")
Back to Journals » International Journal of General Medicine » Volume 13
Vocal Feminization for Transgender Women: Current Strategies and Patient Perspectives
Authors Kim HT
Received 7 August 2019
Accepted for publication 30 January 2020
Published 12 February 2020 Volume 2020:13 Pages 43—52
DOI https://doi.org/10.2147/IJGM.S205102
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Hyung-Tae Kim
Yeson Voice Center, Institute of Performing Art Medicine, Seoul, South Korea
Correspondence: Hyung-Tae Kim
874 Eonjuro, Gangnamgu, Seoul 06017, South Korea
Tel +82 2 3444 0550
Fax +82 2 3443 2621
Email [email protected]
Abstract: Voice feminization for transgender women is a highly complicated comprehensive transition process. Voice feminization has been thought to be equal to pitch elevation. Thus, many surgical procedures have only focused on pitch raising for voice feminization. However, voice feminization should not only consider voice pitch but also consider gender differences in physical, neurophysiological, and acoustical characteristics of voice. That is why voice therapy has been the preferred choice for the feminization of the voice. Considering gender difference of phonatory system, the method for voice feminization consists of changing the following four critical elements: fundamental frequency, resonance frequency related to vocal tract volume and length, formant tuning, and phonatory pattern. Voice feminizing process can be generally divided into non-surgical feminization and surgical feminization. As a non-surgical procedure, feminization voice therapy consists of increasing fundamental frequency, improving oral and pharyngeal resonance, and behavioral therapy. Surgical feminization usually can be achieved by external approach or endoscopic approach. Based on three factors (length, tension and mass) of vocal fold for pitch modulation, surgical procedure can be classified as one-factor, two-factors and three-factors modification of vocal folds. Recent systematic reviews and meta-analysis studies have reported positive outcomes for both the voice therapy and voice feminization surgery. The benefits of voice therapy, as it is highly satisfactory, mostly increase vocal pitch, and are noninvasive. However, the surgical voice feminization of three-factors modification of vocal folds is also highly competent and provides a maximum absolute increase in vocal pitch. Voice feminization is a long transition journey for physical, neurophysiological, and psychosomatic changes that convert a male phonatory system to a female phonatory system. Therefore, strategies for voice feminization should be individualized according to the individual’s physical condition, the desired change in voice pitch, economic conditions, and social roles.
Keywords: pitch raising surgery, voice feminization, vocal folds, voice therapy, formant tuning, retraining phonatory pattern
Introduction
Voice feminization has appeared from the 16th century from the castrati in Italian opera. At that time, women were not allowed to sing in churches. Thus, castrati singers made their first appearance in the Sistine Chapel in 1562 and covered the high register of singing.1 Castrato’s voice characteristics are strictly the consequence of hormonal castration. He kept child’s voice and child’s high-pitched harmonics with a component. That might be the first voice feminization surgery.1 Under such factual background, voice feminization surgery has been recently performed for various voice disorders such as androgenital syndrome, ovarian tumor-producing male hormone, testicular feminization, aplastic anemia patients who have been treated by androgen hormone, and transgender women.
Kitajima reported an initial surgical study for experimental vocal pitch increase in 1979.2 After addressing the understanding of laryngeal physiology about pitch modulation, surgical methods to increase vocal fold tension including cricothyroid approximation (CTA)3 and anterior commissure advancement (ACA)4,5 have been described. However, evidence of the efficacy of such procedure is limited and peer-reviewed publications are mostly limited to a few case reports.3–5 Two studies that did systematically examine separate cohorts of 14 male to female (MTF) transsexuals who underwent surgery for androphonia were those reported by Brown et al regarding CTA6 and Wagner et al who assessed ACA, CTA, or both.7 Alteration of vocal fold mass can be accomplished by scarification of vocal folds,3 steroid injection of vocal folds,3 or reduction of vocal fold mass by CO2 laser vaporization.8,9 Vaporization of discrete portions of vocal folds with CO2 laser can also significantly raise vocal pitch, as demonstrated in dogs by Tanabe et al.8 It appears that decrease in mass and increase in stiffness resulting from the scarring process of vocal fold tissue account for significant rise in vocal pitch. Donald has described a technique in which both length and mass of vocal folds are surgically altered by removing an anterior portion of vocal folds and creating an anterior web.10 After that, various modified procedures for raising the pitch of voice with anterior web creation11 or reducing the size of vocal folds and thyroid cartilage12 have been reported. However, when improvements provided by the various procedures are insufficient, postoperative results will show an unnatural voice with decrease of vocal quality, loudness, and vocal range.13
For a long time, it has been accepted that the following three fundamental principles are essential preconditions for raising of the pitch; tension increase, mass thinning, and shortening of the length of vocal folds.2,3 However, pitch is a functional acoustic result not only coming from vocal fold tension, mass, and length but also coming from subglottic pressure and resultant change in pharyngeal dimensions for modifying resonance.14 Most importantly, although phonation is under voluntary control, exceedingly complex activities necessary to produce a smooth, clear voice are under phonatory feedback reflex control.15 Voice feminization should consider these three fundamental principles as well as phonatory feedback reflex control and phonatory pattern change for feminine resonance generation. Therefore, considering the neurophysiological complexity of voice feminization, voice therapy has more advantages than starting surgical treatment with the first line.
The ideal voice feminization process may lead to complete female phonatory morphometric changes. For voice feminization, it is necessary to precisely conduct the process of modification of structural and morphometrical male phonatory organs into female’s one. Understanding the morphometric difference of phonatory organ between males and females is a crucial process for developing strategies to feminize voice.
Morphometric Differences of the Laryngeal Framework and Vocal Tract Configuration Between Males and Females
Generally, transgender women have grown their phonatory organ significantly after puberty. Such growth impacts on gender difference of voice pitch and quality. During puberty in males, the laryngeal framework, including vocal folds, considerably grows and downward located. It is associated with vocal tract elongation and vocal tract volumetric expansion.16,17 Studies on morphometric data of the human larynx in the literature have shown no sexual dimorphism of the larynx during childhood.18–20 Although sex differences of the larynx are not prominent in infancy, they can have significant morphometric changes of the larynx due to testosterone at puberty in males.21
When measurement data of vocal folds length were averaged from four studies, the length of vocal folds had an average of 22.79 ± 3.27 mm in males and an average of 18.99 ± 1.82 mm in females.20,22–24 Membranous vocal folds had an average length of 14.97 ± 2.01 mm in males and 11.17 ± 0.68 mm in females. Thus, membranous vocal folds length of males was about 25% longer than that of females.20 Other studies also showed a similar proportion of membranous vocal folds difference.25 Therefore, vocal fold should be shortened 25% more of its original length while remaining a minimal of 11 mm for female sized membranous vocal folds when considering voice feminization. Vocal thickness also has a morphometric difference between males and females. The thickness of vocal folds is 6.07 ± 1.11 mm in males and 5.03 ± 1.10 mm in females.20 The width of vocal folds shows about 20% difference between genders. Thus, the length of vocal folds should be shortened over 25% in membranous portion, and thickness should be thinned over 20% in width during voice feminization surgery if the transgender women have a male fundamental frequency.
In the vocal tract dimension, the oral cavity seems to grow in both length and volumetric size. However, the pharyngeal cavity only has significant volumetric increases in adolescents. This indicates that males have considerable longer oral length and more substantial volume than females. Moreover, the pharyngeal volume, but not length, has a considerable gender difference. It can be seen that female resonance is more affected by volume than by length of the pharynx.16
Tongue motion affects the modification of oral cavity length and volume. It also affects hyoid elevation. Readaptation of tongue motion or articulation pattern is one of the critical factors for modulating vocal tract configuration.26,27 Thus, the focus should be on not only laryngeal elevation for decreasing vocal tract length but also on vocal tract narrowing for reducing vocal tract volume within the range of gender difference. As a result, in feminizing strategies, it is necessary to modify vocal folds (fundamental frequency) and vocal tract (resonance frequency) including oral cavity both simultaneously to achieve an acoustic change of gender characteristics.
Strategies for Modification of Fundamental Frequency
Human voices of different people are composed of many frequencies with a sophisticated tone. The acoustic signal produced during speaking must contain at least two independently variable parameters, of which one provides information about pitch and the other provide information about the phonemic content that is characterized by resonance (vocal tract) and articulation (oral cavity).28 A listener’s perception of a speaker’s pitch depends mostly on the fundamental frequency in the speaker’s voice. The fundamental frequency of man is about an octave more in-depth than that of a woman. Feminine voice production requires modification of simultaneous and hierarchic sequential coordination of respiration, vibration, resonation, and articulation. Moreover, to get clear voice quality, these complex activities should be controlled by appropriate feedback reflex mechanism.29 Therefore, the strategy of voice feminization to overcome gender differences in fundamental frequencies should aim the following two factors of voice simultaneously: pitch in phonation and phonemes in articulation.
Until now, voice therapy and surgical procedures have been developed for raising the pitch to increase the fundamental frequency and feminity of the voice. The principle of surgical procedures for raising pitch has to meet requirements of the following three fundamental principles: tension increase, mass thinning, and shortening of the length of vocal folds.2,10,11,30 Morphometrically, vocal folds should be changed to be shorter, thinner, and tighter to raise the pitch. Under this concept, voice feminization surgery has been introduced in the direction of altering the laryngeal framework with vocal folds modification. Pitch raising surgery can be divided physiologically into three basic categories; one-factor, two-factor, and three-factor modifications of fundamental principles.
One-Factor Modification Surgery of Three Fundamental Principles
Modification of Tension of Vocal Folds
Kitajima and colleagues performed the first experimental study for pitch-raising procedure in 1979.2 They analyzed the relationship between voice pitch and cricothyroid distance and reported experimental surgical approximation of anterior cricothyroid distance. They found that voice pitch had a linear relationship with cricothyroid distance. After addressing the understanding of pitch modulation, surgical methods to increase vocal folds tension, including cricothyroid approximation (CTA), have been described.3 CTA was the most popular pitch-raising surgery in past decades. This procedure approximates the anterior portion of the cricoid and thyroid cartilages together by permanent threads. Therefore, the cricothyroid distance decreases and tension of vocal folds increases, thus increasing the pitch. However, CTA might not show satisfied long-term results.31,32
One report described that only 50% of patients were satisfied, and only 31% had a passable voice after surgery.32 Thyroid cartilage of younger patients has not formed a solid concrete framework to prevent postoperative deformity because ossification has not yet occurred. Therefore, surgery is not recommended for young persons under 30 years old. Another criticized factor is CT muscle which is the most important muscle in the control of voice register. CTA can compromise this muscle activity and significantly reduce pitch range, thus inducing unnatural falsetto sound.
Another tension modification surgery besides of CTA is anterior commissure advancement (ACA).4,5 This tension modification surgery was introduced to adjust vocal fold tension, not for transgender women. It was designed only to tighten flaccid vocal folds such as presbylaryngis. The thyroid cartilage portion attached to anterior commissure is wedged and advanced. It is secured in place with tantalum splint. However, postoperative pitch raise is not enough to apply it to transgender women. To intensify pitch increase, Wagner and colleague have tried combined surgery of CTA plus ACA. However, pitch increase after such combined surgery was also limited.7
Modification of Length of Vocal Folds
The first attempt to modify the length of vocal folds to increase fundamental frequency was made by Donald (1982) who introduced a new surgical technique with anterior web creation by endolarynx opening using an external approach for three cases.10 In 1989, Wendler presented the endoscopic technique of Donald’s surgical procedure in an unpublished presentation. Wendler’s method was performed under a rigid laryngoscope and general anesthesia. It consisted of the de-epithelialization of anterior one-third of vocal folds, which was sutured at the level of de-epithelialization area with thread and glue to create anterior glottic web.33
Gross (1999) reported a similar modification method using muscle suture to approximate the anterior glottic portion rather than using glue.11 After the primary form of endoscopic procedure for anterior glottic web formation was established, a similar modified surgery was reported. Some authors have used CO2 laser to vaporize vocal fold anterior portion and suture muscle with absorbable vicryl,34 or using no sutures combined with Radiesse voice gel.35 Radiesse was injected into the anterior one-third of vocal folds to tight contact of the de-epithelialized surface without muscle suture.35 The weak point of this type of surgery was that anterior glottic web formation was unable to modify thickness although it could modify the length of vocal folds. Suturing vocal folds with absorbable suture or intensification of attachment by Radiesse was insufficient to maintain tight shortening of vocal fold muscle. It only could decrease mucosal vibrating length of vocal fold. It could not shorten muscle length of vocal folds. Generally, muscle repair mechanism requires 3 to 6 months of remodeling phase.36,37 Moreover, the wound healing process of the cover portion of vocal folds takes 8 weeks for rearranging and organization of epithelium and basement membrane zone.38 Therefore, considering muscle remodeling and wound healing process, suturing vocal fold muscle with absorbable sutures that are absorbed within 3 or 4 weeks does not produce shortening of the muscle while intensifying scar formation. If the attached point of anterior vocal folds is unable to adhere tightly until complete healing, severe scarred tissue would be formed because this contact area is a very fast-moving part and is the area where tension is concentrated. Incomplete glottic closure will be inevitable. As a result, in some patients who do not follow postoperative instruction or who have to use their voice in the early state, breathiness and weakness of postoperative voice may have appeared.
Modification of Density of Vocal Folds
Initially, alteration of vocal folds mass or density was accomplished by scarification of vocal folds, steroid injection of vocal folds, or reduction of vocal fold mass by CO2 laser vaporization.3,8,9 Tanabe reported the first surgical experimental trial in 1985.8 Vocal folds were cut profoundly and longitudinally. Moreover, triamcinolone was injected into vocal fold muscle. Results of this method were not satisfying and voice quality was pathologic.11
Clinical report of modification of the density of vocal folds was described by Orloff in 2006. The method was called laser-assisted voice adjustment (LAVA).9 In LAVA, the membrane of vocal folds not including vocalis muscle was vaporized by using a CO2 laser to increase the stiffness of the vibrating membrane and to raise the fundamental frequency. Pitch increase averaging 26 Hz was not enough to get a female voice pitch range. Based on LAVA, a modification of the LAVA technique was introduced in 2009. It was called laser reduction glottoplasty (LRG).39 In LRG, the epithelium and vocalis muscle were vaporized by using a CO2 laser and the ablation of vocal folds muscle extended to the anterior point of the vocalis muscle. This surgical procedure was firstly performed for CTA failure cases and has developed as a combined pitch-raising surgery with CTA simultaneously as two-factor (tension and density) modification surgery.
Two-Factor Modification Surgery of Three Fundamental Principles
Modification of Tension and Density of Vocal Folds
In short and long-term results, one-factor modification surgery has not shown attractive outcome as it only induces limited pitch increase. Therefore, some doctors have been performing combined operations that can modify two-factor of fundamental principles to achieve higher pitch increase. Koçak and colleague have performed laser reduction glottoplasty (LRG) for treating cases with unsatisfied outcome after CTA surgery.39 They changed two factors such as tension and density and reported a mean postoperative pitch increase of 45 Hz.39
Modification of Tension and Length of Vocal Folds
Clinically, CTA and Wendler’s glottoplasty have been performed simultaneously by some doctors. This combined surgical method is sometimes referred to as “double surgery” or “ triple surgery”, including thyroid cartilage reduction (Adam’s apple shaving) among patients. This surgical outcome has not been verified yet because results have not been published. However, physiologically, this combined surgery might be an unnecessary procedure for pitch raising as this procedure can compromise cricothyroid (CT) muscle function known to adjust and control the voice register and interfere with feedback control system of thyroarytenoid (TA) muscle simultaneously. In the late period, the pitch goes down, and hoarse and rough voice might be developed due to loss of significant function to control the clarity of sound caused by disruption of feedback adjustment of CT and TA muscles.
Modification of Length and Density of Vocal Folds
Theoretically, two-factor modification surgery can be conducted by Wendler glottoplasty plus LAVA or LRG simultaneously under one endoscopic field of view. Pitch improvement of this type of two-factor modification surgeries was limited to be about 32 Hz of increase in fundamental frequency.40
Three-Factor Modification Surgery of Three Fundamental Principles
External Approach
An ideal surgical method needs to satisfy all three fundamental principles, not just one or two principles. Kunachak (2000) has reported an external approach to modify three factors, including the laryngeal framework. It can reduce the size of vocal folds and thyroid cartilage. In that approach, the anterior column of the thyroid cartilage and anterior vocal fold are removed with an external approach, thus reducing the larynx as well as shortening and tensioning the vocal folds to raise the pitch.12 This procedure can improve the external shape of the larynx and the pitch. Although this surgical procedure is ideal, it is highly aggressive. In addition, it results in an unnaturally high postoperative pitch increase up to 320 Hz. This surgical procedure compromises the laryngeal feedback reflex system of vocal fold due to cutting of the vocal fold muscle. It also increases the chance of muscle tension discrepancy and asymmetry of vocal folds that can induce diplophonia and dysphonia.
Thomas and colleagues have reported the modification surgery of thyroid cartilage and vocal folds reduction called feminization laryngoplasty, including thyrohyoid approximation.41 They tried to modify the pharyngeal length by thyrohyoid approximation to alter the resonant frequency.41 However, it is difficult to assume that thyrohyoid approximation can increase the resonant frequency because the volume of the oral and pharyngeal cavity mostly affected by tongue and hyoid motion has more influence on resonant frequency.42 On the contrary, it may have some hyperfunctional effects on the extralaryngeal muscle seen in patients with muscle tension dysphonia.
Endoscopic Approach
As another three-factor modification surgery with endoscopic approach, Kim has introduced vocal fold shortening with retrodisplacement of the anterior commissure (VFSRAC).29 This procedure seems to be similar to the anterior glottic web creation or Wendler glottoplasty. However, compared to other one-factor modification endoscopic surgeries, VFSRAC makes significant different physiological changes. It could modify all three factors (tension, length, and mass) of vocal folds by using permanent suture material and suturing of thyroarytenoid muscle to internal perichondrium of subglottic portion of the thyroid cartilage. Vocal folds can be changed to be shorter, thinner, and tighter by single surgical procedure (Figures 1 and 2).29 In the endoscopic surgical field, VFSRAC can accomplish three-factor modification of vocal folds. Although it provides a normal physiological change, the increase in the pitch is limited to 50.8 Hz above 50 years old, resulting in a lower pitch increase than the mean of 76.6 Hz patients for the entire TG group.
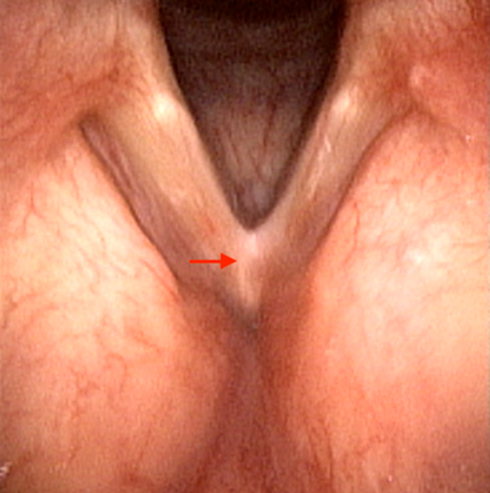 |
Figure 1 Postoperative finding of Wendler glottoplasty. Arrow indicates glottic web. |
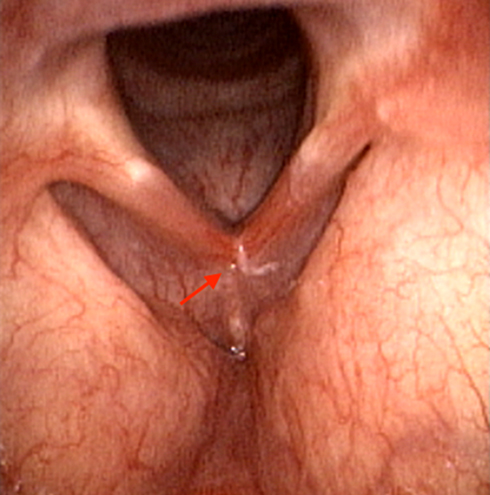 |
Figure 2 Postoperative finding of VFSRAC as a revision surgery of Wendler glottoplasty in the same patient. Arrow indicates a new anterior commissure. |
Generally, thyroid cartilage is calcified by 1.5% and 4% with each year increase in age from birth to 50 years.43 Moreover, significant myopathic changes can develop in the thyroarytenoid muscle with age. They may cause impairment of phonatory function.44,45 Based on physiological condition of aging, external approach of the thyroid and vocal fold reduction might have more beneficial effects on patients aged more than 50 years for pitch raising than endoscopic approach. However, in patients younger than 40 years, choosing less destructive and conservative surgical procedures may help feminize the voice.
Postoperative Outcome After Surgical Procedure
From surgeon’s point of views, we speculate that postoperative outcome depends on how precisely postsurgical vocal folds are symmetrically balanced and how normal regular vibration is generated. Technical problems could induce postoperative dysphonia or insufficient increase of pitch that might be associated with asymmetrical vocal folds level, inappropriate scarred membranous vocal folds, excessive scar formation, tension discrepancy of vocal fold muscle, and distortion of the laryngeal framework. From patient’s point of views, hyperfunctional voice or probable focal laryngeal dystonia causes aggravation of dysphonia, lowering voice pitch and pitch instability without response to voice therapy in long-term postoperative periods.46
In our experience, many patients who have postoperative dysphonia and unsatisfied pitch increase are associated with preoperative laryngeal dystonic voice symptoms or functional voice disorder. Preoperative comprehensive voice analysis and preoperative voice treatment are critical to obtain reasonable satisfied postoperative results. Notably, patients who have laryngeal dystonic voice symptoms are not considered as definite spasmodic dysphonia. They present regular speech pattern. All these patients who had functional dysphonia in preoperative voice assessment described postoperative dysphonia uncontrolled by voice therapy with unsatisfied minimal pitch increase. However, these unpredictable symptoms could be treated by Botox injection.29 Kim has described the following criteria for Botox injection; 1) patients who have strained and strangulated voice, frequent glottal fry in general conversation, and voice tremor or voice breaks on prolonged vowels, or prolonged voiceless consonants; 2) patients who have voice breaks on vowels, one or more breaks per three sentences; 3) patients who show definite three more pitch breaks and irregular vertical striation on the spectrogram of voice analysis; 4) nasopharyngoscopic examination shows intermittent hyperadduction of true vocal folds on vowels with compensatory supraglottic hyperfunctional contracture.46,47 If patient’s subjective and acoustic findings satisfied all criteria shown above, Botox injection into both thyroarytenoid muscles (0.4U each) postoperatively can help prevent the development of unpredictable postoperative dysphonia.29
The reason for the dissatisfaction of long-term consequences of postoperative outcomes under the precondition that there is no problem from the surgical point of view can be found from the patient’s point of view. We speculate that causes of unsatisfied limited pitch increase are associated with both laryngeal problem and neuronal phonatory pattern problem. Reasonable etiologies are: 1) damage to the surgical point or severe scar formation afterward by inappropriate postoperative care during the healing process; 2) benign laryngeal disease such as vocal fold swelling, edema, granuloma or polyposis due to smoking, drinking alcohol or abusing the voice; 3) reverse adaptation of resonance frequency that was induced by lowering the pitch intentionally to overcome the pitch instability or hoarseness due to mismatch between postoperative increased fundamental frequency and the resonant frequency; 4) maladaptation to changed vocal folds instead of making a new phonatory pattern. The problem is to keep one’s original abnormal phonatory pattern that usually uses generating high subglottal pressure and forcing hyperfunctional voice production to increase pitch preoperatively. Laryngeal problems (first to second) would be treated by medication, reoperation, Botox injection, or voice therapy. However, neuronal phonatory pattern problems (third and fourth) require combined medical and retraining of phonatory pattern. In our experience, some cases presented unexpected compensatory hyperfunctional voice with a limited increase of the pitch, although the surgical portion of vocal folds healed well without abnormality on it. This phenomenon is thought to be induced by abnormal adaptation to underlying functional laryngeal disorder that can be compensated for by releasing cricothyroid muscle tension and lowering the pitch. However, these patients showed normal laryngeal EMG finding on cricothyroid muscle and superior laryngeal nerve. They could get a reasonable pitch increase and feminine voice after treating the underlying functional laryngeal disorder and conducting intensive retraining of phonatory pattern.
Voice Therapy for Modification of Fundamental Frequency
Pitch is the most important feature of voice femininity, and it is reported that a minimum F0 value of 180 Hz required for a voice to be perceived as feminine.48 However, Coleman reported that an increase in the pitch is not enough to gain femininity and that there is a relationship between the value of the vowel formant frequency and perceptions of gender.49 Resonance is another vocal characteristic that contributes to the perception of gender, and maybe the second most important acoustic cue.50 In resonance, an increase in the second formant frequency (F2) results in the perception of a feminine voice. And another meaningful feminine perception of the voice is associated with increased breathiness.51 Focusing on the shifting of both F0 and the second formant frequency is the most effective treatment method in changing the perception of gender.52,53 Voice therapy does not have a different process of raising the fundamental frequency and raising the formant frequency for resonance, but rather the process of increasing the second formant frequency to change the resonance of the vocal tract can spontaneously obtain the effect of increasing the fundamental frequency and increasing the femininity of voice.26 Hancock reported 5 years of cases of voice feminization treatment techniques and outcomes. They noted that every transgender woman addressed at least one of the following in treatment goals; increase forward resonance, increase speaking pitch, relaxation technique, increase intonation, reduce phonotraumatic behaviors, improve breath control, feminine non-verbal communication, feminine pragmatics, improve vocal hygiene.54 These therapeutic goals for transgender women are consistent with the most frequently recommended goals in the research literature on voice and communication therapy for transgender women.
Generally, transgender women undergo voice therapy at a much higher rate than phonosurgery because of the easy accessibility and implementation of voice therapy. Fourteen percent of transgender women have undergone voice therapy, whereas only 1% have undergone phonosurgery.55 However, a recent systematic review and meta-analysis study identified only a small number of studies that provided standardized data for feminizing voice therapy. A large load of literature regarding feminizing voice therapy is often nonstandardized and analyzed unreliably.56 And also, there are many variations of technique and strategies to feminize voice. One article identified these variations are in part due to the complex nature of an individual’s baseline and voice goals as well as a lack of standardized treatment among speech language pathologists.57 Of the papers published so far, only two studies investigated the long-term outcomes of voice therapy for transgender women.58,59 Moreover, long-term treatment results remain in the 145–155 Hz high male voice range. Besides, the initial result is that about 50.8% of the subjects are recognized as women, but the long-term result is lowered to 33.1%.59 Therefore, as the substantially more significant number of long-term data of voice therapy are becoming more established, the standard treatment protocols for voice therapy would improve evidence-based treatment strategy for voice feminization of transgender women.
Strategy for Modification of Resonance
Feminization Voice Therapy
In the literature, voice therapy has focused on raising the pitch of speaking, cadence, intonation, resonance, speech rate, phrasing patterns, voice quality, and nonverbal communication patterns.56 Based on gender difference of phonatory organ, voice therapy for feminizing the voice successfully should make more biomechanical changes than physiological movement of vocal folds to raise the pitch to a higher level than its own voice range. Voice therapy should also make changes of vocal tract dimensions to modify oral and pharyngeal resonance. In other words, voice therapy refers to the process of changing a male phonatory organ as a female phonatory organ. However, if the patient has vast morphometric characteristics of the larynx and vocal tract, voice therapy may fail to achieve feminine voice. If the patient is in the opposite case, voice therapy may be sufficient to feminize the voice. In our experience, in patients with relatively high fundamental frequency range above 140 Hz in natural relaxed voice with wide vocal range, small membranous vocal fold at length less than 12 mm, and strong motivation for transitioning, voice therapy alone were able to obtain satisfactory results of voice feminization.
As mentioned earlier, in many studies, voice therapy is being applied to patient with various therapy goals and techniques.26,54,56,58–61 However, given that there are morphometric differences between male and female phonatory organs, voice therapy should focus on changes in resonance frequencies that are related to oral cavity volume and length as well as pharyngeal volume. Oral cavity volume and length are mainly controlled by tongue motion that also affects hyoid motion with modification of laryngeal movement. Tongue motion is crucial to muscle action to modify oral and pharyngeal resonant frequency.26,62 Generally, oral resonance therapy is thought to be very beneficial in increasing forward resonance and femininity of voice.26 In this physiological aspect of resonance of phonatory organ, voice therapy should be undertaken to improve oral resonance and reduce the volume of the pharynx for pharyngeal resonance.
Postoperative Voice Therapy for Formant Tuning and Pattern Memorization
Pitch-raising surgery is unable to modify vocal tract volume, although it can change the dimension of the vocal fold. After performing pitch-raising operation, the fundamental frequency abruptly increases to a higher level. However, increased F0 may not match resonance frequencies in the old phonatory pattern. To resonate the elevated glottal sound appropriately, formants that are resonance frequencies should match F0. In addition, the oral cavity must be made with small space to increase second formant frequency. Formants' frequencies are altered by changes in the spatial shape of the vocal tract that includes location of the primary tongue constriction, opening or closing the jaw, rounding or spreading of lips, and raising or lowering the larynx.63,64
Formant frequencies of resonance of vocal tract may be the second most crucial acoustic cue to voice feminity.26,65 As a basic knowledge of vocal tract resonance, the first formant (R1) is most responsive to changes in mouth opening. The second formant (R2) is most reactive to changes in the size of oral cavity. Tongue forwarding or spreading the lip may increase the frequency of this formant. The third formant (R3) is altered by front versus back constriction of low pharyngeal area.42 The voice femininity is highly related to a high F0 and a raising formant frequency for all four vowels.62 Therefore, based on source-filter theory, postoperatively formant tuning for improving voice feminity and readaptation of the phonatory pattern for achieving vocal tract resonance are essential to feminizing the voice postoperatively. Postsurgical voice therapy techniques to induce such resonance changes include tongue and lips relaxation, oral and pharynx resonance exercise, laryngeal relaxation, and vowel modification.54 Eventually, postoperative voice therapy may raise F0, stabilize the voice pitch, and increase femininity of the voice.56
Another importance of postoperative voice therapy is to prevent reverse adaptation of resonance frequency. Preoperative old phonatory pattern before the surgery has a low male fundamental frequency and adjusted resonance frequency. After the surgery, the fundamental frequency rises but phonatory pattern for resonance remains the same, thus creating a mismatch between postoperative increased fundamental frequency and old formant frequency. To resolve this mismatching, some patients who have undergone surgery have a more relaxed and more convenient compensatory response to intentionally lower the resonance frequency by lowering the larynx, rather than training to tune the two frequency to increased F0.
This reverse adaptation phenomenon is thought to be an adverse compensation mechanism to overcome the pitch instability or hoarseness caused by the mismatch between fundamental frequency and the resonant frequency occurring early after surgery. Occasionally, this might be misdiagnosed for a result of an imperfect operation or a lack of surgical effect. Therefore, long-term postoperative voice therapy is necessary to maintain proper phonatory pattern and suppress the generation of inappropriate patterns as well as acoustic improvement of voice.
After all, voice feminization is a process of changing the male phonatory organs into the shape of the female phonatory organs through voice therapy or surgical treatment, and of internalizing a new phonatory pattern in long-term memory. The pattern transfer from the primary memory into the more permanent secondary memory is facilitated by practice.66 That can be conducted by postoperative voice therapy.
Conclusion
Voice feminization, not just pitch increase, is a very complicated and complexity modulation procedure. It is a comprehensive medical process in which all knowledge of speech science including laryngology, speech language pathology and acoustics must be applied. Voice feminization is a long transition journey that changes a male phonatory system including phonatory organs and pattern to a female phonatory system. From the patient’s perspective, treatment modality and direction should be selected considering the order of the transition process, economic aspect, and social role. From a medical provider’s perspective, the course of treatment should be determined as a method that can maximize the safety of patient’s voice and minimize side effects while feminizing the voice.
Disclosure
The author has no funding, financial relationships, or conflicts of interest to disclose.
References
1. Jenkins JS. The voice of the castrato. Lancet. 1998;351(9119):1877–1880. doi:10.1016/S0140-6736(97)10198-2
2. Kitajima K, Tanabe M, Isshiki N. Cricothyroid distance and vocal pitch. Experimental surgical study to elevate the vocal pitch. Ann Otol Rhinol Laryngol. 1979;88(1 Pt 1):52–55. doi:10.1177/000348947908800109
3. Isshiki N, Taira T, Tanabe M. Surgical alteration of the vocal pitch. J Otolaryngol. 1983;12(5):335–340.
4. Tucker HM. Anterior commissure laryngoplasty for adjustment of vocal fold tension. Ann Otol Rhinol Laryngol. 1985;94(6 Pt 1):547–549. doi:10.1177/000348948509400604
5. LeJeune FE, Guice CE, Samuels PM. Early experiences with vocal ligament tightening. Ann Otol Rhinol Laryngol. 1983;92(5 Pt 1):475–477. doi:10.1177/000348948309200513
6. Brown M, Perry A, Cheesman AD, Pring T. Pitch change in male-to-female transsexuals: has phonosurgery a role to play? Int J Lang Commun Disord. 2000;35(1):129–136. doi:10.1080/136828200247296
7. Wagner I, Fugain C, Monneron-Girard L, Cordier B, Chabolle F. Pitch-raising surgery in fourteen male-to-female transsexuals. Laryngoscope. 2003;113(7):1157–1165. doi:10.1097/00005537-200307000-00011
8. Tanabe M, Haji T, Honjo I, Isshiki N. Surgical treatment for androphonia. An experimental study. Folia Phoniatr (Basel). 1985;37(1):15–21. doi:10.1159/000265774
9. Orloff LA, Mann AP, Damrose JF, Goldman SN. Laser-Assisted Voice Adjustment (LAVA) in Transsexuals. Laryngoscope. 2006;116(4):655–660. doi:10.1097/01.mlg.0000205198.65797.59
10. Donald PJ. Voice change surgery in the transsexual. Head Neck Surg. 1982;4(5):433–437. doi:10.1002/(ISSN)000-000
11. Gross M. Pitch-raising surgery in male-to-female transsexuals. J Voice. 1998;13:246–250. doi:10.1016/S0892-1997(99)80028-9
12. Kunachak S, Prakunhungsit S, Sujjalak K. Thyroid cartilage and vocal fold reduction: a new phonosurgical method for male-to-female transsexuals. Ann Otol Rhinol Laryngol. 2000;109(11):1082–1086. doi:10.1177/000348940010901116
13. Spiegel JH. Phonosurgery for pitch alteration: feminization and masculinization of the voice. Otolaryngol Clin North Am. 2006;39(1):77–86. doi:10.1016/j.otc.2005.10.011
14. van den BERG J. Myoelastic-aerodynamic theory of voice production. J Speech Hear Res. 1958;1(3):227–244. doi:10.1044/jshr.0103.227
15. Tucker HM. The Larynx. In: Physiology of the Larynx. Thieme Medical Publishers, Inc; 1987:21–32.
16. Xue SA, Cheng RWC, Ng LM. Vocal tract dimensional development of adolescents: an acoustic reflection study. Int J Pediatr Otorhinolaryngol. 2010;74(8):907–912. doi:10.1016/j.ijporl.2010.05.010
17. Fitch WT, Giedd J. Morphology and development of the human vocal tract: a study using magnetic resonance imaging. J Acoust Soc Am. 1999;106(3 Pt 1):1511–1522. doi:10.1121/1.427148
18. Eckel HE, Sprinzl GM, Sittel C, Koebke J, Damm M, Stennert E. Anatomy of the glottis and subglottis in the pediatric larynx. HNO. 2000;48(7):501–507. doi:10.1007/s001060050606
19. Eckel HE, Koebke J, Sittel C, Sprinzl GM, Pototschnig C, Stennert E. Morphology of the human larynx during the first five years of life studied on whole organ serial sections. Ann Otol Rhinol Laryngol. 1999;108(3):232–238. doi:10.1177/000348949910800303
20. Jotz GP, Stefani MA, Pereira da Costa Filho O, et al. A morphometric study of the larynx. J Voice. 2014;28(6):668–672. doi:10.1016/j.jvoice.2014.03.008
21. Beckford NS, Rood SR, Schaid D, Schanbacher B. Androgen stimulation and laryngeal development. Ann Otol Rhinol Laryngol. 1985;94(6 Pt 1):634–640. doi:10.1177/000348948509400622
22. Ara A, Khalil M, Sultana SZ, et al. Morphometric study of vocal fold of different sexes of Bangladeshi cadaver. Mymensingh Med J. 2010;19(2):173–175.
23. Eckel HE, Sittel C, Zorowka P, Jerke A. Dimensions of the laryngeal framework in adults. Surg Radiol Anat. 1994;16(1):31–36. doi:10.1007/BF01627918
24. Zappia F, Campani R. The larynx: an anatomical and functional echographic study. Radiol Med. 2000;99(3):138–144.
25. Mobashir MK, Mohamed AERS, Quriba AS, Anany AM, Hassan EM. Linear measurements of vocal folds and laryngeal dimensions in freshly excised human larynges. J Voice. 2018;32(5):525–528. doi:10.1016/j.jvoice.2017.08.024
26. Carew L, Dacakis G, Oates J. The effectiveness of oral resonance therapy on the perception of femininity of voice in male-to-female transsexuals. J Voice. 2007;21(5):591–603. doi:10.1016/j.jvoice.2006.05.005
27. Simpson AP. Dynamic consequences of differences in male and female vocal tract dimensions. J Acoust Soc Am. 2001;109(5 Pt 1):2153–2164. doi:10.1121/1.1356020
28. Schmidt RF, Thews G. Human Physiology. Berlin, Heidelberg: Springer Science & Business Media; 2013.
29. Kim HT. A new conceptual approach for voice feminization: 12 years of experience. Laryngoscope. 2017;127(5):1102–1108. doi:10.1002/lary.26127
30. Isshiki N, Morita H, Okamura H, Hiramoto M. Thyroplasty as a new phonosurgical technique. Acta Otolaryngol. 1974;78(5–6):451–457. doi:10.3109/00016487409126379
31. Koufman JA, Isaacson G. Laryngoplastic phonosurgery. Otolaryngol Clin North Am. 1991;24(5):1151–1177.
32. Yang CY, Palmer AD, Murray KD, Meltzer TR, Cohen JI. Cricothyroid approximation to elevate vocal pitch in male-to-female transsexuals: results of surgery. Ann Otol Rhinol Laryngol. 2002;111(6):477–485. doi:10.1177/000348940211100602
33. Wendler J: Vocal pitch elevation after transsexualism male to female. In:
34. Remacle M, Matar N, Morsomme D, Veduyckt I, Lawson G. Glottoplasty for male-to-female transsexualism: voice results. J Voice. 2011;25(1):120–123. doi:10.1016/j.jvoice.2009.07.004
35. Anderson JA. Pitch elevation in trangendered patients: anterior glottic web formation assisted by temporary injection augmentation. J Voice. 2014;28(6):816–821. doi:10.1016/j.jvoice.2014.05.002
36. Arrington ED, Miller MD. Skeletal muscle injuries. Orthop Clin North Am. 1995;26(3):411–422.
37. Tidball JG. Inflammatory processes in muscle injury and repair. Am J Physiol Regul Integr Comp Physiol. 2005;288(2):R345–53. doi:10.1152/ajpregu.00454.2004
38. Cho SH, Kim HT, Lee IJ, Kim MS, Park HJ. Influence of phonation on basement membrane zone recovery after phonomicrosurgery: a canine model. Ann Otol Rhinol Laryngol. 2000;109(7):658–666. doi:10.1177/000348940010900709
39. Koçak I, Akpınar ME, Cakır ZA, Dogan M, Bengisu S, Celikoyar MM. Laser reduction glottoplasty for managing androphonia after failed cricothyroid approximation surgery. J Voice. 2010;24(6):758–764. doi:10.1016/j.jvoice.2009.06.004
40. Geneid A, Rihkanen H, Kinnari TJ. Long-term outcome of endoscopic shortening and stiffening of the vocal folds to raise the pitch. Eur Arch Otorhinolaryngol. 2015;272(12):3751–3756. doi:10.1007/s00405-015-3721-7
41. Thomas JP, Macmillan C. Feminization laryngoplasty: assessment of surgical pitch elevation. Eur Arch Otorhinolaryngol. 2013;270(10):2695–2700. doi:10.1007/s00405-013-2511-3
42. Raphael LJ, Borden GJ, Harris KS. Speech science primer: physiology, acoustics, and perception of speech. In: The Articulation and Acoustics of Vowels. Wolters Kluwer Health/Lippincott Williams & Wilkins; 2011:88–113.
43. Wenaas AE, Tran B, Ongkasuwan J. The progression of thyroid cartilage calcification as it relates to the utilization of laryngeal ultrasound. Laryngoscope. 2016;126(4):913–917. doi:10.1002/lary.25582
44. Thomas LB, Harrison AL, Stemple JC. Aging thyroarytenoid and limb skeletal muscle: lessons in contrast. J Voice. 2008;22(4):430–450. doi:10.1016/j.jvoice.2006.11.006
45. Kersing W, Jennekens FGI. Age-related changes in human thyroarytenoid muscles: a histological and histochemical study. Eur Arch Otorhinolaryngol. 2004;261(7):386–392. doi:10.1007/s00405-003-0702-z
46. Ludlow CL, Adler CH, Berke GS, et al. Research priorities in spasmodic dysphonia. Otolaryngol Head Neck Surg. 2008;139(4):495–505. doi:10.1016/j.otohns.2008.05.624
47. Barkmeier JM, Case JL, Ludlow CL. Identification of symptoms for spasmodic dysphonia and vocal tremor: a comparison of expert and nonexpert judges. J Commun Disord. 2001;34(1–2):21–37. doi:10.1016/S0021-9924(00)00039-3
48. Gorham-Rowan M, Morris R. Aerodynamic analysis of male-to-female transgender voice. J Voice. 2000;20:251–262. doi:10.1016/j.jvoice.2005.03.004
49. Coleman RO. A comparison of the contributions of two voice quality characteristics to the perception of maleness and femaleness in the voice. J Speech Hear Res. 1976;19:168–180. doi:10.1044/jshr.1901.168
50. Mount MH, Salmon SJ. Changing the vocal characteristics of a post-operative transsexual patient: a longitudinal study. J Commun Disord. 1988;21:229–238. doi:10.1016/0021-9924(88)90031-7
51. Andrews ML, Schmidt CP. Gender presentation: perceptual and acoustical analyses of voice. J Voice. 1997;11:307–313. doi:10.1016/S0892-1997(97)80009-4
52. Hillenbrand JM, Clark MJ. The role of fundamental frequency and formant frequencies in distinguishing the voices of men and women. Atten Percept Psychophys. 2009;71(5):1150–1166. doi:10.3758/APP.71.5.1150
53. Gelfer MP, Mikos VA. The relative contributions of speaking fundamental frequencies to gender identification based on isolated vowels. J Voice. 2005;19:544–554. doi:10.1016/j.jvoice.2004.10.006
54. Hancock AB, Garabedian LM. Transgender voice and communication treatment: a retrospective chart review of 25 cases. Int J Lang Commun Disord. 2013;48(1):54–65. doi:10.1111/j.1460-6984.2012.00185.x
55. James SE, Herman JL, Rankin S, et al. The Report of the 2015 U.S. Transgender Survey. Washington, DC: National Center for Transgender Equality; 2016.
56. Nolan IT, Morrison SD, Arowojolu O, et al. The role of voice therapy and phonosurgery in transgender vocal feminization. J Craniofac Surg. 2019;30(5):1368–1375. doi:10.1097/SCS.0000000000005132
57. Gray ML, Courey MS. Transgender voice and communication. Otolaryngol Clin North Am. 2019;52(4):713–722. doi:10.1016/j.otc.2019.03.007
58. Dacakis G. Long-term maintenance of fundamental frequency increases in male-to-female transsexuals. J Voice. 2000;14(4):549–556. doi:10.1016/S0892-1997(00)80010-7
59. Gelfer MP, Tice RM. Perceptual and acoustic outcomes of voice therapy for male-to-female transgender individuals immediately after therapy and 15 months later. J Voice. 2013;27(3):335–347. doi:10.1016/j.jvoice.2012.07.009
60. Mészáros K, Vitéz LC, Szabolcs I, et al. Efficacy of conservative voice treatment in male-to-female transsexuals. Folia Phoniatr Logop. 2005;57(2):111–118. doi:10.1159/000083572
61. Gelfer MP, Van Dong BR. A preliminary study on the use of vocal function exercises to improve voice in male-to-female transgender clients. J Voice. 2013;27(3):321–334. doi:10.1016/j.jvoice.2012.07.008
62. Gallena SJK, Stickels B, Stickels E. Gender perception after raising vowel fundamental and formant frequencies: considerations for oral resonance research. J Voice. 2018;32(5):592–601. doi:10.1016/j.jvoice.2017.06.023
63. Stevens KN, House AS. An acoustical theory of vowel production and some of its implications. J Speech Hear Res. 1961;4:303–320. doi:10.1044/jshr.0404.303
64. House AS, Stevens KN. Estimation of formant bandwidths from measurements of transient response of the vocal tract. J Speech Hear Disord. 1958;1(4):309–315. doi:10.1044/jshr.0104.309
65. Spencer LE. Speech characteristics of male-to-female transsexuals: a perceptual and acoustic study. Folia Phoniatr (Basel). 1988;40(1):31–42. doi:10.1159/000265881
66. Waugh NC, Norman DA. primary memory. Psychol Rev. 1965;72:89–104. doi:10.1037/h0021797
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.