")
Back to Journals » Cancer Management and Research » Volume 10
Villoglandular adenocarcinoma of cervix: pathologic features, clinical management, and outcome
Authors Guo P , Liu PF, Yang JJ, Ren T, Xiang Y
Received 17 February 2018
Accepted for publication 28 April 2018
Published 26 September 2018 Volume 2018:10 Pages 3955—3961
DOI https://doi.org/10.2147/CMAR.S165817
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Harikrishna Nakshatri
Peng Guo,1,2,* Pengfei Liu,1,* Junjun Yang,1 Tong Ren,1 Yang Xiang1
1Department of Obstetrics and Gynecology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing 100730, People’s Republic of China; 2Department of Obstetrics and Gynecology, The First Affiliated Hospital of Sun Yat-sen University, Guangzhou 510080, People’s Republic of China
*These authors contributed equally to this work
Background: The objective of the study was to investigate the management and prognosis of patients with villoglandular adenocarcinoma (VGA) of the uterine cervix.
Materials and methods: The clinical presentation, pathology, management, and prognosis of 41 patients with VGA or other types of cervical adenocarcinoma (ADC) were retrospectively reviewed.
Results: During the patient follow-up period, the proportion of VGA was 8.1% in the cervical ADC cohort (41/507). The median age of the patients with VGA was 41.0 years. The most common presenting symptom was cervical contactive bleeding. There were 38 patients classified as FIGO stage IA1–IB. The median follow-up period was 38.5 months. There were no patient deaths, and only one patient showed recurrence. One of the patients delivered a healthy baby at 34 weeks of gestation prior to treatment with radical hysterectomy. The HPV HC2 test results showed that most patients were positive for HPV infection. HPV 16, 18, and 56 were positive in the 8 patients with HPV type test results. There were significant differences in the grade, depth of stromal invasion, lymph node metastasis, and recurrence between the VGA cases of FIGO stage I and the other types of cervical ADC of FIGO stage I (p<0.05).
Conclusion: This study confirmed that VGA is a type of well-differentiated cervical cancer characterized by shallow stromal invasion, less lymph node metastasis. VGA is associated with less recurrence than other types of cervical ADC.
Keywords: villoglandular adenocarcinoma, uterine cervix, management, prognosis
Introduction
The incidence of cervical adenocarcinoma (ADC) has increased over the past several decades in young women, and there has been a marked decrease in cervical squamous cell carcinoma (SCC).1,2 The proportion of ADC steadily increased from 5% to more than 20%.3 ADC is more difficult to detect and has a worse outcome than SCC. Additionally, ADC has a higher incidence of lymph node metastasis, distant metastases, recurrences, and worse survival outcome.3–5
Villoglandular adenocarcinoma (VGA) of the cervix was first reported by Young and Scully in 1989.6 VGA is a rare well-differentiated subtype of ADC that usually occurs in young women and is associated with a better prognosis than ADC.7,8 Histologically, VGA is a superficially infiltrative tumor with an exophytic growth with long and slender papillary form, limited mitosis, minimal cytologic atypia, and minimal vascular space invasion.9,10 VGA is characterized as superficially infiltrative and shows infrequent lymph node invasion and lymphovascular space invasion.11,12 Therefore, conservative surgery such as cone biopsy is conducted.13,14 However, the present recognition and evaluation of this rare tumor type is limited. In this study, we reviewed the clinical and pathological features of 41 patients with VGA and investigated the risk factors for clinical treatment and prognosis.
Materials and methods
The data of patients with ADC from January 1995 to January 2017 (Peking Union Medical College Hospital [PUMCH], People’s Republic of China) were retrospectively reviewed, and written informed consent was obtained from each patient. The procedures were approved by the Ethics Committee of Human Experimentation of PUMCH and are in accordance with the Helsinki Declaration of 1964.
In this study, 41 patients with VGA were identified in the cohort of 507 ADC patients. The standards of pathological VGA diagnosis were the following: 1) a diagnosis made based on complete excision of the primary tumor, rather than on biopsy; 2) the tumor presented as a villoglandular structure or papillary structure with vascular axis, and the invasion is limited to the tumor edge without deep infiltration; and 3) the cellular morphology is relatively mild, nuclei show mild or moderate atypia, and karyokinesis is infrequent. In PUMCH, every pathological diagnosis was made by two pathologists and reviewed by a senior pathologist. Every intractable case would be discussed in department to make sure that the histopathological diagnoses were reliable.
The χ2 test was used for comparisons of qualitative data and for the clinicopathological parameters between VGA and other types of ADC. Fisher’s exact test was used when the 2 cells (50%) had an expected count less than 5. A t-test was used for the quantitative data. Statistical significance was assumed as p<0.05. The statistical analyses were performed using the SPSS 13.0 statistical software.
Results
There were 41 patients diagnosed with VGA (8.1%) during the study period. The median patient age was 41.0 years (range, 27–66 years). The most common presenting symptom was cervical contactive bleeding (28/41). The FIGO stage was IA in 4 patients, IB in 34 patients, IIA in 1 patient, and IIB in 2 patients. There were 32 patients who received imaging examinations including color Doppler ultrasonography, magnetic resonance imaging (MRI), computed tomography (CT), and positron emission tomography–computed tomography (PET-CT). The imaging examinations of 28 patients showed cervical placeholder and malignant lesions.
In the cohort of 37 patients who were treated with radical hysterectomy with or without pelvic lymphadenectomy (6/37), 30 patients received bilateral salpingo-oophorectomy (BSO) and 7 received bilateral salpingectomy for ovary conservation. Two patients who desired to preserve fertility received pelvic lymphadenectomy to confirm that there was no lymph node metastasis before receiving further radical vaginal trachelectomy. There were 15 patients who received adjuvant treatments. The detailed treatment descriptions and decisions for treatment are shown in Table 1.
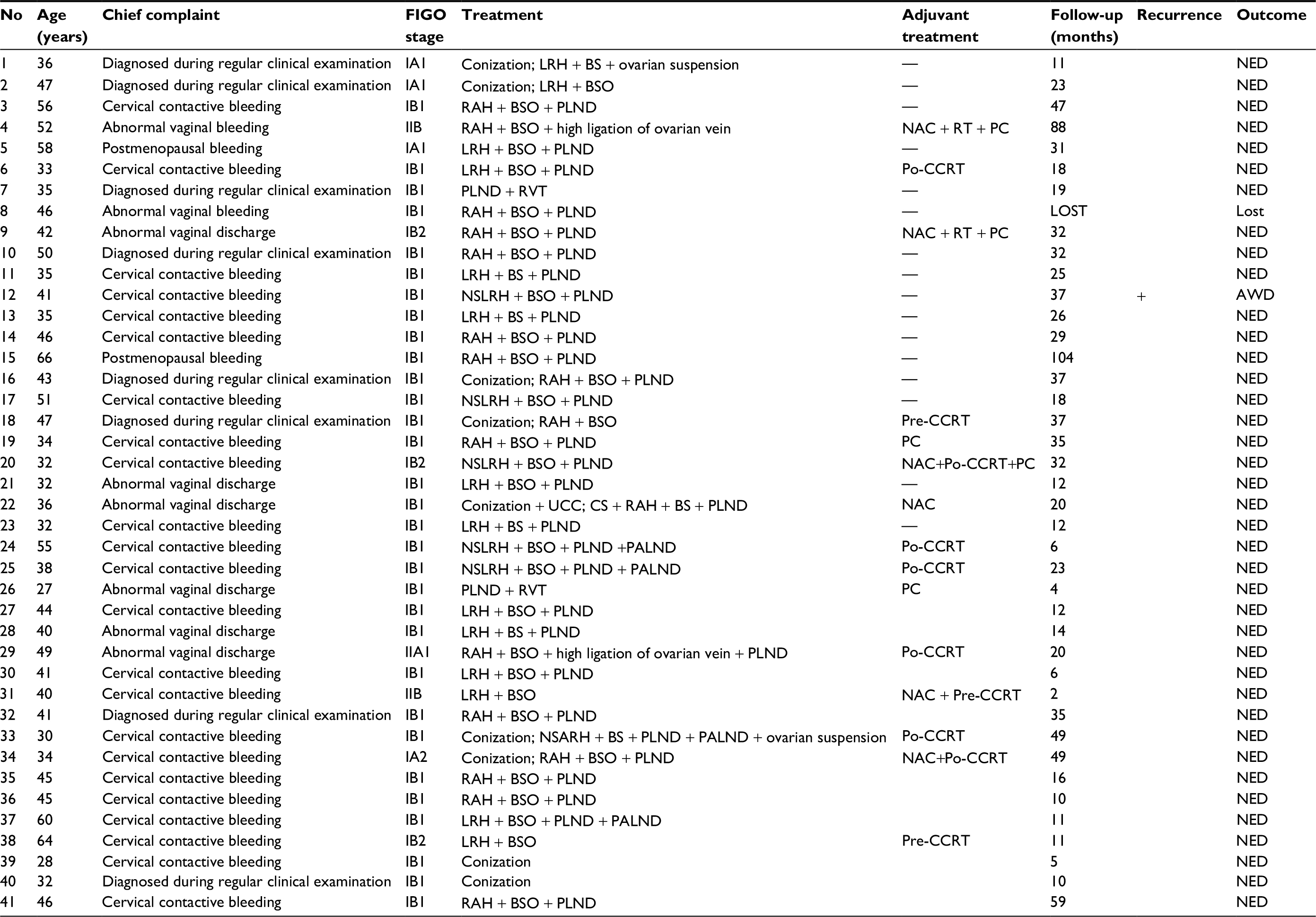 | Table 1 The clinical characteristics, treatment, and follow-up of patients with VGA Abbreviations: VGA, villoglandular adenocarcinoma; AWD, alive with disease; BS, bilateral salpingectomy; BSO, bilateral salpingo-oophorectomy; Po-CCRT, postoperative concurrent chemoradiation therapy; Pre-CCRT, preoperative concurrent chemoradiation therapy; CS, cesarean section; LRH, laparoscopic radical hysterectomy; NAC, neoadjuvant chemotherapy; NED, no evidence of disease; NSARH, nerve-sparing abdominal radical hysterectomy; NSLRH, nerve-sparing laparoscopic radical hysterectomy; PC, postoperative chemotherapy; PALND: paraortic lymph node dissection; PLND, pelvic lymph node dissection; RAH, radical abdominal hysterectomy; RT, radiation therapy; RVT, radical vaginal trachelectomy; UCC, uterine cervical cerclage. |
The median follow-up period was 38.5 months (range 19–121 months), and there were no patient deaths during this time. One patient showed recurrent disease. The presenting symptom of the recurrent patient was cervical contactive bleeding, and the cytological test was negative. Additionally, the CA125 level was elevated (69.1 U/mL). The patient was FIGO stage IB1 and underwent nerve-sparing laparoscopic radical hysterectomy, BSO, and pelvic lymphadenectomy. The pathology showed well-differentiated VGA, and the infiltration depth was 5 mm. There were no adjuvant treatments conducted. The tumor recurred in the pelvic 8 months after initial surgery. The PET-CT indicated there was a highly metabolic lesion on the left side of the pelvic floor, and the serum CA125 level was increased to 71.2 U/mL. Exploratory laparotomy was conducted to remove the pelvic mass. The pathology results indicated metastatic ADC. The immunohistochemistry indicated AE1/AE3 (+), CEA (+), p16 (+), and p53 (+). The patient received 6 courses of postoperative chemotherapy. However, at 20 months after the initial surgery, an ultrasound test showed a mass with low density in the vaginal stump. The biopsy results showed well-differentiated VGA. The patient received concurrent chemoradiation therapy.
One patient was diagnosed with VGA at 13 weeks of gestation with FIGO stage IB1. MRI indicated no signs of lymph node metastasis. The patient received conization and cervical cerclage at 16 weeks of gestation. The pathology showed moderately differentiated VGA and there was a negative margin. The patient received 4 courses of chemotherapy with regimens of paclitaxel (240 mg) plus carboplatin (400 mg) at 20 weeks of gestation. At 34 weeks of gestation, the patient underwent cesarean section, radical abdominal hysterectomy, bilateral salpingectomy, and pelvic lymph node dissection. The postoperative pathology was negative. There was no recurrence during the follow-up period of 37 months, and the baby was healthy.
There were 28 patients who received cytological testing within 3 months prior to surgery. There was 1 patient with atypical squamous cells of undetermined significance, and 3 patients showed cervical ADC. Additionally, there were 5 patients with high-grade squamous intraepithelial lesion and 6 patients with atypical glandular cell. The remaining 13 patients had negative results. We found that 9 of 12 patients with HPV HC2 test results were positive for HPV infection. HPV 16, 18, and 56 were positive in the 8 patients with HPV type test results. The cytology and HPV testing results are shown in Table 2. The immunohistochemistry results indicated positive p16 and Ki-67 expression but negative PR and ER expression in most patients.
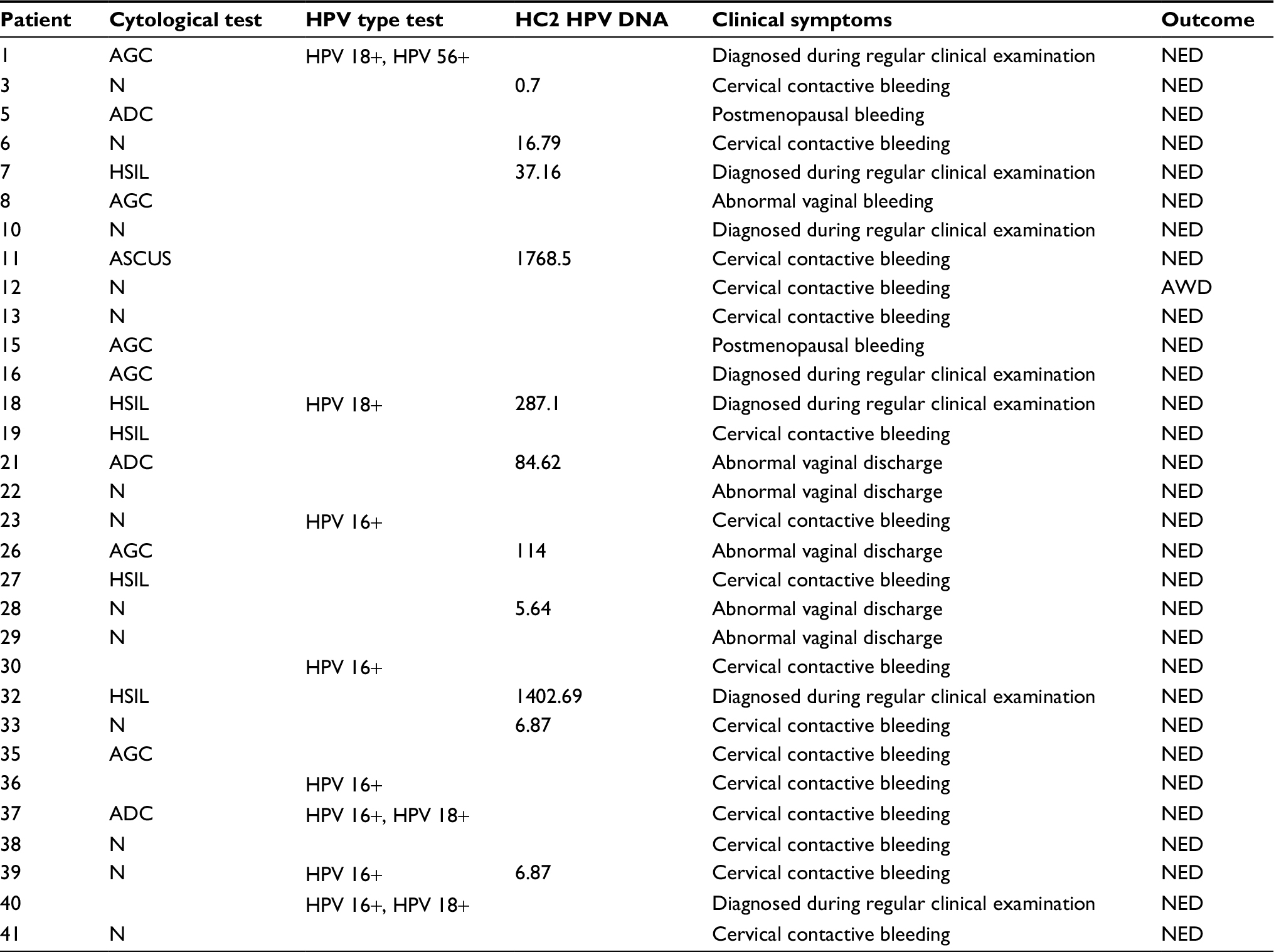 | Table 2 Cytological test and HPV test with VGA of the cervix Abbreviations: VGA, villoglandular adenocarcinoma; ADC, adenocarcinoma; AGC, atypical glandular cell; AWD, alive with disease; ASCUS, atypical squamous cells of undetermined significance; HSIL, high-grade squamous intraepithelial lesion; N, negative; NED, no evidence of disease. |
There were 41 patients with VGA and 326 patients with ADC who received radical hysterectomy in the cohort of 507 ADC patients. The clinicopathological parameters of the 41 patients with VGA and 326 patients with ADC were compared. The data in Table 3 show that there were significant differences in the grade, depth of stromal invasion, lymph node metastasis, and recurrence between the VGA cases of FIGO stage I and the other types of cervical ADC of FIGO stage I (p<0.05). VGA is a type of well-differentiated cervical cancer characterized by shallow stromal invasion, less lymph node metastasis, and less recurrence than other types of cervical ADC.
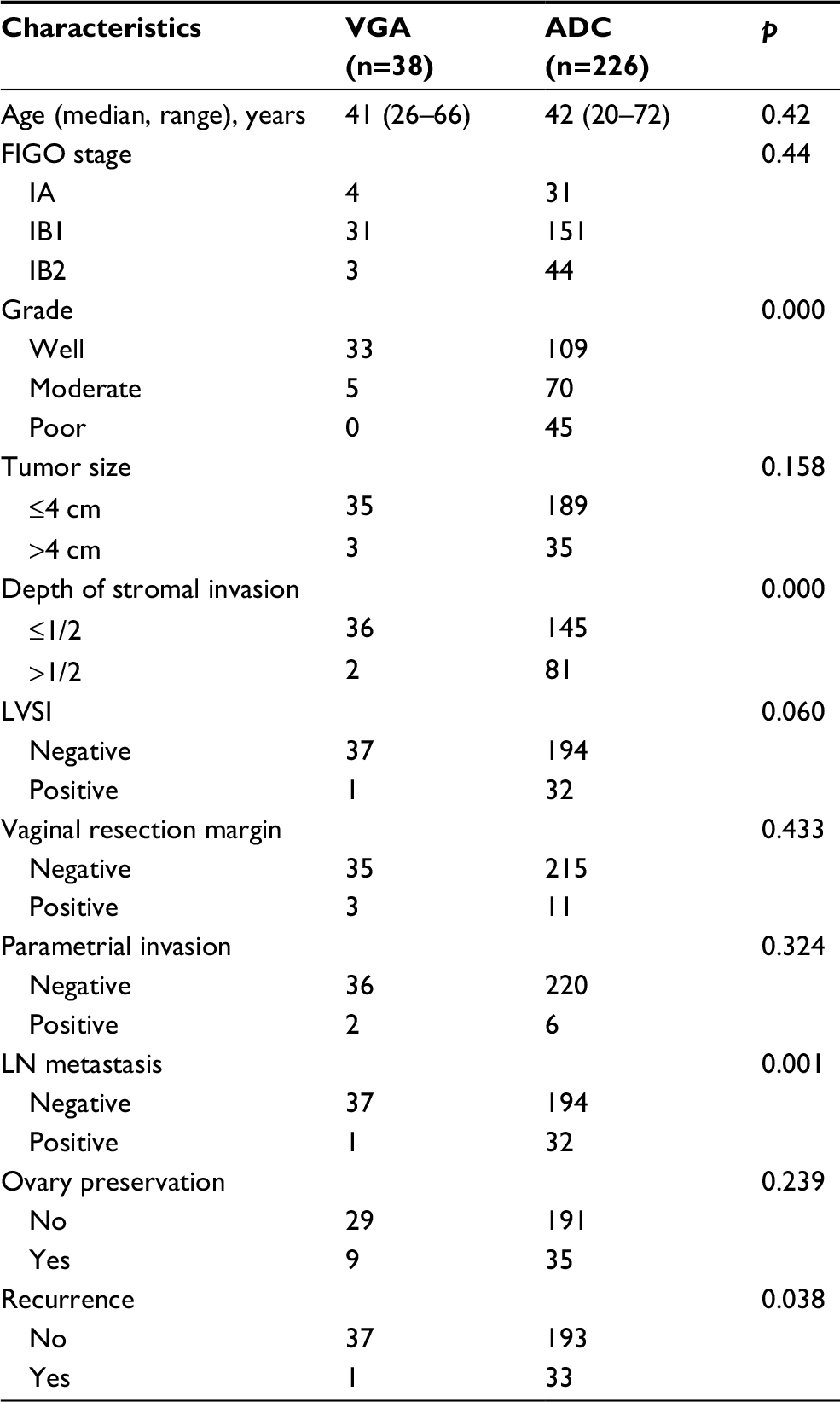 | Table 3 Comparison of VGA with other ADCs of FIGO I on clinicopathological parameters Abbreviations: VGA, villoglandular adenocarcinoma; ADCs, adenocarcinomas; LN, lymph node; LVSI, lymph vascular space invasion. |
Discussion
VGA of the cervix has a younger patient prevalence and better prognosis than other variants of cervical ADC. As shown in Table 4, we reviewed the VGA literature for the cervix and found there were a total of 203 patients with VGA reported. The patients’ ages ranged from 33 to 52 years, and the majority of patients were FIGO stage I. There were 13 patients presenting with LVSI, 7 patients with LN metastasis, 12 patients with recurrence, and 8 patients who died of this disease.6,7,12,13,15–24
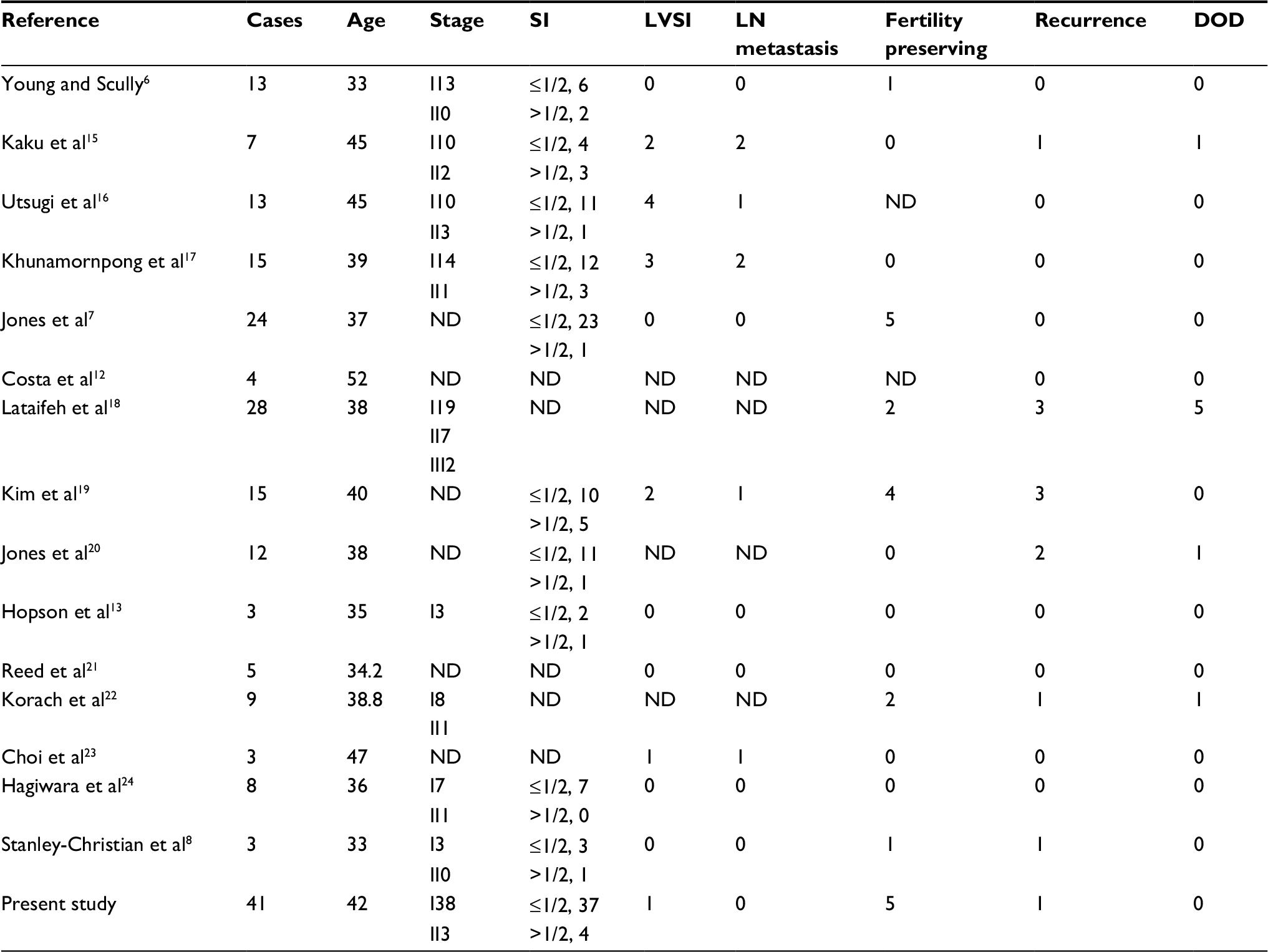 | Table 4 Literature review of VGA Abbreviations: VGA, villoglandular adenocarcinoma; DOD, died of disease; LN, lymph node; LVSI, lymph vascular space invasion; ND, not described; SI, stromal invasion. |
In this study, 1 patient had disease recurrence and was alive with disease. There were no obvious risk factors in this patient except for the consistent elevated serum CA125 level during the preoperative and follow-up period.
The favorable prognosis for VGA patients permits a more conservative surgical approach in selected patients including young women with localized disease and those who wish to maintain fertility.25 There were 16 patients reported in the literature who underwent fertility-preserving surgery such as cervical conization and radical trachelectomy.6,7,12,13,15–24 In this study, 2 patients who desired to preserve fertility received pelvic lymphadenectomy to rule out lymph node metastasis. Radical vaginal trachelectomy was then conducted, and there was no recurrence during the follow-up period. Currently, surgical resection range and treatment options for ADC patients are considered to be uses in VGA patients. But, our clinical data and previous studies indicate that VGA is less invasive than ADCs. As VGA has more positive prognosis, the surgery extent could be narrowed for stage I VGA patients. This is what should be further studied in future.
The treatment for cervical cancer associated with pregnancy is complicated, and there is currently no specific treatment scheme. Previous studies reported less radical fertility-sparing surgery for patients in FIGO stage IA2–IB1. The treatment included laparoscopic pelvic lymphadenectomy and cervical conization, which was then followed by neoadjuvant chemotherapy.26–28 In the VGA patients of this study, we compared the recurrence between with and without adjuvant treatment; the patients with adjuvant treatment showed less recurrence rate (p<0.001). Several studies compared primary surgery or concurrent chemoradiation therapy in pregnant women with FIGO stage IB cervical cancer with delivery delay. Neoadjuvant chemotherapy of paclitaxel plus cisplatin followed by radical surgery and postoperative chemotherapy could be considered a feasible alternative to preserve fertility.29,30 One patient in this study maintained pregnancy until 34 weeks of gestation before radical hysterectomy and delivered a healthy baby. MRI for this patient indicated no lymph node metastasis, and cervical conization confirmed the pathological type, grade, depth of stromal invasion, and lymph vascular space invasion. The patient was treated using neoadjuvant chemotherapy with paclitaxel plus cisplatin during the second trimester.
VGA is a rare tumor type that accounts for approximately 5% in cervical ADCs.15 This tumor is histologically characterized by tall and thin papillae with minimal cellular atypia. The characteristic histological features of various epithelia have been reported, and it is known that the papillae are lined by 1 or more layers of cells with endocervical, endometrioid, or intestinal differentiation.31 In this study, preoperative cytological tests were negative in 11 patients (28.9%). The results from the study by Choi et al indicate the abnormal architectural patterns such as three-dimensional papillary structures, nuclear overlapping, and nuclear hyperchromasia are important clues to suspect the possibility of a VGA. However, liquid-based cytology shows better preserved nuclear details such as prominent nucleoli and irregular nuclear membranes and can facilitate the diagnosis of VGA.23
The etiology of VGA remains unclear. Several studies have suggested that HPV infection was involved in the pathogenesis of VGA. The first report of positive HPV 18 in VGA was published in 2000.32 HPV 18 and 16 were significantly associated with VGA in the study of Jones et al.20 It has been shown that HPV infection might be more prevalent in VGA than in other types of ADC.33 Our results demonstrated that HPV testing might be important in the screening and diagnosis of VGA.
This study is a retrospective review and has several limitations. First, the HPV testing was not prevalent in all patients. Therefore, the pathologic role of HPV in VGA should be further investigated. Second, the sample population is limited for this rare tumor, and it is difficult to distinguish VGA from other types of ADC. Thus, it is critical to perform a meta-analysis or more multicenter prospective studies to investigate the most accurate diagnosis and proper treatment for VGA.
Acknowledgment
This research was supported by National Natural Science Foundation of China (81472446) and China Postdoctoral Science Foundation (2012M510354).
Disclosure
The authors report no conflicts of interest in this work.
References
Mathew A, George PS. Trends in incidence and mortality rates of squamous cell carcinoma and adenocarcinoma of cervix-worldwide. Asian Pac J Cancer Prev. 2009;10(4):645–650. | ||
Seoud M, Tjalma WA, Ronsse V. Cervical adenocarcinoma: moving towards better prevention. Vaccine. 2011;29(49):9148–9158. | ||
Galic V, Herzog TJ, Lewin SN, et al. Prognostic significance of adenocarcinoma histology in women with cervical cancer. Gynecol Oncol. 2012;125(2):287–291. | ||
Lee YY, Choi CH, Kim TJ, et al. A comparison of pure adenocarcinoma and squamous cell carcinoma of the cervix after radical hysterectomy in stage IB-IIA. Gynecol Oncol. 2011;120(3):439–443. | ||
Park JY, Kim DY, Kim JH, Kim YM, Kim YT, Nam JH. Outcomes after radical hysterectomy in patients with early-stage adenocarcinoma of uterine cervix. Br J Cancer. 2010;102(12):1692–1698. | ||
Young RH, Scully RE. Villoglandular papillary adenocarcinoma of the uterine cervix. A clinicopathologic analysis of 13 cases. Cancer. 1989;63(9):1773–1779. | ||
Jones MW, Silverberg SG, Kurman RJ. Well-differentiated villoglandular adenocarcinoma of the uterine cervix: a clinicopathological study of 24 cases. Int J Gynecol Pathol.1993;12(1):1–7. | ||
Stanley-Christian H, Heim BK, Hines JF, Hall KL, Willett GD, Barnes WA. Villoglandular adenocarcinoma of the cervix: a report of three cases and review of literature. Gynecol Oncol. 1997;66(2):327–330. | ||
Khunamornpong S, Siriaunkgul S, Suprasert P. Well-differentiated villoglandular adenocarcinoma of the uterine cervix: cytomorphologic observation of five cases. Diagn Cytopathol. 2002;26(1):10–14. | ||
Novotny DB, Ferlisi P. Villoglandular adenocarcinoma of the cervix: cytologic presentation. Diagn Cytopathol. 1997;17(5):383–387. | ||
Macdonald RD, Kirwan J, Hayat K, Herrington CS, Shawki H. Villoglandular adenocarcinoma of the cervix: clarity is needed on the histological definition for this difficult diagnosis. Gynecol Oncol. 2006;100(1):192–194. | ||
Costa MJ, McIlnay KR, Trelford J. Cervical carcinoma with glandular differentiation: histological evaluation predicts disease recurrence in clinical stage I or II patients. Hum Pathol. 1995;26(8):829–837. | ||
Hopson L, Jones MA, Boyce CR, Tarraza HM Jr. Papillary villoglandular carcinoma of the cervix. Gynecol Oncol. 1990;39(2):221–224. | ||
Ballo MS, Silverberg SG, Sidaway MK. Cytologic features of well-differentiated villoglandular adenocarcinoma of the cervix. Acta Cytol. 1996;40(3):536–540. | ||
Kaku T, Kamura T, Shigematsu T, et al. Adenocarcinoma of the uterine cervix with predominantly villoglandular papillary growth pattern. Gynecol Oncol. 1997;64(1):147–152. | ||
Utsugi K, Shimizu Y, Akiyama F, Umezawa S, Hasumi K. Clinicopathologic features of villoglandular papillary adenocarcinoma of the uterine cervix. Gynecol Oncol. 2004;92(1):64–70. | ||
Khunamornpong S, Maleemonkol S, Siriaunkgul S, Pantusart A. Well-differentiated villoglandular adenocarcinoma of the uterine cervix: a report of 15 cases including two with lymph node metastasis. J Med Assoc Thai. 2001;84(6):882–888. | ||
Lataifeh IM, Al-Hussaini M, Uzan C, Jaradat I, Duvillard P, Morice P. Villoglandular papillary adenocarcinoma of the cervix: a series of 28 cases including two with lymph node metastasis. Int J Gynecol Cancer. 2013;23(5):900–905. | ||
Kim J, Sung JH, Lee E, et al. Prognostic factors influencing decisions about surgical treatment of villoglandular adenocarcinoma of the uterine cervix. Int J Gynecol Cancer. 2014;24(7):1299–1305. | ||
Jones MW, Kounelis S, Papadaki H, et al. Well-differentiated villoglandular adenocarcinoma of the uterine cervix: oncogene/tumor suppressor gene alterations and human papillomavirus genotyping. Int J Gynecol Pathol. 2000;19(2):110–107. | ||
Reed W, Abeler VM, Tropé CG. Villous glandular adenocarcinoma of the uterine cervix. A subtype with favourable prognosis? Tidsskr Nor Laegeforen. 1993;113(20):2569–2571. | ||
Korach J, Machtinger R, Perri T, et al. Villoglandular papillary adenocarcinoma of the uterine cervix: a diagnostic challenge. Acta Obstet Gynecol Scand. 2009;88(3):355–358. | ||
Choi Y, Kim H, Choi H, et al. Liquid-based cytology of villoglandular adenocarcinoma of the cervix: a report of 3 cases. Korean J Pathol. 2012;46(2):215–220. | ||
Hagiwara T, Kaku T, Kobayashi H, Wake N, Saito T. Well-differentiated villoglandular adenocarcinoma of the uterine cervix: assessment of cytological features by histological subtypes. Acta Cytol. 2013;57(1):61–68. | ||
Lakhtakia R, Singh MK, Taneja P, Kapila K, Kumar S. Villoglandular papillary adenocarcinoma of the cervix: case report. J Surg Oncol. 2000;74(4):297–299. | ||
Maneo A, Chiari S, Bonazzi C, Mangioni C. Neoadjuvant chemotherapy and conservative surgery for stage IB1 cervical cancer. Gynecol Oncol. 2008;111(3):438–443. | ||
Landoni F, Parma G, Peiretti M, et al. Chemo-conization in early cervical cancer. Gynecol Oncol. 2007;107(1 Suppl 1):S125–S126. | ||
Kong TW, Lee EJ, Lee Y, Chang SJ, Son JH, Ryu HS. Neoadjuvant and postoperative chemotherapy with paclitaxel plus cisplatin for the treatment of FIGO stage IB cervical cancer in pregnancy. Obstet Gynecol Sci. 2014;57(6):539–543. | ||
Li J, Wang LJ, Zhang BZ, Peng YP, Lin ZQ. Neoadjuvant chemotherapy with paclitaxel plus platinum for invasive cervical cancer in pregnancy: two case report and literature review. Arch Gynecol Obstet. 2011;284(3):779–783. | ||
Fruscio R, Villa A, Chiari S, et al. Delivery delay with neoadjuvant chemotherapy for cervical cancer patients during pregnancy: a series of nine cases and literature review. Gynecol Oncol. 2012;126(2):192–197. | ||
Kurman RJ, Ronnett BM, Sherman ME, Wilkinson EJ. Atlas of Tumor Pathology: Tumours of the Cervix, Vagina and Vulva. 4th Series. Washington, DC: American Registry of Pathology; 2010:179–185. | ||
Yamazawa K, Matsui H, Seki K, et al. Human papillomavirus-positive well-differentiated villoglandular adenocarcinoma of the uterine cervix: a case report and review of the literature. Gynecol Oncol. 2000;77(3):473–477. | ||
Duggan MA, McGregor SE, Benoit JL, Inoue M, Nation JG, Stuart GC. The human papillomavirus status of invasive cervical adenocarcinoma: a clinicopathological and outcome analysis. Hum Pathol. 1995;26(3):319–325. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.