")
Back to Journals » Vascular Health and Risk Management » Volume 15
Visceral bed involvement in thromboangiitis obliterans: a systematic review
Received 13 March 2019
Accepted for publication 16 July 2019
Published 15 August 2019 Volume 2019:15 Pages 317—353
DOI https://doi.org/10.2147/VHRM.S182450
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Faeze Fakour,1 Bahare Fazeli2,3
1Immunology and Microbiology Department, Mashhad Azad University of Medical Sceinces, Mashhad, Iran; 2Immunology Research Center, Inflammation and Inflammatory Diseases Division, Immunology Department, School of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran; 3Vascular Independent Research and Education, European Foundation, Department of Angiology, L.Sacco Hospital, Milan, Italy
Abstract: One of the challenges of thromboangiitis obliterans (TAO) management is in the patients whose other vascular beds are involved and it remains a challenge to know whether to pursue invasive procedures or to continue medical treatment for such TAO patients. The aim of this review was to investigate reports of the involvement of the visceral vessels in TAO and the related clinical manifestations, management approaches and outcomes. According to our systematic review, the frequency of published articles, the organs most commonly involved were the gastrointestinal tract, the heart, the central nervous system, the eye, the kidneys, the urogenital system, the mucocutaneous zones, joints, lymphohematopoietic system and the ear. Notably, reports of the involvement of almost all organs have been made in relation to TAO. There were several reports of TAO presentation in other organs before disease diagnosis, in which the involvement of the extremities presented after visceral involvement. The characteristics of the visceral arteries looked like the arteries of the extremities according to angiography or aortography. Also, in autopsies of TAO patients, the vascular involvement of multiple organs has been noted. Moreover, systemic medical treatment could lead to the recovery of the patient from the onset of visceral TAO. This study reveals that TAO may be a systemic disease and patients should be aware of the possible involvement of other organs along with the attendant warning signs. Also, early systemic medical treatment of such patients may lead to better outcomes and reduce the overall mortality rate.
Keywords: thromboangiitis obliterans, Buerger’s disease, visceral vascular bed, ischemia
Introduction
Until recently, thromboangiitis obliterans (TAO) had been known as a recurrent, non-atherosclerotic segmental inflammatory and occlusive peripheral vascular disease with unknown etiology that is typically seen only in young, male smokers.1 The dominant clinical manifestation of TAO is in the extremities and usually in the medium- to small-sized vessels of the lower and upper limbs, which can lead to limb loss.1 Because of the disease’s unknown etiology, no treatment protocol is available for TAO, and management of TAO remains a medical challenge.
Although smoking cessation is known to be an important part of any suggested treatment, merely stopping smoking cannot prevent amputation and limb loss during disease flare-ups.2 Notably, one of the challenges of TAO management is in the patients whose other vascular beds are involved. For instance, in a TAO patient with coronary artery involvement, it remains a challenge to know whether to pursue invasive procedures or to continue medical treatment. In addition, the prevalence of TAO is low in comparison to other peripheral arterial diseases (PADs), even in countries in which TAO is common. Moreover, involvement of the visceral vessels is occasionally seen in TAO, which means that the involvement of other vascular beds is quite rare.
For these reasons, our understating of the involvement of other organs and their clinical manifestations and outcomes is poor. As a result, the aim of this review was to investigate reports of the involvement of the visceral vessels in TAO and the related clinical manifestations, management approaches and outcomes from January 1947 through December 2018.
Literature search
A systematic search for relevant literature published between January 1, 1947 and December 31, 2018 was performed on the PubMed, Science Direct databases and Google Scholar. The search was done in the English language. The reference lists from the retrieved studies were then hand-searched. Search terms included “thromboangiitis obliterans”, “Buerger’s disease”, “Arthritis”, “Skin”, “Cutaneous”, “Nodular erythema”, “Livedo reticularis”, “Erythromelalgia”, “Purpura”, “Renal”, “Kidney”, “Cardiac”, “Coronary”, “Heart”, “Lung”, “Pulmonary”, “Testis”, “Genital”, “Penis”, “ Nervous system”, “Cerebral”, “Ophthalmic”, “Eye”, “Muscle”, “Muscular” “Hearing”, “Ear”, “Carotid”, “Hematology”, “Anemia”, “Lymphadenopathy”, “Bone”, “Skeleton”, “Stomach”, “Liver”, “Spleen”, “Pancreas”, “Bowel”, “Intestine”, “Mesenteric”, “Celiac” with combinations being searched via Boolean operator.
For data extraction, the indices for the diagnosis of TAO from each article were evaluated. Articles whose angiography characteristics or pathology reports did not quite match TAO diagnosis were excluded from our study. We excluded articles for which the full-text was not in English or for which the full-text was inaccessible. The primary data extraction form included the year of publication, author name(s), number of patients, age, chief complaint, duration of disease, smoking status, disease diagnosis, suggested treatment and treatment outcome, all of which were assessed by the two independent reviewers (F.F. and B.F.).
Our search initially identified 210 studies. We checked for duplicates between databases. The remaining studies were further reduced to 173 after screening of the titles and abstracts. Finally, after applying the exclusion criteria, the total number of relevant studies was reduced to 83.
Result
According to our systematic review, 83 articles were included, 78 of which were case reports and 2 of which were case series papers, with the final 3 being original papers. Fifteen articles were published prior to the 1980s, and 68 articles were published after 1980.
According to the frequency of published articles, the organs most commonly involved were (1) the gastrointestinal (GI) tract, (2) the heart, (3) the central nervous system, (4) the eye, (5) the kidneys, (6) the urogenital system, (7) the mucocutaneous zones, (8) joints, (9) lymphohematopoietic system and (10) the ear. The search results for each organ are summarized in the following 10 tables.
Gastrointestinal tract
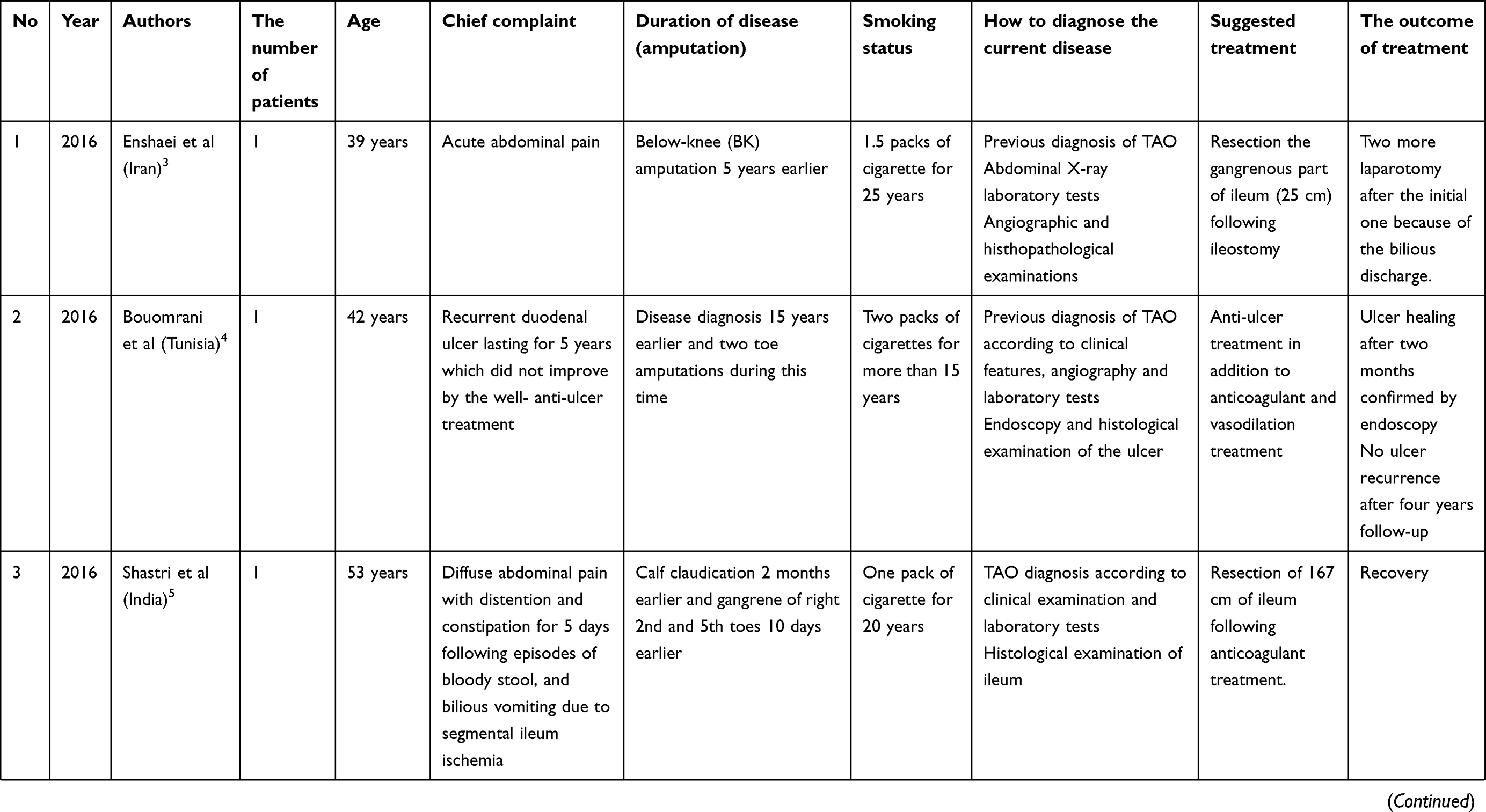
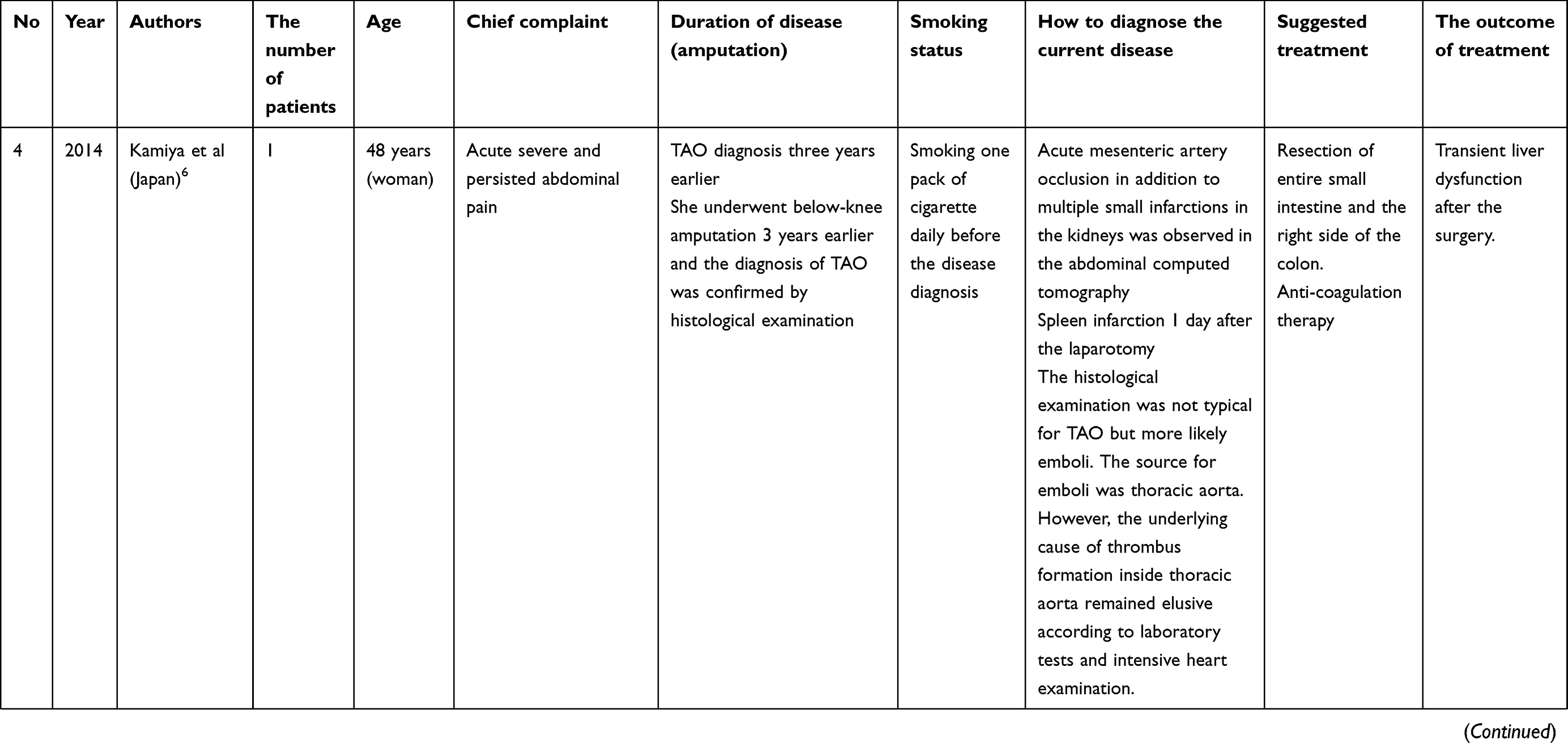
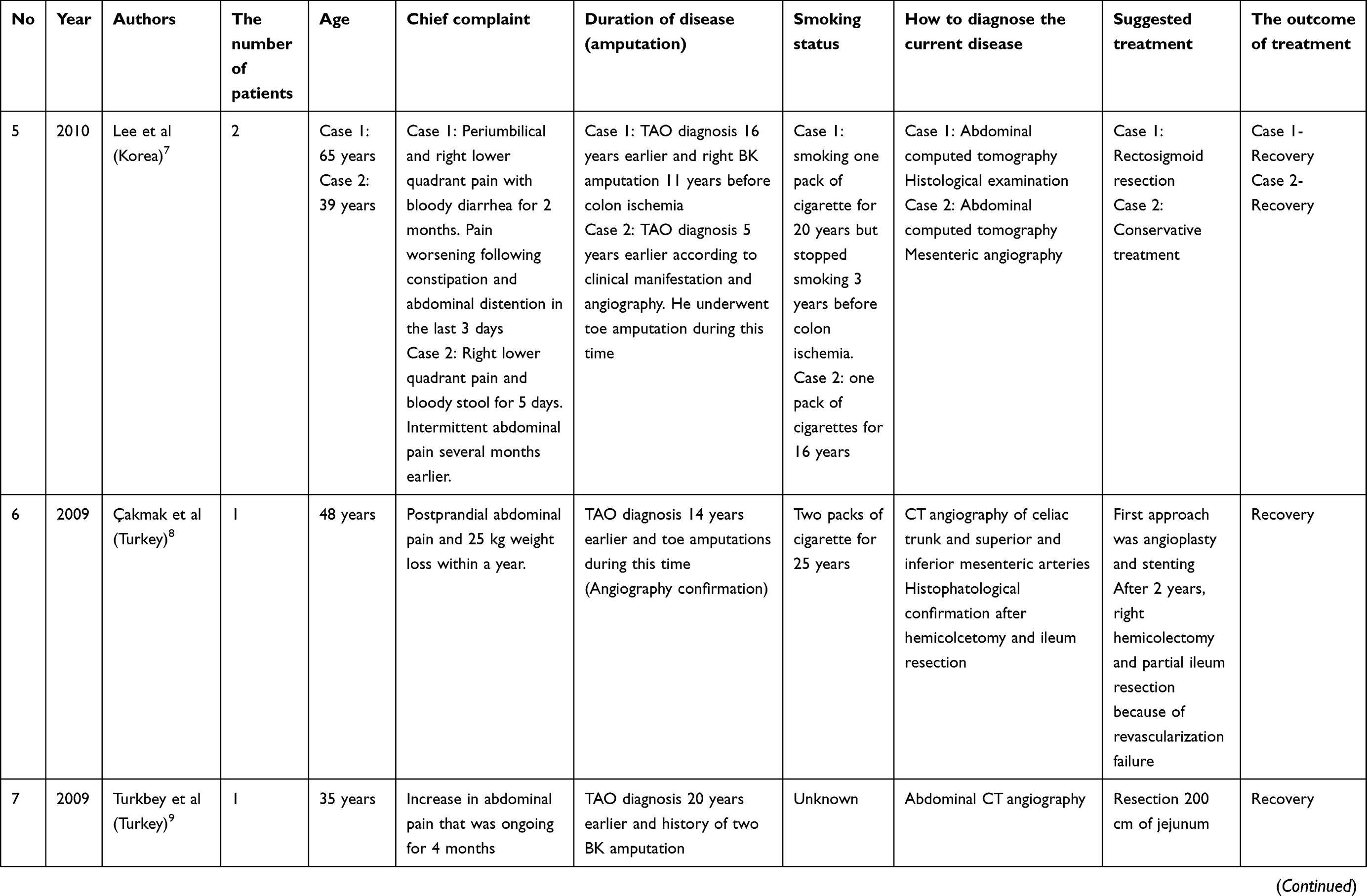
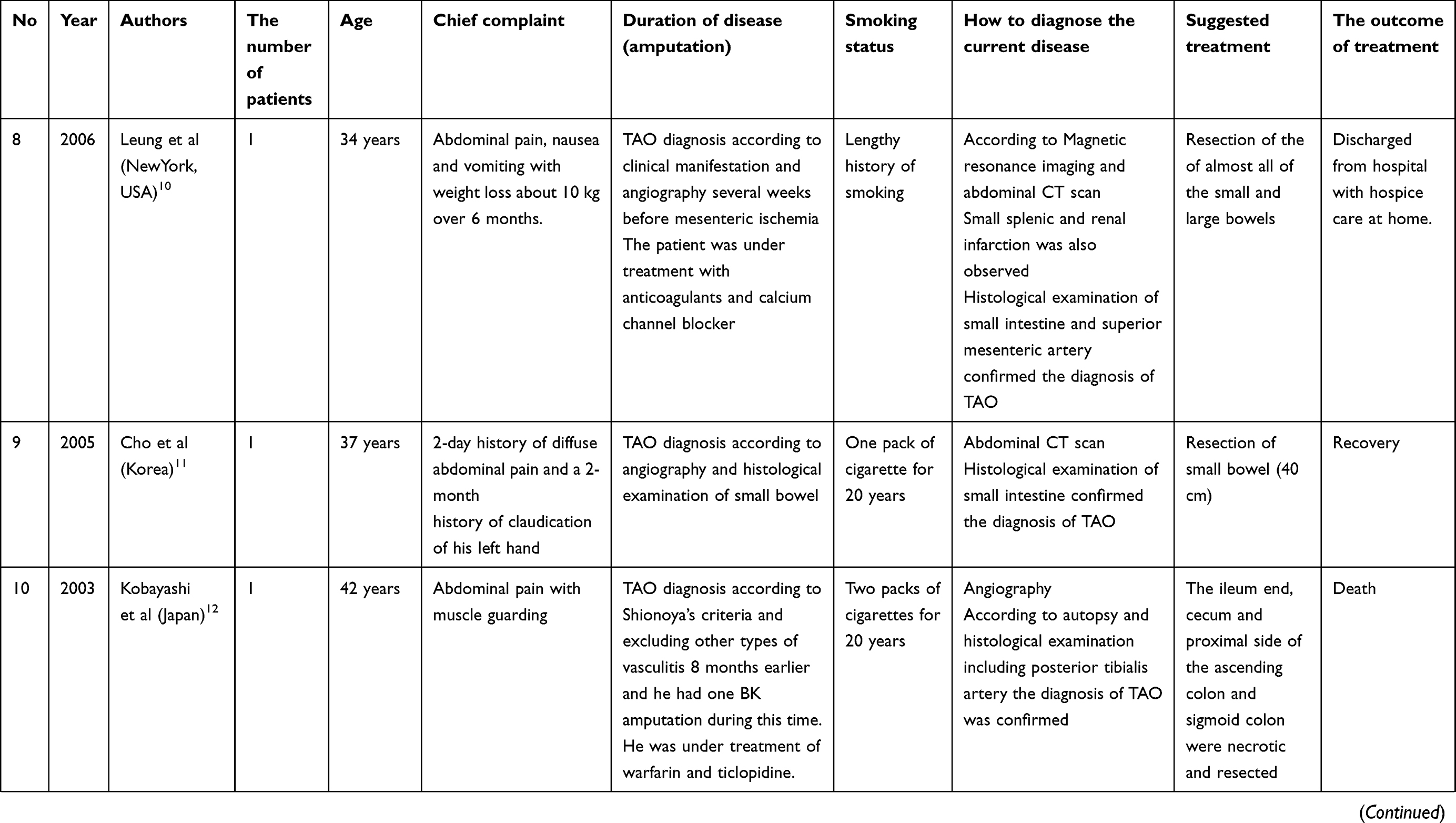
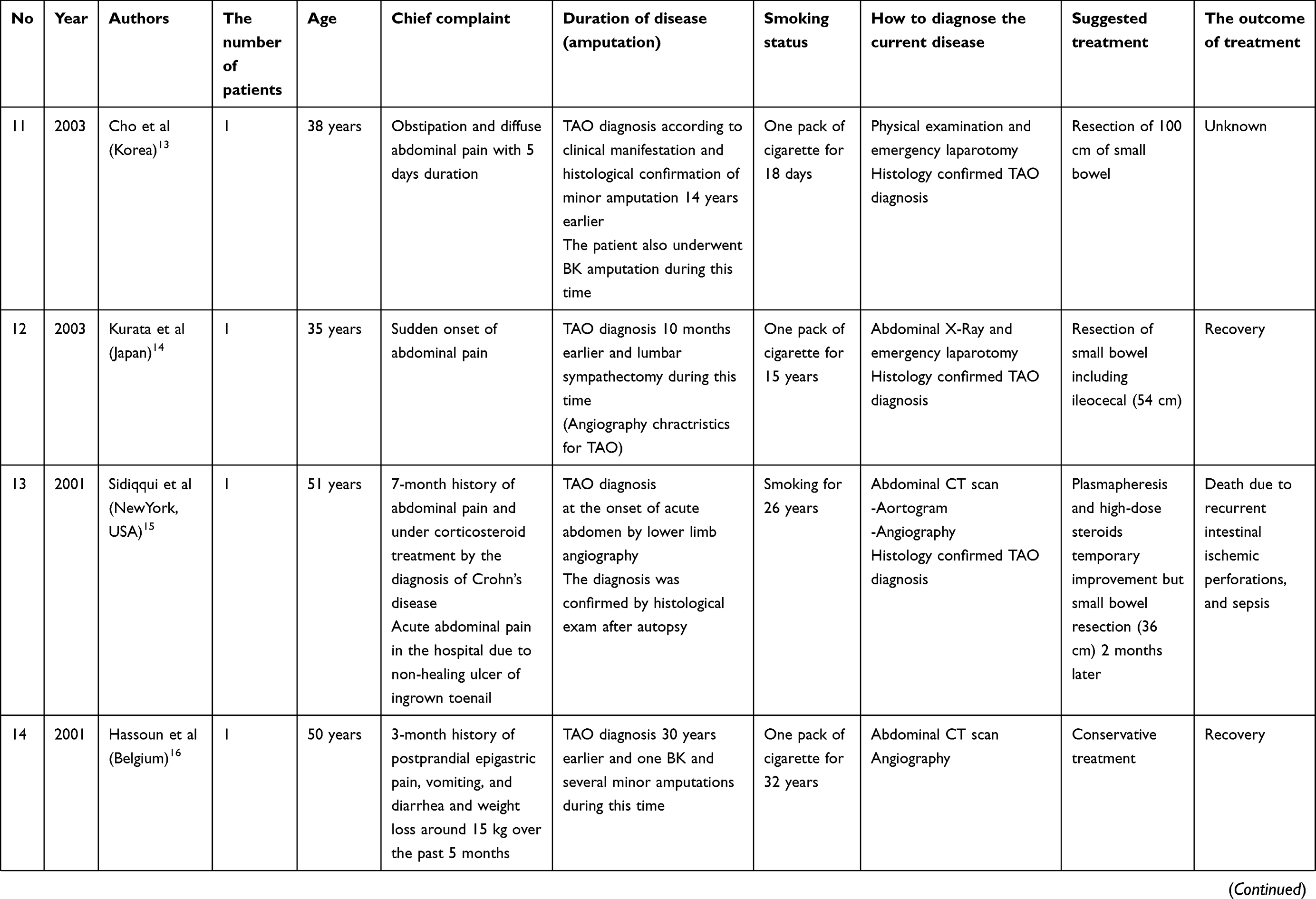
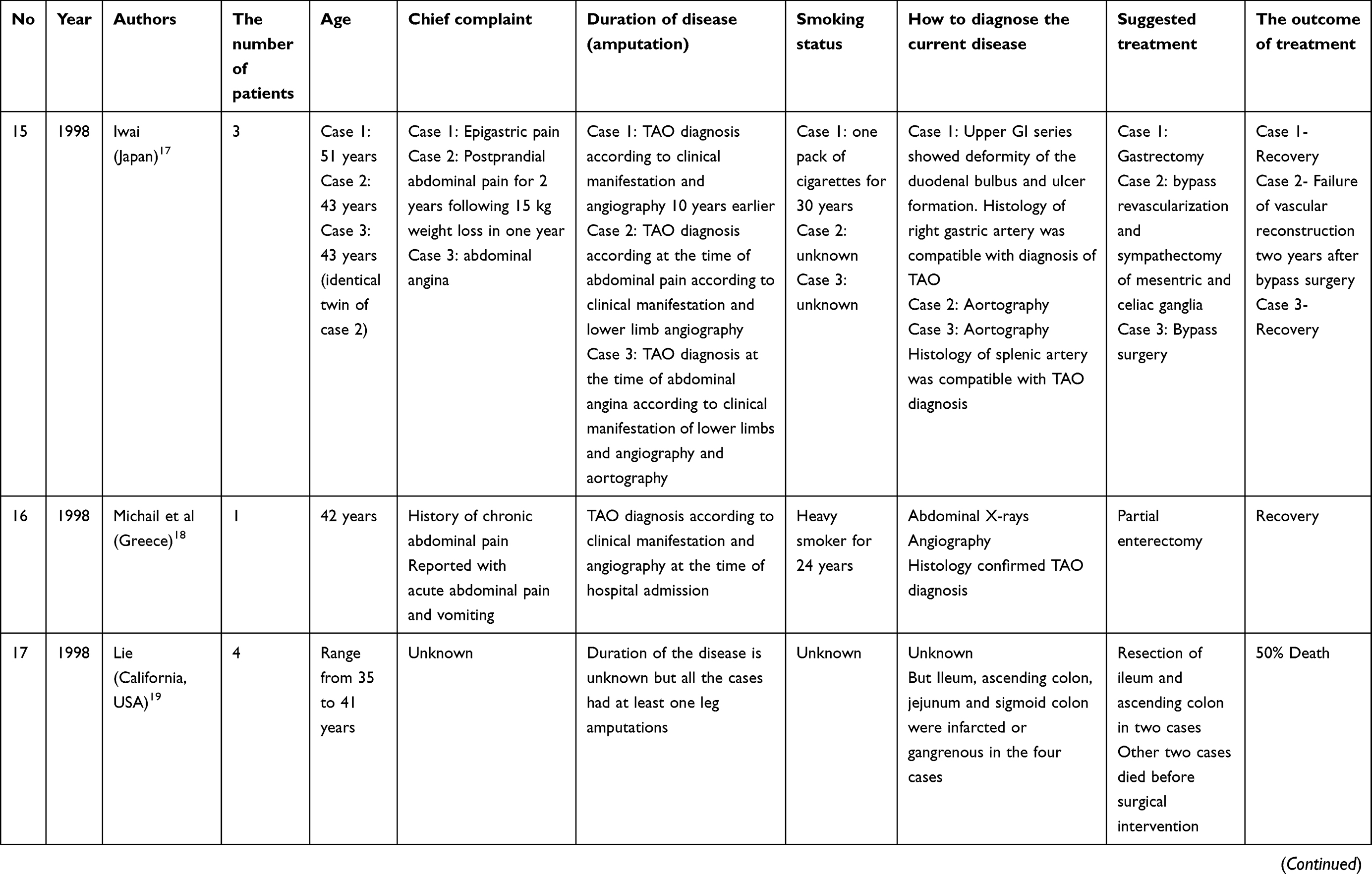
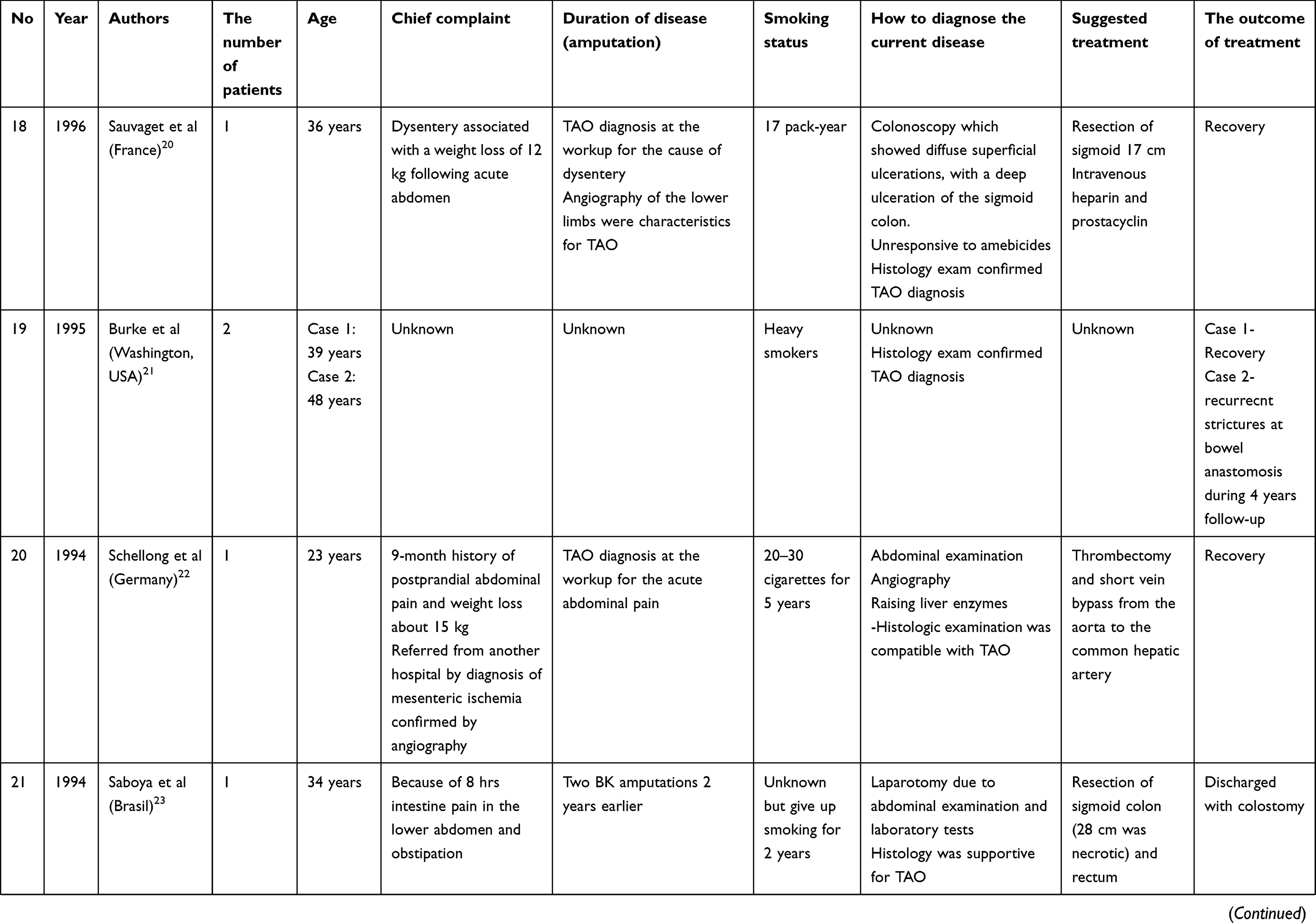
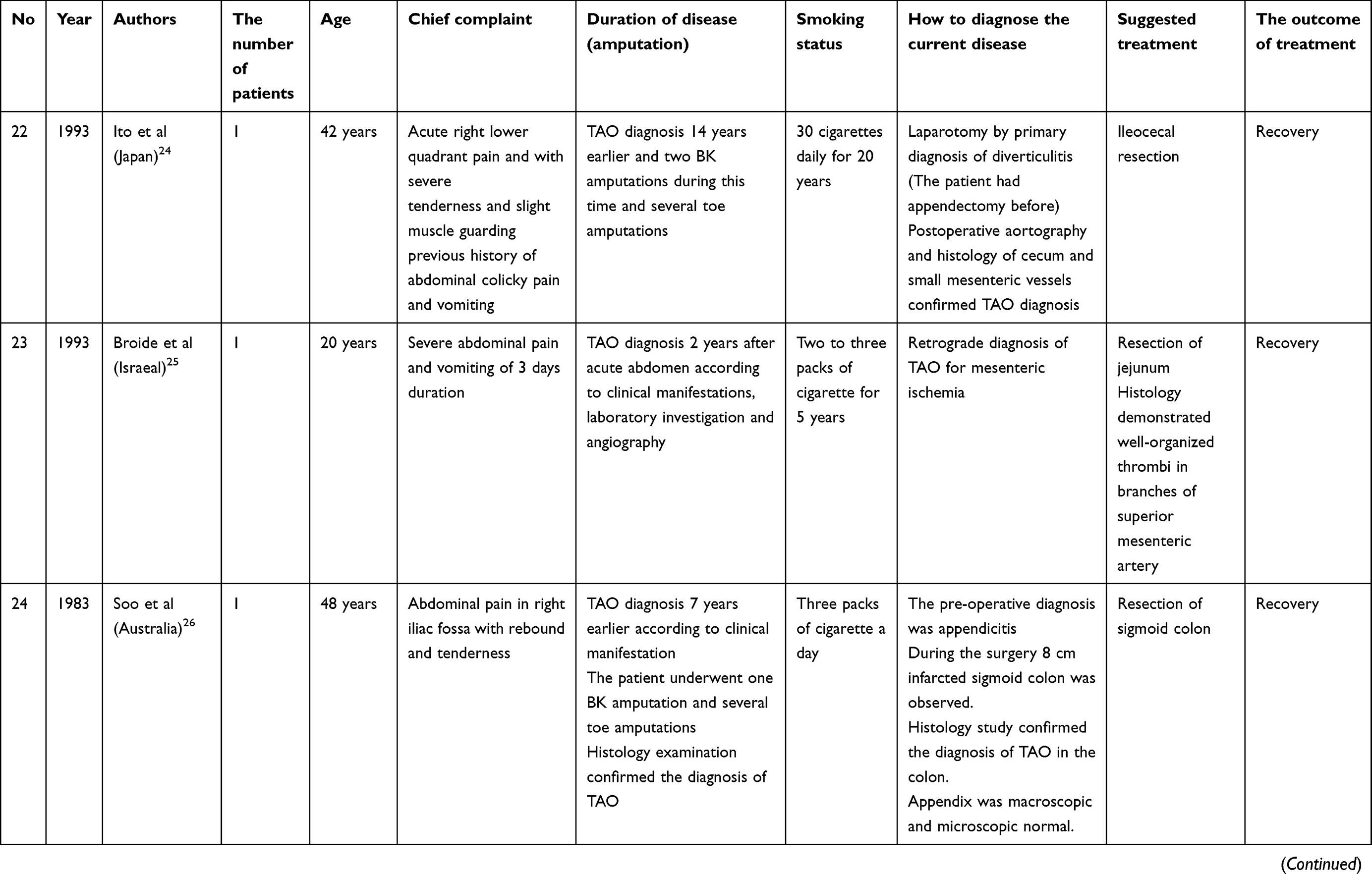
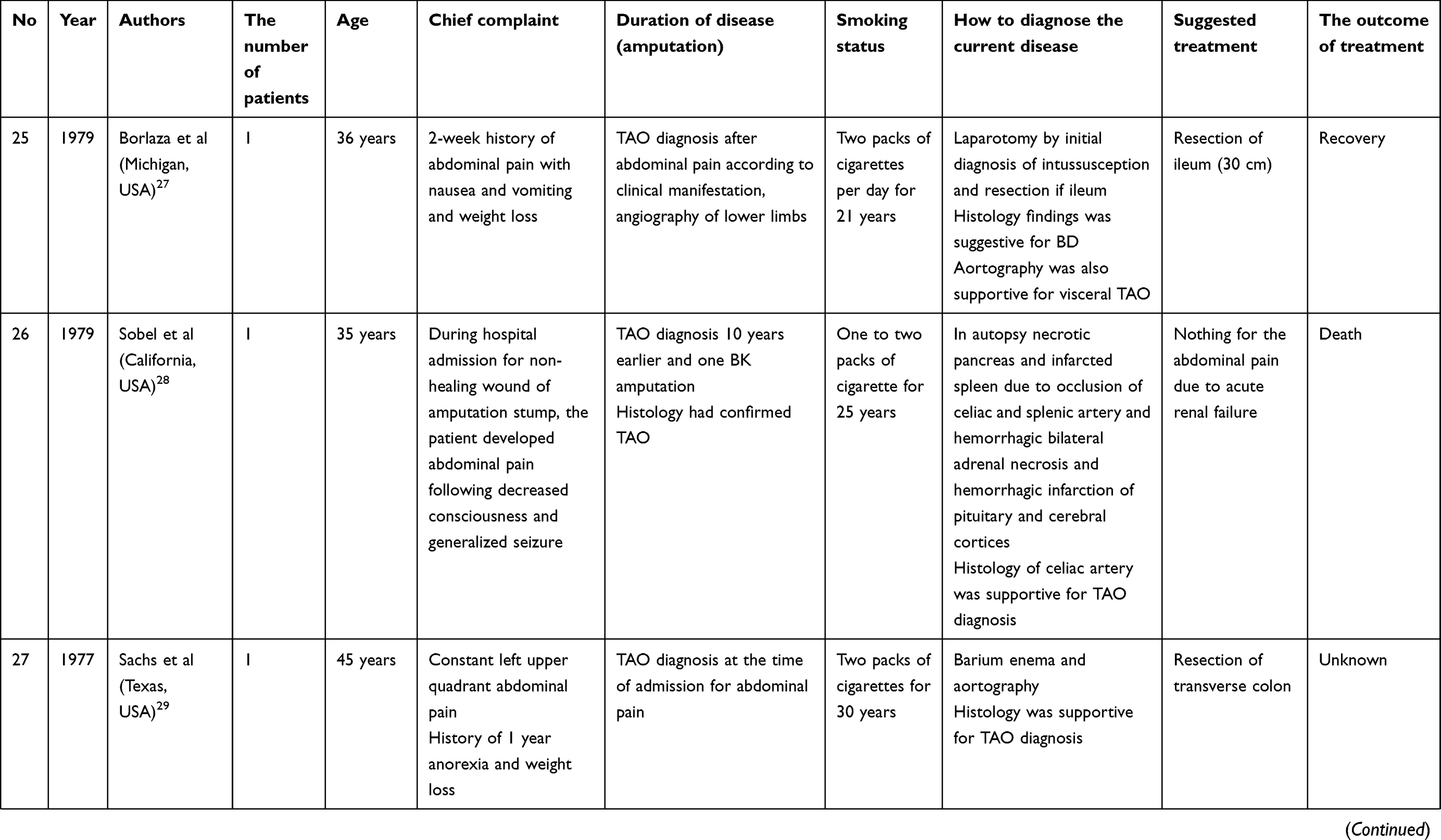
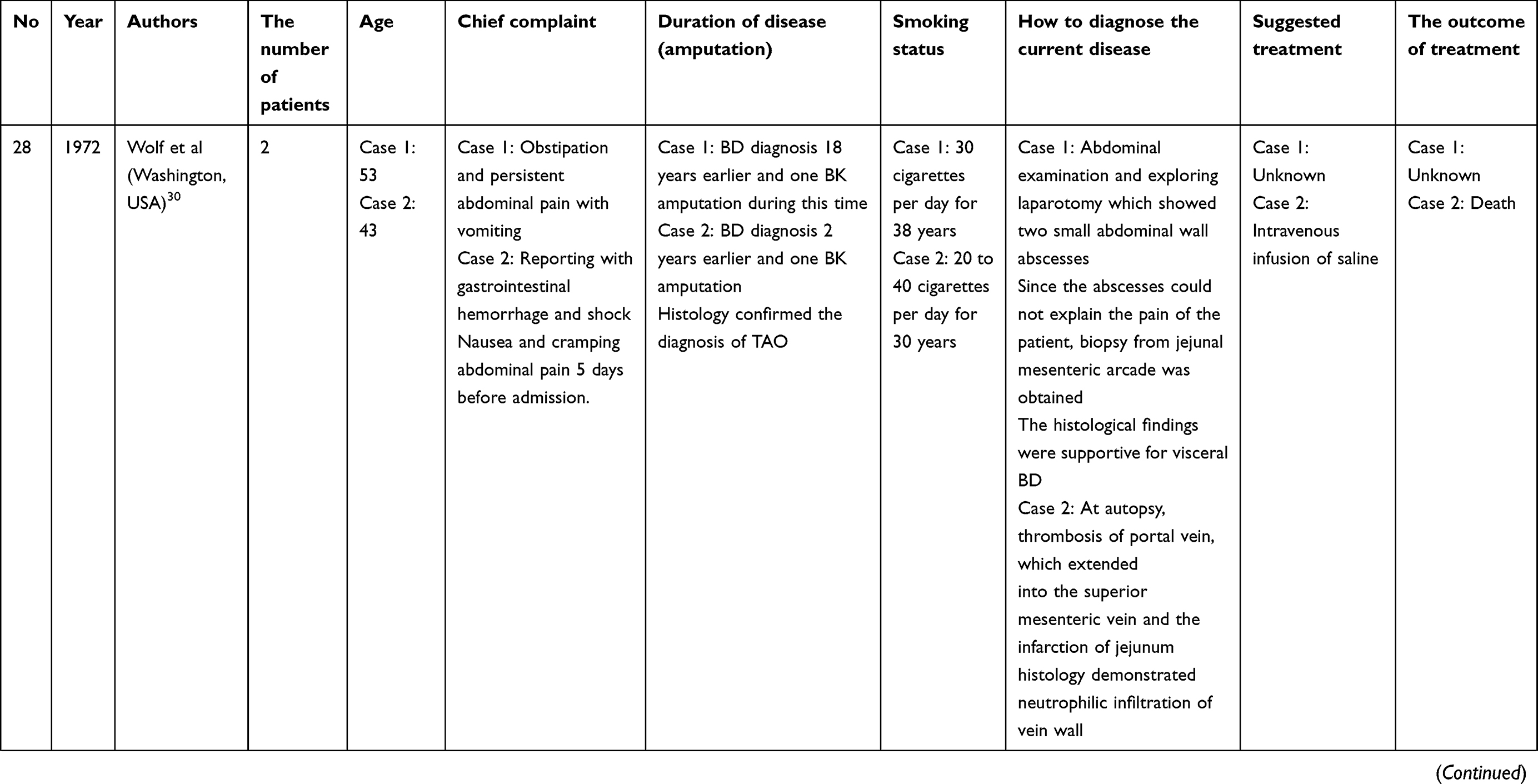
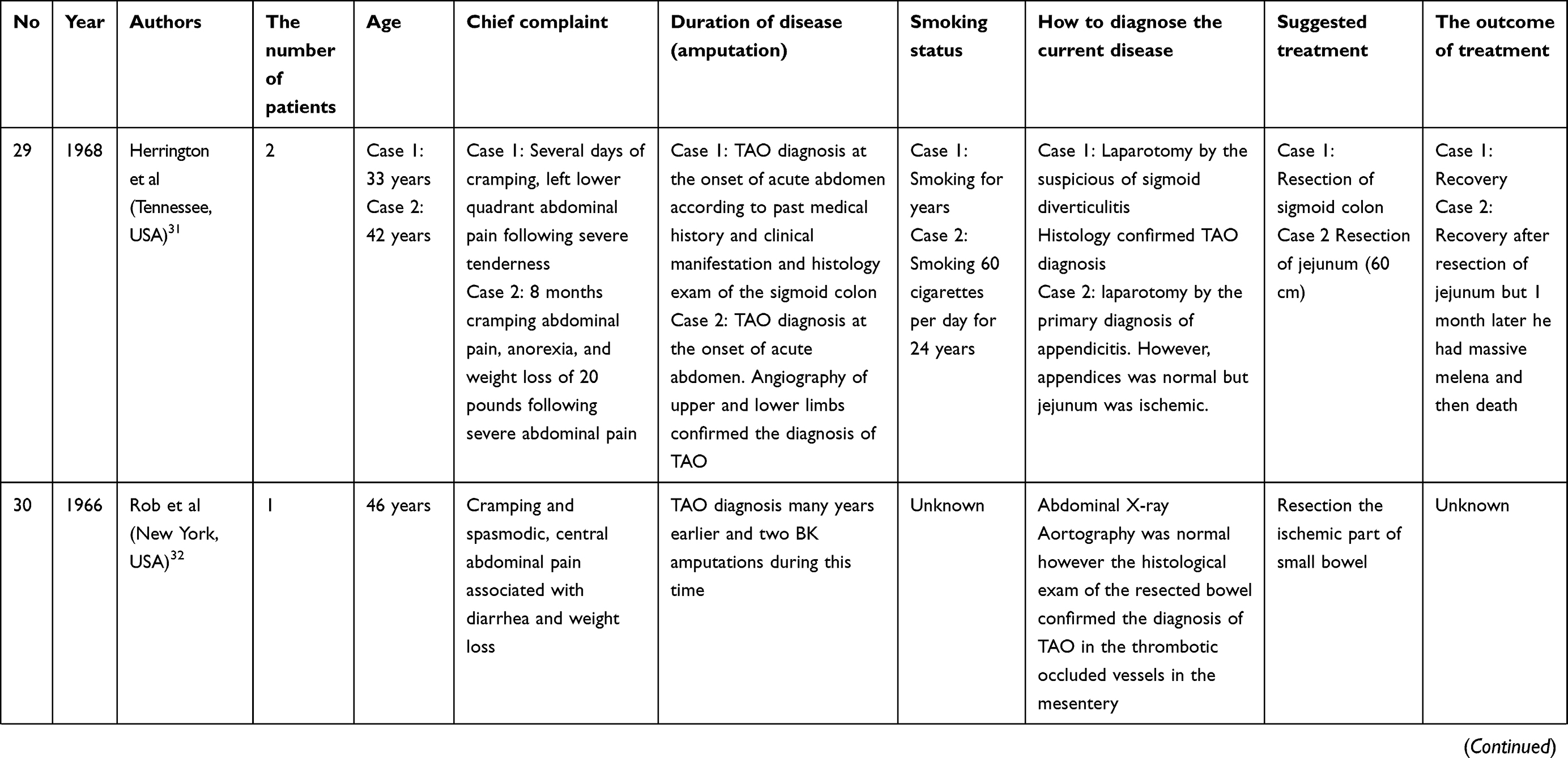
The systematic search returned 45 articles related to the gastrointestinal tract. We were not able to access the full text of nine articles published prior to 1985, and four articles were not in English. Therefore, these 13 articles were excluded from our study. In total, we reviewed 32 articles comprising 41 patients that were published between 1947 and 2016 (Table 1). The mean age of the patients was 41±8 years. The mean number of cigarettes smoked daily was 32±12, and the duration of smoking before mesenteric ischemia was 22±8 years. Only one case was female. In 65% of these cases, TAO diagnosis had occurred approximately 8 years before the mesenteric ischemia. In the remaining cases, TAO was diagnosed at the acute abdomen, and the histology examination of the ischemic bowel confirmed TAO diagnosis. The clinical manifestations of the patients consisted of the onset of diffuse abdominal pain in 44% of the cases, weight loss in 20% of the cases, pain in the right lower abdominal quadrant in 12% of the cases, bloody stool in 10% of the cases, postprandial pain in 8% of the cases and epigastric pain resistant to antiulcer treatment in 6% of the cases.
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
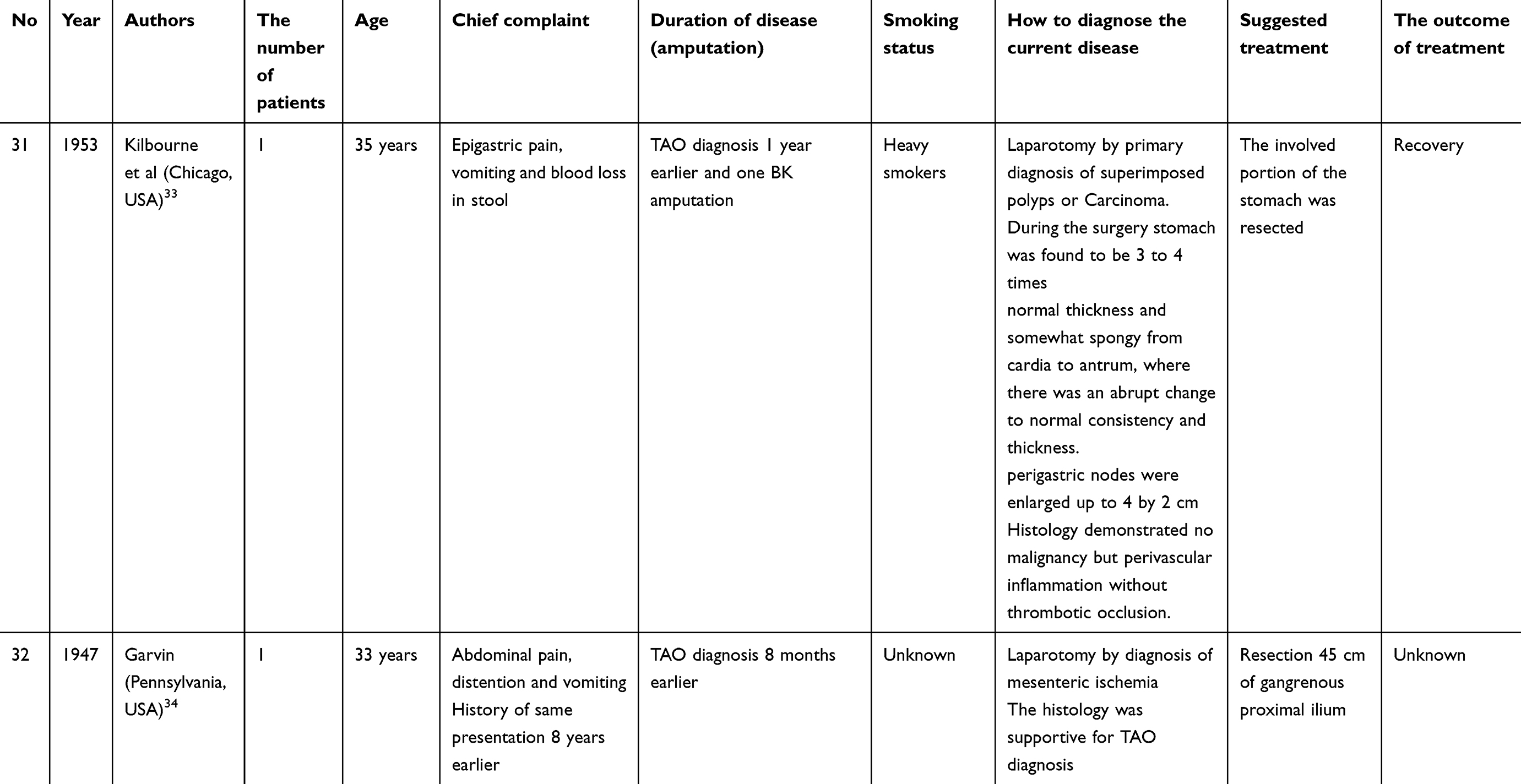 |
Table 1 Data summary of patients with TAO and gastrointestinal tract involvement |
Amongst the included articles, occlusion of the superior mesenteric artery occurred in 53% of the cases, of the inferior mesenteric artery in 12.5% of the cases, of both the superior and inferior mesenteric arteries in 22% of the cases and of the celiac artery and its branches in 12.5% of the cases. Notably, the involvement of the bowels was almost segmental.
However, as observed through aortography, corkscrew collaterals and skip lesions were less prominent than those observed in the lower extremities. The histology study of the visceral vessels and microvessels revealed the same characteristics as the peripheral vessels in TAO. The mortality rate of the patients due to mesenteric ischemia was 16%. Approximately 12% of the patients without signs of peritonitis underwent conservative medical treatment, all of whom improved, although one developed onset of mortal mesenteric ischemia two months after receiving a high dosage of corticosteroids. Endovascular treatment failed in 50% of the four patients in whom it was attempted. The outcome of 12% of the patients has not been reported.
Heart and coronary arteries
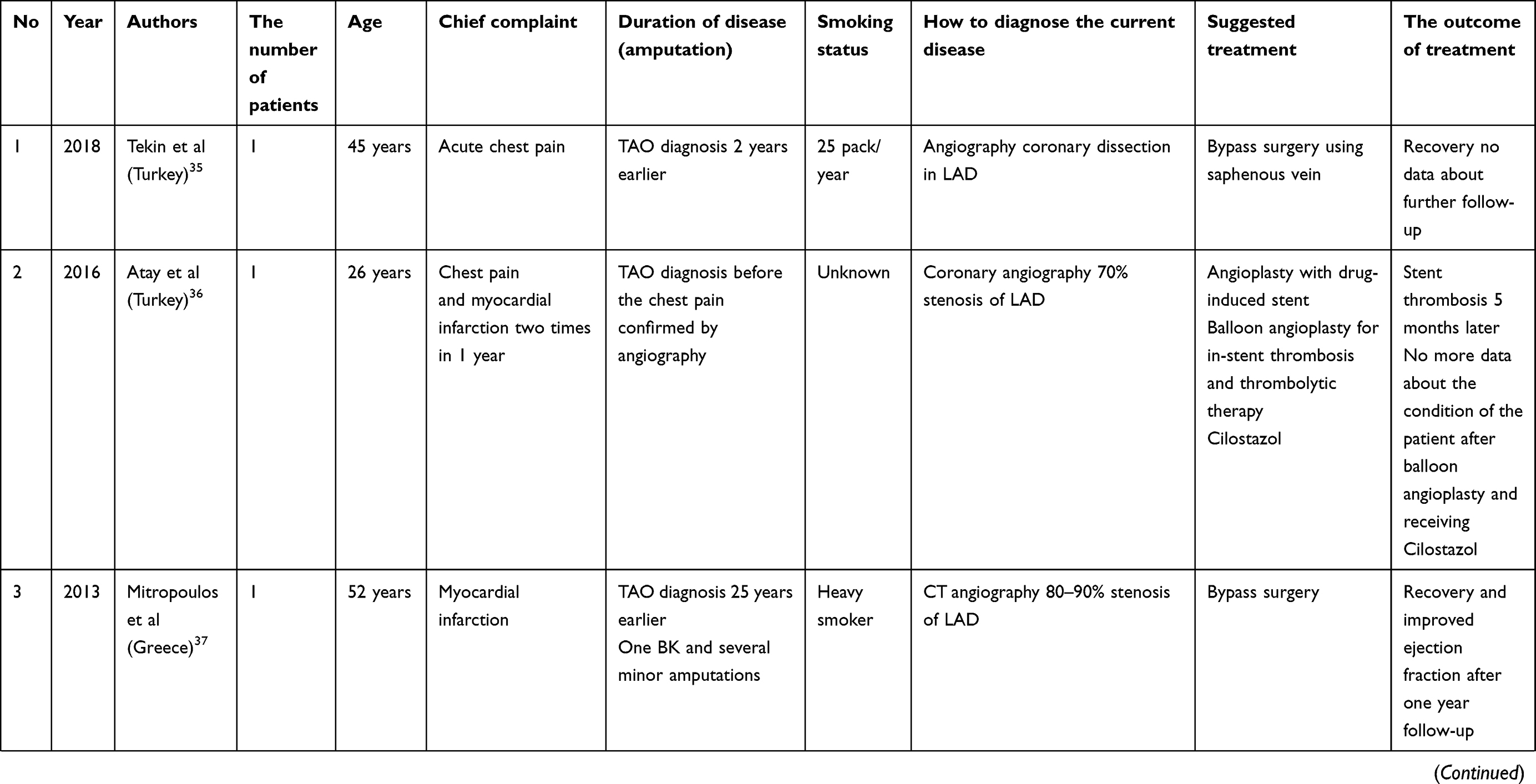
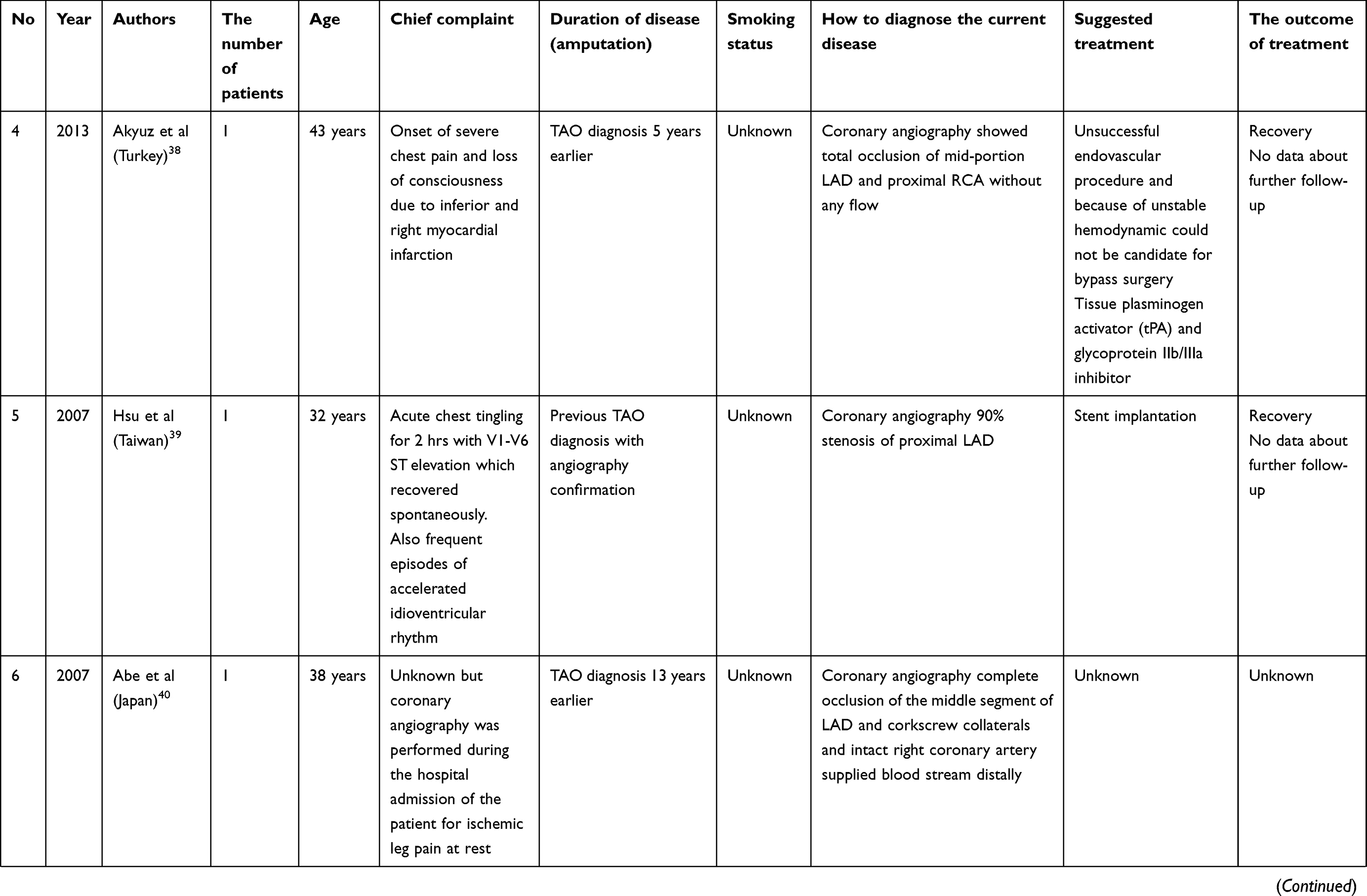
According to a systemic search, we found 20 related articles. We could not have access to the full text of an article in 1986 and four articles were not in English. In one article published in 1977, the diagnosis of TAO was very uncertain according to the clinical manifestations and histology report, and there was no angiography report for that case to support TAO diagnosis. As a result, the article was excluded from our study. In total, 14 articles related to the heart or coronary arteries published between 1985 and 2018 were included, comprising 14 patients (Table 2). The mean age of the patients was 39±10 years. The mean number of cigarettes smoked daily was 27±13 and the duration of smoking before mesenteric ischemia was 21±14 years. Only one patient was female. In 66% of the cases, TAO diagnosis was made approximately 12 years before cardiac event, and in 34% of the cases, TAO diagnosis occurred soon after hospitalization due to cardiac event.
 |
 |
 |
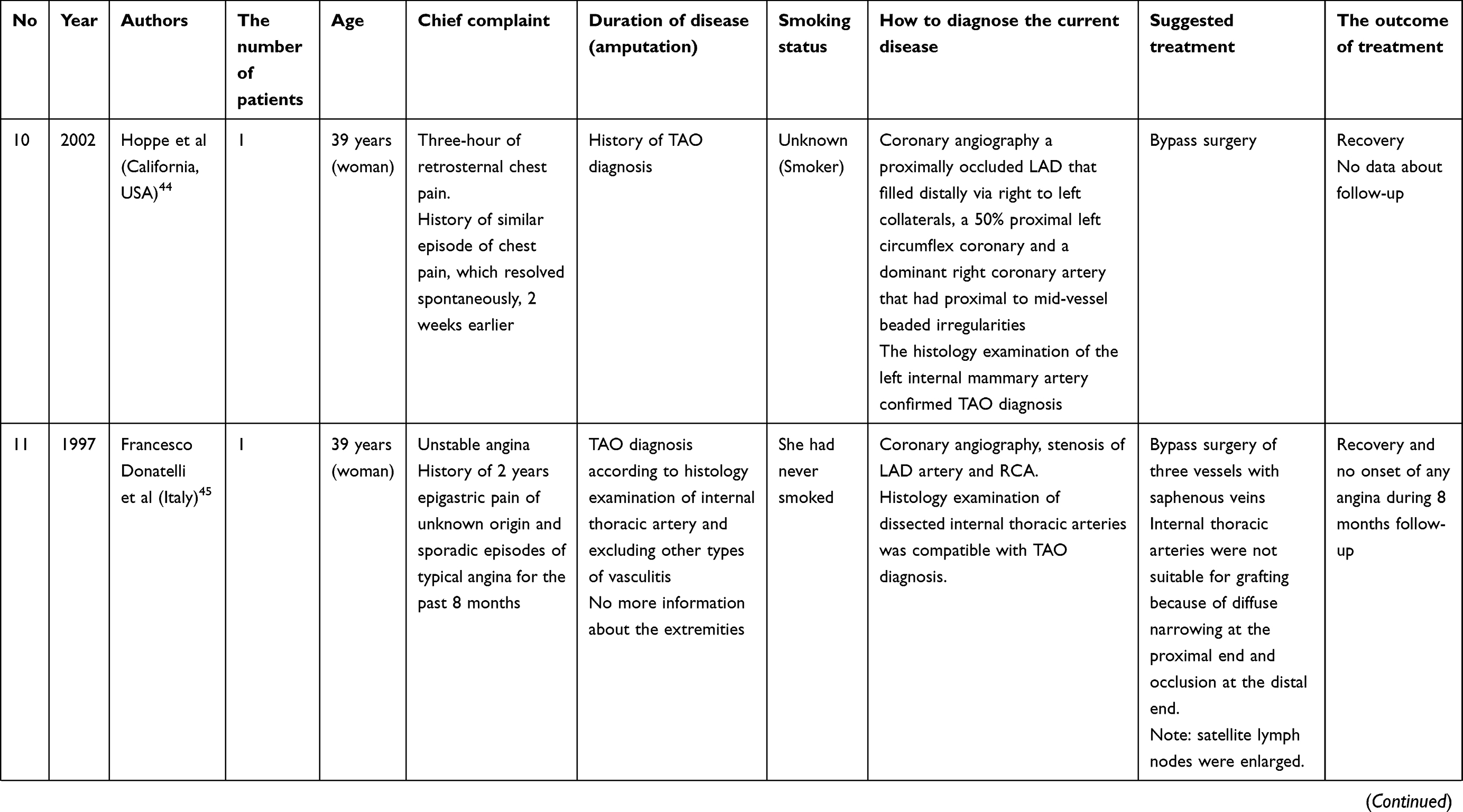 |
Table 2 Data summary of patients with TAO and coronary arteries involvement |
The occlusion of the left anterior descending artery (LAD) and its branches, including the diagonal and circumflex arteries, in addition to right coronary artery (RCA), was observed in 35% of the cases. The involvement of only the LAD occurred in 41% of the cases, of only the RCA in 18% of the cases, and of the circumflex artery in 6% of the cases. In 71% of the cases, coronary artery stenosis was observed, whilst in the remaining cases, complete segmental occlusion and corkscrew collaterals were noted. Approximately 38% of the patients underwent bypass surgery, 38% underwent medical treatment, including intravenous thrombolysis, and 24% underwent endovascular stenting or balloon angioplasty. The saphenous vein was most compatible for bypass surgery in comparison to the internal mammillary artery due to the involvement of that artery. Of the patients who underwent bypass surgery, 80% recovered without bypass graft occlusion due to follow-up occurring approximately 1 year after surgery. About 67% of the vascular stents became occluded between surgery and the 5-month follow-up. All of the patients who received only conservative treatment, including vasodilators, showed improvement, and 67% of the patients who received thrombolytic treatments recovered. None of the patients died as a result of a cardiac event.
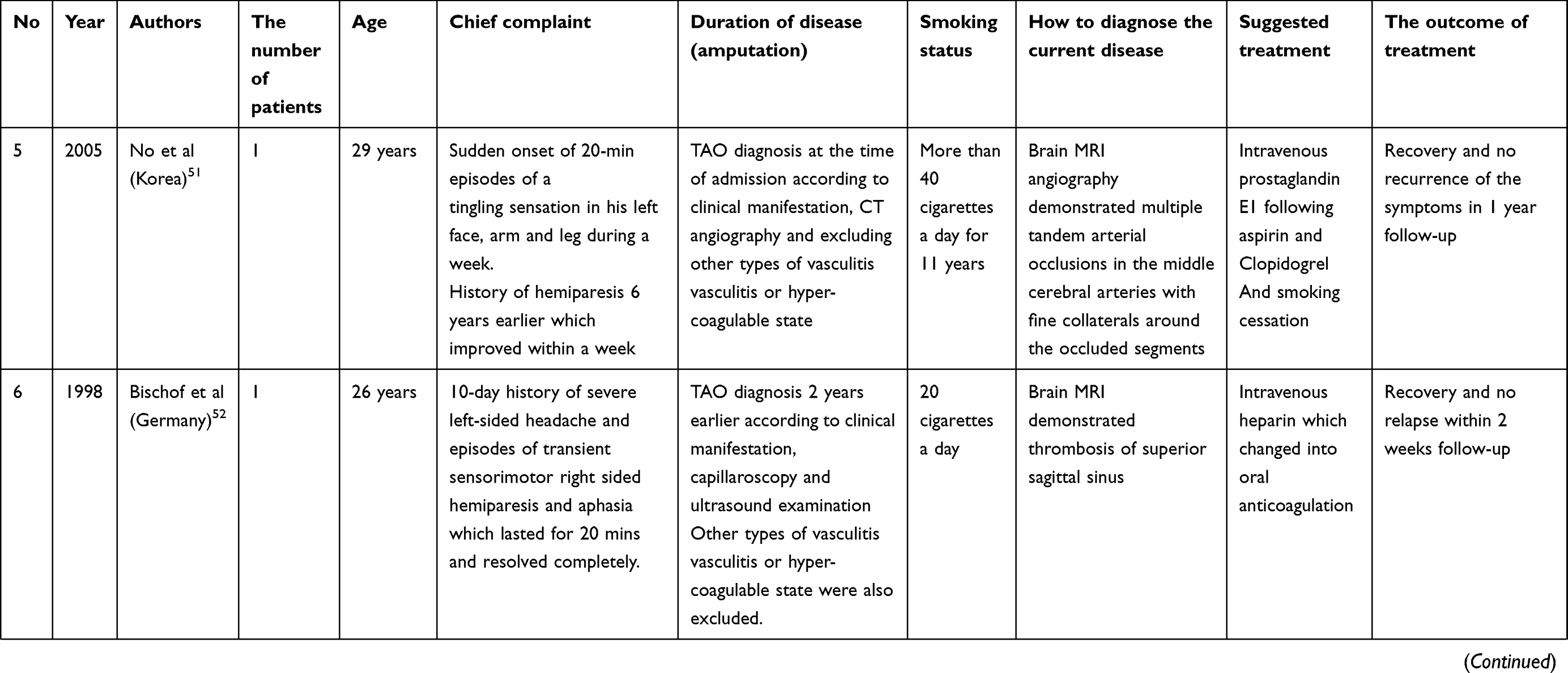
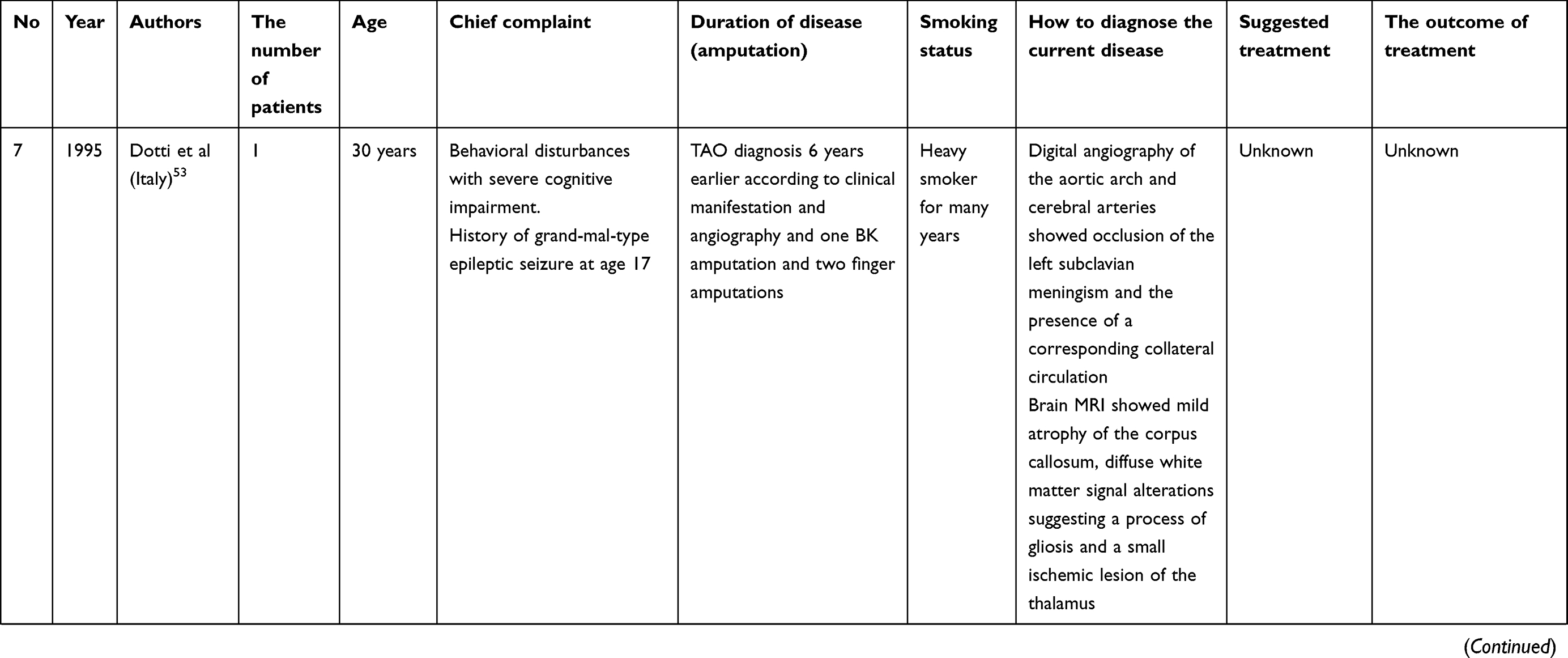
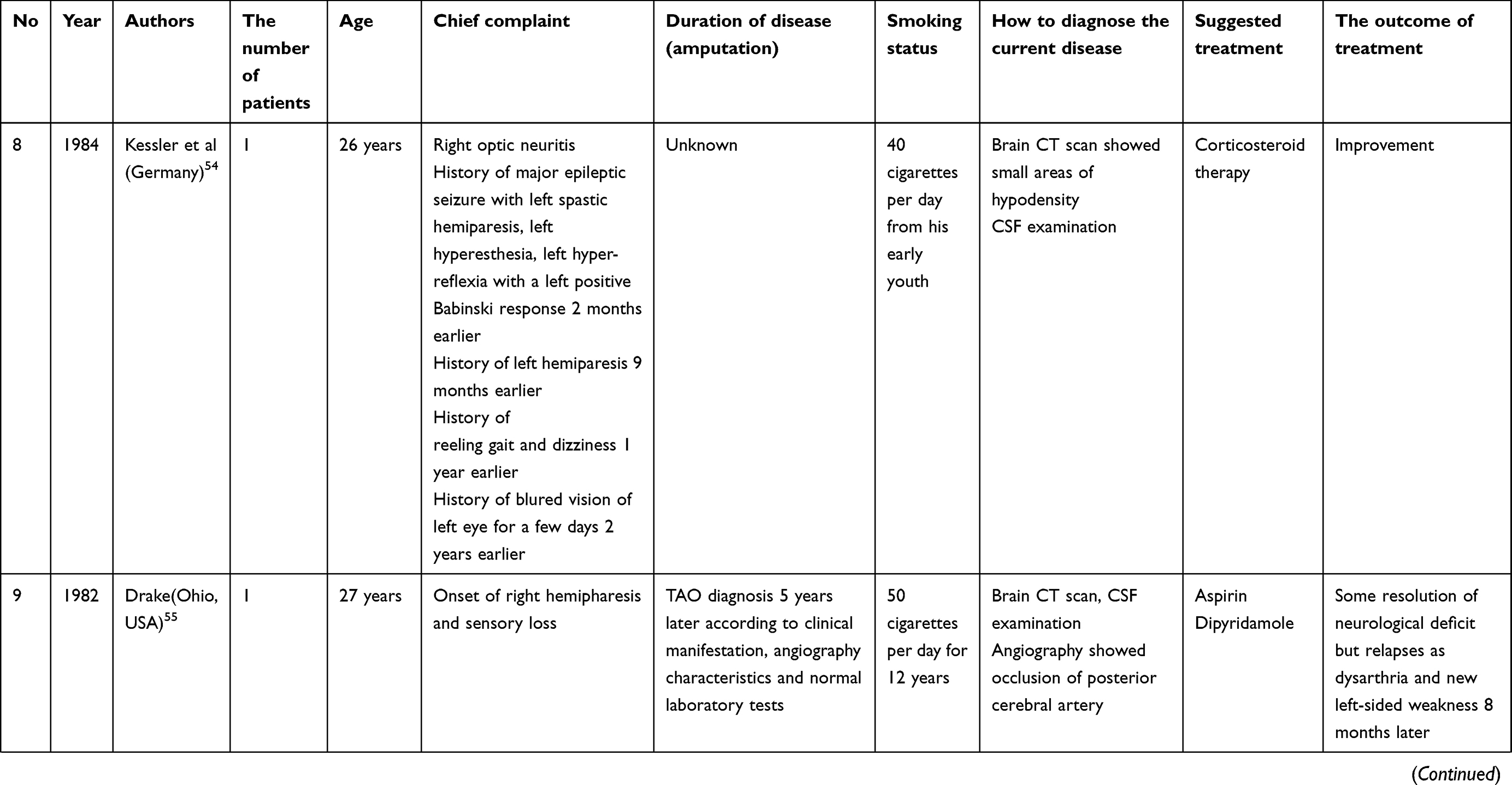
Central nervous system
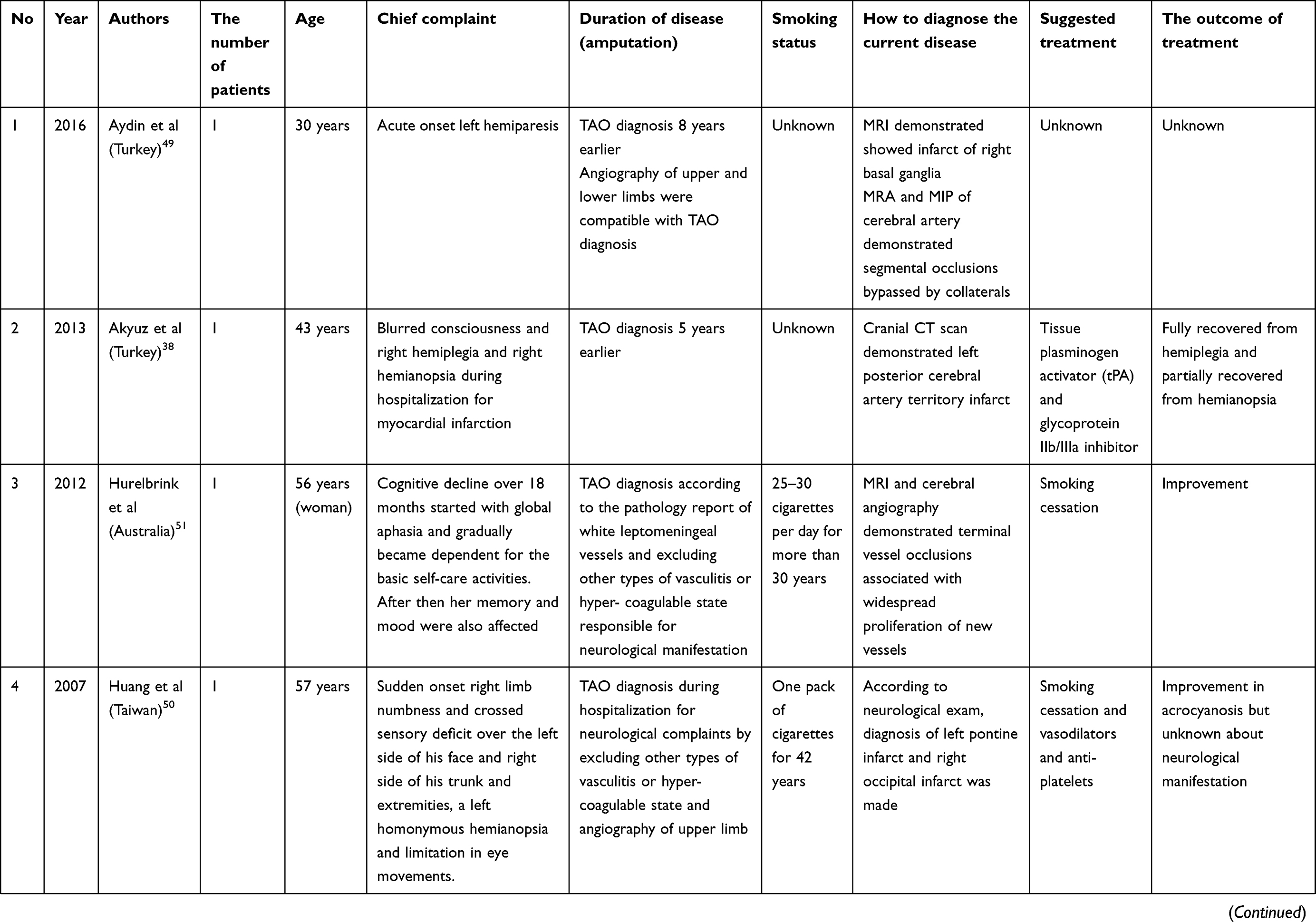
The systematic review revealed 15 articles related to the central nervous system. Four of the articles had been published in a language other than English and were excluded from our study. In total, 12 articles were included that comprised 12 patients and were published between 1952 and 2016 (Table 3). The mean age of the patients was 35±11 years and 81% of the patients were male. The mean number of cigarettes smoked daily was 30±11 and the duration of smoking before mesenteric ischemia was 24±18 years. In 54% of the cases, TAO diagnosis had been made approximately 5 years before neurological complications. In the remaining cases, diagnosis occurred during or after neurological symptoms had developed. The clinical manifestations of the patients consisted of hemiparesis in 27% of the cases, aphasia in 18% of the cases, hemianopia in 13.5% of the cases, behavioral and cognitive impairment in 13.5% of the cases, seizure in 13.5% of the cases, hemiplegia in 10% of the cases, and severe localized headache in 4.5% of the cases. All five patients who completely stopped smoking improved. Vasodilators and anticoagulants did also result in improvement. However, 50% of the patients who received only anticoagulants and anti-platelets showed improvement. The mortality rate due to cerebral ischemia was 8.3%.
 |
 |
 |
 |
Eye
We located six articles related to the eye as a result of the systematic review. One article, published in 1988, reported on three cases of temporal arteritis for which TAO diagnosis was made after histology of the temporal artery. However, in the histology exam, the prominent infiltrating cells were eosinophils. Also, no additional data were available about the clinical manifestation of TAO in the extremities or any angiography examination. Therefore, due to its doubtful diagnosis of TAO, this study was excluded from our review. In total, we included five articles covering five patients that were published between 2006 and 2018 (Table 4). The mean age of the patients was 57±10 years. All cases were male. The mean number of cigarettes smoked daily was 15±7 and the duration of smoking before mesenteric ischemia was 31±11 years. In all cases, eye involvement was observed after TAO diagnosis, which had occurred approximately 18 years earlier. The retinal artery was the most commonly involved artery. Receiving anti-platelets, either with or without corticosteroids, led to partial improvement. However, the treatment strategies and outcomes for 40% of the studies are unknown.
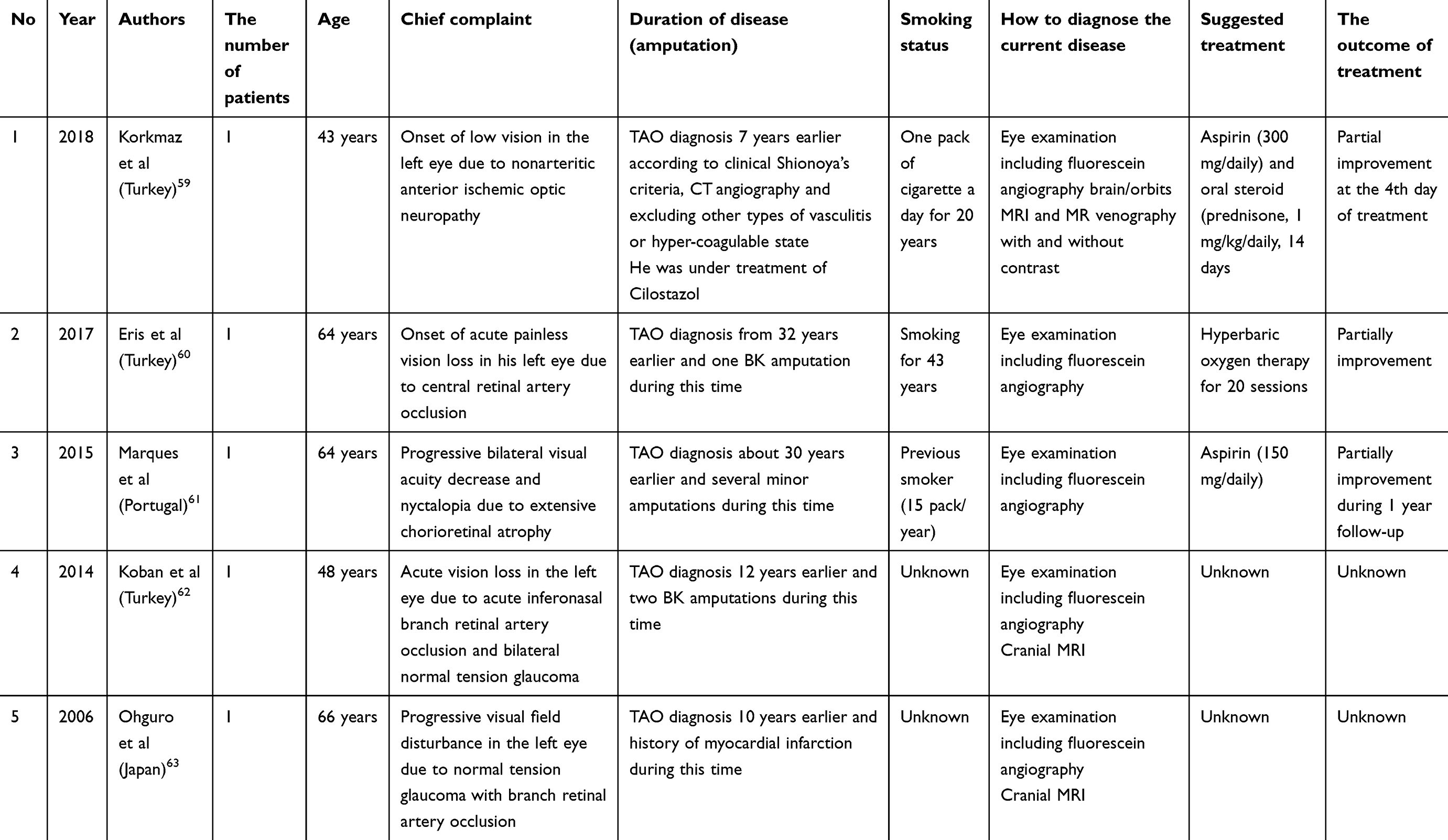 |
Table 4 Data summary of patients with TAO and eye involvement |
Genitalia
According to a systemic search, we found six related articles. One article was not in English; therefore, it was excluded from our study. Totally, five articles were included which consisted of five patients in total and published between 1968 and 2016 (Table 5). The mean age of the patients was 44±20 years and, in 60% of the cases, TAO diagnosis had occurred approximately 13 years before the urogenital events. No pharmaceutical treatment had been pursued for these patients.
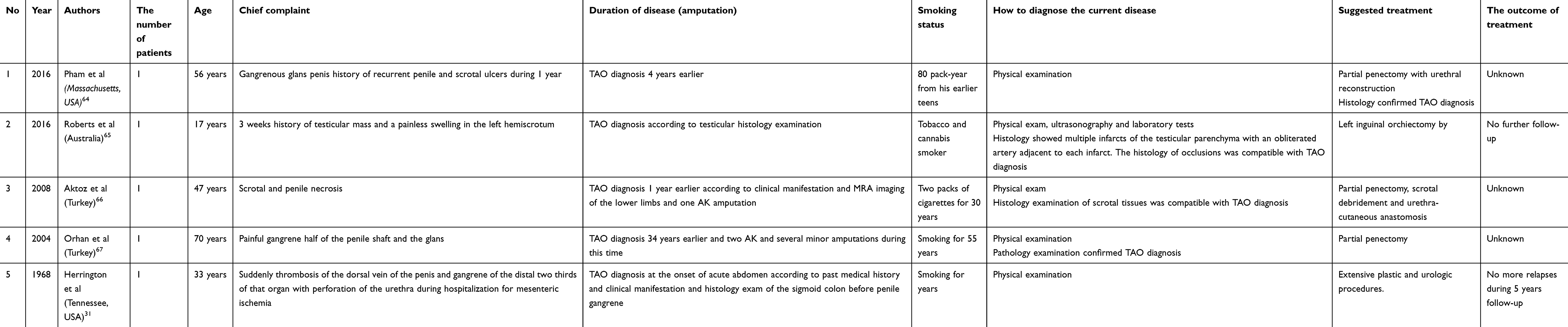 |
Table 5 Data summary of patients with TAO and genitalia involvement |
Kidneys
According to a systemic search, we found seven related articles. We could not have access to the full-text of two articles and one article was not in English. Therefore, they were excluded from our study. Totally, 4 articles included which consisted of 19 patients in total and published between 1959 and 2015 (Table 6). The mean age of the patients was 46±8 and all patients were male. In all cases, renal events had occurred approximately 8 years after TAO diagnosis. The pharmaceutical treatment for these patients is unknown. However, hepato-renal bypass grafting led to the improvement of renal function in one patient.
 |
Table 6 Data summary of patients with TAO and renal involvement |
Mucocutaneous zones
According to a systemic search, we found four related articles which consisted of five patients in total and published between 1980 and 2013 (Table 7). The mean age of the patients was 39±12 years and, in 40% of the cases, skin events had occurred approximately 1.5 years before TAO diagnosis. In 60% of the cases, skin events had occurred approximately 5 years after TAO diagnosis. Stopping smoking and immunosuppressants, including methotrexate and corticosteroids but not vasodilators or anticoagulants, improved the skin lesions.
 |
Table 7 Data summary of patients with TAO and involvement of mucoucutaneous zones |
Lymphohematopoietic system
According to a systemic search, we found six related articles. Three articles were not in English; therefore, they were excluded from our study. Totally, 3 articles were included which consisted of 28 patients in total and published between 1971 and 2016 (Table 8).
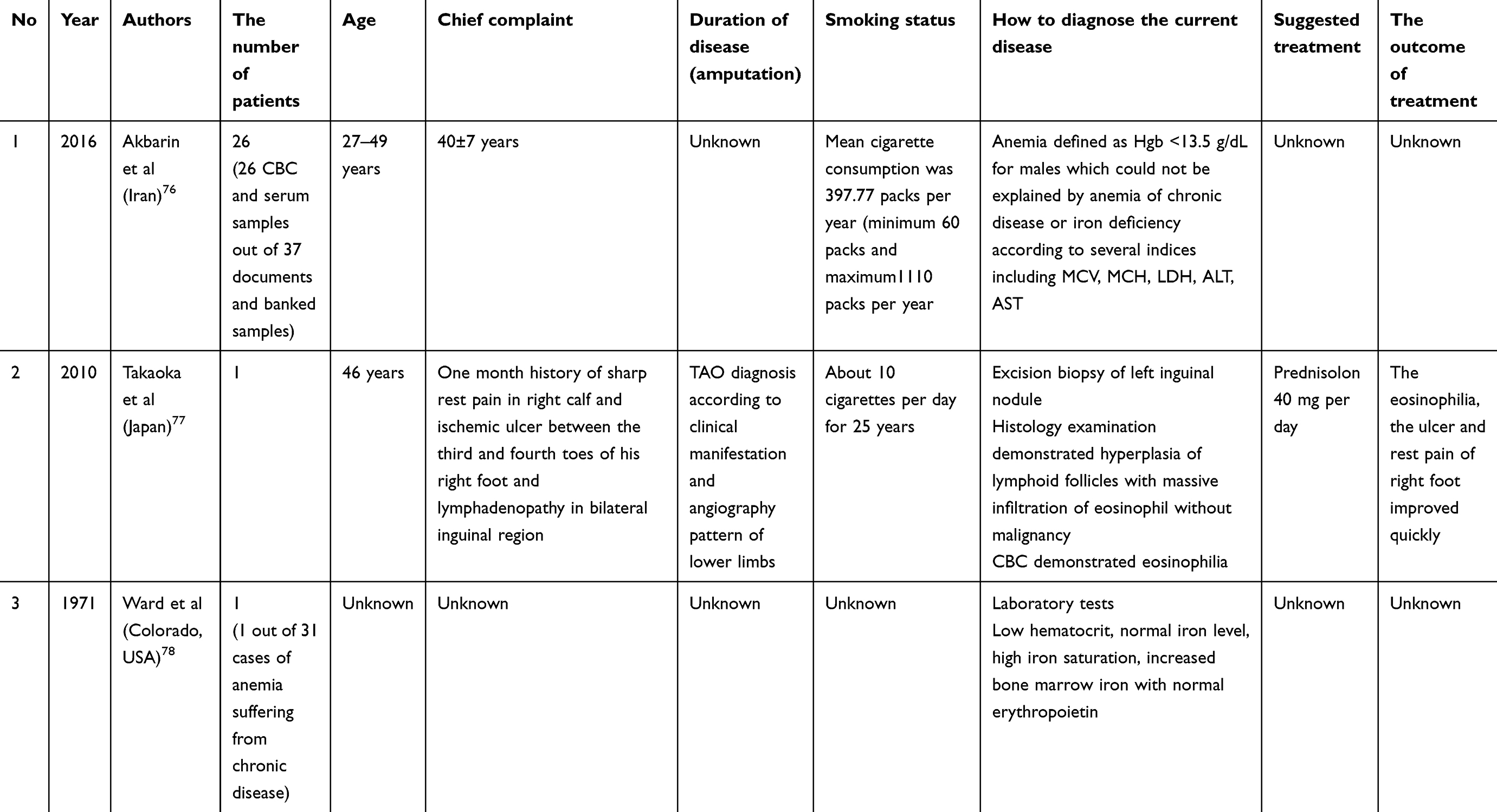 |
Table 8 Data summary of patients with TAO and lymphohematopoietic system involvement |
Joints
The systematic review revealed four articles related to arthritis. We were not able to access the full text of one article and one article had been published in a language other than English. In total, we included 3 articles covering 13 patients that had been published between 1981 and 2003 (Table 9). The mean age of the patients was 45 years and, for one patient, TAO diagnosis was made after the experience of arthralgia. The medical treatment for the patients with arthralgia is unknown. However, one patient who received corticosteroids showed progression in the digital ischemia, despite joint improvement.
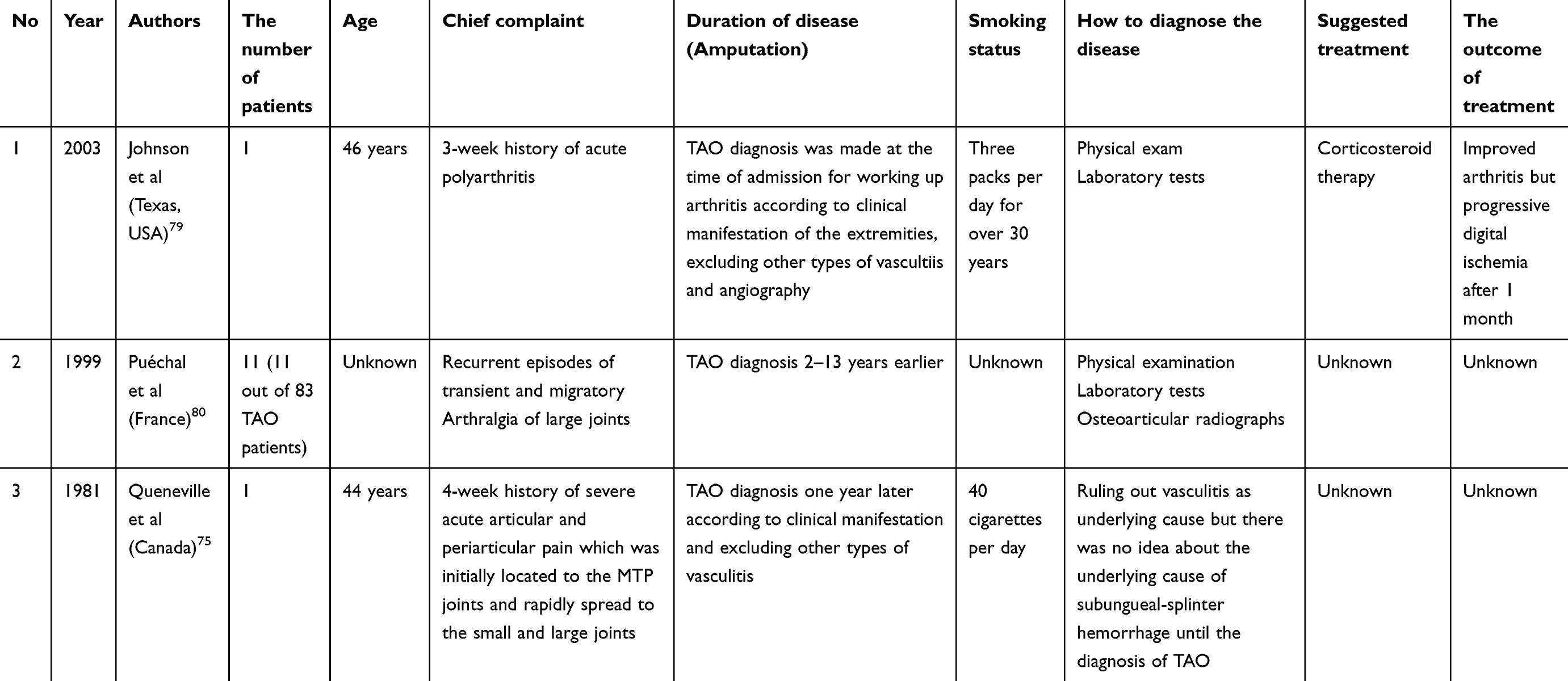 |
Table 9 Data summary of patients with TAO and arthralgia or arthritis |
Ear
According to a systemic search, we found one related article which consisted of one patient in total and published in 1962 (Table 10).
 |
Table 10 Data summary of a patient with TAO and ear involvement |
Discussion
The most challenging aspect of TAO management is its unknown etiology. Even its classification is challenging: it is usually viewed as a peripheral arterial disease rather than a type of vasculitis, and TAO patients are typically referred to angiologists or vascular surgeons as opposed to rheumatologists. This may be because of the unfavorable response of TAO to immunosuppressant medication and its favorable response to smoking cessation. Also, TAO is not known as a systemic disease and, in its diagnostic criteria, only the involvement of the small- and medium-sized arteries of the extremities is considered. Although Leo Buerger was the first to notice visceral arterial involvement in TAO in the first series of patients he evaluated, clinical manifestation of TAO in other organs is nonetheless known as an unusual or progressive form of TAO.
However, according to our systematic search, reports of the involvement of almost all organs have been made in relation to TAO. We also located several reports of TAO presentation in other organs before disease diagnosis, in which the involvement of the extremities presented after visceral involvement. Notably, the characteristics of the visceral arteries in several cases looked like the arteries of the extremities according to coronary angiography or aortography, including skip lesions and corkscrew collaterals. Also, in autopsies of TAO patients, the vascular involvement of multiple organs has been noted. In addition, in some studies, conservative, systemic medical treatment and smoking cessation have led to the recovery of the patient from the onset of visceral TAO.
On the other hand, TAO might be a systemic disease with a main clinical presentation in the extremities. For instance, approximately 30% of the TAO patients in the Fida et al study had abnormal urine analysis, although the patients were symptom-free.71
Moreover, reports of visceral involvement in TAO might be much more numerous than what we uncovered in the literature due to several reasons. One reason is that TAO is not of particular interest to many journals in the fields of angiology and rheumatology, and such case reports are not pursued for publication. Another reason may relate to the poor follow-up of TAO patients. According to our own experience, the main obstacle to follow-up is the mandatory admonition of smoking cessation. For this reason, TAO patients may prefer to ignore the bearable symptoms or to change health care providers. In many cases, TAO patients do not know that other organs can be affected by TAO, as was seen in some studies in which the patients experienced years of postprandial pain or weight loss without any follow-up. In some TAO cases, when we called the patient for follow-up, the family reported that the patient had died after experiencing abdominal or chest pain at younger than 50 years of age. Whilst there were no autopsies, we cannot prove that they died of visceral TAO, but it remains a possibility.
Unfortunately, our search did not reveal any treatment modality for visceral TAO because most of the cases did not have long-term follow-up to evaluate further visceral episodes of the disease. However, according to the current data, smoking cessation seems to be very helpful in patients’ recovery from visceral TAO. Also, more than 65% of the patients who received only medical treatment in the form of a combination of a vasodilator with anticoagulants showed improvement. Anticoagulants and anti-platelets without vasodilators led to an improvement in about 50% of the patients. Moreover, corticosteroids and immunosuppressants, but not anti-thrombotic or vasodilator treatments, did improve the skin and joint manifestations of the disease whilst aggravating the limb ischemia and, in a case of mesenteric ischemia, led to perforation of the bowel, followed by death.15,72,73,79 In terms of invasive treatments, bypass surgery had more acceptable outcomes in comparison to endovascular procedures, including stenting. However, more clinical evidence and clinical trials are needed to determine better management of patients with visceral TAO.
Conclusion
All in all, this study reveals five main points that should be noted:
- If we maintain the belief that visceral involvement is an unusual manifestation of TAO and insist on localizing it to the extremities, we may be pursuing the wrong path in determining the etiopathology of the disease and appropriate treatment.
- All patients with a diagnosis of TAO should be aware of the possible involvement of other organs along with the attendant warning signs, such as postprandial pain, unexplained weight loss, chest pain, any episodes of transient hemiparesis and cognitive and behavioral changes.
- Early, systemic medical treatment of patients suffering from visceral TAO may lead to better outcomes and reduce the overall mortality rate.
- Corticosteroid therapy and endovascular stenting are not recommended for managing visceral TAO.
- More clinical evidence with long-term follow-up is needed to determine a treatment modality for visceral TAO.
Disclosure
The authors declare that there are no conflicts of interest in this work.
References
1. Fazeli B, Rezaee SA. A review on thromboangiitis obliterans pathophysiology: thrombosis and angiitis, which is to blame? Vascular. 2011;19(3):141–153. doi:10.1258/vasc.2010.ra0045
2. Fazeli B, Dadgar Moghadam M, Niroumand S. How to treat a patient with thromboangiitis obliterans: a systematic review. Ann Vasc Surg. 2018;49:219–228. doi:10.1016/j.avsg.2017.10.022
3. Enshaei A, Hajipour B, Masoudi N. Repeated small bowel resection in a patient with Buerger’s disease and intestinal involvement. J Pak Med Assoc. 2016;66(4):467–469.
4. Bouomrani S, Belgacem N, Lassoued N, et al. Recurrent and resistant duodenal ulcer revealing Thromboangiitis obliterans. JMR. 2016;2(5):139–140.
5. Shastri RK. Segmental small bowel ischemia in a patient of buergers disease of lower extremity, a rare case report. OSR-JDMS. 2016;15(4):94–97.
6. Kamiya C, Deguchi J, Kitaoka KT, et al. Obstruction of the superior mesenteric artery due to emboli from the thoracic aorta in a patient with thromboangiitis obliterans. Ann Vasc Dis. 2014;7(3):320–324. doi:10.3400/avd.cr.14-00035
7. Lee KS, Paik CN, Chung WC, et al. Colon ischemia associated with buerger’s disease: case report and review of the literature. Gut Liver. 2010;4(2):287–291. doi:10.5009/gnl.2010.4.2.287
8. Cakmak A, Gyedu A, Akyol C, et al. Occlusion of the celiac trunk, the inferior mesenteric artery and stenosis of the superior mesenteric artery in peripheral thrombangiitis obliterans. VASA. 2009;38:394–396. doi:10.1024/0301-1526.38.4.394
9. Turkbey B, Eldem G, Akpinar E. Mesenteric ischemia in a patient with Buerger’s disease: MDCT findings. JBR-BTR. 2009;92(4):211–212.
10. Leung DK, Haskal ZJSIR. Film panel case: mesenteric involvement and bowel infarction due to buerger disease. J Vasc Interv Radiol. 2006;17:1087–1089. doi:10.1097/01.RVI.0000240426.53079.46
11. Cho YP, Kang GH, Han MS, et al. Mesenteric involvement of acute-stage buerger’s disease as the initial clinical manifestation: report of a case. Surg Today. 2005;35:499–501. doi:10.1007/s00595-004-2955-6
12. Kobayashi M, Kurose K, Kobata T, et al. Ischemic intestinal involvement in a patient with Buerger disease: case report and literature review. J Vasc Surg. 2003;38(1):170–174.
13. Cho YP, Kwon YM, Kwon TW, et al. Mesenteric Buerger’s disease. Ann Vasc Surg. 2003;17:221–223. doi:10.1007/s10016-001-0220-7
14. Kurata A, Nonaka T, Arimura Y, et al. Case reports multiple ulcers with perforation of the small intestine in buerger’s disease: a case report. Gastroenterology. 2003;125(3):911–916. doi:10.1016/s0016-5085(03)01065-5
15. Siddiqui MZ, Reis ED, Soundararajan K, et al. Buerger’s disease affecting mesenteric arteries: a rare cause of intestinal ischemia a case report. Vasc Surg. 2001;35(3):235–238.
16. Hassoun Z, Lacrosse M, De Ronde T. Intestinal involvement in buerger’s disease. J Clin Gastroenterol. 2001;32(1):85–89.
17. Iwai T. Buerger’s disease with intestinal involvement. Int J Cardiol. 1998;66(Suppl 1):
18. Michail PO, Filis KA, Delladetsima JK, et al. Thromboangiitis obliterans (Buerger’s disease) in visceral vessels confirmed by angiographic and histological findings. Eur J Vasc Endovasc Surg. 1998;16(5):445–448.
19. Lie JT. Visceral intestinal Buerger’s disease. Int J Cardiol. 1998;66 Suppl 1(Suppl 1):S249–56.
20. Sauvaget F, Debray M, Hervé de Sigalony JP, et al. Coloni ischemia reveals thromboangiitis obliterans (Buerger’s disease). Gastroenterology. 1996;110(3):900–903. doi:10.1053/gast.1996.v110.pm8608901
21. Burke AP, Sobin LH, Virmani R. Localized vasculitis of the gastrointestinal tract. Am J Surg Pathol. 1995;19(3):338–349.
22. Schellong SM, Bernhards J, Ensslen F, et al. Intestinal type of thromboangiitis obliterans (Buerger’s disease). J Intern Med. 1994;235(1):69–73.
23. Saboya CS, Simardi LH. Segmented colon ischemia associated with thromboangiitis oblitrans. Sao Paulo Med J. 1994;112(2):566–568.
24. Ito M, Nihei Z, Ichikawa W, et al. Intestinal ischemia resulting from buerger’s disease: report of a case. Surg Today. 1993;23(11):988–992.
25. Broide E, Scapa E, Peer A, et al. Buerger’s disease presenting as acute small bowel lschemia. Gastroenterology. 1993;104(4):1192–1195. doi:10.1016/0016-5085(93)90292-k
26. Soo KC, Hollinger-Vernea S, Miller G, et al. Buerger’s disease of the slgmold colon. Aust N Z J Surg. 1983;53(2):111–112.
27. Borlaza GS, Rapp R, Weatherbee L, et al. Visceral angiographic manifestation of thromboangiitis obliterans. South Med J. 1979;72(12):1609–1611. doi:10.1097/00007611-197912000-00037
28. Sobel RA, Ruebner BH. Buerger’s disease involving the celiac artery. Hum Pathol. 1979;10(1):112–115.
29. Sachs IL, Klima T, Frankel NB. Thromboangiitis obliterans of the transverse colon. JAMA. 1977;238(4):336–337.
30. Wolf EA
31. Herrington JL
32. Rob C. Surgical diseases of the celiac and mesenteric arteries. Arch Surg. 1966;93(1):21–32. doi:10.1001/archsurg.1966.01330010023004
33. Kilbourne BC. Coexisting buerger’s disease and giant hypertrophic gastritis report of a case. Q Bull Northwest Univ Med Sch. 1953;27(3):194–200.
34. Garvin EJ. Mesenteric vascular occlusion complicating thromboangiitis obliterans. Am J Surg. 1947;74(2):211–215. doi:10.1016/0002-9610(47)90166-9
35. Tekin Aİ, Arslan Ü. Coronary artery dissection in a patient with buerger’s disease. Braz J Cardiovasc Surg. 2019;34(1):114–117. doi:10.21470/1678-9741-2018-0136
36. Atay M, Saydam O, Işıklı OY, et al. Buerger disease with cardiac involvement in a young patient. Cukurova Med J. 2016;41(2):408–410. doi:10.17826/cutf.203781
37. Mitropoulos F, Eforakopoulos F, Kanakis MA, et al. Diagnostic and therapeutic approach in a patient with buerger’s and coronary artery disease. Case Rep Med. 2013;2013:974184. doi:10.1155/2013/974184
38. Akyuz S, Sungur MA, Donmez C. Rescue thrombolysis in the treatment of cardiac shock and acute stroke. Am J Emerg Med. 2013;31(5):891. doi:10.1016/j.ajem.2012.12.039
39. Hsu P-C, Lin T-H, Su H-M, Voon W-C, Lai W-T, Sheu S-H. Frequent accelerated idioventricular rhythm in a young male of Buerger’s disease with acute myocardial infarction. Int J Cardiol. 2008;127(2):e64–e66. doi:10.1016/j.ijcard.2007.04.037
40. Abe M, Kimura T, Furukawa Y, et al. Coronary Buerger’s disease with a peripheral arterial aneurysm. Eur Heart J. 2007;28(8):928. doi:10.1093/eurheartj/ehl314
41. Miranda JA. Pulmonary vein thrombosis presenting as myocardial infarction. Chest. 2006;130(4):344. doi:10.1378/chest.130.4_MeetingAbstracts.344S-a
42. Hong TE, Faxon DP. Coronary artery disease in patients with buerger’s disease. Rev Cardiovasc Med. 2005;6(4):222–226.
43. Becit N, Unlü Y, Koçak H, et al. Involvement of the coronary artery in a patient with thromboangiitis obliterans. A Case Report. Heart Vessels 2002;16(5):201–203. doi:10.1007/s003800200023
44. Hoppe B, Lu JT, Thistlewaite P, et al. Beyond peripheral arteries in Buerger’s disease: angiographic considerations in thromboangiitisobliterans. Catheter Cardiovasc Interv. 2002;57(3):363–366. doi:10.1002/ccd.10330
45. Donatelli F, Triggiani M, Nascimbene S, et al. Thromboangiitis obliterans of coronary and internal thoracic arteries in a young woman. J Thorac Cardiovasc Surg. 1997;113(4):800–802. doi:10.1016/S0022-5223(97)70243-5
46. Mautner GC, Mautner SL, Lin F, et al. Amounts of coronary arterial luminal narrowing and composition of the material causing the narrowing in buerger’s disease. Am J Cardiol. 1993;71(5):486–490. doi:10.1016/0002-9149(93)90467-q
47. Kim KS, Kim YN, Kim KB, et al. Acute myocardial infarction in a patient with Buerger’s disease. A case report and a review of the literature. Korean J Intern Med. 1987;2(2):278–281. doi:10.3904/kjim.1987.2.2.278
48. Ohno H, Matsuda Y, Takashiba K, et al. Acute myocardial infarction in Buerger’s disease. Am J Cardiol. 1986;57(8):690–691. doi:10.1016/0002-9149(86)90863-5
49. Aydın E, Çınar C, Bozkaya H, et al. Brain infarction in a young patient with Buerger’s disease - a case of cerebral thromboangiitis obliterans. Neurol Asia. 2016;21(4):391–393.
50. Huang WW, Wu CH, Li CF. Late onset buerger’s disease with multiple cerebral infarcts. Tzu Chi Med J. 2007;19:28–31.
51. No YJ, Lee EM, Lee DH, Kim JS. Cerebral angiographic findings in thromboangiitis obliterans. Neuroradiology. 2005;47(12):912–915. doi:10.1007/s00234-005-1445-x
52. Bischof F, Kuntz R, Melms A, Fetter M. Michael. cerebral vein thrombosis in a case with thromboangiitis obliterans. Cerebrovasc Dis. 1999;9(5):295–297. doi:10.1159/000015981
53. Dotti MT, De Stefano N, Vecchione V, Correra G, Federico A. Cerebral thromboangiitis obliterans: clinical and MRI findings in a case. Eur Neurol. 1995;35(4):246–248. doi:10.1159/000117142
54. Kessler C, Reuther R, Berlit P, Carls C, Hofmann W. CAT scan and immunohistochemical findings in a case of cerebral thromboangiitis obliterans(Buerger’s disease). Eur Neurol. 1984;23(1):7–11. doi:10.1159/000115670
55. Drake ME
56. Biller J, Asconapé J, Challa VR, Toole JF, McLean WT. A case for cerebral thromboangiitis obliterans. Stroke. 1981;12(5):686–689.
57. Wolman L. Cerebral thromboangiitis obliterans. J Clin Pathol. 1958;11(2):133–138. doi:10.1136/jcp.11.2.133
58. Lippmann HI. Cerebrovascular thrombosis in patients with buerger’s disease. Circulation. 1952;5(5):680–692. doi:10.1161/01.cir.5.5.680
59. Korkmaz A, Karti O, Top Karti D, Yüksel B, Zengin MO, Kusbeci T. Could Buerger’s disease cause nonarteritic anterior ischemic optic neuropathy?: a rare case report. Neurol Sci. 2018;39(7):1309–1312. doi:10.1007/s10072-018-3325-2
60. Eris E, Sucu ME, Perente I, et al. Retinal artery occlusion secondary to Buerger’s disease (Thromboangiitis obliterans). Case Rep Ophthalmol Med. 2017;2017:3637207.
61. Marques AS, Portelinha J, Almeida A, et al. Chorioretinal atrophy in a patient with Buerger’s disease. Ophtalmologia. 2015;38:139–143.
62. Koban Y, Bilgin G, Cagatay H, et al. The association of normal tension glaucoma with Buerger’s disease: a case report. BMC Ophthalmol. 2014;14:130. doi:10.1186/1471-2415-14-130
63. Ohguro I, Ohguro H, Ohta T, Nakazawa M. A case of normal tension glaucoma associated with Buerger’s disease. Tohoku J Exp Med. 2006;209(1):49–52.
64. Pham KN, Sokoloff MH, Steiger CA. Severe gangrene at the glans penis requiring penectomy as the frst major complication of Buerger’s disease. Am J Clin Exp Urol. 2016;4(1):9–11.
65. Roberts JA, Meyer JP. Buerger’s disease presenting as a testicular mass: A rare presentation of an uncommon disease. Urol Ann. 2016;8(2):249–251. doi:10.4103/0974-7796.179238
66. Aktoz T, Kaplan M, Yalcın O, et al. Penile and scrotal involvement in Buerger’s disease. Andrologia. 2008;40:401–403. doi:10.1111/j.1439-0272.2008.00859.x
67. Orhan I, Onur R, Akpolat N, et al. Penile amputation in Buerger’s disease an unusual cause of organ loss. Scand J Urol Nephrol. 2004;38:188–189. doi:10.1080/00365590410029745
68. Yun HJ, Kim DI, Lee KH, et al. End stage renal disease caused by thromboangiitis obliterans: a case report. J Med Case Rep. 2015;9:174. doi:10.1186/s13256-015-0659-8
69. Goktas S, Bedir S, Bozlar U, Ilica AT, Seckin B. Intrarenal arterial stenosis in a patient with thromboangiitis obliterans. Int J Urol. 2006;13(9):1243–1244. doi:10.1111/j.1442-2042.2006.01546.x
70. Stillaert P, Louagie Y, Donckier J. Emergency hepato-renal artery bypass using a PTFE graft. Acta Chir Belg. 2003;103:524–527.
71. Fida B, Tizianello A, Ruberti U. Functional and histological features of the kidney in thromboangiitis obliterans. Cardiologia. 1959;35:63–83.
72. Li QL, He DH, Huang YH, et al. Thromboangiitis obliterans in two brothers. Exp Ther Med. 2013;6(2):317–320. doi:10.3892/etm.2013.1160
73. Takanashi T, Horigome R, Okuda Y, et al. Buerger’s disease manifesting nodular erythema with livedo reticularis. Intern Med. 2007;46(21):1815–1819. doi:10.2169/internalmedicine.46.0143
74. Quenneville JG, Gossard D. Subungueal-splinter hemorrhage an early sign of thromboangiitis obliterans. Angiology. 1981;32(6):424–432. doi:10.1177/000331978103200609
75. Rye LA, Calhoun NR, Redman RS. Necrotizing sialometaplasia in a patient with Buerger’s disease and Raynaud’s phenomenon. Oral Surg Oral Med Oral Pathol. 1980;49(3):233–236. doi:10.1016/0030-4220(80)90054-7
76. Akbarin MM, Ravari H, Rajabnejad A, Valizadeh N, Fazeli B. Investigation of the etiology of anemia in thromboangiitis obliterans. Int J Angiol. 2016;25(3):153–158. doi:10.1055/s-0035-1571190
77. Takaoka H, Takano H, Nakagawa K, Kobayashi Y, Hiroshima K, Komuro I. Buerger’s disease-like vasculitis associated with Kimura’s disease. Int J Cardiol. 2010;140(2):e23–e26. doi:10.1016/j.ijcard.2008.11.072
78. Ward HP, Kurnick JE, Pisarczyk MJ. Pisarczyk. Serum level of erythropoietin in anemias associated with chronic infection, malignancy and primary hematopoietic disease. J Clin Invest. 1971;50(2):332–335. doi:10.1172/JCI106500
79. Johnson JA, Enzenauer RJ. Enzenauer. Inflammatory arthritis associated with thromboangiitis obliterans. J Clin Rheumatol. 2003;9(1):37–40. doi:10.1097/01.RHU.0000049712.74443.70
80. Puéchal X, Fiessinger JN, Kahan A, Menkès CJ. Rheumatic manifestations in patients with thromboangiitis obliterans (Buerger’s disease). J Rheumatol. 1999;26(8):1764–1768.
81. Kirikae I, Nomura Y, Shitara T, Kobayashi T. Sudden deafness due to Buerger’s disease. Arch Otolaryngol. 1962;75:502–505.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.