")
Back to Journals » Vascular Health and Risk Management » Volume 18
Venous Thromboembolism Among Hospitalized Patients: Incidence and Adequacy of Thromboprophylaxis – A Retrospective Study
Authors Ambra N , Mohammad OH , Naushad VA , Purayil NK , Mohamedali MG, Elzouki AN , Khalid MK, Illahi MN, Palol A, Barman M, Sharif M, Chalihadan S, Punnorath A, Mostafa A, Al Hariri B, Khidir TGM, Varikkodan I
Received 22 April 2022
Accepted for publication 7 July 2022
Published 24 July 2022 Volume 2022:18 Pages 575—587
DOI https://doi.org/10.2147/VHRM.S370344
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Pietro Scicchitano
Naseem Ambra,1 Osama Hashim Mohammad,1,2 Vamanjore A Naushad,1– 3 Nishan K Purayil,1– 3 Mohamed G Mohamedali,1,2 Abdel Naser Elzouki,1– 3 Muayad Kasim Khalid,1 Memon Noor Illahi,1,2 Azeez Palol,1 Manish Barman,1,2 Muhammad Sharif,1,2 Sajid Chalihadan,1 Ashraf Punnorath,1 Abdelrahman Mostafa,1 Bassem Al Hariri,1 Tameem GM Khidir,1 Irfan Varikkodan1
1Department of Medicine, Hamad Medical Corporation, Doha, Qatar; 2Clinical Medicine, Weill Cornell Medicine –Qatar, Doha, Qatar; 3Clinical Department, College of Medicine, QU Health, Qatar University, Doha, Qatar
Correspondence: Naseem Ambra, Department of Medicine, Hamad Medical Corporation, Doha, Qatar, Tel +97455579648, Email [email protected]; [email protected]
Purpose: We aimed to determine the incidence of venous thromboembolism among hospitalized patients in Qatar as well as to analyze the adequacy of VTE assessment and prophylaxis in hospitalized patients.
Design: Retrospective observational study.
Setting: Four hospitals under Hamad Medical Corporation, Qatar.
Participants: Patients over the age of 18 who were hospitalized between January 2015 and December 2019 and developed venous thromboembolism during hospitalization or within a month after discharge were included.
Results: During the study period, 641,994 individuals were admitted to hospitals. The inclusion criteria were satisfied by 209 of them. The mean age was 51.25 years and 54.5% were males. Hypertension and diabetes mellitus were the most common comorbidities found in the overall group. The incidence of VTE was 32.55 [95% CI 28.4, 37.3] per 100,000 admission per year [0.032%]. The annual incidence was least in 2015 (17.8 per 100,000 admissions) and highest in 2018 (44.4 per 100,000 admissions). Eighty-six subjects had DVT, and 109 had PE, whereas 14 had both. And, 67.5% of the patients developed VTE during admission while, 32.5% developed within 1 month of discharge. Moreover, 22.9% of the patients with PE developed pulmonary embolism after discharge from the hospital. VTE assessment was performed on 64.7% of the patients, and 69.7% received VTE prophylaxis in accordance with guidelines.
Conclusion: Although the occurrence of VTE among hospitalized patients in Qatar is low, healthcare providers need additional education and knowledge of VTE assessment and prophylaxis to follow guidelines for all patients at the time of admission. Furthermore, risk assessment for VTE should be done for all patients at the time of discharge to decide on post-discharge prophylaxis so that incidence of VTE after discharge can be minimized. Future studies should focus on patients who developed VTE after discharge from the hospital as well as on various risk factors.
Keywords: deep vein thrombosis, pulmonary embolism, thromboprophylaxis, venous thromboembolism
Introduction
Venous thromboembolism (VTE), which includes pulmonary embolism (PE) and deep vein thrombosis (DVT), is a serious medical condition, which can complicate other clinical conditions leading to increased morbidity and mortality. In the general population, the incidence of VTE is influenced by ethnicity, gender, and age.1 In the United States, around 300,000 new cases of VTE are detected annually. However, it is estimated that 3 to 4 times as many cases occur without symptoms and go unnoticed.2 According to research from California, the annual incidence of DVT among African Americans, Hispanics, Asians, and Pacific Islanders was 293, 139, and 60 per million population, respectively.3 Published studies on incidence of VTE in Asian countries reported that the population-wide incidence is 15–20% lower than that in Europe. In Korea, Taiwan, and Hong Kong, the annual incidence of VTE was 13.8, 15.9, and 19.9 per 100,000 people, respectively.4 In a study conducted in the Middle East, a higher rate of DVT (15.7%) was noted.5 It is also worth noting that the risk of getting VTE increases with age and the age-adjusted incidence rate of VTE was greater in males.6
VTE occurring in hospitalized patients and following discharge is becoming more common around the world, raising serious concerns among medical fraternity. Hospitalization is the most important risk factor for the development of VTE. The risk of VTE in hospitalized patients is 100 times higher than in the general population.7 The incidence of VTE among hospitalized patients varies greatly between nations and between institutions within a country. A systematic review conducted in Europe reported that the prevalence of VTE in hospitalized patients ranged from 3.65% to 14.9%,8 whereas in Asia, it ranged from 11 to 88 incidences per 10,000 hospitalizations.4 Variations in adherence to local VTE prophylaxis guidelines in hospitalized patients, as well as financial constraints, could explain this vast variability.
The risk of developing VTE among hospitalized patients depends on the primary diagnosis for the hospitalization. Patients undergoing major orthopedic surgery are most at risk for VTE, with 50–60% of patients developing DVT.9,10 The risk of VTE in patients undergoing general surgical procedures ranges from 10% to 50%, depending on the nature of surgery and the presence of risk factors.11 With effective VTE prophylaxis, the risk of VTE in this group of patients can be considerably reduced.12,13
A study from the United States reported that 51% of medically ill patients and 56% of surgical patients were at risk of developing VTE.14 They also found that 31% of the patients discharged from the hospital were at risk for VTE [14.] Similarly, the Epidemiologic International Day for the Evaluation of Patients at Risk for Venous thromboembolism in the Acute Hospital Care Setting study (ENDORSE study) reported that surgical patients have a higher risk of thromboembolism than medical patients.15
VTE events occurring in hospitalized patients are a major cause for morbidity and mortality; however, most of these events are preventable by strict adherence to VTE assessment and prophylaxis practice.16 VTE episodes lengthen hospital stays and raise treatment costs. VTE risk persists even after discharge, with a sizable number of episodes happening after discharge.17
VTE can be fatal, or those who survive it are at risk for recurrences, post-thrombotic phlebitis syndrome, and, in rare instances, persistent thromboembolic pulmonary hypertension, which can be debilitating.18,19 The interval between the hospitalization and the development of VTE varies considerably. Past research on a large cohort of hospitalized medically ill patients have reported that the risk of developing VTE is highest in the first 19 days, peaking around the eighth day. Furthermore, a significantly high percentage (56.6%) of VTE occurred after discharge in their study.20 There is no sufficient data regarding the occurrence of VTE after hospitalization in the State of Qatar. Hence, we decided to carry out a study to estimate the incidence, epidemiological characteristics and clinical outcomes of VTE among hospitalized patients as well as to evaluate the adequacy of VTE assessment and prophylaxis in these patients.
Materials and Methods
Study Design and Setting
A retrospective descriptive study was conducted between September 2019 and August 2021. The participating hospitals include Hamad General Hospital, Alkhor Hospital, Al Wakrah Hospital, and Hazem Mebaireek General Hospital under Hamad Medical Corporation (HMC), Doha, Qatar.
Study Participants
The study comprised adult patients over the age of 18 who were admitted to one of the four participating hospitals between January 1, 2015 and December 31, 2019, and developed VTE (DVT, PE, or both) during their hospital stay or within 30 days of discharge. Patients with VTE at the time of admission were excluded from the study, as were those with missing data. The first episode of VTE was used as the index episode in subjects who had more than one episode of VTE.
Diagnosis of VTE
Diagnosis of deep vein thrombosis was made with Doppler venous ultrasound by a radiologist. Diagnosis of pulmonary embolism was made using computerized scan pulmonary angiogram done by a radiologist or by ventilation perfusion scan.
Data Collection
Using the patients’ healthcare numbers, data were retrieved from the clinical information system. Basic demographics, comorbid conditions, primary diagnosis during hospitalization, previous history, and family history of VTE, history of prothrombotic condition, and details of medication were noted.
Statistical Analysis
The data were described using descriptive statistics. For continuous variables, the mean and standard deviations (SD) were used to summarize the data. Frequencies and percentages were used for categorical variables. Pearson’s chi-squared test or Fisher’s exact test were used to examine the differences between groups. A statistically significant p-value of 0.05 was used. SPSS Statistics version 22 was used to analyze the data (IBM, Armonk, NY).
Results
Incidence of VTE
A total of 1450 files of VTE during the study period were reviewed, of which 223 had VTE during hospitalization or within 30 days of discharge. Among this 14 patients were excluded due to missing data and 209 files were included for the final analysis. There were 641,994 admissions during the study period, making the incidence of VTE as 32.55 [95% CI 28.4, 37.3] per 100,000 admission per year [0.032%]. Eighty-six subjects had DVT, and 109 had PE, whereas 14 had both.
On sub-analysis of incidence of VTE annually, it was found that the incidence rate progressively increased over the years. While in 2015, it was 17.88 per 100,000 hospital admissions rising to 40.08 in 2019. The details of annual incidence rate are depicted in Figure 1.
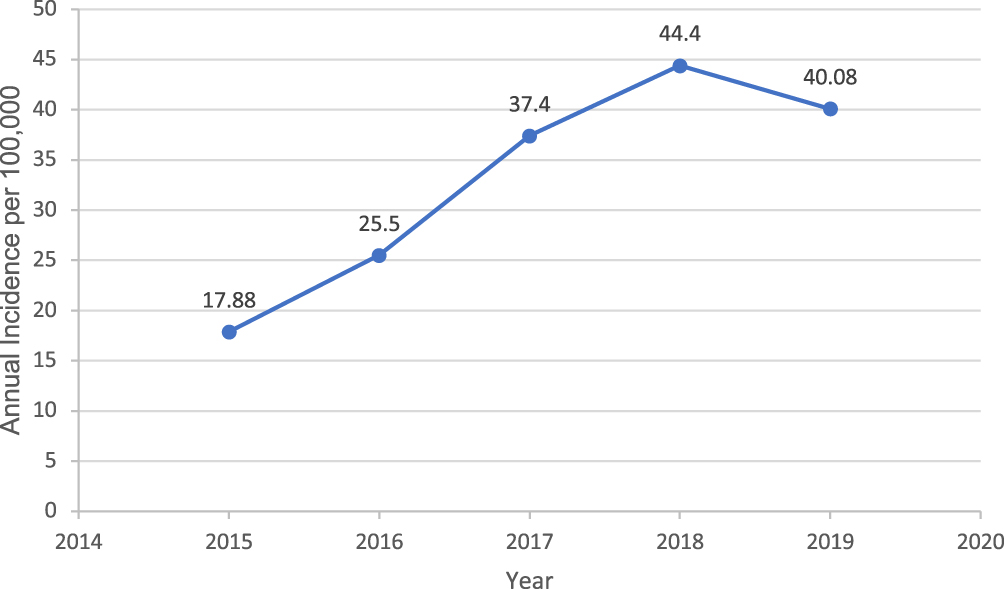 |
Figure 1 Annual incidence of venous thromboembolism among hospitalized patients. |
Basic Demographic Characteristics in the Whole Group
There were 114 males, and the majority were in the 31–45 years age group (mean age, 51.25 ± 18.6 years). A considerable number of the patients had a BMI between 25 and 35 kg/m2 (59.5%). Hypertension (43.4%) and diabetes mellitus (38.3%) were the most common comorbidities observed in the study population. Immobilization and recent surgery were noted in 55.3% and 40.3% of the subjects, respectively. Antiplatelet drugs were used by 21.9% of the participants. Detailed basic demographic characteristics are shown in Table 1 and Table S1.
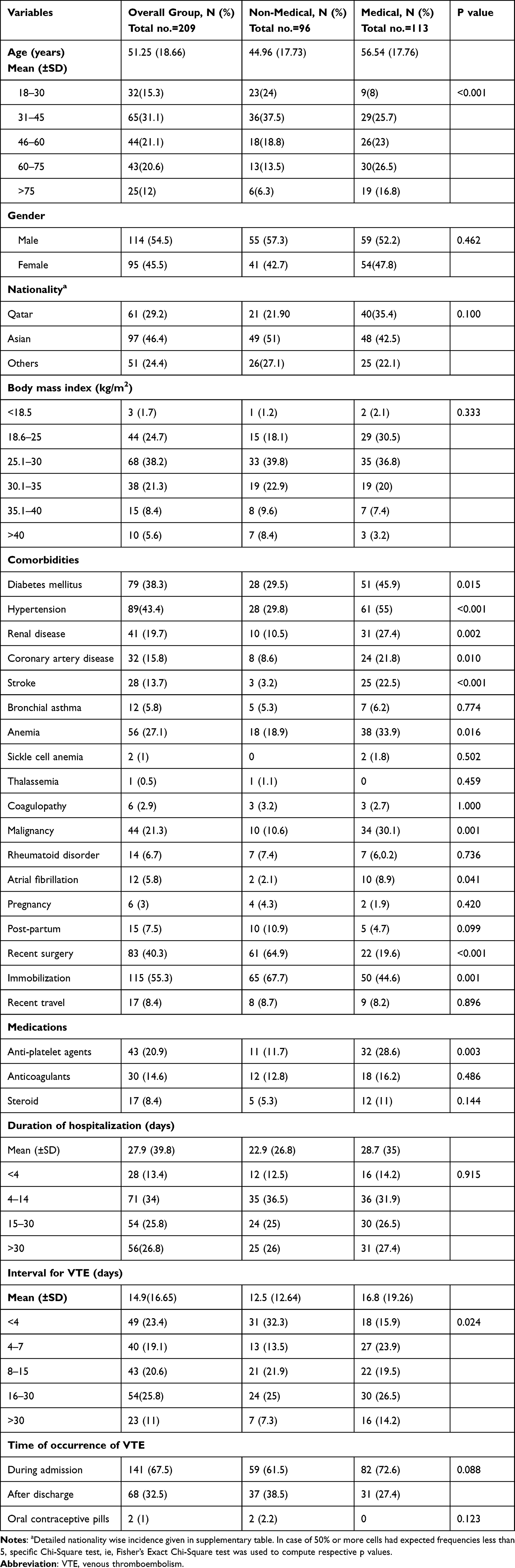 |
Table 1 Basic Characteristics of Whole Cohort and Groups Based on Primary Diagnosis |
On analyzing the duration of hospitalization 34% had 4–14 days of hospital stay, and 26.8% had more than 30 days of hospital stay. On analyzing the interval between hospitalization and development of VTE, it was noted majority developed either between 16 and 30 days (25.8%) or less than 4 days (23.4%). The mean interval to develop DVT was 15.57 days. (SD 15.57). The mean interval to develop PE was 12.97 days (SD 26.79). A sizable number of PE [33 (30.3%)] occurred in less than 4 days. And, 67.5% developed VTE during hospitalization, whereas 32.5% developed within 30 days after discharge (p = 0.008) (Table 1).
Basic Characteristics Based on the Primary Diagnosis
We classified the study subjects into two groups for analysis purposes, based on whether the underlying main diagnosis for admission was medical or non-medical. The mean age of subjects in the medical group (56.54 years ±17.76) was higher than that in the non-medical group (44.96 years ±17.73). Majority of subjects in the non-medical groups were between 31 and 45 years (37.5%), whereas most subjects in the medical groups were between 60 and 75 years (26.5%) followed by 31–45 years age group (25.7%). There was no significant difference in the gender distribution between the two groups.
A higher number of subjects had a BMI of 25.1–30 kg/m2 in both the groups (39.8% in non-medical vs 36.8% in the medical group). Hypertension, diabetes mellitus, and anemia were the most common Comorbid conditions observed in both groups. Coagulopathy was noted only in 3.2% and 2.7% of the non-medical and medical groups, respectively. Cerebrovascular accidents (22.5% vs 3.2%), coronary artery heart diseases (22.5% vs 8.6%), and malignancy (30.1% vs 10.6%) were significantly higher among medical group. Four subjects in the non-medical and two in the medical group were pregnant. As expected, higher number of subjects (64.9%) in the non-medical group had recent surgery compared to 19.6% in the medical group. The immobilization was significantly higher in the non-medical group (67.7% vs 44.6%, p = 0.001).
Most of the patients were hospitalized for 4–14 days in both groups (36.5% in non-medical vs.31.9% in medical). In the medical group, majority developed VTE between 16 and 30 days (26.5%) after hospitalization followed by between 4 and 7 days (23.9%), whereas a higher number of patients developed VTE within 4 days of hospitalization in the non-medical group (32.3% vs 15.9%) followed by 16–30 days (25%), and, 61.5% of the patients in the non-medical and 72.6% in the medical group developed VTE during admission (Table 1).
Basic Characteristics Based on the Type of VTE
There was no significant difference in the mean age of patients between DVT and PE groups (53.17±20.45 Vs 51.05±17.31). DVT was more common in females (57% vs 43%), whereas PE was more common among males (64.2% vs 35.8%). Considerable number of patients in both the groups was admitted for medical reasons in the hospital (52.3% in DVT vs 41.3%in PE). And, 28.4% of the patients in the PE group were admitted for orthopedic/trauma causes.
The mean interval for development of DVT was 15.57 days (±13.78) and for PE was 12.97 days (±15.38). Most of the patients developed DVT between 16 and 30 days of hospitalizations (32.6%) followed by 4–7 days (24.4%), whereas majority developed PE in less than 4 days of hospitalizations (30.3) followed by 8–15 days (23.9%). Higher number of patients developed DVT (59.3% vs 40.7%) as well as PE (77.1% vs 22.9%) during admission, when compared to post discharge events (Table 2).
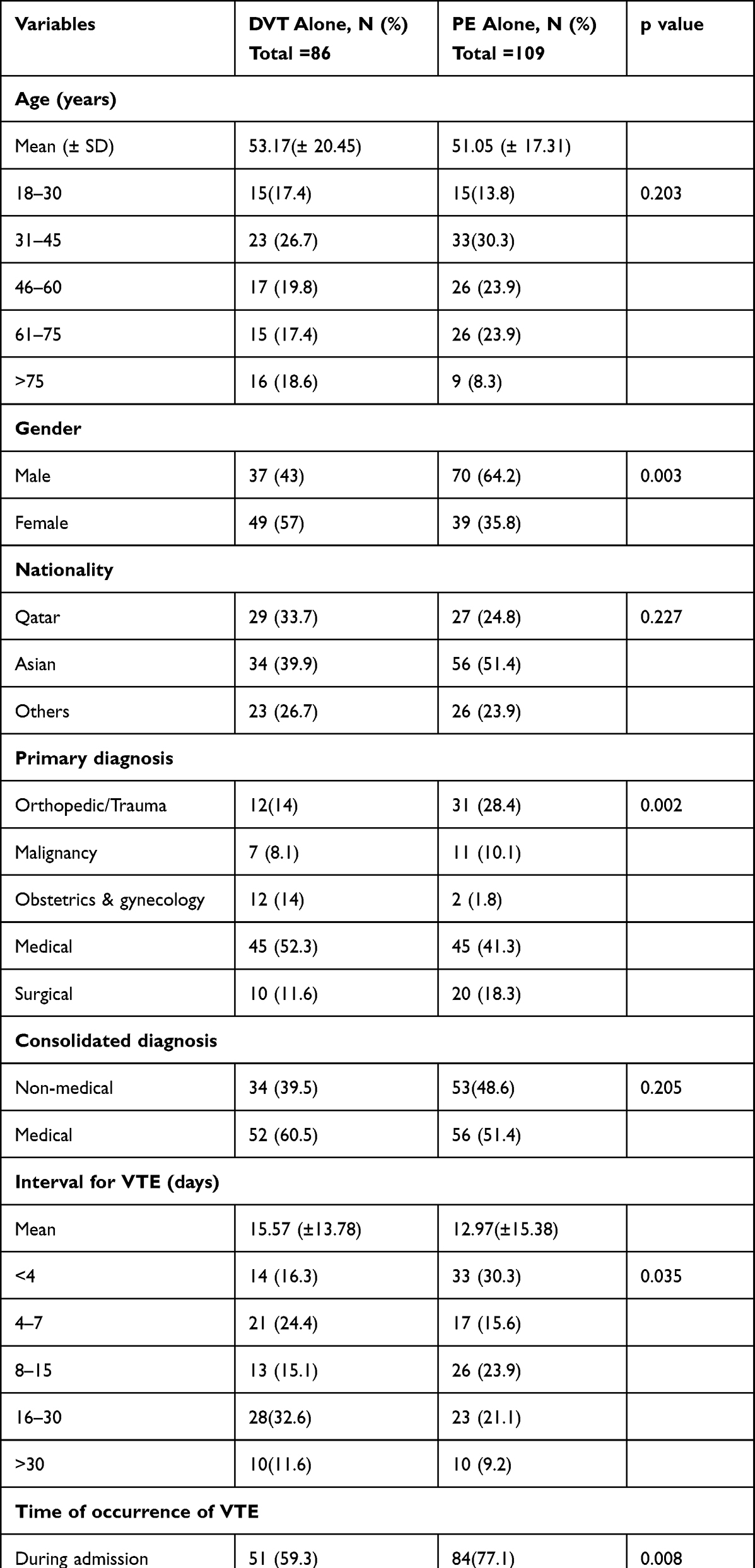 |
Table 2 Basic Characteristics of Patients Based on Type of Venous Thromboembolism |
On analyzing the underlying comorbidities, hypertension was the most common comorbid condition in the DVT and PE groups (49.4%,39.6%) followed by diabetes mellitus (39.3%, 38.5%), respectively. Anemia was found in 35.5% of the patients with DVT while 22.9 patients in the PE group had the same. Higher number of patients in the PE group had recent surgery (49.5% vs 24.7%) (Figure 2). However, there was no statistically significant difference in the comorbidities between the two groups.
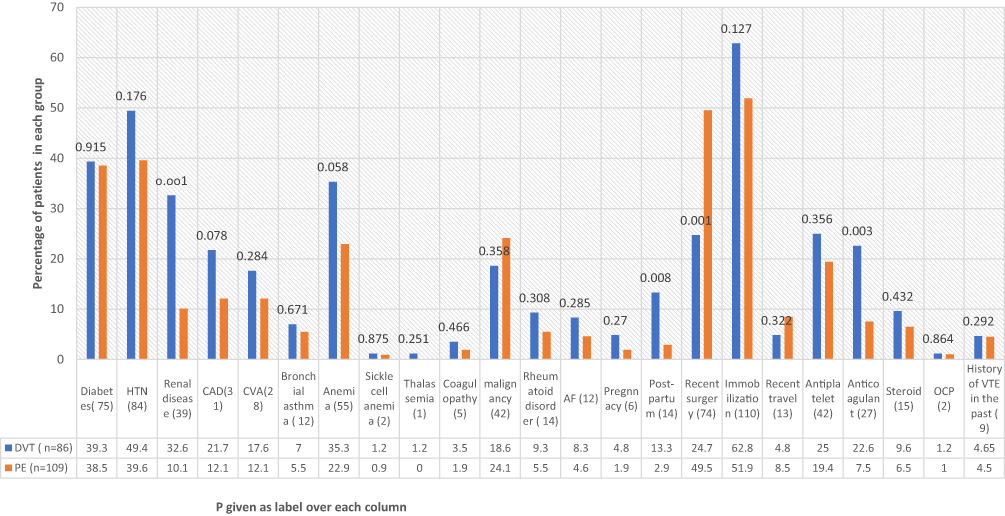 |
Figure 2 Details of comorbidities in DVT and PE groups. |
Compliance with VTE Prophylaxis
In the whole study group, 97 subjects (64.7%) had VTE assessment done during admission. Fifty-six patients had no data about VTE assessment. There was no significant difference in the rate of VTE assessment in the medical (67.9% vs 60.9%, p = 0.369) and the non-medical group. In the overall study group, 69.7% received VTE prophylaxis, whereas 70.2% and 69.1% of the patients received VTE prophylaxis (p = 0.877) in the medical and the non-medical group, respectively.
Among the anticoagulants, enoxaparin was the most prescribed pharmacological agents for prophylaxis. Forty patients (31%) received mechanical prophylaxis (Table 3).
 |
Table 3 Details of VTE Assessment, Prophylaxis and Final Disposition Based on Primary Diagnosis |
Type and Site of VTE
The majority of DVTs occurred in the lower limbs (96.5%). Only three subjects experienced DVT in their upper limbs. In 94.2% of the patients, DVT was unilateral. PE was found to be bilateral in 49.5% of the cases, with the majority being segmental or sub-segmental (53.8%) (Figure 3).
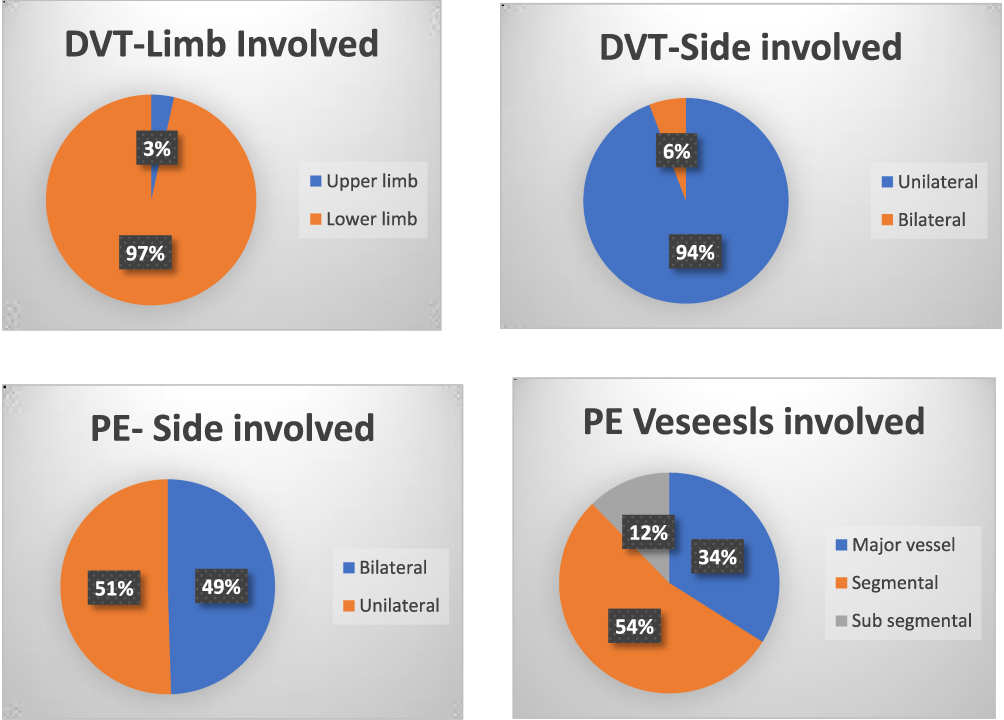 |
Figure 3 Details of the affected site and location of DVT/PE. |
Final Disposition
In the overall cohort 29 patients (13.9%) died, majority from the medical group (27 vs 2).
Discussion
The incidence of VTE during hospitalization or within 1 month after discharge was exceptionally low in our research (0.032%). Reports from the United States showed a higher incidence of VTE in hospitalized patients than in our study. A US study of healthcare claims data reported that 1.59% of medically ill hospitalized patients developed VTE within 90 days.21 Their study differed from the current one in that it only included individuals over the age of 40 and excluded patients with trauma, labor, and delivery.21
Variable rates of VTE among hospitalized patients have been reported in studies conducted in European countries. According to one study, the incidence of postoperative DVT in Europe in 2020 ranged from 0.01% in Portugal to 0.21% in the United Kingdom. The reported incidence of postoperative DVT in France was 1.3%, while it was 0.80% in Australia.22
The incidence of VTE in hospitalized patients differed among Asian nations. A systematic review of nine studies utilizing Asian hospital registries or databases found that the incidence of VTE in admitted patients ranged from 0.11% to 0.88%.4 The variation in VTE rates could be attributed to several factors, including differences in adherence to recommended guidelines and prophylaxis, under diagnosis and underreporting, differences in patient safety monitoring systems,22 and lower thrombophilia in Asian countries compared to Western countries.23 The low incidence of VTE in our study population might be attributable to a variety of factors. First, VTE assessment and prevention is performed routinely at the time of admission for all patients in HMC hospitals and is considered as a key performance indicator of patient care. Second, the majority of Qatar’s population is made up of young, healthy expats of multiethnic origin, which also might have contributed to the low incidence
Nearly two-thirds of patients in our research group had VTE assessment during hospitalization, and more than two-thirds received VTE prophylaxis. This observation on VTE assessment and prevention is based on review of only individuals who had VTE after hospitalization and cannot be generalized to all hospital admissions in Qatar. Furthermore, the missing data on VTE assessment and prophylaxis might have underestimated the compliance rate in our study.
We did not notice any significant difference in VTE assessment and prophylaxis between medical and non-medical group of patients. According to studies from neighboring Middle Eastern nations, the spectrum of VTE prevention in hospitals varies. One study from Saudi Arabia reported that 60.5% of their study subjects received some form of VTE prophylaxis, although only 38.4% received ACCP recommended VTE prophylaxis.24 Another research from seven hospitals in Saudi Arabia found a similar percentage (40.9%) of VTE prophylaxis.25
A sub-analysis of the ENDORSE study from the three Arabian Gulf nations, namely Kuwait, Saudi Arabia, and the United Arab Emirates, revealed that 40.2% of their study populations received prophylaxis in accordance with ACCP guidelines.26 The ENDORSE research, a worldwide cross-sectional study, found that surgical patients had a higher rate of VTE prophylaxis than medical patients (58.5% vs 39.5%).15 The IMPROVE study, which is a multinational ongoing observational study, found 60% of the eligible patients receiving VTE prophylaxis as per ACCP guidelines27 whereas in contrast, the CURVE study from Canada reported that only 16% of their eligible patients received appropriate VTE prophylaxis.28
Even though the majority of VTE incidents in our study subjects occurred during hospitalization, a sizable proportion (32.5%) developed VTE within 1 month after discharge. And, 22.9% of patients with PE in the current study developed pulmonary embolism after discharge from the hospital. This has a clinical significance as PE carries high mortality and morbidity. To reduce the risk of VTE incidents during hospital stay and after discharge, the risk assessment must be a dynamic one and needs to be done periodically. Furthermore, during the discharge process, the treating physician should always take into consideration the patient’s post-discharge risk status for VTE and decide regarding the need for continuing the thromboprophylaxis. Post-discharge incidence of VTE ranged from 18% to 56.6%, according to published statistics.20,21 All high-risk patients should be educated regarding continuing preventive measures at home and to report back to hospital at the earliest in case of any clinical symptoms suggestive of DVT or PE. There is a need for further studies analyzing the subgroup of patients who developed VTE after discharge.
When the interval between admission and the development of VTE is examined, it is found that the majority of events occurred between days 16 and 30 (25.8%) of hospitalization. Nonetheless, it is worth noting that a considerable VTE (23.4%) occurred in less than 4 days of hospitalization. When these figures are examined further, it was discovered that more PE (30.3%) occurred in fewer than 4 days than DVT (16.3%). However, the bulk of DVT (32.6%) incidents occurred 16 days following hospitalization. This demonstrates that PE risk begins soon after admission, underlining the significance of doing an early VTE assessment and initiating prophylaxis at the earliest.
Despite the scientific evidence supporting the benefit of prophylaxis and various guidelines recommending the routine VTE assessment and prophylaxis in real clinical practice, the implementation of the same is low all over the globe.8
The mortality rate in our study was 13.39%. Most of our patients had multiple comorbid conditions or poly-trauma or surgery, which may have contributed or been the primary cause of death, rather than VTE perse. This might have resulted in an overestimation of the death rate. Two distinct studies from Saudi Arabia reported a mortality rate of 14.3%25 and 20.8%,29 respectively, whereas a report from the United Kingdom indicated that in-hospital VTE episodes had a fatality rate of 12%.30 Studies have shown that in most cases the mortality in VTE is linked to underlying comorbid conditions. A study by Carson et al reported that 2.5% of the pulmonary embolism fatalities were caused by the PE itself, with the rest being caused by underlying conditions.31
Limitations
The current study had few limitations. First, for calculating the incidence of VTE, we included all patients admitted to the hospital irrespective of the duration of thospital stay. This might have underestimated the incidence of VTE in our study population. Second, we did not investigate the association between the risk factors and the occurrence of VTE. We wish to emphasize that risk factor stratification was not the major focus of the study. Finally, we did not compare the characteristics of patients who developed VTE in the hospital with those who developed VTE after they were discharged.
Conclusion
In Qatar, the rate of VTE among hospitalized patients was significantly low. Practitioners’ compliance with VTE assessment and adherence to the prophylaxis guidelines is modest. Clinicians should prioritize VTE prophylaxis not just during hospitalization but also at the time of discharge, especially in high-risk patients. More research is needed to investigate the association between VTE and various risk factors, as well as to compare patients who developed VTE during hospital stay to those who developed after discharge. In future studies, we suggest excluding patients who were hospitalized for less than 48 hours while calculating the incidence of VTE.
Ethical Approval
The study was approved by the Institutional Review Board of medical research center, Hamad Medical Corporation, PO Box 3050, Doha, Qatar (Approval number -MRC-01-20-005). The consent was waived due to the retrospective nature of the review. The confidentiality of the included subjects was maintained by not disclosing the identification details and using anonymized data. The study was conducted in full compliance with the principles of “Declaration of Helsinki” Good Clinical Practice (GCP).
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Liao S, Woulfe T, Hyder S, Merriman E, Simpson D, Chunilal S. Incidence of venous thromboembolism in different ethnic groups: a regional direct comparison study. J Thromb Haemost. 2014;12(2):214–219. doi:10.1111/jth.12464
2. Goldhaber SZ, Fanikos J. Cardiology patient pages. Prevention of deep vein thrombosis and pulmonary embolism. Circulation. 2004;110(16):e445–e447. doi:10.1161/01.CIR.0000145141.70264.C5
3. White RH, Zhou H, Romano PS. Incidence of idiopathic deep venous thrombosis and secondary thromboembolism among ethnic groups in California. Ann Intern Med. 1998;128(9):737–740. doi:10.7326/0003-4819-128-9-199805010-00006
4. Lee LH, Gallus A, Jindal R, Wang C, Wu CC. Incidence of venous thromboembolism in Asian populations: a systematic review. Thromb Haemost. 2017;117(12):2243–2260. doi:10.1160/TH17-02-0134
5. Elkhadir A. Prevalence of deep venous thrombosis (DVT) in Jeddah. Int J Med Sci Clin Invent. 2018. doi:10.18535/ijmsci/v5i10.03
6. Silverstein MD, Heit JA, Mohr DN, Petterson TM, O’Fallon WM, Melton LJ. Trends in the incidence of deep vein thrombosis and pulmonary embolism: a 25-year population-based study. Arch Intern Med. 1998;158(6):585–593. doi:10.1001/archinte.158.6.585
7. Heit JA, Melton LJ, Lohse CM, et al. Incidence of venous thromboembolism in hospitalized patient’s vs community residents. Mayo Clin Proc. 2001;76(11):1102–1110. doi:10.4065/76.11.1102
8. Khoury H, Welner S, Kubin M, Folkerts K, Haas S. Disease burden and unmet needs for prevention of venous thromboembolism in medically ill patients in Europe show underutilisation of preventive therapies. Thromb Haemost. 2011;106(4):600–608. doi:10.1160/TH11-03-0168
9. White RH, Henderson MC. Risk factors for venous thromboembolism after total Hip and knee replacement surgery. Curr Opin Pulm Med. 2002;8(5):365–371. doi:10.1097/00063198-200209000-00004
10. Bui MH, Hung DD, Vinh PQ, Hiep NH, Anh LL, Dinh TC. Frequency and risk factor of lower-limb deep vein thrombosis after major orthopedic surgery in Vietnamese patients. Open Access Maced J Med Sci. 2019;7(24):4250–4254. doi:10.3889/oamjms.2019.369
11. Samama MM. Applying risk assessment models in general surgery: effective risk stratification. Blood Coagul Fibrinolysis. 1999;10(Suppl 2):S79–S84.
12. Collins R, Scrimgeour A, Yusuf S, Peto R. Reduction in fatal pulmonary embolism and venous thrombosis by perioperative administration of subcutaneous heparin. Overview of results of randomized trials in general, orthopedic, and urologic surgery. N Engl J Med. 1988;318(18):1162–1173. doi:10.1056/NEJM198805053181805
13. Agnelli G. Prevention of venous thromboembolism in surgical patients. Circulation. 2004;110(24Suppl 1):IV4–IV12. doi:10.1161/01.CIR.0000150639.98514.6c
14. Anderson FA Jr, Zayaruzny M, Heit JA, Fidan D, Cohen AT. Estimated annual numbers of US acute-care hospital patients at risk for venous thromboembolism. Am J Hematol. 2007;82(9):777–782. doi:10.1002/ajh.20983
15. Cohen AT, Tapson VF, Bergmann JF, et al. Venous thromboembolism risk and prophylaxis in the acute hospital care setting (ENDORSE study): a multinational cross-sectional study. Lancet. 2008;371(9610):387–394. doi:10.1016/S0140-6736(08)60202-0
16. Steering IST. Committee for World Thrombosis Day. Thrombosis: a major contributor to the global disease burden. J Thromb Haemost. 2014;12(10):1580–1590. doi:10.1111/jth.12698
17. Kaatz S, Spyropoulos AC. Venous thromboembolism prophylaxis after hospital discharge: transition to preventive care. Hosp Pract. 2011;39(3):7–15. doi:10.3810/hp.2011.08.574
18. Braekkan SK, Grosse SD, Okoroh EM, et al. Venous thromboembolism and subsequent permanent work-related disability. J Thromb Haemost. 2016;14(10):1978–1987. doi:10.1111/jth.13411
19. Kahn SR. The post-thrombotic syndrome. Hematology Am Soc Hematol Educ Program. 2016;2016(1):413–418. doi:10.1182/asheducation-2016.1.413
20. Amin AN, Varker H, Princic N, Lin J, Thompson S, Johnston S. Duration of venous thromboembolism risk across a continuum in medically ill hospitalized patients. J Hosp Med. 2012;7(3):231–238. doi:10.1002/jhm.1002
21. Edelsberg J, Hagiwara M, Taneja C, Oster G. Risk of venous thromboembolism among hospitalized medically ill patients. Am J Health Syst Pharm. 2006;63(20 Suppl 6):S16–S22. doi:10.2146/ajhp060389
22. Nuffield Trust. How does the UK’s post-operative deep vein thrombosis rate compare internationally over time?; 2021. Available from: https://www.nuffieldtrust.org.uk/chart/how-does-The-uk-s-post-operative-deep-vein-thrombosis-rate-compare-internationally-over-time-3.
23. Wang KL, Yap ES, Goto S, Zhang S, Siu CW, Chiang CE. The diagnosis and treatment of venous thromboembolism in Asian patients. Thromb J. 2018;16:4. doi:10.1186/s12959-017-0155-z
24. Kharaba A, Al Aboud M, Kharabah MR, Alyami K, Al Beihany A. Venous thromboembolism risks and prophylaxis in King Fahad Hospital, Madinah, Saudi Arabia. J Epidemiol Glob Health. 2017;7(4):295–298. doi:10.1016/j.jegh.2017.09.003
25. Al-Hameed FM, Al-Dorzi HM, Qadhi AI, et al. Thromboprophylaxis and mortality among patients who developed venous thromboembolism in seven major hospitals in Saudi Arabia. Ann Thorac Med. 2017;12(4):282–289. doi:10.4103/atm.ATM_101_17
26. Alsayegh F, Kamaliddin H, Sheshah E, Bukhamseen N, Alkhuwaitir T, Elhoufi A. Assessment of venous thromboembolism risk and adequacy of prophylaxis in selected acute care medical centres in Arabian Gulf States: results from the ENDORSE study. Med Princ Pract. 2012;21(6):522–528. doi:10.1159/000339081
27. Tapson VF, Decousus H, Pini M, et al. Venous thromboembolism prophylaxis in acutely ill hospitalized medical patients: findings from the international medical prevention registry on venous thromboembolism. Chest. 2007;132(3):936–945. doi:10.1378/chest.06-2993
28. Kahn SR, Panju A, Geerts W, et al. Multicenter evaluation of the use of venous thromboembolism prophylaxis in acutely ill medical patients in Canada. Thromb Res. 2007;119(2):145–155. doi:10.1016/j.thromres.2006.01.011
29. Essam AE, Sharif G, Al-Hameed F. Venous thromboembolism-related mortality and morbidity in King Fahd General Hospital, Jeddah, Kingdom of Saudi Arabia. Ann Thorac Med. 2011;6(4):193–198. doi:10.4103/1817-1737.84772
30. Anderson FA Jr, Wheeler HB, Goldberg RJ, et al. A population-based perspective of the hospital incidence and case-fatality rates of deep vein thrombosis and pulmonary embolism. The Worcester DVT Study. Arch Intern Med. 1991;151(5):933–938. doi:10.1001/archinte.1991.00400050081016
31. Carson JL, Kelley MA, Duff A, et al. The clinical course of pulmonary embolism. N Engl J Med. 1992;326(19):1240–1245. doi:10.1056/NEJM199205073261902
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.