")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 13
Validity of Anthropometric Cut-Offs for Early Diagnosis of Dyslipidemia Among Ethiopian Adults
Authors Kenate S, Tesfaye T , Berhanu Mogas S , Zawdie B , Tesfaye Y , Dadi LS , Tadesse M, Kebede A , Gudina EK , Tamiru D
Received 22 August 2020
Accepted for publication 29 September 2020
Published 20 October 2020 Volume 2020:13 Pages 3831—3837
DOI https://doi.org/10.2147/DMSO.S278291
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Antonio Brunetti
Sileshi Kenate,1 Temamen Tesfaye,2 Solomon Berhanu Mogas,3 Belay Zawdie,4 Yonas Tesfaye,2 Lelisa Sena Dadi,3 Mulualem Tadesse,5 Ayantu Kebede,3 Esayas Kebede Gudina,6 Dessalegn Tamiru4
1Jimma Town Health Office, Jimma, Ethiopia; 2School of Nursing, Jimma University, Jimma, Ethiopia; 3Department of Epidemiology, Jimma University, Jimma, Ethiopia; 4Department of Nutrition and Dietetics, Jimma University, Jimma, Ethiopia; 5Department of Medical Laboratory Sciences, Jimma University, Jimma, Ethiopia; 6Department of Internal Medicine, Jimma University, Jimma, Ethiopia
Correspondence: Dessalegn Tamiru
Department of Nutrition and Dietetics, Jimma University, P. O. Box-378, Jimma, Oromia Region, Ethiopia
Tel +251912373397
Email [email protected]
Introduction: Lack of regional- and local-based cut-off points of lipid profile and/or anthropometric measurements remains one of the challenges in prevention, early detection and control of non-communicable diseases. This study aimed to validate anthropometric-based screening of lipid profiles to develop locally appropriate optimal cut-off points for metabolic syndrome screening.
Methods: A community-based cross-sectional study was conducted among randomly selected 977 adults in Jimma Town, Ethiopia. Data were collected using structured questionnaire, anthropometric and biochemical measurements. Data were analyzed using SPSS windows version 21 and Kappa statistic was used to validate the agreement between anthropometric measurement and lipid profile. A p-value of < 0.05 was considered statistically significant.
Results: Body mass index (BMI) at ≥ 24.5 was used as screening of dyslipidemia (TG≥ 150mg/dl) with slight Kappa coefficient of 0.138 (P< 0.001) among females while it was ≥ 22.2 among males with fair (0.275) Kappa coefficient (P< 0.001). Waist circumference-based screening of dyslipidemia (TG≥ 150mg/dl) at ≥ 78.0cm had negative (− 0.005) Kappa coefficient (Pp< 0.001) among females (sensitivity: 72.6% and specificity: 26.7%). Yet, waist circumference at ≥ 83.7cm had slight Kappa coefficient of 0.13 (P< 0.005) among males (sensitivity: 38% and specificity: 74.9%). Waist hip ratio-based screening of dyslipidemia (TG≥ 150mg/dl) at ≥ 0.82 among females had negative (− 0.001) Kappa coefficient (p=0.763), whereas among males at ≥ 0.88, there was a slight (0.105) Kappa coefficient of (p=0.002) (sensitivity:77.5% and specificity:36.8%). This study showed that anthropometric-based high-density lipoprotein measurement was not applicable.
Conclusion: This study indicated that BMI-based screening of triglyceride was more applicable for both sexes than other anthropometric measurements. Waist circumference and waist-to-hip ratio-based screening of triglyceride were slightly applicable only for males. However, anthropometric-based screening of high-density lipoprotein measurement was not applicable for both sexes. In conclusion, researchers and policy makers need to consider locally validated cut-off points to be used for screening metabolic syndrome in the community.
Keywords: metabolic syndrome, lipid profile, anthropometric measurements, Jimma
Introduction
Metabolic syndrome is a subset of non-communicable diseases (NCDs), which is interconnected by physiological, biochemical, clinical and metabolic factors that directly increases the risk of cardiovascular disease and type 2 diabetes mellitus. Insulin resistance, visceral adiposity, atherogenic dyslipidemia, endothelial dysfunction, genetic susceptibility, elevated blood pressure, hypercoagulable state and chronic stress are among several factors which constitute the syndrome.1 Individuals with metabolic syndrome exhibit a characteristic pattern of abnormalities in serum lipid levels consisting of a low level of high density lipoprotein and an elevated level of triglyceride.2
Different studies show that the burdens of NCDs and their impact on the health of the population and health services are increasing in developing countries. Cardiovascular diseases, cancer, chronic respiratory diseases and diabetes are responsible for 82% of deaths. Currently, low income countries are witnessing epidemiological transition from infectious communicable diseases to chronic non-communicable diseases due to changes in lifestyles, rapid urbanization and diminishing levels of physical activity.3,4 Consequently, non-communicable diseases are predicted to increase globally by 17% and by 27% in the African region in the next 10 years, and projected to overtake communicable diseases as the major cause of morbidity in sub-Saharan Africa by the year 2030.3
The 2017 WHO report progress monitor also showed that NCDs kill 41 million people each year, which is 71% of all global deaths. In Ethiopia, the proportion of death from NCDs has been reported at 42% of all causes of deaths, which accounts for 27% of premature deaths before the age 70 years.5 The increment of NCDs on top of the preexisting highly prevalent communicable diseases, maternal, prenatal and nutritional conditions constrains the already meager health resources and hinders economic development of the country.6
However, it is only relatively recently that NCDs have received attention in low-income countries. Consequently, unrecognized/undiagnosed NCDs are found to be major problems as the individuals are unaware of their status in this regard. It has been indicated that the international anthropometric cutoff for detecting obesity is not appropriate for Ethiopians.7 There is a need to reorient the national health system to ensure recognition of the NCDs burden and improve organization and delivery of NCDs services at primary health care (PHC) level.8,9
Lack of local based cut-off points remains one of the challenges in management, prevention, and control of NCDs, and their modifiable risk factors. Studies show that the international cut-off points for different anthropometric measurements and body composition are not appropriate for the Ethiopian population; it leads to underestimation and misclassifies the risk of metabolic syndrome. Therefore, developing standardized local cut-off points for early detection of metabolic syndrome is crucial for prevention and management of NCDs. Thus, this study aimed to validate anthropometric cut-off points among Ethiopian adults7 through household level screening using waist circumference, waist-to-hip ratio and BMI measurement for estimation and classification of the risk of metabolic syndrome in Jimma Town, Oromia Regional State, Southwest Ethiopia.
Methods
Study Setting
A community-based cross-sectional study was conducted in Jimma Town from June to July 2019 among adults aged ≥18 years. Jimma is found in Southwest Ethiopia, located 352 km from the capital city of Addis Ababa. Sample size was calculated using sensitivity estimation formula10 taking highest prevalence of high density lipoprotein (23.4%) based on a study done in Addis Ababa among Ethiopian adults,11 5% margin of error, 95% confidence level and a 90% anticipated sensitivity.7 Finally, sample size of 977 was calculated by considering 10% non-response rate and 1.5 design effects. Study participants were selected using two-stage cluster sampling technique. Six kebeles (smallest administrative unit) out of 17 were randomly selected. Study participants were selected from each kebele proportionally based on the number of households in each selected kebele using systematic sampling technique.
Inclusion and Exclusion Criteria
All residents who lived in the town for six months prior to the data collection were included into the study. However, adults who had physical deformity (kyphosis and scoliosis), pregnancy, known chronic illness and serious illness were excluded.
Data Collection Procedure
Data were collected using WHO stepwise questionnaire and adapted to the local context. The survey tools included socio-demographic characteristics, anthropometric measurements and laboratory analyses of lipid profile. Height of the study participants was measured to the nearest 0.1 cm using a stadiometer (Seca GmbH & Co. KG, Germany) with the subjects positioned at the Frankfurt Plane and the four points (heel, calf, buttocks and shoulder) touching the vertical stand and their shoes taken off. Before starting the measurements, the stadiometer was checked using calibration rods. Weight was measured using digital weight scale to the nearest 0.1 kg with the subjects wearing light clothes and shoes taken off. The validity of the scale was checked using an object of a known weight of 1kg.
Waist circumference was measured at midpoint between the inferior margin of the last rib and the iliac crest just at wider area using a stretch tape. Just before taking the measurement, participants were requested to stand with their feet together, place their arms at the side of their body with the palms of their hands facing inwards, and breathe out gently. Hip circumference was measured at the level of the greater trochanter of the femur with the subjects wearing pants. All anthropometric measurements were done in triplicate and the average value was used for further analysis. Standardization of anthropometric measurers were done to reduce inter observer error.
The laboratory parameter was determined according to the standard operating procedures. Five 5 mL venous blood samples were collected to determine participant’s lipid profiles in mg/dl. Serum was carried out in ABX Pentra 400 Automated Chemistry Machine (Horiba ABX SAS, 34184) Montpellier12 at Jimma medium Clinical chemistry Core laboratory to determine lipid profile including total cholesterol, high-density lipoprotein (HDL) and triglyceride (TG). Low density lipoprotein (LDL) level was calculated by using Freidwald formula.13
The optimal cut-off values of waist circumference (WC) was 85.3 cm for male and 78.0 cm for females and the values greater than this indicates risk factor for over-nutrition. The optimal cut-off values of waist-to-hip ratio (WHR) were calculated by dividing waist-to-hip in centimeters. The cut-off values were 0.88 cm for male and 0.82 cm for females; values greater than the cut-off value was considered at risk for over-nutrition. Similarly the optimal cut-off of values body mass index (BMI) was 24.5kg/m2 for female and 22.2kg/m2 for male; values greater than the cut off value was considered as at risk for over-nutrition. A lipid level was classified according to WHO classification and triglyceride was considered as normal when it was <150 mg/dl and HDL-C was considered as normal if it is >40 mg/dl male and >50mg/dl for female.14
Data Quality Management
Data collectors were trained for four days before the actual data collection on interviewing approach, anthropometric measurement and data recording. To ensure the quality of the data, a properly designed data collection instrument was used. Calibration of instruments was done to increase the reliability of the measurements. A questionnaire for the survey was first prepared in English language and translated into local languages (Afan-Oromo and Amharic), then back-translated into English to check for consistency. The questionnaire was pretested on 5% of sample size in Agaro Town and based on the pretest, additional adjustments were made based on identified gaps.
Data Processing and Analysis
Data were checked for completeness. The data were cleaned and checked for outliers and missing values. Epi Data version 3.1 and SPSS version 21 were used for data entry and analysis, respectively. The data were checked for normality using QQ-plot. Descriptive analysis was used to describe the study subjects and presented using tables and figures. Validity measures including sensitivity, specificity, positive predictive value, negative predictive value and kappa agreement were used to validate anthropometric based screening of lipid profile. The Kappa coefficient was used to measure the agreement between local anthropometric cut-off points and lipid profiles; and the kappa coefficient were classified as perfect (k=0.81–1.00), substantial (k=0.61–0.80), moderate (k=0.41–0.60), fair (k=0.21–0.40), slight (k=0.01–0.20) and no or poor agreement (k=0).7,15
Results
A total of 915 individuals were included into this study with a 93.7% response rate. The mean age of study participants was 38.35±13.51 years. A large proportion of the respondents (71.5%) were married. The majority of participants were Oromo ethnic (66.0%) and Muslim followers (56.0%). Close to three-fourths (64.5%) of the study participants attended at least primary school (Table 1).
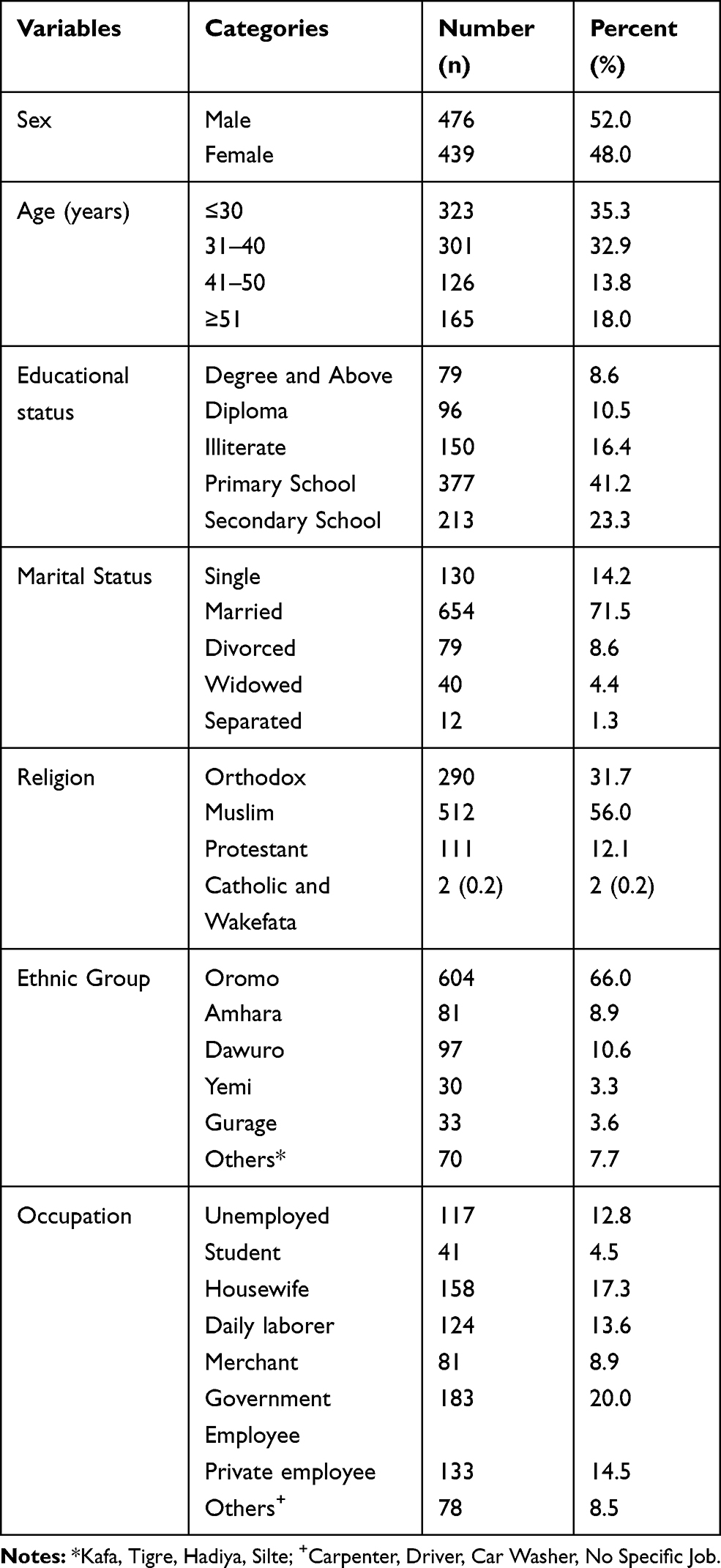 |
Table 1 The Socio-Demographic Characteristics of Adults in Jimma Town, Ethiopia |
BMI-based screening of triglyceride in both sexes had slight Kappa agreement among female and fair agreement among males. Using BMI at ≥24 for screening of hyper triglyceride (TG ≥150mg/dl) among females showed slight (0.12) Kappa agreement (P=0.024) with 72.6% sensitivity and 65.0% specificity. Similarly, in case of male, BMI at ≥22.2kg/m2 based screening of dyslipidemia (TG≥150mg/dl) had fair (0.275) Kappa agreement (P<0.001) with 64.1% sensitivity and 66.8% specificity. Body mass index-based screening of high-density lipoprotein (HDL-C<50mg/dl) among females at ≥24.5kg/m2 had negative (−0.003) Kappa coefficient with 58.0% sensitivity and 41.7% specificity, which is not statistically significant (p=0.949). Similarly, BMI at ≥22.2kg/m2 had a slight (0.032) Kappa coefficient (P=0.449) with 58.1% sensitivity and 45.45% specificity (Table 2).
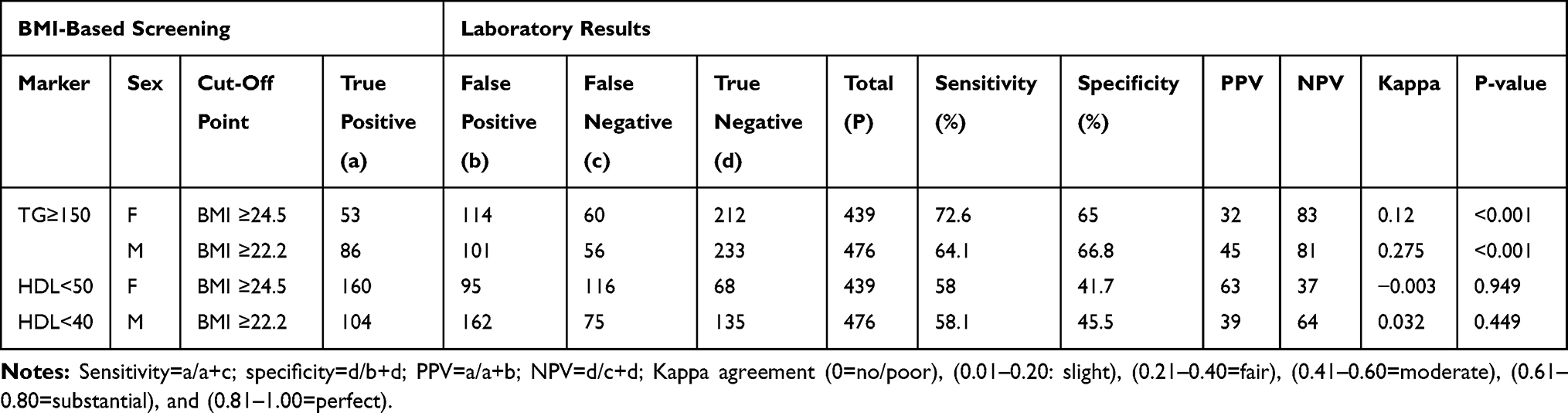 |
Table 2 Comparison of BMI-Based Screening of Triglyceride and HDL with Laboratory Results Among Jimma Town Adults, Ethiopia |
Waist circumference based screening of dyslipidemia (TG≥150mg/dl) at ≥78.0 among females had −0.005 Kappa coefficient with 72.6% sensitivity and 26.7% specificity, which was not statistically significant (p= 0.877). On the other hand, for males, waist circumference at ≥83.7cm based screening of dyslipidemia (TG≥150mg/dl) had slight Kappa agreement of 0.13 (p=0.005) with 38.0% sensitivity and 74.9%, specificity.
Waist circumference based screening of high-density lipoprotein cholesterol (<50mg/dl) at ≥78.0cm had slight Kappa coefficient (0.04) with 27.5% sensitivity and 77.3%, specificity which was not statistically significant (p=0.263). Similarly, for male waist circumference ≥83.7cm based screening of HDL-C had slight Kappa coefficient of 0.02, but not statistically significant (Table 3).
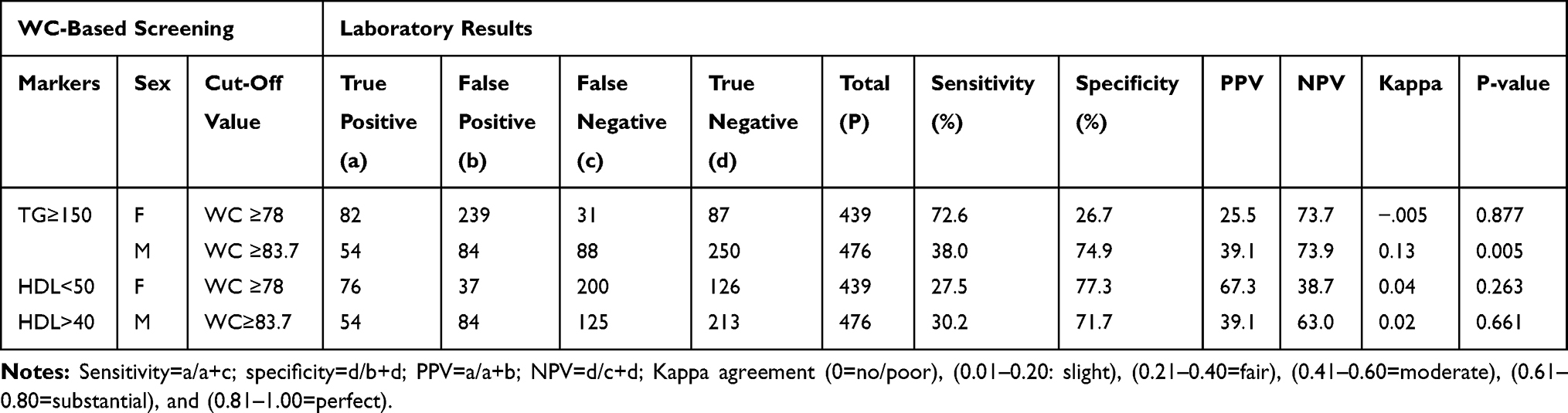 |
Table 3 Comparison of Waist Circumference-Based Screening of Triglyceride and HDL with Laboratory Results Among Adults, Jimma Town, Ethiopia |
Waist circumference to hip ratio based screening of triglyceride was valid only for male at ≥0.88 cm with slight (0.105) Kappa coefficient (p=0.002) and 77.46% sensitivity and 36.83% specificity. However, in case females, WHR at ≥0.82cm was not statistically significant. WHR based screening of high-density lipoprotein cholesterol was not statistically significant for both female (p=0.263), and male (p=0.661) (Table 4).
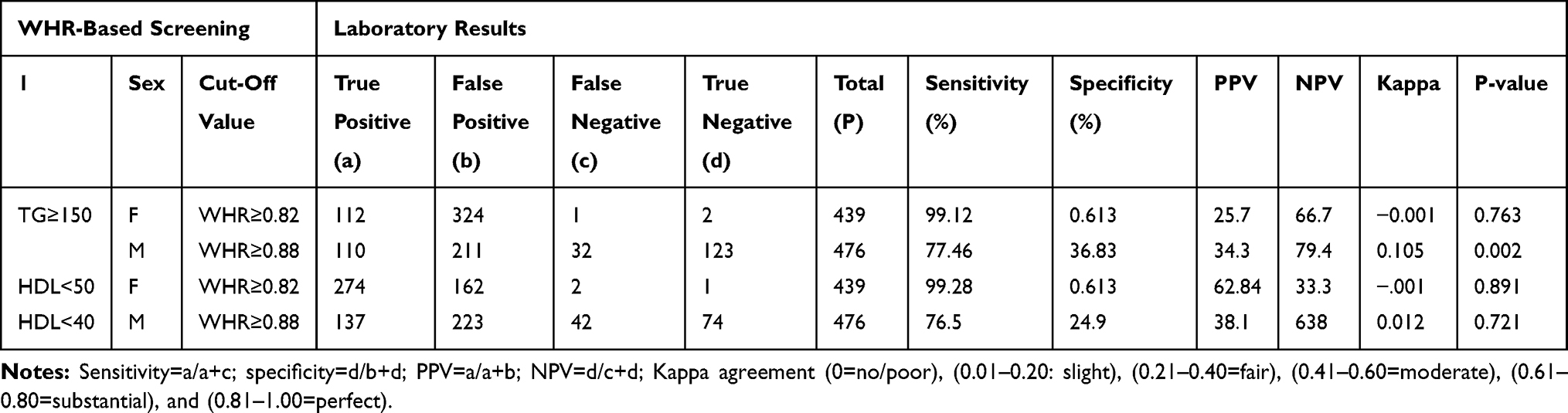 |
Table 4 Comparison of WHR-Based Screening of Triglyceride and HDL with Laboratory Results Among Adults, Jimma Town, Ethiopia |
Discussion
Developing locally appropriate optimal cut-off points using obesity based anthropometric measurement is important for early detection of metabolic syndrome to prevent farther complication and disabled from unrecognized NCD.7 According to the present study, BMI-based screening of triglyceride had fair and slight agreement of Kappa coefficient among males and females, respectively. This finding indicate that though the cut-off points for BMI is not the same for males (≥22.2kg/m2) and females (≥24 kg/m2) like the international cut-off points, it can be used to early detect dyslipidemia among Ethiopian adults. A similar study done in Brazil also revealed that anthropometric indices had slight differences in screening of triglyceride among males and females. This study also revealed that BMI-based screening of triglyceride was applicable when compared with other anthropometric measurements.16 Likewise, other hospital-based studies done in India, Canada and others indicated presence of correlation between BMI and lipid profiles.17–19 However, in this study no significant association was observed between local BMI cut-off points and other lipid profiles like high and low density lipoprotein.
Waist circumference based screening of triglyceride among males showed slight agreement (k=0.13). However, similar studies from Canada and India found that waist circumference was a better predictor of dyslipidemia (TG) in both sexes.18,20,21 Similar to waist circumference, the screening of triglyceride based on wait to hip ratio among males had slight Kappa agreement (k=0.105), which is statistically significant (p=0.002). Study done in India among adult population (≤ 60 years old) and aged group of population in Brazil (60 years old and above) revealed that anthropometric indices of waist to hip ratio was the best indicators for screening dyslipidemia (TG).16,22 This discrepancy might be due to the difference in sample size, age difference or ethnic differences, which can be addressed by a large scale and multi-centered study involving different populations.
Limitations of the Study
Anthropometric measurements are prone to errors. However, this study was conducted with highest precautions in training the anthropometric data collectors, equipment calibration and standardization of procedure to minimize the possibility of error occurrence.
Conclusion
Anthropometric indices can be used as a simple screening for dyslipidemia at primary health care unit. BMI cut-off points at ≥24.5 kg/m2 for females and ≥22.2kg/m2 for males can be used for screening of dyslipidemia (TG≥150mg/dl). Similarly, waist circumference at ≥83.7cm and waist to hip ratio at ≥0.88 can be considered as screening of dyslipidemia (TG≥150mg/dl) among males. Generally, with a further investigation healthcare providers and researchers can use locally validated anthropometric indices as alternative to investigate lipid profiles to be used in the prevention and management of metabolic syndrome and other non-communicable diseases.
Abbreviations
TG, triglycerides; HDL, high-density lipoprotein; LDL, low-density lipoprotein; WC, waist circumference; WHR, waist-to-hip ratio; BMI, body mass index.
Data Sharing Statement
The deidentified datasets used for this study are available from the corresponding author on reasonable request.
Ethical Approval
Ethical approval was obtained from Jimma University Ethical Review Board (Ref. IHRPGD/339/2019) and the study was conducted in accordance with the principles of the Declaration of Helsinki. The verbal consent was taken from study subjects based on the ethical approval letter granted by Jimma University. Prior to the first interview each respondent was informed about objective of the study and privacy during the interview. The privacy of study participants was respected and results regarding the participants made confidential.
Acknowledgments
The authors would like to express their gratitude to Jimma University for facilitating this study. We would also like to thank study participants who gave valuable information.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed on the journal to which the article will be submitted; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the publication of the article.
Disclosure
The authors declare that they have no competing interests.
References
1. Kaur J. A comprehensive review on metabolic syndrome. Cardiol Res Pract. 2014;2014:943162. doi:10.1155/2014/943162
2. Brinck J, Thomas A, Lauer E, et al. Diabetes mellitus is associated with reduced high-density lipoprotein sphingosine-1-phosphate content and impaired. Arterioscler Thromb Vasc Biol. 2016;36(5):817–824. doi:10.1161/ATVBAHA.115.307049
3. World Health Orgnaztion. Global report on diabetes; 2016. Available from: https://apps.who.int/iris/bitstream/10665/204871/1/9789241565257_eng.pdf.
4. Kavishe B, Biraro S, Baisley K, et al. High prevalence of hypertension and of risk factors for non-communicable diseases (NCDs): a population based cross-sectional survey of NCDS and HIV infection in Northwestern Tanzania and Southern Uganda. BMC Med. 2015;13(1):126. doi:10.1186/s12916-015-0357-9
5. Shiferaw F, Letebo M, Misganaw A, et al. Non-communicable diseases in Ethiopia: disease burden, gaps in health care delivery and strategic directions. Ethiop J Health Dev. 2018;32(3).
6. Misganaw A, Haregu T, Deribe K, Tessema G, Deribew A. National mortality burden due to communicable, non-communicable, and other diseases in Ethiopia, 1990 – 2015: findings from the Global Burden of Disease Study 2015. Popul Health Metr. 2017;15(1):29. doi:10.1186/s12963-017-0145-1
7. Sinaga M, Worku M, Yemane T, et al. Optimal cut-off for obesity and markers of metabolic syndrome for Ethiopian adults. Nutr J. 2018;17(1):109. doi:10.1186/s12937-018-0416-0
8. Federal Democratic Republic of Ethiopia. The Ethiopia Noncommunicable Diseases and Injuries (NCDI) commission report summary: addressing the impact of noncommunicable diseases and injuries in Ethiopia. Available from: https://static1.squarespace.com/static/55d4de6de4b011a1673a40a6/t/5bfc17ab21c67c558106119e/1543247788342/Ethiopia+NCDI+Commission+Report+Summary+FINAL.pdf.
9. Asfaw D, Teshome E. Tobacco control and prevention efforts in Ethiopia pre- and post-ratification of WHO FCTC: current challenges and future directions. Tob Induc Dis. 2019;17:13. doi:10.18332/tid/102286
10. Sorana D. Medical diagnostic tests: a review of test anatomy, phases, and statistical treatment of data. Comput Math Methods Med. 2019;2019:1891569. doi:10.1155/2019/1891569
11. Gebreyes Y, Goshu D, Geletew T, et al. Prevalence of high bloodpressure, hyperglycemia, dyslipidemia, metabolic syndrome and their determinants in Ethiopia. PLoS One. 2018;13(5):e0194819. doi:10.1371/journal.pone.0194819
12. Green R, Wachsmann-Hogiu S. Development, history, and future of automated cell counters. Clin Lab Med. 2015;35(1):1–10. doi:10.1016/j.cll.2014.11.003
13. Hajian-Tilaki K. Sample size estimation in diagnostic test studies of biomedical informatics. J Biomed Inform. 2014;48:193–204. doi:10.1016/j.jbi.2014.02.013
14. Sinaga M, Yemane T, Tegene E, Lidstrom D, Belachew T. Performance of newly developed body mass index cut-off for diagnosing obesity among Ethiopian adults. J Physiol Anthropol. 2019;38(1):14. doi:10.1186/s40101-019-0205-2
15. Cohen W. A coefficient of agreement for nominal scales. Educ Psychol Meas. 1960;20(1):37–46. doi:10.1177/001316446002000104
16. Silva R, Fares D, Rodrigues A, Dél T, Matos W, Henrique M. Anthropometric indicators as predictors of serum triglycerides and hypertriglyceridemia in older adults. MedicalExpress. 2014;1(4):202–205. doi:10.5935/MedicalExpress.2014.04.08
17. Manjareeka M, Nanda S, Mishra J, Mishra S. Correlation between anthropometry and lipid profile in healthy subjects of Eastern India. J Midlife Health. 2015;6(4):164–168. doi:10.4103/0976-7800.172302
18. Brenner D, Tepylo K, Eny K, Cahill L, El-Sohemy A. Comparison of body mass index and waist circumference as predictors of cardiometabolic health in a population of young Canadian adults. Diabetol Metab Syndr. 2010;2(1):28. doi:10.1186/1758-5996-2-28
19. Ramoteme L, Martinique S, Sarah J, Makama A. The association between dyslipidemia and anthropometric indicators in black and white adolescents residing in tlokwe municipality, North-West Province, South Africa: the PAHL study. Afr Health Sci. 2011;14(4):929–938. doi:10.4314/ahs.v14i4.23
20. Rao S, Parab-Waingankar P. Performance of waist circumference relative to BMI in predicting risk of obesity and hypertension among affluent Indian adults. Health (Irvine Calif). 2013;05(08):16–22. doi:10.4236/health.2013.58A3003
21. Silvana C, Miralles W, Wollinger LM, et al. Waist-to-height ratio (WHtR) and triglyceride to HDL-c ratio (TG/HDL-c) as predictors of cardiometabolic risk. Nutr Hosp. 2015;31(5):2115–2121. doi:10.3305/nh.2015.31.5.7773
22. Rocha F, Menezes TN, Melo RL, Pedraza DF. Correlation between indicators of abdominal obesity and serum lipids in the elderly. Rev Assoc Med Bras. 2013;59(1):48–55.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.