")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 12
Voluntary HIV Counseling and Testing Among Commercial Motorcyclist Youths: An Exploration of Ethical Challenges and Coping Mechanisms in Dar es Salaam
Authors Mlughu TS, Anaeli A, Joseph R, Sirili N
Received 26 April 2020
Accepted for publication 8 October 2020
Published 3 November 2020 Volume 2020:12 Pages 675—685
DOI https://doi.org/10.2147/HIV.S259997
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Thadei S Mlughu,1 Amani Anaeli,2 Renatha Joseph,1 Nathanael Sirili2
1Department of Bioethics and Health Professionalism, Muhimbili University of Health and Allied Sciences, Dar es Salaam, Tanzania; 2Department of Development Studies, Muhimbili University of Health and Allied Sciences, Dar es Salaam, Tanzania
Correspondence: Nathanael Sirili Department of Developmental Studies
Muhimbili University of Health and Allied Sciences, Dar es Salaam, Tanzania
Email [email protected]
Background: Regardless, the known benefits of voluntary testing and counseling (VCT) in the fight against HIV/AIDS, its uptake is still low among youth. This study explored ethical challenges facing voluntary counseling and testing for HIV/AIDS among youth engaged in commercial motorcycling in Kinondoni municipality, Dar es Salaam city.
Methods: Qualitative exploratory study was carried out to 35 people using key informants’ interviews (KIIs), in-depth interviews (IDIs), and focus group discussions (FGDs). Key informants were purposefully selected based on their roles in VCT services, while the FGD participants and in-depth interview respondents were purposefully selected among youth commercial motorcyclists. Qualitative content data analysis was used to analyze the gathered information.
Findings: Results of this study show that lack of privacy during counseling and treatment, fear of HIV status disclosure to others by counselors and difficulties in counseling are the main ethical challenges facing VCT services among youth in Kinondoni municipality. Shortage of counselors to match the number of VCT services’ clients and lack of on-job training on HIV/AIDS testing and counseling among counselors partly contributed to the revealed ethical challenges. In an attempt to address the ethical challenges, youth peer educators and routine supervision were the available initiatives on improving VCT services among youth.
Conclusion: VCT services face ethical challenges which are either health facility-based, community-based or are at the national level. Addressing the ethical challenges is necessary in order to improve the uptake of VCT services and thus strengthen the fight against HIV/AIDS. Deployment of enough counselors, refresher training to counselors, and raising community awareness on HIV/AIDS and the negative impacts of stigma are among the initial strategies for remedying the situation.
Keywords: ethical challenges, voluntary, counseling, testing, HIV/AIDS, youth and HIV, Tanzania, commercial motorcyclists, shortage of counselors
Introduction
Voluntary Counselling and Testing (VCT) for HIV is the process by which an individual undergoes counseling that enable him or her to make an informed choice about being tested for HIV.1 VCT is the World Health Organization (WHO) recommended tool for HIV/AIDS prevention, care, and treatment.2 However, uptake of VCT has remained low globally, regardless of the campaigns on raising awareness on the importance of VCT.3 Globally more than 40% of people who are living with HIV/AIDS infections are unaware of their HIV/AIDS status.3 The low uptake of VCT hinders global attempts to prevent new HIV infections and limits scale-up of HIV care and treatment.4 Young people are the most vulnerable and most affected section of the global population.5 Worldwide, about 2,500 new infections occur daily among young people aged between 15 and 24 years.6 Specifically, studies have singled out youth commercial motorcyclists with higher prevalence of HIV than the general population, and low frequency of preventive behaviours, including and HIV testing.7 The group of youth commercial motorcyclists’ group is a contemporary vulnerable population and this might have been exacerbated partly by their age and occupation. The low uptake of VCT services at the global scale is attributed to the presence of wrong perceptions, long waiting time in VCT clinics, lack of privacy, and breaching of confidentiality among service providers.8 For instance, in Thailand, 34% of the clients reported breaching of confidentiality by the health workers.9
In sub-Saharan Africa, regardless of the high prevalence of HIV/AIDS infection in this region,10 only 10% of young men and 15% of young women know their HIV status.11 The low uptake of VCT services in Africa has been documented to be negative perception of being at risk of HIV infection, negative perceived benefits of VCT, the belief that knowledge of infection may accelerate disease progression, psychosocial factors including HIV/AIDS-related stigma, discrimination, and concerns about privacy and confidentiality.12
Tanzania, as for other countries in Sub-Saharan Africa, is not exceptional. In Tanzania, 65.8% of young male and 46.3% of young females aged 15–24 years are not aware of their HIV status.11 This happens, amidst the fact that about 90% of Tanzanians know where they can go to test for their HIV/AIDS.8 Fear of stigma and discrimination from relatives, friends, and communities, wrong perception on youth VCT uptake, lack of knowledge, mistrust of the counselors, long waiting time, and distance from the VCT clinics to residences are among the documented factors behind the low uptake of VCT services in Tanzania.11,13,14
Regardless of the factors documented to be responsible for low uptake of VCT services in Tanzania, there is a dearth of studies focusing on ethical challenges that hamper the VCT services uptake among youth commercial motorcyclists in Tanzania. In this context, ethical challenge refers to the situation whereby every alternative is morally wrong and still one has to make a choice.15 Therefore, this study set in to explore ethical challenges facing pre- and post-voluntary HIV/AIDS counseling and testing services among youth commercial motorcyclists in Tanzania by using a case of Kinondoni municipality in Dar es Salaam city.
Methods
Study Design
We adopted a qualitative exploratory case study that employed key Informants’ Interviews (KIIs), In-depth Interviews (IDIs), and Focus Group Discussions (FGDs) to explore ethical challenges facing voluntary HIV/AIDS counseling and testing services among youths engaged in commercial motorcycling. We bounded our case to ethical challenges surrounding VCT services among youth engaged in commercial motorcycling in Kinondoni municipality. A case study approach was appropriate for this study as ethical challenges involve interaction of complex social processes and a case study gives an opportunity to study them in a natural setting.16
Study Area
This study was conducted in Kinondoni municipality, the largest Municipal Council in Dar es Salaam city which comprises 327,704 youths.17 There are 2,137 VCT sites across the country,8 and most of the sites are in Dar-es-Salaam with Kinondoni municipality having the largest share.13
Data Collection
We adopted qualitative techniques using Key Informant Interviews (KIIs) (Appendix 1) Focused Group discussions (FGDs) and In-depth Interviews (IDIs) (Appendix 2) to carry out data collection. The KIIs, FGDs, and IDIs were all carried out in Kiswahili language in the working place of the study participants. The KIIs, FGDs, and IDIs were recorded using a digital audio recorder and field notes were taken by a research assistant.
Key Informant Interviews
We used a semi-structured Kiswahili interview guide to carry out three KIIs with all three counselors that were available at the facilities involved in this study. The three facilities were purposeful selected to include one dispensary, health center, and a hospital. For the case of hospitals where more than one counselor existed, a counselor with bias on youth services was purposively selected. Each KII lasted between 45 minutes and 1 hour. The aim of the KIIs was to get insights of the ethical challenges facing youth in accessing the VCT clinics services from the counselors’ perspectives.
Focus Group Discussion
We used a semi-structured Kiswahili focused group guide to conduct four focused FGDs with 24 youth aged between 18 and 24 years. The youths were purposeful selected among the commercial motorcyclists from four streets containing a large number of youth commercial motorcyclists’ parking lots and were within the catchment of the selected health facilities. From each street, all parking lots were identified and listed with the aid of the leader of the youth commercial motorcyclists in that street. One parking lot with the largest number of youth commercial motorcyclists was purposeful selected from each street. The FGD participants were identified with the aid of the leader of the selected parking lot from each street. The FGDs involved between five and eight youth commercial motorcyclists who had attended at least one health facility that has VCT services and they were aware of the VCT clinic but never went for the VCT services. In all selected parking lots, the number of youth commercial motorcyclists fitting our purpose for FGD selection did not exceed eight. Those who agreed to participate in the study identified a convenient time and place for the FGD. The youth commercial motorcyclists were comfortable to hold the discussions in a venue close to their parking lot. Time for each FGD ranged from 45–90 minutes. After attaining intra-group information saturation, we stopped the discussion.
In-Depth Interviews (IDIs)
Following the FGDs, participants who were found to have rich information concerning the ethical challenges facing youth in accessing the VCT clinics services were purposively recruited for IDIs. We used a Kiswahili semi-structured guide to carry in-depth interviews. After the eighth IDI, there was no new information coming regarding the ethical challenges facing youth in accessing VCT clinics services and therefore we stopped further interview. Each IDI lasted between 30 minutes and 1 hour.
Data Analysis Procedures
The audio-recorded interviews and FGDs were first transcribed verbatim and then translated from Kiswahili to English. The interviews and FGDs transcripts were analyzed using qualitative content analysis following Graneheim and Lundman.18 The qualitative content analysis offers development of categories from the text data inductively. The inductive derivation of categories is important in capturing the experiences of the participants.19
The full transcripts and field notes were first to read and re-read by the author in order to become familiarized with the data and the context. Condensed meaning units were then formed through data reduction. These were related to youth experiences on ethical challenges in VCT services uptake. The condensed meaning units were read and re-read in order to extract the codes. Primary codes were formulated and similar codes were grouped together and through constant comparison were abstracted into sub-categories. Prior to the formulation, all authors discussed and agreed on the revised and final codes. Sub-categories were further analyzed to distinguish their similarities and differences. Similar sub-categories were sorted to form categories that reflect the manifest content of the interviews.
Further, axial coding was carried out for comparisons between and within categories and sub-categories as well as between the counselors and youth motorcycle rider’s data. The entire analysis was then compared with the existing literature and the ideas in the field. This process provided the opportunity to compare and contrast categories and data sources based on how they explain the ethical challenges.
An independent sociologist with bias in social work who was not part of this study read and coded the data following the similar procedures and the interpretation was consistent to our interpretation.
Ethical Consideration
This study was conducted in accordance to the Declaration of Helsinki. Ethical clearance was obtained from the Research and Ethics Committee at Muhimbili University of Health and Allied Sciences. Permission to carry out the study was obtained from Dar es Salaam regional authorities, Kinondoni municipality authorities, Ward Executive Officers, Mtaa Executive Officers of the selected streets, heads of facilities involved, leaders of youth commercial motorcyclists, and the study participants. Written informed consent (Appendix 4) was obtained from each study participant before commencing the interview or discussion. The informed consent contained information on objectives of the study, what participation entails, benefit of participation, risks, privacy, confidentiality of their information, and who to contact for further information from the ethics committee. The participant-informed consent included consent for the publication of their comments.
Findings
We present findings from 35 respondents including three from KIIs, 24 participants from FGDs, and eight from the IDIs. From the analysis of the information gathered from three KIIs’ interview from VCT counselors, four FGDs and eight IDSs from youth commercial motorcyclists,’ three categories emerged as summarized in Table 1. The categories include; unfriendliness of VCT services to the youth, challenging working environment for the HIV/AIDS counselors, and available initiatives on improving VCT services among youth. These categories depict the ethical challenges surrounding the HIV/AIDS VCT services among youth commercial motorcyclists in Kinondoni municipality, Dar-es-Salaam.
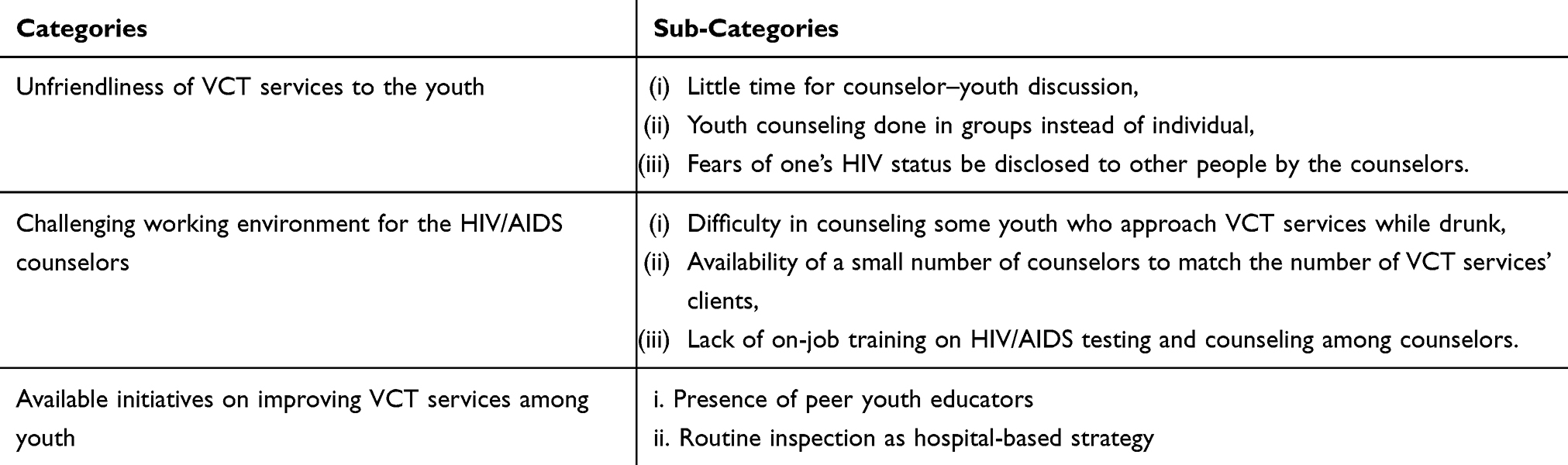 |
Table 1 Summary of the Emerged Ethical Challenges Facing Youth Commercial Motorcycle Riders in Accessing Voluntary HIV Counseling and Testing in Dar es Salaam |
Unfriendliness of VCT Services to the Youth
This emerged as a main category, including sub-categories which were; little time for counselor–youth discussion, youth counseling done in groups instead of individually, and fears of one’s HIV status being disclosed to other people by the counselors.
Little Time for Counselor–Youth Discussion
Participants of this study stated that lack of enough time for counselor–youth engagement limits the youth to express their worries and feelings to be counseled adequately. This was stated to leave the youth unsatisfied and thus those who had neverhad VCT were likely to hesitate in visiting clinics based on such background information. Across facilities, VCT clinics counselors reported little counselor–youth engagement time, which was partly due to the large number of VCT clients and a pressing shortage of counselors. Each VCT clinic where this study was carried out had only one trained counselor to attend all VCT clients including youth. It is worth noting that VCT services also cover most of the Outpatient Department (OPD) cases referred from different clinics within and sometimes outside the facility. Stressing on this matter, one informant said:
VCT counselors spend little time with their clients, they only ask them why they have decided to go for testing, nothing else. Generally, clients lack enough time to share their experience with counselors. (Youth IDI participant #8)
Youth Were Counseled in Groups Instead of Individual
During the data collection, it was revealed that in most of the instances, counseling is operationalized in groups in order to provide services to large numbers of people. The groups of counseling ranged from 3–20 youths, in which people all attended together in the same counseling room. From the FGDs, participants stated that the practice of group counseling in VCT services discouraged them from going to VCT clinics. Among youths, group counseling was reported to make them feel insecure and most of them felt that their freedom and privacy were compromised by this practice. The fear was worsened by the associated stigma and discrimination which the majority of the discussants mentioned to exist in the community to people living with HIV/AIDS. One participant, on focus group discussion, said that:
Counseling session has been done in groups in all counseling houses here. I do not prefer anybody to know my health status. Therefore, if they will change VCT system of group counseling I will go for HIV testing. (Youth FGD 1 participant #3)
Further, our KII respondents confirm that lack of privacy as stated by many youths was existing in their clinics partly due to the large number clients at VCT clinics waiting for services. The situation forced counselors to conduct counseling sessions in groups, which consequently created fear among youth.
Fear of HIV Status Disclosure to Other People by the Counselors
Participants portrayed mistrust of the youths to counselors. Participants expressed that some counselors have a tendency to disclose the clients’ information to either their co-workers, friends, or within the community. The youths reported to have heard this from friends and peers who had attended VCT clinics. This practice was reported to have created unpleasant feelings and anxiety towards attending VCT clinics due to the divulging of information accompanied by labeling of some members of community as HIV positive by some of the community members. Adding on this, one client, on focus group discussion, said:
You know sometimes you may find you need to go for HIV counseling and testing so as to know your HIV status. Once you are informed that there are some counselors with a tendency of disclosing client’s information to unauthorized persons. With this information you hesitate and change your mind and decided not to attend VCT clinic. (Youth FGD2 participant #3)
Respondents from this study stressed the tendency of being labeled by the community, indicating that gossiping about HIV/AIDS infected people by members of the community created mistrust in the counselors. The youths believe that the counselors have the primary obligation to maintain confidentiality of the information of their clients. Further, most of the youths who were also commercial motorcyclists reported to have feared their results to be known to others and, thus, being labeled as HIV positive and becoming discriminated against by their relatives, friends, family members, and sometimes the entire community. Notably, among youths, disclosure of HIV status is perceived as a barrier toward accessing marriage rights in the future. One informant argued as follows:
My fear is to be labeled as HIV positive. I know my relatives and friends will no longer love me. So, it is better to stay until it reaches to the disease stage before going for testing. If I am already infected, I will be having no any other option rather than going for care and treatment. (Youth IDI informant #3)
Challenging Working Environment for the HIV/AIDS Counselors
This was named as the second main category. Under this main category three sub-categories emerged including the following; difficulty in counseling some youth who approach VCT services while drunk, availability of a small number of counselors to match the number of VCT services’ clients, and lack of on-job training on HIV/AIDS testing and counseling among counselors.
Some Youth Approach VCT Services While Drunk
The study found that that some youth rejected their HIV/AIDS testing results or treatment after being diagnosed to be HIV positive. Evidence from Counselors shows that most of those who rejected results were youth who approached VCT clinics while drunk. Despite that situation, VCT counselors tried to cope with the situation and tested them. However, counselors find it difficult on post-testing counseling, especially when these clients were found to be HIV positive. The later were reported to decline the positive results of their HIV/AIDS testing and thus created chaos to the counselors. One counselor explained that:
Sometimes some youth come for counseling and testing while drunk … we cope and we test them … the challenge comes in giving their HIV results, especially when one is HIV positive, most of them have a tendency of rejecting their results. (KII from VCT counselor #1)
Our respondents reported that some youths were diagnosed to be HIV positive while their minds were not prepared to receive such results. Hence some of youths felt they were at risk of death or that the disease marks the end of life here on earth. Based on this fear, some youths were reported to refuse to start treatment. Stressing on this, one counselor said:
You know sometimes youths are coming here in VCT clinics for services but already having their pre-meditated unconfirmed HIV results. So, this wrong perception among the youth create chaos in provision of service because some of them think that being positive is an end of life and nothing can be done to rescue the situation. (KII from VCT Counselor #2)
Treatment services not being housed in the same building with VCT was also mentioned to contribute to some youths to refuse to be enrolled for antiretroviral treatment when diagnosed with HIV. Results from KIIs showed that this tendency was partly due to the fear of being seen by other community members while attending or testing for HIV in one building and later moving to another building known to offer Care and Treatment Clinic (CTC) services. One participant said:
We do not have a treatment service here, the treatment service is available at the next building, so sometimes youth rejects to go there for treatment in the other building … To shield this such youths will be asking to attend further clinic for testing and treatment. (KII from VCT counselor #1)
Availability of Small Number of Counselors to Match the Number of VCT Services’ Clients
The presence of few counselors in VCT clinics that did not match the number of clients in demand for services was reported to create congestion in VCT clinics. Sometimes counselors received a large number of clients while at the same time they were required to accomplish other assigned tasks to perform at the clinic. This situation confounds their performance of core responsibilities and sometimes makes the clients feel disrespected or not fairly treated due to the short time of consultation. Notably, an overwhelming number of clients lead to group counseling and shortening of the counseling time as a coping strategy to minimally attend the clients. On expressing this, one respondent said:
We are very few compared with the number of clients we are receiving per day. In our clinic we are receiving more than 30–50 clients instead of 15 clients per day. (KII from VCT Counselor #1)
Analysis of the response from the KII shows a lack of new recruitment of counselors from the government. In most of the clinics, VCT services were provided by only one professional counselor. The same was responsible of performing all tasks regarding VCT services.
“Initially we were three trained counselors employed here, but one has retired, and another was transferred to another center. I was left alone, so it is difficult for me to perform all responsibilities since there is no new counselor to assist me.“ (KII from VCT Counselor #2)
Lack of On-Job Training on HIV/AIDS Testing and Counseling Among Counselors
Inadequate continuing professional education opportunities among counselors was addressed as a challenge towards good provision of the VCT services. Our respondents recognize that counselor ongoing training skills help in solving most complex and difficult counseling scenarios and assisting clients with issues of disclosure, risk reduction, and avoiding violence. One of the three counselors participated in this study reported that, since she was employed as a counselor more than 5 years ago, she had never attended any formal on-job training and instead using their previously knowledge and work experience to share with others while the situation changes regularly. Notably, HIV/AIDS area is among areas which are changing rapidly with vast of new knowledge being generated.
Ongoing training is very important, sometimes we face dilemmas on making the right decision on disclosure and non-disclosure. For instance, counseling discordant couples poses particular difficulties for many counselors due to the concept being new and was not catered in our old training. (KII from VCT Counselor #3)
Available Initiatives on Improving VCT Services Among Youth
Findings from this study show that some VCT clinics have attempted to implement some measures towards improving of the services by addressing some key challenges. The study documented two sub-categories from this category including the presence of peer youth educators, and routine inspection as a hospital-based strategy.
Presence of Peer Youth Educators
The study revealed that a shortage of human resources has a negative influence on the uptake of VCT services. Across different facilities, study informants expressed on the shortage of human resources, with some of them pointing out in site coping solutions. Counselors reported that in some VCT centers offering free training to volunteer youth educators was found as a main strategy to curb the human resource for health shortage. Further, peer education created the credibility that young people have the power of becoming role models and provided flexibility in meeting the diverse needs of contemporary youths. Peer education was reported by the respondents for being able to support young people in developing positive group norms and in making healthy decisions about HIV/AIDS. Stressing on this, one of the respondents said:
We had trained peer youth educators so as to support us in offering health education to their peer youth. They are so helpful, and every Saturday we had a session of lessons in HIV and reproductive health. (KII from VCT counselor #3)
The results of this study indicated the dire need of bringing on board new counselors on a permanent basis to curbthe shortage of human resources in counseling. All counselors who participated in this study as KII aired their outcry to the government to recruit more counselors to reduce the burden of work as well as improving the quality of their work. Further, the counselor stressed on the need of counselors to be given space to perform their tasks based on their profession and not otherwise. One of the counselors said:
I think there is a need of a government to enroll more healthcare providers particularly for counseling. Whenever they are being employed, they have to perform their tasks basing on their profession. (KII from VCT Counselor #1)
Routine Supportive Supervision as Initiative on Improving VCT Services Among Youth
In running VCT clinic services frequent routine supportive supervision was vital in ensuring good offering of services to clients. However, informants reported that lack of frequent routine supportive supervision from the responsible authorities forced VCT clinics to practice a tendency of writing weekly progress reports within institutions as a coping mechanism. This tendency has contributed a lot in gaining new insights towards performing VCT tasks and solving most complex and difficult counselling scenarios like difficulties on disclosure or non-disclosure of the client HIV status. Emphasizing on this one respondent said:
In our VCT center here we have started a tendency of sending progress report to the authorities every Friday. So, if there are any complex and difficult counselling scenarios like on disclosure or non-disclosure of the client HIV status, we address it and we discussed together. (KII from VCT Counselor #1)
Further, the results of this study acknowledge the supportive supervision from the Ministry of health visiting and observing adherence of the HIV Testing and Counseling (HTC) guideline in offering services of counseling in VCTs. However, respondents of this study reported that sporadic single day monitoring per number of months is obviously not enough to extend the knowledge of the healthcare providers. This can hardly capture the actual situation when such practice is not frequent. The quote below supports this:
Yah sometimes they do monitor, but also it is very rare. In our clinic the last time to see people from ministry for monitoring it was on May. And whenever they came, they use very little time to share with us including imparting new skills and knowledge. (KII from VCT Counselor #2)
Discussion
This was an exploratory study aimed to explore ethical challenges facing VCT services among youth in Kinondoni municipality. From this study we found that ethical challenges were nested within a broad range of challenges revealed as unfriendliness of VCT services to the youth and challenging working environment for the HIV/AIDS counselors. To address these challenges, the health facilities were using peer youth educators and routine inspection as the health facilities strategies.
Unfriendliness of VCT Services to the Youth
Unfriendliness of VCT services to the youth, which was expressed in different sub-categories including little time for counselor–youth discussion, youth counseling done in groups instead of individually, and worries of one’s HIV status being disclosed to other people by the counselors; depicts the existence of major ethical challenges on VCT services provision and access among youth. The unfriendliness of VCT services to the youth is contrary to the National HIV policy,20 which requires the services to be user friendly for increased access and utilization.
Inadequate time for counselors to share experience with youth contributes to low youth attendance to VCT clinics. As revealed by this study, the shortage of counselors in a large number of VCT services partly contributes to this situation. Similar findings have been documented by Biadglegne et al21 in Ethiopia. In this study, physical facility and VCT procedures in which many of the VCT centers were below satisfactory due to the large number of people at the VCT clinics, hence counselors lack enough time to share experience with their clients. Anita22 documented that enough time is needed especially in pre-test counseling because of the stigma and discrimination related to HIV. Clients needed to be aware of these risks and be ready to confront them. The findings of our study contravene the HTC guideline of Tanzania in 2013, which stipulates that the existence of dialog in VCT helps persons to understand and make informed decisions about HTC and helps the client to understand the results of their HIV test, which is essential for their future planning.20
Group counseling sessions in VCT clinics, as revealed in this study, compromise the ethical principle of ensuring privacy to the client.20 This finding corroborates with the idea of Patrice,23 who stated that lack of privacy during the counseling sessions due to inadequate and limited space to be a disappointment to clients attending VCT clinics. Macharia9 documented a tendency of group counseling session leads to many clients not to attend VCT services. Group counseling as revealed by our study is discouraged by the World Health Organization through its guideline for HTC in 2016, that requires counseling to be done to an individual to enable clients to have sufficient time to comprehend information regarding pre-test and post-test counseling in VCT while ensuring their privacy.3 Group counseling might have made youths feelunsecure, as there is no freedom and privacy amidst community where stigma is prevalent. Fear was worsened by the associated stigma and discrimination from friends, relative, and others who might have been or have some connections to the present audience in the counseled group.
Fear of HIV status disclosure to other people rose as an ethical challenge in VCT services. Respect for confidentiality is important to safeguard the well-being of clients and hence ensuring the confidence vested upon them by the society.24 Worries of one’s status to be disclosed to other people by counselors have been documented by Macharia.9 In Thailand, 34% of the clients have raised concerns on breaching of confidentiality by healthcare workers.1 The findings of the current study are consistent with those of Angotti et al,25 which reported that clients did not trust some counselors as they spread information on positive test results to other people, hence clients prefer counselors who do not know them. The findings of this study contradict the HTC guidelines in Tanzania, which requires that the discussion between the client and the HTC provider be confidential unless the client explicitly gives consent to share this information. As such this presents unethical practices once others need to know the client HIV status without consent from the clients.
Challenging Working Environment for the HIV/AIDS Counselors
A trend of some youth to attend VCT clinics while drunk as reported by counselors in this study creates chaos for the counselor on effective provision of VCT services. Notably, clients have a tendency of rejecting their results when diagnosed as HIV positive. The finding of this study is contrary to HTC guidelines of Tanzania 2013 which requires counselors to adhere to standard operating procedures and quality control measures for testing to ensure the provision of correct test results to all clients.20 The control of quality is a dichotomy; it needs both the counselors and clients to be sober. As demonstrated by this, a prepared mind to accept the unpredictable results is needed and this is not guaranteed when one is drunk. Hence this has sometimes been reported to be accompanied with rejection of positive results and thus creates chaos for counselors on enrolling such clients for further treatment services. The tendency of going to the VCT while drunk can be explained by the frustration of youths, who might be at a certain time having affairs with a person suspected or with HIV infection or linked with a chain of infection from a certain HIV positive person. This causes most of the young people to project their results and sometimes thinking alcohol might be a proper solution to calm down their feelings.
The shortage of human resources for health causes congestion in VCT clinics and thus leads to counselors having a short time with clients. This study found that, regardless of the large number of VCT clients, each health facility had only one trained counselor. Nathaniel26 addressed that the critical shortage of trained health workforce in Tanzania is a major challenge facing the health sector and is aggravated by low motivation and maldistribution of the few available staff. This finding is also in line with Kisa,13 who documented that poor working condition among healthcare providers contributes to poor provision of services in VCT clinics and sometimes make the clients feel disrespected or not fairly treated. The use of group counseling might therefore be explained by the fact that any health worker would like to provide services at least to those who attended the facility, hence grouping people in counseling can be viewed as an on-site coping mechanism to serve large numbers of clients in VCTs.
Lack of continuing professional education among counselors was found to threaten the performance of counselors. As revealed by this study all three counselors reported to have received very little or not at all formal on-job training since they have been employed. This jeopardizes their work performance in offering services, especially on solving most complex and difficult counseling scenarios. The need for on-job training is emphasized by Mataboge et al,27 who revealed that healthcare workers face the risk of HIV infection in both their personal and professional lives so training to the health worker remains an important component of empowering healthcare workers about the risks of contracting HIV and the need for the uptake of HCT in order to remain healthy. Again, this finding contradicts the WHO HTC guideline of 2016 which entails basic training and additional technical training as essential for all HIV testing and counseling staff.3 This situation is partly explained by the shortage of health workers, where sending a counselor to the training would mean closing down the facility during her/his absence. Further, the competing demands in health service provision coupled with scarce resources might lead to some of the activities or cadres being left out during the annual or routine continuing professional education.
Available Initiatives on Improving VCT Services Among Youth
The presence of volunteer peer youth educators in many VCT clinics as an initiative strategy has increased the credibility and flexibility in meeting the diverse needs of contemporary youth. The findings of the current study are consistent with Svenson,28 who stated that peer education was a popular and versatile approach for promoting reproductive health and HIV prevention among young people around the world. The same study further recommended that well-designed and well-implemented programs can improve young people’s health-related knowledge, attitudes, and skills and their access to health services. Medley et al29 documented that peer education programs intervention in developing countries are moderately effective at improving of behavioral outcomes, but show no important impact on biological outcomes.
Routine supervision is pointed to as among the strategies of improving VCT services among youth. These findings are consistent with what Rond30 Our findings complement what Charlotta31 explained that external inspectorate work to customize the strategy and practice to support improvement and lasting changes in healthcare services. External supervision is above all about controlling the services, but the control can be practiced in a way that will support the internal improvement work. In VCT clinics, this is important in helping counselors in gaining new insights toward performing VCT tasks and solving most complex dilemmas and difficulties in counselling scenarios. In Tanzania, supportive supervision is one of the core instruments in monitoring and improving service provision in particulars across different service provision levels.
Trustworthiness
The trustworthiness of this study is based on credibility, transferability, dependability, and conformability of the study findings. Credibility is defined as the confidence that can be placed in the truth of the research findings.32 By selecting suitable participants, introducing them to the aim of the study and asking participants permission to participate so as to ensure the credibility of the findings. In addition, the interviews were recorded and notes were taken to ensure that information provided is not missed. In ensuring transferability, the researcher is providing a “thick description” of the study setting and the way purposeful sampling is done. To ensure dependability, the research design was viewed as a prototype model, and what was planned is what was executed. Conformability establishes that data and interpretations of the findings are not fabrications of the researcher’s imagination, but they are from data.33 To achieve conformability, the study uses direct quotes and ensures that findings are abstracted from experiences and ideas of the participants and not the characteristics and preferences of the researcher.
Conclusion
During the exploration of ethical challenges facing voluntary HIV/AIDS counseling and testing services, three categories emerged. From this study, we found that ethical challenges were nested within a broad range of challenges, revealed as unfriendliness of VCT services to the youth and challenging working environment for the HIV/AIDS counselors. The first major category was the unfriendliness of VCT services to youth, and included little time for counselor–youth discussion, youth counseling done in groups instead of individuals, worries of one’s HIV status being disclosed to other people by the counselors, and the second main category being difficult in counseling some youth who approach VCT services while drunk, availability of small number of counselors to match the number of VCT services’ clients and lack of on-job training on HIV/AIDS testing and counseling among counselors. Although findings of this study could not be generalized to other VCT clinics services but this study raise important lesson that while designing VCT clinic services considerations on the voices of the youth commercial motorcyclists on challenges facing them from accessing VCT clinic services should not be undermined. This study reveals that fact, addressing the ethical challenges need to be inclusive including service users, providers, and policymakers to ensure comprehensive solution which will address challenges in a collective manner. The use of local formal and informal structures could play a central role in service improvement.
This study provides pertinent evidence to contemporary sub-Saharan economic transformation epoch where youths are at the heart of transporting people, goods, and services, and thus forming an inimitable emerging occupation exposed to serious health risks. Notably, most young people are a dominant group which is at high risk of succumbing to HIV infection, and thus addressing counseling challenges from the supply and demand side is crucial for improving service accessibility.
Given the economic contemporary transformation in sub-Saharan Africa where youth commercial motorcycle riders play a key role, this study provided evidence that voluntary HIV counseling is hampered by challenges, hence apt interest is desirable to shield youth commercial motorcyclists who are key in spreading of the pandemic. Notably, ethical challenges stand as key non-medical expectation which may avert access to counseling services and thus derail efforts to control the impetus of the pandemic. Further studies are warranted on how best ethics can be maintained given prevailing external constraints dearth.
Disclosure
The authors declare no conflict of interest.
References
1. UNAIDS report on the global AIDS epidemic. Global Report. 2013.
2. WHO. Statement on HIV testing and counseling: WHO, UNAIDS re-affirm opposition to mandatory HIV testing. Health (San Francisco). 2012;2012–2014.
3. WHO. The World Health Organization. HIV Testing Services. 2016.
4. AVERT. Global HIV and AIDS statistics. Averting HIV AIDS. 2015;1.
5. National Bureau of Statistics (NBS). Tanzania HIV/AIDS and Malaria Indicator Survey (THMIS). 2013:95–100
6. UNAIDS. Young people and HIV/AIDS. Opportunity Crisis. 2015.
7. Lindan CP, Anglemyer A, Hladik W, et al. High-risk motorcycle taxi drivers in the HIV/AIDS era: a respondent-driven sampling survey in Kampala, Uganda. Int J STD AIDS. 2015;26:336–345. doi:10.1177/0956462414538006
8. AVERT. HIV and AIDS in Tanzania. 2016.
9. Macharia MP Barriers to HIV Testing and Counseling uptake among young people aged 18–24 years in Nyeri Municipality. 2013.
10. AVERT. HIV and AIDS in sub-Saharan Africa regional overview. 2013.
11. Sanga Z, Kapanda G, Msuya S, Mwangi R. Factors influencing the uptake of Voluntary HIV Counseling and Testing among secondary school students in Arusha City, Tanzania: a cross sectional study. BMC Public Health. 2015;vol. 15:452. doi:10.1186/s12889-015-1771-9
12. Meiberg AE, Bos AER, Onya HE, Schaalma HP. Fear of stigmatization as barrier to voluntary HIV counseling and testing in South Africa. 2008;5:49–54.
13. Mwakatobe KB Use of HIV/AIDS Counseling and Testing Services Among Young People in Tanzania: a Case Study of Kinondoni District. 2007.
14. Meremo A, Mboya B, Ngilangwa D, et al. Barriers to accessibility and utilization of HIV testing and counseling services in Tanzania: experience from Angaza Zaidi programme. Pan Afr Med J. 2016;23:1–12. doi:10.11604/pamj.2016.23.189.5683
15. Ulrich CM, Taylor C, Soeken K, et al. Everyday ethics: ethical issues and stress in nursing practice. J Adv Nurs. 2010;66:2510–2519. doi:10.1111/j.1365-2648.2010.05425.x
16. Creswell JW. Research Design: Qualitative, Quantitative and Mixed Approaches (3rd Edition). Research Design: Qualitative, Quantitative, and Mixed Methods Approaches; 2009. doi:10.2307/1523157.
17. National Bureau of Statistics. The United Republic of Tanzania population distribution by age and sex. 2013:173–175.
18. Graneheim U, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ. Today. 2004;24:105–112. doi:10.1016/j.nedt.2003.10.001
19. Kohlbacher F. The use of qualitative content analysis in case study research. Forum Qual. Soc. Res. 2006;7(Art):21.
20. Welfare M. NACP: National Comprehensive Guidelines for HIV Testing and Counseling in Tanzania. 2013.
21. Biadglegne F, et al. Voluntary HIV counseling and testing service in Northwest Ethiopia: the cases of counselor’s perception, client’s satisfaction, and in-service observations. Ethiopian Medical Journal. 2011;49:169–177.
22. Hardon A, Kageha E, Kinsman J, et al. Dynamics of care, situations of choice: HIV tests in times of ART. Medical Anthropology. 2011;vol. 30:183–201. doi:10.1080/01459740.2011.552455
23. Ngangue P, Gagnon M, Bedard E. Challenges in the Delivery of Public HIV Testing and Counselling (HTC) in Douala, Cameroon: providers perspectives and implications on quality of HTC services. BMC Int Health Human Rights. 2017;vol. 17:1–9. doi:10.1186/s12914-017-0118-2
24. TACAIDS. The Tanzania Commission for AIDS.National HIV and AIDS Response Report. 20–24 2014.
25. Angotti NI, Bula A, Gaydosh L, Kimchi EZ. Increasing the acceptability of HIV counseling and testing with three C’s convenience, confidentiality and credibility. 2009.
26. Sirili N, Kiwara A, Nyongole O, et al. Addressing the human resource for health crisis in Tanzania: the lost in transition syndrome. Tanzan J Health Res. 2014;16:1–9. doi:10.4314/thrb.v16i2.6
27. Mataboge MS, Peu MD, Chinuoya M, et al. Healthcare workers’ experiences of HIV testing in Tshwane, South Africa. Curationis. 2014;vol. 37:E1–8. doi:10.4102/curationis.v37i1.1170
28. Family Health International. Evidence-Based Guidelines for Youth Peer Education. 2010.
29. Medley A, Kennedy C, O’Reilly K, Sweat M. Effectiveness of peer education interventions for HIV prevention in developing countries: a systematic review and meta-analysis. AIDS Educ Prev. 2014;vol. 21:181–206. doi:10.1521/aeap.2009.21.3.181
30. R G. Tools and strategies for quality improvement and patient safety - Patient safety and quality. 2008.
31. Schaefer C, Wiig S. Strategy and practise of external inspection in healthcare services – a Norwegian comparative case study. Saf Health. 2017;vol. 3:3. doi:10.1186/s40886-017-0054-9
32. Anney VN, Dar POB, Salaam E. Ensuring the quality of the findings of qualitative research: looking at trustworthiness criteria. J Emerg Trends Educ Res Policy Stud. 2014;5:276–279.
33. Tobin G, Begley C, Tobin GA, Begley CM. Methodological rigor within a qualitative framework Methodological rigour within a qualitative framework. J Adv Nurs. 2004;48:388–396. doi:10.1111/j.1365-2648.2004.03207.x
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.