")
Back to Journals » International Journal of General Medicine » Volume 14
Value-Added Roles of Medical Students During the COVID-19 Pandemic: Assessment of Medical Students’ Perceptions and Willingness in Sri Lanka
Authors Wickramasinghe ND , Jayarathne SW, Pilapitiya SD
Received 23 May 2021
Accepted for publication 16 June 2021
Published 5 July 2021 Volume 2021:14 Pages 3187—3196
DOI https://doi.org/10.2147/IJGM.S309021
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Nuwan Darshana Wickramasinghe,1 Shamalee Wasana Jayarathne,2 Senaka Devendra Pilapitiya3
1Department of Community Medicine, Faculty of Medicine and Allied Sciences, Rajarata University of Sri Lanka, Saliyapura, 50008, Sri Lanka; 2Medical Education Unit, Faculty of Medicine and Allied Sciences, Rajarata University of Sri Lanka, Saliyapura, 50008, Sri Lanka; 3Department of Medicine, Faculty of Medicine and Allied Sciences, Rajarata University of Sri Lanka, Saliyapura, 50008, Sri Lanka
Correspondence: Nuwan Darshana Wickramasinghe
Department of Community Medicine, Faculty of Medicine and Allied Sciences, Rajarata University of Sri Lanka, Saliyapura, 50008, Sri Lanka
Tel +94772975412
Fax +942522234464
Email [email protected]
Purpose: Since the coronavirus disease 2019 (COVID-19) pandemic is an opportune time to introduce the value-added roles of medical students, this study assessed medical students’ perceptions and willingness to assist in COVID-19 health sector preparedness and response via value-added roles in Sri Lanka.
Methods: A cross-sectional online survey was conducted among all medical students studying in six batches of the Faculty of Medicine and Allied Sciences, Rajarata University of Sri Lanka, in June 2020. A Google form in English with 10 statements about individual perceptions of medical students’ roles and their willingness to assist in the COVID-19 health sector response via value-added roles was used to collect data. The responses were recorded on a five-point Likert scale. The chi-squared test for independence was used to explore the associations between the academic year and the responses to each statement.
Results: Out of 856 (response rate 79.6%) study participants, the majority were females (n=601, 70.2%). The majority (n=804, 93.9%) reported that they have a responsibility to contribute to the country’s COVID-19 health sector response. There was a statistically significant association between medical students’ perceived level of clinical knowledge, having the clinical skills to assist in the COVID-19 health sector response and academic year (p< 0.001). The commonly identified value-added roles were developing (n=770, 89.9%) and disseminating (n=744, 86.9%) health education messages, and field contact tracing activities (n=653, 76.3%). Other value-added roles were assisting the curative health sector in COVID-19 patient management (n=380, 44.4%) and other non-COVID-19 patient management (n=463, 54.1%).
Conclusion: Medical students are mostly willing to engage in preventive health sector value-added roles and, to a lesser extent, in curative health sector value-added roles during the COVID-19 outbreak. However, medical educators need to clearly define the value-added roles and provide adequate training and supervision for medical students across academic years to enable them to combine learning with making meaningful contributions to the health-care system during the COVID-19 pandemic.
Keywords: COVID-19, health sector response, medical students, Sri Lanka, value-added roles
Introduction
As a result of the coronavirus disease 2019 (COVID-19) pandemic, the world is experiencing one of the greatest threats to the global education system at the moment, which could potentially lead to a gigantic educational crisis. Across the globe, many governments have temporarily closed educational institutions, including medical faculties and colleges, in an attempt to contain the spread of the COVID-19 pandemic.1–6
Against the ever-increasing COVID-19 caseload, the health-care sectors of countries across the globe are faced with an inevitable risk of medical demand outpacing the health-care capacity.1,7 Thus, country-specific health sector preparedness and response plans to COVID-19 need to be proactively developed by effectively utilizing the limited resources.7,8 With regard to human resources in the COVID-19 health sector preparedness and response, medical students could be considered as a potential group that could be effectively utilized. Evidence suggests that deployment of the enthusiastic medical student workforce will supplement and expedite the process of existing health-care interventions during the COVID-19 pandemic.9
However, there is no universal consensus on the appropriate roles for medical students during a pandemic; thus, their involvement in health sector responses in countries across the world is different.4,5,10,11 The literature highlights a paradoxical dual role of medical students during the COVID-19 pandemic.12 On one hand, as the future health-care workforce, they potentially form part of a health-care system’s response to public health emergencies, while on the other hand, they are considered as non-essential in clinical delivery.12
Given the novelty of this COVID-19 pandemic, it is evident that the medical schools are ill prepared to respond promptly and comprehensively to a pandemic of such proportions. Hence, it is timely and vital to identify how medical students can contribute to the health sector preparedness and response, which includes both the preventive sector and curative sector. It is an opportune time for the medical schools to define the competency level of each year of medical students to prepare and respond to global health emergencies. The competency level definition and identification process needs to incorporate the inputs from both medical students and academia, which will ultimately facilitate the development of a strategic plan to respond to similar conditions in the future to assist the health-care sector.
The COVID-19 pandemic has provided us with an opportunity to consider the immersion of medical students in the health-care system in Sri Lanka. The “communities of practice” theory of medical education highlights the importance of learning by participation, rather than learning by acquisition, where the mode of learning is authentic work.13 Furthermore, it is suggested that medical schools should offer clinical opportunities to students that would benefit patient care and potentially help to prevent workforce shortages during the COVID-19 pandemic.4 Hence, the COVID-19 pandemic could be a great opportunity for medical students to learn and develop their management skills and personal skills, and to appreciate the importance of the multidisciplinary approach in health-care delivery.
Against this background, we believe that the concept of “value-added medical education” needs to be promoted by global medical educators in view of transforming medical students’ roles into value-added roles, which are defined as
Roles that are experiential and authentic, and have the potential for a positive impact on outcomes related to patients, populations, costs of care, or other processes within the health-care system, and enhance student knowledge, attitudes, and skills in the clinical science.14–16
Since the concept of value-added roles of medical students is relatively novel, the global literature on the concept is limited. Nonetheless, students serving as patient navigators/health coaches, care transition facilitators, population health managers and quality improvement team extenders have been identified as novel value-added roles of medical students.14 More specifically, scant evidence on value-added roles of medical students during the COVID-19 pandemic suggests that in clinical settings, medical students could assist in routine outpatient clinical care and assist in providing care in inpatient services with non-COVID-19 patients.4 In addition, roles such as curating health messages, public health education of different groups in society, assisting health teams to instruct local communities and providing basic health-care services for vulnerable groups are also identified as important value-added roles of medical students during the COVID-19 pandemic.17
Prior to considering the ways of immersing medical students in the health-care systems, it is important to assess the willingness of medical students to contribute to the health sector response to the COVID-19 pandemic. However, global evidence exploring this aspect is scarce. Despite the lack of evidence generated by original research, opinion-based evidence suggests that medical students from varying clinical contexts have expressed their willingness to contribute to the health-care systems during the COVID-19 pandemic.12,18
With regard to the Sri Lankan scenario, the first confirmed case of COVID-19, in a Chinese national, was reported on 27 January 2020 and the first confirmed local case was reported on 11 March 2020.19 The Sri Lankan government implemented both suppression and mitigation measures at the onset of the COVID-19 outbreak in Sri Lanka in a cascading manner, which were reasonably effective for a sustained period in the prevention of widespread community transmission.19,20
At the moment, the Sri Lankan health sector is managing the disease burden of COVID-19 with available human as well as physical resources, largely owing to the fact that there is still no widespread community transmission, which has been attributed to strict suppression and mitigation measures.20 If the health sector is not fully prepared with proactive measures, including effective utilization of any available human resources, the country will find it extremely difficult to cope with the inevitable subsequent waves of the COVID-19 outbreak.
Against this background, it is important to identify the perceptions and willingness of medical students to contribute to the COVID-19 health sector preparedness and response via value-added roles in order to utilize the services of this potential workforce effectively in the future. Hence, the aim of the present study was to assess the medical students’ perceptions and willingness to assist in the COVID-19 health sector preparedness and response via value-added roles in a state-sector medical faculty in Sri Lanka.
Materials and Methods
Study Design and Setting
We carried out a cross-sectional online survey among the medical students at the Faculty of Medicine and Allied Sciences (FMAS), Rajarata University of Sri Lanka (RUSL), for a period of 2 weeks in early June 2020.
At present, six batches of medical students are studying in the FMAS, RUSL. The FMAS is one of the 11 state-sector medical faculties in Sri Lanka. The academic programme is conducted (in English) over a period of 5 years and it consists of four main phases: foundation for medical studies, pre-clinical, para-clinical and clinical phases. The foundation phase is designed to make students familiar with the university setting, to improve their life skills and learning skills, and to make them aware of the basic aspects of medical ethics and professionalism. During the pre-clinical phase, students will acquire basic knowledge and skills in relation to the normal structures and functions of the human body, and the basis for dysfunction. Students obtain theoretical, practical and management knowledge of abnormal structures and functions of the human body during their para-clinical phase. Comprehensive clinical training starts from the third year of the academic programme.
Participants
At present, there are 1075 medical students studying in all six batches in the FMAS, RUSL. Of them, the majority are female students (n=721, 67.1%). We invited all medical students in all six batches (without any exclusion criteria) to participate in the study and we requested those who consented to complete the online survey.
Measures
A multidisciplinary panel of experts representing the fields of medical education, public health and clinical medicine prepared the questionnaire. We perused existing literature related to medical education to identify the potential value-added roles of medical students during the COVID-19 pandemic. Based on the available literature,4,14,17 different context-specific activities related to value-added roles of medical students during the COVID-19 pandemic, which could be easily incorporated into medical education in Sri Lanka, were selected by the expert panel to be considered in the present study.
We prepared a Google form in English, comprising 10 statements about individual medical students’ perceptions and willingness to contribute to the COVID-19 health sector preparedness and response via value-added roles, for data collection. Participants’ responses to each questionnaire item (statement) were recorded on a five-point Likert scale to indicate the extent to which they agreed with the item. We uploaded the online survey to the Moodle, which is the Learning Management System of the faculty, in order to provide an opportunity for easy accessibility by the remote participants. Enrolment in the study was completely voluntary and we attached an online invitation to participate the study to the Google form with details of the study and the basic sections of the questionnaire. We obtained online informed consent from participants prior to completion of the questionnaire. We did not collect any personally identifiable information and we preserved the students’ anonymity.
The fact that experts in the fields of medical education, public health and clinical medicine were involved in this process ensured the judgemental validity of the questionnaire. Out of the 10 statements, seven (statements 2–8) were directly focused on assessing the perceived competencies of medical students to contribute to the COVID-19 health sector response. Reliability assessment of the scale revealed high internal consistency, with a Cronbach’s alpha of 0.742.
Data Analysis
We performed data analysis using IBM SPSS Statistics for Macintosh, version 25.0. We used descriptive statistics with frequency distributions and graphs to present the data. Participants’ responses on the five-point Likert scale for each questionnaire item were dichotomized as “Agree” (by combining the responses “agree” and “strongly agree”) and “Disagree” (by combining the responses “neither agree nor disagree”, “disagree” and “strongly disagree”). Participants’ responses were analysed for the total sample and also according to the academic year of the participants. The chi-squared test for independence was used to explore the association between the academic year and the responses to each statement.
Ethics Approval and Consent to Participate
Ethical clearance to conduct the study was obtained from the Ethics Review Committee of the Faculty of Medicine and Allied Sciences, Rajarata University of Sri Lanka (reference no ERC/2020/40). Informed consent was obtained from all participants prior to online data collection.
Results
Sample Characteristics
A total of 856 medical students completed the online questionnaire and the response rate was 79.6%. The majority were female medical students (n=601, 70.2%). The breakdown of the sample by academic year is given in Figure 1 and fourth year medical students represented the highest percentage (n=180, 21.0%).
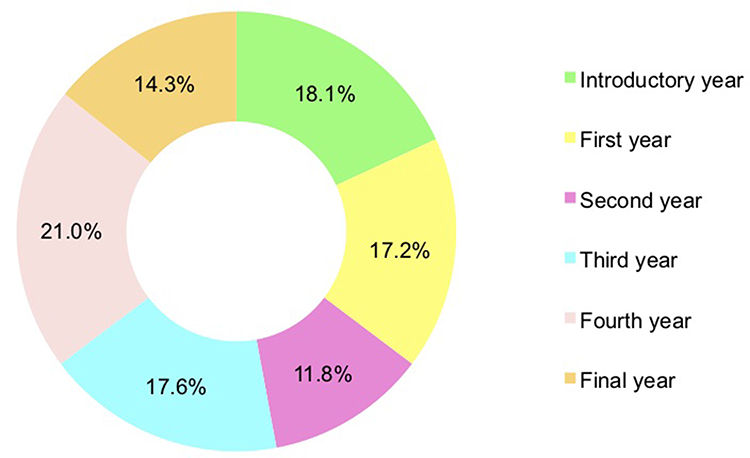 |
Figure 1 Sample of medical students by academic year (n=856). |
Table 1 summarizes the male and female medical students in the sample by academic year.
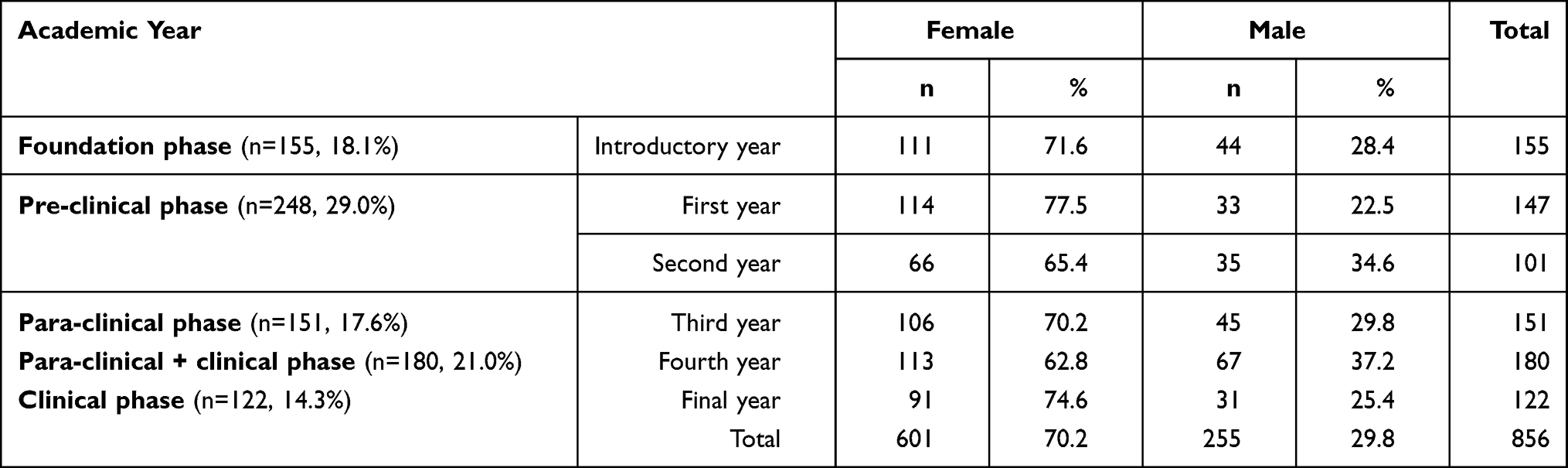 |
Table 1 Sample of Medical Students by Sex and by Academic Year |
Overall Responses of the Sample of Medical Students
The percentage agreements for each of the 10 statements by the sample of medical students are given in Figure 2. The majority (93.9%, n=804) reported that they have a responsibility to contribute to the COVID-19 health sector response in the country.
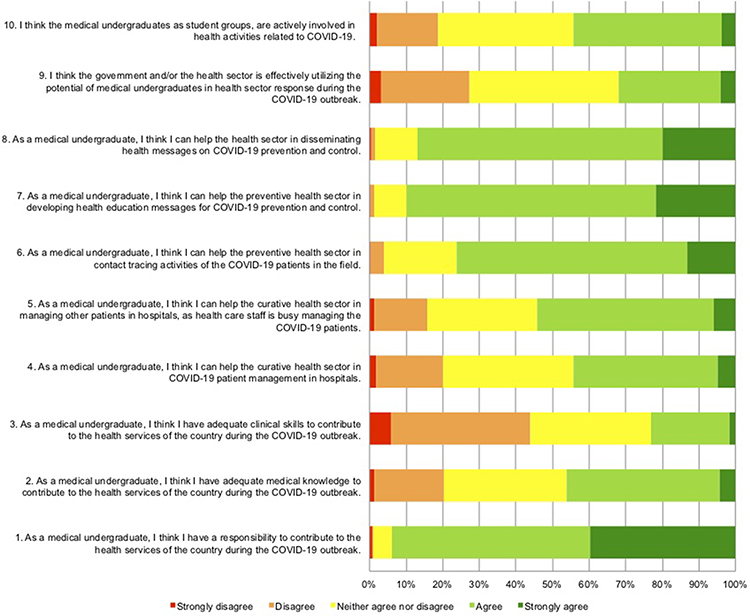 |
Figure 2 Response to each statement by medical students (n=856). |
In relation to the perceived competencies, 46.3% (n=396) believed that they possess adequate medical knowledge to contribute to the COVID-19 health sector response, while only 23.1% (n=198) believed they have adequate clinical skills to contribute effectively.
Regarding the potential value-added roles, the majority reported that they could help in the preventive health sector activities during the COVID-19 outbreak. Most of the students believed that they could assist/participate in developing health education messages (n=770, 89.9%), disseminating health messages (n=744, 86.9%) and field contact tracing activities of the COVID-19 patients (n=653, 76.3%).
In comparison to the responses on value-added roles in preventive health sector activities, a lower percentage of medical students reported that they could assist in the curative health sector activities during the COVID-19 outbreak. Only 44.4% (n=380) believed that they could assist in COVID-19 patient management in the hospitals and 54.1% (n=463) believed that they could assist the curative health sector in managing other patients in hospitals, as health-care staff is busy managing the COVID-19 patients.
Overall, 32.0% (n=274) believed that the government and/or the health sector is/are effectively utilizing the potential of medical students in the health sector response during the COVID-19 outbreak. Compared to that response, a higher percentage of medical students (n=380, 44.4%) believed that medical students, as student groups, are actively involved in health activities related to COVID-19.
Responses of the Sample of Medical Students by Academic Year
The percentage agreements for each of the 10 statements by the sample of medical students according to academic year are summarized in Table 2 and Figure 3.
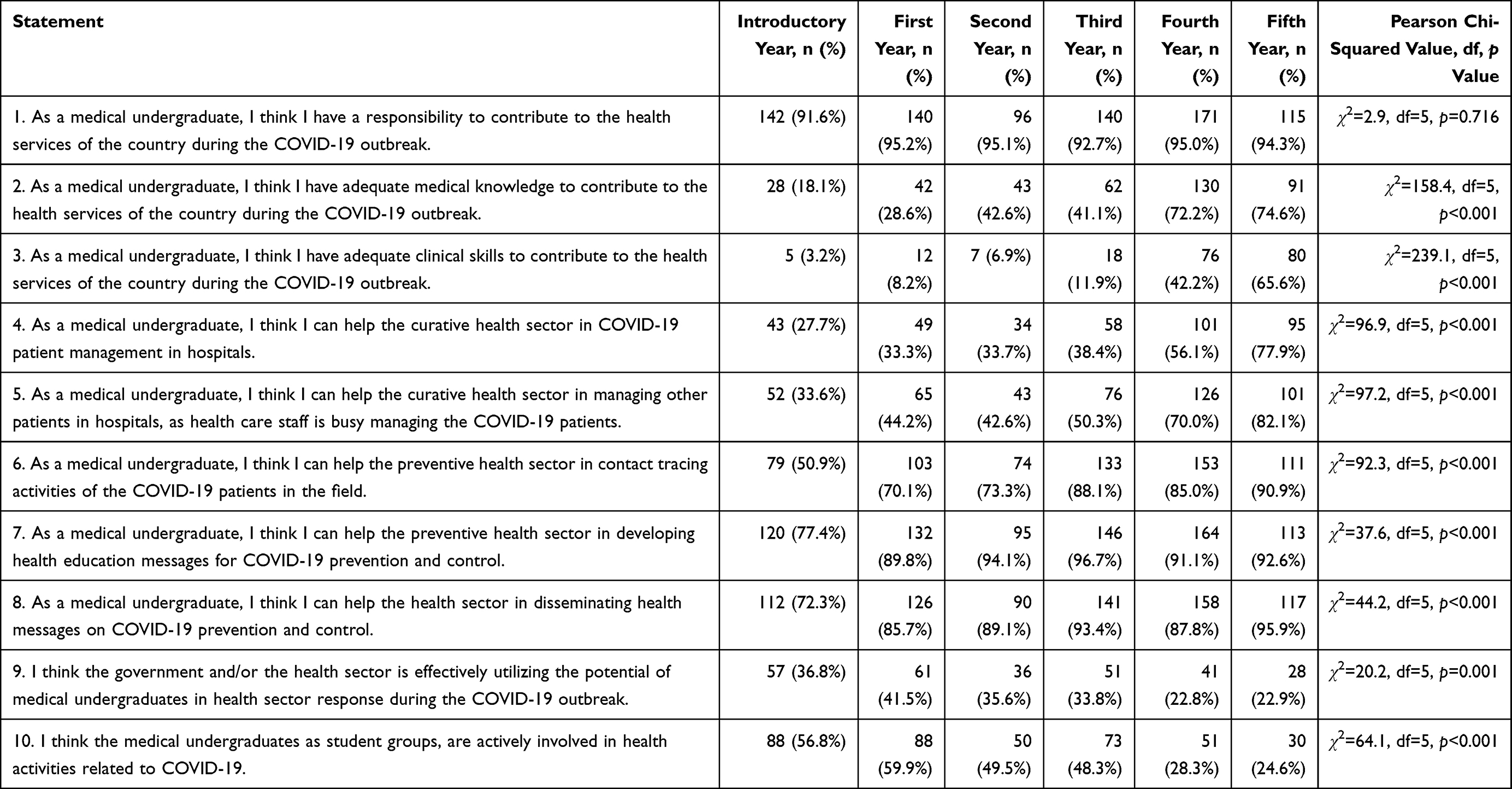 |
Table 2 Medical Students’ Responses to Each Statement by Academic Year |
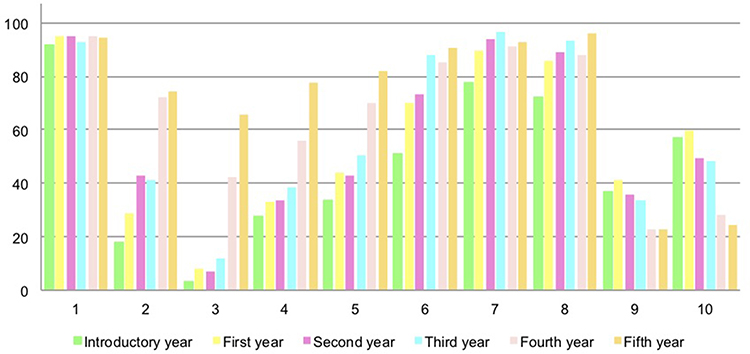 |
Figure 3 Medical students’ responses to each statement by academic year. |
Irrespective of the academic year of study, almost all medical students reported that they have a responsibility to contribute to the health services of the country during the COVID-19 outbreak, and the responses varied from 91.6% to 95.2%. A chi-squared test for independence indicated no statistically significant association between the academic year and responses (χ2(5)=2.9, p=0.716).
It is worth observing that with advancing academic year, the medical students’ perceived level of clinical knowledge and clinical skills to assist in the COVID-19 health sector response increased. The percentage increased from 18.1% in the introductory year to 74.6% in the fifth year regarding the clinical knowledge. A chi-squared test for independence indicated a statistically significant association between the academic year and perceived level of clinical knowledge (χ2(5)=158.4, p<0.001). A more striking difference, from 3.2% in the introductory year to 65.6% in the fifth year, was observed regarding perceived level of clinical skills (χ2(5)=239.1, p<0.001). Additional analyses to assess the association between the phase of academic training (namely, pre-clinical, para-clinical and clinical phases) and perceived level of clinical knowledge (χ2(2)=143.5, p<0.001), and the association between the phase of academic training and perceived level of clinical skills (χ2(2)=215.7, p<0.001), revealed statistically significant associations.
In relation to the perceived ability to contribute to the health sector response, an increasing trend was observed with advancing academic years regarding the perceived ability to contribute to the curative health sector activities. However, a similar increasing trend was not observed in relation to the perceived ability to contribute to the preventive health sector activities.
On the other hand, with advancing academic years a lower number of medical students believed that the government and/or the health sector is/are effectively utilizing the potential of medical students in the health sector response during the COVID-19 outbreak. The association between academic year and responses was found to be statistically significant (χ2(5)=20.2, p=0.001). Similarly, with advancing academic years, a lower number of medical students believed that medical students, as student groups, are actively involved in health activities related to the COVID-19 outbreak (χ2(5)=64.1, p<0.001).
Discussion
Global medical education has faced numerous challenges in continuing traditional teaching–learning activities owing to the COVID-19 pandemic. Hence, this is an opportune time to identify value-added roles of medical students to benefit students, patients and the health systems across the globe. Against this backdrop, the present study aimed to assess medical students’ perceptions of their role and willingness to assist in the COVID-19 health sector preparedness and response.
Accordingly, a cross-sectional study was conducted via the Moodle platform, considering its easy accessibility to the study participants. In addition, experts representing the fields of medical education, public health and clinical medicine prepared the study questionnaire, specifically focusing on simplicity, while including important value-added roles. The majority of the sample were female students and the proportion was similar to that in the student population of FMAS, RUSL.
A study conducted among medical students in Brazil revealed that the sense of purpose or duty, which reflects the moral values linked to the medical profession, was the most important factor that influenced medical students’ desire to work during the COVID-19 pandemic.21 Similarly, in the present study, almost all medical students reported that they have a responsibility to contribute to the COVID-19 health sector response in Sri Lanka, which indirectly highlights their academic and moral obligation. Further, it is important to note that irrespective of the academic year, all medical students were of a similar opinion. In spite of their willingness to be involved in the COVID-19 health sector response, only one-third of students believed that the government and/or the health sector is/are effectively utilizing the potential of medical students in the health sector response during the COVID-19 outbreak. In the context of identifying the readiness to engage in value-added roles, this evidence provides a positive base.
More than twice as many students perceived that they have adequate clinical knowledge in comparison to adequate clinical skills to contribute to the COVID-19 health sector response. Furthermore, with advancing academic year, the medical students’ perceived level of clinical knowledge and clinical skills to assist in the COVID-19 health sector response increased. At the same time, it is important to appreciate the very low level of perceived adequacy of clinical knowledge and skills among the students in the foundation and pre-clinical phases. This observation can be explained by the students in the foundation and pre-clinical phases having minimal exposure to clinical appointments. These findings are in line with the findings of the study conducted among medical students in Brazil, which also revealed increasing perceived competency with advancing academic year. Furthermore, the self-perception of competence is reported as one of the leading factors influencing medical students’ motivation to engage in health-care activities during the COVID-19 pandemic.21 This finding highlights that students can be better integrated into health-care teams by recognizing their meaningful contribution from the first year to the final year. Thus, medical education needs to identify value-added roles for medical students across different levels of academic training in order to combine learning with meaningful contributions to patient care and the health sector.
With regard to potential value-added roles, the majority of medical students reported their willingness, mainly in relation to the preventive sector activities, irrespective of their academic year. Given that these value-added roles, which include developing and disseminating health messages and field contact tracing, need relatively minimal training and supervision, health-care teams could easily incorporate medical students in such activities to reinforce the existing health-care workforce. The importance of having opportunities to incorporate creativity in medical education is widely recognized.21–24 Hence, the involvement of the creative and energetic younger health workforce could be a fruitful investment in this regard.
During the COVID-19 pandemic, clinical teaching and training has been greatly affected;4,6,25 thus, the introduction of value-added activities in clinical settings would be of high significance and would also yield reciprocal benefits. Evidence suggests that opportunities created for medical students to actively engage in the COVID-19 pandemic would reinforce vital values in medical education, such as altruism, service experience during a critical period, professional solidarity and a disposition to serve society.4,21 According to the communities of practice theory, this allows learning by participation rather than learning by acquisition for medical students. However, considering the competency gap in their perceived level of relevant clinical knowledge and skills, such activities need to be carried out under meticulous supervision in safe working environments. In light of the findings of the present study, providing more opportunities and training in managing other patients in hospitals for final year medical students, as health-care staff is busy managing the COVID-19 patients, would be beneficial to manage the work overload in clinical health-care settings.
Limitations
There are some limitations related to the study that need to be taken into consideration in interpreting the results. Given that the present study was conducted in a single medical faculty in Sri Lanka, generalization of the findings to other settings needs to be done with caution, considering educational and cultural differences. Even though the response rate of the study was approximately 80%, which is relatively high in comparison to the response rates reported in online surveys, the possibility of non-respondents having different perceptions has not been explored in this study. In addition, since medical students in the foundation and pre-clinical phases have minimal exposure to clinical appointments, the statements on perceived level of clinical skills and perceived ability to assist in patient care have limited applicability to that student group.
Conclusion
Medical students believe that they have a responsibility to contribute to the COVID-19 health sector response in Sri Lanka. They are mostly willing to be engaged in preventive health sector value-added roles and to a lesser extent in curative health sector value-added roles during the COVID-19 outbreak. Furthermore, with advancing academic year, the medical students’ perceived level of clinical knowledge and clinical skills to assist in the COVID-19 health sector response increased. In this context, medical educators need to clearly define the value-added roles and provide adequate training and supervision for medical students, from the first year to the final year, to combine learning with meaningful contributions to patient care and the health-care system during the COVID-19 pandemic. Furthermore, with the predictions of the COVID-19 pandemic overwhelming the existing health-care systems across the globe, it is important that policy makers consider how to deploy medical students optimally within health-care systems.
Abbreviations
COVID-19, coronavirus disease 2019; FMAS, Faculty of Medicine and Allied Sciences; RUSL, Rajarata University of Sri Lanka.
Acknowledgment
The authors wish to thank all medical students who participated in this study.
Disclosure
The authors report no conflicts of interest in this work. This research received no specific grants from any funding agency in the public, commercial or not-for-profit sectors.
References
1. Bank I, Wijnen-Meijer M. Why should medical students (not) be recruited to care for patients with COVID-19? BMC Med Educ. 2020;20(1):1–5. doi:10.1186/s12909-020-02261-8
2. Yu NZ, Li ZJ, Chong YM, et al. Chinese medical students’ interest in COVID-19 pandemic. World J Virol. 2020;9(3):38. doi:10.5501/wjv.v9.i3.38
3. Armstrong A, Jeevaratnam J, Murphy G, et al. A plastic surgery service response to COVID-19 in one of the largest teaching hospitals in Europe. J Plast Reconstr Aesthet Surg. 2020;73(6):1174–1205. doi:10.1016/j.bjps.2020.03.027
4. Miller DG, Pierson L, Doernberg S. The role of medical students during the COVID-19 pandemic. Ann Intern Med. 2020;173(2):145–146. doi:10.7326/M20-1281
5. Mahase E. Covid-19: portugal closes all medical schools after 31 cases confirmed in the country. BMJ. 2020;368:M986. doi:10.1136/bmj.m986
6. Rose S. Medical student education in the time of COVID-19. JAMA. 2020;323(21):2131–2132. doi:10.1001/jama.2020.5227
7. Walker PG, Whittaker C, Watson OJ, et al. The impact of COVID-19 and strategies for mitigation and suppression in low-and middle-income countries. Science. 2020;369(6502):413–422. doi:10.1126/science.abc0035
8. World Health Organization. Responding to community spread of COVID-19: interim guidance; 2020.
9. Hasan MT. Considering voluntary contribution of medical students to tackle COVID-19 crisis at hospitals in Bangladesh & similar settings. PsyArXiv. 2020.
10. Stokes DC. Senior medical students in the COVID-19 response: an opportunity to be proactive. Acad Emerg Med. 2020;27(4):343–345. doi:10.1111/acem.13972
11. Harvey A. Covid-19: medical students and FY1 doctors to be given early registration to help combat covid-19. BMJ. 2020;368:m1268. doi:10.1136/bmj.m1268
12. Baker DM, Bhatia S, Brown S, et al. Medical student involvement in the COVID-19 response. Lancet. 2020;395(10232):1254. doi:10.1016/S0140-6736(20)30795-9
13. Morris CS. On communities of practice in medical education. Acad Med. 2018;93(12):1752. doi:10.1097/ACM.0000000000002462
14. Gonzalo JD, Dekhtyar M, Hawkins RE, Wolpaw DR. How can medical students add value? Identifying roles, barriers, and strategies to advance the value of undergraduate medical education to patient care and the health system. Acad Med. 2017;92(9):1294–1301. doi:10.1097/ACM.0000000000001662
15. Gonzalo JD, Dekhtyar M, Starr SR, et al. Health systems science curricula in undergraduate medical education: identifying and defining a potential curricular framework. Acad Med. 2017;92(1):123–131. doi:10.1097/ACM.0000000000001177
16. Gonzalo JD, Graaf D, Johannes B, Blatt B, Wolpaw DR. Adding value to the health care system: identifying value-added systems roles for medical students. Am J Med. 2017;32(3):261–270.
17. Patrinely JR, Zakria D, Berkowitz ST, Johnson DB, Totten DJ. COVID-19: the emerging role of medical student involvement. Med Sci Educ. 2020;30(4):1641–1643. doi:10.1007/s40670-020-01052-6
18. Thomson E, Lovegrove S. ‘Let us Help’—Why senior medical students are the next step in battling the COVID-19 pandemic. Int J Clin Pract. 2020;74:e13516. doi:10.1111/ijcp.13516
19. Hewage S, Wickramasinghe N, Jayakody S, Samaranayake D, Prathapan S, Arambepola C. Social distancing and its impact on flattening the COVID-19 curve in Sri Lanka. JCCPSL. 2020;26(1):65–70.
20. Ediriweera DS, de Silva NR, Malavige NG, de Silva HJ. An epidemiological model to aid decision-making for COVID-19 control in Sri Lanka. medRxiv. 2020.
21. Tempski P, Arantes-Costa FM, Kobayasi R, et al. Medical students’ perceptions and motivations during the COVID-19 pandemic. PLoS One. 2021;16(3):e0248627. doi:10.1371/journal.pone.0248627
22. Green MJ, Myers K, Watson K, Czerwiec MK, Shapiro D, Draus S. Creativity in medical education: the value of having medical students make stuff. J Med Humanit. 2016;37(4):475–483. doi:10.1007/s10912-016-9397-1
23. Kim Y, Lee YH. Creativity in medical education: concepts related to creative capacity. Yeungnam Univ J Med. 2020;37(2):79. doi:10.12701/yujm.2019.00458
24. Shaywitz DA, Ausiello DA. Preserving creativity in medicine. PLoS Med. 2004;1(3):e34. doi:10.1371/journal.pmed.0010034
25. Roll R, Chiu M, Huang C. Answering the call to action: COVID-19 curriculum design by students for students. Acad Med. 2020;95(11):e6–e6. doi:10.1097/ACM.0000000000003588
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.