")
Back to Journals » Cancer Management and Research » Volume 12
Value of Visceral Fat Area in the Preoperative Discrimination of Peritoneal Metastasis from Gastric Cancer in Patients with Different Body Mass Index: A Prospective Study
Authors Huang H, Yang X, Sun J, Zhu C, Wang X, Zeng Y, Xu J , Mao C , Shen X
Received 12 April 2020
Accepted for publication 27 June 2020
Published 28 July 2020 Volume 2020:12 Pages 6523—6532
DOI https://doi.org/10.2147/CMAR.S257849
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ahmet Emre Eşkazan
He Huang,1,* Xinxin Yang,2,* Jing Sun,2,* Ce Zhu,2 Xiang Wang,2 Yunpeng Zeng,2 Jingxuan Xu,2 Chenchen Mao,2 Xian Shen2,3
1Department of General Surgery, The Second Affiliated Hospital, Wenzhou Medical University, Wenzhou, Zhejiang, People’s Republic of China; 2Department of Gastrointestinal Surgery, The Second Affiliated Hospital, Wenzhou Medical University, Wenzhou, Zhejiang, People’s Republic of China; 3Department of Gastrointestinal Surgery, The First Affiliated Hospital, Wenzhou Medical University, Wenzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chenchen Mao; Xian Shen
Department of Gastrointestinal Surgery, The Second Affiliated Hospital, Wenzhou Medical University, No. 109 West College Road, Wenzhou, Zhejiang Province, People’s Republic of China
Tel +86 577 8800 2709
Email [email protected]; [email protected]
Purpose: Although peritoneal metastasis (PM) is associated with poor prognosis in gastric cancer (GC) patients, it is difficult to discriminate preoperatively. Our previous study has demonstrated visceral fat area (VFA) is a better obesity index than body mass index (BMI) in predicting abdominal metastasis. This study aimed to further explore the relationship between obesity and PM.
Patients and Methods: VFA was retrieved for 859 consecutive patients undergoing radical gastrectomy between January 1, 2009, and December 31, 2013. A receiver operating characteristic curve analysis was used to determine the BMI-specific cutoff values for VFA. Univariate and multivariate analyses evaluating the risk factors for PM at different BMI levels were performed.
Results: The optimal cutoff values for VFA were 67.28, 88.03, and 175.32 cm2 for low, normal, and high BMI patients, respectively, and 18 (15.52%), 220 (40.15%), and 61 (31.28%) patients were classified as having high VFA in each group. Univariate logistic regression revealed that the association between high VFA and PM was not dependent on BMI (odds ratio [OR]=9.048, P=0.007 for low BMI, OR=3.827, P< 0.001 for normal BMI, and OR=2.460, P=0.049 for high BMI). In multivariate logistic regression analysis, high VFA (OR=3.816, P< 0.001) and vascular invasion (OR=1.951, P=0.039) were independent risk factors for PM only in the normal BMI group.
Conclusion: VFA only effectively predicted PM for GC patients with normal BMI, rather than those with low and high BMI. More attentions should be paid to those GC patients with high VFA and normal BMI.
Keywords: gastric cancer, peritoneal metastasis, obesity, visceral fat area, body mass index
Introduction
Gastric cancer (GC) is the fourth most common cancer worldwide and the third leading cause of cancer-related deaths (723,000 deaths) worldwide.1,2 Most GC patients do not succumb to their primary tumor but instead to peritoneal metastasis (PM), which is common in advanced gastric cancer,3 but is even more apparent after the primary lesion has been removed.4 Nearly 50% of the deaths due to GC could be ascribed to PM5 and patients with PM of GC experience poorer prognosis with a median survival of 4–7 months.6,7 However, PM in GC may remain asymptomatic for a long period in most cases6 and is detected in only 14% of GC patients at initial examination8 and is often initially diagnosed intraoperatively, which is not ideal for surgeons to determine the most appropriate therapeutic approach. Thus, it is essential to develop effective methods to discriminate patients at a high risk of PM promptly.
Recently, obesity has also been recognized as an independent risk factor for several cancers.9 It is reported that nearly 40% of all cancers can be attributed to overweight and obesity.10 In particular, over 60% of endometrial, postmenopausal breast and colorectal cancers have been attributed to obesity.11,12 However, obesity characterized by body mass index (BMI) is only a measure of general adiposity and may not fully quantify the role of visceral adiposity in cancer risk. Moreover, visceral adipose tissue is increasingly recognized as an endocrine organ that synthesizes obesity-mediated hormones and cytokines which have been directly implicated in cancer risk.13 Furthermore, visceral fat area (VFA) has been demonstrated to be more strongly associated with postoperative complications such as incisional hernia14 and postsurgical gastroparesis syndrome15 after gastrointestinal operation than elevated BMI.
Similarly, our previous study also found that VFA was a more useful indicator of PM risk than BMI.16 In this study, we evaluated the predictive value of the VFA for PM in gastric cancer patients with different BMI levels, and further explore the relationship between obesity and PM, via screening of patients at high risk of PM preoperatively.
Patients and Methods
Study Design and Patient Population
All patients who underwent radical gastrectomy at the Gastrointestinal Surgical Department, Second Affiliated Hospital of Wenzhou Medical University and the First Affiliated Hospital of Wenzhou Medical University in China between January 1, 2009, and December 31, 2013, were identified. Demographic information and operative details were prospectively collected and patients were grouped according to their BMI into “low BMI (BMI <18.5 kg/m2),” “normal BMI (BMI 18.5–24 kg/m2),” and “high BMI (BMI ≥24 kg/m2)” groups. All participants provided written informed consent prior to study participation. This project was approved by the Ethical Review Board of the Second Affiliated Hospital of Wenzhou Medical University.
Inclusion/Exclusion Criteria
All adult patients who met the following criteria were included for analysis: (a) histopathologically confirmed gastric adenocarcinoma and planned to receive radical gastrectomy; (b) adult patients (18 years of age or older); (c) had abdominal-computed tomography (CT) image within 1 month before surgery; (d) signed informed consent and agreed to participate in this study. The exclusion criteria included patients who: (a) lacked preoperative abdominal-computed tomography (CT) image (performed CT in other hospitals); (b) lacked the data on weight or height needed to calculate BMI; (c) had cancer metastasis which could not be cured during surgery; (d) patients who had undergone partial gastrectomy with remnant GC. Operation were performed routinely following the Japanese Gastric Cancer Treatment Guidelines 2010 (version 3).
Diagnosis of PM
PM was diagnosed according to the criteria of the Japanese Classification of Gastric Cancer (15th edition): metastases were limited to the greater omentum, lesser omentum, anterior lobe of the transverse mesocolon, pancreatic capsule, and spleen and metastasis in the upper abdominal peritoneum (visceral peritoneum above the transverse position and parietal peritoneum above the umbilicus). PM was diagnosed from intraoperative frozen sections and postoperative diagnostic pathology.
VFA Measurement
As mentioned above, all patients received abdominal CT scan preoperatively. The umbilicus level imaging was selected for measurement from the Picture Archiving and Communication System (PACS). The Hounsfield scale was used to distinguish adipose tissue from other tissues; here, adipose tissue was defined as within the range of −140 to −50 Hounsfield units (HU). The total fat area was calculated using a dedicated processing system (version 3.0.11.3, BN17 32-bit; INFINITT Healthcare Co., Ltd., Seoul, South Korea).
Cutoff Point for VFA
We determined the cutoff point for VFA as the maximal Youden index value on a receiver operating characteristic (ROC) curve. Patients in each subgroup were then divided into two groups based on this cutoff point—the “high VFA group” and the “low VFA group.”
Statistical Analysis
The Kolmogorov–Smirnov test was performed to assess the distribution equality of continuous parameters. Normally distributed data are presented as mean ± standard deviation (SD), whereas non-normally distributed data are presented as medians and interquartile ranges (IQRs). Continuous normally distributed data were compared using t-test while Mann–Whitney U-test was used for continuous, non-normally distributed data. Categorical data were compared using the chi-squared test or Fisher’s exact test. Univariate logistic regression analysis of all potential baseline predictors was performed to compute the odds ratios (ORs) with their 95% confidence intervals (CIs). Variables with a trend (P<0.05) in the univariate analysis were selected as potential parameters, and then, a forward stepwise variable selection was used to establish a multivariable logistic regression model. All P-values were two-sided, and P<0.05 was considered statistically significant. All statistical analyses were performed using SPSS software (version 22.0; SPSS Inc., Chicago, IL, USA) and R software (version 3.0.1; http://www.Rproject.org).
Results
An overview of the patient population is provided in Table 1. A total of 859 patients met the inclusion criteria and were enrolled in the analysis and 87 (10.13%) patients were diagnosed with PM as per the criteria mentioned above. The mean age of the patients was 63.63±11.28 years and majority of them were men (672, 78.23%). The mean VFA and tumor size of the patients were 89.60±60.91 cm2 and 3.88±2.23 cm, respectively. Other Clinical and demographic characteristics of the cohort have been reported in our previous study.
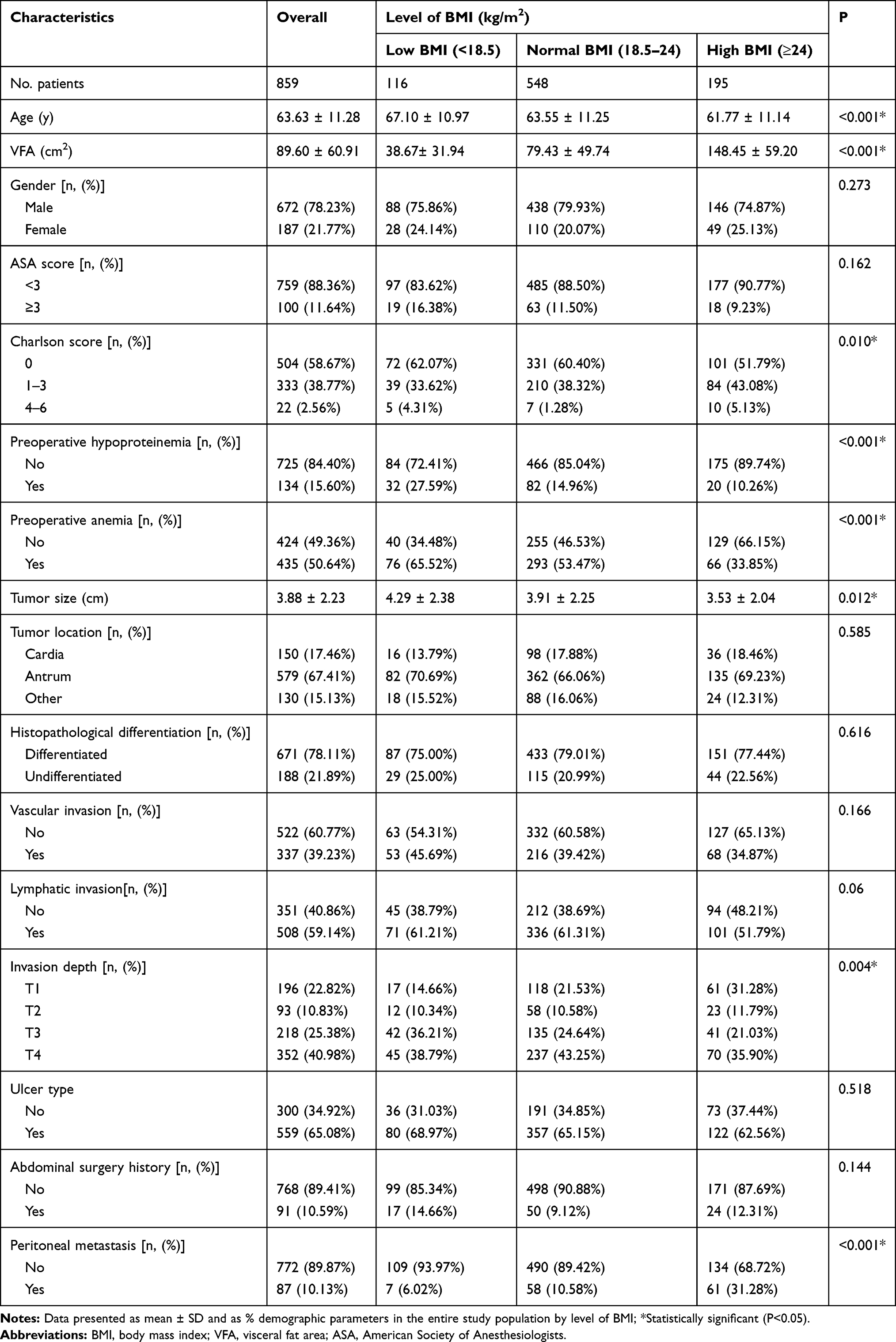 |
Table 1 Characteristics of the Patients |
Clinical and Demographic Characteristics in Different BMI Groups
Patients were subdivided into low BMI group (BMI <18.5 kg/m2), normal BMI group (BMI 18.5–24 kg/m2) and high BMI group (BMI ≥24 kg/m2), and each group contained 116, 548, and 195 patients, respectively. As shown in Table 1, patients in the low BMI group were older (P<0.001) and more likely to have lower VFA (P<0.001) and larger tumor size (P=0.012) compared to those in the normal and high BMI groups. Univariate associations were found between BMI level and some clinical and demographic characteristics. The rates for preoperative hypoproteinemia (P<0.001) and preoperative anemia (P<0.001) decreased with an increasing level of BMI. Higher Charlson score (P=0.010) were found with increasing BMI. Additionally, there were also significant differences in Invasion depth between different BMI groups (P=0.004). The frequency of PM was significantly higher among patients with high BMI compared to those with low and normal (31.28% vs 6.02% vs 10.58%, respectively, P<0.001).
VFA Characteristics
The overview of the VFA level in different BMI groups is shown in Figure 1. Patients with PM of GC had a significantly higher VFA in the normal BMI group (P<0.001) and in high BMI group (P=0.030) compared to those without PM. Although no statistical significance was found, patients with PM were more likely to have higher VFA than those without in the low BMI group.
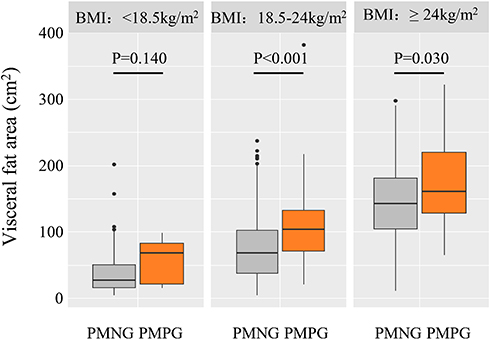 |
Figure 1 Distribution of VFA between PM and non-PM in different BMI groups. |
Cutoff Values for VFA in Different BMI Groups
According to the study including criteria, 116 of low BMI patients, 548 of normal BMI patients and 195 of high BMI patients were subdivided (Table 1). ROC curves of VFA were used to identify PM in each of the three groups, and the AUC were 0.658, 0.616, and 0.685 (Figure 2), respectively. The optimal cutoff values for VFA were 67.28, 88.03, and 175.32 cm2 for patients with low, normal and high BMI, respectively. Using these cutoff values, 18 (15.52%), 220 (40.15%), and 61 (31.28%) patients were classified as high VFA in each group.
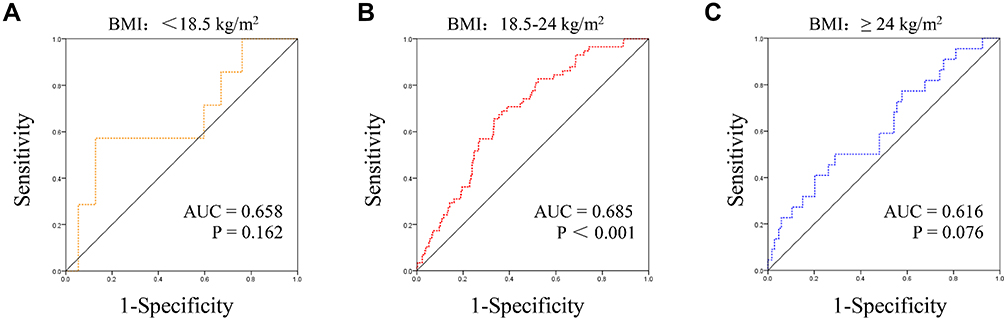 |
Figure 2 ROC curves to identify PM in different BMI groups. The area under the ROC curve (AUC) values for VFA were shown. (A) ROC curve in low BMI group. (B) ROC curve in normal BMI group. (C) ROC curve in high BMI group. |
Association Between Clinical and Demographic Characteristics and PM in Different BMI Groups
As shown in Table 2, PM was associated with high VFA (P=0.007), histopathological differentiation (P=0.012), and abdominal surgery history (P=0.046) in the low BMI cohort in univariate analysis. However, in multivariate logistic regression analysis, none of the three characteristics achieved statistical significance. In contrast, the univariate analysis identified VFA (P<0.001), tumor size (P=0.016), vascular invasion (P<0.001), lymphatic invasion (P=0.001), and invasion depth (P=0.376 for T2, P=0.011 for T3, and P=0.002 for T4) as factors that correlated significantly with PM in normal BMI patients. Subsequent multivariate logistic regression analysis identified VFA (OR=3.816, P<0.001) and vascular invasion (OR=1.951, P=0.039) as independent risk factors for PM. For the high BMI group, VFA (P=0.049), Charlson score (P=0.030), tumor size (P=0.001), vascular invasion (P<0.001), lymphatic invasion (P=0.043), invasion depth (P=0.163 for T2, P=0.021 for T3, and P=0.017 for T4), and abdominal surgery history (P=0.030) were statistically significant in the univariate analysis, and only vascular invasion (OR=4.460, P=0.028) and abdominal surgery history (OR=5.321, P=0.023) were independent predictors of PM in multivariate logistic regression analysis.
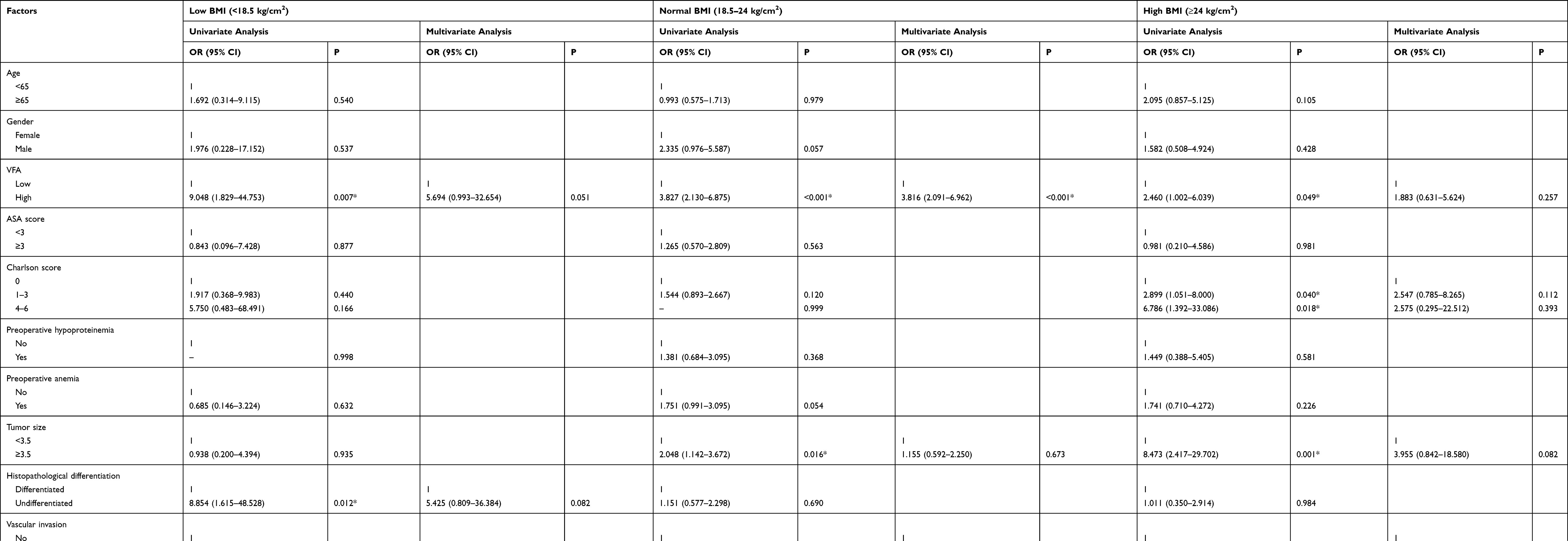 |
Table 2 Univariate and Multivariate Analyses to Evaluate Potential Predictive Factors for Peritoneal Metastasis in Patients with Different BMI Levels |
Discussion
Overweight and obesity are important lifestyle-related public health problems in the world,17 and the number of overweight or obese people has already surpassed the number of underweight people for the first time according to recent studies.18 In the literature, overweight and obesity is usually determined using the easily calculated BMI. BMI is classified as normal (BMI <25 kg/m2), overweight (BMI 25–30 kg/m2), and obese (BMI ≥30 kg/m2) according to the WHO standard.19 In this study, the Chinese standard20,21 was used and BMI was classified as low (BMI <18.5 kg/m2), normal (BMI 18.5–24 kg/m2), high (BMI ≥24 kg/m2), as all the patients enrolled were Chinese.
Recently, increasing attention has been paid to VFA and BMI as obesity indexes. Previous studies found VFA to be superior to BMI in accurately and effectively predicting the effect of obesity on adverse postoperative outcomes22–24 after radical colectomy as well as radical gastrectomy. However, all the studies focused on the comparison of two indications and whether VFA is a better parameter than BMI remains controversial. Similarly, our previous study also only demonstrated that VFA was superior to BMI in predicting PM based on the direct comparison of two variables; thus, we designed this prospective cohort study with the aim of investigating the role of VFA for PM after eliminating BMI differences. To the best of our knowledge, this is the first prospective cohort study focusing on this contentious question.
Despite the controversy of which is better, both VFA and BMI are obesity parameters. There was a positive correlation between BMI and VFA in general in the study although patients with a high BMI may not have a high VFA. Considering that patients were subdivided according to the BMI, the cutoff value for VFA in the previous study was inappropriate for the overall patients. We thus performed ROC curve analysis in all the three BMI groups and cutoff values of 67.28 cm2, 88.03 cm2 and 175.32 cm2, respectively, were defined for high VFA, which was quite different from our previous work.16 However, there is still a lack of consensus on the VFA cutoff for Chinese and VFA cutoff varies from study to study.25,26 Using these cutoffs, 15.52%, 40.15%, 31.28% of patients in our cohort met this definition of high VFA, and these high VFA patients were more likely to develop PM than low VFA patients.
We further confirmed that high VFA was an independent risk factor for PM in the normal BMI group. This may be partly because of the state of low-grade chronic inflammation of adipose tissue in obesity. By generating reactive oxygen species (ROS), which have mitogenic properties at low concentrations, tumor further progressed.27,28 On the other hand, insulin resistance in obese patients may promotes secretion of IGF-1 and thus promote mitogenic and proangiogenic pathways and inhibit apoptosis, consequently cause a majority of the proliferative effects and promote tumor development and metastasis.29 However, no such results were found in the low and high BMI groups. For patients with low BMI, only 15.52% of the patients were determined as high VFA. Combined with the low incidence of PM (6.02%, 7 in 116) in this group, even no factor was found to be independently associated with PM in the multivariate analysis, which may be attributed to statistical bias to some extent. For high VFA patients, the incidence of the PM in the study was the highest (31.28%, 61 in 195), which was also apparently higher than that reported in other studies.30,31 However, the prediction of VFA for PM may be severely weakened by the high BMI of the population.
Many studies have focused on evaluating the PM status in gastric cancers.31–33 Despite the poor overall sensitivity,34 CT is still the most common tool for detecting PM before operation. Although a previous study16 already demonstrated the relationship between VFA and PM, this study also found VFA was relevant only in normal BMI patients. As an abdominal CT scan is routinely performed as a common test for preoperative evaluation, the development of software technology also makes VFA measurements easier. Thus, more attentions should be paid to high VFA patients, especially for high VFA and normal BMI patients.
This study has some limitations. First, our study sample size was small, 87 patients were diagnosed with PM and only 7 PM patients were found in the low BMI group, which may seriously affect the accuracy of the analysis. Second, this was a single-center study, and most of the patients came from Southeast China; thus, the findings may not be generalizable to other settings. As body shape is inherently different between locations and races, our results need to be validated by further studies from other medical centers. Third, although ROC curves are appropriate for establishing VFA cutoff values in each group, a standardized cutoff value is urgently needed. Finally, a randomized clinical trial was needed to further confirm that whether reduce VFA can decrease the risk of peritoneal metastasis in GC patients with normal BMI.
Conclusion
Our previous study demonstrated VFA is a better obesity index than BMI in predicting abdominal metastasis. This study further determined the relationship between VFA and PM of GC across patients with different BMI levels. We found that GC patients with high VFA in and normal BMI were at higher risk of PM compared to those with low or high BMI. Thus, more attention should also be paid to GC patients with high VFA and normal BMI.
Abbreviation
VFA, visceral fat area; GC, gastric cancer; PM, peritoneal metastasis; BMI, body mass index; OR, odds ratio; CT, computed tomography; PACS, picture archiving and communication system; HU, Hounsfield units; ROC, receiver operating characteristic; SD, standard deviation; CI, confidence interval; IOR, interquartile range; AUC, area under curve; ROS, reactive oxygen species.
Acknowledgments
We thank Editage Group for polishing the draft of this manuscript.
Disclosure
All of the authors declare no conflict of interests.
References
1. Torre LA, Bray F, Siegel RL, et al. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65(2):87–108. doi:10.3322/caac.21262
2. Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136(5):E359–86. doi:10.1002/ijc.29210
3. Qin R, Yang Y, Qin W, et al. The value of serum immunoglobulin g glycome in the preoperative discrimination of peritoneal metastasis from advanced gastric cancer. J Cancer. 2019;10(12):2811–2821. doi:10.7150/jca.31380
4. Wang C, Shi M, Ji J, et al. A self-enforcing HOXA11/Stat3 feedback loop promotes stemness properties and peritoneal metastasis in gastric cancer cells. Theranostics. 2019;9(25):7628–7647. doi:10.7150/thno.36277
5. Maehara Y, Hasuda S, Koga T, et al. Postoperative outcome and sites of recurrence in patients following curative resection of gastric cancer. Br J Surg. 2000;87(3):353–357. doi:10.1046/j.1365-2168.2000.01358.x
6. Glockzin G, Piso P. Current status and future directions in gastric cancer with peritoneal dissemination. Surg Oncol Clin N Am. 2012;21(4):625–633. doi:10.1016/j.soc.2012.07.002
7. Rau B, Brandl A, Piso P, et al. Peritoneal metastasis in gastric cancer: results from the German database. Gastric Cancer. 2020;23:11–22. doi:10.1007/s10120-019-00978-0
8. Thomassen I, van Gestel YR, van Ramshorst B, et al. Peritoneal carcinomatosis of gastric origin: a population-based study on incidence, survival and risk factors. Int J Cancer. 2014;134(3):622–628. doi:10.1002/ijc.28373
9. Lega IC, Lipscombe LL. Review: diabetes, obesity and cancer - pathophysiology and clinical implications. Endocr Rev. 2020;41:33–52. doi:10.1210/endrev/bnz014
10. Keum N, Greenwood DC, Lee DH, et al. Adult weight gain and adiposity-related cancers: a dose-response meta-analysis of prospective observational studies. J Natl Cancer Inst. 2015;107(2). doi:10.1093/jnci/djv088
11. Arnold M, Pandeya N, Byrnes G, et al. Global burden of cancer attributable to high body-mass index in 2012: a population-based study. Lancet Oncol. 2015;16(1):36–46. doi:10.1016/S1470-2045(14)71123-4
12. Lopez-Suarez A. Burden of cancer attributable to obesity, type 2 diabetes and associated risk factors. Metabolism. 2019;92:136–146. doi:10.1016/j.metabol.2018.10.013
13. Avgerinos KI, Spyrou N, Mantzoros CS, et al. Obesity and cancer risk: emerging biological mechanisms and perspectives. Metabolism. 2019;92:121–135. doi:10.1016/j.metabol.2018.11.001
14. Aquina CT, Rickles AS, Probst CP, et al. Visceral obesity, not elevated BMI, is strongly associated with incisional hernia after colorectal surgery. Dis Colon Rectum. 2015;58(2):220–227. doi:10.1097/DCR.0000000000000261
15. Chen XD, Mao -C-C, Zhang W-T, et al. A quantified risk-scoring system and rating model for postsurgical gastroparesis syndrome in gastric cancer patients. J Surg Oncol. 2017;116(4):533–544. doi:10.1002/jso.24691
16. Chen X, Chen W, Huang Y, et al. A quantified risk-scoring system including the visceral fat area for peritoneal metastasis of gastric cancer. Cancer Manag Res. 2019;11:2903–2913. doi:10.2147/CMAR.S194356
17. Davis GJ. Guidelines for healthy weight. N Engl J Med. 1999;341(27):2097–2098.
18. Risk NC. Factor collaboration (Ncd-RisC). Trends in adult body-mass index in 200 countries from 1975 to 2014: a pooled analysis of 1698 population-based measurement studies with 19.2 million participants. Lancet. 2016;387(10026):1377–1396. doi:10.1016/S0140-6736(16)30054-X
19. World Health Organization. Obesity: Preventing and Managing the Global Epidemic. Report of a WHO Consultation. Vol. 894. World Health Organization; 2000:
20. Zhou BF, Cooperative Meta-Analysis Group of the Working Group on Obesity in China. Predictive values of body mass index and waist circumference for risk factors of certain related diseases in Chinese adults–study on optimal cut-off points of body mass index and waist circumference in Chinese adults. Biomed Environ Sci. 2002;15(1):83–96.
21. Chen CM. Overview of obesity in Mainland China. Obes Rev. 2008;9(Suppl 1):14–21. doi:10.1111/j.1467-789X.2007.00433.x
22. Yang SJ, Li HR, Zhang WH, et al. Visceral fat area (VFA) superior to BMI for predicting postoperative complications after radical gastrectomy: a prospective cohort study. J Gastrointest Surg. 2019:1–9.
23. Zhai T-S, Kang Y, Ren WH, et al. Elevated visceral fat area is associated with adverse postoperative outcome of radical colectomy for colon adenocarcinoma patients. ANZ J Surg. 2019;89(9):E368–E372. doi:10.1111/ans.15283
24. Liu Y, Guo D, Niu Z, et al. Prediction of the risk of laparoscopy-assisted gastrectomy by comparing visceral fat area and body mass index. Gastroenterol Res Pract. 2018;2018:1359626. doi:10.1155/2018/1359626
25. Examination Committee of Criteria for ‘Obesity Disease’ in Japan. New criteria for ‘obesity disease’ in Japan. Circ J. 2002;66(11):987–992. doi:10.1253/circj.66.987
26. Zhou CJ, Cheng YF, Xie LZ, et al. Metabolic syndrome, as defined based on parameters including visceral fat area, predicts complications after surgery for rectal cancer. Obes Surg. 2020;30:319–326.
27. Ziech D, Franco R, Pappa A, et al. Reactive oxygen species (ROS)–induced genetic and epigenetic alterations in human carcinogenesis. Mutat Res. 2011;711(1–2):167–173. doi:10.1016/j.mrfmmm.2011.02.015
28. Kim YJ, Kim EH, Hahm KB. Oxidative stress in inflammation-based gastrointestinal tract diseases: challenges and opportunities. J Gastroenterol Hepatol. 2012;27(6):1004–1010. doi:10.1111/j.1440-1746.2012.07108.x
29. Samani AA, Yakar S, LeRoith D, et al. The role of the IGF system in cancer growth and metastasis: overview and recent insights. Endocr Rev. 2007;28(1):20–47.
30. Kim M, Jeong WK, Lim S, et al. Gastric cancer: development and validation of a CT-based model to predict peritoneal metastasis. Acta Radiol. 2020;61:732–742.
31. Liu S, He J, Liu S, et al. Radiomics analysis using contrast-enhanced CT for preoperative prediction of occult peritoneal metastasis in advanced gastric cancer. Eur Radiol. 2020;30:239–246.
32. Chang DK, Kim JW, Kim BK, et al. Clinical significance of CT-defined minimal ascites in patients with gastric cancer. World J Gastroenterol. 2005;11(42):6587–6592. doi:10.3748/wjg.v11.i42.6587
33. Yan C, Zhu Z-G, Yan M, et al. [Value of multidetector-row CT in the preoperative prediction of peritoneal metastasis from gastric cancer: a single-center and large-scale study]. Zhonghua Wei Chang Wai Ke Za Zhi. 2010;13(2):106–110.
34. Wang Z, Chen JQ. Imaging in assessing hepatic and peritoneal metastases of gastric cancer: a systematic review. BMC Gastroenterol. 2011;11:19. doi:10.1186/1471-230X-11-19
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.