")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 11 » Issue 1
Vitamin D should be supplemented more actively in elderly patients with coronary heart disease combined with COPD
Received 2 February 2016
Accepted for publication 31 March 2016
Published 21 June 2016 Volume 2016:11(1) Pages 1359—1365
DOI https://doi.org/10.2147/COPD.S105671
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Ling Zhang,1 Qiao-ying Yuan2
1Department of Out-patient Clinic, 2Department of Nutriology, Southwest Hospital, The Third Military Medical University, Chongqing, People’s Republic of China
Objective: It is not clear whether vitamin D should be actively supplemented in elderly patients suffering from an acute attack of COPD (AECOPD) and coronary heart disease (CHD).
Patients and methods: The patients were divided into three groups according to specific criteria: patients with AECOPD (group A), patients with COPD combined with CHD (group B), and patients with CHD (group C). We measured the levels of vitamin D and analyzed the correlation between vitamin D and important electrolytes, including prealbumin, creatinine, hemoglobin, cystatin C, blood fat, blood calcium, and blood magnesium, and the nutrition state of the whole body. The serum B-type natriuretic peptide (BNP) was measured using an ELISA kit.
Results: The vitamin D level in group B was the lowest, followed by group A. When compared with group C, they all had statistical significance (P<0.05), but there was no statistical difference between groups A and B. There was no difference among the three groups when prealbumin, creatinine, hemoglobin, cystatin C, blood fat, blood calcium, and blood magnesium were compared. The level of BNP in the three groups increased, but it had no obvious correlation with the level of vitamin D (P>0.05).
Conclusion: When elderly patients have coronary artery disease with AECOPD, vitamin D levels were obviously lower and were negatively correlated with the BNP. Low vitamin D levels, as well as poor nutrition, affect cardiopulmonary function and quality of living of elderly patients, especially female patients. Therefore, vitamin D should be supplemented more actively in the female patients suffering from AECOPD and CHD.
Keywords: COPD, CHD, cardiac function, vitamin D, nutrition
Introduction
With the aging of the population, morbidity due to COPD increases each year. COPD affects the whole body and causes constitutional symptoms. Especially, COPD with coronary heart disease (CHD) causes damage to the cardiopulmonary function, which severely affects the quality of life of the patients,1–5 thus making it a challenge and difficult to treat in elderly patients. In recent years, some studies have demonstrated that other than viruses, bacteria were the main triggers of COPD exacerbations. Vitamin D levels are also closely correlated with the occurrence of cardiopulmonary diseases, such as ischemic heart disease, high blood pressure, cardiac failure, and COPD.
Vitamin D plays an important role in preventing lung inflammation and an unbalanced oxidation–antioxidation process. It can also play a beneficial role in cardiovascular protection by affecting the renin–angiotensin system, regulating blood glucose levels, reducing the inflammatory reaction of vasculature,6–10 and resisting myocardial hypertrophy and hyperplasia. However, researchers also found that taking large doses of vitamin D does not reduce the frequency of progression of the disease of patients with COPD. Additionally, until now, no study had verified that vitamin D reduced the frequency of CHD. It is disputed as to whether patients with COPD and CHD need vitamin D supplementation and whether they benefit from vitamin D. Also, it is not clear how vitamin D counteracts the CHD. There is a lack of information obtained from clinical experiments and few studies on the condition of vitamin D metabolism in elderly patients with acute attack of COPD (AECOPD) combined with CHD. There have been no studies on whether vitamin D metabolism is different among patients with COPD (acute or stable phase) with CHD and patients with pure COPD and pure CHD or whether the vitamin D level is lower when two diseases combine together and when the supplementation of vitamin D shall be more often, which needs further research. Comprehensive research on these questions has important clinical significance. However, it is not clear which group of people need extra vitamin D, especially when there is a dispute about whether patients with COPD need active vitamin D supplementation and whether vitamin D also has an effect on the state of nutritional status and internal environment (such as electrolyte) of the patients. Therefore, in this study, we explored the level of vitamin D metabolism in patients with acute COPD and a stable period with CHD, which provides clinical suggestion to the reasonable supplementation of vitamin D for elderly patients with pure COPD, CHD, or COPD with CHD.
Patients and methods
We collected the data from elderly COPD patients who were hospitalized in the Southwest Hospital (The Third Military Medical University, Chongqing, People’s Republic of China) from January 2013 to March 2014. Those who met the specific criteria were divided into three groups: 68 cases of AECOPD (group A), 45 cases of COPD with CHD (group B), and 44 cases of CHD not combined with AECOPD (group C). All the patients in group A met the following diagnostic criteria of an AECOPD: medical history, symptom, sign, chest computed tomography, and other imageological examinations, combined with the time of admission to hospital or past lung function testing results: FEV1/FVC (forced vital capacity rate of 1 second) <70%, and the percentage of FEV1 in predicted value was <80% after the application of bronchodilators, excluding bronchial asthma, bronchiectasis, phthisis, diffuse panbronchiolitis, etc. All the patients in group C met the diagnostic criteria of CHD (while excluding the patients with combined AECOPD): finding of proof of myocardial ischemia or coronary obstruction through medical history, symptom, and sign, combined with auxiliary examination, and clarify a diagnosis for the past of the patients with CHD through electrocardiogram, ultrasonic cardiogram, myocardial perfusion imaging, coronary computed tomography, and coronary angiogram. Patients of group B had CHD and AECOPD at the same time. The protocols for treating AECOPD, COPD of the stable period, and CHD were the same. The exclusion criteria were 1) endocrine diseases of bone metabolism; 2) having accepted treatment with diphosphonate or parathyroid hormone, or having had traumatic fracture in the past 90 days; 3) having accepted radiotherapy in the past 4 weeks; 4) having other diseases, such as tumor, type I diabetes, and parathyroid gland-related diseases affecting vitamin D level; and 5) no history of using the medicines that affect vitamin D metabolism, such as phenobarbital, dilantin, etc. Experimental protocols were approved by the Ethic Committee of Third Military Medical University, Chongqing, People’s Republic of China. Written informed patient consent was obtained.
Cardiac ultrasound and cardiac functional analysis
The GEVivid 7 ultrasonic cardiogram equipment 220V, 50Hz, PAL, holographic color doppler ultrasonic diagnostic system, manufactured by GE Company in the US, was used with the transducer frequency at 4S and 7S. It synchronously records the electrocardiogram, and it records and analyses three parameters: ejection fraction (EF), shortening fraction (FS), and end diastolic volume (EDV) of left ventricle according to different ultrasonic sections.
Bone metabolism detection
An early morning, fasted venous blood sample was collected. The lowest detection limit was ≤3 ng/mL, and vitamin D levels lower than the detection limit were computed as 3 ng/mL. Total 25-hydroxyl vitamin D (25 OH D) was measured using direct competitive immunoassay.
Determination of prealbumin, creatinine, hemoglobin, cystatin C, blood calcium, blood magnesium, and BNP
The doctor took 3–5 mL of limosis venous blood in the morning and detected prealbumin, creatinine, hemoglobin, cystatin C, blood calcium, blood magnesium, and B-type natriuretic peptide (BNP) through a fully automatic blood biochemical analyzer after the samples were centrifuged. We used a kit to detect the BNP.
Correlation analysis
We performed correlated regression analysis between vitamin D and prealbumin, blood fat, creatinine, hemoglobin, blood calcium, other electrolytes, and the nutrition state. We also performed correlation analysis between vitamin D and BNP, EF, FS, and heart rate.
Statistical method
The data are expressed as the mean ± standard deviation. Analysis of variance (SPSS 14.0 statistical software; SPSS Inc., Chicago, IL, USA) was used to assess the data. P<0.05 was considered statistically significant. Viability was compared across multiple experimental groups using a one-way analysis of variance followed by post hoc Tukey analysis to determine significant differences (P<0.05) between the different groups. Relationships between continuous variables were examined using simple linear regression analyses. Nonnormally distributed data were log-transformed before analysis.
Results
General situation of the three groups of patients
Group A had 68 patients, including 48 male patients and 20 female patients, and the average age of the patients was 73 years and 82 years, respectively. There were 28 male patients and 17 female patients in group B, and the average age of group B was 75 years and 85 years, respectively. There were 21 male patients and 23 female patients in group C, and the average age was 79 years and 83 years, respectively. The common concomitant diseases found together in selected patients include hypertensive disease, diabetes mellitus, osteoporosis, hyperplasia of prostate, cardiac insufficiency, respiratory failure, malnutrition, etc.
Comparison and statistical analysis of vitamin D levels
The comparison and statistical analysis of the vitamin D levels of patients in the three groups revealed some interesting results (Figure 1). When compared with normal vitamin D metabolism levels, the vitamin D level of the patients in all three groups declined, especially for those in group B. When the vitamin D levels in the three groups were compared with each other, there was no statistical difference between group A and group B, but there were statistical differences between the other two-group comparisons. Further analysis of the difference in the vitamin D levels between the male and female patients of the three groups indicated the following: vitamin D levels in the female patients of the three groups were lower than that in the male patients, but there was no statistical difference between group B and group C; the vitamin D levels in the female patients of group A were lower than that in the male patients, and this was statistically different. Analysis in the patients with COPD in the stable period indicated that the average level of vitamin D of the patients in the three groups did not differ very much, but the levels of vitamin D in the female patients were still lower than that in the male patients, especially for group B.
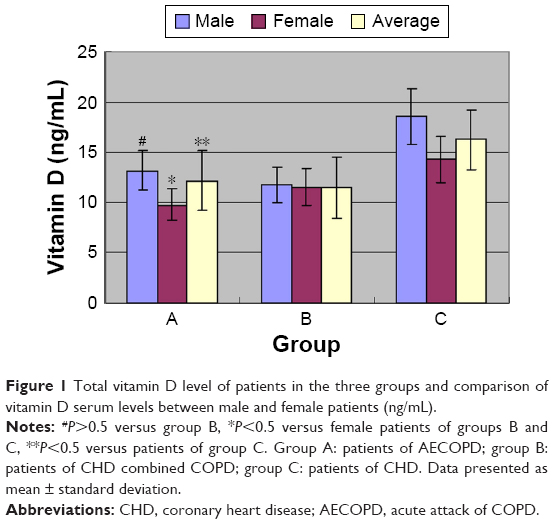 | Figure 1 Total vitamin D level of patients in the three groups and comparison of vitamin D serum levels between male and female patients (ng/mL). |
Correlation analyses between vitamin D and prealbumin, creatinine, hemoglobin, cystatin C, blood calcium, and blood magnesium
For the level of electrolytes, the statistical analysis indicated that the levels of blood magnesium and blood calcium of the three groups of patients were not lower than the common range, but they were close to the normal lower limit. In the three groups, the level of blood calcium of patients of group B was much lower, while the level of blood magnesium was higher (Figure 2). The level of cystatin C in the three groups of patients was higher than the normal value. The value of creatinine was normal but was close to the normal higher limit. The level of cystatin C and creatinine of group B increases, but there was no statistical difference.
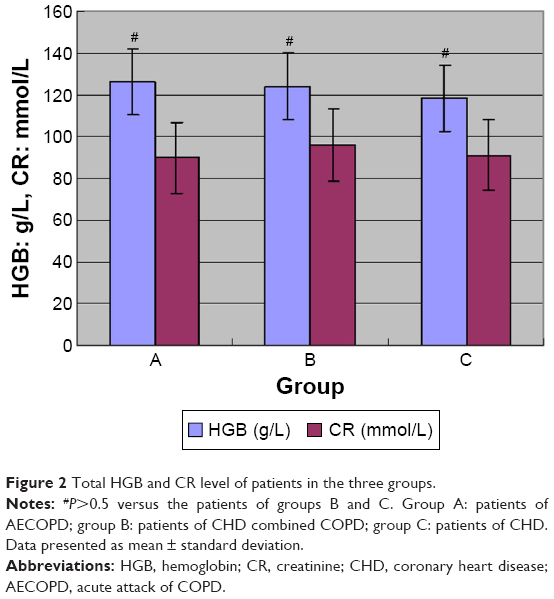 | Figure 2 Total HGB and CR level of patients in the three groups. |
State of nutrition
The state of nutrition (such as blood fat and hemoglobin) was analyzed in the three groups of patients.
The comparison of hemoglobin between the three groups indicates the following: the level of hemoglobin in the patients in group A was higher than that observed for groups B and C (Figure 3). The level of prealbumin in the patients in all the groups declined, especially in group B. Though there are no obvious statistical differences for apolipoprotein A1, apolipoprotein B, high-density lipoprotein cholesterol, and low-density lipoprotein cholesterol between the three groups, group B tended to be lower.
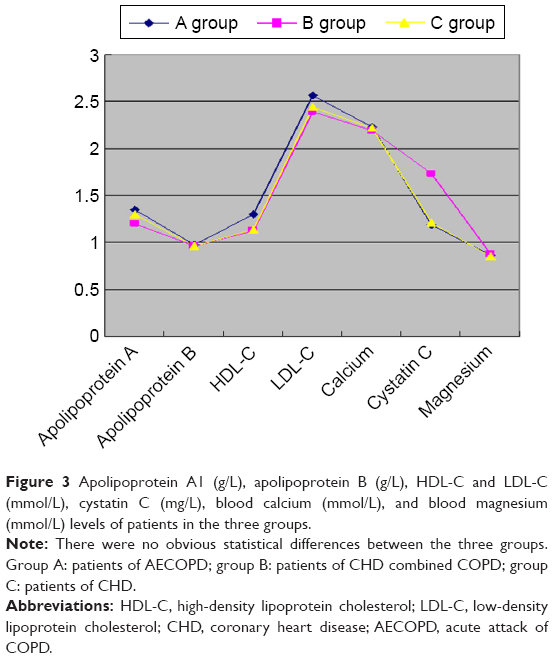 | Figure 3 Apolipoprotein A1 (g/L), apolipoprotein B (g/L), HDL-C and LDL-C (mmol/L), cystatin C (mg/L), blood calcium (mmol/L), and blood magnesium (mmol/L) levels of patients in the three groups. |
State of cardiac function in the three groups of patients
The level of BNP in the three groups of patients increased significantly, especially for group B, followed by group C, and then group A, which was the lowest (Figure 4). A comparison of the groups showed that there was a statistically significant difference between group A and group B. FS and EF do not decline much, and there was no difference between the three groups. When compared with normal values, EDV for the three groups of patients did not exceed the normal high limit level. However, a comparison of the three groups shows that, compared with group A, EDV of group B increased and attained statistical significance. Heart rate analysis indicated that the average rate for the three groups of patients was <100 beats/min, but it was within the normal high limit. There was no statistical difference between the three groups.
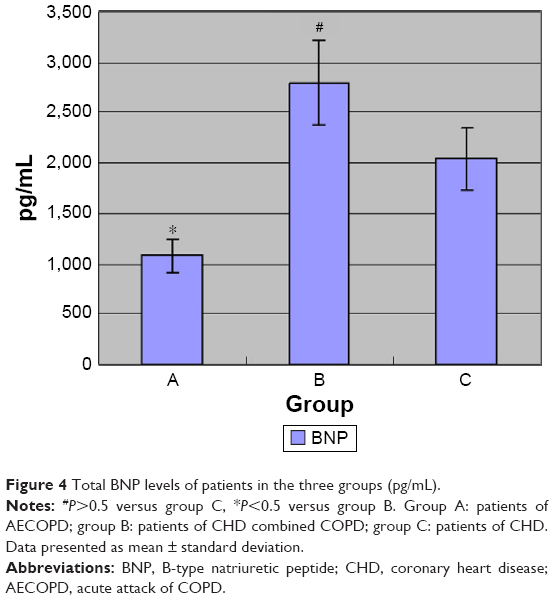 | Figure 4 Total BNP levels of patients in the three groups (pg/mL). |
Analysis of the correlation of vitamin D with cardiac function and BNP
Correlation analysis in statistics showed that EF, FS, EDV and other detection index of cardiac function, and the heart rate had no obvious correlation with vitamin D levels (Figure 5). Additionally, BNP was negatively correlated with vitamin D levels. This correlation was low, and there was no statistically significant difference.
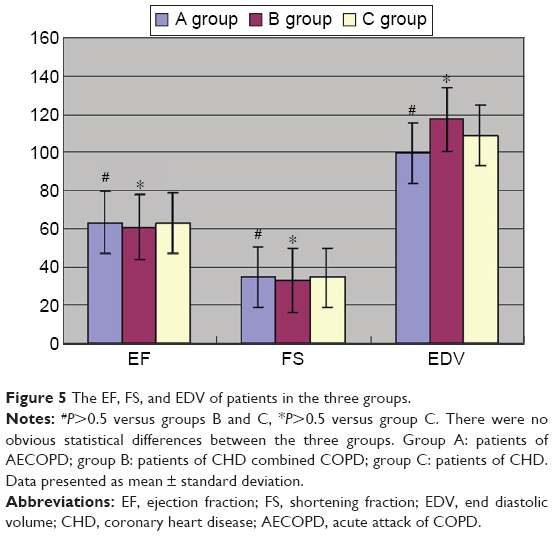 | Figure 5 The EF, FS, and EDV of patients in the three groups. |
Discussion
A previous study showed that vitamin D can directly act on heart tissue and the vascular bed. Through investigation of model knockout mice that do not express the vitamin D acceptor, Li et al at the University of Chicago found that these mice had renin–angiotensin–aldosterone system activity than the control.11 They also had cardiac hypertrophy, which proves that the new composite vitamin D analog can block renin expression in vitro. Supplementing vitamin D in patients with cardiac failure can obviously reduce the level of inflammatory cytokines related to the pathophysiology of cardiac failure. On the other hand, the low content of serum 25 OH D is correlated with low vital capacity, traumatic immune control, and respiratory tract inflammation. Since most of the patients with COPD have insufficient vitamin D levels, vitamin D can do more than prevent osteoporosis for the patients with COPD.5,12–15 Therefore, we studied vitamin D metabolism levels in the three groups of patients with AECOPD, AECOPD with CHD, and CHD. We explored the correlation with cardiac function and BNP and analyzed the state of nutrition. This provides suggestions for the prevention of COPD with and without cardiovascular disease through reasonable supplementation with vitamin D.
This study included 157 patients with severe AECOPD. We found that the vitamin D level declined in all three groups of patients. In particular, the patients with AECOPD with CHD had lower vitamin D levels, while there was no obvious difference in the stable period of COPD. Therefore, we concluded that recent exacerbation of chronic bronchitis in the patients may be correlated with the low levels of vitamin D. After further analysis, we found that it was correlated with composite factors, such as poor pulmonary function affecting the capacity for action, skeletal muscle dysfunction, and inhalation or vein use of glucocorticoid, while exacerbation of COPD may cause the decrease in vitamin D levels in return. Further analysis revealed that the comparison of patients with pure COPD and patients in group B revealed no statistical difference. This indicates that the patients with COPD had severe vitamin D deficiency, while the vitamin D deficiency in patients with pure CHD was not as severe as that of patients with pure COPD. However, once the patients develop AECOPD, the vitamin D deficiency become severe. Therefore, these kinds of patients need to pay attention to supplementation of vitamin D. The vitamin D levels in female patients were lower than that in the male patients, which may be related to factors such as less exercise, lower weight, and post-menopause internal secretion changes. Therefore, female patients with COPD combined with CHD should pay more attention to supplementation of vitamin D and the detrimental effects caused by low vitamin D levels.
We explored the correlation with cardiac function and BNP. This provides suggestions for the prevention of COPD with and without cardiovascular disease through reasonable supplementation with vitamin D. The prealbumin (normal value =0.28–0.36 g/L) can reflect the nutrition state of the whole body of patients earlier than albumin. This study shows that the prealbumin has stronger specificity and is more sensitive in monitoring malnutrition and the stress reaction of the body. Blood magnesium and blood calcium take part in important physiological activities in muscle and myocardium, and vitamin D has an effect on the metabolism of calcium and magnesium. The electrolyte and nutrition state of the three groups of patients revealed that group B had the lowest calcium ion levels but with the highest magnesium levels. However, these results were not statistically significant, and vitamin D levels had no correlation with blood magnesium and blood calcium levels.
Analysis of blood fat metabolism levels among the three groups revealed that there was no obvious difference in apolipoprotein A1, apolipoprotein B, high-density lipoprotein cholesterol, or low-density lipoprotein cholesterol. This means that there is less change in fat metabolism of the patients with AECOPD and patients with CHD. In patients with COPD with CHD, the concentration of hemoglobin was higher than that in the patients with CHD. The concentration increased in group A, which was correlated with chronic anoxia of the patients. The lowest prealbumin levels were observed in patients in group B, followed by group A, indicating that the poor nutritional state was an important factor affecting the quality of life and body state of the patients. Cystatin C levels were higher than the normal value, while creatinine was in the normal range, which showed that it is important to prevent renal function damage to the patients in early period, and the doctor should pay attention to observation of urine volume and avoid the drugs damaging the kidney. The prealbumin and albumin blood levels are poor indicators of nutritional status and more reflective of inflammation.
The result showed that patients in group B had the highest BNP levels, accompanied by severely damaged cardiac function. It should be noted that the BNP levels in patients with pure COPD were higher than the normal value. This means that chronic anoxia and inflammatory factor led to different degrees of damage to cardiac function in the patients with COPD. Therefore, during correction of anoxia and improvement of pulmonary function, attention should be paid to early maintenance and long-term improvement of cardiac function.
Some studies16 showed that the level of vitamin D and BNP was negatively correlated. The routine BNP detection of COPD patients with a history of heart failure can be useful for newly diagnosed or undiagnosed heart failure. BNP is more than just a biomarker. As a matter of fact, BNP may be a response to disease remission. The increase in the BNP concentration in patients with COPD indicates the doctor should start-up the treatment plan to improve the heart function. During differentiation of cardiogenic and pulmonary dyspnea, it should be taken into consideration that BNP levels may increase in patients with acute attacks of chronic bronchitis. From the changes in cardiac function, we noticed that EF and FS reflected that the indexes of cardiac ejection and myocardial contraction speed were not obviously correlated with vitamin D levels. However, the EDV of group B increased substantially, further indicating that the early changes in the cardiac function were mainly diastole damage. Especially for the patients with COPD with CHD, the concentration of BNP increases with the decrease of 25 OH D in blood circulation, but there was no obvious statistical significance.
Clinical doctors pay more attention to vitamin D levels in patients with COPD, but vitamin D deficiencies in patients with CHD are usually ignored. Therefore, we suggest that these doctors pay attention to the vitamin D metabolism in elderly patients with CHD. It should be noted that CHD is also a chronic and systemic disease. Our research is just the first step in the use of vitamin D in cardiopulmonary diseases. More work is needed to advocate the use of vitamin D for the treatment and prevention of COPD.
In general, vitamin D metabolism plays an important role in maintaining the stable state of cardiac and pulmonary functions of elderly patients. It is necessary and important to provide more active and proper vitamin D supplements to elderly patients (especially female patients) with CHD with AECOPD. Our research shows that poor nutritional state and internal environment disturbances may be closely correlated with the cardiopulmonary function of the patients, and the abnormal state of the whole body affects vitamin D metabolism and cardiopulmonary function in return. The doctor should also be paid to improve the nutritional state of the whole body of the patient. This is better for improving the overall state of this kind of patients. However, the dose of vitamin D, course of treatment, and opportunity should be further verified through clinical trials. For the patients with CHD with COPD, the doctor at least should suggest and urge patients to eat a healthy, balanced diet, rich in calcium and vitamin D, and avoid smoking and drinking alcohol. The low vitamin D levels might be partly or entirely secondary to the reduced appetite and housebound status (hence lack of sunlight exposure) of such patients.
Limitations of the study
Because the cases selected for the groups were strictly controlled, the total number of cases selected into the groups in 2 years is limited. Patients in the three groups had multiple complications, which may affect the level and function of vitamin D, so more cases are needed. We need to increase the amount of study samples and lengthen the time of follow-up studies to further comprehend and distinguish the beneficial effect on the patients with COPD and patients with COPD with CHD.
Acknowledgments
We are grateful for the support of Bo Zheng, MD, from Southwest Hospital, the Third Military Medical University. This article is the project of the National Natural Science Foundation of China (81271657).
Disclosure
The authors report no conflicts of interest in this work.
References
Thyssen JP, Thuesen B, Huth C, et al. Skin barrier abnormality caused by filaggrin (FLG) mutations is associated with increased serum 25-hydroxy vitamin D concentrations. J Allergy Clin Immunol. 2012;157(3):249–250. | ||
Pfeffer PE, Hawrylowicz CM. Vitamin D and lung disease. Thorax. 2012;67(11):1018–1020. | ||
Skaaby T, Husemoen LL, Pisinger C, et al. Vitamin D state and cause-specific mortality: a general population study. PLoS One. 2012;7(12):e52423. | ||
Lehouck A, Mathieu C, Carremans C, et al. High doses of vitamin D to reduce exacerbations in chronic obstructive pulmonary disease: a randomized trial. Ann Intern Med. 2012;156(2):105–114. | ||
GOLD [homepage on the Internet]. From the Global Strategy for the Diagnosis, Management and Prevention of COPD, Global Initiative for Chronic Obstructive Lung Disease (GOLD); 2014. Available from: http://www.goldcopd.org/. Accessed April 23, 2016. | ||
Rittayamai N, Chuaychoo B, Sriwijitkamol A. Prevalence of osteoporosis and osteopenia in Thai COPD patients. J Med Assoc Thai. 2012;95(8):1021–1027. | ||
Singh S, Loke YK. An overview of the benefits and drawbacks of inhaled corticosteroids in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2010;5:189–195. | ||
Grant WB. Effect of follow-up time on the relation between prediagnostic serum 25-hydroxyvitamin D and all-cause mortality rate. Dermatoendocrinol. 2012;4(2):198–202. | ||
Jorde R, Sneve M, Hutchinson M, Emaus N, Figenschau Y, Grimnes G. Tracking of serum 25-hydroxyvitamin D levels during 14 years in a population based study and during 12 months in an intervention study. Am J Epidemiol. 2010;171(8):903–908. | ||
Thomsen RW, Lange P, Hellquist B, et al. Validity and under recording of diagnosis of COPD in the Danish National Patient Registry. Respir Med. 2011;105(7):1063–1068. | ||
Li YC, Pirro AE, Amling M, et al. Targeted ablation of the vitamin D receptor: an animal model of vitamin D-dependent rickets type II with alopecia. Proc Natl Acad Sci U S A. 1994:9831–9835. | ||
Ginde AA, Mansbach JM, Camargo CA Jr. Association between serum 25-hydroxyvitamin D level and upper respiratory tract infection in the Third National Health and Nutrition Examination Survey. Arch Intern Med. 2009;169(4):384–390. | ||
Bai P, Sun Y, Jin J, et al. Disturbance of the OPG/RANK/RANKL pathway and systemic inflammation in COPD patients with emphysema and osteoporosis. Respir Res. 2011;12:157. | ||
Olmos JM, Hernández JL, Llorca J, Nan D, Valero C, González-Macías J. Effects of 25-hydroxyvitamin D3 therapy on bone turnover markers and PTH levels in postmenopausal osteoporotic women treated with alendronate. J Clin Endocrinol Metab. 2012;97(12):4491–4497. | ||
Kruger MC, Ha PC, Todd JM, et al. High-calcium, vitamin D fortified milk is effective in improving bone turnover markers and vitamin D state in healthy postmenopausal Chinese women. Eur J Clin Nutr. 2012;66(7):856–861. | ||
Cazzolaa M, Rogliania P, Materad MG. Cardiovascular disease in patients with COPD. Lancet Respir Med. 2015;3(8):593–595. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.