")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
Value of Combination of the A2DS2 Score and IL-6 in Predicting Stroke-Associated Pneumonia
Authors Yang J, Dai Y, Zhang Z , Chen Y
Received 27 June 2020
Accepted for publication 7 September 2020
Published 9 October 2020 Volume 2020:16 Pages 2353—2359
DOI https://doi.org/10.2147/NDT.S268878
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Yuping Ning
Jun Yang,1 Yonghong Dai,1 Zuowen Zhang,2 Yue Chen3
1Department of Critical Care Medicine, Central Hospital of Jiangjin District, Chongqing 402260, People’s Republic of China; 2Department of Neurology, Central Hospital of Jiangjin District, Chongqing 402260, People’s Republic of China; 3Department of Rehabilitation, Central Hospital of Jiangjin District, Chongqing 402260, People’s Republic of China
Correspondence: Yue Chen
Department of Rehabilitation, Central Hospital of Jiangjin District, Chongqing Dingshan Street, Jiangjin District, Chongqing 402260, People’s Republic of China
Tel +86-15823491696
Email [email protected]
Purpose: To evaluate the value of the combination of the age, atrial fibrillation, dysphagia, male sex, and National Institutes of Health Stroke Scale (A2DS2) score and serum interleukin 6 (IL-6) concentration in predicting stroke-associated pneumonia (SAP).
Patients and Methods: A total of 398 patients with acute ischemic stroke (AIS) from the medical ward was included in this retrospective study. They were divided into the SAP group and non-SAP group according to the diagnostic criteria of SAP. Multivariate analysis was performed to analyze the association between the A2DS2 score, serum IL-6 concentration, and SAP using a backward stepwise logistic regression model. The receiver operating characteristic (ROC) curve was used to evaluate the value of the A2DS2 score, serum IL-6 concentration and combination of A2DS2 score and IL-6 in predicting SAP.
Results: SAP was diagnosed in 70 patients (17.6%). Multivariate analysis showed that the A2DS2 score (odds ratio [OR]: 2.25, 95% confidence interval [CI]: 1.17– 4.99, P=0.017) and serum IL-6 concentration (OR: 1.76, 95% CI: 1.44– 1.95, P< 0.001) was independently associated with SAP after adjusting for age, smoking, hypertension, hyperlipidemia, and atrial fibrillation. When the A2DS2 score, serum IL-6 concentration and combination of A2DS2 score and IL-6 were employed to predict SAP, the AUC was 0.824 (SE: 0.026, 95% CI: 0.773– 0.875), 0.715 (SE: 0.034, 95% CI: 0.641– 0.788) and 0.917 (SE: 0.015, 95% CI: 0.887– 0.946), respectively. The AUC of combinative prediction was significantly higher than independent prediction (0.917 vs. 0.824, Z=3.098, P< 0.001; 0.917 vs. 0.715, Z=5.436, P< 0.001).
Conclusion: The addition of serum IL-6 to the A2DS2 score could significantly enhance the AUC of predicting SAP in AIS patients from the medical ward.
Keywords: stroke-associated pneumonia; SAP, A2DS2 score, interleukin 6, multivariate analysis, receiver operating characteristic curve; ROC
Introduction
Stroke is one of the most common cerebrovascular diseases with high incidence and mortality.1 Acute ischemic stroke (AIS) is the most common type of stroke, accounting for 80% of the total stroke cases.2 Many complications occur following a stroke, such as pneumonia, epilepsy, hemorrhagic transformation, secondary infections, etc. Stroke-associated pneumonia (SAP) is a frequent and feared complication after acute stroke, associated with increased mortality and length of hospital stay and poor prognosis.3–6 Thus, early detection and appropriate treatment for SAP should be emphasized in order to improve the prognosis of stroke patients.
Many baseline clinical variables may predispose individuals to SAP, such as age, the severity of stroke, dysphagia, location, and type of stroke, etc.7–10 Several risk stratification scores for predicting SAP have been derived based on these routinely available variables. Among them, the Age, Atrial Fibrillation, Dysphagia, Male sex, and National Institutes of Health Stroke Scale (A2DS2) score proposed by Hoffmann et al is a simple and effective tool for predicting SAP during hospitalization,11 which may have the best performance in identifying patients at high risk of SAP.12,13 Stroke is associated with altered systemic immunity, predisposing patients to infections and immunosuppression.14 Therefore, biomarkers involved in the immune changes and systemic inflammatory response may be associated with occurrence of SAP. A study has demonstrated that interleukin 6 (IL-6) may be a reliable biomarker for prediction of stroke-associated infection (SAI) after AIS.15 However, the value of the combination of the A2DS2 score and IL-6 in predicting SAP remains unclarified. In this study, the value of a combination of the A2DS2 score and serum IL-6 concentration in predicting SAP was evaluated with the receiver operating characteristic (ROC) curve through a single center retrospective case series study.
Patients and Methods
Patients
Consecutive patients with AIS were retrospectively enrolled in the medical ward of Central Hospital of Jiangjin District, Chongqing between July 2016 and October 2019. Inclusion criteria included: 1) patients confirmed by cranial magnetic resonance imaging (MRI) or computed tomography (CT) within 24 h after admission; 2) patients admitted within 7 days following onset of stroke; and 3) patients with complete clinical data. Exclusion criteria included: 1) pre-existing pneumonia before admission; 2) transient ischemic attack (TIA); 3) lacking the A2DS2 scoring items; 4) patients who were died or discharged within 3 days following onset of stroke; 5) preventive antibiotic therapy; 6) active infection or pyrexia within the 2 weeks before admission; 7) other post-stroke infections (non-SAP); 8) patients with ventilation who develop pneumonia during the first 7 days after the onset of stroke; 9) medical history of any other central nervous system disease, such as cerebral hemorrhage, brain trauma, hydrocephalus, Parkinson’s disease, etc. This study was performed in accordance with the Declaration of Helsinki and permitted by the Ethics Committee of Central Hospital of Jiangjin District, Chongqing. All patients provided written informed consent, and that consent was obtained from the study participants prior to study commencement.
Diagnosis of SAP
SAP was diagnosed retrospectively from medical records by two experienced neurologists according to the modified Centers for Disease Control and Prevention criteria for hospital-acquired pneumonia,16 based on clinical and laboratory examinations, including cough, fever, new purulent sputum, positive sputum culture, or auscultatory respiratory crackles. Suspected pneumonia patients, based on clinical symptoms and typical chest X-ray were diagnosed and confirmed through sputum cultures and chest CT.17
Data Collection
The following data were collected, including demographic data (sex and age), vascular risk factors (smoking, drinking, diabetes, hypertension, hyperlipidemia, coronary heart disease, atrial fibrillation, and previous history of stroke or TIA), laboratory examinations at admission (triacylglycerol [TG], low-density lipoprotein cholesterol [LDL-C], high-density lipoprotein cholesterol [HDL-C], glycosylated hemoglobin [GHb], and total cholesterol [TC]), duration from stroke onset to admission, Trial of org 10,172 in acute stroke treatment (TOAST) classification (Large artery atherosclerosis, cardioembolism, small vessel occlusion, other determined, and undetermined), treatment methods (intravenous thrombolysis, anticoagulants, statins, and antiplatelet agents), and the A2DS2 score at admission.
The A2DS2 score included the following items:11 1) 1 point for age ≥75-years-old; 2) 1 point for atrial fibrillation that was diagnosed by standard electrocardiogram or Holter monitor; 3) 2 points for dysphagia; 4) 1 point for male sex; and 5) 5 points for a National Institute of Health stroke scale (NIHSS) score >16 points and 3 points for an NIHSS score ranging from 5 to 15 points.
Detection of Serum IL-6 Concentrations
All patients were collected for blood samples within 24 h of admission, following overnight fasting. Serums were separated through centrifugation at 3000 g for 10 min and then stored at −80°C. Serum IL-6 concentrations were detected using Human IL-6 ELISA Kit (abcam, Shanghai, China) through the colorimetric method. Detection was performed strictly following the manufacturer’s instructions.
Statistical Analysis
The SPSS version 22.0 (SPSS Inc., USA) was used to perform statistical analysis and significance was set at two-sided P<0.05. Kolmogorov–Smirnov test was used to evaluate the distribution of quantitative data. Normally distributed data were expressed as mean ± standard deviation, and the Student’s t test was used to compare intergroup differences; and non-normally distributed data were expressed as median (M) and interquartile range (IQR), and Mann–Whitney U-test was used to compare intergroup differences. Qualitative data were expressed as percentages or ratios (%), and the Chi-square test was used to compare intergroup differences. Variables with two-sided P<0.10 in univariate analysis were then included in multivariate analysis employing a backward stepwise logistic regression model. ROC curve was used to evaluate the predictive value. The ROC curve, used to evaluate the predictive value of a combination of the A2DS2 score and serum IL-6 concentration, was drawn with the probability derived from the logistic regression model. The area under curve (AUC) was compared with the Z test.
Results
General Data
A total of 451 consecutive patients with AIS were enrolled. Among them, 8 patients were excluded due to being transferred to the Department of Neurosurgery for surgical treatment, 25 patients due to incomplete clinical data, and 20 patients due to meeting the exclusion criteria. Finally, 398 patients were included in this study. They included 238 males (59.8%) and 160 females (40.2%) with an average age of (62±9) years. SAP was diagnosed in 70 patients (17.6%). The average time of SAP onset was (4.12±1.57) d after admission.
Univariate Analysis
Univariate analysis (Table 1) demonstrated that age, smoking, hypertension, atrial fibrillation, the serum IL-6 concentration, and A2DS2 score were statistically different between AIS patients with SAP and without SAP (P<0.05), and the rest of the variables were not statistically different (P>0.05).
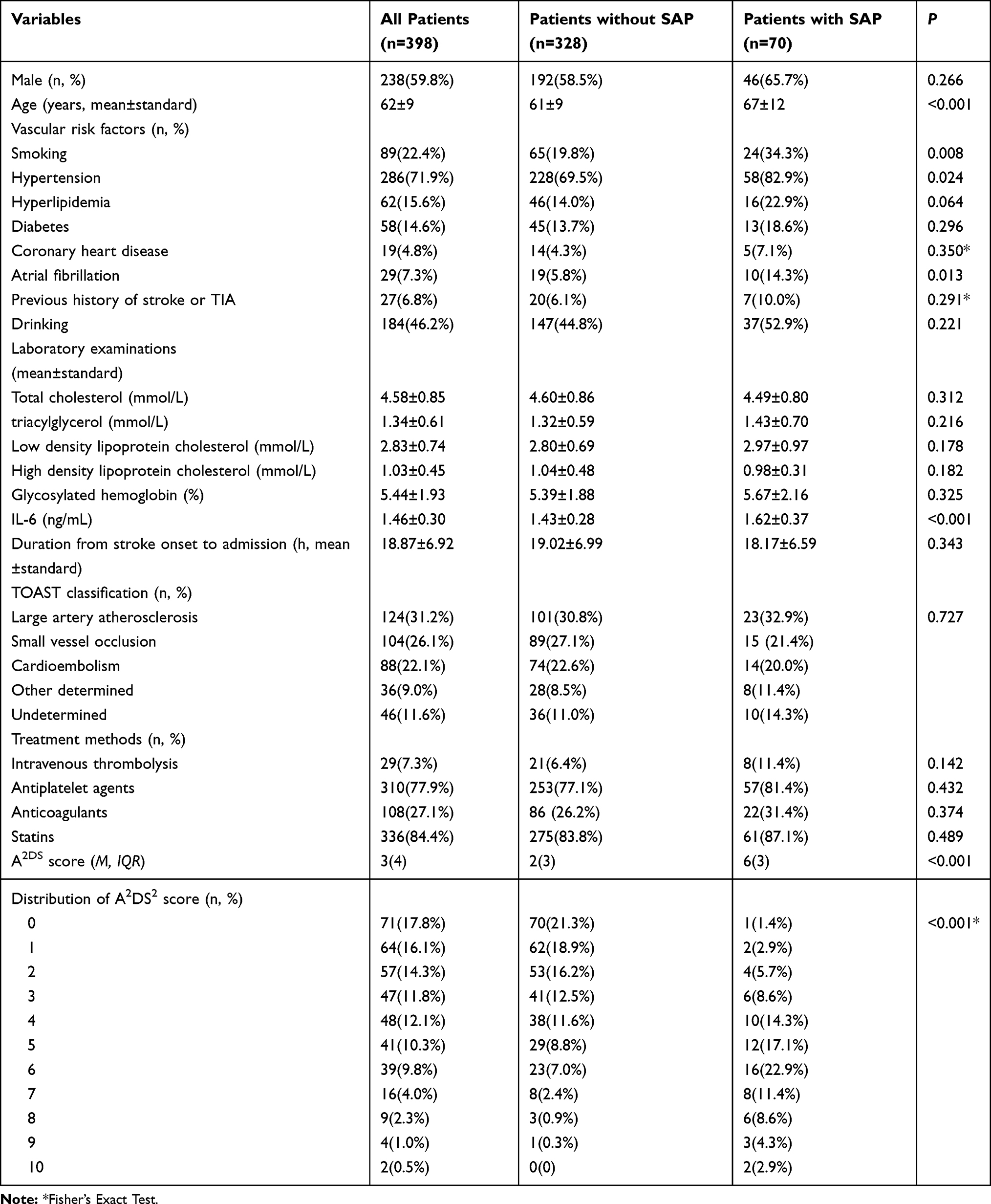 |
Table 1 Results of Univariate Analysis Between AIS Patients With SAP and Without SAP |
The average concentration of serum IL-6 was (1.46±0.30) ng/mL. Stroke severity was evaluated with the NIHSS. The serum IL-6 concentration was higher in AIS patients with an NIHSS score ≥ 5 than in AIS patients with an NIHSS score < 5 (1.48±0.32 vs. 1.40±0.26, n1=109, n2=289, t=2.335, P=0.020). Lesion size was divided into large (>50 × 50 mm and > 5 slices), moderate (≤15 × 15 mm and > 5 slices or > 50 × 50 mm and ≤ 5 slices), and small (≤15 × 15 mm and ≤ 5 slices). The serum IL-6 concentration demonstrated the tendency of large infract volume > moderate infract volume > small infract volume (1.54±0.34 vs. 1.43±0.29 vs. 1.30±0.21, n1=192, n2=119, n3=87, all P< 0.05).
Multivariate Analysis
Age, smoking, hypertension, hyperlipidemia, atrial fibrillation, the A2DS2 score, and serum IL-6 concentration were included in a backward stepwise logistic regression model. The results of multivariate analysis showed that the serum IL-6 concentration (odds ratio [OR]: 1.76, 95% confidence interval [CI]: 1.44–1.95, P<0.001) and A2DS2 score (OR: 2.25, 95% CI: 1.17–4.99, P=0.017) were independently associated with SAP after adjusting for age, smoking, hypertension, hyperlipidemia, and atrial fibrillation.
Predictive Value
When the A2DS2 score, serum IL-6 concentration and combination of A2DS2 score and IL-6 were employed to predict SAP, the AUC was 0.824 (SE: 0.026, 95% CI: 0.773–0.875), 0.715 (SE: 0.034, 95% CI: 0.641–0.788) and 0.917 (SE: 0.015, 95% CI: 0.887–0.946), respectively (Figure 1). The AUC of combinative prediction was significantly higher than independent prediction (0.917 vs. 0.824, Z=3.098, P<0.001; 0.917 vs. 0.715, Z=5.436, P<0.001). The clinical utility indexes for the A2DS2 score, serum IL-6 concentration, and combination of the A2DS2 score, and IL-6 in predicting SAP are shown in Table 2.
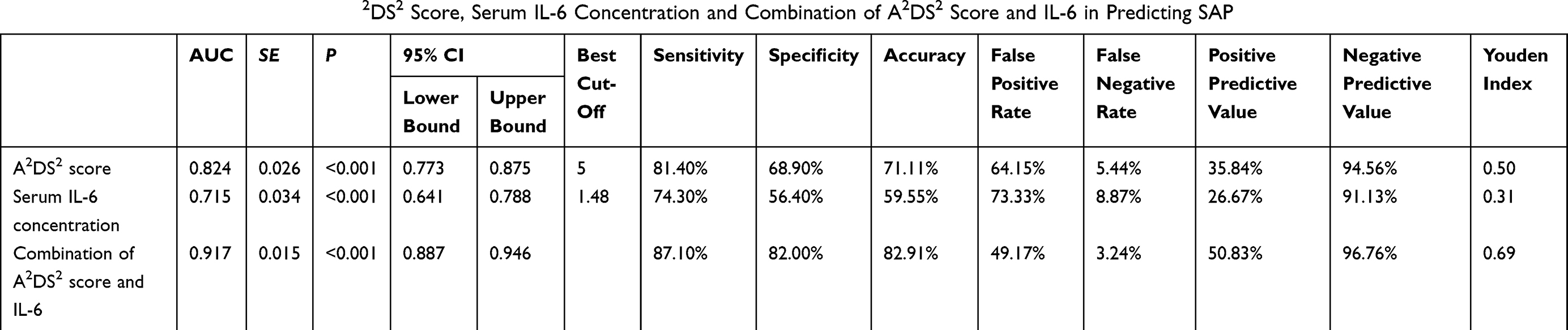 |
Table 2 Clinical Utility Indexes for the A2DS2 Score, Serum IL-6 Concentration and Combination of A2DS2 Score and IL-6 in Predicting SAP |
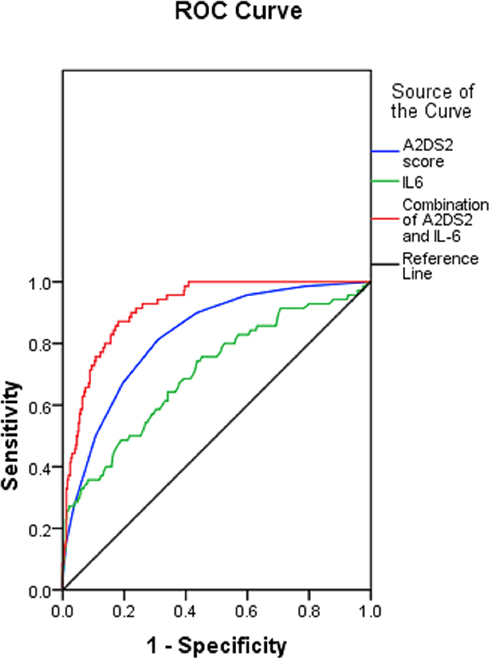 |
Figure 1 ROC curves for the A2DS2 score, serum IL-6 concentration and combination of A2DS2 score and IL-6 in predicting SAP. |
Discussion
SAP refers to pneumonia happening during the first 7 days after the onset of stroke in non-ventilated patients,17 and its incidence is reported to range from 2.3% to 44%.18–21 It is a common and severe complication after acute stroke, associated with increased mortality and length of hospital stay, and poor prognosis.3–6 Studies have shown that SAP can increase the 30-day, 1-year, and 3-year mortality significantly.19,22,23 Patients with SAP have a threefold increased risk in the 30-day mortality after adjusting for severity of admission, compared to patients without SAP.19 Therefore, early detection and appropriate treatment of SAP is of critical importance for reducing mortality and improving the clinical prognosis of stroke patients.
The A2DS2 score, in which scoring items includes age, atrial fibrillation, dysphagia, male sex, and NIHSS,11 has been confirmed to be a simple and effective tool in predicting SAP during hospitalization in several counties, including Spain,12 Singapore,13 France,18 Denmark,24 the UK,25 and China.26–28 The A2DS2 score has a total score of 10. Hoffmann et al demonstrated that the best cut-off of the A2DS2 score was 4.5, and a cut-off of ≥4 had a sensitivity of 91% and a specificity of 57%.11 Li et al showed that the best cut-off of the A2DS2 score was 4.5 when it was applied to the Chinese population, and the AUC was up to 0.836.27 Therefore, the A2DS2 score had a high predictive value. In our study, the AUC of the A2DS2 score applied in predicting SAP was 0.824, and the best cut-off was 5.
Stroke is associated with altered systemic immunity, predisposing patients to infections and immunosuppression.14 Therefore, biomarkers involved in the immune changes and systemic inflammatory response may be able to predict the occurrence of SAP. Pro-inflammatory cytokines have plausible biological actions that predispose towards infection. IL-6 is a pro-inflammatory cytokine and has a significantly elevated level in acute stroke,29 which is correlated with poor prognosis and larger infarct volumes.30–32
IL-6 can activate the production of acute-phase proteins from the liver,33 including activation of CRP production in AIS.34 Thus, it may be associated with defense against infections through the acute phase response. In addition, IL-6 may also play a role in determining cellular immunity. Many studies in animal models and humans have implied that acute stroke may induce depression of the immune system with an elevated susceptibility to infections.35 The characteristics of stroke-caused immunosuppression include impaired cell-mediated immunity and excessive anti-inflammatory cytokines.35 Immunosuppression following stroke may, at least in part, be correlated with catecholamine actions on lymphocytes and mechanistic links exist between the autonomic nervous system, the hypothalamic-pituitary-adrenal axis (HPAA), IL-6 and infection.36–38 Thus, it can be speculated that elevated susceptibility to infections following stroke may, at least partly, be promoted by increased IL-6 levels operating via catecholamines, which in turn cause immunosuppression. Kwan et al demonstrated that patients with SAI, in particular pneumonia, had elevated IL-6 levels and higher mortality, and IL-6 was an independent risk factor of SAI (OR = 19.2, 95% CI: 3.68~100).15 They concluded that IL-6 might be a critical biomarker for the prediction of SAI. In this study, the serum IL-6 concentration was independently associated with occurrence of SAP. The AUC of the serum IL-6 concentration applied in predicting SAP was 0.715, and the best cut-off was 1.48 ng/mL. Moreover, the value of the combination of A2DS2 score and IL-6 in predicting SAP was evaluated. Its AUC was 0.917 with a sensitivity of 87.1% and a specificity of 82.0%, significantly higher than the A2DS2 score or IL-6. The addition of serum IL-6 to the A2DS2 score significantly enhanced the AUC of predicting SAP in AIS patients from the medical ward. In this study, the cost of detecting serum IL-6 concentrations was low (about 25 RMB for each detection). Therefore, serum IL-6 could be applied in screening for SAP in AIS patients from the medical ward.
The limitations of this study included: 1) the sample size was small; and 2) the included patients were from the medical ward; therefore, data characteristics were limited to specific AIS patients.
Conclusion
The addition of serum IL-6 to the A2DS2 score could significantly enhance the AUC of predicting SAP in AIS patients from the medical ward. Therefore, it could be applied in screening for SAP in AIS patients from the medical ward.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
All the authors do not have any conflicts of interest.
References
1. Thrift AG, Thayabaranathan T, Howard G, et al. Global stroke statistics. Int J Stroke. 2017;12(1):13–32. doi:10.1177/1747493016676285
2. Macrez R, Ali C, Toutirais O, et al. Stroke and the immune system: from pathophysiology to new therapeutic strategies. Lancet Neurol. 2011;10(5):471–480. doi:10.1016/S1474-4422(11)70066-7
3. Koennecke HC, Belz W, Berfelde D, et al. Berlin Stroke Register Investigators. Factors influencing in-hospital mortality and morbidity in patients treated on a stroke unit. Neurology. 2011;77(10):965–972. doi:10.1212/WNL.0b013e31822dc795
4. Kishore AK, Vail A, Bray BD, et al. Clinical risk scores for predicting stroke-associated pneumonia: a systematic review. Eur Stroke J. 2016;1(2):76–84. doi:10.1177/2396987316651759
5. Katzan IL, Dawson NV, Thomas CL, et al. The cost of pneumonia after acute stroke. Neurology. 2007;68(22):1938–1943. doi:10.1212/01.wnl.0000263187.08969.45
6. Li Y, Zhang Y, Ma L, et al. Risk of stroke-associated pneumonia during hospitalization: predictive ability of combined A2DS2 score and hyperglycemia. BMC Neurol. 2019;19(1):298. doi:10.1186/s12883-019-1497-x
7. Finlayson O, Kapral M, Hall R, et al. Canadian Stroke Network; Stroke Outcome Research Canada (SORCan) Working Group. Risk factors, inpatient care, and outcomes of pneumonia after ischemic stroke. Neurology. 2011;77(14):1338–1345. doi:10.1212/WNL.0b013e31823152b1
8. Chumbler NR, Williams LS, Wells CK, et al. Derivation and validation of a clinical system for predicting pneumonia in acute stroke. Neuroepidemiology. 2010;34(4):193–199. doi:10.1159/000289350
9. Sellars C, Bowie L, Bagg J, et al. Risk factors for chest infection in acute stroke: a prospective cohort study. Stroke. 2007;38(8):2284–2291. doi:10.1161/STROKEAHA.106.478156
10. Kemmling A, Lev MH, Payabvash S, et al. Hospital acquired pneumonia is linked to right hemispheric periinsular stroke. PLoS One. 2013;8(8):e71141. doi:10.1371/journal.pone.0071141
11. Hoffmann S, Malzahn U, Harms H, et al. Berlin stroke register and the stroke register of Northwest Germany. Development of a clinical score (A2DS2) to predict pneumonia in acute ischemic stroke. Stroke. 2012;43(10):2617–2623. doi:10.1161/STROKEAHA.112.653055
12. Zapata-Arriaza E, Moniche F, Blanca PG, et al. External validation of the ISAN, A2DS2, and AIS-APS scores for predicting stroke-associated pneumonia. J Stroke Cerebrovasc Dis. 2018;27(3):673–676. doi:10.1016/j.jstrokecerebrovasdis.2017.09.059
13. Tu TM, Phua SS, Acharyya S, et al. Predicting pneumonia in acute ischaemic stroke: comparison of five prediction scoring models. Ann Acad Med Singapore. 2017;46(6):237–244.
14. Meisel C, Schwab JM, Prass K, et al. Central nervous system injury-induced immune deficiency syndrome. Nat Rev Neurosci. 2005;6(10):775–786. doi:10.1038/nrn1765
15. Kwan J, Horsfield G, Bryant T, et al. IL-6 is a predictive biomarker for stroke associated infection and future mortality in the elderly after an ischemic stroke. Exp Gerontol. 2013;48(9):960–965. doi:10.1016/j.exger.2013.07.003
16. Garner JS, Jarvis WR, Emori TG, et al. CDC definitions for nosocomial infections, 1988. Am J Infect Control. 1988;16(3):128–140. doi:10.1016/0196-6553(88)90053-3
17. Smith CJ, Kishore AK, Vail A, et al. Diagnosis of stroke-associated pneumonia: recommendations from the pneumonia in stroke consensus group. Stroke. 2015;46(8):2335–2340. doi:10.1161/STROKEAHA.115.009617
18. Cugy E, Sibon I. Stroke-associated pneumonia risk score: validity in a French stroke unit. J Stroke Cerebrovasc Dis. 2017;26(1):225–229. doi:10.1016/j.jstrokecerebrovasdis.2016.09.015
19. Katzan IL, Cebul RD, Husak SH, et al. The effect of pneumonia on mortality among patients hospitalized for acute stroke. Neurology. 2003;60(4):620–625. doi:10.1212/01.WNL.0000046586.38284.60
20. Langhorne P, Stott DJ, Robertson L, et al. Medical complications after stroke: a multicenter study. Stroke. 2000;31(6):1223–1229. doi:10.1161/01.STR.31.6.1223
21. Ji R, Shen H, Pan Y, et al. China National Stroke Registry Investigators. Novel risk score to predict pneumonia after acute ischemic stroke. Stroke. 2013;44(5):1303–1309. doi:10.1161/STROKEAHA.111.000598
22. Ingeman A, Andersen G, Hundborg HH, et al. In-hospital medical complications, length of stay, and mortality among stroke unit patients. Stroke. 2011;42(11):3214–3218. doi:10.1161/STROKEAHA.110.610881
23. Yu YJ, Weng WC, Su FC, et al. Association between pneumonia in acute stroke stage and 3-year mortality in patients with acute first-ever ischemic stroke. J Clin Neurosci. 2016;33:124–128. doi:10.1016/j.jocn.2016.02.039
24. Jeon CY, Furuya EY, Berman MF, et al. The role of pre-operative and post-operative glucose control in surgical-site infections and mortality. PLoS One. 2012;7(9):e45616. doi:10.1371/journal.pone.0045616
25. Smith CJ, Bray BD, Hoffman A, et al. Intercollegiate Stroke Working Party Group. Can a novel clinical risk score improve pneumonia prediction in acute stroke care? A UK multicenter cohort study. J Am Heart Assoc. 2015;4(1):e001307. doi:10.1161/JAHA.114.001307
26. Zhang X, Yu S, Wei L, et al. The A2DS2 score as a predictor of pneumonia and in-hospital death after acute ischemic stroke in Chinese populations. PLoS One. 2016;11(3):e0150298. doi:10.1371/journal.pone.0150298
27. Li Y, Song B, Fang H, et al. External validation of the A2DS2 score to predict stroke-associated pneumonia in a Chinese population: a prospective cohort study. PLoS One. 2014;9(10):e109665. doi:10.1371/journal.pone.0109665
28. Lu Y, Liu XY, Chen YJ, et al. Serum iron and A(2)DS(2) score in stroke-associated pneumonia. Int J Clin Exp Med. 2015;8(4):6163–6170.
29. Pera J, Zawadzka M, Kaminska B, et al. Influence of chemical and ischemic preconditioning on cytokine expression after focal brain ischemia. J Neurosci Res. 2004;78(1):132–140. doi:10.1002/jnr.20232
30. Smith CJ, Emsley HC, Gavin CM, et al. Peak plasma interleukin-6 and other peripheral markers of inflammation in the first week of ischaemic stroke correlate with brain infarct volume, stroke severity and long-term outcome. BMC Neurol. 2004;4:2. doi:10.1186/1471-2377-4-2
31. Smith CJ, Emsley HC, Vail A, et al. Variability of the systemic acute phase response after ischemic stroke. J Neurol Sci. 2006;251(1–2):77–81. doi:10.1016/j.jns.2006.09.011
32. Whiteley W, Wardlaw J, Dennis M, et al. The use of blood biomarkers to predict poor outcome after acute transient ischemic attack or ischemic stroke. Stroke. 2012;43(1):86–91. doi:10.1161/STROKEAHA.111.634089
33. Ramadori G, Christ B. Cytokines and the hepatic acute-phase response. Semin Liver Dis. 1999;19(2):141–155. doi:10.1055/s-2007-1007106
34. Waje-Andreassen U, Kråkenes J, Ulvestad E, et al. IL-6: an early marker for outcome in acute ischemic stroke. Acta Neurol Scand. 2005;111(6):360–365. doi:10.1111/j.1600-0404.2005.00416.x
35. Haeusler KG, Schmidt WU, Föhring F, et al. Cellular immunodepression preceding infectious complications after acute ischemic stroke in humans. Cerebrovasc Dis. 2008;25(1–2):50–58. doi:10.1159/000111499
36. Johansson A, Olsson T, Carlberg B, et al. Hypercortisolism after stroke–partly cytokine-mediated? J Neurol Sci. 1997;147(1):43–47. doi:10.1016/S0022-510X(96)05308-7
37. Harms H, Reimnitz P, Bohner G, et al. Influence of stroke localization on autonomic activation, immunodepression, and post-stroke infection. Cerebrovasc Dis. 2011;32(6):552–560. doi:10.1159/000331922
38. Szczudlik A, Dziedzic T, Bartus S, et al. Serum interleukin-6 predicts cortisol release in acute stroke patients. J Endocrinol Invest. 2004;27(1):37–41. doi:10.1007/BF03350908
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.