")
Back to Journals » Open Access Surgery » Volume 12
Varicose vein invasive intervention at university hospital of Nepal, our experience in the last six years
Authors Karmacharya RM, Shrestha BK, Shrestha B, Singh AK, Bhandari N , Dhakal P , Dahal S
Received 8 May 2019
Accepted for publication 26 August 2019
Published 10 September 2019 Volume 2019:12 Pages 21—25
DOI https://doi.org/10.2147/OAS.S214962
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Luigi Bonavina
RM Karmacharya, BK Shrestha, B Shrestha, AK Singh, N Bhandari, P Dhakal, S Dahal
Department of Surgery, Dhulikhel Hospital, Kathmandu University Hospital, Dhulikhel, Kavre, Nepal
Correspondence: RM Karmacharya
Department of Surgery (Cardio Thoracic and Vascular), Dhulikhel Hospital, Kathmandu University Hospital, Dhulikhel Hospital Road, PO Box no 45210, Dhulikhel, Kavrepalanchok, Nepal
Tel +977 981 872 9013
Email [email protected]
Introduction: Varicose vein is a common venous condition affecting quality of life presenting as an asymptomatic condition to a feeling of heaviness, pain, pigmentation, palpable superficial veins, itchiness and ulceration. Proper management of varicose vein is of huge importance due to its high prevalence and the impact it has on patients’ quality of life, productivity as well as on health-care resource burden. Various conservative and invasive interventions are available for the management of varicose veins. Here we present our experience with the invasive intervention of varicose veins during a period of six years at a tertiary care center (Dhulikhel Hospital) in Nepal. Although Radio Frequency Ablation (RFA) is recently introduced in Nepal, it has shown promising outcome.
Method: This is a retrospective descriptive cross-sectional study between the years 2013 and 2018 at the Dhulikhel Hospital among patients that underwent surgical management of varicose veins. For ease in interpretation, patients who underwent surgery for both lower limbs in the same setting are considered as separate cases.
Results: In a total of 533 limbs, the most common vein involved was isolated great saphenous vein in 70.4%. In terms of side affected, 157 patients (33.8%) were affected on the right side, 238 (51.3%) were affected on the left side and 69 (14.9%) patients had bilateral involvement. The most common clinical feature was prominent vein present in 94.5% limbs. This was followed by pain in 55.7%, pigmentation in 25.3%, itchiness in 14.6% and ulceration in 13.1%. Mean hospital stay was 1.1 days (S.D. 0.64, Range 0–3). In terms of complication, one case with deep vein thrombosis (0.18%) developed in the seventh postoperative period. There was skin burn in two cases (0.53% of RFA cases) and in 11 cases (2.06%) there was painful superficial thrombosed veins of which three required excision under local anesthesia (0.56%).
Conclusion: There are multiple invasive interventions for varicose veins. With the availability of the facilities, RFA is the procedure of choice in feasible cases. The most common complication after surgical treatment was painful thrombosed superficial veins. DVT was a rare complication.
Keywords: varicose veins, varicose vein surgery, radiofrequency ablation
Introduction
Varicose vein is a fairly common venous condition affecting quality of life and has various treatment modalities at the current time.1,2 Presentation of varicose veins, though usually asymptomatic, can range from a feeling of heaviness, pain, pigmentation, palpable superficial veins, itchiness to ulceration.2,3 They occur in a quarter of the adult population.1 There has been a rise in the quantity of treatment modalities, with advances seen more in operative measures than in conservative therapies.4,5 The treatment of varicose veins includes lifestyle modification, physiotherapy, compression stockings, sclerotherapy, open surgery, and minimal invasive endovenous surgery.6
Studies on a large number of varicose vein cases and their operative management have shown that this disease is predominant in the male population, with the left side affected more than the right side, with 90% involvement of the great saphenous vein (GSV).7,8 The studies have mentioned different surgical treatment modalities from conventional open surgery to minimally invasive radiofrequency ablation.
Proper management of varicose vein is important due to the high prevalence and impact on patients’ quality of life, productivity and health-care resource burden.1,6 The health-care system in Nepal is divided into primary, secondary, and tertiary in the public sector.9 However, there are private and community centers providing healthcare to people in conjunction with the public health facilities provided by the government. There is a lack of publications relating to varicose veins with a large patient population in Nepal. Here we present our experience in the management of varicose veins during the period of six years at a tertiary care center, Dhulikhel Hospital which is a community-based hospital in Nepal. As newer treatment modalities of varicose veins have just been introduced in Nepal, this article serves as an important stepping stone for further progress in this field.
Methodology
This is a retrospective descriptive cross-sectional study including all patients subjected to invasive intervention of varicose veins at Dhulikhel hospital from January 2013 to December 2018. Cases treated with sclerotherapy alone were not included in the study. Ethical approval was taken from the Institutional Review Committee of Kathmandu University School of Medical Sciences. Patient consent to review their medical records was also obtained.
Radiofrequency ablation (RFA) was done in all cases involving great saphenous vein (characterized by diameter of GSV more than 5 mm, superficial dilated and tortuous veins commonly in the anteromedial aspect of thigh and calf, reflux in the saphenofemoral junction (SFJ) and dilated SFJ) unless there were contraindications for RFA.10 For RFA, we used VNUS closure fast RF generator with 60 cm or 100 cm long RF catheter. The distance between the RFA catheter tip and SFJ should be at least 2 cm, and 10 cc of normal saline were injected between GSV and skin for ultrasound guidance. About 10 cc/cm normal saline was injected between the treated vessel segment and skin. For ultrasound, Siemens Acuson P300 machine (Munich, Germany) was used with a linear probe at 7.5 MHz to 12 MHz with appropriate gain and zoom. For patients who were subjected to surgery before the availability of RFA facilities (August 2014), we did SFJ flush ligation, ligation of tributaries, and segmental perforation and invagination (PIN) stripping. After RFA, we examined the residual varicose veins by intraoperative doppler ultrasonography to note the presence of dilated veins, distal insufficiency points, and dilated perforators. We performed the necessary phlebectomy and perforator ligation when indicated. For varicose veins involving short saphenous vein (SSV) characterized typically by varicose veins in the posterolateral part of the thigh draining into saphenopopliteal junction (SPJ), we did SPJ ligation with necessary phlebectomy and perforator ligation. For varicose veins involving more than one system and involving two limbs, we mixed surgical procedures as per the necessity. Also, in patients in whom surgery was performed for bilateral lower limbs in the same setting, they were taken as separate cases, and complications as well as other parameters specific to each limb are seen separately for ease in interpretation. All the cases were done under spinal anesthesia, except in cases where spinal anesthesia could not be given, where general anesthesia was given. Immediately following the procedure, a compression bandage was applied over the limb. After discharge, the first follow-up is done on the 3rd to 4th day, after which the second follow up is done on the 10th to 12th day for taking out the suture. The compression bandage is used till the 12th day, after which a compression stocking is advised for the next 18 days (total of 1 month of compression).
We managed the database in Microsoft Excel (version 2013, Microsoft Corporation, Redmond, WA, USA) and analyzed them in SPSS 13.0 (SPSS Inc., Chicago, IL, USA). Scalar variables were expressed in mean, standard deviation and range. Nominal variables were expressed in percentage.
Results
There was a total of 464 patients who underwent the procedure. Of these, 157 patients (33.8%) were affected on the right side, 238 (51.3%) were affected on the left side and 69 (14.9%) patients had bilateral involvement. The procedure was done on 533 limbs for varicose veins of which 317 (59.5%) were male and 216 (40.5%) were female. In 521 limbs (97.7%) the procedure was done under spinal anesthesia while in 12 limbs (2.3%) the procedure was done under general anesthesia as there was a contraindication of spinal anesthesia. Eighty-nine percent had a history of prolonged standing (more than six hours of standing per day, at least six days a week). Regarding duration in months, mean duration was 25.6 months (SD 60.6 months, Range 1 month to 360 months).
Table 1 shows the percentage of patients with different clinical features. The most common clinical feature was prominent vein present in 94.5% limbs. This was followed by pain in 55.7%, pigmentation in 25.3%, itchiness in 14.6% and ulceration in 13.1%.
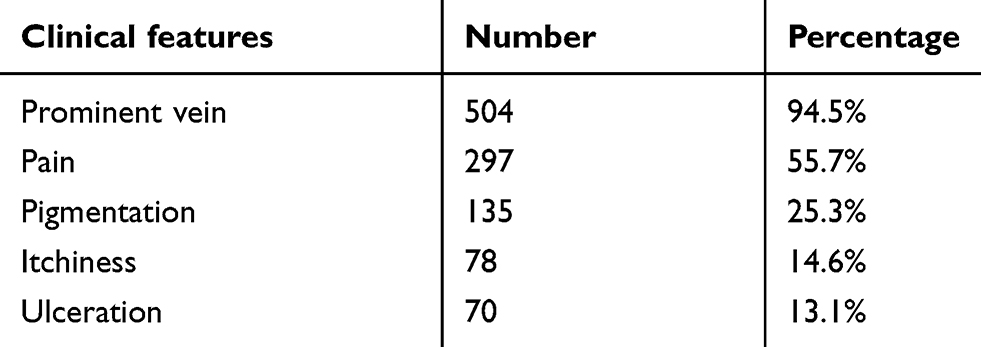 |
Table 1 Clinical features |
In terms of clinical classification (C stage) there were 15.3% patients in C2, 34.5% in C3, 37.1% in C4, 6.0% in C5 and 7.1% in C6 stage as mentioned in Table 2.
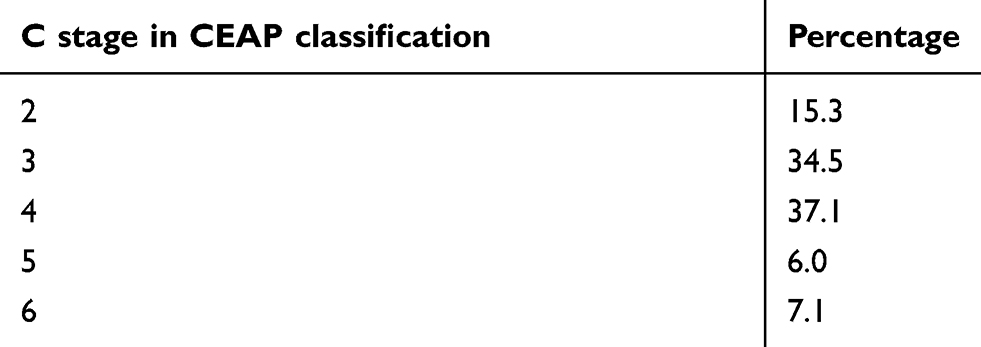 |
Table 2 C stage in CEAP classification |
Table 3 shows the total number and percentage of limbs with different veins involved. The most common vein involved was isolated great saphenous vein (GSV) in 70.4%. This was followed by the involvement of short saphenous vein (SSV) in 21.9%, involvement of both GSV and SSV in 6.9%, isolated intersaphenous vein in 0.4% and isolated perforator in 0.4%.
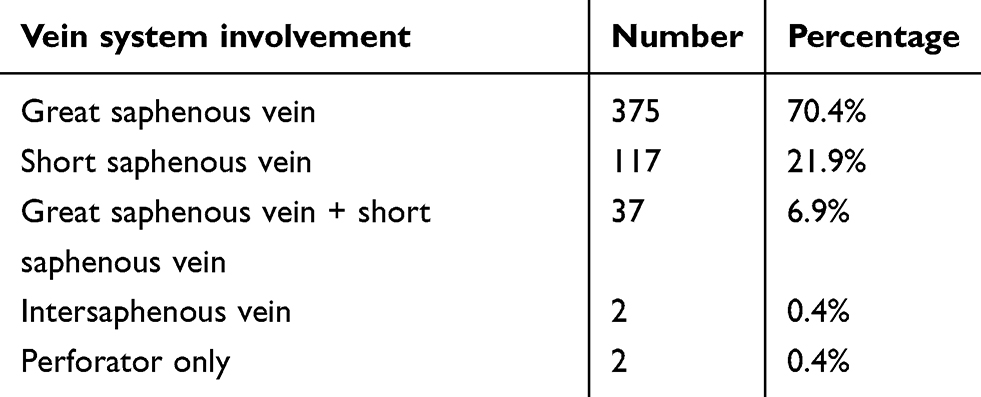 |
Table 3 Vein system |
Details of the procedure done are explained in Table 4. Conventional open surgery was done in 35 (6.6%) limbs before the availability of RFA facility. In 117 limbs (22%) SPJ ligation was done. In 340 limbs (63.8%) RFA with or without phlebectomy was done. In 37 cases (6.9%) RFA with SPJ ligation was done.
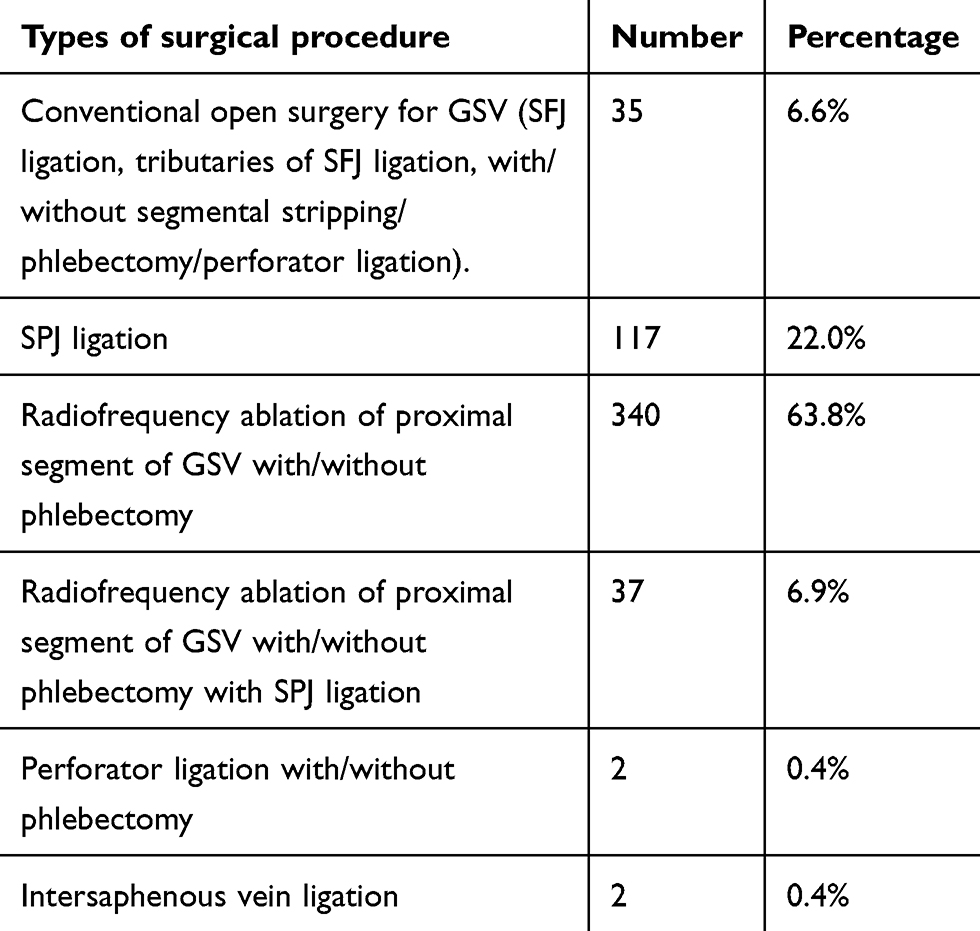 |
Table 4 Types of surgical procedure |
Mean hospital stay was 1.1 days (S.D. 0.64, range 0–3). In terms of complication, a case with deep vein thrombosis (0.18%) developed in the seventh postoperative period was detected during follow up and was managed by anticoagulation. Of the cases where RFA was performed, there was skin burn in two cases (0.53%), which was detected during follow up. In 11 cases there was painful superficial thrombosed veins (2.06%), of which three required excision under local anesthesia (0.56%). Regarding the case with DVT, the patient did not have swelling at the time of discharge but on first follow up on 7th postoperative day she presented with left leg swelling and pain while walking. During Doppler ultrasonography there were features of DVT in the femoral vein and this was managed with anticoagulation.
Discussion
Prominent veins, pain, pigmentation, itchiness, and ulceration are common presenting features of varicose vein in our study. This is similar to a population-based study in Malaysia done in patients with prominent veins; the most common symptom was pain present in 80% of cases.11
For classification of varicose veins, CEAP classification is commonly used of which Clinical (C Stage) is more useful.12 In our study, there were 13.1% of patients in stage 5 or more (presence of ulceration).
Conventional open surgery and radiofrequency ablation of GSV are common options for surgical management of GSV varicose veins and this can be done in adjunct with phlebectomy, perforator ligation, or sclerotherapy as per the need.12 For varicose veins of SSV, SPJ ligation with/without phlebectomy, perforator ligation, and sclerotherapy are surgical treatment modalities.12 After the start of RFA in Dhulikhel Hospital from August 2013, this surgical modality was done in all the possible cases.
In a study done in the western part of Nepal on the surgical outcome of varicose veins, varicose vein was predominantly seen in males (70.37% vs 29.63% in females).13 The highest proportion of patients had SFJ flush ligation, segmental stripping of GSV and necessary phlebectomies.13 In our earlier series of studies, open surgery was done before radiofrequency ablation of varicose veins was available in Nepal; 88.2% involved GSV while 21.8% involved SSV.14 Hospital admission was required for more days in the patient group where stripping (segmental) was done, compared to the patient group where stripping was not required (3.0 days vs 2.28 days, p<0.01).14 In our study comparing conventional open surgery and initial series of RFA cases, RFA was associated with significant advantage in terms of less hospital admission, less pain, earlier return to work, earlier ability to walk normally (ability to walk >20 m on level ground unassisted) and had lower presence of significant bruise (bruise >5×5 cm).15
In 10 years’ experience of varicose vein surgery at Nigeria consisting of 45 patients, 67% were male patients while 33% were female patients.16 The left to right ratio of the affected limb was 5:2.16 The great saphenous vein involvement was three times that of the short saphenous vein.16 Male predominance and more prevalence in the left leg were also noted in our series. Some known reasons for higher occurrence in left leg are longer iliac veins in the left side compared to the right side, right iliac artery crossing left iliac vein, which may cause compression, and increased tortuosity of left iliac veins.17,18 Similar other studies have mentioned left side involvement from 53.8% to 65%.11
In terms of complication rates, deep vein thrombosis (DVT) is one of the complications of varicose vein surgery. Although the incidence of DVT after conventional surgery was found to be 5.3%, and that after endovenous surgery was around 1%, the occurrence of DVT in our series was only 0.18%.19,20 In a study done in Italy on outcomes after RFA for varicose veins, the incidence of DVT was noted to be 0.9%.21 Recommendations for preventing deep vein thrombosis during surgery for varicose veins are early ambulation and post-procedural use of compression stocking.20,22
Skin burn is a potential complication after RFA which can be reduced by strict adherence to adequate instillation of normal saline in the subcutaneous plane.22 With this technique the skin burn has reduced from 1.8% to 0.5%.22
A review study of 28 articles published from 1942 to 2003 shows female preponderance in the prevalence of varicose veins. In an analysis of varicose vein surgery in India involving 170 patients, they found male predominance (74.7%) and the left side more common than the right side.7 They had a very high proportion of patients with ulceration (57.6%).7 Another study from India comprising varicose vein patients subjected to surgery also had male predominance (70.9%). This variation might be related to the difference in health-seeking behavior among males and females in this part of the world.23,24 In the study 70 (87.5%) limbs had surgery for GSV and the remaining 10 had surgery for SSV (12.5%).8
Conclusion
Conservative management, open surgery, and minimally invasive surgical treatment modalities are common treatment options for varicose veins. Varicose vein in our setting was more common in males and was more seen on the left side. The most common complication after surgical treatment was painful thrombosed superficial veins. DVT was a rare complication. Availability of newer minimal invasive intervention of varicose veins like radiofrequency ablation in our setup makes the optimal management of most cases of varicose veins possible. However, in some cases, there is still a role for conventional treatment modalities. There is still room for more analytical studies to be done in the field of varicose veins in Nepal.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kayssi A, Pope M, Vucemilo I, Werneck C. Endovenous radiofrequency ablation for the treatment of varicose veins. Can J Surg. 2015;58:85–86. doi:10.1503/cjs
2. Hudson BF, Ogden J, Whiteley MS. A thematic analysis of experiences of varicose veins and minimally invasive surgery under local anaesthesia. J Clin Nurs. 2015;24:1502–1512. doi:10.1111/jocn.2015.24.issue-11pt12
3. Barstow C, Kassop D. Cardiovascular disease: chronic venous insufficiency and varicose veins. FP Essent. 2019;479:16–20.
4. Somasundaram SK, Weerasekera A, Worku D, et al. Office based endovenous radiofrequency ablation of truncal veins: a case for moving varicose vein treatment out of operating theatres. Eur J Vasc Endovasc Surg. 2019. (online first). doi:10.1016/j.ejvs.2019.05.020
5. Goodyear SJ, Nyamekye IK. Radiofrequency ablation of varicose veins: best practice techniques and evidence. Phlebology. 2015;30:9–17. doi:10.1177/0268355515592771
6. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3217733/pdf/2011-0212.pdf. Tisi PV. Varicose veins. BMJ Clin Evid. 2011;01:212.
7. Joseph N, Abhishai B, Faizan TM, Devi MU, Abna A, Juneja I. A multicenter review of epidemiology and management of varicose veins for national guidance. Ann Med Surg. 2016;8:21–27. doi:10.1016/j.amsu.2016.04.024
8. Singh KK, Surjyalal Sharma A, Sunil Singh L, Mahadev P. Prevalence and surgical outcomes of varicose veins at Regional Institute of Medical Sciences, Imphal. J Indian Acad Clin Med. 2013;14:209–213.
9. Ministry of Health/ Nepal,New ERA/Nepal, Nepal Health Sector Support Program-NHSSP/Nepal, and ICF. Nepal Health Facility Survey 2015. Kathmandu, Nepal: Government of Nepal, Ministry of Health; 2017.
10. Karmacharya RM, Shrestha BK. Prediction of saphenofemoral junction incompetence by measurement of great saphenous vein size at the level of femoral condyle. Indian J Vasc Endovasc Surg. 2018;5:92–94.
11. Murli NL, Navin ID. Classical varicose vein surgery in a diverse ethnic community. Med J Malaysia. 2008;63:193–198.
12. Lin F, Zhang S, Sun Y, Ren S, Liu P. The management of varicose veins. Int Surg. 2015;100:185–189. doi:10.9738/INTSURG-D-14-00084.1
13. Shah S, Koirala S, Pradhan S, Pradhan A. Surgical outcomes of varicose veins at Universal College of Medical Sciences, Bhairahawa, Nepal. J Universal Coll Med Sci. 2018;4:14–16. doi:10.3126/jucms.v4i2.19085
14. Karmacharya RM, Shyakya YR, Shrestha B. Analysis of consecutive open surgeries for varicose vein at Dhulikhel hospital. Kathmandu Univ Med J. 2014;12:190–193. doi:10.3126/kumj.v12i3.13716
15. Karmacharya RM, Pradhan S, Shakya YR, et al. Study of open surgical method and radio frequency ablation of varicose vein cases at Dhulikhel hospital, a tertiary care center of rural Nepal. Int J Health Sci Res. 2014;4(10):43–46.
16. Ia N, Jc E, Ezemba N, Jm C, Lf I, Cn N. Management of varicose veins of the lower extremities: a 10-year institutional experience. Vasc Med Surg. 2017;05. doi:10.4172/2329-6925.1000309
17. Callam MJ. Epidemiology of varicose veins. Br J Surg. 1994;81:167–173. doi:10.1002/bjs.1800810123
18. Frohn MN. Leg varicose veins and deep vein thrombosis. Lancet. 1976;308:1019–1020. doi:10.1016/S0140-6736(76)90850-3
19. Tellings SS, Ceulen RPM, Sommer A. Surgery and endovenous techniques for the treatment of small saphenous varicose veins: a review of the literature. Phlebology. 2011;26:179–184. doi:10.1258/phleb.2010.009095
20. van Rij AM, Chai J, Hill GB, Christie RA. Incidence of deep vein thrombosis after varicose vein surgery. Br J Surg. 2004;91:1582–1585. doi:10.1002/(ISSN)1365-2168
21. Sette Bruno D. Endovenous radiofrequency ablation for the treatment of varicose veins: a single centre experience. World J Vasc Surg. 2018;1:1–5.
22. Anwar MA, Lane TRA, Davies AH, Franklin IJ. Complications of radiofrequency ablation of varicose veins. Phlebology. 2012;27:34–39. doi:10.1258/phleb.2012.012s21
23. Ahmed SM, Adams AM, Chowdhury M, Bhuiya A. Gender, socioeconomic development and health-seeking behaviour in Bangladesh. Soc Sci Med. 2000;51:361–371. doi:10.1016/S0277-9536(99)00461-X
24. Shaikh BT, Hatcher J. Health seeking behaviour and health service utilization in Pakistan: challenging the policy makers. J Public Health. 2005;27:49–54. doi:10.1093/pubmed/fdh207
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.