")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 10
Violent victimization of adult patients with severe mental illness: a systematic review
Authors Latalova K , Kamaradova D, Prasko J
Received 23 May 2014
Accepted for publication 21 July 2014
Published 9 October 2014 Volume 2014:10 Pages 1925—1939
DOI https://doi.org/10.2147/NDT.S68321
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Klara Latalova,1,2 Dana Kamaradova,1,2 Jan Prasko1,2
1Faculty of Medicine and Dentistry, Palacky University Olomouc, Olomouc, Czech Republic; 2Department of Psychiatry, University Hospital Olomouc, Olomouc, Czech Republic
Abstract: The aims of this paper are to review data on the prevalence and correlates of violent victimization of persons with severe mental illness, to critically evaluate the literature, and to explore possible approaches for future research. PubMed/MEDLINE and PsycINFO databases were searched using several terms related to severe mental illness in successive combinations with terms describing victimization. The searches identified 34 studies. Nine epidemiological studies indicate that patients with severe mental illness are more likely to be violently victimized than other community members. Young age, comorbid substance use, and homelessness are risk factors for victimization. Victimized patients are more likely to engage in violent behavior than other members of the community. Violent victimization of persons with severe mental illness has long-term adverse consequences for the course of their illness, and further impairs the quality of lives of patients and their families. Victimization of persons with severe mental illness is a serious medical and social problem. Prevention and management of victimization should become a part of routine clinical care for patients with severe mental illness.
Keywords: victimization, violence, severe mental illness, schizophrenia, bipolar disorder
Introduction
Victimization of the mentally ill has a very long history. The Roman encyclopedist Celsus (~25 BC to ~50 AD) recommended “torture, starvation, fetters, or flogging” as treatments for mental illness.1 Bizarre behaviors of the mentally ill were sometimes thought to indicate possession by Satan, resulting in occasional victimization in the witch trials of the 16th and 17th centuries.2
Victimization of the mentally ill has taken on different forms, but it has never stopped. Deinstitutionalization, started in the mid-1950s and largely completed in the mid-1990s,3 resulted in an influx of persons with severe mental illness into communities, where they are at considerable risk for homelessness3,4 as well as criminal and other victimization.5 Verbal abuse and other harassment of the mentally ill by local teenagers and neighbors is also common.6,7
Violent victimization of persons with severe mental illness presents obvious dangers of physical trauma; it has long-term adverse consequences for the course of mental illness, and it further impairs the quality of patients’ lives. As this review will show, its prevalence is high. Thus, victimization is a major public health problem.
However, it has attracted much less attention than violent behavior by the patients in spite of the fact that violent victimization of patients occurs more frequently than violent offending by the patient.8,9 In spite of the lower frequency of offending in comparison with victimization, victimized patients may be violent, and relationships between victimization and offending exist.
Victimization in childhood is a frequent precursor of mental illness,10,11 violent behavior,12 and victimization in adulthood.13,14
However, childhood victimization is beyond the scope of this review, which focuses on victimization of adults with severe mental illness.
The impetus for writing this review was the recent explosion of work in the area of victimization and severe mental illness. Previous reviews focusing on this problem located only nine9 or ten8 relevant publications. More recent reviews deal exclusively with domestic violence and do not focus on the severe mental disorder of the victims.15,16 The goal of this review is to update and expand data on prevalence, correlates, and impact of adult victimization among individuals with severe mental illness.
Methods
The PsycINFO and PubMed/MEDLINE databases were searched using the terms “psychosis”, “psychoses”, “psychotic”, “mental disorders”, “psychiatry”, “psychopathology”, “severe mental illness”, “major depression”, “schizophrenia”, and “bipolar disorder” in successive combinations with “victimization”, “victimisation”, “victimized”, “victimised”, and “victim*”. The search covered the time up to June 22, 2014; no backwards time constraint was used (the start time was whatever the search engines provided). No constraints on the language of publication were imposed. Availability of explicit data on the rates of prevalence of victimization over a definite period was a criterion of eligibility for inclusion of the reports in our review. The subjects had to be at least 18 years old, and had to be diagnosed with a severe mental illness such as schizophrenia, bipolar disorders, major depression, or other psychotic disorders. Furthermore, the included studies had to have been published in peer-reviewed journals. Excluded were books, book chapters, commentaries, reviews, and dissertations. The procedure for the inclusion of publications is shown in Figure 1. The final studies yielded by the search are summarized in Tables 1 and 2.
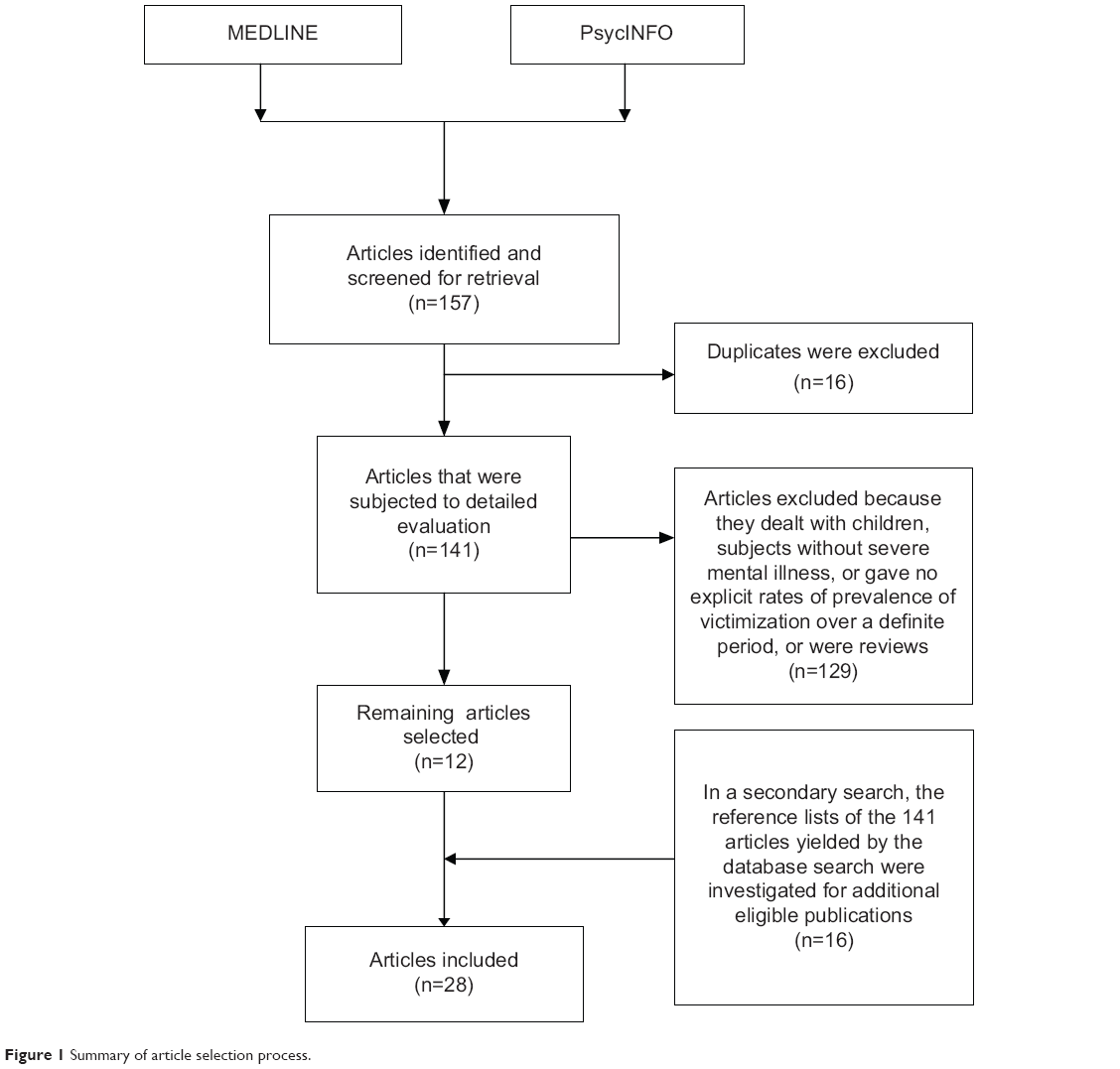 | Figure 1 Summary of article selection process. |
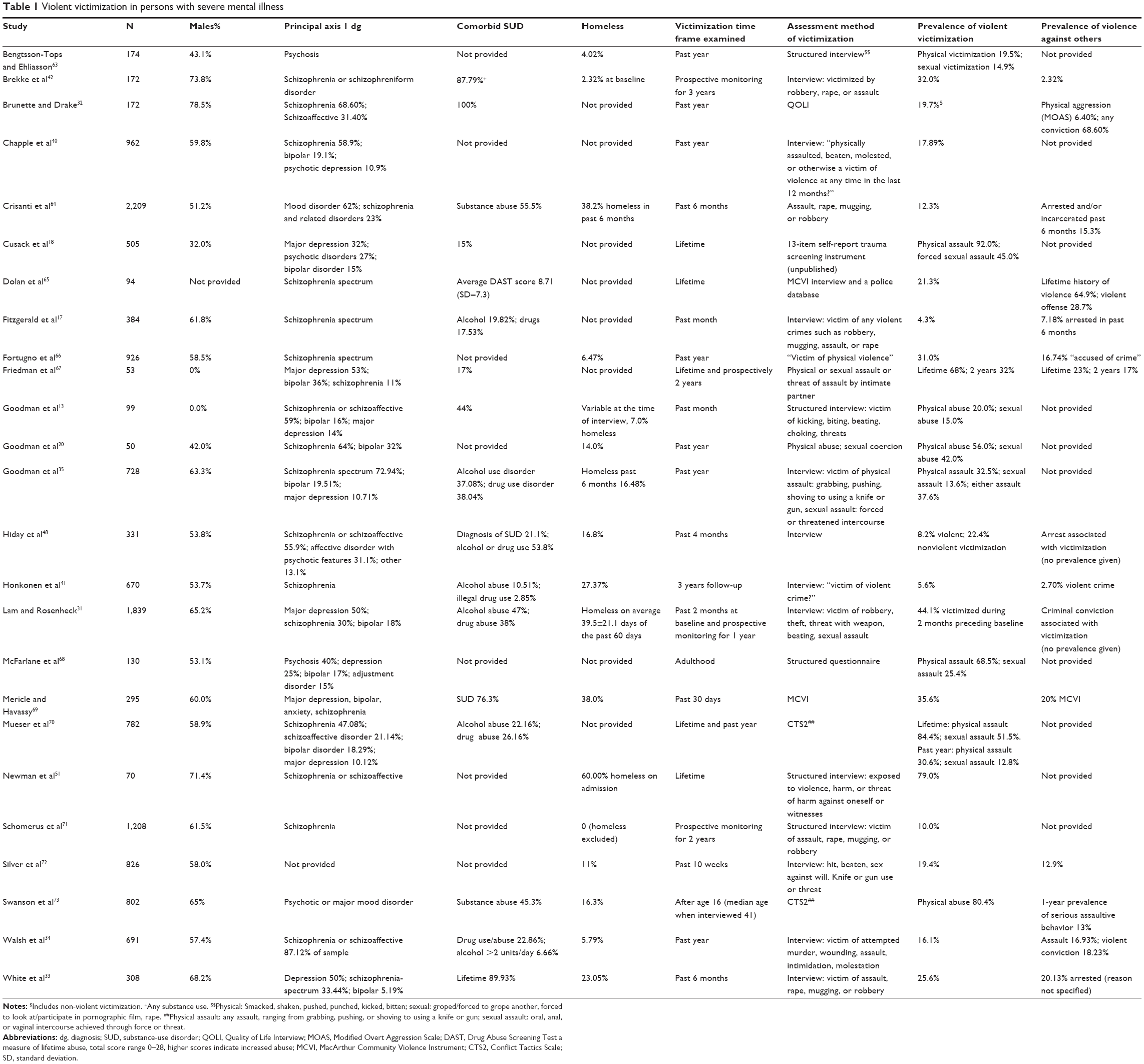 | Table 1 Violent victimization in persons with severe mental illness |
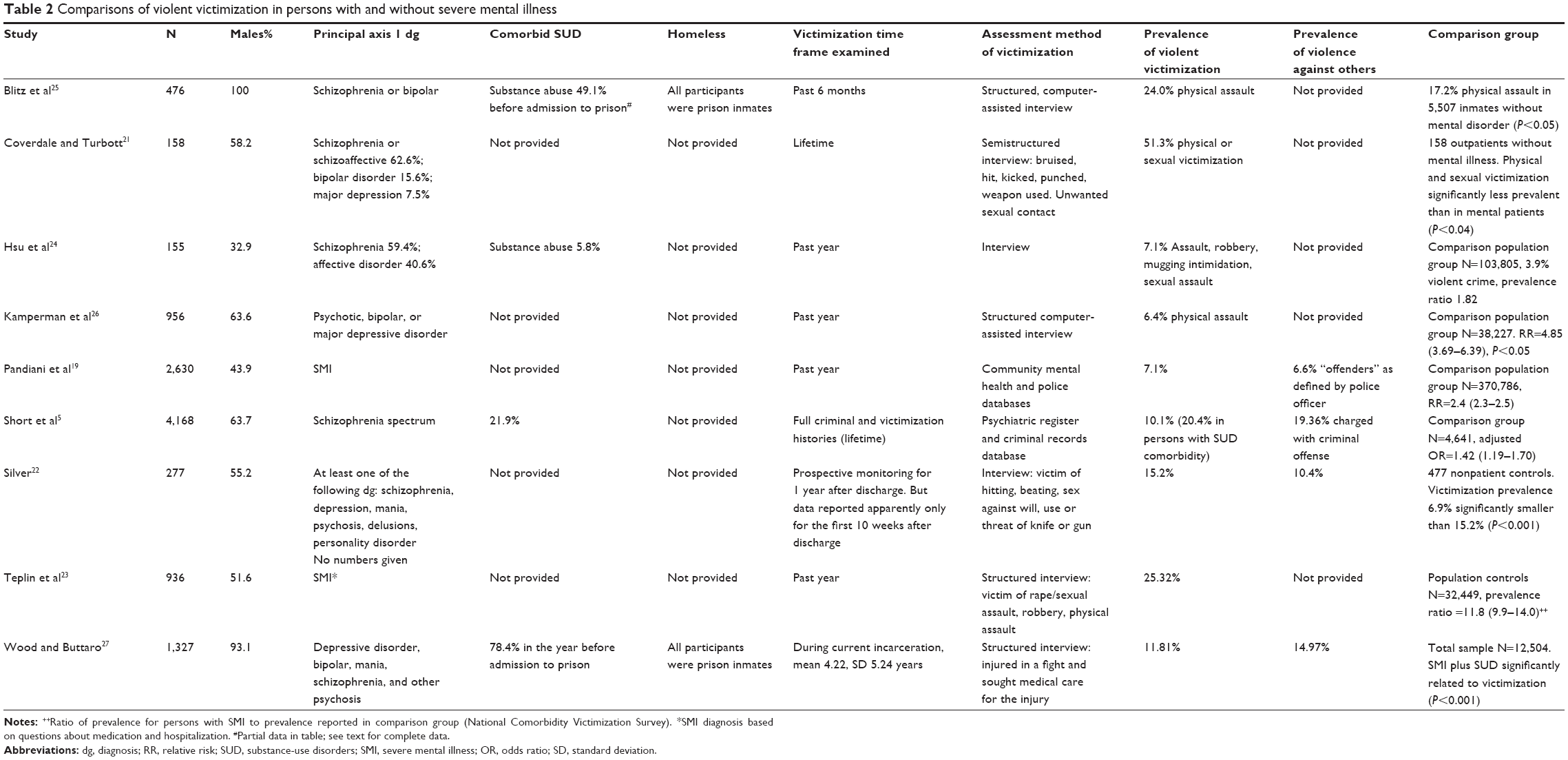 | Table 2 Comparisons of violent victimization in persons with and without severe mental illness |
Results
Prevalence of victimization
The search detected 34 articles reporting empirical observations on the prevalence of violent victimization of adult individuals with diagnosed severe mental illness. Tables 1 and 2 display the demographic and clinical data as well as descriptors of violent victimization and, when available, data on violent offending by the study participants.
The reported prevalence of violent victimization ranges between 4.3%17 and 92%,18 but these data are not comparable since the first report covers the past month and the second one the lifetime. By limiting the data to studies that used the time frame of 1 year for the assessment of victimization, we could detect the range 7.1%–56%.19,20 Again, these studies are difficult to compare. The respective Ns are 50 and 2,610. The larger study is based on police records, whereas the smaller one interviewed each patient. Similar discrepancies in the number of participants, their diagnoses, time frames and methods of data collection, and definitions of victimization are clearly demonstrated in Table 1. The estimates of the prevalence of victimization in patients with severe mental illness vary widely with the methods used by the authors.
Rather than attempting to determine the “true” prevalence of victimization in patients with severe mental illness, it is useful to ask whether this prevalence is different from that in the general (or another control) population. Nine studies provided comparisons of the prevalence of victimization in persons with severe mental illness with that observed in nonaffected control populations.5,19,21–27 These studies are summarized in Table 2, which provides numerical data.
An epidemiological study of victimization and perpetration was conducted in prison population in the United States.25 A sample of 7,785 subjects aged 18 or older (7,221 men and 564 women) completed a survey. Mental disorder was based on self-reported mental health treatment ever for particular mental disorders. Prior treatment for schizophrenia, bipolar disorder, depression, posttraumatic stress disorder (PTSD), or anxiety disorder was reported in 24.8% of the total sample. Rates of physical victimization for males with any mental disorder were 1.6 times (inmate-on-inmate) and 1.2 times (staff-on-inmate) higher than that of males with no mental disorder. Female inmates with mental disorder were 1.7 times more likely to report being physically victimized by another inmate than were their counterparts with no mental disorder. Thus, both males and females with histories of mental disorder were disproportionately represented among victims of physical violence inside the prison. Data on a subset of 476 inmates with a history of schizophrenia or bipolar disorder are presented in Table 2. A New Zealand study compared victimization rates of 158 outpatients with severe mental illness with 158 outpatients recruited from the waiting rooms of medical, surgical, and other clinics.21 Compared with the controls, patients were significantly more likely to report a history of sexual or physical abuse during adulthood. Female patients were significantly more likely to be sexually and physically abused than male patients, and those sexually abused were significantly more likely to report a history of sexual abuse during childhood. A relatively small study conducted in Taiwan reported 1-year prevalence of violent victimization of patients with severe mental illness somewhat higher than in the general population.24
A Dutch epidemiological survey included a random sample of 956 severely mentally ill outpatients and compared their victimization rate with that obtained in a general population sample (N=38,227).26 The prevalence of violent victimization by physical assault was significantly higher in the outpatients (Table 2). The prevalence of sexual harassment or assault was 5.4%, and the relative risk in comparison with the control population was 3.94 (3.05–5.05).
The next epidemiological study compared crime victimization rates among 2,610 adults with serious mental illness with those observed in a sample of general population (N=370,786).19 Among the 2,610 adults, 7.1% were identified as crime victims by police officers, a significantly higher rate in comparison with the control population. To compare Pandiani et al’s19 data with other publications, we calculated the odds ratio (OR) using the numbers provided in the first line of Table 1 (OR=2.51).
A US study reported by Silver22 used data from one of the sites of the MacArthur Foundation’s Violence Risk Assessment Study.28 A sample of discharged psychiatric patients (N=270) was compared with a sample of nonpatients (general population) drawn from the same neighborhoods (N=477). Violent victimization of the patients was assessed by an interview covering their experiences during the first 10 weeks after discharge from the hospital. An analogous interview was conducted with nonpatient controls. The prevalence of violent victimization in discharged patients was significantly greater than in controls (Table 2).
A large epidemiological study was conducted by Short et al in the Australian state of Victoria.5 The study compared the rates of reported crime victimization in 4,168 schizophrenia-spectrum patients with 4,641 randomly selected community members. The schizophrenia-spectrum sample comprised all persons in a statewide psychiatric case register who were first diagnosed with a schizophrenia-spectrum disorder in the years 1975, 1980, 1985, 1990, 1995, 2000, and 2005. To extract full criminal and victimization histories, each case in the schizophrenia-spectrum and community samples was linked with a criminal records database. Cases first diagnosed with a schizophrenia-spectrum disorder in each of the cohort years (1975, 1980, 1985, 1990, 1995, 2000, and 2005) were matched by age and year of birth with cases in the community sample, whenever a match existed.
Compared to community controls, patients with schizophrenia-spectrum disorders were significantly more likely to have a record of violent victimization (10.1% vs 6.6%, OR=1.42, 95% confidence interval [CI]=1.19–1.70), but less likely to have an official record of victimization overall (28.7% vs 39.1%, OR=0.5, 95% CI=0.45–0.56).
While victimization rates have remained relatively constant over time in the community sample, there has been a steady increase in lifetime victimization records among those in the schizophrenia-spectrum sample, from 15.3% in those first diagnosed in 1975 up to 37.4% in those first diagnosed in 2005. These rates appear to have reached a plateau at around 37% since 1995.5 Thus, over the approximate period of deinstitutionalization, the rate of recorded victimization has more than doubled in schizophrenia-spectrum patients. It seems that increased violent victimization may have been an unintended consequence of deinstitutionalization of the mentally ill.
The finding that the patients were less likely to have an official record of overall victimization was unexpected. A possible explanation is that people with severe mental illness are less likely to report less serious victimization to police than other members of the community.5 This uncertainty illustrates the limitations of research relying exclusively on official records without a direct contact with the study participants.
Teplin et al determined the prevalence of crime victimization among persons with severe mental illness and compared it with general population data from the National Crime Victimization Survey (NCVS), controlling for income and demographic differences between the samples.23 The NCVS, an annual study of approximately 43,000 households comprising nearly 80,000 persons, is conducted by the US Bureau of the Census on behalf of the Department of Justice. Interviewers administered the NCVS29 to 936 randomly selected patients with severe mental illness sampled from 16 randomly selected mental health agencies in Chicago, IL, USA. The comparison group comprised 32,449 participants in the NCVS. A total of 25.3% of persons with severe mental illness compared with 2.8% of population controls had been victims of a violent crime in the past year, a rate significantly higher.
A US study found that the combination of (self-reported) history of severe mental illness and substance-use disorder was significantly related to sustained and inflicted physical assaults during prison incarceration.27 More than half of the victims of assault in prison were charged with or convicted of assaulting others. This sample is noted for a very high comorbidity rate between severe mental illness and substance-use disorders.
In summary, nine studies comprising a total of 11,083 persons with severe mental illness and 569,505 members of control populations concluded that the risk of violent victimization was greater in the patients with severe mental illness. The risk increase in each of the studies was statistically significant. However, the size of the risk varies across studies. The risk for patients may vary depending on the community in which they are living. Methodological differences between the studies may have contributed to the variation of risk estimates.
Victimization correlates and contributing factors
Sex and age effects
Relations between sex and risk for any type of violent victimization have been studied; some of the research focused on sexual violence. Patients with severe mental illness are vulnerable to sexual violence, including rape and sexual assault. Rape is defined as the unlawful penetration of a person against the will of the victim, with use or threatened use of force, or attempting such an act. Sexual assault is defined across a wide range of victimizations, separate from rape or attempted rape. These crimes include attacks or attempted attacks generally involving unwanted sexual contact between a victim and the offender. Sexual assault may or may not involve force and includes grabbing or fondling. Sexual assault also includes verbal threats.30
The multicenter US study described in the preceding section on homelessness enrolled 640 females and 1,199 males with severe mental illness.31 Statistically significant sex differences were found in several types of reported victimization. Women were more likely to report being beaten (20.6% vs 12.9% for men, χ2=139.28, df=1, P<0.001) or threatened with a weapon. Sexual assault was more frequently reported in women (15.3% more than that in men, 1.3%). Younger age was associated with sexual, but not other types of victimization. More information on the studies is given in Tables 1 and 2.
Another US study examined sex differences in 37 women and 135 men with schizophrenia and substance-use disorders.32 Women were more likely to be victimized than men (χ2=4.37, df=1, P<0.04). These results were supported by a study of 209 males and 99 females in San Francisco, which found female sex associated with victimization (OR=2.02, 95% CI=1.2–3.5).33
A study that was discussed in detail, in the “Prevalence of victimization” section, enrolled 149 males and 121 females discharged from a psychiatric hospital.22 Logistic regression showed that being male and being younger than 25 years was associated with violent victimization; the respective ORs are 1.71 and 1.67. Both ORs were statistically significant at the 0.05 level, but CIs were not provided.
Similar results emerged from a UK study (discussed in the preceding section) that included 294 females and 397 males with severe mental illness.34 Males were somewhat more likely to be victimized than females (OR=1.56, 95% CI=1.02–2.40, P<0.05). Participants aged 18–39 years were more likely to be victimized than those in the 40–64 age range (OR=2.32, 95% CI=1.45–3.71, P<0.001).
A study that was described in detail in the section “Prevalence of victimization” reported separately on the risks of rape/attempted rape and sexual assault in persons with severe mental illness.23 A total of 2.43% of persons with severe mental illness compared with 0.11% of population controls had been victims of rape or attempted rape in the past year, with an adjusted prevalence ratio of 22.5 (P<0.001). The respective numbers for sexual assault were 1.00% and 0.07% with a prevalence ratio of 15.0 (P<0.001). Separate data for men and women with mental illness on rape/sexual assault were provided. The annual prevalence for men was 0.8% and for women 4.3% (P<0.02). For women, the prevalence ratio relative to the control population was 18.5 (11.2–30.4) (P<0.001).23
Separate data for mentally ill men and women on sexual harassment and assault were also provided in another study described in the section “Prevalence of victimization”.26 The annual prevalence for men was 3.0% and for women 9.8%. The relative risk for men was 0.30 (0.17–0.53), indicating a significantly higher risk for women (P<0.05). Both sexes had a significantly higher risk for sexual harassment and assault relative to the general population (P<0.05).
A multicenter US study interviewed 321 women and 461 men with severe mental illness.35 The reported prevalence of rape/sexual assault in the past year was 20.3% in women and 7.6% in men, whereas the prevalence of physical (nonsexual) assault was 25.6% in women and 34.1% in men. The sex differences for sexual assault and physical assault were statistically significant, with χ2 values, respectively, 26.66 (P<0.001) and 6.39 (P<0.01). Assault (any type) was significantly associated with younger age in both sexes. No association between sex and victimization was found in a UK study of 632 patients with severe mental illness.36
In summary, it is clear that women with severe mental illness are more likely to be subjected to sexual violence than males with severe mental illness than females or males without severe mental illness. The risk of nonsexual violent victimization was found to be higher in females in some studies but in males in other studies. It is possible that further research will reveal that risk for specific subtypes of nonsexual victimization may differ between sexes. Victimization rates appeared to decrease with age. Interactions between age and sex have not been explored, and merit future research.
Comorbid substance use and personality disorders
Alcohol is “abundantly present in the day-to-day violent confrontation”.37 This applies to drinkers with and without mental illness and to assailants as well as to victims. In a classic study of murder in the general population, approximately one in four homicides was precipitated by the victims, and drinking alcohol by the victim was identified as a precipitating factor.38 In the general population, substance abuse increases approximately nine-fold the risk of homicidal death.39
An overview of studies of comorbid substance use is given in Tables 1 and 2. The sample of 4,168 schizophrenia-spectrum patients discussed earlier5 consisted of patients with (N=913) and without (N=3,255) a diagnosed comorbid substance-use disorder. The comorbidity was associated in substantial elevations of prevalence and risk of violent victimization.
A study of 1,839 largely homeless patients using mental health services showed a statistically significant relationship between the number of days they were intoxicated and being robbed (r=0.09, P<0.05), threatened with a weapon (r=0.11, P<0.001), or beaten (r=0.15, P<0.001).31 In an Australian study of 962 individuals with psychosis, the odds of being a victim were increased in those who had a lifetime history of substance abuse (OR=1.49, 95% CI=1.03–2.17).40
A Finnish study included 670 patients diagnosed with schizophrenia, 37 of whom were victims of a violent crime over a period of 3 years.41 There was a total of 70 alcohol abusers. The OR (abusers compared to nonabusers) was 5.44 (95% CI=2.62–11.25). The risk of victimization in patients with mental illness increased with the number of illicit drugs used,34 the level of substance use,42 alcohol use,24 and psychostimulants.43
There are probably multiple mechanisms of substance use affecting risk of victimization. An intoxicated, stuporous person is obviously an easy target of criminals. On the other hand, alcohol and stimulants may lead to loss of behavioral controls and provocative conduct, resulting in victim-precipitated violence. Illegal activities involved in the procurement of illicit drugs may lead to violence and victimization, as described in detail elsewhere.44 In any event, the data reviewed here should further energize efforts to detect and treat substance-use disorder comorbid with severe mental illness.
Comorbid antisocial personality disorder is well known to increase the risk of violence in severe mental illness.45 In a UK prospective study of 632 patients with severe mental illness, the presence of comorbid cluster B personality disorder (dissocial, impulsive, histrionic, and borderline) was strongly associated with violent victimization (OR=5.90, 95% CI=2.09–16.66, P<0.01).36 In a sample of 205 adult UK patients, retrospectively assessed history of conduct disorder prior to age 18 was associated with increased risk for violent victimization (OR=2.19, 95% CI=1.18–4.05).46
In summary, there is a preponderance of evidence suggesting that the abuse of alcohol or illicit drugs increases the risk of violent victimization of persons with severe mental illness. The abusing patients are approximately 1.3–5.4 times more likely to be violently victimized than their nonabusing counterparts.
Homelessness
Relationships between homelessness and victimization of the mentally ill have been studied for several decades (see Tables 1 and 2 for an overview of the studies to be discussed). The study of 1,839 patients briefly mentioned in the preceding section31 was a multicenter US project that interviewed participants at study entry and at 3 and 12 months after entry. Self-reports of victimization obtained at study entry revealed that 44% of the participants were victimized during the past 2 months. The study found statistically significant relationships between being robbed and the number of days the participants were homeless (r=0.15, P<0.001). Thus, participants who had been recently victimized at the time of the baseline interview reported spending more time on the streets and in shelters at the time of the follow-up interviews at 3 and 12 months. This was interpreted to mean that recent victimization had a significant impact on client outcomes in terms of increased homelessness.31
In a UK study, 691 subjects with established psychotic disorders were interviewed to establish the 1-year prevalence of violent victimization.34 Sixteen percent of patients reported being violently victimized. Victims of violence were significantly more likely to report homelessness; adjusted OR=2.67 (95% CI=1.23–5.77). A similar finding was reported in an Australian sample of 962 individuals with psychosis.40 Homelessness increased the risk of violent victimization; OR=2.51 (95% CI=1.57–4.02). A study examined history of victimization in 308 severely mentally ill adults in San Francisco, CA, USA.33 Being homeless (OR=2.1, 95% CI=1.2–3.8, P=0.013) was associated with reporting violent victimization.
A cross-sectional study aimed to determine the prevalence and correlates of violent victimization among homeless people in Sydney, NSW, Australia.43 Clients of a shelter for homeless, substance-using adults were interviewed about their drug use, mental health, and violent victimization in the previous 12 months. Participants reported complex drug use histories and high levels of victimization, depression, PTSD, and schizophrenia or other psychotic disorders. Being female, schizophrenia/psychotic disorder, PTSD, depression and regular use of psychostimulants were associated with increased risk of victimization. The authors concluded that a longitudinal study to determine whether victimization prolongs homelessness is warranted. Clinical staff working with homeless populations need to be aware of the likelihood of past and future victimization and its effects on mental health. Homeless persons may benefit from learning to identify risk situations for victimization and how to de-escalate potentially violent situations.43
Statistics aside, common sense would seem to suggest that being out at night on the streets raises the risk of being victimized. It is possible that there is a bidirectional causation, with homelessness increasing the risk of victimization, and vice versa. Longitudinal prospective studies will be needed to resolve these questions.
In summary, the available evidence indicates that homelessness and violent victimization are associated with each other in persons with severe mental illness. When the computation of the OR is set so that homelessness is entered as a risk factor for victimization, then homelessness increases the risk approximately two- to threefold. However, the cross-sectional studies that generated these ORs33,34,40 cannot resolve questions pertaining to causality, mainly because they ignore the time sequence of events. It is possible that, instead of homelessness increasing the risk of victimization, victimization can be one of the factors that causally contribute to homelessness, as suggested by the results reviewed in the first paragraph of this section.31
Victimization and offending in patients with severe mental illness
This topic has been studied from two perspectives: comparisons of rates (or risks) of victimization and offending, and relationships between these two variables. An early and influential paper representing the first perspective was briefly mentioned in the section “Comorbid substance use and personality disorders”.42 The authors concluded that individuals in their sample of 172 individuals with severe mental illness in Los Angeles were at least 14 times more likely to be victims of a violent crime than to be arrested for one.42
The first perspective has been reviewed in a study which found that among outpatients, 2%–13% had perpetrated violence in the past 6 months to 3 years, compared with 20%–34% who had been violently victimized. Studies combining outpatients and inpatients reported that 12%–22% had perpetrated violence in the past 6–18 months, compared with 35% who had been a victim in the past year.8 Thus, the existing literature indicates that the prevalence of victimization in patients with severe mental illness is greater than the prevalence of violent behavior or violent offending.
The second perspective is concerned with relationships between victimization and offending. Several studies addressed this problem. A US study of 1,839 patients with severe mental illness examined the relationship between victimization and offending.31 History of a criminal conviction was associated with having been robbed (r=0.09, P<0.05), threatened with a weapon (r=0.12, P<0.001), and beaten (r=0.10, P<0.01).
Relationships between victimization and offending were examined in a sample of 331 involuntarily admitted patients with severe mental illness.47 The sample is described in a related publication48 by the same group summarized in Table 1. The authors examined the effects of victimization on violence. Their analysis used a measure of violence perpetrated by the patients as the dependent variable; the independent variables were demographic, clinical, and social. Young age, substance-use problems, and being a victim of a crime predicted patients’ violence significantly and independently of each other. For victimization, the OR=1.76 (95% CI=1.11–2.79, P<0.05).
Logistic regression was used to estimate the bivariate association between being violent toward others and violent victimization. The OR=7.12 (P<0.001).22 Patients with severe mental illness who had been charged with a criminal offense (n=807) were more likely (OR=4.80, 95% CI=3.71–6.20, P≤0.001) than nonoffenders with severe mental illness (n=2,413) to have a record of violent victimization, and more likely (OR=3.07, 95% CI=2.55–3.69, P≤0.001) to have a record of nonviolent victimization, after controlling for the effects of age, sex, and substance-use disorders.5
Emerging evidence reveals the importance of temporal relationship between victimization and subsequent violent behavior. A study examined prospectively whether recent victimization increases the risk of future violence.49 It was found that violent victimization in the past 6 months significantly predicted violent behavior in the subsequent 2 years in a sample of 167 patients. Logistic regression yielded the OR=1.92 (P≤0.039).
In summary, a statistically significant relationship between victimization and violent behavior by patients with severe mental illness has been clearly established in cross-sectional studies and in one recent prospective longitudinal study.
Impact, prevention, and management of victimization
Victimization of persons with severe mental illness is not without adverse consequences. Recent victimization was demonstrated to elevate the risk of homelessness and reduce the quality of life in a study that was described in detail in the section “Homelessness”.31
A study aimed to identify proximal and distal factors associated with real-life community functioning among 225 men with severe mental illness in Canada, Finland, Germany, and Sweden.50 Participants were assessed at discharge from hospital and at 6-monthly intervals during a 2-year period. Five predictors were significantly associated with patients’ real-life functioning: two adult lifetime variables – a diagnosis of drug abuse/dependence and level of education, and three current variables – victimization, depression, and medication noncompliance. The standardized regression coefficient between the community functioning score and the number of victimizations in the year preceding the assessment was -0.28 (95% CI=-0.43 to -0.12), P=0.000, indicating that the impairment of community functioning increased highly significantly with victimization.50
The contributions of violent victimization and noninterpersonal traumatic experiences to symptomatology were examined in a US study of 70 schizophrenia or schizoaffective disorder patients.51 A total of 22 patients met the criteria for a past diagnosis of PTSD during their lifetime. Patients with comorbid PTSD presented with significantly more anxiety and dysphoria symptoms and schizophrenia illness chronicity than their non-PTSD counterparts. Past traumatic and victimization experiences were significantly associated with patients’ symptom severity and illness course.51
Systematic approaches to reduce or prevent victimization in persons with severe mental illness have not yet been formulated. It turned out that protection from criminal victimization appears to be a positive, unintended consequence of outpatient commitment.52 In a US study of 188 involuntarily hospitalized patients, 99 were randomly assigned to be released and 85 to continue under outpatient commitment after hospital discharge. An additional group of patients with a recent history of serious violent behavior (N=39) was nonrandomly assigned to at least a brief period of outpatient commitment following hospital discharge. All three groups were followed for 1 year. Subjects who were ordered to outpatient commitment were less likely to be criminally victimized than those who were released without outpatient commitment. Multivariate analysis indicated that outpatient commitment reduced the risk of criminal victimization and that outpatient commitment had its effect through improved medication adherence, reduced substance use or abuse, and fewer violent incidents.52
Finally, caring for patients with severe mental illness results in considerable strain. A study of 289 family caregivers revealed that violent victimization of the patients increases the caregivers’ financial burden.53
In summary, victimization has a negative impact on many aspects of the lives of patients and their families. Outpatient commitment may be one of the possible ways to reduce the risk of victimization.
Discussion
Patients with severe mental illness are more likely to be violently victimized than other community members. The risk for patients may vary depending on the community in which they are living. Past traumatic and victimization experiences are significantly associated with patients’ symptom severity and illness course. Women with severe mental illness are more likely to be subjected to sexual violence than males with severe mental illness, and females or males without severe mental illness. It is not clear whether nonsexual violent victimization is more frequent in males or females with severe mental illness. Victimization rates appear to decrease with age.
Relationship between victimization and violent behavior by patients with severe mental illness has been clearly confirmed. It is not clear whether past victimization predicts future violence, or past violence predicts future victimization, or both.
Although patients with serious mental illness are more likely to be victims than perpetrators of violence, it should be noted they commit more violent perpetration than the general public. The elevated risk for violence is partly due to comorbid substance use54 and partly to mental illness itself.55,56
There are multiple reasons why persons with severe mental illness are more likely to be victimized than their peers in general population. The illness impairs their ability to manage conflict situations as well as expressing negative feelings and putting demands on others.57 These problems contribute to higher risk for victimization as well as perpetration, and the mentally ill may be involved in confrontations in which they ultimately become victimized. It is not always clear who started the fight. Psychotic symptoms increase the likelihood of being victimized. Specifically, threat-control/override delusions were reported to significantly increase the risk.58 These delusions include beliefs that there are people seeking to harm the patient (threat) or that outside forces are in control of his/her mind (control/override).
The mentally ill live predominantly in socially disorganized areas characterized by high levels of crime and victimization.59 They are frequently homeless. In general, life on the streets elevates the risk of victimization.60 Finally, comorbid substance-use disorders increase the risk of victimization by several mechanisms described earlier.
Routine clinical care after discharge should include assertive management of medication adherence, as well as vigorous effort to detect and treat comorbid-substance-use disorders. In order to deal with ongoing victimization, it has to be detected by the clinician. That means that questions regarding this issue should be included into routine psychiatric examinations of persons with severe mental illness. Concurrently, the possibility of current or past PTSD should be explored. When victimization is present, the clinician should design and implement interventions to help the patients protect themselves. If possible and appropriate, the patient’s family should be involved in these efforts. Reducing homelessness among persons with severe mental illness will go a long way toward reducing victimization. Cognitive-behavioral programs that reduce rearrest and rehospitalization rates in patients with severe mental illness and histories of aggression and crime61,62 should also be helpful in reducing victimization.
The literature covered by this review has multiple limitations. The assessment methods of victimization vary quite widely across studies. The assessments usually rely on self-reports. There is some evidence that individuals with severe mental illness can, in most cases, provide consistent information about traumatic events;20 nevertheless, reliability of such self-reports may be questioned. The definition of severe mental illness, the principal inclusion criterion for subjects in individual studies, is not always clearly stated, and there is great variation across studies in this respect. Similar problems are apparent with definitions of substance-use disorder and homelessness. These methodological variations may explain the variable results. There is very limited information about the role of treatment in preventing victimization. Another limitation is the cross-sectional design of most studies, which limits inferences about causal mechanisms. Future studies should standardize diagnostic and other assessment procedures, and use longitudinal designs.
Conclusion
Patients with severe mental illness are more likely to be violently victimized than other community members. The risk for patients may vary depending on the community in which they are living. Past traumatic and victimization experiences are significantly associated with patients’ symptom severity and illness course. Women with severe mental illness are more likely to be subjected to sexual violence than males with severe mental illness, and females or males without severe mental illness. It is not clear whether nonsexual violent victimization is more frequent in males or females with severe mental illness. Victimization rates appear to decrease with age. Relationship between victimization and violent behavior by patients with severe mental illness has been clearly confirmed. It is not clear whether past victimization predicts future violence, or past violence predicts future victimization, or both. Reduction of homelessness, treating comorbid substance-use disorders, assertive management of medication adherence, and cognitive-behavioral programs can contribute to reducing of victimization of patients with severe mental illness.
Acknowledgment
This work was supported by the Internal Grant Agency of the Ministry of Health of the Czech Republic NT 11047-2010/4.
Disclosure
The authors report no conflicts of interest in this work.
References
Stone MH. A brief history of psychiatry. In: Tasman A, Kay J, Lieberman JA, editors. Psychiatry. 2nd ed. Chichester, England: John Wiley & Sons, Ltd.; 2003:177–210. | ||
Schoeneman TJ. The role of mental illness in the European witch hunts of the sixteenth and seventeenth centuries. J Hist Behav Sci. 1977;13:337–351. | ||
Lamb HR. Deinstitutionalization at the beginning of the new millennium. Harv Rev Psychiatry. 1998;6:1–10. | ||
Lamb HR. Deinstitutionalization and the homeless mentally ill. Hosp Community Psychiatry. 1984;35:899–907. | ||
Short TB, Thomas S, Luebbers S, Mullen P, Ogloff JR. A case-linkage study of crime victimisation in schizophrenia-spectrum disorders over a period of deinstitutionalisation. BMC Psychiatry. 2013;13:66. | ||
Berzins KM, Petch A, Atkinson JM. Prevalence and experience of harassment of people with mental health problems living in the community. Br J Psychiatry. 2003;183:526–533. | ||
Tsigebrhan R, Shibre T, Medhin G, Fekadu A, Hanlon C. Violence and violent victimization in people with severe mental illness in a rural low-income country setting: a comparative cross-sectional community study. Schizophr Res. 2014;152(1):275–282. | ||
Choe JY, Teplin LA, Abram KM. Perpetration of violence, violent victimization, and severe mental illness: balancing public health concerns. Psychiatr Serv. 2008;59:153–164. | ||
Maniglio R. Severe mental illness and criminal victimization: a systematic review. Acta Psychiatr Scand. 2009;119:180–191. | ||
Van WR, van NM, Myin-Germeys I, van OJ. Childhood trauma as a cause of psychosis: linking genes, psychology, and biology. Can J Psychiatry. 2013;58:44–51. | ||
Sideli L, Mule A, La BD, Murray RM. Do child abuse and maltreatment increase risk of schizophrenia? Psychiatry Investig. 2012;9:87–99. | ||
Huizinga D, Haberstick BC, Smolen A, et al. Childhood maltreatment, subsequent antisocial behavior, and the role of monoamine oxidase A genotype. Biol Psychiatry. 2006;60:677–683. | ||
Goodman LA, Dutton MA, Harris M. Episodically homeless women with serious mental illness: prevalence of physical and sexual assault. Am J Orthopsychiatry. 1995;65:468–478. | ||
Marley JA, Buila S. Crimes against people with mental illness: types, perpetrators, and influencing factors. Soc Work. 2001;46:115–124. | ||
Trevillion K, Oram S, Feder G, Howard LM. Experiences of domestic violence and mental disorders: a systematic review and meta-analysis. PLoS One. 2012;7:e51740. | ||
Oram S, Trevillion K, Feder G, Howard LM. Prevalence of experiences of domestic violence among psychiatric patients: systematic review. Br J Psychiatry. 2013;202:94–99. | ||
Fitzgerald PB, de Castella AR, Filia KM, Filia SL, Benitez J, Kulkarni J. Victimization of patients with schizophrenia and related disorders. Aust N Z J Psychiatry. 2005;39:169–174. | ||
Cusack KJ, Frueh BC, Brady KT. Trauma history screening in a community mental health center. Psychiatr Serv. 2004;55:157–162. | ||
Pandiani JA, Banks SM, Carroll BB, Schlueter MR. Crime victims and criminal offenders among adults with serious mental illness. Psychiatr Serv. 2007;58:1483–1485. | ||
Goodman LA, Thompson KM, Weinfurt K, et al. Reliability of reports of violent victimization and posttraumatic stress disorder among men and women with serious mental illness. J Trauma Stress. 1999;12:587–599. | ||
Coverdale JH, Turbott SH. Sexual and physical abuse of chronically ill psychiatric outpatients compared with a matched sample of medical outpatients. J Nerv Ment Dis. 2000;188:440–445. | ||
Silver E. Mental disorder and violent victimization: the mediating role of involvement in conflicted social relationships. Criminology. 2002;40:191–212. | ||
Teplin LA, McClelland GM, Abram KM, Weiner DM. Crime victimization in adults with severe mental illness: comparison with the National Crime Victimization Survey. Arch Gen Psychiatry. 2005;62:911–921. | ||
Hsu CC, Sheu CJ, Liu SI, Sun YW, Wu SI, Lin Y. Crime victimization of persons with severe mental illness in Taiwan. Aust N Z J Psychiatry. 2009;43:460–466. | ||
Blitz CL, Wolff N, Shi J. Physical victimization in prison: the role of mental illness. Int J Law Psychiatry. 2008;31:385–393. | ||
Kamperman AM, Henrichs J, Bogaerts S, et al. Criminal victimisation in people with severe mental illness: a multi-site prevalence and incidence survey in the Netherlands. PLoS One. 2014;9:e91029. | ||
Wood SR, Buttaro A Jr. Co-occurring severe mental illnesses and substance abuse disorders as predictors of state prison inmate assaults. Crime Delinquency. 2013;59(4):510–535. | ||
Steadman HJ, Mulvey EP, Monahan J, et al. Violence by people discharged from acute psychiatric inpatient facilities and by others in the same neighborhoods. Arch Gen Psychiatry. 1998;55:393–401. | ||
US Bureau of the Census. Technical Background on the Redesigned National Crime Victimization Survey. Washington, DC: US Bureau of the Census; 1994. | ||
Planty M, Langton L, Krebs C, Berzofsky M, Smiley-McDonald H. Female Victims of Sexual Violence, 1994–2010. Washington, DC: U.S. Department of Justice, Office of Justice Programs, Bureau of Justice Statistics; 2013. | ||
Lam JA, Rosenheck R. The effect of victimization on clinical outcomes of homeless persons with serious mental illness. Psychiatr Serv. 1998;49:678–683. | ||
Brunette MF, Drake RE. Gender differences in patients with schizophrenia and substance abuse. Compr Psychiatry. 1997;38:109–116. | ||
White MC, Chafetz L, Collins-Bride G, Nickens J. History of arrest, incarceration and victimization in community-based severely mentally ill. J Community Health. 2006;31:123–135. | ||
Walsh E, Moran P, Scott C, et al; UK700 Group. Prevalence of violent victimisation in severe mental illness. Br J Psychiatry. 2003;183:233–238. | ||
Goodman LA, Salyers MP, Mueser KT, et al. Recent victimization in women and men with severe mental illness: prevalence and correlates. J Trauma Stress. 2001;14:615–632. | ||
Dean K, Moran P, Fahy T, et al. Predictors of violent victimization amongst those with psychosis. Acta Psychiatr Scand. 2007;116:345–353. | ||
Pernanen K. Alcohol in Human Violence. 1 ed. New York: The Guilford Press; 1991. | ||
Wolfgang ME. Patterns in Criminal Homicide. Philadelphia: University of Pennsylvania; 1958. | ||
Crump C, Sundquist K, Winkleby MA, Sundquist J. Mental disorders and vulnerability to homicidal death: Swedish nationwide cohort study. BMJ. 2013;346:f557. | ||
Chapple B, Chant D, Nolan P, Cardy S, Whiteford H, McGrath J. Correlates of victimisation amongst people with psychosis. Soc Psychiatry Psychiatr Epidemiol. 2004;39:836–840. | ||
Honkonen T, Henriksson M, Koivisto AM, Stengard E, Salokangas RK. Violent victimization in schizophrenia. Soc Psychiatry Psychiatr Epidemiol. 2004;39:606–612. | ||
Brekke JS, Prindle C, Bae SW, Long JD. Risks for individuals with schizophrenia who are living in the community. Psychiatr Serv. 2001;52:1358–1366. | ||
Larney S, Conroy E, Mills KL, Burns L, Teesson M. Factors associated with violent victimisation among homeless adults in Sydney, Australia. Aust N Z J Public Health. 2009;33:347–351. | ||
Volavka J. Neurobiology of Violence. 2 ed. Washington, DC: American Psychiatric Publishing, Inc; 2002. | ||
Volavka J. Comorbid personality disorders and violent behavior in psychotic patients. Psychiatr Q. 2014;85:65–78. | ||
Hodgins S, Cree A, Alderton J, Mak T. From conduct disorder to severe mental illness: associations with aggressive behaviour, crime and victimization. Psychol Med. 2008;38:975–987. | ||
Hiday VA, Swanson JW, Swartz MS, Borum R, Wagner HR. Victimization: a link between mental illness and violence? Int J Law Psychiatry. 2001;24:559–572. | ||
Hiday VA, Swartz MS, Swanson JW, Borum R, Wagner HR. Criminal victimization of persons with severe mental illness. Psychiatr Serv. 1999;50:62–68. | ||
Sadeh N, Binder RL, McNiel DE. Recent victimization increases risk for violence in justice-involved persons with mental illness. Law Hum Behav. 2014;38:119–125. | ||
Hodgins S, Lincoln T, Mak T. Experiences of victimisation and depression are associated with community functioning among men with schizophrenia. Soc Psychiatry Psychiatr Epidemiol. 2009;44:448–457. | ||
Newman JM, Turnbull A, Berman BA, Rodrigues S, Serper MR. Impact of traumatic and violent victimization experiences in individuals with schizophrenia and schizoaffective disorder. J Nerv Ment Dis. 2010;198:708–714. | ||
Hiday VA, Swartz MS, Swanson JW, Borum R, Wagner HR. Impact of outpatient commitment on victimization of people with severe mental illness. Am J Psychiatry. 2002;159:1403–1411. | ||
Thompson MS. Violence and the costs of caring for a family member with severe mental illness. J Health Soc Behav. 2007;48:318–333. | ||
Fazel S, Langstrom N, Hjern A, Grann M, Lichtenstein P. Schizophrenia, substance abuse, and violent crime. JAMA. 2009;301:2016–2023. | ||
Van Dorn R, Volavka J, Johnson N. Mental disorder and violence: is there a relationship beyond substance use? Soc Psychiatry Psychiatr Epidemiol. 2012;47:487–503. | ||
Volavka J, Swanson J. Violent behavior in mental illness: the role of substance abuse. JAMA. 2010;304:563–564. | ||
Bellack AS, Mueser KT, Wade J, Sayers S, Morrison RL. The ability of schizophrenics to perceive and cope with negative affect. Br J Psychiatry. 1992;160:473–480. | ||
Teasdale B. Mental disorder and violent victimization. Crim Justice Behav. 2009;36:513–530. | ||
Logdberg B, Nilsson LL, Levander MT, Levander S. Schizophrenia, neighbourhood, and crime. Acta Psychiatr Scand. 2004;110:92–97. | ||
Simons RL, Whitbeck LB, Bales A. Life on the streets: victimization and psychological distress among the adult homeless. J Interpers Violence. 1989;14(4):482–501. | ||
Haddock G, Barrowclough C, Shaw JJ, Dunn G, Novaco RW, Tarrier N. Cognitive-behavioural therapy v. social activity therapy for people with psychosis and a history of violence: randomised controlled trial. Br J Psychiatry. 2009;194:152–157. | ||
Yates KF, Kunz M, Khan A, Volavka J, Rabinowitz S. Psychiatric patients with histories of aggression and crime five years after discharge from a cognitive-behavioral program. J Forensic Psychiatry Psychol. 2010;21:167–188. | ||
Bengtsson-Tops A, Ehliasson K. Victimization in individuals suffering from psychosis: a Swedish cross-sectional study. J Psychiatr Ment Health Nurs. 2012;19:23–30. | ||
Crisanti AS, Frueh BC, Archambeau O, Steffen JJ, Wolff N. Prevalence and correlates of criminal victimization among new admissions to outpatient mental health services in Hawaii. Community Ment Health J. 2014;50:296–304. | ||
Dolan M, O’Malley K, McGregor K. The role of psychopathic traits and substance abuse in predicting violent victimization in patients with schizophrenia spectrum disorders. Pers Ment Health. 2013;7(1):28–38. | ||
Fortugno F, Katsakou C, Bremner S, et al. Symptoms associated with victimization in patients with schizophrenia and related disorders. PLoS One. 2013;8:e58142. | ||
Friedman SH, Loue S, Goldman Heaphy EL, Mendez N. Intimate partner violence victimization and perpetration by Puerto Rican women with severe mental illnesses. Community Ment Health J. 2011;47:156–163. | ||
McFarlane A, Schrader G, Bookless C, Browne D. Prevalence of victimization, posttraumatic stress disorder and violent behaviour in the seriously mentally ill. Aust N Z J Psychiatry. 2006;40:1010–1015. | ||
Mericle AA, Havassy BE. Characteristics of recent violence among entrants to acute mental health and substance abuse services. Soc Psychiatry Psychiatr Epidemiol. 2008;43:392–402. | ||
Mueser KT, Salyers MP, Rosenberg SD, et al; 5 Site Health and Risk Study Research Committee. Interpersonal trauma and posttraumatic stress disorder in patients with severe mental illness: demographic, clinical, and health correlates. Schizophr Bull. 2004;30:45–57. | ||
Schomerus G, Heider D, Angermeyer MC, et al. Urban residence, victimhood and the appraisal of personal safety in people with schizophrenia: results from the European Schizophrenia Cohort (EuroSC). Psychol Med. 2008;38:591–597. | ||
Silver E, Piquero AR, Jennings WG, Piquero NL, Leiber M. Assessing the violent offending and violent victimization overlap among discharged psychiatric patients. Law Hum Behav. 2011;35:49–59. | ||
Swanson JW, Swartz MS, Essock SM, et al. The social-environmental context of violent behavior in persons treated for severe mental illness. Am J Public Health. 2002;92:1523–1531. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.