")
Back to Journals » OncoTargets and Therapy » Volume 8
Value of detection of serum human epididymis secretory protein 4 and carbohydrate antigen 125 in diagnosis of early endometrial cancer of different pathological subtypes
Authors Liu X, Zhao F, Hu L, Sun Y
Received 29 January 2015
Accepted for publication 16 March 2015
Published 26 May 2015 Volume 2015:8 Pages 1239—1243
DOI https://doi.org/10.2147/OTT.S81853
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Daniele Santini
Xingui Liu,1 Fengting Zhao,2 Linli Hu,1 Yingpu Sun1
1Reproductive Medical Center of the First Affiliated Hospital, Zhengzhou University, Zhengzhou, Henan, People’s Republic of China; 2Clinical Laboratory, the First Affiliated Hospital, Zhengzhou University, Zhengzhou, Henan, People’s Republic of China
Abstract: This study explored the value of detection of human epididymis secretory protein 4 (HE4) and carbohydrate antigen 125 (CA125) from serum in diagnosis of early endometrial cancer of different pathological subtypes and discussed the mechanism of HE4 and CA125 in diagnosis. In this study, enzyme-linked immunosorbent assay and chemiluminescent immunoassay were used to detect HE4 and CA125 from serum in endometrial cancer and control groups. Besides, the concentration of HE4 and CA125 was compared in these two groups, and the expression of CA125 and HE4 and clinicopathological characteristics in patients with endometrial cancer were also analyzed. Compared with the control group, the expression of HE4 was much higher in serum of patients with endometrial cancer, while there was no obvious change in the expression of CA125. The threshold detection value was acquired by receiver operating characteristic analysis method, that is, 141.5 pmol/L and 54.5 U/L, respectively. When comparing the concentration of HE4 in patients with endometrial cancer at the early stage (stage I) with healthy people, the difference therein had statistical significance, but there was no obvious difference in CA125. HE4 and CA125 in diagnosis of endometrial cancer in the stages I and II were found with no statistically significant difference. The difference of HE4 in the stages II and III had statistical significance while the difference of CA125 had no statistical significance. The specificity of both HE4 and CA125 was 95%, and the sensitivity of HE4 to uterine papillary serous carcinomas was higher than that to endometrioid adenocarcinoma. Thus, the serum HE4 is much better than CA125 in detecting the endometrial cancer at an early stage.
Keywords: HE4, detection of CA125, endometrial cancer
Introduction
Endometrial cancer, an epithelial malignant tumor, occurs mostly in endometrium of female during menopause, with diverse types. The tumor marker carbohydrate antigen 125 (CA125) is widely applied in the diagnosis and detection of different tumors recently. However, CA125 was less effective in the diagnosis of endometrial cancer compared with the diagnosis of other gynecological cancers. CA125 can only produce obvious effect in diagnosing some common tumors in advanced stage. Among the pathological subtypes of endometrial cancer, papillary serous adenocarcinoma is one of the most malignant diseases, which develops rapidly in the advanced stage. However, there is still lack of effective tumor markers for diagnosis. Human epididymis secretory protein 4 (HE4), a kind of new tumor marker, enjoys a quite low content in healthy tissues and benign tumor of human beings. However, it is more effective than CA125 in the diagnosis of epithelial ovarian cancer. Thus, the study further studied the diagnosis of early endometrial cancer by HE4 and CA125 based on the observation of different diagnosis methods for endometrial cancer.
For example, Meizhen et al put forth the accuracy of diagnosing endometrial cancer by hysteroscopy combined with dilatation and curettage,1 and determined the reliability of cervical involvement. Their study found that this method obviously improved the accuracy of preoperative diagnosis of patients with endometrial cancer. By detecting the concentration of serum chitinase protein in serum from patients with endometrial cancer, healthy people, and patients with hysteromyoma, Xiaohui et al proved the clinical value of applying YKL-40 in diagnosis of endometrial cancer and supervision of condition.2 Bin et al applied enzyme-linked immunosorbent assay (ELISA) to make a preliminary detection of concentration of serum HE4 from patients with endometrial cancer,3 and their study found that HE4 detection was valuable for the diagnosis of endometrial cancer and prognosis judgment. Because there were no further researches on applying HE4 into the diagnosis of early epithelial ovarian cancer or on applying HE4 to the diagnosis of endometrial cancer, this study collected the serum samples from 93 patients with endometrial cancer in different clinical stages and different pathological types and 100 serum samples from healthy female donors in our hospital. The level of HE4 and CA125 in samples was detected by ELISA and chemiluminescent immunoassay. Besides, this article evaluated the value of HE4 for the diagnosis of endometrial cancer in different pathological types and clinical stages and then further discussed the value of HE4 in detecting the prognosis of patients with early endometrial cancer.
Materials and methods
General data
This study selected 93 patients who were found with irregular vaginal bleeding or discharge and diagnosed as endometrial cancer based on diagnostic curettage and who received treatment in our hospital from January 2012 to December 2013. These patients all ranged from 38 to 75 years (mean 59 years). This study has been approved by the ethics committee of the First Hospital of Zhengzhou University and all patients signed the informed consent. Of the 93 patients, 27 patients had endometrial serous papillary adenocarcinoma and 66 patients had endometrioid adenocarcinoma. All these 93 patients were once treated with complete hysterectomy and pelvic lymphadenectomy but had not been treated by neoadjuvant chemotherapy before surgery. The staging for resected tissues was determined by histopathology, including 54 cases of stage I, 18 cases of stage II, and 14 cases of stage III. Besides, this study also recruited 100 healthy females without any gynecopathy. These females were all willing to donate their blood sample as control.
Sample collection
All 93 patients had 5 mL blood sample drawn intravenously on an empty stomach in the morning. Patients with endometrial cancer had blood drawn before surgery. All blood samples were treated with double-blood coding and then reserved in refrigerator at 4°C; these blood samples would be centrifuged within 8 days and preserved in refrigerator at 80°C below zero.
Detection of serum HE4 and CA125
This study used the serum HE4 kits for detection (ELISA) from CanAg Diagnostics AB. The detection standard was 0–150 pmol/L, and the detection range was 0–900 pmol/L. Serum CA125 kits from Shanghai Yulong Biotech Co. Ltd (chemiluminescent immunoassay) were used for detection. The detection standard was 0–35 U/L. Methods were carried out according to the instructions on the kits.
Statistical analysis
All statistical data were expressed in mean ± variance. The comparison of separate samples between groups was carried out by Wilcoxon rank-sum test, and the comparison of completely random and multiple samples was carried out by Kruskal–Wallis H test (the detection standard α=0.017). Receiver operating characteristic analysis method was adopted to determine the value of HE4 and CA125 in the diagnosis of endometrial cancer, and the threshold was calculated by the maximum Youden index method. The detection standard here was α=0.05.
Results
Level of HE4 and CA125
The concentration of serum HE4 and CA125 from patients with endometrial cancer was 209.8±27.3 pmol/L and 39.2±9.4 U/L, respectively, while the two from the healthy females were 95±14.6 pmol/L and 29.1±8.5 U/L, respectively. Figure 1 shows that the threshold of HE4 and CA125 in the diagnosis of endometrial cancer was 141.5 pmol/L and 54.5 U/L, respectively, by receiver operating characteristic method.
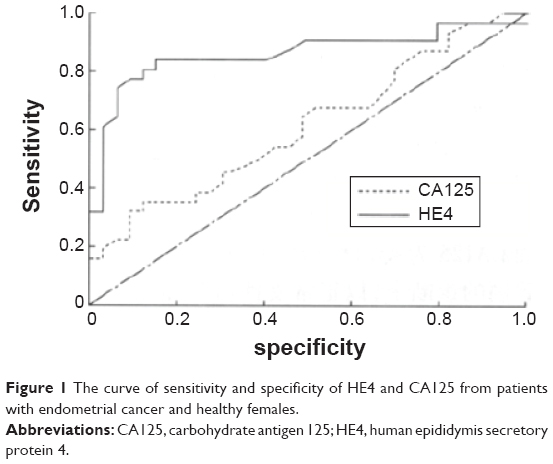 | Figure 1 The curve of sensitivity and specificity of HE4 and CA125 from patients with endometrial cancer and healthy females. |
Comparison of HE4 in different stages of endometrial cancer
The concentration of serum HE4 turned to be higher with the increase of stages of endometrial cancer, and there was no statistical significance in the difference between the stages I and II (P<0.017), while there was a statistical significance in the difference between the stages I and III and the stages II and III (P<0.017). The serum HE4 from patients with endometrial cancer and healthy females in the stage I was 170 and 86 pmol/L, respectively, and the difference within was of statistical significance (P<0.05; Table 1).
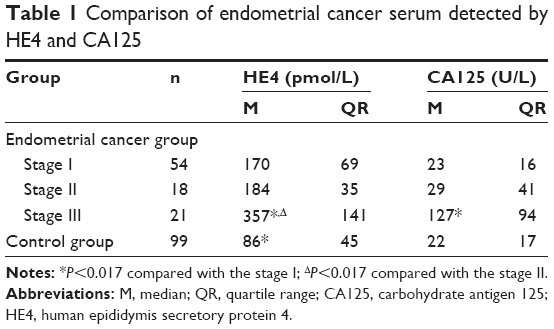 | Table 1 Comparison of endometrial cancer serum detected by HE4 and CA125 |
Comparison of CA125 in different stages of endometrial cancer
The concentration of serum CA125 turned to be higher with the increase of stages of endometrial cancer, and there was no statistical significance in the difference between the stages I and II (P>0.017), while the difference between the stages I and III was of statistical significance (P<0.017). The serum CA125 from patients with endometrial cancer in the stage I and from healthy females was detected to be 23 and 22 U/L, respectively, and the difference between the two had no statistical significance (Table 1).
Comparison of diagnosis value
Table 2 and Table 3 show that the sensitivity of HE4 to diagnosis of endometrioid adenocarcinoma was obviously lower than that to diagnosis of uterine papillary serous carcinomas (P<0.05).
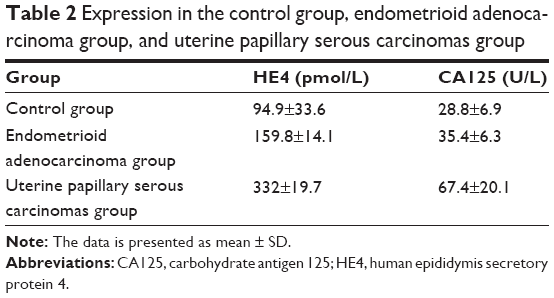 | Table 2 Expression in the control group, endometrioid adenocarcinoma group, and uterine papillary serous carcinomas group |
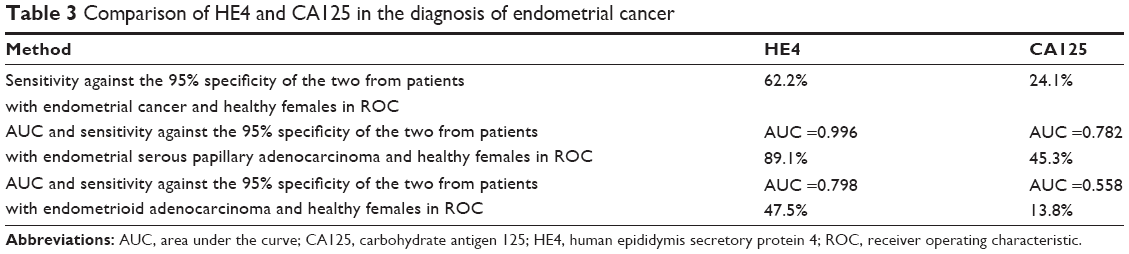 | Table 3 Comparison of HE4 and CA125 in the diagnosis of endometrial cancer |
Discussion
Kirchhoff et al reported at first that they had cloned the cDNA of HE4 gene in the epithelial cells of human distal epididymis.4 They found that this section of gene was about 12,000 bytes, composing of five exons and four introns; it could be sliced in different ways, and there were four orotic acid proteins of disulfide bond core domain in the coding. Meanwhile, it was also found that HE4 might be the protease inhibitor related to mature sperm. Thus, HE4 is considered as the protein related to epididymis specificity and reproduction. It has been revealed that HE4 accounted for a large proportion in ovarian epithelial cancer but a low proportion in normal tissues and benign tumor, which gave the hint that it produced certain effect on the diagnosis of ovarian cancer.5,6
The expression of HE4 protein in tissues of ovarian cancer was positively related to the staging of tumor. Patients with advanced ovarian cancer are found to have a higher expression of serum HE4 than those with early ovarian cancer. Yuping and Guohua found that the expression of serum HE4 improved with the increase of clinical stage.7 The HE4 level from patients with ovarian cancer in the stage I was quite different from that in the stages III and IV. Xia et al used ELISA to detect the level of HE4 from 21 patients with benign ovarian epithelial tumor,8 twelve patients with interactive ovarian epithelial tumor, and 49 patients with ovarian cancer, to study the relation between the detection of serum HE4 and the clinical pathological characteristics of patients with ovarian epithelial tumor. Based on statistical analysis, it was found that the HE4 level in ovarian cancer group was much higher than that in the benign ovarian epithelial tumor group and the interactive ovarian tumor group, and the serum HE4 level in patients with ovarian cancer in the clinical stages II and IV was much higher than that in the clinical stages I and II. Therefore, it was supposed that HE4 might be related to the development of ovarian cancer. Meanwhile, the study results showed that the serum HE4 level in patients with serous cancer was obviously higher than those with mucous cancer. If the diagnosis of early ovarian cancer simply depended on the single serum tumor marker, like CA125, there would be a limited sensitivity and specificity. To date, the major measure to diagnose ovarian cancer clinically is to apply multiple serum tumor markers for a joint detection so as to compensate the defects of single tumor marker detection.9 Studies taking HE4 as the tumor marker for endometrial cancer are just beginning. HE4 is better than other tumor markers, such as CA72-4 and SMRP, in the diagnosis of early endometrial cancer.10
HE4 is a new detection index. A lot of studies both at home and abroad8,11 reveal that HE4 does not express in normal ovarian epithelial cells, expresses in the tissues such as normal endometrium gland, oviduct, Bartholin’s gland tissues, and cervical gland, and expresses high in ovarian serous and ovarian endometrioid adenocarcinoma cells.7,8 This hints that HE4 is likely to be the tumor marker with diagnosis value. Jianwei11 found that compared with CA125, HE4 was quite low in sensitivity and high in specificity as the separate tumor marker in the diagnosis of epithelial-to-mesenchymal transition and malignant pelvic tumor, which was quite beneficial to the diagnosis of EMT and malignant pelvic mutations. Their study also showed that in the diagnosis of EMT and malignant pelvic mutations by CA125 combined with HE4, their sensitivity and specificity sustained a high level, which proved the diagnosis value of serum HE4 and CA125 for EMT and malignant pelvic mutations.
In this study, HE4 obviously increased in the detection of early endometrial cancer. Compared with healthy females, the difference had statistical significance. However, there was no obvious increase tendency in the comparison of patients with early endometrial cancer and the healthy females. Thus, HE4 is of greater significance to the diagnosis of early endometrial cancer than CA125. During the detection of different stages of endometrial cancer, there was no difference in HE4 and CA125 between the stages I and II (P>0.017) but an obvious difference between the stages I and III. Besides, there was a difference in HE4 between the stages II and III but no difference in CA125. Based on the analysis as above, it was believed that HE4 was more sensitive to the detection between the stages II and III than CA125. CA125 in stages I, II, and III endometrial carcinoma was detected to be remarkably different, so did HE4. However, comparison of HE4 and CA125 between stages I and II ended up without significant difference, while notable difference was found between stages I and III. As for comparison between stages II and III, HE4 determination showed statistical significance that did not occur to CA125, indicating more sensitive detection of HE4 than CA125 between stages II and III, which was of great importance in clinical treatment prejudgment.
Uterine papillary serous carcinomas, which are one of the most malignant pathological subtypes among different types of endometrial cancer, develop rapidly but recover difficultly. In addition, its prognosis is worse than the endometrioid adenocarcinoma in the same period,12 and it is on the path of metastasis. The cases of endometrial serous papillary adenocarcinoma have something in common with ovarian serous papillary adenocarcinoma. In the diagnosis of uterine papillary serous carcinomas, CA125 is not as sensitive as the ovarian serous papillary adenocarcinoma.13 It is shown in Table 3 that the sensitivity of HE4 to endometrial papillary adenocarcinoma was higher than that to endometrioid adenocarcinoma. Incidence of endometrial papillary adenocarcinoma is low. Although the endometrial papillary adenocarcinoma relatively constituted a higher ratio in the groups of this study, endometrioid adenocarcinoma was dominated on the whole.
There is an obvious difference in the level of HE4 in patients with different types of endometrial cancer. Uterine papillary serous carcinomas demonstrate a higher level of HE4 compared with endometrioid adenocarcinoma. However, whether the expression of HE4 in the detection of other types of endometrial cancer is meaningful remains to be proved by more experimental studies and evidence. With the further exploration on HE4, further research will be carried out on the early diagnosis and prognosis of ovarian and endometrial cancers.
Acknowledgment
This project is supported by the National Natural Science Foundation of China (Study on miRNA 221/222 Mediated Human Embryo Nidation, No U1304315).
Disclosure
The authors report no conflicts of interest in this work.
References
Meizhen J, Haiyan J, Fengyi H, et al. Value of hysteroscopy and dilatation and curettage in preoperative diagnosis of endometrial carcinoma. Chin Pract Med. 2014;(22):34–36. | ||
Xiaohui S, Jiangtao F, Yan L, et al. Preliminary research of serum YKL-40 in the diagnosis of endometrail carcinoma. J Pract Obstet Gynecol. 2011;27(2):121–124. | ||
Bin C, Xiaowei X, Xuelian L, et al. The application of human epididymis protein 4 in diagnosis of endometrial cancer. J Pract Obstet Gynecol. 2012;28(5):354–356. | ||
Kirchhoff C, Habben I, Ivell R, et al. A major human epididymis-specific cDNA encodes a protein with sequence homology to extracellular protease inhibitors. J Biol Reprod. 1991;45(2):350–357. | ||
Hough CD, Baust CA, Pizer ES, et al. Large-scale serial analysis of gene expression reveals genes deferentially expressed in ovarian cancer. Cancer Res. 2000;60(31):6281. | ||
Schummer M, Ng WV, Bumgarner RE, et al. Comparative hybridization of an array of 21,500 ovarian cDNAs for the discovery of genes over expressed in ovarian carcinomas. Gene. 1999;23(2):375. | ||
Yuping F, Guohua T. Value of combined detection of HE4 and CA125 in early diagnosis of ovarian cancer. Labeled Immunoassays Clin Med. 2010;17(6):368. | ||
Xia C, Ping Z, Xiaoyan L. Relationship between the serum human epididymis secretory protein 4 and clinical pathological features in patients with epithelial ovarian cancer. Labeled Immunoassays Clin Med. 2010;17(6):365–367. | ||
Li J, Dowdy S, Tipton T, et al. HE4 as a biomarker for ovarian and endometrial cancer management. Expert Rev Mol Diagn. 2009;9(6):555–566. | ||
Huhtinen K, Suvitie P, Hiissa J, et al. Serum HE4 concentration differentiates malignant ovarian tumors from ovarian endometriotic cysts. Br J Cancer. 2009;100(8):1315–1319. | ||
Jianwei Z. Detection of serum HE4 combined with CA125 in diagnosis of endometriosis and pelvic malignancy. Shandong Med J. 2014;54(25):84–85. | ||
Rahaman J, Steiner N, Hayes MP, Chuang L, Fishman D, Gretz Iii H. Chemotherapy for gynecologic cancers. Mt Sinai J Med. 2009;76(6):577–588. | ||
Nosov V, Su F, Amneus M, et al. Validation of serum biomarkers for detection of early-stage ovarian cancer. Am J Obstet Gynecol. 2009;200(6):639. e1–639. e5. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.