")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 17
Value of Combining of the NLR and the Fibrinogen Level for Predicting Stroke-Associated Pneumonia
Authors Cheng W, Chen L, Yu H, Lu D , Yu R, Chen J
Received 14 March 2021
Accepted for publication 14 May 2021
Published 28 May 2021 Volume 2021:17 Pages 1697—1705
DOI https://doi.org/10.2147/NDT.S311036
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Yuping Ning
Wei Cheng,1,* Lichang Chen,1,* Huapeng Yu,1 Dongzhu Lu,1 Rong Yu,1 Jian Chen2
1Department of Respiratory Medicine, Zhujiang Hospital, Southern Medical University, Guangzhou, People’s Republic of China; 2Department of Neurology, Zhujiang Hospital, Southern Medical University, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jian Chen
Department of Neurology, Zhujiang Hospital of Southern Medical University, No. 253, Industrial Avenue, Guangzhou, Guangdong, 510280, People’s Republic of China
Tel +86 18665000975
Fax +86 02062783083
Email [email protected]
Purpose: To evaluate the value of the NLR (neutrophil-to-lymphocyte ratio) and the fibrinogen level in predicting stroke-associated pneumonia (SAP) in acute ischemic stroke (AIS) patients.
Patients and Methods: In total, we enrolled 734 medical-ward patients with AIS in this retrospective study. Patients were divided into SAP (n=52) and non-SAP (n=682) groups according to the diagnostic criteria of SAP. Binary logistic regression analysis was used to analyze the relationship between the NLR, serum fibrinogen concentration and SAP. Receiver operating characteristic (ROC) curves were generated to identify the optimal cutoff points and assess the diagnostic value of the NLR, serum fibrinogen and the combination of NLR and fibrinogen in predicting SAP.
Results: SAP occurred in 52 (7.08%) patients among the enrolled AIS patients. Binary logistic regression analysis showed that the NLR (odds ratio [OR]: 2.802, 95% confidence interval [CI]: 1.302– 6.032, P=0.008) and serum fibrinogen concentration (OR: 7.850, 95% CI: 3.636– 16.949, P=0.000) were independently associated with a higher risk of SAP incidence after adjusting for age, sex, ASPECT score, atrial fibrillation, nasogastric tube feeding, LDL-C and TC, temperature at admission and mechanical ventilation. The optimal cutoff points of the NLR and serum fibrinogen to distinguish SAP among AIS patients were 3.603 (AUC, 0.690; NPV, 95.78; PPV, 19.01) and 4.595 (AUC, 0.727; NPV, 95.60; PPV, 24.49), respectively. When the combination of NLR and fibrinogen was used to predict SAP, the optimal cutoff points were > 2.436 for NLR and > 3.24 for fibrinogen (AUC, 0.758; NPV, 98.50; PPV, 11.80).
Conclusion: The NLR and serum fibrinogen might have greater negative diagnostic value in predicting SAP among AIS patients. Combining the NLR and serum fibrinogen showed an increased AUC for predicting SAP among AIS patients.
Keywords: stroke-associated pneumonia, neutrophil-to-lymphocyte ratio, fibrinogen, receiver operating characteristic curve
Introduction
Stroke is a debilitating disease and a leading cause of mortality and disability worldwide, which results in heavy social and economic burdens.1,2 A growing amount of evidence has revealed that stroke-associated pneumonia (SAP) is one of the most frequent and serious medical complications, with morbidity ranging from 3% to 47%;3–7 moreover, SAP is characterized by an unfavorable functional outcome after acute ischemic stroke (AIS) and leads to higher mortality and morbidity as well as a lengthened hospitalization duration.8–11 Thus, early identification and effective prevention are more critical and urgent than the treatment of stroke-associated pneumonia.
Evidence has demonstrated that inflammation is not only important in the pathophysiology of stroke but also indispensable in the occurrence and development of SAP. In addition, as demonstrated in recent studies, immunomodulation after stroke can increase the susceptibility to pneumonia.12–14 The neutrophil-to-lymphocyte ratio (NLR) is a commonly used hematological parameter of infection and systemic inflammation. Increased NLR levels may be an independent predictor for unfavorable clinical prognosis after stroke.15–17 Some evidence has revealed that patients with a higher NLR have an increased susceptibility to SAP.18
Fibrinogen is not only the final product of the coagulation cascade but also the classic acute phase reactant and an effective modifier of inflammatory processes. Substantial evidence indicates that hyperfibrinogenemia plays a vital function in the pathogenesis of AIS and is involved in poor prognoses, such as increased in-hospital mortality, cognitive impairment, and recurrent ischemic events.19–27 Fibrinogen plays critical roles in chronic low-grade inflammation.28 Whether it may reflect the inflammatory state in stroke patients remains unclear. Our study is the first to evaluate the clinical utility of fibrinogen in the prediction of SAP. At the same time, we attempted to combine the NLR and the fibrinogen level to provide a basis for identifying SAP among patients with AIS.
Patients and Methods
Patients
Our study was conducted at Zhujiang Hospital of Southern Medical University. Inclusion criteria were as follows: 1) patients diagnosed based on imaging evidence (cranial magnetic resonance imaging or computed tomography) and relevant clinical symptoms within 24 h after admission; 2) patients admitted within 7 days of stroke onset; and 3) patients with complete clinical information. Exclusion criteria were as follows: 1) pre-existing pneumonia or active infection before admission; 2) a medical history of cancer, hematologic disease, any other CNS injury and ongoing immunosuppressant treatment; 3) transitory ischemic attack (TIA); 4) cerebral hemorrhage; 5) patients who were discharged or died during the first 3 days of hospitalization; and 6) preventive antibiotic therapy. This study was permitted by the Ethics Committee of Zhujiang Hospital of Southern Medical University. The requirement for informed consent was waived by the committee because of the observational and retrospective nature of the investigation. According to the inclusion and exclusion criteria described above, a total of 734 consecutive patients with AIS were retrospectively included in this study between January 2017 and December 2019 (Figure 1).
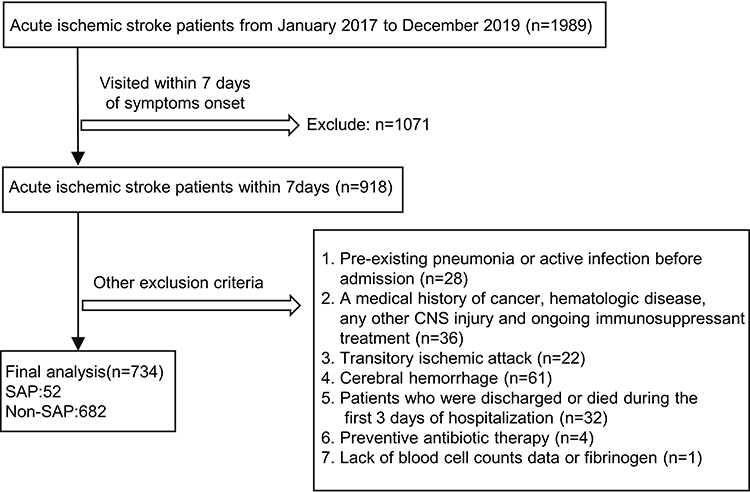 |
Figure 1 Enrollment flow chart of study cohort. |
Diagnosis of SAP
SAP was diagnosed based on the 2015 diagnosis consensus29 according to clinical and laboratory examinations and was confirmed through sputum culture results and chest CT scans retrospectively from medical records.
Data Collection
The collected data were as follows: demographic data (sex and age), diabetes, hypertension, atrial fibrillation, chronic obstructive pulmonary disease and previous history of stroke or TIA, systolic pressure and diastolic pressure at admission, temperature at admission, nasogastric tube feeding, mechanical ventilation, laboratory examinations at admission (triacylglycerol [TG], low-density lipoprotein cholesterol [LDL-C] and total cholesterol [TC], blood glucose, homocysteine, urea, creatinine, albumin, neutrophils, lymphocytes, fibrinogen) and the ASPECT score at admission.
All blood samples were collected within 24 h of admission from participants in a fasting status. WBCs were counted through an automated cell counter, and the NLR was calculated as the absolute neutrophil count divided by the absolute lymphocyte count. The serum fibrinogen concentrations were detected by the modified Clauss method.
Statistical Analysis
First, all enrolled patients were divided into SAP and non-SAP groups. The distribution of quantitative data was tested by the Kolmogorov–Smirnov method. Normally distributed data were defined as the mean (SD), while non-normally distributed data were expressed as the median (range). To compare differences between parameters of SAP and non-SAP, the independent sample Student’s t-test and Mann–Whitney U-test were used for normal distributions and non-normal distributions, respectively. Qualitative data are presented as numbers (percentages), and the chi-square test was applied to compare subgroup differences.
Next, to evaluate the baseline characteristics of AIS patients who had a higher NLR or fibrinogen and make comparisons between the basic characteristics of the high and low NLR groups or fibrinogen groups, we dichotomized the enrolled patients with the cutoff values of NLR (3.603) and fibrinogen (4.595), which were obtained from the ROC curve. Additionally, associations between different NLR and fibrinogen levels and the risk of SAP were estimated using the univariate analysis and binary logistic regression analysis analyses. We adjusted for all potential confounders (Parameters with P value less than 0.05 in univariate analysis), including age, sex, ASPECT score, atrial fibrillation, nasogastric tube feeding, LDL-C and TC, temperature at admission and mechanical ventilation. The results are presented as odds ratios (ORs) along with 95% confidence intervals (CIs), and the lower value group for NLR and fibrinogen was set as the reference.
Finally, the ROC curve was used to evaluate the diagnostic value of a combination of the NLR and serum fibrinogen concentration or either parameter alone, simultaneously obtaining the optimal cutoff point of NLR and fibrinogen for SAP. The differences in the areas under the curves (AUCs) were compared by the DeLong test. P values < 0.05 were considered to be statistically significant. The analysis of AUCs was performed with MedCalc software (Version 18.2.1). Other statistical analyses were performed using SPSS software (IBM SPSS 22.0).
Results
In this study, a total of 734 patients with AIS were included. Five of them received Intravenous thrombolysis (IVT) and four received Endovascular treatment (EVT). SAP was diagnosed in 52 patients (7.08%), and non-SAP was diagnosed in 682 patients (92.92%).
A comparison of the clinical and laboratory parameters between the SAP and non-SAP groups is shown in Table 1. As demonstrated in Table 1, the SAP group showed significantly older age and higher temperature, diastolic pressure, WBCs, and neutrophils, as well as a higher prevalence of atrial fibrillation, nasogastric tube feeding and mechanical ventilation than patients with non-SAP (p<0.05). They also had lower TC, LDL and ASPECT scores than the non-SAP group. Moreover, patients with SAP had a significantly higher NLR and higher fibrinogen levels than the non-SAP group (NLR: 3.61 [2.08–5.81] versus 2.09 [1.54–2.99]; P=0.000. Fibrinogen: 4.18 [3.41–5.75] versus 3.30 [2.87–3.90]; P=0.000, Table 1). There were no statistically significant differences in the rest of the parameters (P>0.05).
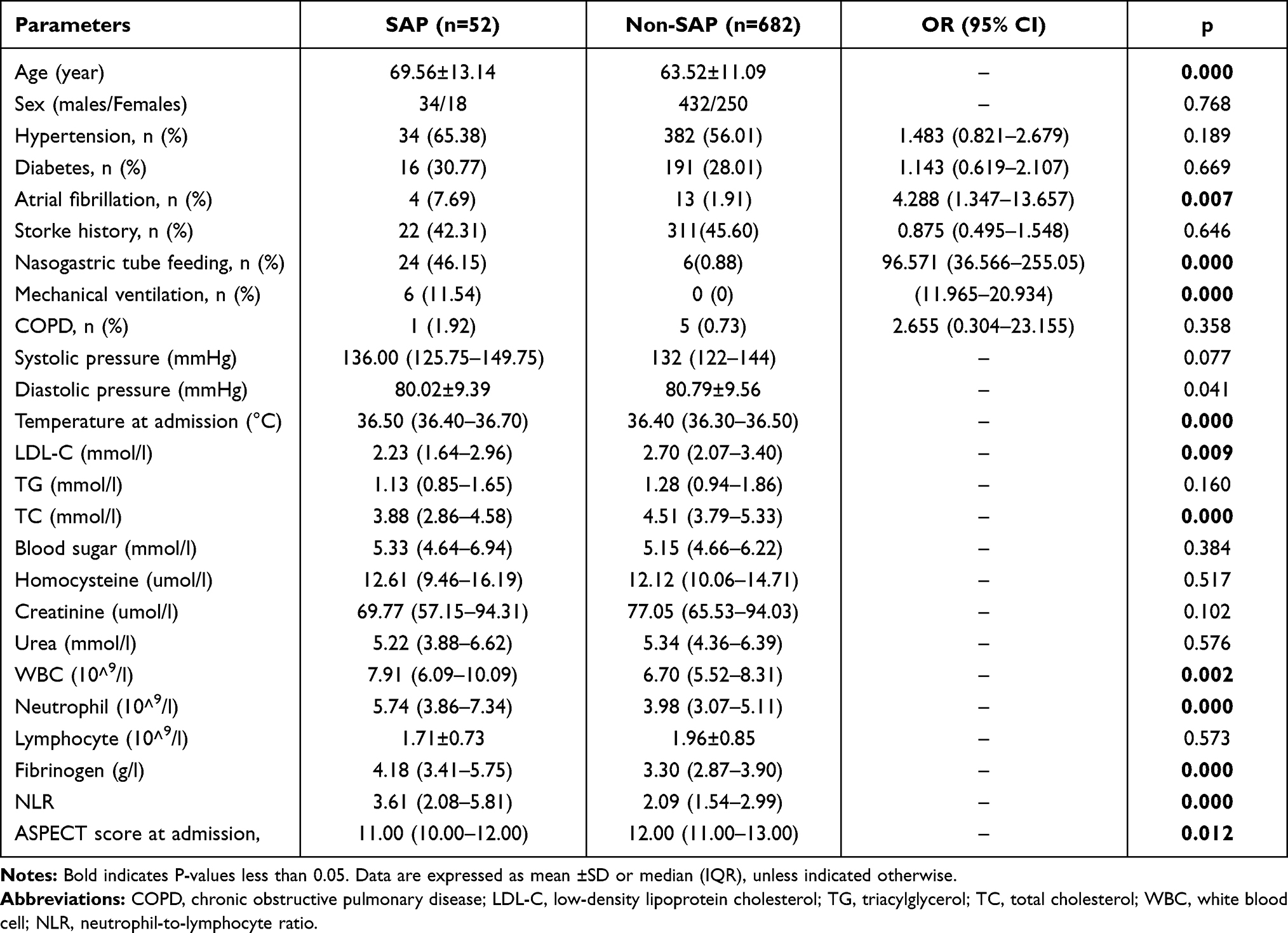 |
Table 1 Baseline Characteristics of SAP and Non-SAP Patients with Acute Ischemic Stroke (N=734) |
When we made a comparison between the higher and the lower NLR groups, AIS patients in the higher NLR groups presented older age; higher rates of atrial fibrillation, diabetes mellitus, nasogastric tube feeding and mechanical ventilation; lower frequencies of stroke history; and lower ASPECT scores than did patients in the lower NLR group. In the higher fibrinogen group of AIS patients, we observed older age; a higher proportion of diabetes mellitus, atrial fibrillation and nasogastric tube feeding; and lower ASPECT scores than did patients in the lower NLR group (Table 2). The results of the univariate analysis showed that patients with admission NLRs in the higher group (≥3.603) had a higher risk of developing SAP than patients in lower group had (<3.603) (odds ratio [OR]: 5.535, 95% confidence interval [CI]: 2.982–9.508, P=0.000). The same result was also found for fibrinogen. After adjusting for confounders, we still found a strong association of either NLR ≥ 3.603 or fibrinogen ≥4.595 with an increased risk of SAP after AIS (NLR: aOR 4.389, 95% CI 2.399–8.029, p = 0.000 Model 1; aOR: 2.802, 95% CI 1.302–6.032, p=0.008 Model 2. Fibrinogen: aOR: 6.394, 95% CI 3.491–11.712, p = 0.000 Model 1; aOR: 7.850, 95% CI 3.636–16.949, p = 0.000 Model 2, Table 3).
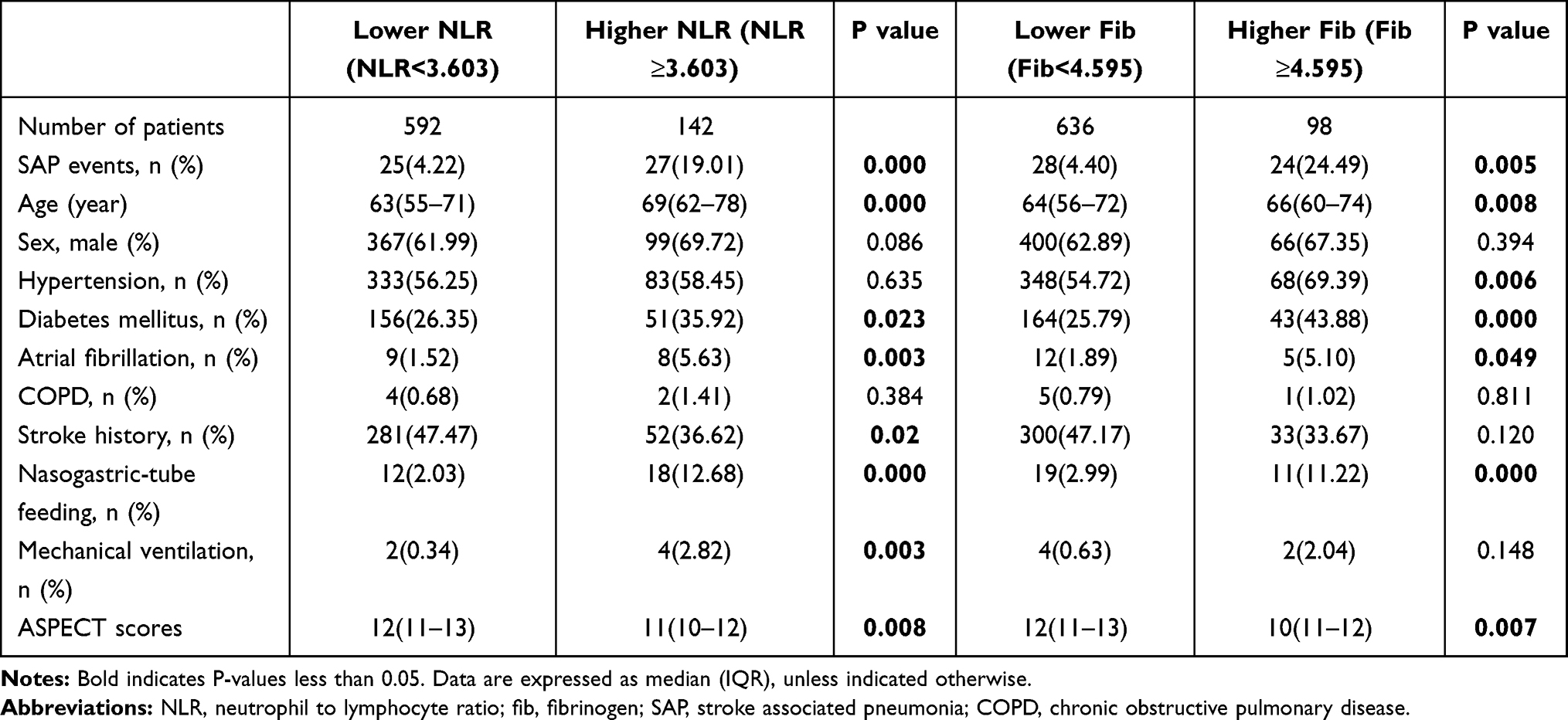 |
Table 2 Baseline Characteristics of Patients with Lower/Higher NLRs and Fibrinogen (N=734) |
 |
Table 3 Multivariate Analysis of the Association of NLR and Fibrinogen with SAP Among AIS Patients |
Significant differences were found between the SAP and non-SAP groups in terms of the following indicators: age, temperature, LDL, TC, WBCs, neutrophils, fibrinogen, NLR, ASPECT score, atrial fibrillation, nasogastric tube feeding and mechanical ventilation. Thus, these are probably potential diagnostic indicators for discriminating SAP from AIS. To evaluate the value of the aforementioned indicators, we used ROC curves to differentiate SAP patients from AIS patients. The AUCs and the optimal cutoff values are shown in Table 4. The largest AUCs for diagnosing SAP were the NLR (AUC, 0.690) and the fibrinogen level (AUC, 0.727), along with the optimal cutoff points, were 3.603 and 4.595, respectively. Therefore, we combined NLR and fibrinogen (AUC=0.758) to improve the diagnostic value. The optimal cutoff points for recognizing SAP from AIS were NLR>2.436 and fibrinogen>3.24 with a sensitivity of 90.38% and a specificity of 48.53%, offering a positive predictive value (PPV) of 12.01% and offering a negative predictive value (NPV) of 98.78% for SAP (Figure 2). The AUC of NLR and fibrinogen was significantly higher than either parameter alone (P<0.05).
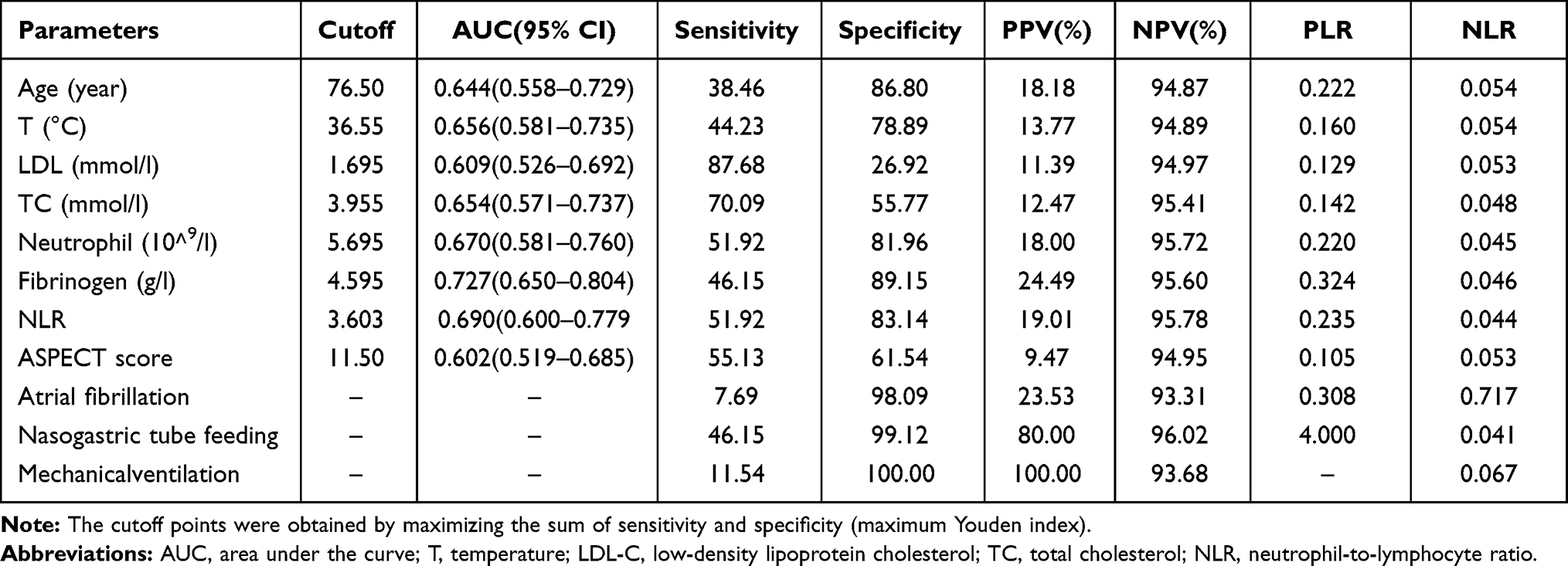 |
Table 4 Optimal Cutoff Values for the Prediction of SAP |
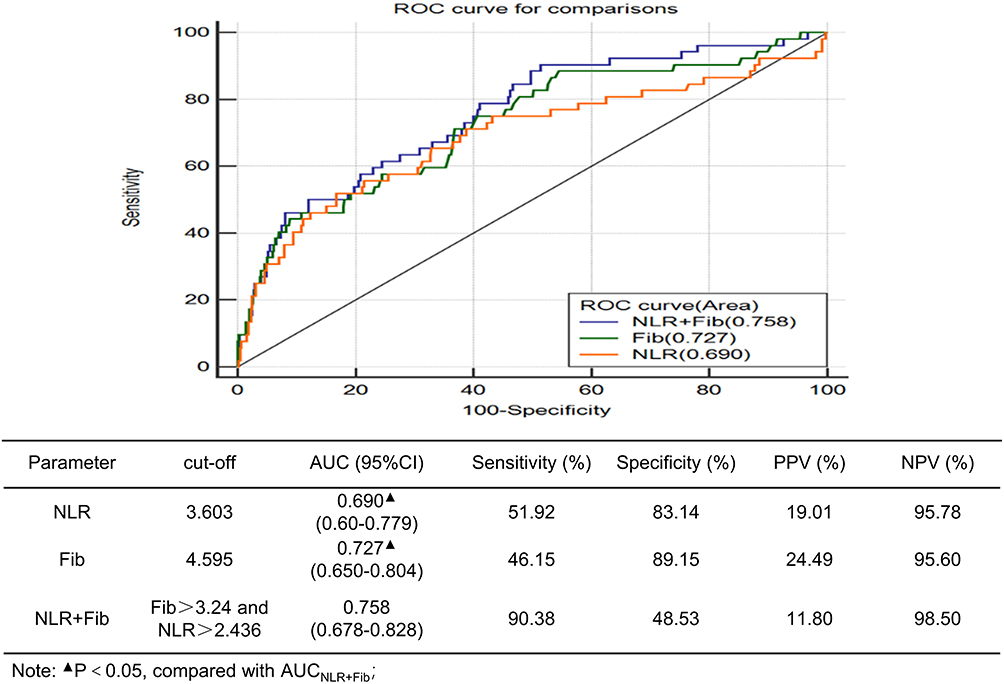 |
Figure 2 ROC curves for NLR, Fib and combination of NLR and Fib in predicting SAP (n=734). Abbreviations: AUC, area under the curve; NLR, neutrophil-to-lymphocyte ratio; Fib, fibrinogen. |
Discussion
As one of numerous frequent complications after stroke, SAP is associated with an extended hospital stay, higher rates of recurrence, worsening of the neurological outcome and subsequent increases in care and financial burdens.8–10 Thus, it is important for stroke patients to obtain an early diagnosis and effective control of SAP, thereby improving their survival rate as well as their quality of life. To our knowledge, compared with the current existing literature, our study is the first to investigate the prognostic role of the NLR and the fibrinogen level in AIS patients related to SAP risk. Furthermore, we evaluated the diagnostic value of combining NLR and fibrinogen in predicting SAP among AIS patients at an early clinical stage.
Currently, the pathophysiological mechanisms of SAP are not well understood; nevertheless, there are several possible explanations. First, stroke-induced immunodepression syndrome (SIDS) is recognized as a key contributor to SAP.12,30 The well-balanced interplay between the immune system and central nervous system (CNS) is vital to the prognosis of acute stroke patients and could be disturbed by acute stroke, thereby resulting in SIDS and predisposing individuals to pulmonary infections.31 Neutrophils not only serve in major immunomodulatory functions during acute inflammation but may also be the first activated immune cells to reach the site of the ischemic brain to regulate and orchestrate the inflammatory response after cerebral ischemia.32,33 In addition, another indispensable component of the immune system is lymphocytes, which are specific for CNS antigens and can increase inflammatory responses in injured brain tissue, thus resulting in a poor prognosis in AIS patients.30 A recent study revealed an inverse correlation between the percentage of lymphocytes and the NIHSS scores, which are usually used to evaluate stroke severity.34
The NLR combines well-known traditional inflammatory indicators, neutrophilia and lymphocytopenia, showing a better predictive value in bacterial infection.35–38 Furthermore, previous studies have reported that the NLR is closely linked to some metabolic diseases, such as diabetes mellitus, which are also recognized as risk factors for SAP.5,39 As illustrated in Table 2, patients in the higher NLR group had more risk factors for SAP. Another explanation may be that stroke severity is a strong risk factor for SAP40–42 Some studies have pointed out that nasogastric tube feeding and mechanical ventilation are correlated with an increased incidence of SAP.43–46 Consistent with previous studies, our study showed that the higher NLR group exhibited a higher prevalence of nasogastric tube feeding and mechanical ventilation than patients with a lower NLR, which can further predispose AIS patients to immunosuppression and, consequently, infections. Therefore, the NLR may act as a biomarker of severe stroke individuals who are prone to SAP.
Fibrinogen, as a liver-produced acute phase protein and a nonspecific inflammatory marker, may rise during any inflammatory process and function in regulating systemic inflammatory signals.47–50 A study underscored that fibrinogen could deposit within inflammatory foci and that extravascular deposits would exacerbate inflammation.28 Although the liver is the chief site of fibrinogen synthesis, epithelial cells from different tissues, including pulmonary tissues, can express fibrinogen genes. Haidaris et al reported that biosynthesis and secretion of fibrinogen can be induced by pulmonary epithelial cells in response to inflammation.51 As described before, fibrinogen may be a better marker in predicting the pulmonary inflammation state. Furthermore, as fibrinogen is a blood coagulation protein, studies have shown that hyperfibrinogenemia is associated with a negative effect on the outcome of AIS.19–21 In our study, we demonstrated that higher fibrinogen levels led to increased odds of SAP. Neutrophils are critical for immune reactions in pneumonia.52 Fibrinogen protects neutrophils from the cytotoxicity of circulating histones or leucocidins during NETosis (neutrophil extracellular traps) and delays NET formation induced by ionomycin.53 In sum, we included fibrinogen and NLR as predictors to determine the SAP prognosis more accurately.
We observed that the SAP group had a prominently higher NLR or higher fibrinogen level than the non-SAP group. The percentage of SAP in the group with NLR≥3.603 was 19.01% (27/142), which was markedly higher than that in the group with NLR<3.603 (4.22%, 25/592) (OR: 5.325, 95% CI: 2.982–9.508, P=0.000). Similarly, we found that fibrinogen had the same result. In addition, we found a strong association between NLR or fibrinogen and SAP, regardless of adjusting for potential confounding factors. These revealed that both NLR and fibrinogen were effective predictors of SAP, which was independent of certain established risk factors (age, sex, LDL-C, TC, temperature at admission, the ASPECT score, atrial fibrillation, nasogastric tube feeding and mechanical ventilation). Therefore, NLR and fibrinogen detection could have predictive value for SAP among patients with AIS.
Furthermore, our study showed that the AUC of the NLR used to predict SAP was 0.690, with an optimal cutoff of 3.603, and that the AUC of fibrinogen was 0.727, with the best cutoff being 4.595. Here the NPV of SAP for NLR (95.78%) and fibrinogen (95.60%) was higher than the PPV (NLR: 19.01%; fibrinogen: 24.49%), which indicates that lower NLR and lower fibrinogen are more likely to help clinicians to exclude SAP, while patients with higher NLRs and higher fibrinogen levels need further examinations to clarify the etiology. The addition of serum fibrinogen to the NLR was found to possess better predictive ability for SAP among AIS patients. The AUC was 0.758 (with cutoff points of >2.436 for NLR and >3.24 for fibrinogen), which showed significantly better diagnostic value of SAP than either parameter alone. Herein, the cost of detecting the complete blood count and serum fibrinogen was economical in clinical practice. Overall, because the combined biomarkers have higher predictive ability than individual biomarkers, combined biomarkers may contribute to distinguishing AIS patients with a high risk of developing SAP at an early clinical stage, thereby facilitating timely clinical intervention and appropriate treatment.
There are several limitations of our current study that merit consideration. First, our study was limited by a small sample size from a single center, which could have caused patient bias. Hence, further multicenter and prospective studies are necessary. Second, NLR and fibrinogen were merely measured at admission, and therefore, we could not monitor the changes in NLR and fibrinogen dynamically, which may be associated with disease progression. Third, the time course for SAP was unclear. We cannot conclude that there is a causal association between longer hospitalization and SAP. Finally, due to our selected patient population, our study cannot be applied to patients with intracerebral hemorrhage. We hope future studies can evaluate the combined NLR and fibrinogen values as a predictive biomarker in all types of stroke patients.
Conclusion
Early diagnosis and timely intervention are very important and can improve outcomes, promote survival rates and reduce the care and financial burden of SAP. Our current study showed that, compared with single biomarkers, combined NLR and fibrinogen values had the highest predictive value for SAP among AIS patients from the medical ward. Taken together, our results suggest that NLR >2.436 and fibrinogen > 3.24 can be applied to screen for SAP in AIS patients at an early stage in clinical practice. Nonetheless, it is necessary to carry out further investigations for a better demonstration of the function of the NLR and fibrinogen as well as their effect mechanism(s) relating to different aspects of AIS.
Data Sharing Statement
The datasets used and analysed during this study are available from the corresponding author on reasonable request.
Ethics and Consent Statements
This study adheres to the principles of the Declaration of Helsinki. The protocol was approved by the Ethics Committee of Zhujiang Hospital of Southern Medical University, China (Ethical Approval no. 2020-KY-046-01. Because it is a retrospective study that contained no identifiable data, informed consent was waived. Patients’ privacy and personal identity information were well protected.
Acknowledgments
The authors thank all the participants. And thank the clinical worker for their cooperation.
Disclosure
The authors have no conflicts of interest in this work.
References
1. Roth GA, Abate D, Abate KH, et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1736–1788.
2. Feigin VL, Norrving B, Mensah GA. Global burden of stroke. Circ Res. 2017;120(3):439–448. doi:10.1161/CIRCRESAHA.116.308413
3. Ovbiagele B, Hills NK, Saver JL, et al. Frequency and determinants of pneumonia and urinary tract infection during stroke hospitalization. J Stroke Cerebrovasc Dis. 2006;15(5):209–213. doi:10.1016/j.jstrokecerebrovasdis.2006.05.004
4. Finlayson O, Kapral M, Hall R, et al. Risk factors, inpatient care, and outcomes of pneumonia after ischemic stroke. Neurology. 2011;77(14):1338–1345. doi:10.1212/WNL.0b013e31823152b1
5. Patel UK, Kodumuri N, Dave M, et al. Stroke-associated pneumonia: a retrospective study of risk factors and outcomes. Neurologist. 2020;25(3):39–48. doi:10.1097/NRL.0000000000000269
6. Harms H, Grittner U, Dröge H, et al. Predicting post-stroke pneumonia: the PANTHERIS score. Acta Neurol Scand. 2013;128(3):178–184. doi:10.1111/ane.12095
7. Upadya A, Thorevska N, Sena KN, et al. Predictors and consequences of pneumonia in critically ill patients with stroke. J Crit Care. 2004;19(1):16–22. doi:10.1016/j.jcrc.2004.02.004
8. Li Y, Zhang Y, Ma L, et al. Risk of stroke-associated pneumonia during hospitalization: predictive ability of combined ADS score and hyperglycemia. BMC Neurol. 2019;19(1):298. doi:10.1186/s12883-019-1497-x
9. Teh WH, Smith CJ, Barlas RS, et al. Impact of stroke-associated pneumonia on mortality, length of hospitalization, and functional outcome. Acta Neurol Scand. 2018;138(4):293–300. doi:10.1111/ane.12956
10. Kishore AK, Vail A, Bray BD, et al. Clinical risk scores for predicting stroke-associated pneumonia: a systematic review. Eur Stroke J. 2016;1(2):76–84. doi:10.1177/2396987316651759
11. Yang J, Dai Y, Zhang Z, et al. Value of combination of the ADS score and IL-6 in predicting stroke-associated pneumonia. Neuropsychiatr Dis Treat. 2020;16:2353–2359. doi:10.2147/NDT.S268878
12. Hoffmann S, Harms H, Ulm L, et al. Stroke-induced immunodepression and dysphagia independently predict stroke-associated pneumonia - the PREDICT Study. J Cereb Blood Flow Metab. 2017;37(12):3671–3682. doi:10.1177/0271678X16671964
13. Feng HX, Cheng Y, Zhu W, et al. T-lymphocyte subsets as a predictive biomarker for stroke-associated pneumonia. Am J Transl Res. 2018;10(12):4367–4375.
14. Liu DD, Chu S-F, Chen C, et al. Research progress in stroke-induced immunodepression syndrome (SIDS) and stroke-associated pneumonia (SAP). Neurochem Int. 2018;114:42–54. doi:10.1016/j.neuint.2018.01.002
15. Wang L, Song Q, Wang C, et al. Neutrophil to lymphocyte ratio predicts poor outcomes after acute ischemic stroke: a Cohort Study and systematic review. J Neurol Sci. 2019;406:116445. doi:10.1016/j.jns.2019.116445
16. Wan J, Wang X, Zhen Y, et al. The predictive role of the neutrophil-lymphocyte ratio in the prognosis of adult patients with stroke. Chin Neurosurg J. 2020;6(1):22. doi:10.1186/s41016-020-00201-5
17. Semerano A, Strambo D, Martino G, et al. Leukocyte counts and ratios are predictive of stroke outcome and hemorrhagic complications independently of infections. Front Neurol. 2020;11:201. doi:10.3389/fneur.2020.00201
18. Nam KW, Kim TJ, Lee JS, et al. High neutrophil-to-lymphocyte ratio predicts stroke-associated pneumonia. Stroke. 2018;49(8):1886–1892. doi:10.1161/STROKEAHA.118.021228
19. Swarowska M, Janowska A, Polczak A, et al. The sustained increase of plasma fibrinogen during ischemic stroke predicts worse outcome independently of baseline fibrinogen level. Inflammation. 2014;37(4):1142–1147. doi:10.1007/s10753-014-9838-9
20. Swarowska M, Polczak A, Pera J, et al. Hyperfibrinogenemia predicts long-term risk of death after ischemic stroke. J Thromb Thrombolysis. 2014;38(4):517–521. doi:10.1007/s11239-014-1122-1
21. You S, Yin X, Liu H, et al. Hyperfibrinogenemia is significantly associated with an increased risk of in-hospital mortality in acute ischemic stroke patients. Curr Neurovasc Res. 2017;14(3):242–249. doi:10.2174/1567202614666170621103604
22. Di Napoli M, Papa F. Inflammation, hemostatic markers, and antithrombotic agents in relation to long-term risk of new cardiovascular events in first-ever ischemic stroke patients. Stroke. 2002;33(7):1763–1771. doi:10.1161/01.STR.0000019124.54361.08
23. Shenhar-Tsarfaty S, Ben Assayag E, Bova I, et al. Persistent hyperfibrinogenemia in acute ischemic stroke/transient ischemic attack (TIA). Thromb Haemost. 2008;99(1):169–173. doi:10.1160/TH07-08-0484
24. Woodward M, Lowe GD, Campbell DJ, et al. Associations of inflammatory and hemostatic variables with the risk of recurrent stroke. Stroke. 2005;36(10):2143–2147. doi:10.1161/01.STR.0000181754.38408.4c
25. Rothwell PM, Howard SC, Power DA, et al. Fibrinogen concentration and risk of ischemic stroke and acute coronary events in 5113 patients with transient ischemic attack and minor ischemic stroke. Stroke. 2004;35(10):2300–2305. doi:10.1161/01.STR.0000141701.36371.d1
26. Aono Y, Ohkubo T, Kikuya M, et al. Plasma fibrinogen, ambulatory blood pressure, and silent cerebrovascular lesions: the Ohasama Study. Arterioscler Thromb Vasc Biol. 2007;27(4):963–968. doi:10.1161/01.ATV.0000258947.17570.38
27. Zhang L, Li X, Wang D, et al. Risk factors of recurrent ischemic events after acute noncardiogenic ischemic stroke. Curr Pharm Des. 2019;25(45):4827–4834. doi:10.2174/1381612825666191029103756
28. Luyendyk JP, Schoenecker JG, Flick MJ. The multifaceted role of fibrinogen in tissue injury and inflammation. Blood. 2019;133(6):511–520. doi:10.1182/blood-2018-07-818211
29. Smith CJ, Kishore AK, Vail A, et al. Diagnosis of stroke-associated pneumonia: recommendations from the pneumonia in stroke consensus group. Stroke. 2015;46(8):2335–2340. doi:10.1161/STROKEAHA.115.009617
30. Chamorro Á, Meisel A, Planas AM, et al. The immunology of acute stroke. Nat Rev Neurol. 2012;8(7):401–410. doi:10.1038/nrneurol.2012.98
31. Dirnagl U, Klehmet J, Braun JS, et al. Stroke-induced immunodepression: experimental evidence and clinical relevance. Stroke. 2007;38(2):770–773. doi:10.1161/01.STR.0000251441.89665.bc
32. Strecker JK, Schmidt A, Schäbitz WR, et al. Neutrophil granulocytes in cerebral ischemia - evolution from killers to key players. Neurochem Int. 2017;107:117–126. doi:10.1016/j.neuint.2016.11.006
33. Cai W, Liu S, Hu M, et al. Functional dynamics of neutrophils after ischemic stroke. Transl Stroke Res. 2020;11(1):108–121. doi:10.1007/s12975-019-00694-y
34. Xiao J, Qiu QW, Qin C, et al. Dynamic changes of peripheral blood lymphocyte subsets in acute ischemic stroke and prognostic value. Brain Behav. 2020;e01919.
35. de Jager CP, Wever PC, Gemen EF, et al. The neutrophil-lymphocyte count ratio in patients with community-acquired pneumonia. PLoS One. 2012;7(10):e46561. doi:10.1371/journal.pone.0046561
36. Liu X, Shen Y, Wang H, et al. Prognostic significance of neutrophil-to-lymphocyte ratio in patients with sepsis: a Prospective Observational Study. Mediators Inflamm. 2016;2016:8191254. doi:10.1155/2016/8191254
37. Curbelo J, Luquero Bueno S, Galván-Román JM, et al. Inflammation biomarkers in blood as mortality predictors in community-acquired pneumonia admitted patients: importance of comparison with neutrophil count percentage or neutrophil-lymphocyte ratio. PLoS One. 2017;12(3):e0173947. doi:10.1371/journal.pone.0173947
38. Berhane M, Melku M, Amsalu A, et al. The role of neutrophil to lymphocyte count ratio in the differential diagnosis of pulmonary tuberculosis and bacterial community-acquired pneumonia: a Cross-Sectional Study at Ayder and Mekelle Hospitals, Ethiopia. Clin Lab. 2019;65(4). doi:10.7754/Clin.Lab.2018.180833
39. Imtiaz F, Shafique K, Mirza SS, et al. Neutrophil lymphocyte ratio as a measure of systemic inflammation in prevalent chronic diseases in Asian population. Int Arch Med. 2012;5(1):2. doi:10.1186/1755-7682-5-2
40. Walter U, Knoblich R, Steinhagen V, et al. Predictors of pneumonia in acute stroke patients admitted to a neurological intensive care unit. J Neurol. 2007;254(10):1323–1329. doi:10.1007/s00415-007-0520-0
41. Hannawi Y, Hannawi B, Rao CPV, et al. Stroke-associated pneumonia: major advances and obstacles. Stroke Cerebrovasc Dis. 2013;35(5):430–443. doi:10.1159/000350199
42. Meisel C, Schwab JM, Prass K, et al. Central nervous system injury-induced immune deficiency syndrome. Nat Rev Neurosci. 2005;6(10):775–786. doi:10.1038/nrn1765
43. de Montmollin E, Ruckly S, Schwebel C, et al. Pneumonia in acute ischemic stroke patients requiring invasive ventilation: impact on short and long-term outcomes. J Infect. 2019;79(3):220–227. doi:10.1016/j.jinf.2019.06.012
44. Gujjar AR, Deibert E, Manno EM, et al. Mechanical ventilation for ischemic stroke and intracerebral hemorrhage: indications, timing, and outcome. Neurology. 1998;51(2):447–451. doi:10.1212/WNL.51.2.447
45. Leibovitz A, Plotnikov G, Habot B, et al. Pathogenic colonization of oral flora in frail elderly patients fed by nasogastric tube or percutaneous enterogastric tube. J Gerontol a Biol Sci Med Sci. 2003;58(1):52–55. doi:10.1093/gerona/58.1.M52
46. Gomes GF, Pisani JC, Macedo ED, et al. The nasogastric feeding tube as a risk factor for aspiration and aspiration pneumonia. Curr Opin Clin Nutr. 2003;6(3):327–333. doi:10.1097/01.mco.0000068970.34812.8b
47. Castell JV, Gómez-Lechón MJ, David M, et al. Acute-phase response of human hepatocytes: regulation of acute-phase protein synthesis by interleukin-6. Hepatology. 1990;12(5):1179–1186. doi:10.1002/hep.1840120517
48. Davalos D, Akassoglou K. Fibrinogen as a key regulator of inflammation in disease. Semin Immunopathol. 2012;34(1):43–62. doi:10.1007/s00281-011-0290-8
49. Huang W, Wang S, Zhang H, et al. Prognostic significance of combined fibrinogen concentration and neutrophil-to-lymphocyte ratio in patients with resectable non-small cell lung cancer. Cancer Biol Med. 2018;15(1):88–96. doi:10.20892/j.issn.2095-3941.2017.0124
50. Ubaldo O, Lazaro M, Aventura ET, et al. Can serum fibrinogen predict ARDS? Infect Dis. 2020;13:1178633720943505.
51. Haidaris PJ. Induction of fibrinogen biosynthesis and secretion from cultured pulmonary epithelial cells. Blood. 1997;89(3):873–882. doi:10.1182/blood.V89.3.873
52. Nathan C. Neutrophils and immunity: challenges and opportunities. Nat Rev Immunol. 2006;6(3):173–182. doi:10.1038/nri1785
53. Locke M, Francis RJ, Tsaousi E, et al. Fibrinogen protects neutrophils from the cytotoxic effects of histones and delays neutrophil extracellular trap formation induced by ionomycin. Sci Rep. 2020;10(1):11694. doi:10.1038/s41598-020-68584-0
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.