")
Back to Journals » Clinical Ophthalmology » Volume 14
Visual Impairment and Mental Health: Unmet Needs and Treatment Options
Authors Demmin DL, Silverstein SM
Received 18 April 2020
Accepted for publication 6 August 2020
Published 3 December 2020 Volume 2020:14 Pages 4229—4251
DOI https://doi.org/10.2147/OPTH.S258783
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Docia L Demmin,1 Steven M Silverstein2
1Department of Psychology, Rutgers University, Piscataway, NJ, USA; 2Departments of Psychiatry, Neuroscience, and Ophthalmology, University of Rochester, Rochester, NY, USA
Correspondence: Docia L Demmin
Department of Psychology, Rutgers University, 152 Frelinghuysen Road, Piscataway, NJ 08854, USA
Tel +1 732 235 2848
Email [email protected]
Purpose: An estimated 2.2 billion people are visually impaired worldwide. Given that age-related vision loss is a primary cause of vision impairment, this number is projected to rise with increases in average lifespan. Vision loss often results in significant disability and is associated with a substantial economic burden, reduced quality-of-life, concurrent medical issues, and mental health problems. In this review, the mental health needs of people with vision impairment are examined.
Patients and methods: A review of recent literature on mental health outcomes and current treatments in people with visual impairment was conducted.
Results: Considerable data indicate that rates of depression and anxiety are elevated among people with visual impairments. Moreover, individuals of lower socioeconomic status may be at increased risk for vision impairment and subsequent mental health problems. Existing psychosocial interventions for improving mental health in people with visual impairment show some promise, but are limited by low adherence and lack generalizability.
Conclusion: In order to improve outcomes, a better understanding of the mechanisms linking visual impairment and poor mental health is needed. It will also be essential to develop more effective interventions and expand access to services to improve the detection and treatment of mental health problems in this population.
Keywords: visual impairment, vision loss, mental health, psychosocial interventions
Introduction
Impairments in vision are highly prevalent, affecting roughly 2.2 billion people worldwide.1 Of these individuals, approximately 36 million are blind, and an estimated 217 million have marked (ie, moderate-to-severe) visual impairment.2 In the US, age-related vision loss is a leading cause of disability among aging adults, primarily resulting from eye diseases such as macular degeneration, cataracts, glaucoma, and diabetic retinopathy.3 Consequently, as increases in longevity raise the average age of the population, the incidence of visual impairment is also projected to grow, with global rates of blindness tripling and moderate-to-severe vision impairment doubling over the next 30 years.2 As the prevalence of vision impairments continues to rise, so does the need to better understand the wide-ranging impact of these impairments on an individual’s mental health, quality-of-life, and overall well-being.
Vision impairments often result in significant disability and are associated with a substantial economic burden (estimated at more than $3 trillion globally) attributable to both direct and indirect (eg, productivity loss) costs.4 In addition to the economic impact of blindness and vision loss, vision impairment is associated with reduced quality-of-life,5 unintentional injuries,6 and loneliness.7 Moreover, individuals with visual impairment may be at greater risk for developing mental health problems, such as depression and anxiety.8 However, because vision loss is conceptualized as a physical problem, the psychological sequelae of vision impairment may be under-recognized. In this review we examine the prevalence, development, and treatment of mental health problems in visually impaired populations.
Part I: Vision Loss and Mental Health
Depression in Visually Impaired Populations
A sizable body of literature suggests that people with vision impairment are at increased risk for specific mental health problems. In particular, a number of studies have demonstrated a link between vision impairment and depression (eg,9–11). Nearly one third of individuals with visual impairments and disabling eye diseases experience mild depressive symptoms,12 while 10.7–45.2% of study samples report clinically significant (ie, moderate-to-severe) depressive symptoms.10–14 In one study of adults aged 20 and older, 10.7% of individuals with visual acuity impairment (ie, worse than 20/40, but not including complete blindness) endorsed clinically significant levels of depression, as opposed to 6.8% of people without acuity impairment.11 In a study of adults with more severe visual impairment (acuity worse than 20/60 or blindness), 45.2% of the sample reported moderate depressive symptoms as compared to 16.6% in the normal to near-normal vision group.10 Additionally, data from community samples indicates that people with low vision and/or blindness are 1.6–2.8-times more likely to develop depression compared to those without vision impairment,10,11 even after controlling for demographic variables (but not after accounting for socioeconomic and health characteristics11). However, visual impairment has been shown to increase the risk of depression (hazard ratio=1.22), even after adjusting for demographic, socioeconomic, and health factors.9 Subjective evaluations of vision loss also appear to be linked with depression. In several studies, individuals with reported loss of visual function (eg, difficulty reading newsprint, going down steps) endorsed higher levels of depressive symptoms, with 11.3–20.8% experiencing moderate-to-severe depression,11,15 as compared to 4.8% of people with no impairment in visual function.11 Moreover, in one of these studies a relationship between depressive symptom severity and number of reported visual function problems was observed.11 These findings indicate that rates of depression are significantly increased in people with varying degrees of vision loss.
Importantly, elevated rates of depressive symptoms have been observed in a range of different visually impaired populations. For example, in a study of retinitis pigmentosa, approximately 26% of the sample reported clinically significant depressive symptoms, despite relatively normal (central) visual acuity.16 Similarly, nearly 30% of individuals with non-infectious ocular inflammatory disease but normal to near normal acuity endorsed mild-to-severe levels of depression.17 However, other findings indicate that certain eye conditions may confer a relatively greater risk for depression. In a study by Cumurcu et al,18 depression scores were significantly higher among people with pseudoexfoliative glaucoma, which has been associated with faster rates of progression and poorer treatment response, compared with primary open-angle glaucoma and age-matched controls, although groups did not differ significantly in rates of depressive disorder diagnoses. In another study, patients with primary angle-closure glaucoma, where vision loss occurs rapidly, reported higher levels of depressive symptoms than did patients with primary open-angle glaucoma, where vision loss is progressive, and normal-vision controls.19 Some data also suggest that depression severity may depend on the nature and onset of vision loss. For example, Koenes and Karshmer20 reported that depression scores were significantly higher in a sample of adolescents who were legally blind since birth relative to their sighted peers (though still within the mild range). However, in another study there was no significant difference between adolescents with congenital blindness and peers without visual impairment in terms of depression scores,21 and a third study found rates of psychiatric comorbidity were lower among blind children and adolescents (approximately 9%) when compared with community prevalence estimates (approximately 13%).22 Thus, while depression is a significant problem for many people with vision impairment, vision loss very early in life may be associated with less severe depression, perhaps due to a lesser need to relearn life skills compared to people who lose vision later in life.
Anxiety in Visually Impaired Populations
Fewer studies have investigated rates of anxiety among visually impaired populations. However, there is some evidence for increased prevalence. Donoyama and Takeda23 found that massage practitioners with visual impairment reported higher levels of anxiety in comparison to same-age individuals in the general population. In newly-diagnosed glaucoma patients, roughly 35% of the study sample reported experiencing nervousness, anxiety, or stress; however, none of these patients had significant visual impairment (acuity 20/40 or better) and anxiety symptom severity did not correlated with degree of vision impairment.24 This suggests that concern about having to live with vision loss in the future, and/or having to cope with knowledge that one has a progressive condition, can contribute to anxiety, even in the absence of reduced visual abilities. In another study of adolescents, endorsements of symptoms related to anxiety, tension, and general distress (eg, obsessive-compulsive related symptoms, paranoid symptoms, hostility, total symptoms) were significantly higher in those with vision impairment compared to those without.25 Additionally, Bolat et al21 reported that anxiety levels among adolescents with congenital blindness were elevated relative to their sighted peers. In a small sample of female veterans with significant vision loss (ie, acuity 6/60 or worse) or blindness, 11.1% endorsed elevated levels of PTSD-related symptoms, while one in five met criteria for a probable anxiety disorder diagnosis.14 In another study, patients with primary angle-closure (rapid progression) and primary open-angle (gradual progression) glaucoma reported greater levels of anxiety symptoms than did controls, but prevalence was highest among those with primary angle-closure glaucoma.19 However, Cumurcu et al18 found no significant differences in anxiety symptom scores or diagnoses among individuals with pseudoexfoliative glaucoma, primary open-angle glaucoma, and normal vision controls. Therefore, in contrast to a robust association between vision impairment and depression, anxiety may be less pervasive among individuals with vision loss, and its emergence may be significantly mediated by other factors.
Age-Related Vision Loss and Mental Health
Impairments in vision are closely linked with age, and rates of blindness and vision loss increase dramatically with each decade of life over 40 years of age.26,27 Among older adults, age-related macular degeneration (AMD) is a primary cause of vision loss, affecting an estimated 196 million people globally in 2020.28 As opposed to complete blindness, age-related causes of vision loss often result in partial sight or low vision. However, impairments are generally not correctable by usual means (ie, glasses, contacts, surgical procedures), and individuals commonly experience gradual and continued deterioration.3 Thus, people with age-related vision loss constitute a large percentage of the visual impairment population.26,28
As mental health conditions are already fairly prevalent among older adults, with estimates of major depression ranging from 1–5% in community samples,29 older adults with vision impairments may be at even greater risk for mental health problems. Indeed, visual disability has been identified as a strong indicator of depression in older adults.30 In studies of older adults with vision loss a high prevalence of several mental health conditions, but particularly depression, has been observed.31–34 Data indicate that up to 8.6% of older adults with vision loss meet criteria for a depressive disorder,33,35 a notably higher percentage than found in the general aging population29, and 10.9–43% report clinically significant levels of depressive symptoms.32,–33,–36–41 Seniors with comorbid depression and vision impairment have higher rates of smoking, obesity, physical inactivity,42 and poorer evaluations of health,37 potentially resulting from depressive symptomatology. Nevertheless, even after controlling for socio-economic and health-related factors, vision loss has been identified as a significant predictor of depression in aging adults, both cross-sectionally and longitudinally.34,39,43 In AMD, the prevalence of depression may be even higher. In studies of AMD, 10.5–44.4% of participants report moderate-to-severe symptoms of depression,44–48 and up to 32.5% meet major depressive disorder criteria.49 Notably, depression rates are similarly elevated in both non-neovascular (ie, dry) AMD, whereby layers of the macula progressively deteriorate, and neovascular (ie, wet) AMD, which involves more rapid and severe vision loss.50 While AMD is always bilateral, disease progression is not necessarily equilateral; however, data indicate that nearly 30% of patients develop a depressive disorder within a few months of acquiring AMD in their second eye.47 Increased AMD severity has also been linked with more severe depressive symptoms,44,51 and in some studies a relationship between depressive symptom severity and degree of visual impairment has been observed,44 but not all.48 Therefore, depression is a significant issue in visually impaired older adults, and particularly among those with AMD.
Anxiety is also problematic in older adults with visual impairment, although findings have been somewhat mixed. Aging adults with vision impairment have a much higher prevalence of anxiety disorders in comparison to elderly general population samples, between 7.5–8.6%.33,35 Reported estimates of clinically significant anxiety symptoms range from 8.7–15.6% of visually impaired older adults.33,38,40,45 Additionally, in comparison to elderly adults with other conditions (ie, diabetes, cardiovascular problems), seniors with vision loss endorse a greater number of anxiety symptoms.52 In AMD, elevated levels of anxiety symptoms have been reported in 9.6–30.1% of study samples.44,45 However, other studies have not observed increased rates of anxiety among visually impaired older adults relative to normal-vision peers, after controlling for age, gender, and other potential confounders (eg, health behaviors, life events, etc.).36 Some data indicate the risk for anxiety symptoms may be dependent upon the form of ocular pathology in elderly adults. For example, Eramudugolla et al45 observed a relationship between anxiety symptoms and self-reported cataracts in aging adults, but not other eye diseases (eg, AMD, glaucoma) after controlling for demographic, health, and clinical (eg, treatment, disability) characteristics. Similarly, Augustin et al44 found no association between anxiety symptom severity and visual acuity in patients with AMD after adjusting for demographic variables. Further supporting a weaker relationship with visual disability than in depression, vision loss predicted anxiety cross-sectionally but not longitudinally in a sample of aging adults.34 However, while anxiety may not be as strongly related to vision loss as is depression, it is still a significant symptom for many people, and it may emerge even before significant visual disability becomes evident. It is also important to note that there are additional factors that may contribute to anxiety and that need further study, including loss of visual acuity and reductions in night vision, which can occur in the absence of eye disease.
Other Psychological Problems
An increased risk of suicide has also been documented in visually impaired populations. Suicidal ideation has been linked with vision impairment in elderly adults,53–55 and risk increases with severity of impairment.53 Vision loss has also been identified as an independent risk factor for suicide among aging adults, and its associated risk is greater than that associated with malignant disease and neurological disorders.56 In a general population sample, visual acuity was negatively correlated with suicidal ideation and attempts, and individuals with the poorest acuity were 2–3-times more likely to report suicidal ideation or suicide attempts than were those with near-normal vision, even after adjusting for socioeconomic variables.57 Interestingly, no association between visual acuity and depressive symptoms was observed in this study.57 Notably, an increased risk of suicide has not been reported in all studies. Stensman et al58 reported no association between visual impairment and rates of suicide, and Meyer-Rochow et al59 found elevated rates of suicide only among males with vision loss. In a longitudinal study of adults in the US, individuals with vision impairment were reported to be at elevated risk for suicide after a mean follow-up of 11 years, but completed suicide was not significantly more likely for those with visual impairment as compared to those without, after controlling for other demographic and health factors.60 However, visual impairment was found to significantly increase suicide risk by 18% indirectly, through effects on reported health (eg, quality of health, number of nonocular health conditions).60 Together, these data indicate that vision impairment may heighten risk for suicide, by means of both direct and indirect effects.
Interestingly, visual hallucinations may be quite prevalent among individuals with visual impairment (see Menon et al61 for a review). About 41–59% of patients with visual impairment report experiencing elementary visual hallucinations (eg, colored lights, flashes;61–64). According to reviews, complex visual hallucinations (eg, formed objects/people) are experienced by 5–17.5% of individuals with vision impairment,61,65 and this is referred to as Charles Bonnet Syndrome (CBS). While CBS is most prevalent in older adults with vision impairment, particularly AMD, it has also been reported in children66 and has been linked with sudden vision loss.67 The experience of visual hallucinations among visually impaired populations is sometimes reported to be neutral and non-distressing.61,65 However, an estimated one quarter of patients display anger, anxiety, or mild paranoia as a result of these experiences.61 Depression,68 social isolation,69 and cognitive impairment69,70 have also been reported in association with CBS. Though diagnostically CBS requires that insight regarding hallucinations remain intact, patients may nevertheless become confused by these experiences initially and may react accordingly.61,65 Visual hallucinations may also be under-reported by people with visual impairments for fear of being perceived as clinically unstable or psychotic.61,65 Indeed, CBS is often not recognized by medical providers and can be incorrectly identified as a primary psychiatric disorder.61 Health professionals must be aware of the wide range of symptoms associated with vision impairment.
The Nature of the Relationship Between Vision Impairment and Mental Health
People with vision impairment may experience mental health difficulties for a variety of reasons. Included among these is the emotional distress that is associated with losing one’s sight. Blindness is reported to be one of the most feared health problems; survey data indicate that a greater proportion of individuals fear blindness than fear cancer or paralysis.71 Self-reported reactions to vision loss include anxiety,72 worry,73 frustration,74 social withdrawal,75 and embarrassment.74 Additionally, for individuals with progressive vision loss, substantial fear and anxiety may be experienced in anticipation of further reductions in sight.72 Qualitative data indicate that people with vision loss and blindness may develop negative self-perceptions as a result of societal stigma and experience feelings of loss, similar to bereavement.76 Vision-specific distress (ie, emotional reactions to vision loss) has been identified as a robust predictor of depressive symptom severity,12,77 independent of degree and duration of vision impairment.12 Importantly, while vision-specific distress and depression may be strongly related, they are also distinct in their associated risk factors.77 Thus, distress that is associated with vision loss may be a mechanism by which depression risk is increased in some people with visual impairment.
Vision-specific distress may also account for the association between subjective evaluations of visual function and depressive symptom severity.17,78 In a national sample of adults with vision loss, subjective reports of visual function were predictive of depression even after controlling for demographic, socioeconomic, and health factors, whereas ophthalmologist-measured impairments were not.11 Similarly, among people with newly-diagnosed glaucoma (with acuity of 20/40 or better), perceptions of difficulty with vision-related tasks was associated with depressive symptom severity, but objective measures of visual function (eg, acuity) were not correlated with depression scores.24 In patients with retinitis pigmentosa, Hahm et al16 also observed that subjective evaluations of visual function were lower among those who reported elevated levels of depressive symptoms, as compared to those without significant mood problems. These studies indicate that even the perceived loss of vision may generate significant distress and result in mental health problems.
Depression may also stem from impairments in functioning related to vision loss. As mentioned previously, individuals with vision loss experience a variety of functional limitations,76,79 such as difficulty walking, reading, and driving.80 Older adults with vision impairment report greater difficulty performing activities of daily living (ADLs) than do aging adults with respiratory, cardiovascular, and metabolic conditions.52 Moreover, research indicates that people with subjective and objective difficulties performing necessary ADLs are at elevated risk for depression.81–84 Qualitative interviews indicate that individuals with visual impairments may experience negative emotions when they are no longer able to engage in work or meaningful activities that are central to their identity.74 While both vision impairment and depression are independently associated with functional decline, together these conditions may result in even greater disability than either condition alone. For example, Bookwala and Lawson85 found that poorer self-reported visual function predicted greater depression in a sample of aging adults; however, a significant indirect effect of vision impairment on depressive symptom severity was also observed, via increased functional limitations and social isolation. In another study, older adults with both vision loss and depression reported greater difficulty performing a number of ADLs as compared to those with either condition alone.86 Thus, for some individuals with vision impairment, the development of mood problems may be a consequence of functional impairment.
Age is another factor that may contribute towards an increased risk for mental health problems in people with visual impairment. As stated above, rates of visual impairment increase substantially with age,26 and 6.6% of adults over 65 are visually impaired in the US.87 Depressive symptoms are commonly experienced by aging adults in the general population, and often go untreated.88 Furthermore, factors associated with the onset of depression later in life include functional impairment and poor health.89,90 Therefore, age may be a confounding variable in the high prevalence of depression in people with visual impairments. However, in a population-based study of older adults with vision loss, younger age was identified as a significant predictor of depressive symptoms, after controlling for additional health factors,78 suggesting that individuals with vision impairment may be at heightened risk for mental health problems in the transition into later adulthood, possibly because of negative expectations about the future. Depression risk may also depend on type and severity of visual impairment, as shown in a 10-year follow-up study of people aged 65 and older. Older adults with a recent decline in distance visual function were at a 3-fold risk of developing depressive symptoms over the follow-up period. Conversely, older adults reporting depressive symptoms at baseline had a 62% increased likelihood of having visual function loss after 10 years, even after controlling for sociodemographic variables, medical comorbidity, cognitive impairment, antidepressant use, and past depressive episodes.91 These data demonstrate that multiple variables, including pre-vision loss tendencies towards depression, attitudes and expectations about aging, age-related vision loss, and age and severity of vision loss may contribute to increases in depression in older adults.
Individuals with vision impairment may also experience distress with regards to treatment. For example, injections, directly into the eye, of vascular endothelial growth factor inhibitors (anti-VEGF) are an available treatment for people with neovascular (ie, wet) AMD.92 Anti-VEGF treatment may be perceived as stressful due to anticipatory anxiety about pain or discomfort.93 However, one study observed that 56% of patients with neovascular AMD had anxiety regarding anti-VEGF treatment, but only 3.3% of patients reported anxiety related to injection pain; rather most patients reported concern regarding potential complications and treatment efficacy.94 Additionally, anxiety surrounding anti-VEGF treatment did not change with the number of injections received, indicating that these symptoms may be somewhat enduring.94 Treatment providers must be aware that visually impaired populations may experience anxiety concerning their health, healthcare, and treatment options.
Overall, the relationship between mental health and vision impairment may be bidirectional (see Figure 1).11 For instance, depression might elevate risk for ocular disease through a number of poor health behaviors, such as an unhealthy diet, tobacco and other substance use, and treatment non-compliance.42,95,96 Antidepressant medications may also have ocular effects. Both tricyclic antidepressants and selective serotonin reuptake inhibitors (SSRIs) have been associated with an increased risk for mydriasis (pupil dilation) which in turn increases the risk of angle-closure glaucoma.97 Additionally, known neurotransmitter dysfunction (eg, dopamine, GABA) in the brain in people with depression may have implications for the visual system overall, including for ocular function (eg, reduced retinal sensitivity98,99) and visual processing (eg, reduced contrast sensitivity100,101). However, while at times mental health problems may be an antecedent to vision loss, the literature reviewed above indicates that often mental health problems are a consequence of vision impairment. Distress and functional impairment that are associated with vision loss may elicit a variety of psychological problems, and, in particular, affect one’s mood.85,86,102 As noted above, knowing that one has a disorder of vision can have psychological consequences, even in the absence of obvious visual impairment. Furthermore, among visually impaired and visually disabled individuals, depression and anxiety may be worsened as a result of social isolation or an inability to work.74,85 However, the effects of each of these factors may be intertwined. In a study of adults with vision loss, reduced activity participation due to vision impairment was related to depression, however, vision-specific distress was identified as a mediator of this effect.12 The relationship between age, mental health, and vision loss also appears to be bidirectional. In a longitudinal study of older adults, Frank et al34 found that self-reported vision status was a significant predictor of future depression, whereas baseline depression and anxiety were associated with future self-reported vision impairment, even after adjusting for sociodemographic and other health characteristics. Thus, more longitudinal studies are needed, in individuals across the lifespan, in order to clarify the direct and indirect effects of vision impairment on mental health.
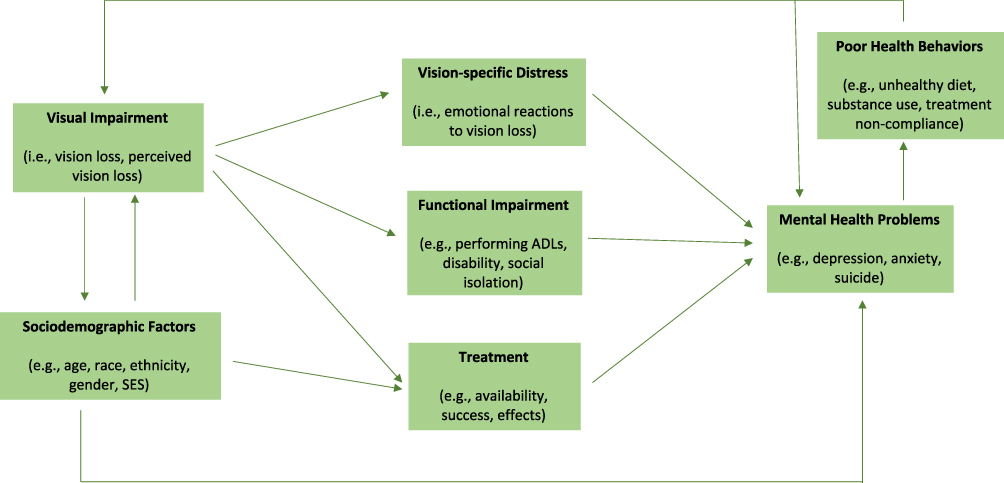 |
Figure 1 Bidirectional interaction between visual impairment and mental health problems. |
Socioeconomic and Demographic Considerations
Low socioeconomic status is a risk factor for vision impairment (see103 for review). Globally, low vision has been associated with economic disadvantage.104,105 Rates of visual impairment are higher in low income countries as compared to high income countries, and the prevalence of blindness has been inversely correlated with nations’ gross domestic product (GDP).105 Across many nations, visual impairment has been linked with household income,106 and people living in impoverished neighborhoods have been reported to be at increased risk of vision impairment or blindness.107–111 A relationship between visual impairment and education has also been widely observed, where lower education attainment is associated with higher rates of visual impairment.106,112,113 For example, a study in the US reported that rates of visual impairment were highest among individuals who did not graduate from high school.114 In addition, social class may be a factor in visual impairment risk. Among middle-aged working adults in England, the prevalence of vision impairment was reported to be 1.9% among professionals (Class I) and 5% among unskilled manual workers (Class V), and risk for visual impairment increased by 28% with each descent in social grade.115 Individuals with lower socioeconomic position are more likely than those of higher socioeconomic position to develop vision impairment, in both developed and developing nations.109,111,112,116 Furthermore, in a British longitudinal birth cohort study an association between low socioeconomic position in childhood and earlier adulthood and risk for visual impairment in mid-adulthood was observed.115 Results from an annual household survey administered to nearly 70,000 adults in the US over a 3-year period indicated that lower levels of education and household income were associated with vision impairment, even after adjusting for demographic characteristics, health behaviors (eg, smoking), health conditions (eg, diabetes, hypertension), and healthcare access (eg, medical insurance).114 However, another study found that substance use mediated the relationship between low socioeconomic status and vision impairment.117 Nevertheless, together these data indicate that socioeconomic disadvantage increases the likelihood of vision impairment, directly and/or indirectly.
Certain demographic variables have also been linked with heightened risk of vision impairment.103 Some data indicate that race and ethnicity are not related to the prevalence of visual impairments, after controlling for age, socioeconomic variables, and refractive error.118 However, in a study of visual impairment in a Latino/Hispanic population, the prevalence of vision impairment was much higher than rates reported in non-Hispanic White samples and other population-based studies in the US.119 Additionally, in a study of older adults with vision loss, non-White ethnicity was associated with a greater risk for depression, even after controlling for age, gender, and health.120 Data also indicate that African-Americans experience the highest prevalence of visual impairment,27 and may be at especially high risk for conditions such as open-angle glaucoma.121 Still, it is uncertain whether an increased prevalence of vision impairment in certain racial or ethnic groups might be a function of low socioeconomic status and/or marginalization, particularly as these variables are not always controlled for (eg, Rahi et al115). Gender is another factor that has been associated with visual impairment risk.122,123 According to recent estimates, the prevalence of vision impairment in women is 1.3-times that of men.27 One potential explanation for the relationship between vision loss and gender is that the average lifespan of women is longer than that of men, and as rates of vision impairment increase significantly with age it might be expected that women would experience a higher prevalence of visual impairment and eye disease.123,124 Nonetheless, even after controlling for age, higher rates of vision impairment in women have been observed.125 Other studies, however, report that rates of vision loss are fairly equal among men and women after age adjustments.26 Importantly, among older adults with vision loss, female gender has been identified as a unique predictor of subthreshold depression, after adjusting for age, psychiatric history, and health status.126 These data are consistent with findings of higher rates of depression and anxiety among women as compared to men in the general population (potentially resulting from gender (eg, symptom manifestation) and sex differences (eg, hormonal effects, genetic predisposition)127,128); and suggests that women with vision impairment may be at increased risk for developing mental health problems. Thus, the risk for visual impairment and related outcomes may be influenced by demographic characteristics, such as ethnicity and gender.
Health Inequity as a Result of Socioeconomic Disadvantage in Visually Impaired Populations
In visually impaired populations a number of individual and societal factors may interact to restrict access to services. Both physical and mental healthcare may be limited by financial barriers.129,130 For example, in one study of older adults with visual impairment, those who reported severe levels of depressive symptoms had less education, lower income, and were more likely to be a racial or ethnic minority,42 and these populations may have less access to quality eye care and lower quality health insurance. Relatedly, many mental health providers may not offer a sliding scale or accept Medicare/Medicaid insurance.129 As an example, among AMD patients, depression scores were significantly improved in older adults who received four to 12 anti-VEGF treatments as compared to those who received three or less injections.94 However, these treatments can be quite costly, and so the full course of treatment may not be accessible to a portion of individuals with AMD. As another example, cataract surgery is a cost-effective intervention131 and has been shown to ameliorate hallucinations and depression among people with vision impairment.61,132 Nevertheless, these vision problems may remain untreated in many individuals with visual impairment, as many people of low socioeconomic status are less likely to receive even basic eye care services (eg, spectacle coverage).107 Therefore, people with vision impairment, many of whom are socioeconomically disadvantaged, may encounter a variety of obstacles to accessing adequate healthcare, and this can contribute to both poorer vision and mental health outcomes.
Part II: Mental Health Assessment and Treatment in People Visual Impairment
Although data demonstrate an elevated prevalence of mental health issues in people with visual impairments, these problems remain largely untreated.39,133 For example, a high prevalence of clinically significant anxiety and depression are reported by individuals with AMD, yet studies indicate that up to 91% are not receiving treatment for these mental health issues.94 Similarly, in a large sample of visually impaired older adults, 34% who met criteria for a mood or anxiety disorder reported not receiving any mental health services over the previous 6 months.35 Most strikingly, in a study of 143 adults with vision impairment, 14.7% qualified as moderately depressed and 27.3% met the cut-off for mild depression, however, only 12% of the study sample was prescribed antidepressant medication and none were currently receiving any counseling or mental health support.12 Treatment of mental health problems in visually impaired populations may be lacking for numerous reasons, but one issue may be the tendency of both patients and providers to focus on the physical aspects of vision loss, or the need to re-learn practical skills, rather than the psychological and emotional impact,133 perhaps based on the misguided assumption that mood will necessarily improve after new skills are learned. Another contributor to lack of mental health treatment is that people who experience vision loss may be more inclined to rely on personal resources (ie, to attempt to maintain their independence), rather than to seek help.35,134 Additionally, a shortage of knowledgeable mental health providers with training or experience in treating individuals with vision impairment may create a barrier to receiving services. In a survey that assessed a range of disabilities, mental health clinicians rated visual impairment as one of the most difficult populations to serve for reasons such as a lack of funding, accessibility, and expertise.129 Lack of integrated care (eg, lack of mental health screening, and the presence of mental health professionals co-located at ophthalmology clinics) also contributes to suboptimal identification and treatment of mental health issues among people with eye conditions. Finally, although antidepressants have been associated with improvements in both depressive symptom severity and visual function in people with AMD, some people may be disinclined to take psychotropic medication for a number of reasons (eg, side-effects, drug interactions, etc.).42 Additionally, antidepressant medications may be less effective for those with milder or treatment-resistant depression.135 Therefore, effective psychological interventions that can be widely disseminated are needed in order to address the mental health concerns of people with vision impairment.
Below, we review current approaches to treating mental health problems in people with vision impairment. To identify articles to include in this review a literature search was conducted. Selection criteria included peer-reviewed studies of interventions aimed at improving mental health (ie, psychological well-being) in people with visual impairment. Electronic databases (eg, PubMed; Google Scholar) were searched using combinations of these keywords: “vision impairment”, “visual impairment”, “treatment”, “intervention”, “mental health”, “depression”, and “anxiety”, and reference lists of the identified studies were examined for potentially relevant articles. As the overarching goal of this review is to promote a greater understanding of the mental health needs of people with vision impairment, an exhaustive review of the treatment literature is not presented here. Rather, only those articles which were determined to be most representative and informative of the current status of behavioral treatments were included in the review.
Self-Management Interventions
Early approaches to improving mental health in people with vision impairment focused on self-management techniques. Self-management interventions have been found to be effective in improving a range of health outcomes among individuals with chronic conditions, including asthma, arthritis, and diabetes.136 Individuals learn to monitor their condition (ie, disease progression), and to manage any physical and psychosocial consequences that may have an impact on their quality-of-life.136 Several studies have investigated the outcomes of self-management interventions delivered in group format to individuals with AMD.137 In these studies, self-management was significantly more effective than were control conditions at reducing psychological distress and improving self-efficacy and functioning in patients with AMD.137,138 Furthermore, these effects were sustained up to six months after intervention end.139,140 Self-management has also been shown to bolster the effects of usual care in people with age-related vision loss. In one study, self-management combined with usual care led to greater participation in life situations and adaptation to vision loss, fewer depressive symptoms, better physical and mental quality-of-life, and increased self-efficacy in comparison to usual care alone, and many of these effects were maintained up to 12-weeks post-treatment.141 However, these positive outcomes were not replicated in a sample of older adults with a broader range of eye conditions (ie, a less specific disease-related focus) and fewer baseline psychological symptoms.142 Thus, self-management approaches may be most beneficial for individuals who are experiencing significant psychological distress, and perhaps who can identify a specific cause of their visual changes (Table 1).
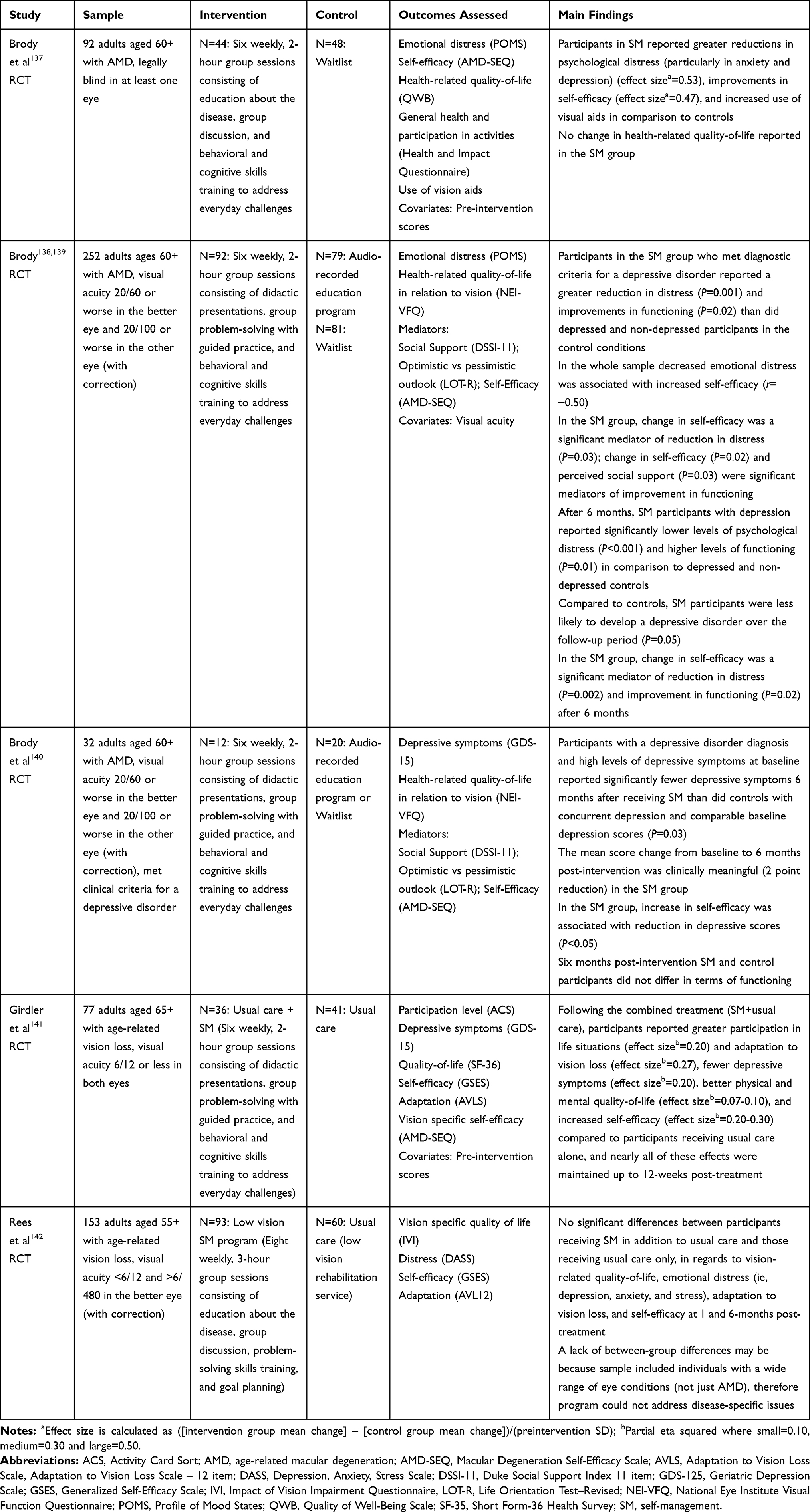 |
Table 1 Self-Management (SM) Interventions |
Problem-Solving Interventions
Problem-solving treatment (PST) may also be beneficial for individuals with vision impairment. PST is a manualized intervention that involves learning skills such as how to define problems, establish realistic goals, generate, choose, and implement solutions, and, finally, evaluate outcomes.143,144 PST is a brief intervention that can be delivered by non-specialists (ie, general practitioners, nurses) and thus has applicability for primary care settings.143,145 Randomized controlled trials in general psychiatric samples indicate that PST is equally as effective as antidepressant medication alone, and the combination of PST and antidepressant medication in managing depressive symptoms.146 In a randomized control trial comparing the effects of PST to usual care, PST was more effective in preventing depression in older adults with AMD after two months, but the difference between the interventions was no longer significant after six months.144,147 Thus, PST may delay the onset of depression in people with AMD, however, additional sessions or booster treatments may be necessary in order to prevent the emergence of depression as time goes on and the condition worsens.144,147 Additionally, another study found that 6–8 sessions of PST delivered to older adults with vision loss and significant (ie, moderate-to-severe) depressive symptoms led to a reduction in depressive symptom scores, but the change was not clinically significant.120 Nevertheless, PST may offer several advantages over other treatment approaches. For example, in many cases PST is delivered by Master’s or Bachelor’s level clinicians or nurses (eg,48,102,144), thereby expanding patient access to treatment. More recently, PST was delivered to individuals with vision impairment and significant depressive symptoms via phone (ie, telehealth).148 After three months, participants reported significant improvement in depressive symptom severity, health-related quality-of-life, and confidence in using problem-focused coping skills.148 Additionally, one mechanism by which PST may be effective is by encouraging continuation of valued activities.144 This is an important aspect of treatment given the association between functional decline and depression in people with vision loss.36,42,102 In comparison to supportive therapy, PST demonstrated similar outcomes in terms of activity engagement, self-reported visual function, physical health status, and depressive symptom severity in people with AMD. However, PST has led to greater improvements in vision-related quality-of-life and increased use of adaptive coping strategies at 3- and 6-months post-treatment.149 Notably, while PST and supportive therapy are similar, PST is unique in its incorporation of problem-solving skills training. Thus, learning effective methods for solving problems may be especially beneficial for people with vision loss (Table 2).
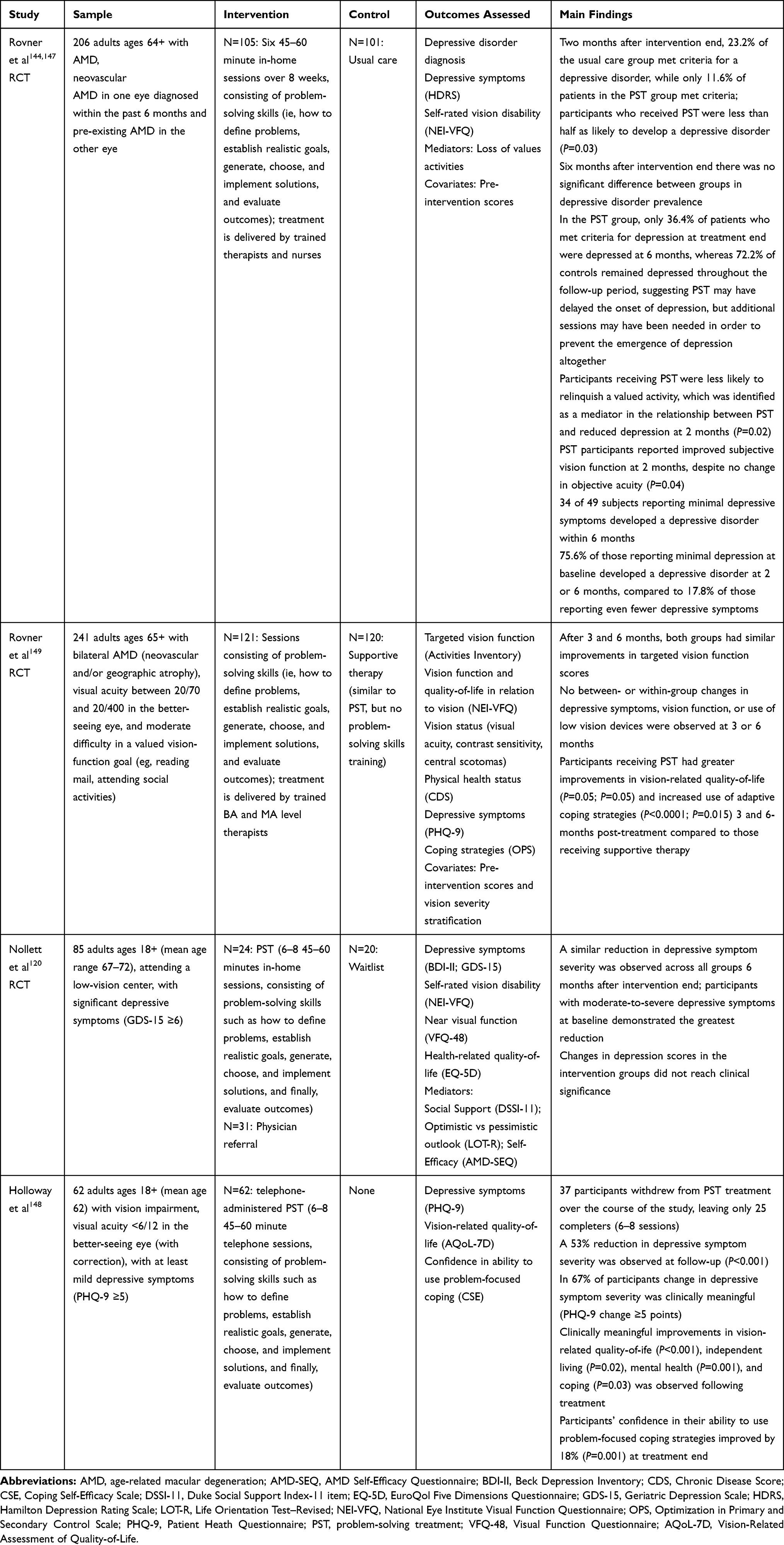 |
Table 2 Problem-Solving Treatment (PST) |
Vision Rehabilitation
Another behavioral intervention that may hold promise for improving psychiatric symptoms in visually impaired populations is vision rehabilitation. These programs typically involve a combination of low vision clinical services (eg, prescription of adaptive devices and instruction on use), rehabilitation training (eg, skills of daily living), orientation and mobility training (eg, safe travel procedures), and counseling and support groups to help with adaptation to disability and improve quality-of-life.150 The primary aim of vision rehabilitation programs is to maintain or improve an individual’s current level of functioning. However, by promoting self-efficacy, vision rehabilitation may also lessen depression risk in people with visual impairment.151 Importantly, studies have found that specific treatment components of low vision clinical services, counseling, and the use of optical devices were associated with significant change in depression scores, whereas skills training and the use of adaptive devices were not.151,152 Despite these findings, counseling services are typically only offered as a supplement to functional rehabilitation, and, in one study, were received by as few as 16% of participants.151 Thus, while targeting visual functioning may also have an impact on psychological functioning in elderly adults with vision loss, directly addressing the emotional aspects of vision loss is a necessary part of treatment that may lead to more robust improvements in mental health (Table 3).
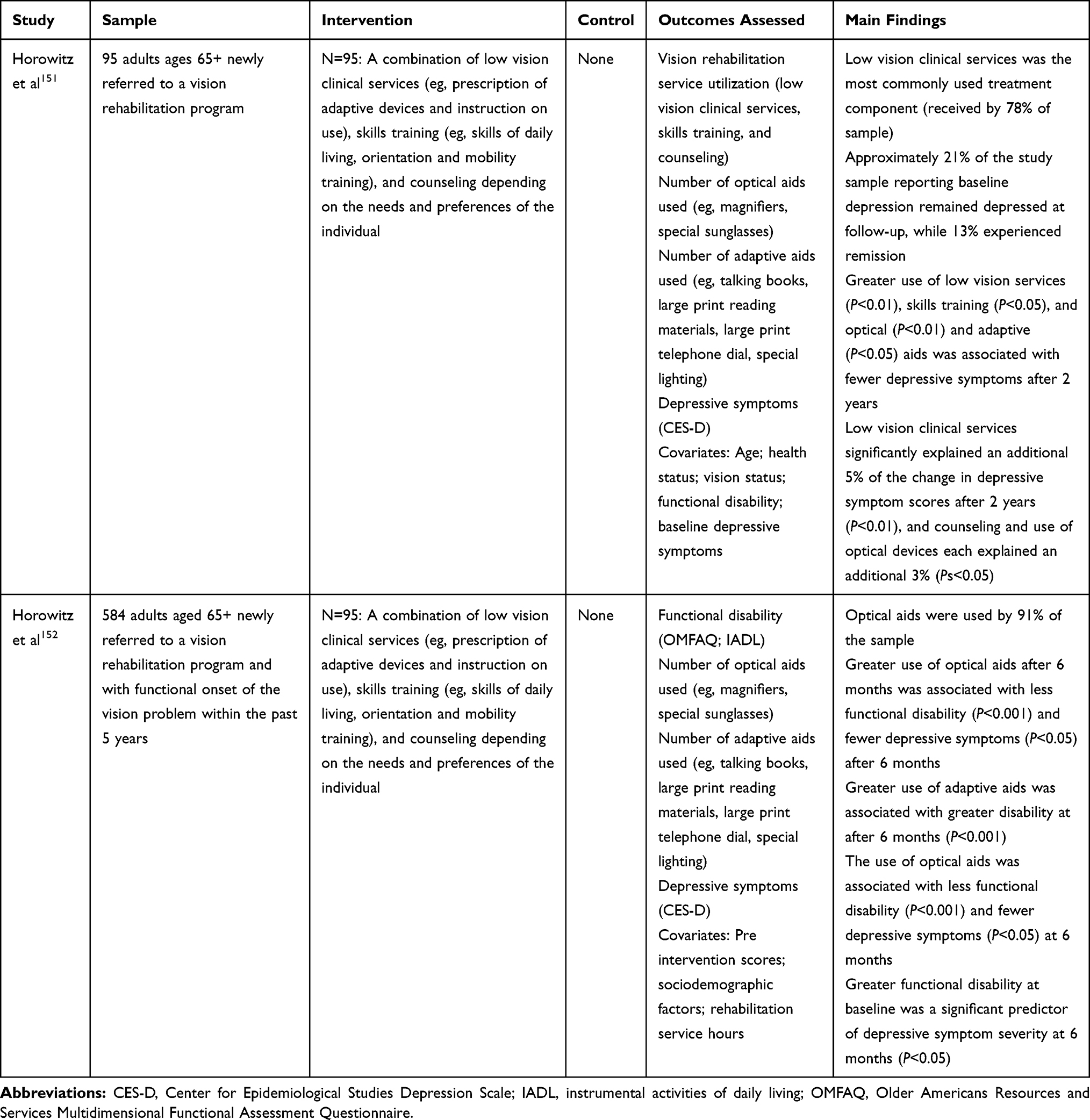 |
Table 3 Vision Rehabilitation Interventions |
Cognitive Behavioral Interventions
Among individuals with AMD, modified cognitive-behavioral interventions have been used to improve depression and anxiety symptoms, with some success. In one study, a single component of cognitive behavioral treatment, behavioral activation, in conjunction with low vision rehabilitation was significantly more effective in preventing depression in patients with AMD compared with supportive therapy combined with low vision rehabilitation.153 A follow-up mediation analysis demonstrated that improvement in depression scores following behavioral activation and low vision rehabilitation was explained by an increase in social engagement.153 Self-guided CBT has also led to a significantly greater reduction in depressive symptoms among patients with AMD relative to usual care, although improvements in other outcomes, including anxiety and self-efficacy, were not observed.154 Cognitive and behavioral approaches have also been tested in other visually impaired populations, such as people with blindness. In one study, individuals with blindness receiving Rational Emotive Behavior Therapy (REBT), a type of cognitive therapy, reported significant reductions in irrational beliefs, depression, anxiety, and stress and improvements in self-esteem, while these same changes were not observed in the control group.113 Moreover, these mental health effects were maintained in the REBT group up to 1-month post-treatment.113 Together, these findings suggest that cognitive behavioral interventions may be effective in improving psychological functioning of adults with varying degrees of vision loss (Table 4).
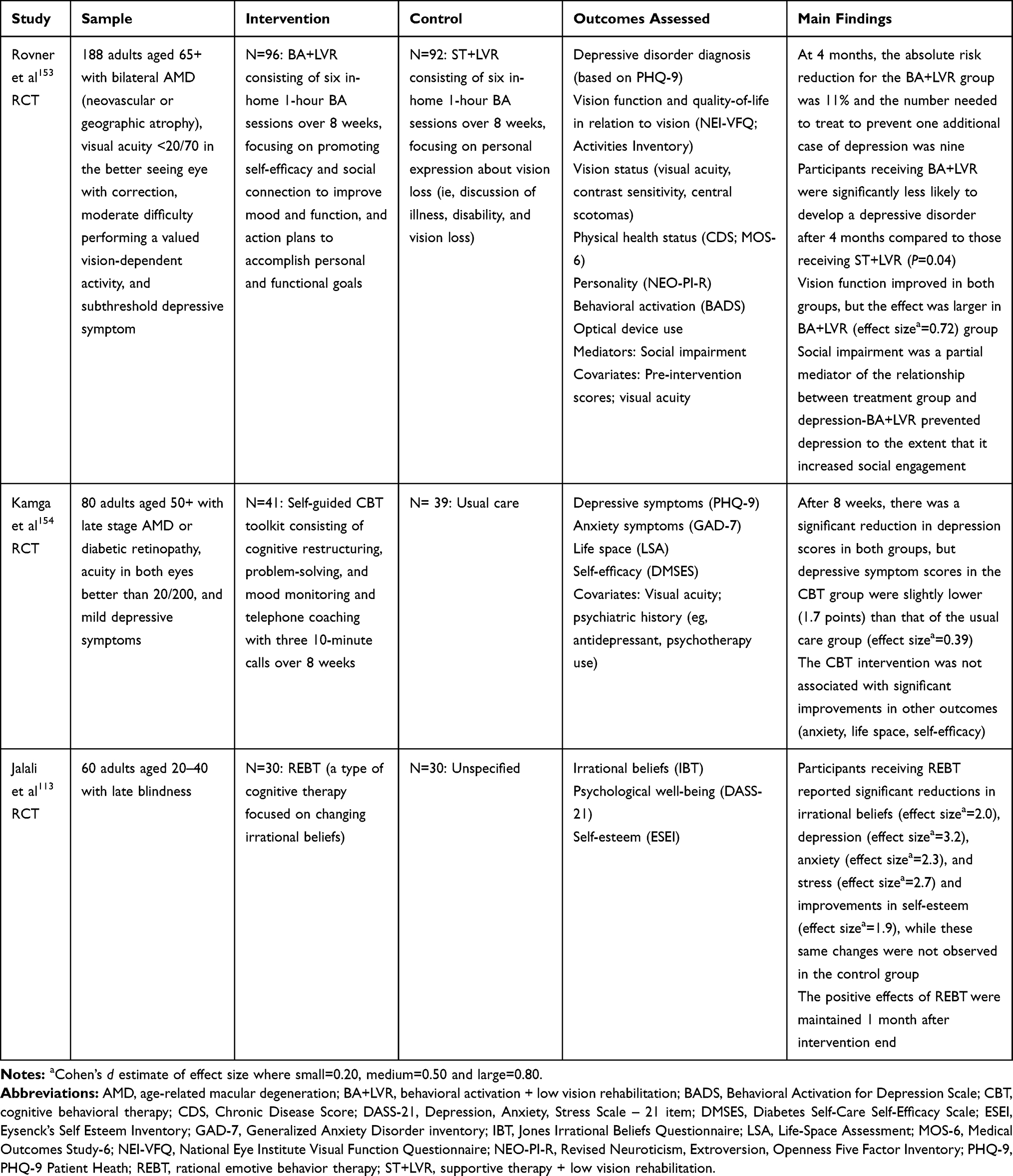 |
Table 4 Cognitive Behavioral Therapy (CBT) Interventions |
Stepped Care Interventions
In the last decade, stepped care has been a recommended approach to treating individuals with mild-to-moderate levels of depression and anxiety.155 Stepped care has also demonstrated success in reducing the incidence of depressive and anxiety disorders among older adults in the general population who experience subthreshold symptoms.156 Stepped care increases efficiency of behavioral health care delivery by initially providing patients with the least intensive interventions and then moving to more intensive services as required (ie, if symptoms remain near baseline levels).157 In a multi-site randomized control trial, van der Aa et al157 tested the effectiveness of stepped care in ameliorating depression and anxiety in older adults with vision loss. Compared to individuals receiving usual care, those in the stepped care group reported significantly greater improvements in depressive and anxiety symptoms and vision-related quality-of-life at treatment end.157 Older adults receiving stepped care were also less likely than controls to develop depressive or anxiety disorder over a 2-year follow-up period. However, 25–30% of elderly patients in the stepped care group that qualified for guided self-help or PST were either non-compliant or not fully adherent to treatment protocols and reported finding these steps to be unnecessary or too burdensome.157 Additionally, a considerable number (~30%) of older adults receiving stepped care developed depression, though half of these individuals reported a history of depressive or anxiety disorders.157 Thus, while stepped care may be effective in preventing the onset of mental health problems in older adults with vision impairment, it may be less effective in preventing the recurrence of depression in those with preexisting or past symptoms. As anxiety and depression are relatively common in the population at large, and may be especially prevalent among individuals with vision impairment (reviewed above), this signifies a significant limitation of this approach, although it is a limitation shared with many other interventions for many other health conditions. Nevertheless, stepped care has demonstrated superiority to usual care in terms of cost-effectiveness.158 Therefore, stepped care models may offer some advantage over traditional approaches in targeting mental health problems in older adults with vision impairment (Table 5).
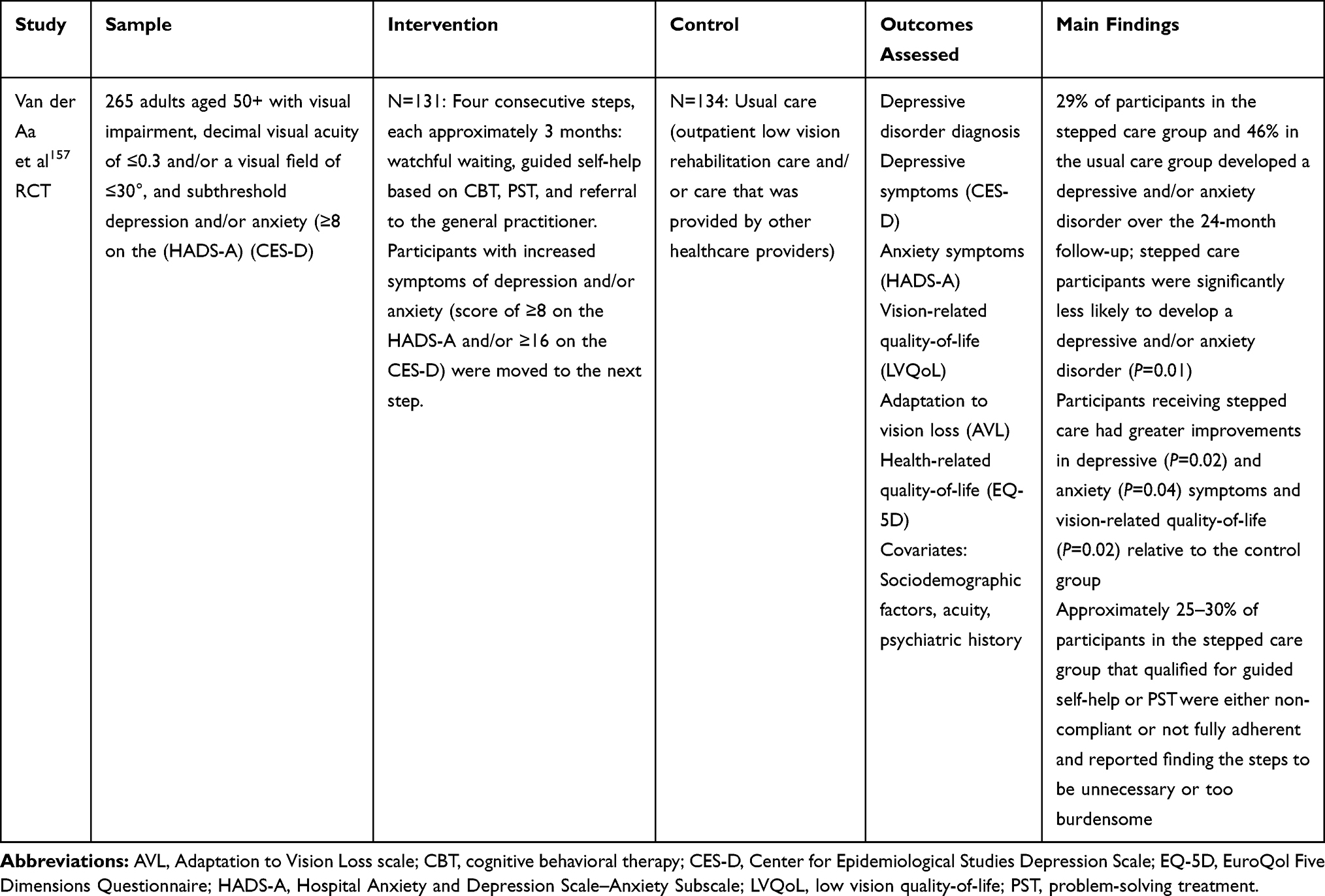 |
Table 5 Stepped Care Interventions |
Additional Considerations
Although studies of behavioral interventions for the prevention and treatment of mental health problems in people with vision impairment have reported some positive results, these treatments are lacking in several ways. Many of these interventions are focused almost exclusively on improving functionality through skills training.144,151 Though functional impairment has been linked to depressive symptoms in individuals with vision impairment,36,102 vision-specific distress has also been identified as an important contributor to depression in this population.12 Therefore, more targeted interventions for psychological and emotional difficulties associated with vision loss may be needed. Indeed, Wahl et al159 compared the effects of an emotion-focused treatment with a problem-focused approach in patients with AMD and found that, while problem-solving therapy was associated with an increase in active problem orientation and adaptation to vision loss, only those in the emotion-focused therapy group experienced a significant decrease in depressive symptoms (though the effect size was small). Additionally, many current treatments for mental health problems in people with vision impairment are severely limited in their effectiveness. Findings from a meta-analysis indicate that, overall, psychosocial interventions have a small significant effect on improving depression in people with vision impairment, and this effect is linked with age, whereby lower age was associated with better outcomes.160 However, after removing a study outlier with a small sample size, younger age of participants, and shorter follow-up period, the effect of the included interventions on depressive symptoms was no longer significant.160 Similarly negligible results were obtained for anxiety symptoms, with psychosocial interventions leading to a medium-sized reduction in anxiety symptoms in comparison to control conditions, without statistical significance.160 Likewise, the assessed psychosocial interventions did not appear to have a significant impact on psychological stress or well-being, but again a relationship was observed between younger age and better outcomes.160 Outcomes of these interventions may also depend largely on the age of the individual. While prior studies of psychosocial interventions demonstrate some degree of efficacy in older adults with vision loss, and particularly AMD,161 meta-analytic findings indicate that improvements are less robust in elderly samples.160 Related to this finding, risk and protective factors for mental health problems in older adults may be different from those of younger people,29 and therefore treatment may need to be adapted to fit the individual needs of the consumer.160 One issue relevant to this point is that with increasing age there is more likely to be failure of other bodily systems, and other situations (eg, loss of a spouse) that promote depression. Therefore, interventions that are associated with a significant reduction in depression in younger patients may appear to have reduced benefit in older patients, even if the absolute level of change is the same in both populations (owing to increased baseline depression levels in the latter group). Finally, the relatively high rates of treatment non-adherence and attrition reported in some studies41,137,148 is problematic and limits the interpretation of results, especially their generalizability. In short, overall, there is evidence of mild-to-moderate effects of existing approaches for treating mental health problems in people with visual impairment broadly. Further efforts are needed to develop novel interventions that can be applied to a wider range of individuals with vision impairment, and to develop interventions for people with more severe depression and/or who are nonadherent with recommended treatment.
Improving Mental Health Treatment in People with Vision Impairment
Vision loss affects all aspects of one’s life. The findings reviewed indicate that mental health problems are a significant burden for many people with vision impairment.,9–11 However, despite the widespread prevalence of these issues, screening and treatment remain inadequate. Better outcomes may be achieved if several changes are made. First, more rigorous evaluation of current treatment approaches is warranted. In addition to measuring long-term outcomes, treatment efficacy needs to be tested in a broader sample of people with vision impairment, including children and individuals with complete blindness. More work is also needed to identify mechanisms of change (eg, reductions in vision-specific distress,12 maintaining valued activities,144 recovery of self-esteem, increased hope for the future, etc.).162 Related to this, in addition to screening for level of issues such as depression and anxiety, screening should adequately capture the patient’s stage of emotional adjustment to vision loss162 so that the treatment approach matches the patient’s perspective on his/her condition. In addition to targeting mental health problems, it is critical to focus on poor adherence, especially for people who could be receiving an effective intervention. Dismantling studies are also needed to identify important treatment components, as was done in a study of AMD when the effects of a single cognitive-behavioral component, behavioral activation, was examined in combination with vision rehabilitation, and results were positive.153 Additionally, client characteristics that may influence treatment outcomes, such as age,89,90,120 severity and duration of vision loss,19,20,22,24 and prognosis of the disease18,94 need to be recognized. It is also important that these factors, and other potentially confounding variables (eg, functioning, social support, psychiatric history, family history of eye disease), are controlled for in studies of treatment effectiveness. Finally, at least some subpopulations (eg, AMD patients with low income and with psychological denial of disability) may require a greater focus on issues that interfere with treatment adherence, as poor adherence may affect outcomes more than the disease in cases where effective treatments are available.
In order to improve access to care, structural changes may be required. This may include integrating services, such as behavioral health and ophthalmology, or even general healthcare given high rates of medical comorbidity in this population.31,86 Relatedly, routine screening for mental health problems in eye care settings may be beneficial, and has high acceptability among patients (ie, considered a “good idea”).39 A discussion between patients and their providers regarding the relationship between visual impairment and mental health, and factors that may increase risk for mental health problems, may improve access and engagement in mental health services. Furthermore, providing information and educating patients and their families on the potential effects of vision loss on functioning over time may facilitate the development of self-supportive strategies that allow patients to better manage future challenges. An expansion of current treatment options is also needed in order to serve a wider range of individuals with vision loss. Though data are limited, there is some evidence that peer support groups for people with vision impairment have positive effects on mental health,163 and in qualitative studies patients report benefiting from their peers in a multitude of ways (eg, providing role models of success, allowing comparison with those more unfortunate).164 In addition, delivering therapy by phone148 or through mobile applications may increase treatment accessibility, particularly among individuals with mild or moderate symptom levels that may be undetected by general health providers. Further introduction of established mental health interventions to visually impaired populations is also essential, especially regarding treatments that have demonstrated efficacy in general depression populations, as mood symptoms may be especially problematic in people with vision impairment.9,11 For instance, acceptance and commitment therapy (ACT) is a “third wave” form of cognitive therapy that encourages acceptance of events (vs experiential avoidance) and behavior change that is guided by goals and values, and has demonstrated superiority over other treatments in improving depression, anxiety, and other mental health problems among people with physical health conditions,165 such as chronic pain.166 In older adults with vision impairment, a relationship between lower acceptance of vision loss and subthreshold depression has been reported126 and avoidant coping has been identified as a unique predictor of both vision-specific distress and depressive symptoms.77 Thus, an intervention aimed at enhancing psychological adjustment and coping, such as ACT, may have a positive effect in people with vision loss. In summary, implementing a variety of changes to improve the detection and treatment of mental health problems in people with vision impairment may lessen health inequity and improve outcomes in this population.
Summary and Conclusions
Vision impairment has a substantial personal and global impact.4,5,31 Besides high rates of physical comorbidity, people with visual impairments are at risk for poor mental health outcomes.9–11 Importantly, approximately 68% of vision impairment is avoidable.167 While blindness as a result of age-related disease (eg, AMD, diabetic retinopathy, glaucoma) is not reversible at this point, many impairments can be corrected or altogether avoided131 with better attention to eye health, and doing so should prevent development of some mental health problems. However, better screening for mental health changes and greater availability of effective treatments, and of adequately trained (with regard to understand the psychological consequences of vision loss) mental health professionals, are necessary as well. It is also critical to increase our understanding of the range of psychological and psychosocial effects associated with visual disability (and anticipation of it) and the mechanisms that contribute to the onset and maintenance of mental health problems in this population. While it is important to address both the emotional and practical needs of people with visual impairment, historically, mental health concerns have been largely overlooked in these individuals. Proper attention to mental health issues is likely to be a complex endeavor, however, as it requires widespread screening, careful attention to the patient’s stage of emotional adjustment to living with vision loss, development of novel interventions, availability of trained practitioners, and addressing health disparities related to socio-economic status.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Report on Vision. World Health Organization; 2019.
2. Bourne RRA, Flaxman SR, Braithwaite T, et al. Magnitude, temporal trends, and projections of the global prevalence of blindness and distance and near vision impairment: a systematic review and meta-analysis. Lancet Global Health. 2017;5(9):e888–e897. doi:10.1016/S2214-109X(17)30293-0
3. Pelletier AL, Rojas-Roldan L, Coffin J. Vision Loss in Older Adults. Am Fam Physician. 2016;94(3):219–226.
4. Gordois A, Cutler H, Pezzullo L, et al. An estimation of the worldwide economic and health burden of visual impairment. Glob Public Health. 2012;7(5):465–481. doi:10.1080/17441692.2011.634815
5. Khorrami-Nejad M, Sarabandi A, Akbari M-R, Askarizadeh F. The impact of visual impairment on quality of life. Med Hypothesis Discov Innov Ophthalmol. 2016;5(3):96–103.
6. Dhital A, Pey T, Stanford MR. Visual loss and falls: a review. Eye. 2010;24(9):1437–1446. doi:10.1038/eye.2010.60
7. Brunes A, Hansen B, Heir T. Loneliness among adults with visual impairment: prevalence, associated factors, and relationship to life satisfaction. Health Qual Life Outcomes. 2019;17(1). doi:10.1186/s12955-019-1096-y
8. Nyman SR, Gosney MA, Victor CR. Psychosocial impact of visual impairment in working-age adults. Br J Ophthalmol. 2010;94(11):1427–1431. doi:10.1136/bjo.2009.164814
9. Choi HG, Lee MJ, Lee S-M. Visual impairment and risk of depression: A longitudinal follow-up study using a national sample cohort. Sci Rep. 2018;8:1. doi:10.1038/s41598-018-20374-5
10. Mayro EL, Murchison AP, Hark LA, et al. Prevalence of depressive symptoms and associated factors in an urban, ophthalmic population. Eur J Ophthalmol. 2020:112067212090170. doi:10.1177/1120672120901701.
11. Zhang X, Bullard KM, Cotch MF, et al. Association between depression and functional vision loss in persons 20 years of age or older in the United States, NHANES 2005-2008. JAMA Ophthalmol. 2013;131(5):573. doi:10.1001/jamaophthalmol.2013.2597
12. Rees G, Tee HW, Marella M, Fenwick E, Dirani M, Lamoureux EL. Vision-specific distress and depressive symptoms in people with vision impairment. Invest Opthalmol Visual Sci. 2010;51(6):2891. doi:10.1167/iovs.09-5080
13. Li W, Zhong B, Liu X, et al. Depressive symptoms among the visually disabled in Wuhan: an epidemiological survey. Shanghai Arch Psychiatry. 2013;25(5):306–313. doi:10.3969/j.issn.1002-0829.2013.05.006
14. Stevelink SAM, Fear NT. Psychosocial impact of visual impairment and coping strategies in female ex-Service personnel. J R Army Med Corps. 2016;162(2):129–133. doi:10.1136/jramc-2015-000518
15. Schuster AK, Tesarz J, Rezapour J, Beutel ME, Bertram B, Pfeiffer N. Visual impairment is associated with depressive symptoms—results from the Nationwide German DEGS1 study. Front Psychiatry. 2018;9. doi:10.3389/fpsyt.2018.00114
16. Hahm B-J, Shin Y-W, Shim E-J, et al. Depression and the vision-related quality of life in patients with retinitis pigmentosa. Br J Ophthalmol. 2008;92(5):650–654. doi:10.1136/bjo.2007.127092
17. Qian Y, Glaser T, Esterberg E, Acharya NR. Depression and visual functioning in patients with ocular inflammatory disease. Am J Ophthalmol. 2012;153(2):370–378.e2. doi:10.1016/j.ajo.2011.06.028
18. Cumurcu T, Cumurcu BE, Celikel FC, Etikan I. Depression and anxiety in patients with pseudoexfoliative glaucoma. Gen Hosp Psychiatry. 2006;28(6):509–515. doi:10.1016/j.genhosppsych.2006.09.004
19. Kong X, Yan M, Sun X, Xiao Z. Anxiety and depression are more prevalent in primary angle closure glaucoma than in primary open-angle glaucoma. J Glaucoma. 2015;24(5):e57–e63. doi:10.1097/IJG.0000000000000025
20. Koenes SG, Karshmer JF. Depression: a comparison study between blind and sighted adolescents. Issues Ment Health Nurs. 2000;21(3):269–279. doi:10.1080/016128400248086
21. Bolat N, Doğangün B, Yavuz M, Demir T, Kayaalp L. Depression and anxiety levels and self-concept characteristics of adolescents with congenital complete visual impairment. Turk Psikiyatri Derg. 2011;22(2):77–82.
22. Bakhla AK, Sinha VK, Verma V, Sarkhel S. Prevalence of psychiatric morbidity in visually impaired children. Indian Pediatr. 2011;48(3):225–227. doi:10.1007/s13312-011-0050-9
23. Donoyama N, Takeda F. Mental Health and Related Factors among Massage Practitioners with Visual Impairment. Ind Health. 2007;45(2):191–198. doi:10.2486/indhealth.45.191
24. Jampel HD, Frick KD, Janz NK, et al. Depression and mood indicators in newly diagnosed glaucoma patients. Am J Ophthalmol. 2007;144(2):238–244.e1. doi:10.1016/j.ajo.2007.04.048
25. Garaigordobil M, Bernarás E. Self-concept, self-esteem, personality traits and psychopathological symptoms in adolescents with and without visual impairment. Span J Psychol. 2009;12(1):149–160. doi:10.1017/S1138741600001566
26. Congdon N, O’Colmain B, Klaver CCW, et al. Causes and prevalence of visual impairment among adults in the United States. Arch Ophthalmol. 2004;122(4):477–485. doi:10.1001/archopht.122.4.477
27. Varma R, Vajaranant TS, Burkemper B, et al. Visual impairment and blindness in adults in the United States: demographic and geographic variations from 2015 to 2050. JAMA Ophthalmol. 2016;134(7):802. doi:10.1001/jamaophthalmol.2016.1284
28. Wong WL, Su X, Li X, et al. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: a systematic review and meta-analysis. Lancet Global Health. 2014;2(2):e106–e116. doi:10.1016/S2214-109X(13)70145-1
29. Fiske A, Wetherell JL, Gatz M. Depression in older adults. Annu Rev Clin Psychol. 2009;5(1):363–389. doi:10.1146/annurev.clinpsy.032408.153621
30. Wassink-Vossen S, Collard RM, Wardenaar KJ, et al. Trajectories and determinants of functional limitations in late-life depression: a 2-year prospective cohort study. Eur Psychiatry. 2019;62:90–96. doi:10.1016/j.eurpsy.2019.09.003
31. Court H, McLean G, Guthrie B, Mercer SW, Smith DJ. Visual impairment is associated with physical and mental comorbidities in older adults: a cross-sectional study. BMC Med. 2014;12:1. doi:10.1186/s12916-014-0181-7
32. Horowitz A. Major and subthreshold depression among older adults seeking vision rehabilitation services. Am J Geriatric Psychiatry. 2005;13(3):180–187. doi:10.1176/appi.ajgp.13.3.180
33. van der Aa HPA, Comijs HC, Penninx BWJH, van Rens GHMB, van Nispen RMA. Major depressive and anxiety disorders in visually impaired older adults. Invest Ophthalmol Vis Sci. 2015;56(2):849–854. doi:10.1167/iovs.14-15848
34. Frank CR, Xiang X, Stagg BC, Ehrlich JR. Longitudinal associations of self-reported vision impairment with symptoms of anxiety and depression among older adults in the United States. JAMA Ophthalmol. 2019;137(7):793. doi:10.1001/jamaophthalmol.2019.1085
35. van der Aa HPA, Hoeben M, Rainey L, van Rens GHMB, Vreeken HL, van Nispen RMA. Why visually impaired older adults often do not receive mental health services: the patient’s perspective. Qual Life Res. 2015;24(4):969–978. doi:10.1007/s11136-014-0835-0
36. Evans JR, Fletcher AE, Wormald RPL. Depression and anxiety in visually impaired older people. Ophthalmology. 2007;114(2):283–288. doi:10.1016/j.ophtha.2006.10.006
37. Hayman KJ, Kerse NM, La Grow SJ, Wouldes T, Robertson MC, Campbell AJ. Depression in older people: visual impairment and subjective ratings of health. OptometryVision Sci. 2007;84(11):1024–1030. doi:10.1097/OPX.0b013e318157a6b1
38. Heesterbeek TJ, van der Aa HPA, van Rens GHMB, Twisk JWR, van Nispen RMA. The incidence and predictors of depressive and anxiety symptoms in older adults with vision impairment: a longitudinal prospective cohort study. Ophthalmic Physiol Optics. 2017;37(4):385–398. doi:10.1111/opo.12388
39. Holloway EE, Sturrock BA, Lamoureux EL, Keeffe JE, Rees G. Depression screening among older adults attending low-vision rehabilitation and eye-care services: characteristics of those who screen positive and client acceptability of screening: depression screening in low vision. Australas J Ageing. 2015;34(4):229–234. doi:10.1111/ajag.12159
40. Mabuchi F, Yoshimura K, Kashiwagi K, et al. High prevalence of anxiety and depression in patients with primary open-angle glaucoma. J Glaucoma. 2008;17(7):552–557. doi:10.1097/IJG.0b013e31816299d4
41. Nollett CL, Bray N, Bunce C, et al. High prevalence of untreated depression in patients accessing low-vision services. Ophthalmology. 2016;123(2):440–441. doi:10.1016/j.ophtha.2015.07.009
42. Jones GC, Rovner BW, Crews JE, Danielson ML. Effects of depressive symptoms on health behavior practices among older adults with vision loss. Rehabil Psychol. 2009;54(2):164–172. doi:10.1037/a0015910
43. Chou K-L. Combined effect of vision and hearing impairment on depression in older adults: evidence from the English Longitudinal Study of Ageing. J Affect Disord. 2008;106(1–2):191–196. doi:10.1016/j.jad.2007.05.028
44. Augustin A, Sahel J-A, Bandello F, et al. Anxiety and Depression Prevalence Rates in Age-Related Macular Degeneration. Invest Opthalmol Visual Sci. 2007;48(4):1498. doi:10.1167/iovs.06-0761
45. Eramudugolla R, Wood J, Anstey KJ. Co-morbidity of depression and anxiety in common age-related eye diseases: a population-based study of 662 adults. Front Aging Neurosci. 2013;5. doi:10.3389/fnagi.2013.00056
46. Mathew RS, Delbaere K, Lord SR, Beaumont P, Vaegan MMC. Depressive symptoms and quality of life in people with age- related macular degeneration: quality of life and AMD. Ophthalmic Physiol Optics. 2011;31(4):375–380. doi:10.1111/j.1475-1313.2011.00848.x
47. Rovner BW, Casten RJ. Neuroticism predicts depression and disability in age-related macular degeneration. J Am Geriatr Soc. 2001;49(8):1097–1100. doi:10.1046/j.1532-5415.2001.49215.x
48. Rovner BW, Casten RJ. Activity loss and depression in age-related macular degeneration. Am J Geriatric Psychiatry. 2002;10(3):305–310. doi:10.1097/00019442-200205000-00010
49. Brody BL, Gamst AC, Williams RA, et al. Depression, visual acuity, comorbidity, and disability associated with age-related macular degeneration. Ophthalmology. 2001;108(10):1893–1900. doi:10.1016/S0161-6420(01)00754-0
50. Dawson SR, Mallen CD, Gouldstone MB, Yarham R, Mansell G. The prevalence of anxiety and depression in people with age-related macular degeneration: a systematic review of observational study data. BMC Ophthalmol. 2014;14:1. doi:10.1186/1471-2415-14-78
51. Soubrane G. Burden and health care resource utilization in neovascular age-related macular degeneration: findings of a multicountry study. Arch Ophthalmol. 2007;125(9):1249. doi:10.1001/archopht.125.9.1249
52. Kempen GIJM, Ballemans J, Ranchor AV, van Rens GHMB, Zijlstra GAR. Erratum to: the impact of low vision on activities of daily living, symptoms of depression, feelings of anxiety and social support in community-living older adults seeking vision rehabilitation services. Qual Life Res. 2012;21(8):1413. doi:10.1007/s11136-011-0103-5
53. Cosh S, Carrière I, Daien V, Tzourio C, Delcourt C, Helmer C. Sensory loss and suicide ideation in older adults: findings from the Three-City cohort study. Int Psychogeriatrics. 2019;31(1):139–145. doi:10.1017/S104161021800056X
54. Forsell Y, Jorm AF, Winblad B. Suicidal thoughts and associated factors in an elderly population. Acta Psychiatr Scand. 1997;95(2):108–111. doi:10.1111/j.1600-0447.1997.tb00382.x
55. Kim Y, Kwak Y, Kim J. The association between suicide ideation and sensory impairment among elderly Koreans. Aging Ment Health. 2015;19(7):658–665. doi:10.1080/13607863.2014.989812
56. Waern M. Burden of illness and suicide in elderly people: case-control study. BMJ. 2002;324(7350):1355. doi:10.1136/bmj.324.7350.1355
57. Rim TH, Lee CS, Lee SC, Chung B, Kim SS. Epidemiologic Survey Committee of the Korean Ophthalmological Society. Influence of visual acuity on suicidal ideation, suicide attempts and depression in South Korea. Br J Ophthalmol. 2015;99(8):1112–1119. doi:10.1136/bjophthalmol-2014-306518
58. Stensman R, Sundqvist-Stensman U-B. Physical disease and disability among 416 suicide cases in Sweden. Scand J Soc Med. 1988;16(3):149–153. doi:10.1177/140349488801600305
59. Meyer-Rochow VB, Hakko H, Ojamo M, Uusitalo H, Timonen M. Suicides in visually impaired persons: a nation-wide register-linked study from finland based on thirty years of data. Voracek M, ed. PLoS One. 2015;10(10):e0141583. doi:10.1371/journal.pone.0141583
60. Lam BL. Reported visual impairment and risk of suicide: the 1986-1996 national health interview surveys. Arch Ophthalmol. 2008;126(7):975. doi:10.1001/archopht.126.7.975
61. Menon GJ, Rahman I, Menon SJ, Dutton GN. Complex Visual Hallucinations in the Visually Impaired. Surv Ophthalmol. 2003;48(1):58–72. doi:10.1016/S0039-6257(02)00414-9
62. Brown GC. Visual symptoms associated with choroidal neovascularization: photopsias and the charles bonnet syndrome. Arch Ophthalmol. 1992;110(9):1251. doi:10.1001/archopht.1992.01080210069027
63. Lepore FE. Spontaneous visual phenomena with visual loss: 104 patients with lesions of retinal and neural afferent pathways. Neurology. 1990;40(3 Part1):444. doi:10.1212/WNL.40.3_Part_1.444
64. Vaphiades MS, Celesia GG, Brigell MG. Positive spontaneous visual phenomena limited to the hemianopic field in lesions of central visual pathways. Neurology. 1996;47(2):408–417. doi:10.1212/WNL.47.2.408
65. Schadlu AP, Schadlu R, Shepherd JB. Charles Bonnet syndrome: a review. Curr Opin Ophthalmol. 2009;20(3):219–222. doi:10.1097/ICU.0b013e328329b643
66. Schwartz TL, Vahgei L. Charles Bonnet syndrome in children. J Am Assoc Ped Ophthalmol Strabismus. 1998;2(5):310–313. doi:10.1016/S1091-8531(98)90091-X
67. Tan CSH, Sabel BA, Goh K-Y. Visual hallucinations during visual recovery after central retinal artery occlusion. Arch Neurol. 2006;63(4):598. doi:10.1001/archneur.63.4.598
68. Schultz G, Melzack R. Visual hallucinations and mental state: a study of 14 Charles Bonnet syndrome hallucinators. J Nerv Ment Dis. 1993;181(10):639–643. doi:10.1097/00005053-199310000-00011
69. Holroyd S, Rabins PV, Finkelstein D, Lavrisha M. Visual hallucinations in patients from an ophthalmology clinic and medical clinic population. J Nerv Ment Dis. 1994;182(5):273–276. doi:10.1097/00005053-199405000-00004
70. Cole MG. Charles Bonnet hallucinations: a case series *. Can J Psychiatry. 1992;37(4):267–270. doi:10.1177/070674379203700411
71. Giridhar P, Dandona R, Prasad MN, Kovai V, Dandona L. Fear of blindness and perceptions about blind people. The Andhra Pradesh Eye Disease Study. Indian J Ophthalmol. 2002;50(3):239–246.
72. De Leo D, Hickey PA, Meneghel G, Cantor CH. Blindness, Fear of Sight Loss, and Suicide. Psychosomatics. 1999;40(4):339–344. doi:10.1016/S0033-3182(99)71229-6
73. Wong EYH, Guymer RH, Hassell JB, Keeffe JE. The Experience of Age-related Macular Degeneration. J Vis Impair Blind. 2004;98(10):629–640. doi:10.1177/0145482X0409801007
74. Teitelman J, Copolillo A. Psychosocial Issues in Older Adults’ Adjustment to Vision Loss: findings From Qualitative Interviews and Focus Groups. Am J Occupational Ther. 2005;59(4):409–417. doi:10.5014/ajot.59.4.409
75. Alma MA, van der Mei SF, Melis-Dankers BJM, van Tilburg TG, Groothoff JW, Suurmeijer TPBM. Participation of the elderly after vision loss. Disabil Rehabil. 2011;33(1):63–72. doi:10.3109/09638288.2010.488711
76. Thurston M, Thurston A, McLeod J. Socio-emotional effects of the transition from sight to blindness. Br J Visual Impairment. 2010;28(2):90–112. doi:10.1177/0264619609359304
77. Rees G, Xie J, Holloway EE, et al. Identifying Distinct Risk Factors for Vision-Specific Distress and Depressive Symptoms in People With Vision Impairment. Invest Opthalmol Visual Sci. 2013;54(12):7431. doi:10.1167/iovs.13-12153
78. Nollett CL, Ryan B, Bray N, et al. Depressive symptoms in people with vision impairment: a cross-sectional study to identify who is most at risk. BMJ Open. 2019;9(1):e026163. doi:10.1136/bmjopen-2018-026163
79. Wallhagen MI, Strawbridge WJ, Shema SJ, Kurata J, Kaplan GA. Comparative Impact of Hearing and Vision Impairment On Subsequent Functioning. J Am Geriatr Soc. 2001;49(8):1086–1092. doi:10.1046/j.1532-5415.2001.49213.x
80. Brown JC, Goldstein JE, Chan TL, Massof R, Ramulu P. Characterizing functional complaints in patients seeking outpatient low-vision services in the United States. Ophthalmology. 2014;121(8):1655–1662.e1. doi:10.1016/j.ophtha.2014.02.030
81. McDermott S, Moran R, Platt T, Dasari S. Health conditions among women with a disability. J Women’s Health. 2007;16(5):713–720. doi:10.1089/jwh.2007.0363
82. Mitra M, Wilber N, Allen D, Walker DK. Prevalence and correlates of depression as a secondary condition among adults with disabilities. Am J Orthopsychiatry. 2005;75(1):76–85. doi:10.1037/0002-9432.75.1.76
83. Okoro CA, Strine TW, Balluz LS, Crews JE, Mokdad AH. Prevalence and correlates of depressive symptoms among United States adults with disabilities using assistive technology. Prev Med. 2010;50(4):204–209. doi:10.1016/j.ypmed.2010.01.008
84. Robinson-Whelen S, Taylor HB, Hughes RB, Nosek MA. Depressive symptoms in women with physical disabilities: identifying correlates to inform practice. Arch Phys Med Rehabil. 2013;94(12):2410–2416. doi:10.1016/j.apmr.2013.07.013
85. Bookwala J, Lawson B. Poor vision, functioning, and depressive symptoms: a test of the activity restriction model. The Gerontologist. 2011;51(6):798–808. doi:10.1093/geront/gnr051
86. Crews JE, Jones GC, Kim JH. Double jeopardy: the effects of comorbid conditions among older people with vision loss. J Vis Impair Blind. 2006;100(1_suppl):824–848. doi:10.1177/0145482X0610001S07
87. Erickson W, Lee C, von Schrader S Disability Statistics from the American Community Survey (ACS). Cornell University Yang-Tan Institute (YTI); 2017. www.disabilitystatistics.org.
88. Kok RM, Reynolds CF. Management of depression in older adults: a review. JAMA. 2017;317(20):2114. doi:10.1001/jama.2017.5706
89. Chang-Quan H, Xue-Mei Z, Bi-Rong D, Zhen-Chan L, Ji-Rong Y, Qing-Xiu L. Health status and risk for depression among the elderly: a meta-analysis of published literature. Age Ageing. 2010;39(1):23–30. doi:10.1093/ageing/afp187
90. Lenze EJ, Rogers JC, Martire LM, et al. The association of late-life depression and anxiety with physical disability: a review of the literature and prospectus for future research. Am J Geriatric Psychiatry. 2001;9(2):113–135. doi:10.1097/00019442-200105000-00004
91. Carrière I, Delcourt C, Daien V, et al. A prospective study of the bi-directional association between vision loss and depression in the elderly. J Affect Disord. 2013;151(1):164–170. doi:10.1016/j.jad.2013.05.071
92. Gillies MC, Campain A, Barthelmes D, et al. Long-Term outcomes of treatment of neovascular age-related macular degeneration. Ophthalmology. 2015;122(9):1837–1845. doi:10.1016/j.ophtha.2015.05.010
93. Senra H, Ali Z, Balaskas K, Aslam T. Psychological impact of anti-VEGF treatments for wet macular degeneration—a review. Graefe’s Arch Clin Exp Ophthalmol. 2016;254(10):1873–1880. doi:10.1007/s00417-016-3384-0
94. Senra H, Balaskas K, Mahmoodi N, Aslam T. Experience of Anti-VEGF treatment and clinical levels of depression and anxiety in patients with wet age-related macular degeneration. Am J Ophthalmol. 2017;177:213–224. doi:10.1016/j.ajo.2017.03.005
95. Ford DE. Optimizing outcomes for patients with depression and chronic medical illnesses. Am J Med. 2008;121(11):S38–S44. doi:10.1016/j.amjmed.2008.09.012
96. Verger P, Lions C, Ventelou B. Is depression associated with health risk-related behaviour clusters in adults? Eur J Public Health. 2009;19(6):618–624. doi:10.1093/eurpub/ckp057
97. Richa S, Yazbek J-C. Ocular adverse effects of common psychotropic agents: a review. CNS Drugs. 2010;24(6):501–526. doi:10.2165/11533180-000000000-00000
98. Lavoie M-P, Lam RW, Bouchard G, et al. Evidence of a biological effect of light therapy on the retina of patients with seasonal affective disorder. Biol Psychiatry. 2009;66(3):253–258. doi:10.1016/j.biopsych.2008.11.020
99. Hébert M, Dumont M, Lachapelle P. Electrophysiological evidence suggesting a seasonal modulation of retinal sensitivity in subsyndromal winter depression. J Affect Disord. 2002;68(2–3):191–202. doi:10.1016/S0165-0327(00)00192-0
100. Bubl E, Ebert D, Kern E, van Elst LT, Bach M. Effect of antidepressive therapy on retinal contrast processing in depressive disorder. Br J Psychiatry. 2012;201(2):151–158. doi:10.1192/bjp.bp.111.100560
101. Fam J, Rush AJ, Haaland B, Barbier S, Luu C. Visual contrast sensitivity in major depressive disorder. J Psychosom Res. 2013;75(1):83–86. doi:10.1016/j.jpsychores.2013.03.008
102. Rovner BW, Zisselman PM, Shmuely-Dulitzki Y. Depression and disability in older people with impaired vision: a follow-up study. J Am Geriatr Soc. 1996;44(2):181–184. doi:10.1111/j.1532-5415.1996.tb02436.x
103. Lansingh V, Carter M, Ulldemolins A, Valencia L, Eckert K. Social inequalities in blindness and visual impairment: a review of social determinants. Indian J Ophthalmol. 2012;60(5):368. doi:10.4103/0301-4738.100529
104. Ehrlich JR, Stagg BC, Andrews C, Kumagai A, Musch DC. Vision impairment and receipt of eye care among older adults in low- and middle-income countries. JAMA Ophthalmol. 2019;137(2):146. doi:10.1001/jamaophthalmol.2018.5449
105. Wang W, Yan W, Müller A, Keel S, He M. Association of socioeconomics with prevalence of visual impairment and blindness. JAMA Ophthalmol. 2017;135(12):1295. doi:10.1001/jamaophthalmol.2017.3449
106. Perruccio AV, Badley EM, Trope GE. A Canadian population-based study of vision problems: assessing the significance of socioeconomic status. Can J Ophthalmol. 2010;45(5):477–483. doi:10.3129/i10-061
107. Gilbert CE, Shah SP, Jadoon MZ, et al. Poverty and blindness in Pakistan: results from the Pakistan national blindness and visual impairment survey. BMJ. 2008;336(7634):29–32. doi:10.1136/bmj.39395.500046.AE
108. Kirtland KA, Saaddine JB, Geiss LS, et al. Geographic disparity of severe vision loss - United States, 2009-2013. MMWR Morb Mortal Wkly Rep. 2015;64(19):513–517.
109. Wah W, Earnest A, Sabanayagam C, et al. Composite measures of individual and area-level socio-economic status are associated with visual impairment in Singapore. PLoS One. 2015;10(11):e0142302. doi:10.1371/journal.pone.0142302
110. Yip JLY, Luben R, Hayat S, et al. Area deprivation, individual socioeconomic status and low vision in the EPIC-Norfolk Eye Study. J Epidemiol Community Health. 2014;68(3):204–210. doi:10.1136/jech-2013-203265
111. Zheng Y, Lamoureux E, Finkelstein E, et al. Independent impact of area-level socioeconomic measures on visual impairment. Invest Opthalmol Visual Sci. 2011;52(12):8799. doi:10.1167/iovs.11-7700
112. Cockburn N, Steven D, Lecuona K, et al. Prevalence, causes and socio-economic determinants of vision loss in Cape Town, South Africa. Atashili J, ed. PLoS One. 2012;7(2):e30718. doi:10.1371/journal.pone.0030718
113. Jalali MDM, Moussavi MS, Yazdi SAA, Fadardi JS. Effectiveness of rational emotive behavior therapy on psychological well-being of people with late blindness. J Rational Emot Ognitive Behav Ther. 2014;32(4):233–247. doi:10.1007/s10942-014-0191-6
114. Chou C-F, Beckles GLA, Zhang X, Saaddine JB. Association of socioeconomic position with sensory impairment among us working-aged adults. Am J Public Health. 2015;105(6):1262–1268. doi:10.2105/AJPH.2014.302475
115. Rahi JS, Cumberland PM, Peckham CS. Visual function in working-age adults early life influences and associations with health and social outcomes. Ophthalmology. 2009;116(10):1866–1871. doi:10.1016/j.ophtha.2009.03.007
116. Dandona R. Moderate visual impairment in India: the Andhra Pradesh eye disease study. Br J Ophthalmol. 2002;86(4):373–377. doi:10.1136/bjo.86.4.373
117. Yan X, Chen L, Yan H. Socio-economic status, visual impairment and the mediating role of lifestyles in developed rural areas of China. Zhou X, ed. PLoS One. 2019;14(4):e0215329. doi:10.1371/journal.pone.0215329
118. Wilson CJ, Rust G, Levine R, Alema-Mensah E. Disparities in vision impairment among adults in the United States. Ethn Dis. 2008;18(2Suppl2):
119. Varma R, Chung J, Foong AWP, Torres M, Choudhury F, SP A. Four-year incidence and progression of visual impairment in Latinos: the Los Angeles Latino eye study. Am J Ophthalmol. 2010;149(5):713–727. doi:10.1016/j.ajo.2009.12.011
120. Nollett CL, Bray N, Bunce C, et al. Depression in Visual Impairment Trial (DEPVIT): a randomized clinical trial of depression treatments in people with low vision. Invest Opthalmol Visual Sci. 2016;57(10):4247. doi:10.1167/iovs.16-19345
121. Julia Salinas RS, Aishat Mohammed NHF, Warren JZ. Primary open-angle glaucoma in individuals of african descent: a review of risk factors. J Clin Exp Ophthalmol. 2015;06:04. doi:10.4172/2155-9570.1000450
122. Abou-Gareeb I, Lewallen S, Bassett K, Courtright P. Gender and blindness: a meta-analysis of population-based prevalence surveys. Ophthalmic Epidemiol. 2001;8(1):39–56. doi:10.1076/opep.8.1.39.1540
123. Clayton JA, Davis AF. Sex/gender disparities and women’s eye health. Curr Eye Res. 2015;40(2):102–109. doi:10.3109/02713683.2014.986333
124. Doyal L, Das-Bhaumik RG. Sex, gender and blindness: a new framework for equity. BMJ Open Ophthalmol. 2018;3(1):e000135. doi:10.1136/bmjophth-2017-000135
125. Mganga H, Lewallen S, Courtright P. Overcoming gender inequity in prevention of blindness and visual impairment in Africa. Middle East Afr J Ophthalmol. 2011;18(2):98–101. doi:10.4103/0974-9233.80695
126. van der Aa HPA, Xie J, Rees G, et al. Validated prediction model of depression in visually impaired older adults. Ophthalmology. 2016;123(5):1164–1166. doi:10.1016/j.ophtha.2015.11.028
127. Albert P. Why is depression more prevalent in women? J Psychiatry Neurosci. 2015;40(4):219–221. doi:10.1503/jpn.150205
128. Baxter AJ, Scott KM, Ferrari AJ, Norman RE, Vos T, Whiteford HA. Challenging the myth of an “epidemic” of common mental disorders: trends in the global prevalence of anxiety and depression between 1990 and 2010. Depress Anxiety. 2014;31(6):506–516. doi:10.1002/da.22230
129. Leigh IW, Powers L, Vash C, Nettles R. Survey of psychological services to clients with disabilities: the need for awareness. Rehabil Psychol. 2004;49(1):48–54. doi:10.1037/0090-5550.49.1.48
130. Ruggeri M, Bonetto C, Lasalvia A, et al. Feasibility and effectiveness of a multi-element psychosocial intervention for first-episode psychosis: results from the cluster-randomized controlled GET UP PIANO trial in a catchment area of 10 million inhabitants. Schizophr Bull. 2015;41(5):1192–1203. doi:10.1093/schbul/sbv058
131. Taylor HR, Pezzullo ML, Nesbitt SJ, Keeffe JE. Costs of interventions for visual impairment. Am J Ophthalmol. 2007;143(4):561–565.e1. doi:10.1016/j.ajo.2006.10.055
132. Ishii K, Kabata T, Oshika T. The impact of cataract surgery on cognitive impairment and depressive mental status in elderly patients. Am J Ophthalmol. 2008;146(3):404–409. doi:10.1016/j.ajo.2008.05.014
133. Nyman SR, Gosney MA, Victor CR. Emotional well-being in people with sight loss: lessons from the grey literature. Br J Visual Impairment. 2010;28(3):175–203. doi:10.1177/0264619610374171
134. Brennan M, Horowitz A, Reinhardt JP, Cimarolli V, Benn DT, Leonard R. In their own words: strategies developed by visually impaired elders to cope with vision loss. J Gerontol Soc Work. 2001;35(1):107–129. doi:10.1300/J083v35n01_08
135. Penn E, Tracy DK. The drugs don’t work? antidepressants and the current and future pharmacological management of depression. Ther Advan Psychopharmacol. 2012;2(5):179–188. doi:10.1177/2045125312445469
136. Barlow J, Wright C, Sheasby J, Turner A, Hainsworth J. Self-management approaches for people with chronic conditions: a review. Patient Educ Couns. 2002;48(2):177–187. doi:10.1016/S0738-3991(02)00032-0
137. Brody BL, Williams RA, Thomas RG, Kaplan RM, Chu RM, Brown SI. Age-related macular degeneration: A randomized clinical trial of a self-management intervention. Ann Behav Med. 1999;21(4):322–329. doi:10.1007/BF02895965
138. Brody BL. Self-management of age-related macular degeneration and quality of life: a randomized controlled trial. Arch Ophthalmol. 2002;120(11):1477. doi:10.1001/archopht.120.11.1477
139. Brody BL. Self-management of age-related macular degeneration at the 6-month follow-up: a randomized controlled trial. Arch Ophthalmol. 2005;123(1):46. doi:10.1001/archopht.123.1.46
140. Brody BL, Roch-Levecq A-C, Kaplan RM, Moutier CY, Brown SI. Age-related macular degeneration: self-management and reduction of depressive symptoms in a randomized, controlled study: AMD self-management and reduced depressive symptoms. J Am Geriatr Soc. 2006;54(10):1557–1562. doi:10.1111/j.1532-5415.2006.00881.x
141. Girdler SJ, Boldy DP, Dhaliwal SS, Crowley M, Packer TL. Vision self-management for older adults: a randomised controlled trial. Br J Ophthalmol. 2010;94(2):223–228. doi:10.1136/bjo.2008.147538
142. Rees G, Xie J, Chiang PP, et al. A randomised controlled trial of a self-management programme for low vision implemented in low vision rehabilitation services. Patient Educ Couns. 2015;98(2):174–181. doi:10.1016/j.pec.2014.11.008
143. Gath D, Mynors-Wallis L. Problem-solving treatment in primary care. In Clark DM, Fairburn CG, editors. Science and Practice of Cognitive Behaviour Therapy. Oxford, UK: Oxford University Press; 1997:415–431.
144. Rovner BW, Casten RJ, Hegel MT, Leiby BE, Tasman WS. Preventing depression in age-related macular degeneration. Arch Gen Psychiatry. 2007;64(8):886. doi:10.1001/archpsyc.64.8.886
145. Mynors-Wallis L. Problem-solving treatment: evidence for effectiveness and feasibility in primary care. Int J Psychiatry Med. 1996;26(3):249–262. doi:10.2190/0HVY-CD2F-0KC7-FVTB
146. Mynors-Wallis LM. Randomised controlled trial of problem solving treatment, antidepressant medication, and combined treatment for major depression in primary care. BMJ. 2000;320(7226):26–30. doi:10.1136/bmj.320.7226.26
147. Rovner BW, Casten RJ. Preventing late-life depression in age-related macular degeneration. Am J Geriatric Psychiatry. 2008;16(6):454–459. doi:10.1097/JGP.0b013e31816b7342
148. Holloway E, Sturrock B, Lamoureux E, et al. Delivering problem-solving treatment in low-vision rehabilitation: A pilot feasibility study. Rehabil Psychol. 2018;63(3):349–356. doi:10.1037/rep0000217
149. Rovner BW, Casten RJ, Hegel MT, et al. Improving function in age-related macular degeneration. Ophthalmology. 2013;120(8):1649–1655. doi:10.1016/j.ophtha.2013.01.022
150. Stelmack J. Emergence of a rehabilitation medicine model for low vision service delivery, policy, and funding. Optometry J Am Optometric Assoc. 2005;76(5):318–326. doi:10.1016/S1529-1839(05)70315-8
151. Horowitz A, Reinhardt JP, Boerner K. The effect of rehabilitation on depression among visually disabled older adults. Aging Ment Health. 2005;9(6):563–570. doi:10.1080/13607860500193500
152. Horowitz A, Brennan M, Reinhardt JP, MacMillan T. The impact of assistive device use on disability and depression among older adults with age-related vision impairments. J Gerontol B Psychol Sci Soc Sci. 2006;61(5):S274–S280. doi:10.1093/geronb/61.5.S274
153. Rovner BW, Casten RJ, Hegel MT, et al. Low vision depression prevention trial in age-related macular degeneration. Ophthalmology. 2014;121(11):2204–2211. doi:10.1016/j.ophtha.2014.05.002
154. Kamga H, McCusker J, Yaffe M, et al. Self-care tools to treat depressive symptoms in patients with age-related eye disease: a randomized controlled clinical trial: self-care tools and depressive symptoms. Clin Experiment Ophthalmol. 2017;45(4):371–378. doi:10.1111/ceo.12890
155. Kendrick T, Pilling S. Common mental health disorders — identification and pathways to care: NICE clinical guideline. Br J General Pract. 2012;62(594):47–49. doi:10.3399/bjgp12X616481
156. Van’t Veer-tazelaar PJ, van Marwijk HWJ, van Oppen P, et al. Stepped-care prevention of anxiety and depression in late life: a randomized controlled trial. Arch Gen Psychiatry. 2009;66(3):297. doi:10.1001/archgenpsychiatry.2008.555
157. van der Aa HPA, van Rens GHMB, Comijs HC, et al. Stepped care for depression and anxiety in visually impaired older adults: multicentre randomised controlled trial. BMJ. 2015:h6127. doi:10.1136/bmj.h6127.
158. van der Aa HPA, van Rens GHMB, Bosmans JE, Comijs HC, van Nispen RMA. Economic evaluation of stepped-care versus usual care for depression and anxiety in older adults with vision impairment: randomized controlled trial. BMC Psychiatry. 2017;17:1. doi:10.1186/s12888-017-1437-5
159. Wahl H-W, Kämmerer A, Holz F, et al. Psychosocial intervention for age-related macular degeneration: a pilot project. J Vis Impair Blind. 2006;100(9):533–544. doi:10.1177/0145482X0610000905
160. van der Aa HPA, Margrain TH, van Rens GHMB, Heymans MW, van Nispen RMA. Psychosocial interventions to improve mental health in adults with vision impairment: systematic review and meta-analysis. Ophthalmic Physiol Optics. 2016;36(5):584–606. doi:10.1111/opo.12313
161. Senra H, Macedo AF, Nunes N, Balaskas K, Aslam T, Costa E. Psychological and psychosocial interventions for depression and anxiety in patients with age-related macular degeneration: a systematic review. Am J Geriatric Psychiatry. 2019;27(8):755–773. doi:10.1016/j.jagp.2019.03.001
162. Tuttle DW, Tuttle NR. Self-Esteem and Adjusting with Blindness: The Process of Responding to Life’s Demands.
163. Bradley P, Mitchell J, Bradley C. Peer support for people newly diagnosed with macular degeneration: A pilot study. Int Congress Series. 2005;1282:211–215. doi:10.1016/j.ics.2005.04.001
164. Kleinschmidt JJ. Older adults’ perspectives on their successful adjustment to vision loss. J Vis Impair Blind. 1999;93(2):69–81. doi:10.1177/0145482X9909300202
165. A-Tjak JGL, Davis ML, Morina N, et al. A meta-analysis of the efficacy of acceptance and commitment therapy for clinically relevant mental and physical health problems. Psychother Psychosom. 2015;84(1):30–36. doi:10.1159/000365764
166. Veehof MM, Trompetter HR, Bohlmeijer ET, Schreurs KMG. Acceptance- and mindfulness-based interventions for the treatment of chronic pain: a meta-analytic review. Cogn Behav Ther. 2016;45(1):5–31. doi:10.1080/16506073.2015.1098724
167. Bourne RRA, Stevens GA, White RA, et al. Causes of vision loss worldwide, 1990–2010: a systematic analysis. Lancet Global Health. 2013;1(6):e339–e349. doi:10.1016/S2214-109X(13)70113-X
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.