an individual who is suspected of having HIV were described as losing weight and often leaving their usual area of residence for fear of stigma. One of the participants argued that, “Although we do not know who has HIV or not, people suspect those who get thinner and have a continuous loss of weight are likely to have HIV. I did not see someone who have died of HIV, since such people leave their usual residence to hide from potential discrimination” [M57, KII Teltele]. Another participant argued, “I know a man who died in our neighborhood presumably due to HIV. The guy has completely lost his flesh and finally died” [W39, FGD, Dubuluk]. Findings generally show that consequences at individual level are related to physical emaciation and death. Participants did not provide strong evidence with examples on what has happened to families and communities in their neighborhood or Borana in general due to HIV. Nonetheless, participants unanimously argued that HIV would compromise the family’s life and eventually Borana as a community will be losers. One of the participants argued that, “Strong Borana men are often liked by several women and they are the ones who easily catch HIV. This is a serious concern for Borana, as we will lose our strong men” [M52, KII, Alawaye].
Discussion
Following Chamber’s3 conceptualization of vulnerability as an exposure to risk and defenselessness due to a lack of the measures that would facilitate coping with the risk. Watts and Bohle4 simplified vulnerability as a factor of threat, lack of ability to cope and evidence of being subjected to consequences. Findings from this study helped to expound on HIV as a threat and socio-cultural factors facilitating infections in Borana as well as local coping mechanisms. The finding has also depicted the fact that vulnerability to HIV infection in the Borana pastoral community is facilitated by continued practices.
As a “disease with no cure” and recognized as a threat for the Borana community, individual susceptibility to the risk of HIV infection is related to men’s mobility, “other women’s” search for business opportunity at market places and continued extramarital concurrent sexual engagement. Men encounter HIV due to their role and consequent encounter with “other women” who are not regular partners. This has evident implication in exposing not only them but also their women sexual partners as well as being connected to the sexual network of the index man.21,22 As is evident from the findings and further shown in Figure 1, different factors operate together to facilitate vulnerability to HIV infection among the Borana pastoral community.
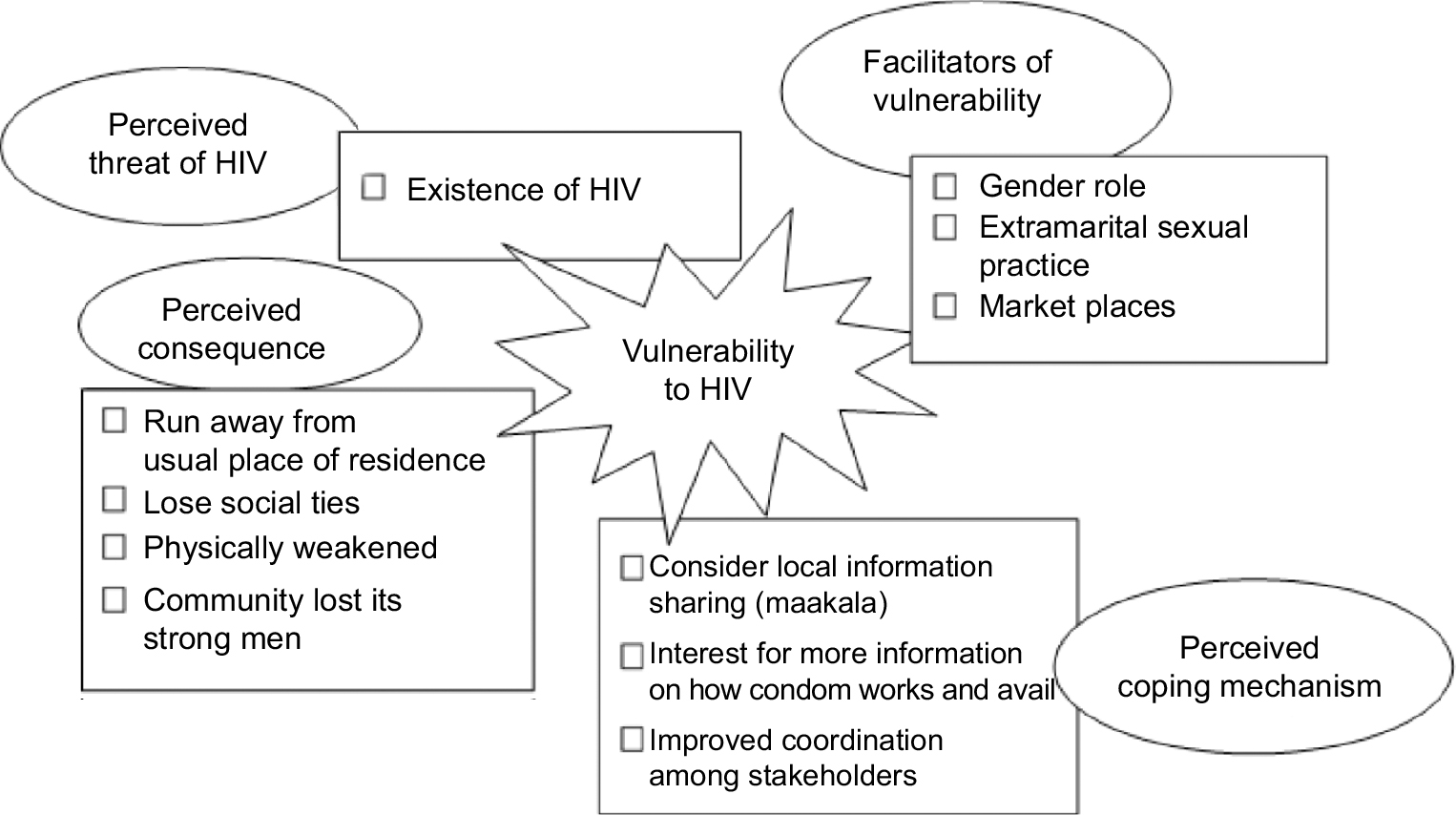 | Figure 1 Factors of vulnerability to HIV infection among the Borana pastoral community, Ethiopia. |
Figure 1 clearly depicts that vulnerability to HIV infection is facilitated by market places as hot spots and men’s encounters with “other women” that are not regular sexual partners at those places, extramarital concurrent sexual practices are believed to contribute to the spread of HIV infection. Countrywide, HIV in Ethiopia prevails mostly in urban settings and small towns as compared to rural areas.12 As a result, marketplaces in Borana are known to attract livestock traders, owners and commercial sex workers from within the country. So, these market places are contact points for different groups of people with different interests and are hotspots for HIV infection. Unlike economic and biological interests that are documented to drive multiple sexual partnerships,12,13,16 in Borana, extramarital sexual activity is facilitated by socio-cultural and economic interest other than biological drive.15,18 Extramarital concurrent sexual engagement has far-reaching social, cultural and economic reasons other than biological desire.15
Coping with the evident threat of HIV infection has continued to be compromised by limitations of awareness about HIV at individual and group level on the one hand and weak programmatic response on the other hand. It was found that HIV is believed to have no cure and those who bridge socio-cultural values and religious principles are more affected. Beyond such broad conception, limited awareness about causes and prevention methods remain the case. Existing prevention interventions were blamed to have failed to meet local contexts in connection to abstinence, faithfulness and condom use. A previous study has shown that, for Borana, there is an established communication route and there are individuals who the public recognizes as sources of information.23 Nonetheless, existing evidence and practice shows that HIV prevention campaigns target abstinence, faithfulness and condom use.5,12,13 In Borana, faithfulness is expected and enforced before marriage while extramarital sexual practice may not be ruled out following marriage while in as much as condom use is potentially acceptable there remains limited awareness on how they work and the implications of using them. Thus, coping with the spread of HIV has major limitations in Borana.
This study has involved different sections of the population and multiple settings using different qualitative methods. As a result, the findings are quite strong with programmatic implications for pastoral communities. Nonetheless, biological studies to determine the current level of prevalence would also help to determine the spread of HIV among the Borana pastoral community.
Conclusion
Following Watts and Bohle’s suggestion factors of vulnerability in Borana generated useful evidence that justifies the fact that vulnerability to HIV infection is facilitated by factors that work in tandem to determine a community’s vulnerability to HIV infection. The finding underscores that vulnerability is way beyond individual behavior where socio-cultural, economic and biological factors work in tandem to facilitate HIV infection. Intervention programs are expected to be designed to address the different factors at the same time.
Acknowledgments
I sincerely thank Prof Marcel Tanner who, during my PhD work, guided me and instilled in me the need to translate research results to solve practical problems. I would like to thank those who supported me while I was in Borana and shared their knowledge related to the research theme. I appreciate Jatani Dida who started as my research assistant but became a good friend and continued to help in my effort to know more about the Borana pastoral community. Financial support from NCCR North-South during the initial phase is duly acknowledged.
Disclosure
The author reports no conflicts of interest in this work.
References
World Health Organization. Planning Guide for the Health Sector Response to HIV/AIDS. Geneva: WHO; 2011. | ||
Nirupama N. Vulnerability and risk perception in the management of HIV/AIDS: public priorities in a global pandemic. Risk Manage Health Policy. 2008;1:7–14. | ||
Chambers R. Vulnerability, Coping and Policy (Editorial Introduction). IDS Bulletin; 37(4):33–40. | ||
Watts MJ, Bohle HG. The space of vulnerability: the causal structure of hunger and famine. Prog Hum Geogr. 1993;17(1):43–67. | ||
UNAIDS. Addressing Societal Causes of HIV Risk and Vulnerability: Report on the Global AIDS Epidemic. Geneva:UNAIDS; 2008. | ||
Higgins J, Hoffman S, Dworkin SL. Rethinking gender, heterosexual men and women’s vulnerability to HIV/AIDS. Am J Pub Health. 2010;100(3):435–445. | ||
Fagbamigbe AF, Lawal AM, Idemudia ES. Modelling self-assessed vulnerability to HIV and its associated factors in a HIV-burdened country. SAHARA-J. 2017;14(1):140–152. | ||
Auerbach JD, Parkhurst JO, Cáceres CF. Addressing social drivers of HIV/AIDS for the long-term response: conceptual and methodological considerations. Glob Public Health. 2011;6(Suppl 3):S293–S309. | ||
Johnson BT, Michie S, Snyder LB. Effects of behavioral intervention content on HIV prevention outcomes: a meta-review of meta-analyses. J Acquir Immune Defic Syndr. 2014;66(Suppl 3):S259–S270. | ||
Ramjee G, Daniels B. Women and HIV in sub-Saharan Africa. AIDS Res Ther. 2013;10(1):30. | ||
Jennifer FK, Vinh-Kim N. The Fourth Wave: Violence, Gender, Culture and HIV in the 21st C. Paris: UNESCO; 2011. | ||
Berhane Y, Mekonnen Y, Seyoum E, Gelmon L, Wilson D. HIV/AIDS in Ethiopia: An Epidemiological Synthesis. Washington DC: World Bank, Global HIV/AIDS program series; 2008. | ||
Yibeltal A. HIV/AIDS in Ethiopia: An Epidemiological Synthesis. Addis Ababa: Federal HIV and AIDS Prevention and Control Office; 2014. | ||
Kaba M, Taye G, Gizaw M, Mitiku I, Adugna Z, Tesfaye A. A qualitative study of vulnerability to HIV infection: places and persons in urban settings of Ethiopia. Ethiop J Health Dev. 2016;30(3):105–111. | ||
Mirgissa K, Ibrahim A, Damen HM. Extramarital sexual practices and perceived association with HIV infection among the Borana pastoral community. Ethiop J Health Dev. 2013;27(1):25–32. | ||
Miz-Hasab Research Centre. HIV/AIDS and Gender in Ethiopia: The Case of Ten Weredas in Oromia and Southern Nations and Nationalities People’s Region. Addis Ababa:Miz-Hasab research center; 2004. | ||
Tefera B, Ahmed Y. Contribution of the anti HIV/AIDS community conversation programs in preventing and controlling the spread of HIV/AIDS. Ethiop J Health Dev. 2013;27(3):216–229. | ||
Mela Research. Know Your HIV Epidemic/Know Your HIV Response (KYE/KYR) Synthesis in Oromia, Ethiopia. Addis Ababa, Ethiopia; 2014. | ||
Asmarom L. Gada: three approaches to the study of African society. 1st ed. New York: Free Press; 1973. | ||
Adugna A. Oromiya: demography and health. November 2017. Available from: www.EthioDemographyAndHealth.Org. | ||
Anteneh ZA. Prevalence and correlates of multiple sexual partnerships among private college students in Bahir Dar City, Northwest Ethiopia. Sci J Publ Health. 2013;1(1):9. | ||
Kenyon CR, Tsoumanis A, Schwartz IS. HIV prevalence correlates with high-risk sexual behavior in Ethiopia’s regions. PLoS One. 2015;10(10):e0140835. | ||
Mirgissa K. Tapping local resources for HIV prevention among the Borana pastoral community. Ethiop J Health Dev. 2013;27(1):33–39. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.