")
Back to Journals » ImmunoTargets and Therapy » Volume 8
Varicella zoster virus vaccines: an update
Authors Gabutti G , Bolognesi N , Sandri F , Florescu C, Stefanati A
Received 11 April 2019
Accepted for publication 6 June 2019
Published 6 August 2019 Volume 2019:8 Pages 15—28
DOI https://doi.org/10.2147/ITT.S176383
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Michael Shurin
Giovanni Gabutti,1 Niccolò Bolognesi,2 Federica Sandri,2 Caterina Florescu,2 Armando Stefanati1
1Department of Medical Sciences, University of Ferrara, Ferrara, Italy; 2Postgraduate School of Hygiene and Preventive Medicine, University of Ferrara, Ferrara, Italy
Abstract: Varicella zoster virus (VZV) is the etiological agent of varicella, a highly infectious, self-limiting disease with serious complications. The decline in cell-mediated immunity (CMI) that occurs with aging or immunodepression causes a reactivation of the latent VZV as herpes zoster (HZ). Prevention of VZV through varicella vaccination strategies allows to avoid the primary infection in newborns and susceptible subjects. Available monovalent and combined VZV vaccines are effective, safe and generally well tolerated. Universal varicella vaccination has significantly impacted on incidence, complications and deaths related to this disease. Prevention of HZ through vaccination is a priority to avoid the significant burden of its incidence and complications. Currently two HZ vaccines are available. The recombinant zoster vaccine (RZV), approved by the FDA in 2017 and Zoster Vaccine Live (ZVL) licensed in the United States by the FDA in 2006. The advisory committee on immunization practices (ACIP) preferentially recommends RZV. ZVL remains an option for prevention of HZ in immunocompetent adults aged ≥60 years, although the CMI tends to wane a few years after vaccination.
Keywords: epidemiology, varicella vaccine, recombinant zoster vaccine, Zoster Vaccine Live, vaccination strategies
Varicella: background
Epidemiology
Varicella zoster virus (VZV) is a highly contagious, neurotropic α-herpesvirus that infects humans, with no animal reservoir. Primary infection, usually during childhood, causes varicella. The virus remains latent in the sensory nerve ganglia and subsequently, due to the waning cellular immunity (CMI) to VZV (due to aging or some immunosuppressing states), can reactivate, causing herpes zoster (HZ).1,2
VZV is ubiquitous, however it is difficult to estimate its global burden, mainly because the only available data come from non-homogeneous surveillance systems. Most data on the epidemiology of varicella are from high-income countries; in this area, in the pre-vaccination era, >90% infections occurred before adolescence and less than 5% of adults remained susceptible to the virus.3
Conversely, in many tropical areas, the acquisition of the infection occurred in older age, with consequent greater susceptibility among young adults (14–19%, 26% and up to 50% of susceptible adults in Saudi Arabia, India and Sri Lanka, respectively).4 The reasons for this difference in the age of acquiring primary VZV infection are poorly understood and probably include the influence of climate, population density and the risk of exposure of subjects to the pathogen.
Varicella shows a strong seasonality in temperate environments and in most tropical areas, with peaks of incidence in winter and spring, or in the coldest and driest months in the tropics.5 In the pre-vaccination era, the epidemic peaks occurred with an inter-epidemic cycle of 2–5 years.6
The annual incidence rates of varicella in Europe, before the introduction of vaccination, were estimated between 7.05 (Greece) and 16.1 (Netherlands) for 100,000<5-year-old children, corresponding respectively to seroprevalence rates of 35.3% and 80.6%.7
In many countries, the annual incidence of varicella corresponded roughly to a birth cohort.8
Clinical aspects
Although varicella is usually a self-limiting disease, serious complications can occur in pediatric patients, mediated by the virus or by a secondary bacterial infection. Furthermore, VZV infection in adulthood is related to more serious symptoms and longer clinical course than in children.
Globally, serious complications, with hospitalization, are estimated around 4.2 million per year.9
The extra-cutaneous complications affecting the central nervous system range from cerebellar ataxia (1 case in 4,000) for which the prognosis is usually good, to encephalitis (1 in 33,000–50,000 cases). Rarely, (about 1 in 40,000 cases) these complications can lead to death, especially among immunocompromised subjects.10
The most common complications are secondary bacterial infections of the skin and soft tissues in children and pneumonia, usually viral, in adults. The groups at highest risk for serious complications and death are newborns, pregnant women and severely immunocompromised individuals.
Varicella acquired in the first trimesters of gestation can cause serious congenital diseases in the newborn in about 1–2% of affected pregnancies.11
VZV infection in pregnant women, even if rare, can lead to very severe manifestations, both in the mother and in the fetus. Newborns are at risk especially if the mother develops varicella within 5 days before or 2 days after delivery.
Historically, the mortality rate for congenital varicella was about 30%, but the availability of VZV immunoglobulins and intensive supportive therapy reduced mortality of about 7%.12
Globally, specific mortality for varicella is considerably lower than deaths due to the other infectious diseases such as measles, pertussis, rotavirus or invasive pneumococcal infection; however, varicella cannot be deemed a trivial infectious disease, considering its complications.
The mortality rate for varicella, in high-income countries, in the pre-vaccination era, was about 3 in 100,000 cases.11 In 2010, the mortality rate was 0.1 per 100,000 in comparison to 1.7 and 1.1 for measles and pertussis, respectively.6
The introduction and implementation of universal vaccination in many European countries and other parts of the world have had a significant impact on incidence, hospitalizations and mortality rates, demonstrating the effectiveness of this strategy.2,13
Herpes zoster: background
Epidemiology
HZ is an acute vesicular dermatitis, characterized by radicular pain, related to the reactivation of VZV in the sensory ganglia and to a decline in VZV-specific CMI.14 HZ presents a dermatomal distribution corresponding to the ganglion where the VZV is latent.15,16
Primary varicella infection causes a permanent latency of the virus in the sensory ganglia and elicits a cellular immune response that usually prevents the reactivation and spread of VZV for a long time. Exposure to the virus (exogenous and/or endogenous) stimulates the host immunity.5
The incidence of HZ is related to the age of the population. Generally the incidence and severity of HZ increase with age,17 in relation to the progressive decline of VZV-specific CMI.15
Although age is the most common risk factor for HZ, an increased incidence of HZ has also been associated with immunosuppression related to certain co-morbidities, such as solid tumors, hematological malignancies, HIV infection, autoimmune diseases and to immunosuppressive treatment. In these subjects the clinical picture can be atypical, more serious and has a longer duration.18
Globally, the incidence is 2–3 cases/1,000, up to 5/1,000 and 6–7/1,000 person/year in the age groups 20–50 years, >60 years and 70–80 years, respectively.19
The age-specific incidence of HZ is well documented in North America, Europe and Asia-Pacific; while few data are available in countries such as Africa, Asia and Latin America.20
It is estimated that at least 25% of subjects will experience an HZ episode during their lifetime; two-thirds of the world’s cases involve >50 year-old subjects.
Considering the changing demography of the population, a further increase in the number of cases is expected in the future. At European Union (EU) level it is estimated that over 1.7 million cases of HZ occur each year.21
HZ is a major global health problem and incidence increases ≥50 years of age, due to the growing number of elderly, co-morbidity and/or immunosuppression.20 The incidence rate of HZ in cancers patients receiving immunosuppressive chemotherapy is estimated to be 3–4 times higher (12/1,000 person/year) than in the overall population.18
Clinical aspects
HZ has a significant impact on health, quality of life and health care costs, which increases with age and correlates with its possible complications.22 The most common complication is post-herpetic neuralgia (PHN), defined as persistent pain, for >90 days, after resolution of the rash with a highly negative impact on patients’ quality of life. Other complications include secondary bacterial infections at the level of the involved dermatome, ophthalmic complications and different degrees of segmental paresis, which can be located in extraocular muscles, limbs, abdominal wall or diaphragm. Ten to 20% of HZ cases involve the viral reactivation in the first branch of the trigeminal nerve (Herpes Zoster Ophthalmic [HZO]). Twenty to 70% of patients with HZO develop complications (blepharitis, keratoconjunctivitis, iritis, scleritis and acute retinal necrosis). Neurological complications are less frequent than ocular complications and may include ophthalmoplegia, optic neuritis and ptosis.19
In immunocompromised patients, the dissemination of HZ beyond the distribution of the involved dermatome is possible, spreading to other organs (e.g., encephalitis) and making the condition potentially lethal.23
Ischemic events such as stroke and transient ischemic attacks have been documented in subjects with previous HZ, particularly ophthalmic. Furthermore, in the elderly HZ can lead to a permanent loss of independence and an inability to recover the lifestyle, interests and level of activity prior the disease.24
HZ is an important public health problem associated with frequent and debilitating complications.25 It is noteworthy that the therapeutic options for HZ-related complications have limited efficacy.
Therefore the prevention of HZ is a priority,22 especially in high-risk individuals with chronic conditions (patients with diabetes mellitus, autoimmune diseases, renal insufficiency and neoplasms).16,26
Because of the significant burden caused by HZ and its complications, mainly PHN, the adoption of a preventive strategy seems to be particularly promising.22,24 Vaccination is an important tool to reduce the epidemiological, clinical and economic burden of HZ and to reduce the negative impact on the quality of life.27
Live attenuated varicella vaccine
Available products
The VZV vaccine, which contains live attenuated virus derived from the OKA strain, was created by Dr. Takahashi at Biken Institute, Osaka, in 1974.28
The wild-type OKA strain virus was first isolated by a varicella-infected child and then attenuated through sequential passage in embryonal cell culture.29
Albeit WHO does not indicate a minimum number of plaque-forming units (PFU) per single vaccine dose, it demands that this should be specified by individual national authorities. The viral amount needed to obtain authorization should keep into consideration the scientific evidences of safety and effectiveness provided by clinical trials. Licensed vaccines contain 1,000–17,000 PFU.6
Currently, two monovalent vaccines, derived from the OKA strain (Merck and GSK), are available. Two other attenuated combined quadrivalent MMRV vaccines have been developed (Merck and GSK) in order to facilitate their integration in current pediatric vaccination programs.
The monovalent vaccine was first authorized in 1987 in Japan; the combined MMRV vaccine, on the other hand, was licensed 2005 in the US, for healthy children aged 12 months up to 12-years-old, relying on its safety and non-inferior immunogenicity compared to monovalent MMR and varicella vaccines.3 All vaccines are licensed for use in subjects aged 12 months or older.
Schedule and vaccine efficacy/effectiveness
A two-dose schedule is recommended; the first dose must be administered at 12–15 months of age and the second at 4–6 years of age or respecting the minimum interval between the doses, as indicated in the SmPC. Two doses are recommended in susceptible adolescents and adults as well, particularly in health care workers.
Several studies have shown the need of a two-dose schedule also for MMRV vaccines, to grant an optimal protection,30 respecting the minimum interval between the two doses indicated in the SmPC.
For both formulations (monovalent VZV and combined MMRV) different schedules are possible: an accelerated one (second dose is administrated 1 month after the first dose) and a regular one (second dose follows 1–6 years after the initial dose). Increasing time interval between doses improves immune response but increases the risk of secondary vaccination failures (breakthrough events).31
The route of administration is subcutaneous; nevertheless intramuscular route is safe and effective.6
In countries where varicella represents a major public health problem, WHO recommends taking into consideration the introduction in pediatric immunization programs, provided that at least an 80% coverage rate is achieved. In countries with a high percentage of susceptible people aged 15 years or older, WHO recommends a two-dose schedule for susceptible adolescents and adults.30
Varicella vaccine effectiveness varies depending upon the schedule (one or two doses). Data show that in children the effectiveness of a single dose of a single dose is 85% in the prevention of all forms of varicella and ≥95% against severe forms.9 In a recent meta-analysis, varicella vaccine effectiveness with a two-dose schedule has been 92% (IC 95% 88–95).32
Taking into consideration effectiveness data, the humoral and cell-mediated immunity (CMI) improvement after the second administration and the incidence decline in the US, following the recommendation of a second dose in children,33 the Advisory Committee on Immunization Practices (ACIP) recommends a two-dose schedule against varicella, aiming to prevent all varicella forms.34
Live attenuated vaccines give a long-lasting immunity response, however, the exact duration of protection is still uncertain.
Several studies have indicated that people immunized against VZV have antibodies at least 10 or 20 years after the vaccination; however, these studies were performed when vaccine use was not very widespread and wild-type virus broadly circulated. A case-control study conducted from 1997 to 2003 showed that a single vaccine dose is 97% and 86% effective in the first and second year after vaccination, respectively. From the second to the eighth year after immunization, effectiveness ranges between 86% and 81%.35
A trial regarding varicella vaccine, performed in the US on 914 healthy children, aged 4.7 years on average, showed a vaccine effectiveness of 100% and 98% after 1 year and 2 years, respectively. A third study, with a 10 year follow-up, compared persistent immunity level in those who had a single vaccine dose and those who had both doses and estimated a 94.4% and 98.3% vaccine effectiveness, respectively.36
Safety profile
Live varicella vaccine is safe and well tolerated; is contraindicated in subjects with an anaphylactic reaction to any vaccine components (included neomycin), during pregnancy (because of the theoretical fetal risk) and in subjects with primary or acquired immunodeficiency. Pregnancy should be avoided 4 weeks after immunization.37
Severe adverse vaccine-correlated reactions have been very rarely reported and occurred almost exclusively in immunocompromised patients, not recognized at administration time.38
A systematic review on safety of the varicella vaccines points out that monovalent vaccine is very well tolerated and the most common adverse events reported after vaccination include slight tenderness, redness as well as skin eruption (rash) at injection site.39
MMRV vaccine showed good safety profiles too, with the exception of a higher fever and rash incidence.40,41
Both available tetravalent vaccines have been associated with an increased febrile seizure rate 6–12 days after first dose, in comparison to co-administration of MMR and varicella vaccine. Several studies on MMRV vaccine have demonstrated that febrile seizure’s incidence is 1 case in 2,300–2,600 children aged 12–23 months31,42 and such episodes have not been associated with any long-term sequelae.43 Moreover, an increased risk of febrile seizures after the second dose has not been noticed.44 Noteworthy, the highest febrile seizure risk occurs in pediatric age, overlapping with the timing of MMR and varicella vaccines administration.45
MMRV vaccine use simplifies the administration, by giving protection against multiple illnesses with a single injection. This contributes improving the vaccine coverage and decreasing health costs;46 anyway, co-administration of varicella and MMR vaccines decreases, but does not eliminate, the risk of fever peak or febrile seizures.40,41
Live attenuated HZ vaccine
In 1965 Edgar Hope-Simpson observed that the incidence and severity of HZ increased with age and hypothesized that the cause was a decline in VZV-specific CMI; he also observed that HZ recurrences were relatively rare among immunocompetent persons hypothesizing that the HZ episode induced a reactivation of immunity sufficient to protect against a subsequent episode.47
This important discovery led to the development of a vaccine able to enhance the VZV-CMI, reducing the incidence and severity of the disease, useful for subjects with a positive history of varicella.48
The development of a live attenuated varicella vaccine opened the way for an HZ vaccine.5
A high dose of live attenuated vaccine (OKA strain; >19,400 PFU; ZVL) allows the reactivation of the VZV-CMI and reduces the frequency and severity of HZ. ZVL is similar to the varicella vaccine but has a higher antigen content (>14 times greater).49 Each dose contains a minimum of 19,400 PFU (4.29 log10) of VZV/OKA strain, when reconstituted.
Preliminary studies have been conducted to establish the safety and immunogenicity of higher doses of OKA vaccine, to select a dose able to increase VZV-CMI with minimal side effects and to verify its safety and efficacy in elderly subjects with common co-morbidities.48,50,51
The pre-licensure RCT showed that ZVL is effective in preventing HZ and PHN.22
ZVL was licensed by FDA in 2006 as a live attenuated vaccine indicated for the prevention of HZ and PHN in immunocompetent adults aged ≥50 years and it is recommended by the ACIP for use in immunocompetent adults ≥60 years.49,51,52
Several studies have shown the safety and efficacy of ZVL in immunocompetent adults.49,53–56
Evaluation of the safety profile 10 years after the licensing of ZVL was consistent with results observed in clinical trials. Serious adverse events have rarely been reported and mainly in individuals who had contraindications for this vaccine.57
ZVL is effective in preventing the disease but the protection tends to decay over time.49,58 In general, ZVL is well tolerated, has few systemic adverse events and mild to moderate injection site adverse events.59,60
Regarding vaccination efficacy (VE) of ZVL and its duration, in the last update of the SmPC it is specified that against HZ and PHN this has been evaluated for a maximum of eight years after vaccination. VE estimates by age at the time of vaccination and mean VE estimates for the first 3 and 5 years indicate an age-related decrease.61
Subjects with previous episodes of HZ, co-morbidities such as chronic renal failure, diabetes mellitus, rheumatoid arthritis and chronic lung disease, can be vaccinated.52 ZVL is not indicated in children and adolescents and for the prevention of varicella; it can be co-administered with inactivated influenza vaccine and 23-valent pneumococcal polysaccharide vaccine.61
ZVL should be administered as a single dose of 0.65 ml subcutaneously in the deltoid region of the upper arm.49
ZVL is contraindicated in patients with primary and acquired immunodeficiency, in patients who are on immunosuppressive therapy, in patients with untreated TB and in pregnancy.61
For the evaluation of long-term immunogenicity, the effects of a second dose of vaccine were verified 10 years after the first.62 The booster dose increases the CMI to levels comparable to those obtained in subjects of the same age who received the first dose; this indicates that the immune memory persists >10 years after vaccination. Further studies to assess the long-term persistency of the immunity are underway.63
The effectiveness studies confirm that the ZVL vaccine is associated with a lower incidence of HZ among immunocompetent adults in populations with different characteristics.64,65,66
The evaluation of the impact of vaccination in the elderly in the UK has shown a similar effectiveness in the different age classes and an adequate duration of protection, indicating a better cost–benefit ratio than expected.64 ZVL is effective against HZ and its complications and reduces the incidence of the disease, regardless of age and co-morbidity, but the duration of protection decreases over time.67
Some studies have evaluated the effectiveness in not seriously immunosuppressed individuals, in patients with renal or autoimmune conditions. These patients are at increased risk of HZ and complications and the response to the vaccine may be lower due to immunosuppression.25,65,66
ZVL may not be associated with an increased risk of HZ after vaccination in patients treated with biological immunosuppressive drugs. However, in current recommendations, ZVL is contraindicated in patients receiving this type of medication due to a lack of available data.68
The effectiveness data, emerging from the use of ZVL in the UK, indicate that in the first 3 years of the vaccination program, 17,000 cases of HZ and 3300 cases of PHN were avoided in a population eligible for vaccination of 5.5 million people.69
A review on cost-effectiveness of ZVL reports that most studies (12 out of 15) show that vaccination against HZ is likely to be cost-effective. Differences in results are likely due to varying assumptions about duration of vaccine protection and quality-adjusted life years (QALY) loss due to HZ.70
Despite strong evidence supporting its effectiveness, the vaccination practice remains not optimal with unsatisfactory coverage in particular groups of patients.64 Consequently substantial efforts should be made to increase the use of the vaccine.25
Recombinant zoster vaccine
The HZ recombinant adjuvanted vaccine (RZV) was approved by the FDA in 201749 and by the European Commission in 2018.71 RZV contains the glycoprotein E (gE) of VZV, essential for the replication and intercellular viral diffusion and target of the specific immune response, and the AS01B adjuvant that stimulates the innate immune response activation.72,73
Preclinical trials have shown that the AS01B adjuvant also enhances the specific antibody and cell-mediated response.74 Phase I/II trials showed that, in comparison to ZVL, RZV induces a greater and more lasting immune response, both cell-mediated and humoral, in subject of all ages.74
A multicenter phase II RCT on ≥50-year-old subjects showed that RZV guarantees a significantly higher response than a non-adjuvanted subunit (gE) vaccine and placebo. Regarding the tolerability profile, RZV showed a higher occurrence of adverse reactions, mostly mild to moderate and transient.75 Another phase II study evaluated the safety and immunogenicity profile of different RZV formulations and schedules showing that the two-dose vaccine schedule leads to a gE-specific clonal expansion of CD4+ T-lymphocytes up to 3 times higher than the mono-administration of adjuvanted vaccine or to the administration of two doses of the non-adjuvanted vaccine, with a response that remains high over time. Among the options tested, those with two doses of 50 or 100 µg of gE/AS01B gave a humoral response equal to or greater than those of the other groups. It also emerged that the non-adjuvanted vaccine is not capable of inducing a satisfactory cell-mediated response.76 A third follow-up study on subjects who received gE/AS01B adjuvanted vaccine with a 50 µg dosage showed that after 72 months both cell-mediated and humoral response tend to decrease 20–25% lower in comparison to 36 months, while remaining satisfactory and significantly higher than the pre-vaccination status.77 In 2018, Schwarz et al examined the same subjects 9 years after the first administration to evaluate the humoral and cell-mediated immune response, confirming that these continue to remain significantly higher compared to the pre-vaccination status and estimating that this immunity will remain elevated for at least 15 years after vaccination.78
The waning of immune response observed between 3 and 7 years after the vaccination with ZVL led to the idea of administering the RZV vaccine even in those already vaccinated with ZVL. Grupping et al evaluated the humoral and cell-mediated immune response to the RZV vaccine comparing subjects vaccinated with ZVL in the previous 5 years and never vaccinated. The results showed a non-inferiority of the previously vaccinated group compared to the never vaccinated, supporting the hypothesis of administering RZV to subjects previously vaccinated with ZVL.79
The optimal time between the two doses of RZV was evaluated in the study by Lal et al in 2018: the second dose of vaccine should be administered between 2 and 6 months after the first dose.78
Vink et al showed a comparable antibody response after both subcutaneous and intramuscular administration but a greater reactogenicity using the subcutaneous route.80
The preclinical trials that evaluated the efficacy of RZV were the ZOE-50 in 2015 and the ZOE-70 in 2016. The first is a multicenter randomized case-control study on subjects aged ≥50 years that estimated the efficacy of RZV at 97.2%.81 The second study, carried out on subjects aged ≥70 years, showed that the efficacy is comparable in older subjects.72 Three years after vaccination, the immune response was persistent in the subjects enrolled in both trials.73 Similarly, in the follow-up evaluation of enrolled subjects, non-PHN complications and HZ-associated hospitalizations were lower than in the placebo group.82
RZV provides the opportunity to evaluate the vaccination of subjects with impaired immune status, at greater risk of contracting HZ and unable to get vaccinated with ZVL. The data currently available suggest that RZV is safe and immunogenic in HIV+ immunocompromised patients and in autologous hematopoietic stem cell transplant recipients.83–85
The ACIP, that comprises medical and public health experts who develop recommendations on the use of vaccines in the civilian population of the US, recommends the use of RZV in subjects on low-dose immunosuppressive therapy (<20 mg/die of prednisone or equivalent or in therapy with topical steroids or inhalers), before starting an immunosuppressive therapy, or after recovering from a temporary immunosuppression. Since immunocompromised subjects or those receiving medium-high doses of immunosuppressants were excluded from preclinical efficacy studies (ZOE-50 and ZOE-70), ACIP does not recommend vaccination with RZV, but anticipates the possibility of revising this position when new evidence will be available.49
From a safety standpoint, 85% of the 6773 vaccinated subjects reported local or systemic reactions after receiving RZV in preclinical trials. However, the number of severe adverse events was similar in the RZV and placebo groups.86
After licensing, adverse vaccine events were monitored through the Adverse Event Reporting System (VAERS),87 a US national passive surveillance system. The first 8 months of post-licensing monitoring of RZV in the US showed a safety profile consistent with that observed in pre-licensed clinical trials.88 Of the 4381 reported adverse events (136 per 100,000 doses), 97% were non-serious, and 3% were severe. The most common adverse reactions were pyrexia (23.6%), injection site pain (22.5%), injection site erythema (20.1%), pain (19.5%), chills (19.3%), headache (16.7%), fatigue (15.8%), pain in extremity (15.8%), injection site swelling (13.4%), myalgia (12.1%). Compared to ZVL, for which HZ and rash were reported as common adverse reactions,59 RZV had a greater number of systemic reactions (e.g., fever).
Concerning the pharmaco-economic aspects, the CDC analysis estimates that RZV compared with no vaccination costs $ 31,000/QALY for immunocompetent adults aged ≥50 years. The number of subjects to be vaccinated with RZV to prevent one case of HZ and one of PHN are 11–17 and 70–187, respectively. Compared to vaccination with ZVL, RZV is able to prevent a greater number of HZ cases at a lower cost.49
According to Curran et al, RZV is more effective and less expensive (at a price of $280 for two doses) compared to ZVL (price $231 for a dose) in subjects aged ≥60 years. The incremental cost-effectiveness ratio (ICER) compared to no vaccination ranged from $20,038 to $30,084/QALY.89
The analysis performed by De Boer et al in the Netherlands concluded that, despite a two-dose strategy, RZV is superior in reducing the burden of HZ compared to a single dose or a dose + booster of ZVL. The more cost-effective alternative between RZV and ZVL will mainly depend on the cost of the vaccines. Vaccination of risk groups such as subjects undergoing autologous stem cell transplant could however result in an improvement in cost-effective outcomes compared to immunocompetent subjects only.90
A study on the German population to assess the optimal starting age for the vaccination campaign against HZ has evaluated the cost-effectiveness of RZV. With an ICER of €37,000/QALY for the cohort ≥60 years and €44,000/QALY for the cohort ≥70 years, the analyses shows that the best value from a public health and economic standpoint would be obtained by vaccinating the German population at age 60 or 65 years.91 A similar study carried out in Hong Kong to assess both gender and optimal age for the use of RZV concluded that the range 60–70 years for both genders is the most cost-effective.92
A further cost-effectiveness analysis performed in the US by Curran et al to evaluate the revaccination with RZV in all ≥60-year-old subjects previously vaccinated with a dose of ZVL as recommended by ACIP49 showed a saving of $96 million compared to no additional vaccination (ICER $58,793/QALY saved) and $84 million compared to revaccination with ZVL.93
According to ACIP indications, RZV can be used in adults aged ≥50 years, regardless of previous vaccination for varicella or ZVL. However, ZVL remains among the vaccines recommended in immunocompetent subjects over 60 years.49
The schedule includes two doses of RZV with an interval of 2–6 months independently of previous vaccinations with ZVL. The vaccination cycle should not be repeated if more than 6 months have passed since the first dose, although the efficacy of alternative time intervals has not been evaluated and could expose you to the risk of HZ between the two doses. If the second dose of RZV is given less than 4 weeks after the first, the second dose should be repeated. RZV should not be given <2 months after receipt of ZVL.
As suggested by the CDC guidelines for recombinant vaccines, RZV can be co-administered with other vaccines in a different anatomical site.94 There is evidence that co-administration of RZV with the quadrivalent split flu vaccine does not cause interference in the immune response.95 Evaluation of co-administration with 23-valent pneumococcal polysaccharide vaccine (PPSV23) and tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis vaccine (Tdap, GSK) is ongoing. The safety and efficacy of concomitant administration of two adjuvanted vaccines (e.g., RZV and adjuvanted influenza vaccine [aTIV]) have not been evaluated.
RZV recipients should be informed about expected systemic and local reactogenicity before vaccination. Reactions to the first dose do not predict reaction to the second dose and vaccine recipient should be encouraged to complete the two-dose cycle.
Patients with a history of HZ should receive RZV to avoid recurrence. Vaccination should be delayed until acute stage of HZ is over; adults with chronic medical conditions should receive RZV.
Screening for varicella before vaccination is not recommended, but in persons known to be VZV negative via laboratory serology, ACIP guidelines for varicella vaccination should be followed. RZV has not been evaluated in VZV seronegative subjects and is not indicated for the prevention of varicella.
A history of severe allergic reactions, such as anaphylaxis, to any component of the vaccine is a contraindication for the administration of RZV. No data are available to establish whether RZV is safe in pregnant or lactating women. Delaying vaccination with RZV should be considered in such circumstances.49
Global vaccination strategies
A WHO position paper on VZV and HZ vaccines provides a guide to member States for setting up large-scale immunization programs.6
Varicella
The live attenuated VZV vaccine (OKA strain) was first licensed in Germany and Sweden in 1984.96 In South Korea, a live attenuated virus vaccine containing a different strain has been used since 1993 (MAV/06).97
In US vaccination programs a dose of VZV vaccine has been implemented since 1995.98 The introduction of VZV vaccination has led to a substantial reduction in morbidity and mortality, with a reduction in incidence >70% in communities with vaccination coverage of 80% among children aged 19–35 months and a decrease of varicella incidence in all age groups99 In 2006 a second dose of vaccine was introduced, obtaining a further decrease in the incidence to 2 cases per 1,000 patient-years. No child developed the disease after receiving 2 doses of vaccine.99
Varicella vaccination can follow a one or two-dose schedule. The second dose makes it possible to achieve greater protection against all forms of varicella32 Beyond the economic debate on the use of one or two doses of vaccine,100,101 the choice should be based mainly on the goal of the vaccination program: elimination or prevention of severe cases. An Italian study has showed that among coverage, vaccine efficacy, number of doses and interval between doses, ensuring a high coverage remains the critical success factor for significant varicella prevention.102
As of December 2014, the varicella vaccine was recommended in 33 countries, mostly with a high socio-economic level (Table 1).103 This means that despite the proven effectiveness, many countries have not yet entered routine vaccination programs. In the EU, in 2015 only 6 nations had introduced a universal vaccination for children, 2 at regional level (including Italy) and 17 recommended vaccination to only some susceptible risk groups.104 In 2017, Italy introduced compulsory varicella vaccination for all newborns.105
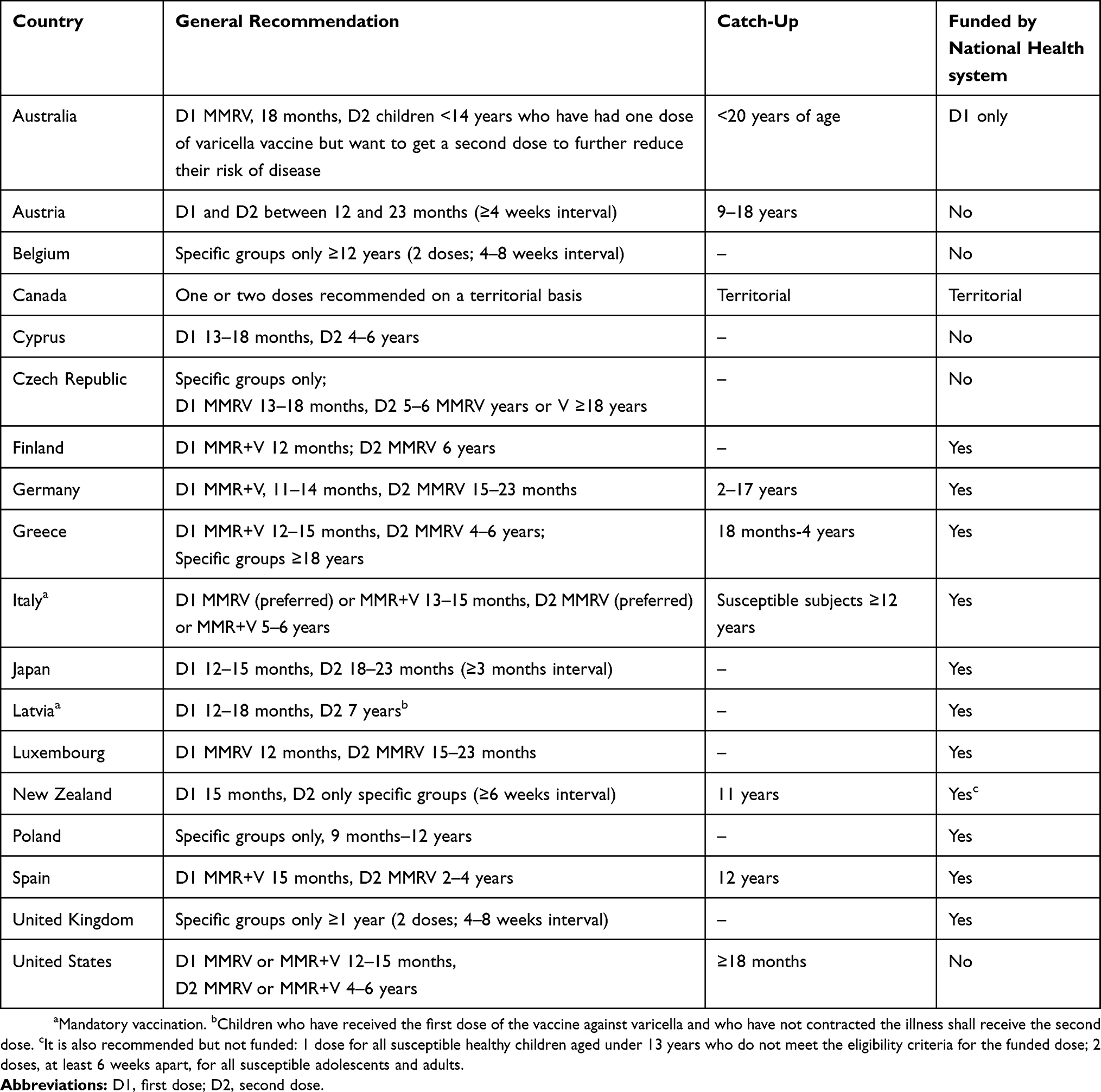 |
Table 1 Varicella vaccination; recommendations by country |
One of the concerns emerging from the introduction of universal VZV vaccination programs is the possible increase in the mean age of infection, due to a lower exposure of the population to VZV. Since the complication rate in the adult population is higher than in children, this could lead to an increase in morbidity and mortality in age groups not affected by the vaccination program.
The evidence shows that, if vaccination coverage is maintained between 30% and 70% for a long time, the shift in the age of infection can lead to an increase in morbidity and mortality in high-income countries.106
Modeling studies on low- and middle-income countries in different geographical regions with different seroprevalence rates (South-East Asia, Pacific, Latin America, Caribbean and Africa) have instead shown that vaccine coverage must be kept at least equal to 60% to produce a substantial reduction in morbidity.107 In detail, in countries with low- and middle-income with a medium to high seropositivity there is a risk of shifting the age of infection when the vaccination coverage with 1 dose remains between 20% and 80% in the long term, with a possible increase in mortality. In countries with a very low seropositivity (less than 20–30% in 20-year-olds) and a high incidence of the disease, a minimal shift in the age of infection is expected, with an important reduction in the morbidity and mortality related to varicella at intermediate rates of vaccination coverage.6
A further worry arising from the implementation of VZV vaccination programs concerns the possible increase in incidence of HZ due to the reduction of the exogenous booster effect on immunity.108 However, the existing evidence is conflicting, with some studies indicating that exposure to circulating VZV is protective against HZ in adults with latent VZV109,110 and others suggesting that the protective effect is minimal or absent.111–113 Some studies have shown an increase in the incidence of HZ after the introduction of varicella vaccination programs, while others have not, and there is no concrete evidence that this trend is related to VZV vaccination compared to other possible factors (demographic increase of the elderly population, increase in chronic conditions, use of oral corticosteroids, secular trends).103,114 Concerning the latency and re-activation of vaccine type virus, cases of zoster have been reported in vaccinated children whose VZV was typed as Oka (vaccine) strain. However the incidence of zoster was 5 times lower in vaccinated children than in control group and there was no difference in clinical severity of zoster caused by vaccine-type virus.115
Furthermore, the recent licensing of HZ vaccines and their introduction into national vaccination schedules could allow a re-evaluation of the epidemiological and economic aspects that led to the refusal to adopt a universal vaccination of newborns in some countries.116
Herpes zoster
The 2014 WHO position paper does not offer recommendations regarding HZ vaccination due to a lack of vaccine efficacy data at the time of publication6
ZVL was first licensed in the US by the FDA in 2006117 RZV was approved by the FDA in 2017 for use in adults aged 50 or older49 A study carried out in the US in 2014 among adults aged ≥60 years resulted in a coverage rate of 31.8%, with wide variability between federal States.118
In Canada ZVL was approved in 2009 and RZV in 2017. Currently, the vaccination of adults aged ≥50 years with two doses of RZV is recommended, including in subjects previously vaccinated with ZVL.119
In Europe, the European Medicines Agency (EMA) has licensed ZVL for subjects aged ≥60 years (2006) and later for those ≥50 years of age (2007).120 RZV was licensed by the European Commission on March 21, 2018.71 ZVL was included among the recommended vaccinations of 6 countries (Austria, Czech Republic, France, Greece, Italy, UK) and is funded by the National Health System in 4 (France, Greece, Italy, UK).121
In Germany the Robert Koch Institute has recommended RZV since December 2018 for all adults aged ≥60 years. ZVL is not recommended.122
In Italy HZ vaccination has been included in the National Plan for Vaccine Prevention (PNPV) 2017–2019123 (and offered free of charge in some regions) with a dose of ZVL in 65-year-olds and in subjects at risk aged ≥50 years.
In Austria, the Impfplan Österreich 2019 recommends vaccination in subjects aged ≥50 years with RZV although this vaccine is not yet available in the country124
In Australia, HZ vaccination is recommended for adults ≥50 years of age living together with immunosuppressed subjects, and all adults aged ≥60 years.120 However, the National Immunization Program (NIP) states that HZ vaccination is offered free of charge with a single dose of ZVL in adults aged 70–79 years.125
In New Zealand, from 1 April 2018, the immunization schedule included a dose of ZVL for subjects aged ≥65 years, with a catch-up program in individuals aged 66–88 years, scheduled until 31 March 2020.126
In Japan, a varicella vaccine live (VVL) was approved for the prevention of HZ in individuals aged ≥50 years as an extended use in March 2016. The titer of the VVL used for HZ prevention is similar to that of the ZVL (42,000–67,000 PFU per dose) (Table 2).127,128
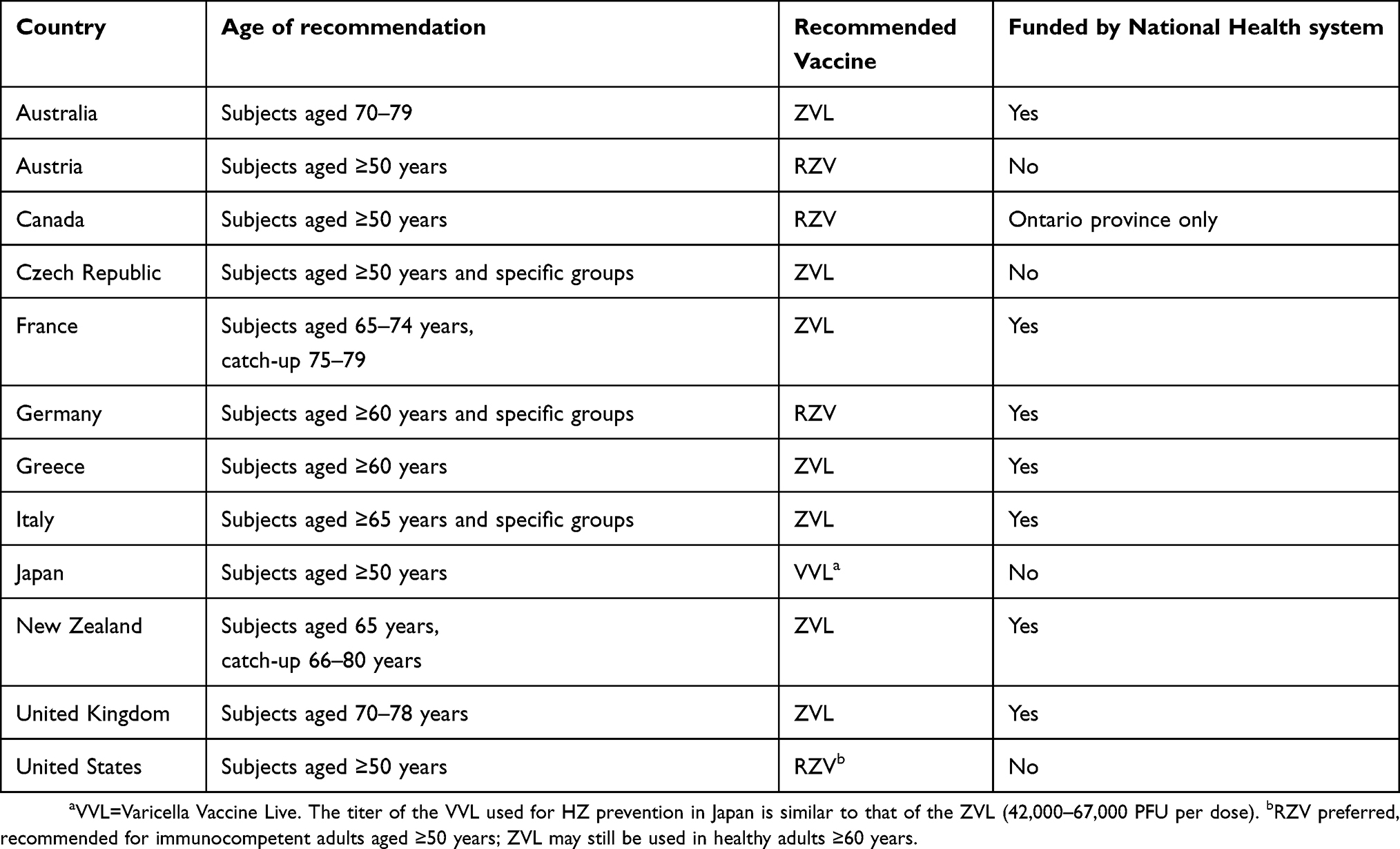 |
Table 2 Herpes zoster vaccination; recommendations by country |
Disclosure
GG received grants from Sanofi Pasteur, MSD (Merck & Co.), GlaxoSmithKline Biologicals S.A., Novartis, Pfizer, MSD Italy, PaxVax and Seqirus for taking part in advisory boards, expert meetings, for acting as a speaker and/or organizer of meetings/congresses and as a principal investigator and chief of Operative Unit in Randomized Clinical Trials (RCTs). GG has also acted as a member of the IDMC (Independent Data Monitoring Committee) of the ZOE50 and ZOE70 RCTs. The authors report no other conflicts of interest in this work.
References
1. Arvin AM. Varicella-zoster virus. Clin Microbiol Rev. 1996;9(3):361–381. doi:10.1128/CMR.9.3.361
2. Heininger U, Seward JF. Varicella. Lancet. 2006;368(9544):1365–1376. doi:10.1016/S0140-6736(06)69561-5
3. Centers for Disease Control and Prevention. Epidemiology and Prevention of Vaccine-Preventable Diseases. 13th ed. Hamborsky J, Kroger A, Wolfe S, editors.
4. Malavige GN, Jones L, Kamaladasa SD, et al. Viral load, clinical disease severity and cellular immune responses in primary varicella zoster virus infection in Sri Lanka. Zimmer J, ed. PLoS One. 2008;3(11):e3789. doi:10.1371/journal.pone.0003789
5. Gershon AA, Breuer J, Cohen JI, et al. Varicella zoster virus infection. Nat Rev Dis Prim. 2015;1:15016. doi:10.1038/nrdp.2015.16
6. Varicella and herpes zoster vaccines: WHO position paper, June 2014. Wkly Epidemiol Rec. 2014;(25):265–288. Available from: https://www.who.int/immunization/policy/position_papers/varicella/en/. Accessed March 1, 2019.
7. Spoulou V, Alain S, Gabutti G, et al. Implementing universal varicella vaccination in Europe. Pediatr Infect Dis J. 2019;38(2):181–188. doi:10.1097/INF.0000000000002185
8. Warren-Gash C, Forbes H, Breuer J. Varicella and herpes zoster vaccine development: lessons learned. Expert Rev Vaccines. 2017;16(12):1191–1201. doi:10.1080/14760584.2017.1394843
9. Seward JF, Marin M. Varicella disease burden and varicella vaccines. WHO Sage Meet. 2014. Available from: http://www.who.int/immunization/sage/meetings/2014/april/2_SAGE_April_VZV_Seward_Varicella.pdf. Accessed March 3, 2019.
10. Meyer PA, Seward JF, Jumaan AO, Wharton M. Varicella mortality: trends before vaccine licensure in the United States, 1970–1994. J Infect Dis. 2000;182(2):383–390. doi:10.1086/jid.2000.182.issue-2
11. Riera-Montes M, Bollaerts K, Heininger U, et al. Estimation of the burden of varicella in Europe before the introduction of universal childhood immunization. BMC Infect Dis. 2017;17(1):353. doi:10.1186/s12879-017-2757-2
12. Advisory Committee on Immunization Practices Centers for Disease Control and Prevention (CDC). Guiding principles for development of ACIP recommendations for vaccination during pregnancy and breastfeeding. MMWR Morb Mortal Wkly Rep. 2008;57(21):580.
13. Streng A, Grote V, Carr D, Hagemann C, Liese JG. Varicella routine vaccination and the effects on varicella epidemiology – results from the Bavarian Varicella Surveillance Project (BaVariPro), 2006-2011. BMC Infect Dis. 2013;13(1):303. doi:10.1186/1471-2334-13-303
14. Steain M, Sutherland JP, Rodriguez M, et al. Analysis of T cell responses during active varicella-zoster virus reactivation in human ganglia. J Virol. 2014;88(5):2704–2716. doi:10.1128/JVI.03445-13
15. Brosio F, Masetti G, Matteo G, Stefanati A, Gabutti G. A novel nonlive, adjuvanted herpes zoster subunit vaccine: a report on the emerging clinical data and safety profile. Infect Drug Resist. 2018;11:1401–1411. doi:10.2147/IDR.S148303
16. Ohfuji S, Ito K, Inoue M, et al. Safety of live attenuated varicella-zoster vaccine in patients with underlying illnesses compared with healthy adults: a prospective cohort study. BMC Infect Dis. 2019;19(1):95. doi:10.1186/s12879-019-3719-7
17. Bricout H, Haugh M, Olatunde O, Gil Prieto R. Herpes zoster-associated mortality in Europe: a systematic review. BMC Public Health. 2015;15(1):466. doi:10.1186/s12889-015-1753-y
18. Vink P, Delgado Mingorance I, Maximiano Alonso C, et al. Immunogenicity and safety of the adjuvanted recombinant zoster vaccine in patients with solid tumors, vaccinated before or during chemotherapy: A randomized trial. Cancer. 2019. doi:10.1002/cncr.31909
19. Johnson RW, Alvarez-Pasquin M-J, Bijl M, et al. Herpes zoster epidemiology, management, and disease and economic burden in Europe: a multidisciplinary perspective. Ther Adv Vaccines. 2015;3(4):109–120. doi:10.1177/2051013615599151
20. Kawai K, Gebremeskel BG, Acosta CJ. Systematic review of incidence and complications of herpes zoster: towards a global perspective. BMJ Open. 2014;4(6):e004833–e004833. doi:10.1136/bmjopen-2014-004833
21. Gabutti G, Franco E, Bonanni P, et al. Reducing the burden of Herpes Zoster in Italy. Hum Vaccin Immunother. 2015;11(1):101. doi:10.4161/hv.34363
22. Marin M, Yawn BP, Hales CM, et al. Herpes zoster vaccine effectiveness and manifestations of herpes zoster and associated pain by vaccination status. Hum Vaccin Immunother. 2015;11(5):1157–1164. doi:10.1080/21645515.2015.1016681
23. Rommelaere M, Maréchal C, Yombi J-C, Goffin E, Kanaan N. Disseminated varicella zoster virus infection in adult renal transplant recipients: outcome and risk factors. Transplant Proc. 2012;44(9):2814–2817. doi:10.1016/j.transproceed.2012.09.090
24. Zorzoli E, Pica F, Masetti G, Franco E, Volpi A, Gabutti G. Herpes zoster in frail elderly patients: prevalence, impact, management, and preventive strategies. Aging Clin Exp Res. 2018;30(7):693–702. doi:10.1007/s40520-018-0956-3
25. Langan SM, Smeeth L, Margolis DJ, Thomas SL. Herpes zoster vaccine effectiveness against incident herpes zoster and post-herpetic neuralgia in an older us population: a cohort study. Harbarth S, ed. PLoS Med. 2013;10(4):e1001420. doi:10.1371/journal.pmed.1001420
26. Gabutti G, Valente N, Kuhdari P, Lupi S, Stefanati A. Prevention of herpes zoster and its complications: from the clinic to the real-life experience with the vaccine. J Med Microbiol. 2016;65(12):1363–1369. doi:10.1099/jmm.0.000386
27. Panatto D, Bragazzi NL, Rizzitelli E, et al. Evaluation of the economic burden of Herpes Zoster (HZ) infection. Hum Vaccin Immunother. 2015;11(1):245–262. doi:10.4161/hv.36160
28. Takahashi M, Otsuka T, Okuno Y, Asano Y, Yazaki T. Live vaccine used to prevent the spread of varicella in children in hospital. Lancet (London, England). 1974;2(7892):1288–1290. doi:10.1016/S0140-6736(74)90144-5
29. WHO. Observed rate of vaccine reactions - Varicella zoster virus vaccine. Inf Sheet WHO. 2012;4. Available from: https://www.who.int/vaccine_safety/initiative/tools/Varicella_Zoster_Vaccine_rates_information_sheet.pdf. Accessed March 2, 2019.
30. Prymula R, Bergsaker MR, Esposito S, et al. Protection against varicella with two doses of combined measles-mumps-rubella-varicella vaccine versus one dose of monovalent varicella vaccine: a multicentre, observer-blind, randomised, controlled trial. Lancet. 2014;383(9925):1313–1324. doi:10.1016/S0140-6736(13)61612-8
31. Bonanni P, Gershon A, Gershon M, et al. Primary versus secondary failure after varicella vaccination: implications for interval between 2 doses. Pediatr Infect Dis J. 2013;32(7):e305–e13. doi:10.1097/INF.0b013e31828b7def
32. Marin M, Marti M, Kambhampati A, Jeram SM, Seward JF. Global varicella vaccine effectiveness: a meta-analysis. Pediatrics. 2016;137(3):e20153741. doi:10.1542/peds.2015-3741
33. Centers for Disease Control and Prevention (CDC). National, state, and urban area vaccination coverage among children aged. 19-35 months–united States, 2005. MMWR Morb Mortal Wkly Rep. 2006;55(36):988–993.
34. Bialek SR, Perella D, Zhang J, et al. Impact of a routine two-dose varicella vaccination program on varicella epidemiology. Pediatrics. 2013;132(5):e1134–40. doi:10.1542/peds.2013-0863
35. Vázquez M, LaRussa PS, Gershon AA, et al. Effectiveness Over Time of Varicella Vaccine. JAMA. 2004;291(7):851. doi:10.1001/jama.291.7.851
36. Kuter B, Matthews H, Shinefield H, et al. Ten year follow-up of healthy children who received one or two injections of varicella vaccine. Pediatr Infect Dis J. 2004;23(2):132–137. doi:10.1097/01.inf.0000109287.97518.67
37. Cameron JC, Allan G, Johnston F, Finn A, Heath PT, Booy R. Severe complications of chickenpox in hospitalised children in the UK and Ireland. Arch Dis Child. 2007;92(12):1062–1066. doi:10.1136/adc.2007.123232
38. Galea SA, Sweet A, Beninger P, et al. The Safety Profile of Varicella Vaccine: A 10‐Year Review. J Infect Dis. 2008;197(s2):S165–S169.
39. Kanra G, Ceyhan M, Özmert E. Safety and immunogenicity of live attenuated varicella vaccine in 9-month-old children. Pediatr Int. 2000;42(6):674–677.
40. Leung JH, Hirai HW, Tsoi KK. Immunogenicity and reactogenicity of tetravalent vaccine for measles, mumps, rubella and varicella (MMRV) in healthy children: a meta-analysis of randomized controlled trials. Expert Rev Vaccines. 2015;14(8):1149–1157. doi:10.1586/14760584.2015.1057572
41. Ma S-J, Li X, Xiong Y-Q, Yao A-L, Chen Q. Combination measles-mumps-rubella-varicella vaccine in healthy children: a systematic review and meta-analysis of immunogenicity and safety. Medicine (Baltimore). 2015;94(44):e1721. doi:10.1097/MD.0000000000000874
42. Jacobsen SJ, Ackerson BK, Sy LS, et al. Observational safety study of febrile convulsion following first dose MMRV vaccination in a managed care setting. Vaccine. 2009;27(34):4656–4661. doi:10.1016/j.vaccine.2009.05.056
43. Klein NP, Fireman B, Yih WK, et al. Measles-mumps-rubella-varicella combination vaccine and the risk of febrile seizures. Pediatrics. 2010;126(1):e1–e8. doi:10.1542/peds.2010-0665
44. Macartney K, Gidding HF, Trinh L, et al. Evaluation of combination measles-mumps-rubella-varicella vaccine introduction in Australia. JAMA Pediatr. 2017;171(10):992. doi:10.1001/jamapediatrics.2017.1965
45. Gabutti G, Kuhdari P, Ferioli S, Trucchi C. Hospital admissions for seizure in Italy: a decennial retrospective analysis with a special focus on the burden in the pediatric age. Neurol Sci. 2015;36(9):1667–1673. doi:10.1007/s10072-015-2230-1
46. Knuf M, Faber J, Barth I, Habermehl P. A combination vaccine against measles, mumps, rubella and varicella. Drugs Today (Barc). 2008;44(4):279–292. doi:10.1358/dot.2008.44.4.1210755
47. Hope-Simpson R. The nature of Herpes Zoster: a long-term study and a new Hypothesis. Proc R Soc Med. 1965;58(1):9–20.
48. Oxman MN. Zoster vaccine: current status and future prospects. Clin Infect Dis. 2010;51(2):197–213. doi:10.1086/652976
49. Dooling KL, Guo A, Patel M, et al. Recommendations of the advisory committee on immunization practices for use of herpes zoster vaccines. MMWR Morb Mortal Wkly Rep. 2018;67(3):103–108. doi:10.15585/mmwr.mm6731e2
50. Simberkoff MS, Arbeit RD, Johnson GR, et al. Safety of herpes zoster vaccine in the shingles prevention study. Ann Intern Med. 2010;152(9):545. doi:10.7326/0003-4819-152-9-201005040-00004
51. Zussman J, Young L. Zoster vaccine live for the prevention of shingles in the elderly patient. Clin Interv Aging. 2008;3(2):241–250.
52. Rafael Harpaz MD, Ortega-Sanchez IR
53. Schmader KE, Johnson GR, Saddier P, et al. Effect of a zoster vaccine on herpes zoster-related interference with functional status and health-related quality-of-life measures in older adults. J Am Geriatr Soc. 2010;58(9):1634–1641. doi:10.1111/j.1532-5415.2010.03021.x
54. Oxman MN, Levin MJ, Shingles Prevention Study Group. Vaccination against Herpes Zoster and postherpetic neuralgia. J Infect Dis. 2008;197(s2):S228–S236. doi:10.1086/522159
55. Lu P, Euler GL, Jumaan AO, Harpaz R. Herpes zoster vaccination among adults aged 60 years or older in the United States, 2007: uptake of the first new vaccine to target seniors. Vaccine. 2009;27(6):882–887. doi:10.1016/j.vaccine.2008.11.077
56. Schmader KE, Levin MJ, Gnann JW, et al. Efficacy, safety, and tolerability of Herpes Zoster vaccine in persons aged 50–59 Years. Clin Infect Dis. 2012;54(7):922–928. doi:10.1093/cid/cir970
57. Willis ED, Woodward M, Brown E, et al. Herpes zoster vaccine live: A 10 year review of post-marketing safety experience. Vaccine. 2017;35(52):7231–7239. doi:10.1016/j.vaccine.2017.11.013
58. Gabutti G, Valente N, Sulcaj N, Stefanati A. Evaluation of efficacy and effectiveness of live attenuated zoster vaccine. J Prev Med Hyg. 2014;55(4):130–136.
59. Miller ER, Lewis P, Shimabukuro TT, et al. Post-licensure safety surveillance of zoster vaccine live (Zostavax®) in the United States, Vaccine Adverse Event Reporting System (VAERS), 2006–2015. Hum Vaccin Immunother. 2018;14(8):1963–1969. doi:10.1080/21645515.2018.1456598
60. Gagliardi AM, Gomes Silva BN, Torloni MR, Soares BG. Vaccines for preventing herpes zoster in older adults. In: Gagliardi AM, editor. Cochrane Database of Systematic Reviews. Vol. 10. Chichester, UK: John Wiley & Sons, Ltd; 2012:CD008858.
61. European Medicines Agency (EMA). SmPC Zostavax Available from: https://www.ema.europa.eu/en/documents/product-information/zostavax-epar-product-information_en.pdf.
62. Levin MJ, Schmader KE, Pang L, et al. Cellular and humoral responses to a second dose of Herpes Zoster vaccine administered 10 years after the first dose among older adults. J Infect Dis. 2016;213(1):14–22. doi:10.1093/infdis/jiv480
63. Reddy KP. Herpes Zoster vaccine: time for a boost? J Gen Intern Med. 2017;32(2):145–147. doi:10.1007/s11606-016-3885-x
64. Walker JL, Andrews NJ, Amirthalingam G, Forbes H, Langan SM, Thomas SL. Effectiveness of herpes zoster vaccination in an older United Kingdom population. Vaccine. 2018;36(17):2371–2377. doi:10.1016/j.vaccine.2018.02.021
65. Yun H, Xie F, Baddley JW, Winthrop K, Saag KG, Curtis JR. Longterm effectiveness of Herpes Zoster vaccine among patients with autoimmune and inflammatory diseases. J Rheumatol. 2017;44(7):1083–1087. doi:10.3899/jrheum.160685
66. Tseng HF, Luo Y, Shi J, et al. Effectiveness of Herpes Zoster vaccine in patients 60 years and older with end-stage renal disease. Clin Infect Dis. 2015;62(4):civ930. doi:10.1093/cid/civ930
67. Izurieta HS, Wernecke M, Kelman J, et al. Effectiveness and duration of protection provided by the live-attenuated Herpes Zoster vaccine in the medicare population ages 65 years and older. Clin Infect Dis. 2017;64(6):785–793. doi:10.1093/cid/ciw854
68. Zhang J, Xie F, Delzell E, et al. Association between vaccination for herpes zoster and risk of Herpes Zoster infection among older patients with selected immune-mediated diseases. JAMA. 2012;308(1):43–49. doi:10.1001/jama.2012.7304
69. Amirthalingam G, Andrews N, Keel P, et al. Evaluation of the effect of the herpes zoster vaccination programme 3 years after its introduction in England: a population-based study. Lancet Public Heal. 2018;3(2):e82–e90. doi:10.1016/S2468-2667(17)30234-7
70. Kawai K, Preaud E, Baron-Papillon F, Largeron N, Acosta CJ. Cost-effectiveness of vaccination against herpes zoster and postherpetic neuralgia: a critical review. Vaccine. 2014;32(15):1645–1653. doi:10.1016/j.vaccine.2014.01.058
71. European Commission, Commission implementing decision of 21.3.2018, granting marketing authorisation under Regulation (EC) No 726/2004 of the European Parliament and of the Council for “Shingrix - herpes zoster vaccine (recombinant, adjuvanted)”, a medicinal product for human use. Available from: https://ec.europa.eu/health/documents/community-register/2018/20180321140171/dec_140171_en.pdf.
72. Cunningham AL, Lal H, Kovac M, et al. Efficacy of the Herpes Zoster subunit vaccine in adults 70 years of age or older. N Engl J Med. 2016;375(11):1019–1032. doi:10.1056/NEJMoa1603800
73. Cunningham AL, Heineman TC, Lal H, et al. Immune responses to a recombinant glycoprotein E Herpes Zoster vaccine in adults aged 50 years or older. J Infect Dis. 2018;217(11):1750–1760. doi:10.1093/infdis/jiy095
74. Dendouga N, Fochesato M, Lockman L, Mossman S, Giannini SL. Cell-mediated immune responses to a varicella-zoster virus glycoprotein E vaccine using both a TLR agonist and QS21 in mice. Vaccine. 2012;30(20):3126–3135. doi:10.1016/j.vaccine.2012.01.088
75. Chlibek R, Bayas JM, Collins H, et al. Safety and Immunogenicity of an AS01-adjuvanted varicella-zoster virus subunit candidate vaccine against Herpes Zoster in adults ≥50 years of age. J Infect Dis. 2013;208(12):1953–1961. doi:10.1093/infdis/jit365
76. Chlibek R, Smetana J, Pauksens K, et al. Safety and immunogenicity of three different formulations of an adjuvanted varicella-zoster virus subunit candidate vaccine in older adults: A phase II, randomized, controlled study. Vaccine. 2014;32(15):1745–1753. doi:10.1016/j.vaccine.2014.01.019
77. Chlibek R, Pauksens K, Rombo L, et al. Long-term immunogenicity and safety of an investigational herpes zoster subunit vaccine in older adults. Vaccine. 2016;34(6):863–868. doi:10.1016/j.vaccine.2015.09.073
78. Schwarz TF, Volpe S, Catteau G, et al. Persistence of immune response to an adjuvanted varicella-zoster virus subunit vaccine for up to year nine in older adults. Hum Vaccin Immunother. 2018;14(6):1370–1377. doi:10.1080/21645515.2018.1442162
79. Grupping K, Campora L, Douha M, et al. Immunogenicity and safety of the HZ/su adjuvanted herpes zoster subunit vaccine in adults previously vaccinated with a live attenuated Herpes Zoster vaccine. J Infect Dis. 2017;216(11):1343–1351. doi:10.1093/infdis/jix482
80. Vink P, Shiramoto M, Ogawa M, et al. Safety and immunogenicity of a Herpes Zoster subunit vaccine in Japanese population aged ≥50 years when administered subcutaneously vs. intramuscularly. Hum Vaccin Immunother. 2017;13(3):574. doi:10.1080/21645515.2016.1232787
81. Lal H, Cunningham AL, Godeaux O, et al. Efficacy of an adjuvanted Herpes Zoster subunit vaccine in older adults. N Engl J Med. 2015;372(22):2087–2096. doi:10.1056/NEJMoa1501184
82. Kovac M, Lal H, Cunningham AL, et al. Complications of herpes zoster in immunocompetent older adults: incidence in vaccine and placebo groups in two large phase 3 trials. Vaccine. 2018;36(12):1537–1541. doi:10.1016/j.vaccine.2018.02.029
83. Stadtmauer EA, Sullivan KM, Marty FM, et al. A phase 1/2 study of an adjuvanted varicella-zoster virus subunit vaccine in autologous hematopoietic cell transplant recipients. Blood. 2014;124(19):2921–2929. doi:10.1182/blood-2014-04-573048
84. Berkowitz EM, Moyle G, Stellbrink H-J, et al. Safety and Immunogenicity of an adjuvanted Herpes Zoster subunit candidate vaccine in HIV-infected adults: a phase 1/2a randomized, placebo-controlled study. J Infect Dis. 2015;211(8):1279–1287. doi:10.1093/infdis/jiu606
85. Winston DJ, Mullane KM, Cornely OA, et al. Inactivated varicella zoster vaccine in autologous haemopoietic stem-cell transplant recipients: an international, multicentre, randomised, double-blind, placebo-controlled trial. Lancet. 2018;391(10135):2116–2127. doi:10.1016/S0140-6736(18)30631-7
86. Food and Drug Administration. FDA briefing document: Shingrix (Zoster Vaccine Recombinant, Adjuvanted).
87. Shimabukuro TT, Nguyen M, Martin D, DeStefano F. Safety monitoring in the Vaccine Adverse Event Reporting System (VAERS). Vaccine. 2015;33(36):4398–4405. doi:10.1016/j.vaccine.2015.07.035
88. Hesse EM, Shimabukuro TT, Su JR, et al. Postlicensure safety surveillance of recombinant Zoster vaccine (Shingrix) - United States, October 2017-June 2018. MMWR Morb Mortal Wkly Rep. 2019;68(4):91–94. doi:10.15585/mmwr.mm6804a4
89. Le P, Rothberg MB. Determining the optimal vaccination schedule for Herpes Zoster: a cost-effectiveness analysis. J Gen Intern Med. 2017;32(2):159–167. doi:10.1007/s11606-016-3844-6
90. de Boer PT, van Lier A, de Melker H, et al. Cost-effectiveness of vaccination of immunocompetent older adults against herpes zoster in the Netherlands: a comparison between the adjuvanted subunit and live-attenuated vaccines. BMC Med. 2018;16(1):228. doi:10.1186/s12916-018-1213-5
91. Van Oorschot D, Anastassopoulou A, Poulsen Nautrup B, et al. Cost-effectiveness of the recombinant zoster vaccine in the German population aged ≥60 years old. Hum Vaccin Immunother. 2019;15(1):34–44. doi:10.1080/21645515.2018.1509645
92. You JHS, Ming W, Tsang OT, Chan PK. Optimal gender-specific age for cost-effective vaccination with adjuvanted herpes zoster subunit vaccine in Chinese adults. van Wouwe JP, ed. PLoS One. 2019;14(1):e0210005. doi:10.1371/journal.pone.0210005
93. Curran D, Patterson BJ, Van Oorschot D, et al. Cost-effectiveness of an adjuvanted recombinant Zoster vaccine in older adults in the United States who have been previously vaccinated with Zoster vaccine live. Hum Vaccin Immunother. 2019;15(4):765–771.
94. Kroger AT, Vázquez M. General Best Practice Guidelines for Immunization. Best Practices Guidance of the Advisory Committee on Immunization Practices (ACIP). Available from: https://www.cdc.gov/vaccines/hcp/acip-recs/general-recs/index.html. Published 2011.
95. Schwarz TF, Aggarwal N, Moeckesch B, et al. Immunogenicity and safety of an adjuvanted Herpes Zoster subunit vaccine coadministered with seasonal influenza vaccine in adults aged 50 years or older. J Infect Dis. 2017;216(11):1352–1361. doi:10.1093/infdis/jix481
96. WHO. Requirements for varicella vaccine (live), WHO Technical Report Series, No. 848. Available from: http://www.who.int/biologicals/publications/trs/areas/vaccines/varicella/WHO_TRS_848_A1.pdf. Published 1994.
97. Oh SH, Choi EH, Shin SH, et al. Varicella and varicella vaccination in South Korea. Clin Vaccine Immunol. 2014;21(5):762–768. doi:10.1128/CVI.00645-13
98. CDC. Chickenpox [www.cdc.gov]; 2018. Available from: https://www.cdc.gov/chickenpox/hcp/index.html#vaccination-impact.
99. Seward JF, Watson BM, Peterson CL, et al. Varicella disease after introduction of varicella vaccine in the United States, 1995-2000. JAMA. 2002;287(5):606–611. doi:10.1001/jama.287.5.606
100. Prevention of Varicella: Recommendations of the Advisory Committee on Immunization Practices (ACIP). Available from: https://www.cdc.gov/mmwr/preview/mmwrhtmL/rr5604a1.htm.
101. Banz K, Iseli A, Aebi C, Brunner M, Schmutz AM, Heininger U. Economic evaluation of varicella vaccination in Swiss children and adolescents. Hum Vaccin. 2009;5(12):847–857. doi:10.4161/hv.9898
102. Holl K, Sauboin C, Amodio E, Bonanni P, Gabutti G. Coverage, efficacy or dosing interval: which factor predominantly influences the impact of routine childhood vaccination for the prevention of varicella? A model-based study for Italy. BMC Public Health. 2016;16(1):1103. doi:10.1186/s12889-016-3738-x
103. Wutzler P, Bonanni P, Burgess M, Gershon A, Sáfadi MA, Casabona G. Varicella vaccination - the global experience. Expert Rev Vaccines. 2017;16(8):833–843. doi:10.1080/14760584.2017.1343669
104. ECDC. Varicella vaccination in the European Union. Available from: https://ecdc.europa.eu/en/varicella. Published 2015.
105. Law-Decree 7 June 2017, N. 73. Disposizioni Urgenti in Materia Di Prevenzione Vaccinale. [Urgent Dispositions regarding Vaccination Prevention]. Italy: GU serie generale n.130 del 7-06-2017. Italian.
106. Thiry N, Beutels P, Van Damme P, Van Doorslaer E. Economic evaluations of varicella vaccination programmes. Pharmacoeconomics. 2003;21(1):13–38. doi:10.2165/00019053-200321010-00002
107. Brisson M, Racine E, Drolet M. The Potential Impact of Varicella Vaccination in Low to Middle Income Countries : A Feasibility Modeling Study Report to the SAGE Working Group on Varicella and Herpes Zoster Vaccines. Available from: https://www.who.int/immunization/sage/meetings/2014/april/5_the_potential_impact_varicella_vaccination_low_middle_income_countries_feasibility_modeling.pdf?ua=1. Accessed March 7, 2019.
108. Edmunds WJ, Brisson M. The effect of vaccination on the epidemiology of varicella Zoster virus. J Infect. 2002;44(4):211–219. doi:10.1053/jinf.2002.0988
109. Brisson M, Edmunds WJ, Gay NJ, Law B, De Serres G. Modelling the impact of immunization on the epidemiology of varicella zoster virus. Epidemiol Infect. 2000;125(3):651–669. doi:10.1017/S0950268800004714
110. Thomas SL, Wheeler JG, Hall AJ. Contacts with varicella or with children and protection against herpes zoster in adults: a case-control study. Lancet. 2002;360(9334):678–682.
111. Marin M, Meissner HC, Seward JF. Varicella prevention in the United States: a review of successes and challenges. Pediatrics. 2008;122(3):e744–e751. doi:10.1542/peds.2008-0567
112. Guris D, Jumaan AO, Mascola L, et al. Changing varicella epidemiology in active surveillance sites—united States, 1995–2005. J Infect Dis. 2008;197(s2):S71–S75.
113. Tanuseputro P, Zagorski B, Chan KJ, Kwong JC. Population-based incidence of herpes zoster after introduction of a publicly funded varicella vaccination program. Vaccine. 2011;29(47):8580–8584. doi:10.1016/j.vaccine.2011.09.024
114. Toyama N, Shiraki K. Universal varicella vaccination increased the incidence of herpes zoster in the child-rearing generation as its short-term effect. J Dermatol Sci. 2018;92(1):89–96. doi:10.1016/j.jdermsci.2018.07.003
115. Gershon AA. Is chickenpox so bad, what do we know about immunity to varicella zoster virus, and what does it tell us about the future? J Infect. 2017;74(Suppl 1):S27–S33. doi:10.1016/j.jinf.2016.12.016
116. Marchetti S, Guzzetta G, Flem E, Mirinaviciute G, Scalia Tomba G, Manfredi P. Modeling the impact of combined vaccination programs against varicella and herpes zoster in Norway. Vaccine. 2018;36(8):1116–1125. doi:10.1016/j.vaccine.2018.01.038
117. CDC. CDC′s advisory committee recommends “Shingles” vaccination, press release. Available from: https://www.cdc.gov/media/pressrel/r061026.htm. Published 2006.
118. Lu P-J, O’Halloran A, Williams WW, Harpaz R. National and State-Specific Shingles Vaccination Among Adults Aged ≥60 Years. Am J Prev Med. 2017;52(3):362–372. doi:10.1016/j.amepre.2016.08.031
119. Herpes Zoster (Shingles) Vaccine: Canadian Immunization Guide - Canada.ca. Available from: https://www.canada.ca/en/public-health/services/publications/healthy-living/canadian-immunization-guide-part-4-active-vaccines/page-8-herpes-zoster-(shingles)-vaccine.html.
120. EMA. Zostavax | European Medicines Agency. Available from: https://www.ema.europa.eu/en/medicines/human/EPAR/zostavax. Published 2016.
121. ECDC. ECDC vaccine scheduler. Avaolable from: https://vaccine-schedule.ecdc.europa.eu/Scheduler/ByDisease?SelectedDiseaseId=51&SelectedCountryIdByDisease=−1.
122. Robert Koch Institut - Impfungen A-Z - Gürtelrose (Herpes zoster) [Robert Koch Institut - Vaccinations A-Z - Shingles (Herpes Zoster)]. Avalaible from: https://www.rki.de/SharedDocs/FAQ/Herpes_zoster/FAQ-Liste.html?nn=2375548.
123. Italian Ministry of Health. Piano Nazionale Prevenzione Vaccinale 192017–2019. [National vaccinal prevention plan 2017-2019]. Available from: http://www.salute.gov.it/portale/documentazione/p6_2_2_1.jsp?lingua=italiano&id=2571.
124. Bundesministerium für Arbeit Soziales Gesundheit und Konsumentenschutz. Impfplan Österreich 2019, Version 1. [Austrian Vaccination Plan 2019, version 1]. Available from: https://www.sozialministerium.at/site/Gesundheit/Krankheiten_und_Impfen/Impfen/Oesterreichischer_Impfplan_2019.
125. National Immunisation Program Schedule | Australian Government Department of Health. Available from: https://beta.health.gov.au/health-topics/immunisation/immunisation-throughout-life/national-immunisation-program-schedule.
126. New Zealand Ministry of Health. Immunisation Handbook 2017. Available from: https://www.health.govt.nz/publication/immunisation-handbook-2017. Published 2018.
127. Hoshi S, Kondo M, Okubo I. Cost-effectiveness of varicella vaccine against herpes zoster and post-herpetic neuralgia for elderly in Japan. Vaccine. 2017;35(24):3264–3271. doi:10.1016/j.vaccine.2017.04.046
128. National Institute of Infectious Diseases. 日本の予防接種スケジュール. [Japan vaccination schedule]. Avalaible from: https://www.niid.go.jp/niid/ja/vaccine-j/2525-v-schedule.html.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.