")
Back to Journals » International Journal of General Medicine » Volume 15
Vision-Related Quality of Life and Association Between Retinal Parameters in Patients with Non-Arteritic Anterior Ischemic Optic Neuropathy
Authors Su Y, Bai G, Tian H, Zhang S, Liu Y, Zhang G , Liu L , Chen K
Received 25 February 2022
Accepted for publication 16 May 2022
Published 24 May 2022 Volume 2022:15 Pages 5173—5179
DOI https://doi.org/10.2147/IJGM.S364051
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yufang Su,1,* Gang Bai,2,* Hong Tian,3,* Song Zhang,4 Yingru Liu,1 Guisen Zhang,2 Lei Liu,5 Kang Chen6
1Department of Glaucoma, Baotou Chaoju Eye Hospital, Baotou, People’s Republic of China; 2Department of Glaucoma, Hohhot Chaoju Eye Hospital, Hohhot, People’s Republic of China; 3Department of Cataract, Baotou Kunlun Chaoju Eye Hospital, Baotou, People’s Republic of China; 4Department of Graduate School, China Medical University, Shenyang, People’s Republic of China; 5Guangdong Eye Institute, Department of Ophthalmology, Guangdong Provincial People’s Hospital, Guangdong Academy of Medical Sciences, Guangzhou, People’s Republic of China; 6Department of Ophthalmology, The First Affiliated Hospital of China Medical University, Shenyang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lei Liu; Kang Chen, Tel +86 13889378662 ; +86 13804999194, Email [email protected]; [email protected]
Purpose: To evaluate visual-related quality of life (VR-QoL) and its association with optic nerve head microvasculature in individuals with nonarteritic anterior ischemic optic neuropathy (NAION) evaluated at the acute stage.
Methods: In this retrospective case-control study, 23 NAION eyes at the acute stage and 25 age and gender matched healthy eyes were included, respectively. All included eyes underwent a complete ophthalmic examination including optical coherence tomography (OCT) and OCT angiography (OCTA). The Chinese version of the National Eye Institute Visual Function Questionnaire-25 (CHI-NEI-VFQ-25) was applied to assess VR-QoL in individuals consecutively visited at an ophthalmic center. Descriptive and analytic statistics were employed.
Results: There were no significant differences on age, gender, socioeconomic and education level (P > 0.05), but best-corrected visual acuity (BCVA) differences were reported between cases and controls (P < 0.05). Each peripapillary retinal nerve fiber layer (RNFL) thickness was higher but peripapillary vessel density (VD) and VR-QoL scores for all subscales were significantly lower in cases when compared with controls, respectively (P < 0.05). Particularly, pearson’s partial correlation analysis restricted to eyes with NAION revealed stronger correlations between peripapillary RNFL measurements, VD and VR-QoL.
Conclusion: NAION at the acute stage affects VR-QoL in Chinese individuals. Some peripapillary RNFL measurements and VD correlated with VR-QoL. Retinal anatomic and blood flow examinations and inventions in patients with NAION are necessary to facilitate VR-QoL and disease control.
Keywords: nonarteritic anterior ischemic optic neuropathy, CHI-NEI-VFQ-25, OCTA, OCT, quality of life
Introduction
Nonarteritic anterior ischemic optic neuropathy (NAION) is mainly caused by posterior ciliary artery circulation disorder, the most common non-glaucoma optic neuropathy in middle-aged and elderly patients, and the second most common optic neuropathy after glaucoma.1,2 The insufficient blood supply to the optic nerve head leads to acute edema, ischemia and other pathophysiology of the optic nerve head.3 Clinically, in the acute phase, it is mostly manifested as painless loss of vision occurring over hours to days or optic disc edema, and visual field defects, which have a serious impact on the life and work of the patient.4
Previous studies demonstrated that there were significant differences in peripapillary retinal nerve fiber layer (RNFL) thickness and peripapillary vessel density (VD) between eyes with NAION and healthy controls.5–8 However, the comprehensive quadrants of RNFL thickness and VD are less studied.
The National Eye Institute Visual Functioning Questionnaire - 25 (NEI-VFQ-25) has been developed to identify quality of life among individuals with ocular diseases.9 The NEI-VFQ-25 form consists of three dimension sections including general health and vision, difficulty with activities and responses to vision problem. The Chinese version of the NEI-VFQ-25 (CHI-NEI-VFQ-25) has been further developed with well reliability and validity in assessing vision-specific quality of life among Chinese patients with myopia and cataract.10–12 To the best of our knowledge, little is presently known about the impact of visual impairments on the quality of life of Chinese patients with NAION. The aim of the current study is to evaluate vision-related quality of life (VR-QoL) among patients with NAION in China, using the CHI-NEI-VFQ-25. Measurements of the patients in eight quadrants for peripapillary RNFL and VD, together with analyses of their associations with VR-QoL will be investigated.
Methodology
A hospital-based case-control study was conducted from 1 September 2020 to 30 June 2021 at the Baotou Chaoju Eye Hospital, Baotou, China.
Included cases were selected during the routine visit in ophthalmology clinic of an adult patient (≥ 18 years) who meets the diagnostic criteria defined by acute (< 3 weeks) painless visual loss, a positive relative afferent pupillary defect (RAPD), color vision impairment, visual field defect typical of RNFL bundle damage, documented optic disc edema at the acute stage in the involved eye and crowded optic disc in the fellow eye.13 The NAION eye with swollen disc was included from each participant. If patient exhibited bilateral NAION, the severe eye was included. Exclusion criteria included: (1) perioperative anterior ischemic optic neuropathy; (2) traumatic optic neuropathy; (3) suspected arteritic anterior ischemic optic neuropathy; (4) other ophthalmologic pathology such as dense cataract, severe macular disease, or visually significant retinopathy.
Right eyes of healthy control participants were included and identical to the cases in characteristics such as age, and gender of the cases, but were free from NAION.
This study complied with the criteria of the Declaration of Helsinki for Medical Research involving Human Subjects and was approved by the Institutional Review Board (IRB) of the Baotou Chaoju Eye Hospital (No. 20190101). Written informed consent was provided by all participants.
Demographic data (age, gender, education level and monthly income) and medical history (hypertension, diabetes or other systematic diseases) were recorded. All included participants received comprehensive ophthalmological examination, including best-corrected visual acuity (BCVA) measurement (5 m Standard Logarithm Visual Acuity chart in decimal notations), slit-lamp microscopy, intraocular pressure (IOP), dilated fundus examination, automated visual field examination (24-2 Swedish Interactive Threshold Algorithm; Humphrey Field Analyser II; Carl Zeiss Meditec, Inc., Dublin, CA, USA), flash visual evoked potential (FVEP) test (UTAS-E3000LKC, Multifocal Visual Diagnostic Test System, IKC Technologies, Gaithersburg, MD, USA), fundus fluorescein angiography (FFA, Heidelberg Engineering, Heidelberg, Germany), optical coherence tomography (OCT) and OCT angiography (Optovue Inc., Fremont, CA, USA). 4.5 mm × 4.5 mm centered on the optic nerve head (ONH) scans were performed. The instrument has an A-scan rate of 70,000 per second, using a light source centered on 840 nm. Only high-quality images-defined by scans with scan quality >7/10 (and without artifacts) were included. Structural OCT images with quantitative measures in all regions of peripapillary retinal nerve fiber layer (pRNFL) thickness (peripapillary temporal upper, pTU; peripapillary superior temporal, pST; peripapillary superior nasal, pSN; peripapillary nasal upper, pNU; peripapillary nasal lower, pNL; peripapillary inferior nasal, pIN; peripapillary inferior temporal, pIT; peripapillary temporal lower, pTL) were scored. The peripapillary area of VD was divided into 8 peripapillary sectors automatically according to the GarwayHeath method: nasal superior (NS), nasal inferior (NI), inferior nasal (IN), inferior temporal (IT), temporal inferior (TI), temporal superior (TS), superior temporal (ST), and superior nasal (SN). Two experienced ophthalmologists, who independently interpreted the optic changes, were blinded to the findings of conventional ophthalmoscopy.
The CHI-NEI-VFQ-25 was used to assess the quality of life of patients with NAION. Both cases and controls were evaluated in an interview, using the CHI-NEI-VFQ-25. The CHI-NEI-VFQ-25 consisted of 25 questions divided into 12 subscales, which include one subscale related to general health and 11 vision-related subscales including general vision, ocular pain, near activities, distance activities, social functioning, mental health, role difficulties, dependency, driving, color vision, and peripheral vision. The original answer from participant to each question was converted to 0–100 points, of which, 100 indicated the best possible health status, while 0 indicated the worst health status. The subscale scores were the average of one or more questions.
Statistical Analysis
Statistical analysis was performed using SPSS 25.0 (IBM Corporation, Armonk, NY, USA). Mean and standard deviation (SD) or median and interquartile range [IQR] were described for numerical variables and proportion (%) for categorical variables. For comparisons between eyes with NAION and healthy controls, the Mann-Whitney Wilcoxon test for continuous variables and chi-squared test for categorical variables were performed. The associations of VR-QoL and OCT as well as OCTA parameters with NAION were evaluated, and partial correlation coefficient was calculated after adjusting for age, gender, BCVA, education level and monthly income. Statistical significance was set at P < 0.05.
Results
Twenty-three NAION eyes as cases and 25 age and gender matched health eyes as controls were included. Table 1 shows the demographic, lifestyle and medical history characteristics of the subjects. There were no significant differences on age, gender, medical history, education level, monthly income and spherical equivalent (SE) (all P > 0.05). Eyes with NAION appeared to have a worse BCVA compared with to controls (P = 0.002).
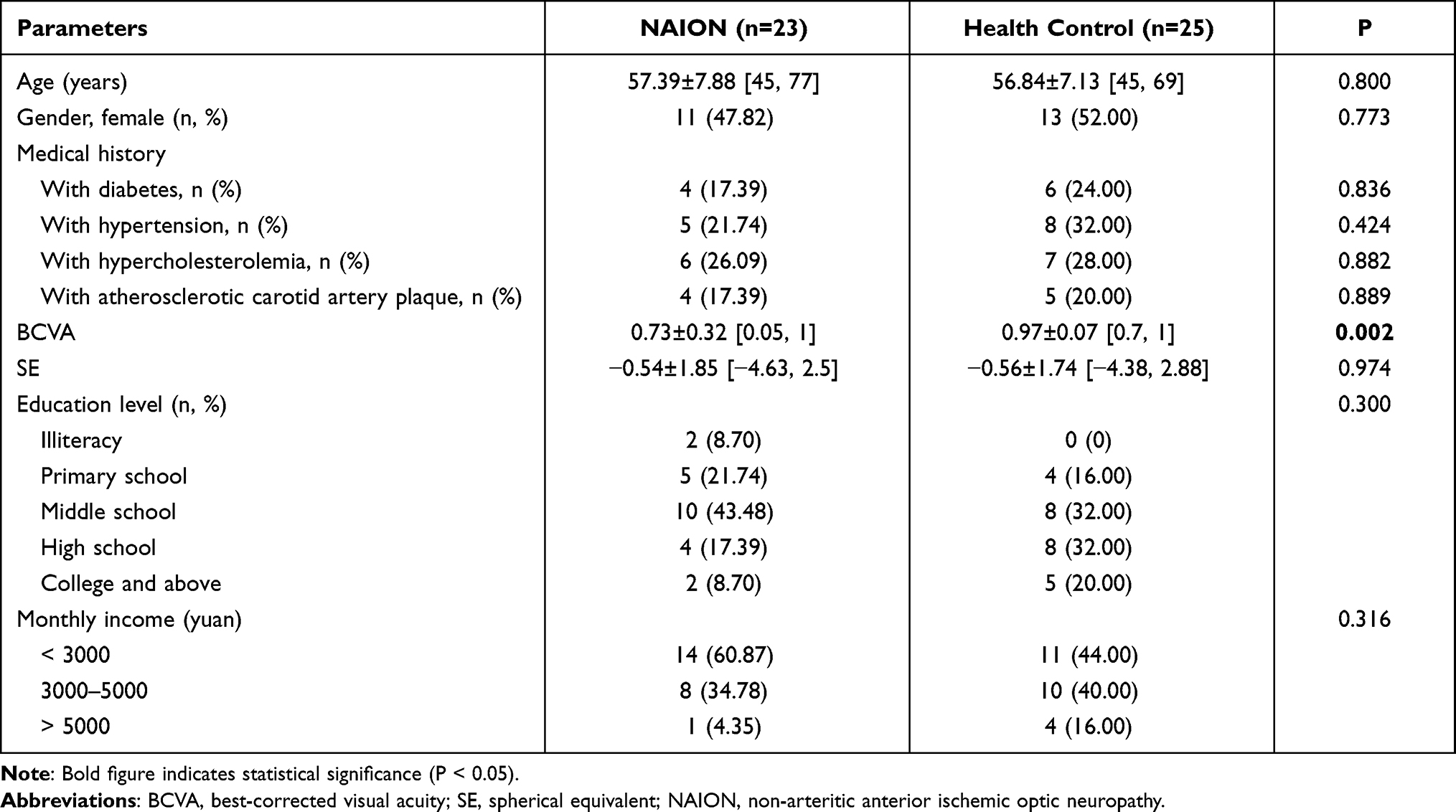 |
Table 1 General Situation of the NAION and Control Groups |
There were significant differences in mean measurements of all the peripapillary RNFL and VD parameters between the two groups (Table 2, P < 0.05). Additionally, visual field parameters (visual field index, mean deviation, and pattern standard deviation), and P100 amplitude were significantly worse in eyes with NAION than those in healthy eyes (Table 2, P < 0.05).
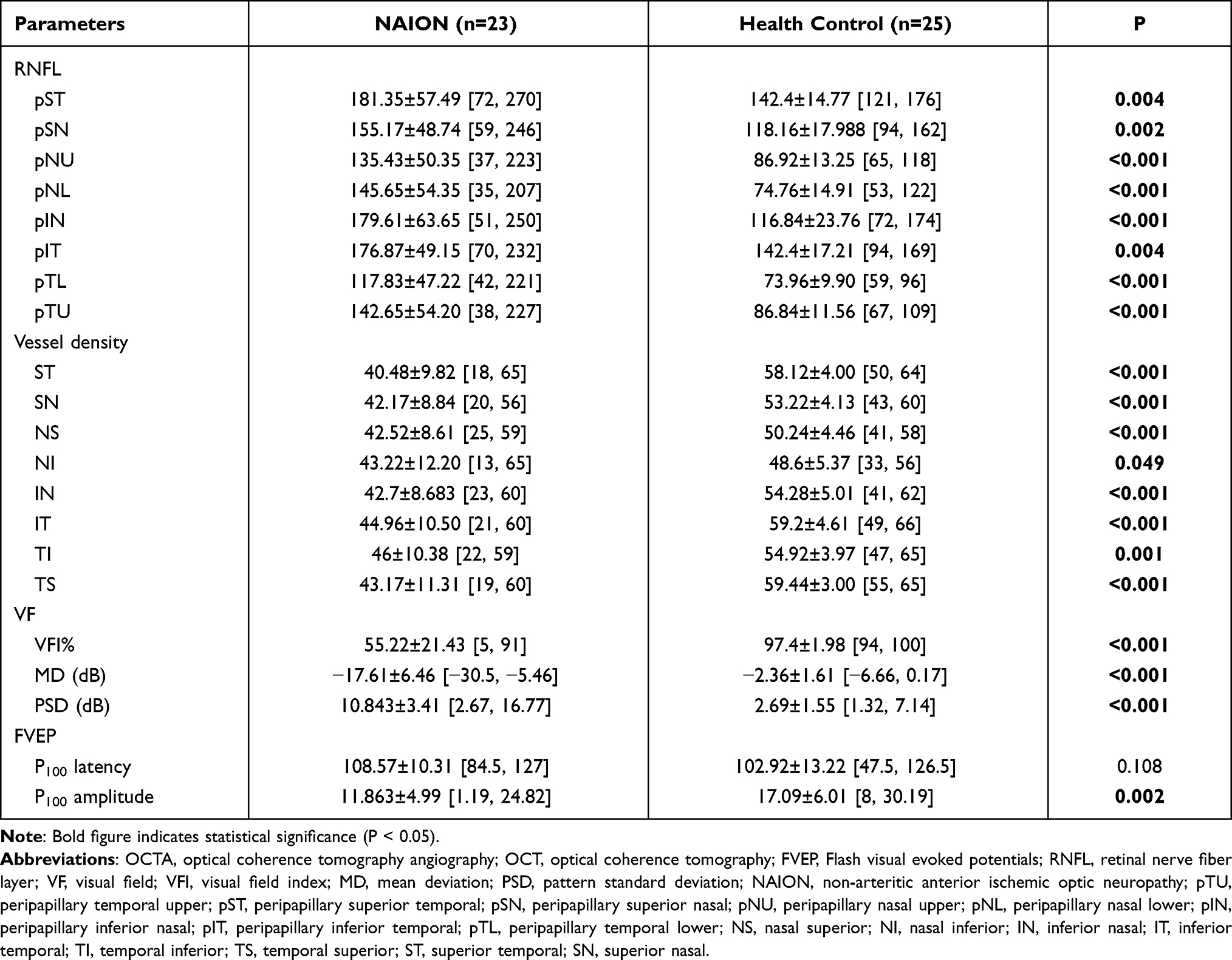 |
Table 2 OCT and OCTA Parameters of the NAION and Control Groups |
The CHI-NEI-VFQ-25 sub-scales scores of eyes with NAION are shown in Table 3. The sub-scales, that exhibited the lowest scores, were driving (32.61 ± 42.04), general health (54.35 ± 17.92), role difficulties (60.87 ± 28.28), social functioning (61.59 ± 7.42), and general vision (66.96 ± 15.50). In contrast, mental health, ocular pain, and dependency were moderately affected, while the remaining sub-scales (near activities, distance activities, color vision, and peripheral vision) were only slightly affected. The composite score for eyes with NAION was equal to 77.57 ± 11.85. Patients with NAION exhibited significantly lower scores in comparison with healthy controls, regarding general vision, ocular pain, near activities, distance activities, social functioning, mental health, role difficulties, dependency driving, color vision, peripheral vision, and composite score of CHI-NEI-VFQ-25 (P < 0.05).
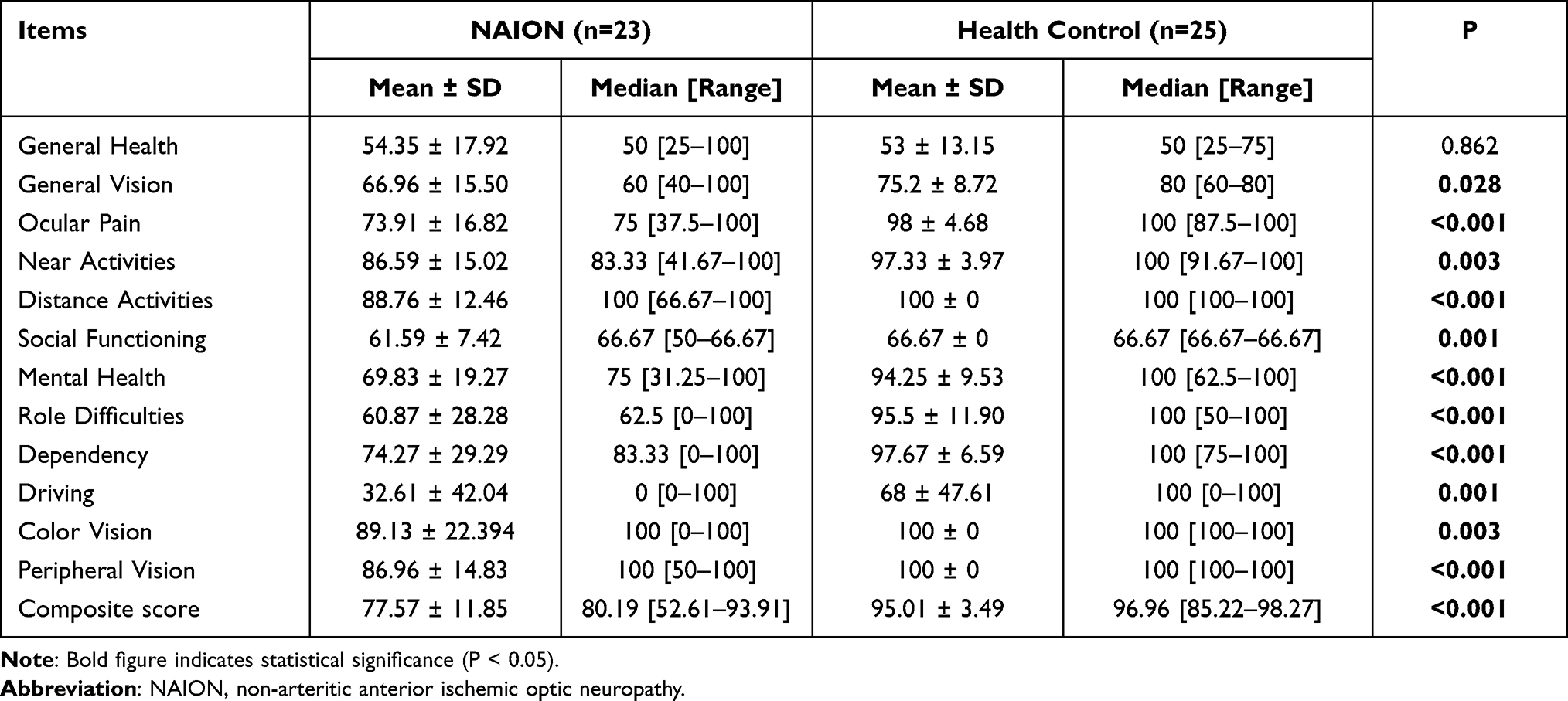 |
Table 3 Mann–Whitney Test Results for the CHI-NEI-VFQ-25 Subscale and Composite Scores |
Table S1 depicts potential associations between RNFL, VD, visual field, and FVEP parameters and VR-QoL among eyes with NAION. The partial correlation coefficient showed that VD in ST was associated with decreased general health scores (ρ = −0.533, P = 0.023); RNFL in pIN (ρ = 0.474, P = 0.047) and VD in TS (ρ = 0.502, P = 0.034) were associated with ocular pain. Near activities were associated with RNFL in pTL (ρ = - 0.484, P = 0.042). Furthermore, VD in NI (ρ = 0.552, P = 0.018) and IN (ρ = 0.596, P = 0.009) were both associated with mental health scores, respectively.
Discussion
To the best of our knowledge, this is the first report on the structure-function characteristics and VR-QoL in patients with NAION. Main findings of the present case-control study suggest that there were significant differences in VR-QoL in patients with NAION compared with healthy control. Furthermore, these differences appeared to be correlated with some parameters of RNFL and VD domains. It is also noteworthy that the parameters of RNFL, VD, visual field and FVEP were significantly affected by NAION.
NAION comprises a major proportion of optic neuropathy in individuals older than 50 years of age,14,15 but few researches of VR-QoL have performed on these patients. Paolilo et al found that neuromyelitis optica spectrum disorder (NMOSD), as a severe optic neuropathy, is associated with low quality-of-life (QoL) in adults.16 Moreover, another case-control study among thyroid eye disease (TED) patients with or without dysthyroid optic neuropathy (DON) showed that VR-QoL was more severely impaired in TED patients with DON by CHI-NEI-VFQ-25 scores.17 Ashraf et al conducted a cross-sectional analysis, which indicated participants with immunodeficiency virus-related neuroretinal disorder had lower values for the composite score and the following subscales: near vision, distance vision, social functioning, mental health, dependency, driving, color vision, and peripheral vision. However, general vision, ocular pain, and role limitations were not affected by the disease.18 Many previous findings were not considered for potential confounders. Factors, such as education level, income, and comorbid illness may impact VR-QoL significantly,19–21 thus, a case-control study design matching these factors should be considered. In our matched case-control study, NAION significantly decreased VR-QoL in most of the measured parameters, except general health. Notably, all of cases had not received any treatment before inclusion, but the lack of information about the disease course may have biased results. Despite this issue, our findings reflect the reality of the VR-QoL in patients with NAION.
In current study, we observed that NAION patients had significant visual decline, and a decrease in peripapillary VD compared with healthy controls but experienced an increase in peripapillary RNFL, which implied that functional and anatomic changes, existed in NAION patients. Findings were consistent with recent prospective observational study by Aghsaei et al, which indicated that radial peripapillary VD was significantly decreased at acute NAION stage.5 Further, in their study, they also observed the vascular changes from acute NAION to chronic NAION stage. Similarly, radial peripapillary VD was significantly lower in eyes with chronic NAION than healthy eyes although recovered from active disc edema. In contrast, Wang et al retrospective case-control study revealed the NAION group exhibited significantly lower RNFL thicknesses.22 The reason for this discrepancy was due to the reduction of RNFL thickness as the disease progressed toward optic atrophy (late stage). Taken together, the anatomic changes of NAION should be considered as stages of the disease.
This study had several notable advantages. First, we used matched case-control study, which could minimize the bias without the impact of confounders. Second, CHI-NEI-VFQ-25 was used to evaluate VR-QoL, which could more closely mirror the actual practice of visual function. Third, we first investigated the impact of NAION on QoL and analyzed its correlation with functional and anatomic parameters. However, current study has some limitations beyond the inherent flaws of a retrospective case-control study. First, the sample size was relatively small, which may have limited the statistical power. Although we have discussed this difference in RNLF parameters - VRQoL and correlation with retinal parameters can change in atrophic stage of the disease. Future larger scale, longitudinal, cohorts’ studies should be performed to evaluate the QoL in NAION patients. Second, this study was performed in a city hospital and all of the patients in current study were urban inhabitants, thus, our findings may not be generalizable to all the current condition of NAION patients. Third, a self-reported questionnaire to assess the information about socio-demographic characteristics and chronic diseases was used.
Conclusion
In conclusion, patients with NAION may have worse impacts on most domains of CHI-NEI-VFQ-25, except for similar general health in NAION patients compared to healthy control. There was significant changes in functional and anatomic parameters among eyes with NAION, and some of them correlated with VR-QoL. These findings on elder adults make NAION prevention to be more of a solution to a problem, and also provide important information to better understand the VR-QoL of NAION.
Data Sharing Statement
The data used for the preparation of this manuscript can be available from the corresponding author (L.L.) with formal request.
Acknowledgments
We are grateful to the patients of Non-arteritic Anterior Ischemic Optic Neuropathy and controls who have participated. We also appreciate the data support and research assistance provided by the hospital’s information center and medical examination center.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Daudin JB, Bluwol E, Chaine G, Rohart C. Artérite à cellules géantes révélée par des nodules cotonneux. [Cotton-wool spots as first ocular manifestation of giant cell arteritis]. J Fr Ophtalmol. 2006;29(10):e28. French. doi:10.1016/s0181-5512(06)73912-2
2. Hayreh SS, Zimmerman MB. Nonarteritic anterior ischemic optic neuropathy: natural history of visual outcome. Ophthalmology. 2008;115(2):298–305 e292. doi:10.1016/j.ophtha.2007.05.027
3. Liu B, Yu Y, Liu W, Deng T, Xiang D. Risk factors for non-arteritic anterior ischemic optic neuropathy: a large scale meta-analysis. Front Med. 2021;8:618353. doi:10.3389/fmed.2021.618353
4. Zhao P, Lv H, Guo P, et al. Altered brain functional connectivity at resting-state in patients with non-arteritic anterior ischemic optic neuropathy. Front Neurosci. 2021;15:712256. doi:10.3389/fnins.2021.712256
5. Aghsaei Fard M, Ghahvechian H, Subramanian PS. Follow-up of nonarteritic anterior ischemic optic neuropathy with optical coherence tomography angiography. J Neuroophthalmol. 2021;41(4):e433–e439. doi:10.1097/WNO.0000000000000997
6. Fu Z, Li H, Wang Y. Implication of retrobulbar and internal carotid artery blood-flow-volume alterations for the pathogenesis of non-arteritic anterior ischemic optic neuropathy. BMC Ophthalmol. 2021;21(1):309. doi:10.1186/s12886-021-02075-2
7. Augstburger E, Ballino A, Keilani C, Robin M, Baudouin C, Labbe A. Follow-up of nonarteritic anterior ischemic optic neuropathy with optical coherence tomography angiography. Invest Ophthalmol Vis Sci. 2021;62(2):42. doi:10.1167/iovs.62.4.42
8. Lee Y, Park KA, Oh SY. Changes in the structure of retinal layers over time in non-arteritic anterior ischaemic optic neuropathy. Eye. 2021;35(6):1748–1757. doi:10.1038/s41433-020-01152-y
9. Clemons TE, Chew EY, Bressler SB, McBee W; Age-Related Eye Disease Study Research Group. National eye institute visual function questionnaire in the age-related eye disease study (AREDS): AREDS report no. 10. Arch Ophthalmol. 2003;121(2):211–217. doi:10.1001/archopht.121.2.211
10. Chan CW, Wong D, Lam CL, McGhee S, Lai WW. Development of a Chinese version of the National Eye Institute Visual Function Questionnaire (CHI-VFQ-25) as a tool to study patients with eye diseases in Hong Kong. Br J Ophthalmol. 2009;93(11):1431–1436. doi:10.1136/bjo.2009.158428
11. Lang M, Liu T, Zhu Y, Ye J. Five-year results of refractive outcomes and vision-related quality of life after SMILE for the correction of high myopia. Int J Ophthalmol. 2021;14(9):1365–1370. doi:10.18240/ijo.2021.09.11
12. Zhu M, Yu J, Zhang J, Yan Q, Liu Y. Evaluating vision-related quality of life in preoperative age-related cataract patients and analyzing its influencing factors in China: a cross-sectional study. BMC Ophthalmol. 2015;15:160. doi:10.1186/s12886-015-0150-8
13. Dickersin K, Everett D, Feldon S, et al. The Ischemic Optic Neuropathy Decompression Trial Research Group. Optic nerve decompression surgery for nonarteritic anterior ischemic optic neuropathy (NAION) is not effective and may be harmful. JAMA. 1995;273(8):625–632. doi:10.1001/jama.1995.03520320035038.
14. Johnson LN, Arnold AC. Incidence of nonarteritic and arteritic anterior ischemic optic neuropathy. Population-based study in the state of Missouri and Los Angeles County, California. J Neuroophthalmol. 1994;14(1):38–44. doi:10.1097/00041327-199403000-00011
15. Hattenhauer MG, Leavitt JA, Hodge DO, Grill R, Gray DT. Incidence of nonarteritic anterior ischemic optic neuropathy. Am J Ophthalmol. 1997;123(1):103–107. doi:10.1016/S0002-9394(14)70999-7
16. Paolilo RB, da Paz JA, Apostolos-Pereira SL, Rimkus CM, Callegaro D, Sato DK. Reduced quality of life in a pediatric-onset neuromyelitis optica spectrum disorders cohort. Mult Scler Relat Disord. 2021;56:103252. doi:10.1016/j.msard.2021.103252
17. Du Y, Ye H, Li K, et al. Vision-related quality of life tends to be more severely impaired in patients with dysthyroid optic neuropathy. Curr Eye Res. 2014;39(5):532–536. doi:10.3109/02713683.2013.848901
18. Ashraf DC, May KP, Holland GN, et al. Relationship between human immunodeficiency virus neuroretinal disorder and vision-specific quality of life among people with AIDS. Ophthalmology. 2015;122(12):2560–2567. doi:10.1016/j.ophtha.2015.07.037
19. Varma R, Wu J, Chong K, Azen SP, Hays RD; Los Angeles Latino Eye Study Group. Impact of severity and bilaterality of visual impairment on health-related quality of life. Ophthalmology. 2006;113(10):1846–1853. doi:10.1016/j.ophtha.2006.04.028
20. Cheng HC, Guo CY, Chen MJ, Ko YC, Huang N, Liu CJ. Patient-reported vision-related quality of life differences between superior and inferior hemifield visual field defects in primary open-angle glaucoma. JAMA Ophthalmol. 2015;133(3):269–275. doi:10.1001/jamaophthalmol.2014.4908
21. Deng X, Dong P, Zhang L, et al. Health-related quality of life in residents aged 18 years and older with and without disease: findings from the first provincial health services survey of Hunan, China. BMJ Open. 2017;7(9):e015880. doi:10.1136/bmjopen-2017-015880
22. Wang H, Meng ZY, Li SG, Wang JJ, Sun J, Li HY. Macular evaluation of the retinal and choroidal vasculature changes in anterior ischemic optic neuropathy-a case control study. BMC Ophthalmol. 2018;18(1):341. doi:10.1186/s12886-018-1007-8
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.